Back to Journals » Clinical Interventions in Aging » Volume 20
Developing a LASSO Regression-Based Nomogram to Predict Outcomes in Abdominal Aortic Aneurysm Patients Post-Endovascular Aneurysm Repair
Authors Yu F ![]() , Shen D, Lv Y, Zhang G, Yuan P, Cao C, Yang Y, Tang J, Zhang J
, Shen D, Lv Y, Zhang G, Yuan P, Cao C, Yang Y, Tang J, Zhang J
Received 31 August 2024
Accepted for publication 18 July 2025
Published 28 November 2025 Volume 2025:20 Pages 2241—2253
DOI https://doi.org/10.2147/CIA.S493841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Fengyi Yu,1– 4,* Dexin Shen,5,* Yan Lv,1– 4 Ge Zhang,1– 4 Peiyu Yuan,1– 4 Chenxi Cao,1– 4 Yu Yang,1– 4 Junnan Tang,1– 4 Jinying Zhang1– 4
1Department of Cardiology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, 450052, People’s Republic of China; 2Henan Province Key Laboratory of Cardiac Injury and Repair, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, 450052, People’s Republic of China; 3Henan Province Clinical Research Center for Cardiovascular Diseases, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, 450052, People’s Republic of China; 4Henan Key Laboratory of Chronic Disease Prevention and Therapy & Intelligent Health Management, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, 450052, People’s Republic of China; 5Department of Intensive Care Unit, Joint Logistics Force No. 988 Hospital, Zhengzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Junnan Tang, Department of Cardiology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, 450052, People’s Republic of China, Email [email protected] Jinying Zhang, Department of Cardiology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, 450052, People’s Republic of China, Email [email protected]
Introduction: This study aimed to develop a prognostic model to predict outcomes in patients undergoing endovascular aneurysm repair (EVAR) for abdominal aortic aneurysms (AAA).
Methods: 304 participants were divided into training and validation sets in a 7:3 ratio. Six risk factors were identified using LASSO regression, univariate, and multivariate Cox regression analyses: history of stroke, CIA atherosclerosis, age, hemoglobin levels, monocyte count, and large AAA. A nomogram was constructed to predict 1-year and 3-year all-cause mortality (ACM).
Results: A total of 304 AAA patients who underwent EVAR were included in this study (84.87% male; median age 72 [IQR: 65– 77] years). The model showed good predictive performance, with area under the curve (AUC) values of 0.84 (95% CI: 0.79– 0.89) and 0.81 (95% CI: 0.76– 0.86) for 1-year and 3-year mortality in the training set, and 0.71 (95% CI: 0.62– 0.80) and 0.80 (95% CI: 0.73– 0.87) in the validation set.
Discussion: These results suggest the model’s effectiveness in aiding clinicians with risk stratification and tailoring treatment strategies for post-EVAR patients.
Keywords: abdominal aortic aneurysm, prognosis, endovascular aneurysm repair, nomogram
Introduction
An abdominal aortic aneurysm (AAA) is a medical condition characterized by the progressive and irreversible expansion of the aorta. AAA is defined as an enlargement greater than 3 cm or 1.5 times the size of a normal aortic size, typically identified through computed tomography (CT) scans or intravascular ultrasonography. The prevalence of AAA is about 5.5 occurrences per 10,000 males and 1.1 per 10,000 females.1–3 AAAs can grow over time and may eventually rupture, accounting for 1%–2% of the total mortality rates.4 Surgical intervention is often necessary for large AAAs due to the significant risk of rupture. Recently, endovascular aneurysm repair (EVAR) has emerged as a preferred treatment option for AAA patients because it is less invasive and generally requires a shorter hospital stay.5 However, the risk factors associated with mortality for patients undergoing EVAR have yet to be thoroughly examined.
Certain features are associated with worse outcomes in EVAR patients, including large preoperative AAA diameter, infrarenal neck diameter, and aortic thrombus.6,7 While previous studies have explored demographic and morphological risk models, focusing on factors such as gender and cardiovascular history,8,9 there has been limited emphasis on laboratory data. To bridge this gap, we utilized LASSO regression, a method adept at simplifying models and avoiding multicollinearity, making it particularly suitable for clinical application. This approach established a more streamlined and interpretable model, which could assist clinicians in efficiently identifying high-risk EVAR patients. Consequently, in this article, we developed and validated a nomogram with LASSO Cox regression analysis to predict the all-cause mortality (ACM) of AAA in post-EVAR patients.
Materials and Methods
Study Population
AAA patients were enrolled from March 2015 to May 2023 at the First Affiliated Hospital of Zhengzhou University. The inclusion criteria were as follows: (1) AAA diagnosed with computed tomographic angiography (CTA) reports indicating an abdominal aortic diameter larger than 3 cm or 1.5 times the size of a normal aorta, (2) patients undergoing EVAR during hospitalization, and (3) patients ≥ 18 years old. The exclusion criteria were as follows: (1) known history of tumor and immune disease, (2) Marfan syndrome, (3) failed follow-up, (4) ruptured AAA, (5) receiving open surgery. A total of 304 AAA patients were included in this study and were randomly divided into training and validation sets in a 7:3 ratio. The training set was used to construct the nomogram to enhance model accuracy, while the testing set was used for validation. The flowchart of the study is illustrated in Figure 1.
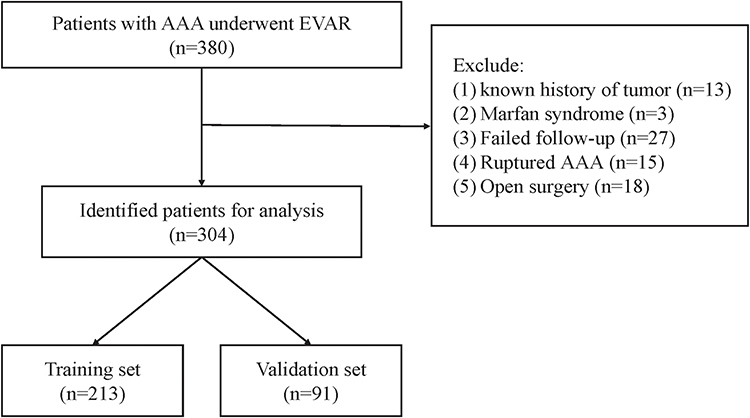 |
Figure 1 Flowchart of Patient Selection and Dataset Division for Analysis. |
The patients underwent standard preoperative evaluation and EVAR procedure with commercially available infrarenal aortic endograft according to clinical guidelines. All procedures included in this analysis were elective EVAR; emergency procedures for ruptured AAA were excluded due to their distinct clinical characteristics and outcomes.
Endpoint and Follow-Up
The primary endpoint of this study was ACM. The median follow-up time of the study was 24 (16–33) months, and the follow-up data on patients’ conditions was obtained through clinic visits. All data involved in the study was collected and preserved in a manner ensuring that none of the subjects could be identified. The study protocol was approved by the ethics committee of the First Affiliated Hospital of Zhengzhou University.
