Back to Journals » Journal of Pain Research » Volume 19
Depressive Symptoms as a Potential Mediator in the Association Between Pain and Cognitive Function: A Cross-Sectional Study
Authors Gao S ![]() , Feng M
, Feng M ![]() , Zhou H, Tao Y, Feng L, Xi Y, Guo H, Nangong J, Yang Y, Zhou Y
, Zhou H, Tao Y, Feng L, Xi Y, Guo H, Nangong J, Yang Y, Zhou Y ![]()
Received 12 January 2026
Accepted for publication 11 May 2026
Published 3 June 2026 Volume 2026:19 595453
DOI https://doi.org/10.2147/JPR.S595453
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Rocío de la Vega
Sizhe Gao, Mingkun Feng, Haibin Zhou, Yan Tao, Lei Feng, Yang Xi, Hongfei Guo, Jiarui Nangong, Yifei Yang, Yan Zhou
Department of Pain Management, Beijing Jishuitan Hospital, Capital Medical University, Beijing, 100035, People’s Republic of China
Correspondence: Yan Zhou, Department of Pain Management, Beijing Jishuitan Hospital, Capital Medical University, No. 31 Xinjiekoudong Street, Xicheng District, Beijing, 10035, People’s Republic of China, Tel + 86 13001151232, Fax +86 10-58516095, Email [email protected]
Objective: To investigate the association between pain intensity and cognitive function, and to explore the influence of demographic, clinical, and mood factors on this relationship.
Design: Cross-sectional study.
Setting: A tertiary comprehensive teaching hospital.
Subjects: 2661 inpatients admitted for pain management who completed cognitive function screening.
Methods: Pain intensity was assessed using the Numeric Rating Scale (NRS). Cognitive function was evaluated with the Montreal Cognitive Assessment (MoCA). Anxiety and depressive symptoms were assessed using the Hamilton Anxiety Scale (HAMA) and the Hamilton Depression Scale (HAMD), respectively. Univariable and multivariable analyses were performed to examine the association between pain intensity and cognitive function, and mediation analysis was conducted to explore potential mediating effects.
Results: The median pain duration was 3.0 months (IQR 0.6– 12.0), and the median admission NRS score was 6 (IQR 4– 6). Among the 2661 patients, 1502 (56.4%) had a MoCA score below 26, indicating mild cognitive impairment. Multiple linear regression model showed that higher pain intensity was significantly associated with higher MoCA (β = 0.22, 95% CI [0.12, 0.33], p < 0.001) after controlling for age, sex, education, pain duration, anxiety, and depression. Mediation analysis showed that baseline pain significantly predicted higher depressive symptoms (β = 0.41, p < 0.001), and depressive symptoms were negatively associated with cognitive performance (β = − 0.16, p < 0.001).
Conclusion: This large-scale cross-sectional study demonstrated a complex association between pain intensity and cognitive performance. While pain was directly associated with cognitive scores, depressive symptoms exerted a significant negative indirect effect, indicating partially opposing pathways. These findings suggest that mood-related mechanisms play a critical role in the pain–cognition relationship, highlighting the importance of integrating mood assessment into pain management.
Keywords: pain, cognitive function, depression, cross-sectional study
Introduction
Pain is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage.1 Pain is a complex, multidimensional experience influenced by a diverse range of biological, psychological, and social factors.2
Pain not only produces abnormal sensory experiences but also significantly impacts cognitive and emotional processing.3 Increasing evidence shows that people with chronic pain often experience impairments in attention, memory, and executive function.4 Patients with chronic pain show measurable impairments on cognitive tests, and such deficits are particularly pronounced in conditions like fibromyalgia, neuropathic pain, and rheumatoid arthritis.5 These findings suggest that pain and cognition share overlapping neural circuits and that chronic nociceptive input may interfere with normal cognitive functioning. Cognitive decline, in turn, further compromises self-care ability and aggravates pain-related disability.
While the direct link between pain and cognitive impairment was documented, the underlying mechanisms driving this association remain incompletely understood. Theoretical models and empirical evidence suggest that psychological distress, particularly depression and anxiety, may serve as a critical mechanistic bridge. Chronic pain acts as a persistent physical and psychological stressor that frequently precipitates depressive symptoms, potentially through shared neurobiological pathways such as altered monoamine neurotransmission, neuroinflammation, and dysregulation of the hypothalamic-pituitary-adrenal axis.6–8 According to the cognitive load theory, this depletion of cognitive resources inevitably impairs attention, working memory, and executive function.9 Therefore, it is both biologically and psychologically highly plausible to conceptualize pain as the primary exposure that exacerbates psychological distress, which in turn compromise cognitive performance.
Although previous studies have explored the pairwise relationships among pain, psychological distress, and cognition, most have relied on relatively small samples or examined these clinical features in isolation.10,11 The extent to which depression quantitatively mediates the pain-cognition pathway within a unified analytic framework remains insufficiently explored.
Given these considerations, the present study aimed to investigate the relationship between pain intensity, depression symptoms and cognitive function in a large-scale population. We proposed the following specific hypotheses: 1) Higher pain intensity is independently associated with both more severe depressive symptoms and poorer cognitive performance.2) Depressive symptoms act as a significant mediator in the association between pain intensity and cognitive function. Understanding these interrelationships may help identify individuals at high risk of cognitive decline. This knowledge could provide a foundation for developing interventions that address both pain and mood to preserve cognitive health.