Clinic and Demographic Characteristics
Blood samples were collected from fasting patients at least 8 hours before EVAR. The collected demographic data included gender, age, smoking status, drinking status and medication history.
Coronary artery disease (CAD) was characterized by a documented history of angina, myocardial infarction, or procedures aimed at coronary revascularization. Similarly, diabetes, hypertension, a prior occurrence of stroke, and chronic obstructive pulmonary disease (COPD) were defined based on previous diagnoses and respective treatment.
The measured laboratory data, including white blood cell (WBC), hemoglobin, neutrophil, lymphocyte, monocyte, low-density lipoprotein cholesterol (LDL-C), fasting blood glucose (FBG), and estimated glomerular filtration rate (eGFR), were collected on the first day of hospitalization after 8-hour fasting.
CTAs were performed with scanners in the First Affiliated Hospital of Zhengzhou University. Data obtained from three-dimensional CTA images included common iliac artery (CIA) atherosclerosis, intraluminal thrombus (ILT) in the aneurysm, AAA diameter, AAA volume, and neck angulation based on the standard measurement method.10 Large AAA was defined as 5.5 cm in males and 5 cm in females. We define a current smoker as an individual who has smoked more than five packs in their lifetime and currently smokes on some days or every day.
Model Construction
In this study, we employed the LASSO regression method to identify key predictors of ACM in post-EVAR patients. LASSO regression performs both variable selection and regularization, improving model accuracy and interpretability. The λ parameter, a critical component of the LASSO method that controls the strength of the penalty applied to the regression coefficients, was selected using a 10-fold cross-validation approach. This technique involves partitioning the dataset into 10 subsets and iteratively training the model on 9 subsets while validating it on the remaining subset to optimize predictive accuracy and prevent overfitting. The choice of λ directly influences the model’s robustness: a higher λ results in greater regularization, potentially excluding more variables to create a simpler and more generalizable model. In contrast, a lower λ might include more variables, improving the model fit but at the risk of capturing noise and overfitting. The final λ value was chosen to achieve a balance between model complexity and predictive power, as demonstrated by the minimized mean squared error observed during cross-validation.
Cox regression analyzes the time to an event while accounting for various covariates. It was employed to determine which selected risk factors independently predict ACM in post-EVAR patients. Parameters with a P value less than 0.05 in the univariate Cox regression analysis were then included in the multivariate Cox regression analysis. To refine the multivariable Cox regression model, we employed the Akaike Information Criterion (AIC)-stepwise method for model selection. The AIC-stepwise approach involves iteratively adding or removing variables based on their contribution to the model’s overall fit, as measured by the AIC score. The AIC balances model complexity and goodness-of-fit by penalizing the inclusion of additional variables that do not significantly enhance predictive power. Variables were sequentially added or removed from the model based on whether their inclusion or exclusion improved the AIC score, continuing until the model with the lowest AIC was identified. This stepwise process ensured that the final model was both parsimonious and robust, including only those variables that provided independent and significant contributions to the prediction of ACM.
Time-dependent receiver operating characteristic (ROC) curves and the area under the curve (AUC) assess the model’s ability to discriminate between different outcomes. They were used to evaluate the predictive accuracy of the nomogram for 1-year and 3-year ACM in post-EVAR patients.
Youden’s Index is a statistic used to determine the optimal cutoff point for a diagnostic test. It is defined as J = Sensitivity + Specificity − 1, where sensitivity is the true positive rate and specificity is the true negative rate. The index ranges from 0 to 1, with higher values indicating better test performance. The optimal cutoff maximizes Youden’s Index, balancing sensitivity and specificity to distinguish between different patient outcomes effectively. We plotted calibration curves to analyze the concordance between predicted mortality and observed ACM events, using bootstrapping with 1000 resamples.
Statistical Analysis
The Kolmogorov–Smirnov test was employed to assess normal distribution, all the continuous variables were not normally distributed, therefore Mann–Whitney U-tests were used for group comparison. Kaplan-Meier (KM) analysis was employed to demonstrate the risk stratification ability of the model. Decision curve analysis (DCA) was utilized to estimate clinical utility. Post hoc power analysis is used to evaluate the adequacy of sample size. All analyses and model development were performed using R Version 4.1.2, and the packages used for analysis are listed in Supplementary Table 1. A two-sided p-value < 0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 304 patients were enrolled in the study based on the exclusion and inclusion criteria. The median age of the population was 72 (65–77), including 46 (15.13%) females and 258 (84.87%) males. 32 (10.53%) and 187 (61.51%) patients were diagnosed with type 2 diabetes (T2DM) and hypertension, respectively. 54 (17.76%) patients had a history of stroke. 159 (52.30%) and 113 (37.17%) patients were diagnosed with CIA atherosclerosis and large AAA based on CTA results. The overall dataset was divided into the training (n = 213) set and validation set (n = 91). There were no significant differences observed between the two datasets (Table 1), suggesting random and reasonable grouping.
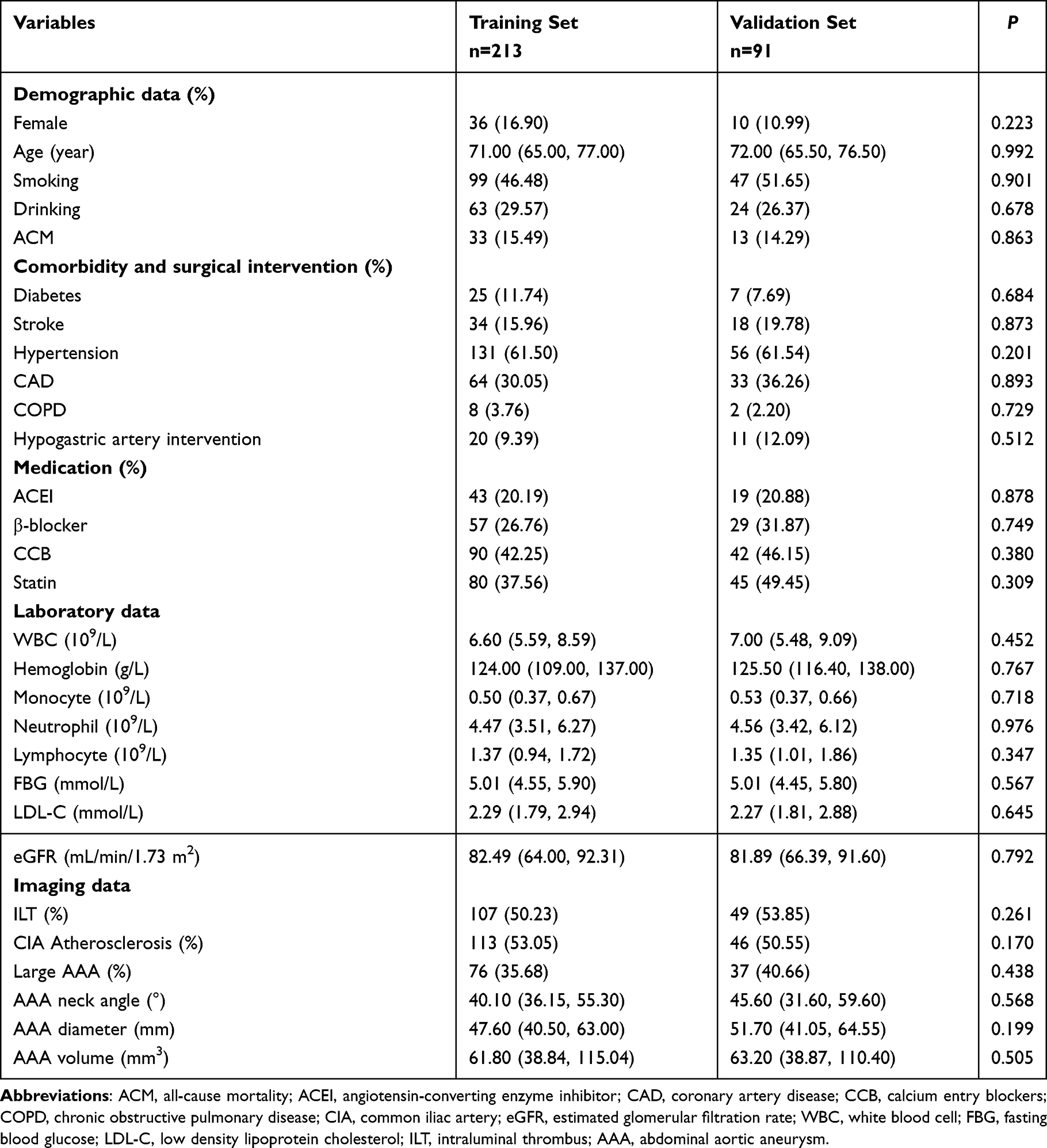 |
Table 1 Clinical Characteristics of Patients in Training and Validation Cohorts |
There was no endoleak reported during hospitalization. During the follow-up period, 46 ACM events were reported (Table 2). Among them, 30 (65.22%) were related to aneurysm and 6 (13.04%) were linked to cardiac death. Notably, the rate of stroke in the ACM group (30.43%) was significantly higher than in the non-ACM group (15.50%). The WBC, and monocyte levels were significantly higher, while the hemoglobin level was lower. Moreover, ACM was inclined to occur in patients with advanced age, ILT, CIA atherosclerosis, larger AAA diameter and volume, which was consistent with our assumptions.
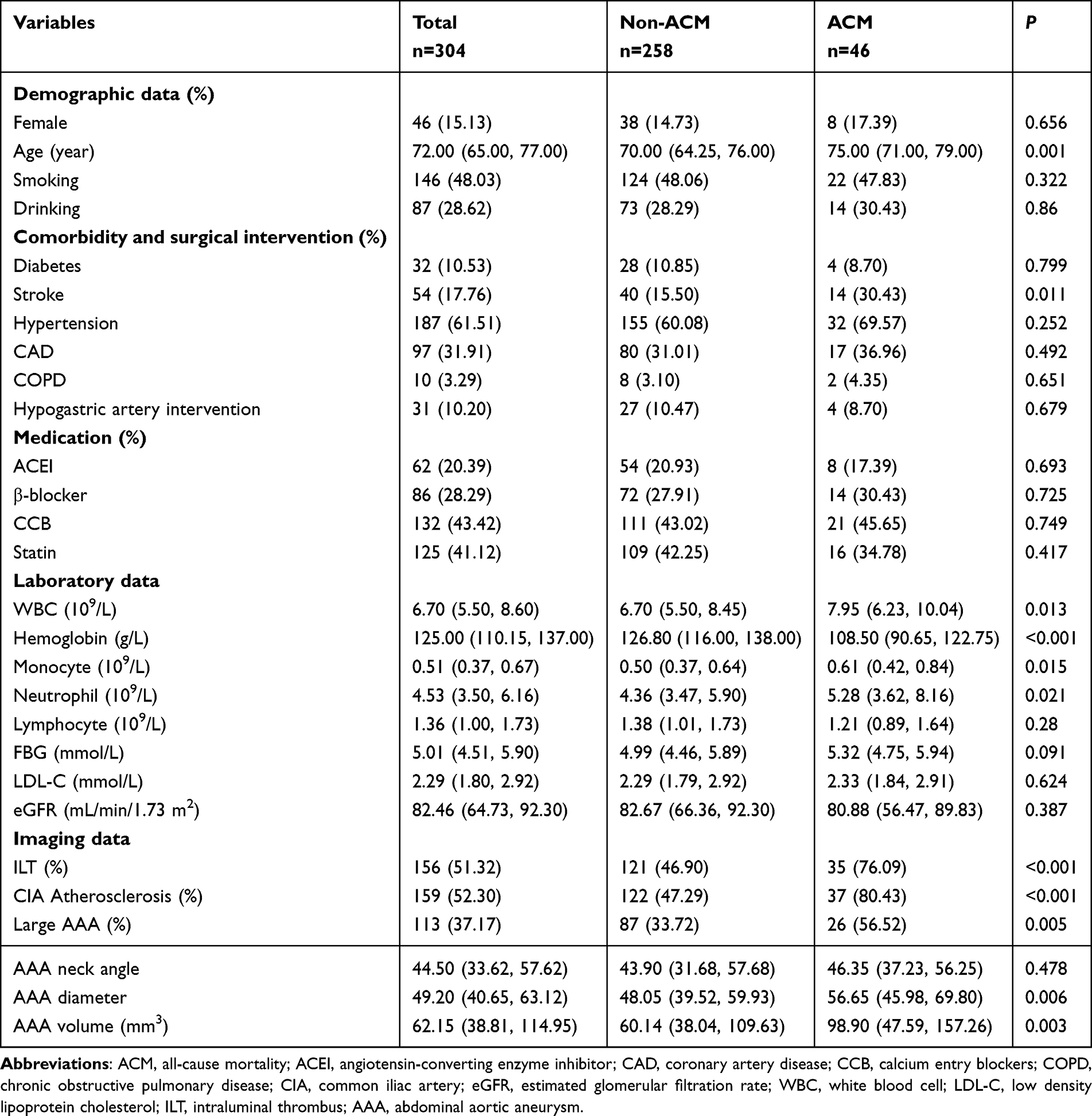 |
Table 2 Clinical Characteristics of Patients with or Without ACM Events |
Variable Analysis and Selection
LASSO regression was used to select variables, effectively addressing multicollinearity and overfitting, and enhancing model interpretability. Figure 2a showed the variation of the parameter coefficients. The model variables were reduced to seven upon achieving the minimum mean squared error of log(λ), and further reduced to five when it reached a standard error (onefold SE) of the minimum distance, as determined by the 10-fold cross-validation (Figure 2b). We preferred to choose the optimal log(λ) and involve seven parameters in the Cox regression analysis.
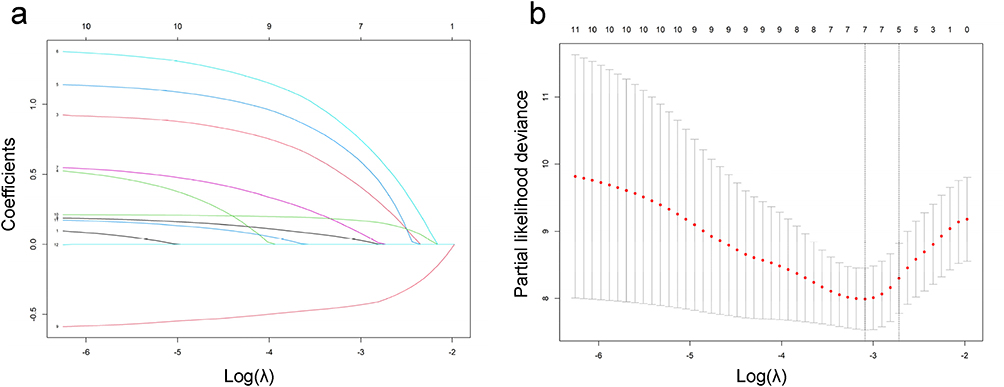 |
Figure 2 Regularization Path and Model Selection for LASSO Regression. (a) Parameter coefficient variation plot. (b) Ten-fold cross-validation identifying optimal log(λ) values. |
Parameters with P < 0.05 in the univariable Cox analysis were entered into the multivariable Cox analysis (Table 3), and the six following variables were independent risk factors of ACM: history of stroke (HR=3.59, 95% CI: 1.67–7.70), CIA atherosclerosis (HR=4.48, 95% CI: 1.92–10.49), age (HR=1.54, 95% CI: 1.07–2.23), hemoglobin (HR=0.53, 95% CI: 0.37–0.76), monocyte (HR=1.28, 95% CI: 1.11–1.47), and large AAA (HR=3.09, 95% CI: 1.43–6.72).
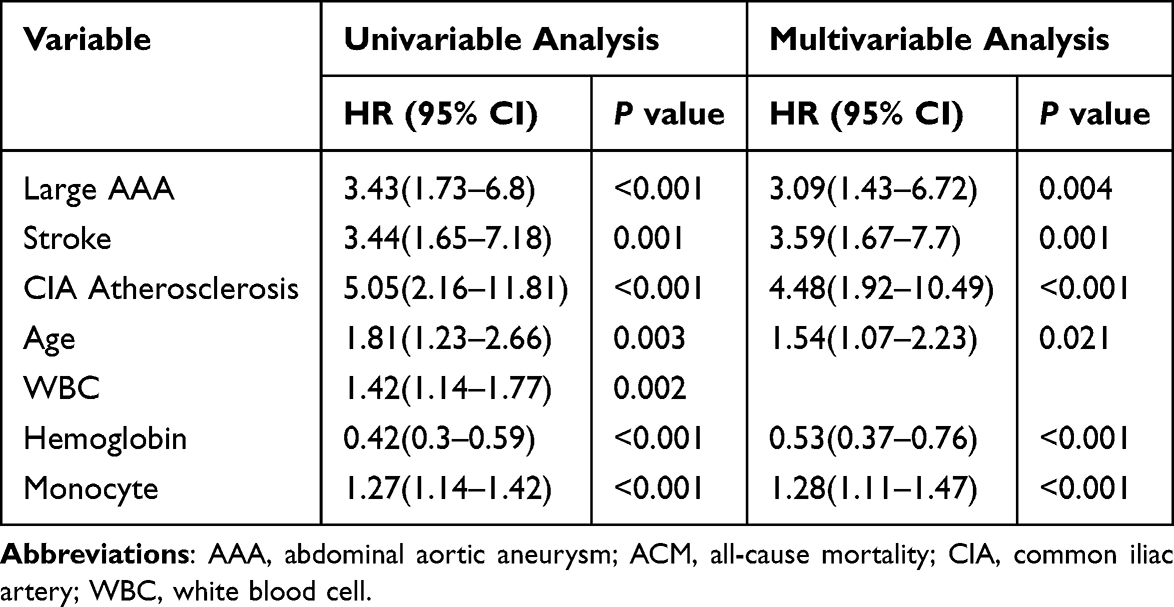 |
Table 3 Univariable and Multivariable Cox Analysis Results |
Nomogram Construction
Based on the six variables, a prognostic nomogram predicting 1- and 3-year mortality for post-EVAR patients was developed with the rms package (Figure 3a). In the nomogram, distinct points on the scale were assigned to each level of the variables. To use the nomogram, the variable of interest was initially located on the horizontal axis of the nomogram, and a straight line was drawn vertically from the variable’s value to the corresponding point on the vertical axis of the nomogram. This process was repeated for each variable included in the model. Once the points for all variables were determined, a cumulative score was derived for each patient by summing the assigned points, and the estimated probabilities of ACM events within the 1- and 3-year timeframes were determined.
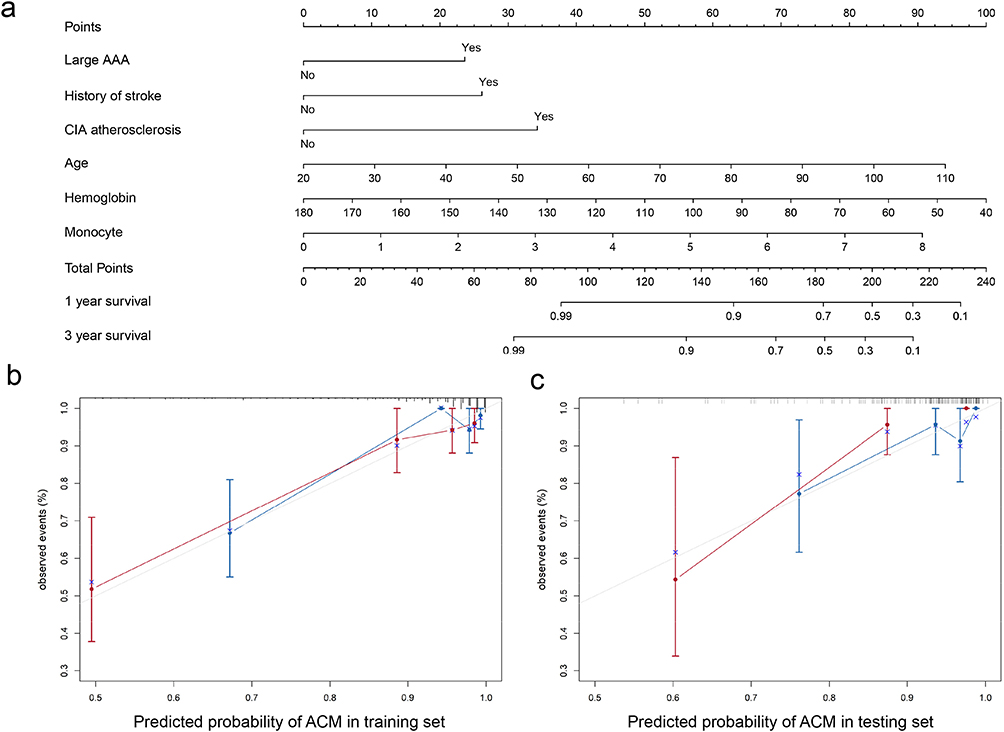 |
Figure 3 Nomogram for Predicting Survival (a) and Calibration Plots for Training (b) and Validation Cohorts (c). |
Model Performance and Clinical Utility
In the internal validation cohort, 13 ACM events (14.39%) were observed during the follow-up period. Calibration curves demonstrated strong concordance between predicted and observed ACM probabilities in both training and validation cohorts (Figure 3b and c), confirming the nomogram’s reliability. Time-dependent ROC curves revealed excellent discriminative performance with AUCs at years 1 and 3 of 0.84 (95% CI: 0.79–0.89) and 0.81 (95% CI: 0.76–0.86) in the training set (Figure 4a), and 0.71 (95% CI: 0.62–0.80) and 0.80 (95% CI: 0.73–0.87) in the validation set (Figure 4b).
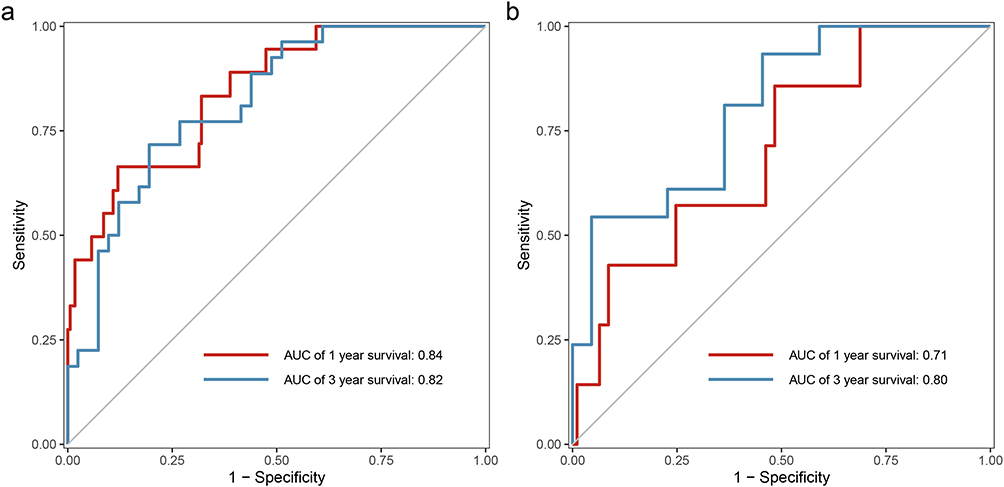 |
Figure 4 ROC Curves for 1-Year (a) and 3-Year (b) Survival Predictions in Training and Testing Sets. |
We employed Youden’s Index to determine the optimal cutoff score (155.1) in the total dataset and stratified patients into high- and low-risk groups. Kaplan-Meier curves demonstrated satisfactory discrimination in both training (Figure 5a) and testing sets (Figure 5b) with statistically significant differences between risk groups (log-rank P<0.05).
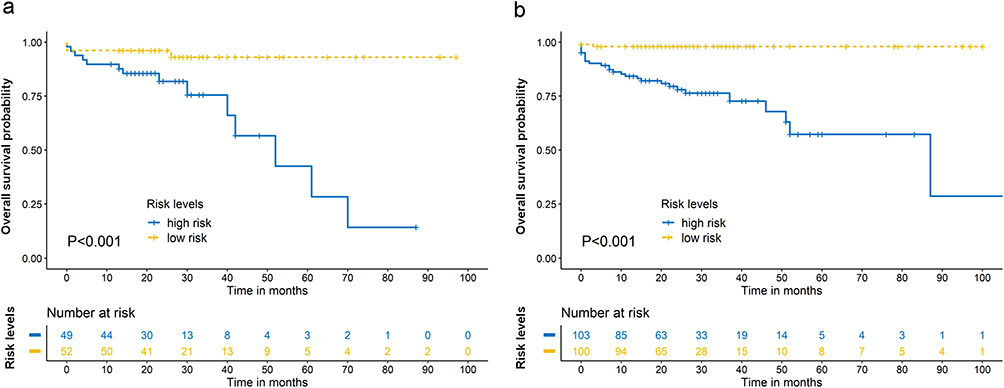 |
Figure 5 Kaplan-Meier Survival Curves for High and Low Risk Groups in Training (a) and Testing (b) Sets. |
Decision curve analysis (DCA) confirmed the clinical utility of our model, demonstrating effective prediction of 1- and 3-year survival (Figure 6). The model’s calibration was assessed using time-dependent Brier scores, which were 0.0691 at 1 year and 0.1136 at 3 years—both lower than the Kaplan-Meier reference model (0.0759 and 0.1203, respectively). These results indicate superior predictive accuracy with good calibration across both short-term and long-term follow-up periods.
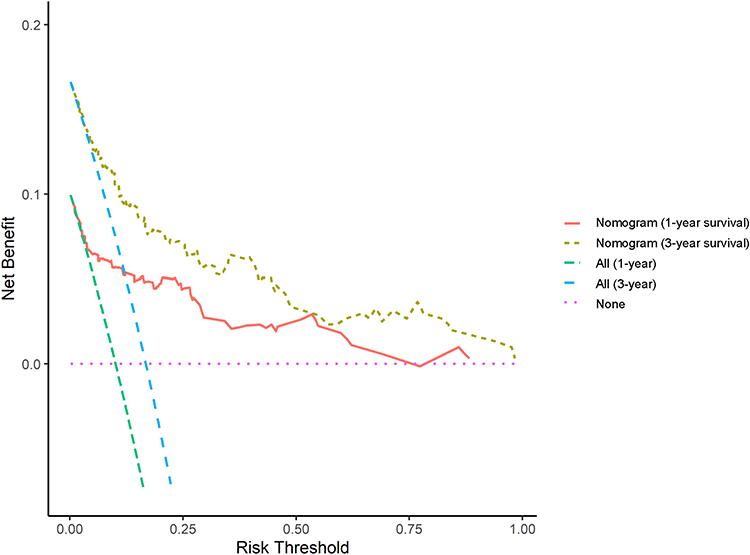 |
Figure 6 Decision Curve Analysis for 1-Year and 3-Year Survival Predictions Using Nomogram. |
A post hoc power analysis based on CIA atherosclerosis—one of the most significant predictors in the final multivariable Cox model (HR = 4.48)—confirmed adequate statistical power. Given the observed event rates (80.43% in the ACM group vs 47.29% in the non-ACM group), the calculated power exceeded 99% using a two-sided test with α = 0.05, confirming sufficient sample size for reliable conclusions.
Discussion
With the increasing population of patients undergoing EVAR, there is a growing need for predictive tools as well. This study employed LASSO-Cox regression analysis to develop a predictive model based on data from our center. Six parameters were associated with ACM events, and these included a history of stroke, CIA atherosclerosis, age, hemoglobin, monocyte, and large AAA. A nomogram was constructed based on those factors to predict outcomes for AAA patients after EVAR, which was validated in internal validation cohorts.
AAA has long posed a significant global health burden due to its progressive nature and the high mortality rate associated with ruptured AAA (rAAA). Numerous studies have investigated the short-term outcomes of patients undergoing endovascular aneurysm repair (EVAR), particularly in emergency settings. For instance, Ye et al analyzed 1124 AAA patients and 6524 healthy controls using a multi-locus genetic risk score linked to AAA incidence and expansion.11 In a study by Tambyraja et al, clinical indicators such as hemoglobin < 9 g/dL, shock (blood pressure < 90 mmHg), and a Glasgow Coma Scale score < 15 were identified as sensitive markers for assessing the health status of rAAA patients and were associated with perioperative mortality, though this model has yet to be validated.12
The choice of surgical intervention for rAAA also significantly impacts patient outcomes. Dittman et al found that patients with a history of aortic repair exhibited higher mortality and morbidity when treated with open repair, recommending EVAR as the preferred approach in rupture cases.13 A meta-analysis conducted by Krisna Pertiwi et al demonstrated that EVAR, especially fenestrated-EVAR, improved short-term outcomes compared to open surgery, though it did not show superiority in long-term outcomes.14 Another meta-analysis reported similar findings, highlighting EVAR’s advantage in reducing peri-operative mortality.15
In addition to surgical strategies, the development of predictive tools and models is critical in improving AAA management. Zhou et al generated a nomogram based on morphological features, including hostile aneurysm neck, conical neck, and angulated neck, with moderate discrimination ability (AUC: 0.81, 95% CI: 0.73–0.89).16 Another study, which involved 205 patients with highly angulated necks, analyzed risk factors for endograft-related complications, such as increasing proximal neck diameter and decreasing seal zone inner curve length.17 The case-control study conducted by Memon et al identified myeloperoxidase as a promising prognostic factor, with an AUC of 0.71.18 Liu et al developed a nomogram to predict type II endoleak after EVAR,19 while Zhao et al assessed risk factors for progression of sub-aneurysmal aorta.20 Another model proposed by Liu et al incorporated both morphological and biomechanical indices to predict AAA rupture risk.21
However, current nomograms and predictive models mostly rely on demographic, anatomical, or procedural variables, often overlooking laboratory biomarkers that may reflect real-time physiological and inflammatory states. Some models also lack interpretability or integration into clinical workflows, reducing their utility in clinical decision-making.
In our study, the new predictive model incorporates laboratory data, which has been relatively underutilized. This inclusion allows for a more comprehensive assessment of patient health and the risk of ACM, potentially capturing nuances in patient conditions that anatomical data alone might miss. The model displayed a great discrimination ability for 1- and 3-year survival predictions with AUCs of 0.88 (95% CI: 0.78–0.98) and 0.87 (95% CI: 0.76–0.98), respectively, in the training cohort. Such insights could assist physicians in identifying high-risk patients and taking proactive measures to prevent adverse events. Overall, utilizing predictive models in AAA patients is promising to enhance patient outcomes and reduce healthcare costs by facilitating early intervention and tailored treatment plans.
Machine learning enhances healthcare by improving diagnostics, personalizing treatments, predicting patient outcomes, and optimizing operations. It aids in analyzing complex medical data for accurate diagnoses, tailoring treatments to individual patients, and predicting risks such as disease progression or post-surgery complications.22,23 In this article, we reported six variables as independent risk factors for ACM. Among them, the diameter of an aneurysm has been the gold standard for evaluating AAA progression and rupture prediction. Therefore, patients with large AAA should receive surgical treatment to prevent adverse outcomes.24 Previous studies have reported that the growth rate of aneurysms in males with diameters of approximately 3 and 5 cm were 1.28 and 3.61 mm per year, respectively. Additionally, the growth rate accelerated by 0.59 mm per year for every 0.5 cm increment in aneurysm diameter. The relationship between diameter and the probability of rupture was consistent across genders, with females carrying a higher risk of rupture across the entire diameter range.25,26 Choi et al found that an aneurysm diameter > 65 mm was a risk factor for type Ib endoleak.27 A recent meta-analysis involving 1514 patients from 11 studies reported that the rupture rate in AAAs 5.5–6, 6.1–7, and >7 cm were 3.5%, 4.1%, and 6.3%, respectively. The study further revealed that the risk of death from other causes surpassed the risk of death from rupture, thereby underscoring the significance of investigating ACM in AAA patients.28
Age is another classic risk factor for AAA patients. Surgical treatment for older patients has always been a problem, even with the improvement of medical technology. Alberga et al identified age as an independent risk factor for adverse outcome, where octogenarians hold a higher risk of peri-operative mortality (1.4% for EVAR and 9.3% for open surgery).29 A predictive model developed by a retrospective study also demonstrated age as an important risk factor (<70 for 0 points, 70–74.9 for 9 points, 75–79.9 for 10 points, and ≥80 for 17 points).30 These analyses could assist clinicians with risk-benefit assessments when deciding on treatment strategies for elderly patients.
Stroke has been identified as a comorbidity among AAA patients. In a study involving 1136 individuals, the prevalence of a prior stroke was 12.3%,31 which was relatively close to our present study (16.9%). However, in another cohort with 206 individuals, the prevalence could reach 38%,32 highlighting a huge variation in the comorbidity prevalence and the need for further research focusing on the history of cerebrovascular diseases.
More interestingly, inflammatory cells, including WBC, neutrophils, and monocytes, significantly differed in patients with adverse outcomes. Among them, monocytes were considered an independent risk factor for ACM, which aligned with previous studies, thereby suggesting the association between monocytosis and cardiovascular disease.33,34 Studies also discovered significant alterations in peripheral blood monocyte subsets and phenotypes, suggesting an active involvement of monocytes in AAA development. Consequently, its role in AAA prognosis requires further investigation.35,36
The findings from this study, through the development of a more comprehensive and accurate predictive model for ACM in post-EVAR patients, have the potential to transform clinical practice by enhancing patient stratification, personalizing treatment plans, supporting informed decision-making, and optimizing resource allocation.
Limitation
Firstly, this study was conducted at a single center, which may limit the generalizability of our findings to other healthcare settings or geographical regions. Patient demographics, treatment protocols, and the prevalence of comorbid conditions can vary significantly across different regions, potentially influencing the model’s predictive accuracy. Secondly, the retrospective and observational design of the study inherently carries the risk of selection bias and residual confounding, despite our efforts to adjust for known confounders. The relatively small sample size and number of ACM events may also limit the robustness of the model, particularly in populations with different baseline risk profiles. Another limitation of our study is the lack of comprehensive data regarding specific endograft device types used in the procedures. Device characteristics and design variations could potentially influence long-term outcomes after EVAR, as different devices may have varying rates of durability, conformability, and fixation mechanisms. Future studies with prospective data collection protocols should aim to systematically document and analyze the impact of different device types on post-EVAR outcomes, which could further refine risk prediction models. Lastly, our model has yet to undergo external validation in independent cohorts. Without external validation, it is difficult to confirm its performance and utility across varied clinical environments. Future studies should aim to validate this nomogram in multi-center cohorts that include diverse populations from different geographical regions and with varying comorbidity profiles. Such efforts would provide a more comprehensive evaluation of the model’s generalizability and ensure its broader clinical applicability.
Conclusion
In this study, we developed a nomogram to predict ACM in patients undergoing EVAR for AAA. Key independent risk factors identified include a history of stroke, CIA atherosclerosis, advanced age, low hemoglobin levels, elevated monocyte count, and the presence of a large AAA. The nomogram demonstrated good predictive accuracy and can enhance clinical decision-making by enabling personalized risk stratification and tailored treatment strategies. Future research should focus on validating the model in diverse cohorts and incorporating additional biomarkers to improve its predictive power.
Abbreviations
AAA, Abdominal aortic aneurysm; ACEI, angiotensin-converting enzyme inhibitor; ACM, all-cause mortality; AUC, area under the curve; CAD, coronary artery disease; CCB, calcium entry blockers; CIA, common iliac artery; COPD, chronic obstructive pulmonary disease; CTA, computed tomographic angiography; DCA, decision curve analysis; eGFR, estimated glomerular filtration rate; EVAR, endovascular aneurysm repair; FBG, fasting blood glucose; ILT, intraluminal thrombus; KM, Kaplan-Meier; LASSO, least absolute shrinkage and selection operator; LDL-C, low-density lipoprotein cholesterol; rAAA, ruptured AAA; ROC, receiver operating characteristic; WBC, white blood cell.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, upon reasonable request.
Ethics Approval
This study has been approved by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University. The details of the study design are documented at http://www.chictr.org.cn (Identifier: ChiCTR2200063122). The data are anonymous, and the requirement for informed consent was therefore waived. Our research conformed to the Declaration of Helsinki. Personal information and data remained confidential and anonymous.
Acknowledgment
The authors wish to acknowledge the assistance of the First Affiliated Hospital of Zhengzhou University with the data extraction.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82222007 and 82170281 to J.T., U2004203 to J.Z.), Henan Province Key R&D Program (No.241111313300) to J.T., Henan Province Medical Science and Technology Key Joint Project (SBGJ202101012) to J.Z., Henan Province Science and Technology Research Joint Project (No.222301420054) to J.T., Henan Thousand Talents Program (No. ZYQR201912131) to J.Z., Funding for Scientific Research and InnovationTeam of The First Affiliated Hospital of Zhengzhou University (QNCXTD2023001 to J.T and ZYCXTD2023008 to J.Z.).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Scott RAP, Bridgewater SG, Ashton HA. Randomized clinical trial of screening for abdominal aortic aneurysm in women. Br J Surg. 2002;89(3):283–285. doi:10.1046/j.0007-1323.2001.02014.x
2. Ashton HA, Gao L, Kim LG, Druce PS, Thompson SG, Scott RAP. Fifteen-year follow-up of a randomized clinical trial of ultrasonographic screening for abdominal aortic aneurysms. Br J Surg. 2007;94(6):696–701. doi:10.1002/bjs.5780
3. Howard DPJ, Banerjee A, Fairhead JF, et al. Population‐based study of incidence of acute abdominal aortic aneurysms with projected impact of screening strategy. J Am Heart Assoc. 2015;4(8):e001926. doi:10.1161/JAHA.115.001926
4. Nordon IM, Hinchliffe RJ, Loftus IM, Thompson MM. Pathophysiology and epidemiology of abdominal aortic aneurysms. Nat Rev Cardiol. 2011;8(2):92–102. doi:10.1038/nrcardio.2010.180
5. Golledge J. Abdominal aortic aneurysm: update on pathogenesis and medical treatments. Nat Rev Cardiol. 2019;16(4):225–242. doi:10.1038/s41569-018-0114-9
6. Oliveira NFG, Ultee K, Van Rijn MJ, et al. Anatomic predictors for late mortality after standard endovascular aneurysm repair. J Vasc Surg. 2019;69(5):1444–1451. doi:10.1016/j.jvs.2018.07.082
7. Waasdorp EJ, De Vries JPPM, Hobo R, Leurs LJ, Buth J, Moll FL. Aneurysm diameter and proximal aortic neck diameter influence clinical outcome of endovascular abdominal aortic repair: a 4-year EUROSTAR experience. Ann Vasc Surg. 2005;19(6):755–761. doi:10.1007/s10016-005-7971-5
8. Kaladji A, Daoudal A, Duménil A, et al. Predictive models of complications after endovascular aortic aneurysm repair. Ann Vasc Surg. 2017;40:19–27. doi:10.1016/j.avsg.2016.08.020
9. Egorova N, Giacovelli JK, Gelijns A, et al. Defining high-risk patients for endovascular aneurysm repair. J Vasc Surg. 2009;50(6):1271–1279.e1. doi:10.1016/j.jvs.2009.06.061
10. Van Keulen JW, Moll FL, Tolenaar JL, Verhagen HJM, Van Herwaarden JA. Validation of a new standardized method to measure proximal aneurysm neck angulation. J Vasc Surg. 2010;51(4):821–828. doi:10.1016/j.jvs.2009.10.114
11. Ye Z, Austin E, Schaid DJ, Kullo IJ. A multi-locus genetic risk score for abdominal aortic aneurysm. Atherosclerosis. 2016;246:274–279. doi:10.1016/j.atherosclerosis.2015.12.031
12. Tambyraja A, Murie J, Chalmers R. Predictors of outcome after abdominal aortic aneurysm rupture: edinburgh ruptured aneurysm score. World J Surg. 2007;31(11):2243–2247. doi:10.1007/s00268-007-9181-5
13. Dittman JM, Murphy B, Dansey KD, et al. Editor’s choice - an endovascular approach to abdominal aortic aneurysm rupture is associated with improved outcomes for patients with prior aortic repair. Eur J Vasc Endovasc Surg. 2024;67(6):904–910. doi:10.1016/j.ejvs.2024.01.020
14. Krisna Pertiwi PF, Sudarma IW, Prana Jagannatha GN, Kosasih AM, Dyah Yustika Dewi CI, Angga Wijaya IGA. Outcomes of advanced EVAR versus open surgery in the management of complex abdominal aortic aneurysm repair: a systematic review and meta-analysis. Asian Cardiovasc Thorac Ann. 2024;32(6–7):375–387. doi:10.1177/02184923241262847
15. Kontopodis N, Galanakis N, Antoniou SA, et al. Meta-analysis and meta-regression analysis of outcomes of endovascular and open repair for ruptured abdominal aortic aneurysm. Eur J Vasc Endovasc Surg. 2020;59(3):399–410. doi:10.1016/j.ejvs.2019.12.023
16. Zhou M, Wang Y, Ding Y, et al. Prognostic nomogram for patients with hostile neck anatomy after endovascular abdominal aortic aneurysm repair. Ann Vasc Surg. 2019;56:132–138. doi:10.1016/j.avsg.2018.07.062
17. Wang S, Hicks CW, Malas MB. Neck diameter and inner curve seal zone predict endograft-related complications in highly angulated necks after endovascular aneurysm repair using the Aorfix endograft. J Vasc Surg. 2018;67(3):760–769. doi:10.1016/j.jvs.2017.07.114
18. Memon AA, Zarrouk M, Ågren-Witteschus S, Sundquist J, Gottsäter A, Sundquist K. Identification of novel diagnostic and prognostic biomarkers for abdominal aortic aneurysm. Eur J Prev Cardiol. 2020;27(2):132–142. doi:10.1177/2047487319873062
19. Liu Z, Chen Y, Qin Y, et al. A nomogram risk assessment model to predict the possibility of type II endoleak-related re-intervention after endovascular aneurysm repair (EVAR). Sci Rep. 2023;13(1):14. doi:10.1038/s41598-022-27356-8
20. Zhao W, Wang G, Xu P, et al. Analysis of high-risk factors associated with the progression of subaneurysmal aorta to abdominal aortic aneurysm in rural area in China. Clin Interv Aging. 2021;16:1573–1580. doi:10.2147/CIA.S321921
21. Liu T, Hu T, Lu W, et al. Morphology and biomechanical index predict the rupture location and rupture risk of abdominal aortic aneurysm. Sci Rep. 2025;15(1):9604. doi:10.1038/s41598-025-94828-y
22. Deo RC. Machine learning in medicine. Circulation. 2015;132(20):1920–1930. doi:10.1161/CIRCULATIONAHA.115.001593
23. Quer G, Arnaout R, Henne M, Arnaout R. Machine learning and the future of cardiovascular care. J Am Coll Cardiol. 2021;77(3):300–313. doi:10.1016/j.jacc.2020.11.030
24. Wanhainen A, Verzini F, Van Herzeele I, et al. Editor’s choice – European society for vascular surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. 2019;57(1):8–93. doi:10.1016/j.ejvs.2018.09.020
25. Bown MJ, Sweeting MJ, Brown LC. Surveillance intervals for small abdominal aortic aneurysms: a meta-analysis. JAMA. 2013;309(8):806. doi:10.1001/jama.2013.950
26. Chaikof EL, Dalman RL, Eskandari MK, et al. The society for vascular surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018;67(1):2–77.e2. doi:10.1016/j.jvs.2017.10.044
27. Choi E, Lee SA, Ko GY, Kim N, Cho YP, Kwon TW. Risk factors for early and late type ib endoleak following endovascular abdominal aortic aneurysm repair. Ann Vasc Surg. 2021;72:507–516. doi:10.1016/j.avsg.2020.08.144
28. Parkinson F, Ferguson S, Lewis P, Williams IM, Twine CP. Rupture rates of untreated large abdominal aortic aneurysms in patients unfit for elective repair. J Vasc Surg. 2015;61(6):1606–1612. doi:10.1016/j.jvs.2014.10.023
29. Alberga AJ, Karthaus EG, Van Zwet EW, et al. Outcomes in octogenarians and the effect of comorbidities after intact abdominal aortic aneurysm repair in the netherlands: a nationwide cohort study. Eur J Vasc Endovasc Surg. 2021;61(6):920–928. doi:10.1016/j.ejvs.2021.02.047
30. Meuli L, Zimmermann A, Menges AL, Stefanikova S, Reutersberg B, Makaloski V. Prognostic model for survival of patients with abdominal aortic aneurysms treated with endovascular aneurysm repair. Sci Rep. 2022;12(1):19540. doi:10.1038/s41598-022-24060-5
31. Singh K. Prevalence of and Risk factors for abdominal aortic aneurysms in a population-based study: the tromso study. Am J Epidemiol. 2001;154(3):236–244. doi:10.1093/aje/154.3.236
32. Dryjski M, Driscoll JL, Blair RC, et al. The small abdominal aortic aneurysm: the eternal dilemma. J Cardiovasc Surg. 1994;35(2):95–100.
33. Idzkowska E, Eljaszewicz A, Miklasz P, Musial WJ, Tycinska AM, Moniuszko M. The role of different monocyte subsets in the pathogenesis of atherosclerosis and acute coronary syndromes. Scand J Immunol. 2015;82(3):163–173. doi:10.1111/sji.12314
34. Yang J, Zhang L, Yu C, Yang XF, Wang H. Monocyte and macrophage differentiation: circulation inflammatory monocyte as biomarker for inflammatory diseases. Biomark Res. 2014;2(1):1. doi:10.1186/2050-7771-2-1
35. Ghigliotti G, Barisione C, Garibaldi S, et al. CD16+ monocyte subsets are increased in large abdominal aortic aneurysms and are differentially related with circulating and cell-associated biochemical and inflammatory biomarkers. Dis Markers. 2013;34(2):131–142. doi:10.1155/2013/836849
36. Rubio-Navarro A, Amaro Villalobos JM, Lindholt JS, et al. Hemoglobin induces monocyte recruitment and CD163-macrophage polarization in abdominal aortic aneurysm. Int J Cardiol. 2015;201:66–78. doi:10.1016/j.ijcard.2015.08.053
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Histological Severity of Cirrhosis Influences Surgical Outcomes of Hepatocellular Carcinoma After Curative Hepatectomy
Liang BY, Gu J, Xiong M, Zhang EL, Zhang ZY, Lau WY, Wang SF, Guan Y, Chen XP, Huang ZY
Journal of Hepatocellular Carcinoma 2022, 9:633-647
Published Date: 23 July 2022
A Nomogram Based on SEER Database for Predicting Prognosis in Patients with Mucinous Ovarian Cancer: A Real-World Study
Zhang K, Feng S, Ge Y, Ding B, Shen Y
International Journal of Women's Health 2022, 14:931-943
Published Date: 26 July 2022
Nomogram for the Preoperative Prediction of the Macrotrabecular-Massive Subtype of Hepatocellular Carcinoma
Shan Y, Yu X, Yang Y, Sun J, Wu S, Mao S, Lu C
Journal of Hepatocellular Carcinoma 2022, 9:717-728
Published Date: 10 August 2022
Establishment and Validation of a Model for Disease-Free Survival Rate Prediction Using the Combination of microRNA-381 and Clinical Indicators in Patients with Breast Cancer
Shen J, Wang M, Li F, Yan H, Wang R, Zhou J
Breast Cancer: Targets and Therapy 2022, 14:375-389
Published Date: 30 November 2022
Development and Validation of a Novel Nomogram Integrated with Hypoxic and Lactate Metabolic Characteristics for Prognosis Prediction in Hepatocellular Carcinoma
Qiu X, Dong L, Wang K, Zhong X, Xu H, Xu S, Guo H, Wei X, Chen W, Xu X
Journal of Hepatocellular Carcinoma 2024, 11:241-255
Published Date: 2 February 2024