Methods
Study Design and Population
This cross-sectional study was approved by the Ethics Committee of Beijing Jishuitan Hospital, Capital Medical University (Approval No. K2025-021-00) and conducted in accordance with the Declaration of Helsinki. All participants received detailed information about the study and provided written informed consent before enrollment. Inpatients admitted for pain management were consecutively recruited from the Department of Pain Management, Beijing Jishuitan Hospital, Capital Medical University, between June 2023 and November 2024. The sampling frame consisted of all adult patients requiring hospitalization for pain-related conditions during this period. As part of the standard clinical pathway in our department, trained clinical staff routinely administered comprehensive assessments, including evaluations of pain intensity, mood, and cognitive function, within the first 12 hours of admission. During the specified period, a total of 7335 patients were initially screened upon admission. Eligible participants were adults (aged ≥ 18 years) who had completed the baseline cognitive function screening and accompanying clinical assessments. Patients were ultimately excluded from the present analysis if they lacked complete data on the primary variables of interest (Numeric Rating Scale, Montreal Cognitive Assessment, Hamilton Anxiety Scale and Hamilton Depression Scale) or were unable to complete the assessments due to severe acute illness or communication barriers at the time of admission.
Assessment of Patient-Reported Outcomes
Pain intensity was evaluated by pain specialists, while cognitive and emotional assessments were conducted by trained neuropsychology technicians.
Instrument
Numeric Rating Scale (NRS)
Pain intensity was assessed using the NRS. Participants were asked to rate their average pain intensity over the past week on a scale from 0 to 10 where 0 indicates “no pain” and 10 represents “the worst imaginable pain.”
Montreal Cognitive Assessment (MoCA)
Cognitive function was assessed using the Beijing version of the Montreal Cognitive Assessment (MoCA‑B), version 7.1. Details of the MoCA‑B are available at http://www.mocatest.org. The MoCA‑B evaluates eight cognitive domains: visuospatial and executive function, naming, memory, attention, language, abstraction, delayed recall, and orientation. Because educational attainment may affect MoCA performance, an education-corrected MoCA score was also calculated by adding 1 point for participants with ≤12 years of education, following the standard MoCA recommendation. A total score below 26 was considered indicative of mild cognitive impairment (MCI).
Hamilton Anxiety Scale (HAMA) and Hamilton Depression Scale (HAMD)
Anxiety symptoms were assessed with the 14‑item Hamilton Anxiety Scale (HAMA),12 which includes two dimensions: psychic anxiety (items 1–6, 14) and somatic anxiety (items 7–13). Each item is rated from 0 to 4, with a total score ≤ 7 indicating no anxiety symptoms. Depressive symptoms were assessed with the 24‑item Hamilton Depression Scale (HAMD),13 which covers seven dimensions: anxiety and somatic symptoms (items 10–13, 15, 17), weight change (item 16), cognitive impairment (items 2, 3, 9, 19–21), diurnal variation (item 18), retardation (items 1, 7, 8, 14), insomnia (items 4–6), and hopelessness (items 22–24). Each item is rated on a 0–4 scale (some items 0–2), and a total score ≤ 7 indicates no depressive symptoms. The Chinese versions of both HAMA and HAMD were used in this study.
Statistical Analysis
All statistical analyses were performed in R (version 4.0) after data cleaning. Demographic characteristics and screening test results across different pain sites were summarized descriptively. Descriptive statistics included means, standard deviations, medians, interquartile ranges (Q1–Q3), and frequencies with percentages for categorical variables. NRS, MoCA, HAMA, and HAMD scores were treated as continuous variables. The Kolmogorov–Smirnov test was used to assess normality.
Between-group comparisons were conducted using appropriate methods according to variable type. Independent-samples t-tests or Mann–Whitney U-tests were applied for continuous data, depending on distribution, while Pearson’s chi‑square test or Fisher’s exact test (when applicable) was used for categorical data. Linear regression was performed to evaluate associations between continuous variables. All tests were two‑tailed, and p < 0.05 was considered statistically significant. We selected covariates based on literature6,11 and clinical experience identifying them as confounders of pain, mood, and cognition literature.
Missing Data Imputation
Patients were included in the final analysis only if they had complete data for NRS, MoCA, HAMA, and HAMD. For the included cohort, missing data were present in certain secondary covariates. To address this and minimize potential bias from excluding cases with missing covariates, multiple imputation by chained equations (MICE) was utilized to impute these missing values. Summary statistics and missing‑data patterns were reviewed to verify data completeness before analysis.
Multivariable Analysis
Multiple linear regression models were used to examine the association between pain-related characteristics and cognitive performance measured by the MoCA. Variance Inflation Factors (VIFs) were calculated for all predictors. Generalized additive models (GAMs) were fitted to test potential nonlinear associations between pain intensity and cognitive function, adjusting for covariates. The fitted smoothed curves with 95% confidence intervals were illustrated.
Mediation Analysis
Structural equation modeling (SEM) was used to examine whether depressive symptoms mediated the association between pain intensity and cognition. Standardized path coefficients were reported for direct, indirect, and total effects, and mediation significance was tested using 5000 bootstrap samples.
Results
Study Participants
Of the 7335 participants enrolled, 2661 had complete data on NRS, MoCA, HAMA, and HAMD and were included in the cross‑sectional analysis (Table 1). Comparison of baseline characteristics between the included and excluded participants revealed no clinically meaningful differences, indicating that the missing data did not introduce substantial selection bias (Table S1). The median age was 61 years (interquartile range [IQR], 51–69), and 57.5% were female. Nearly half (48.0%) had an education level of junior high school or below.
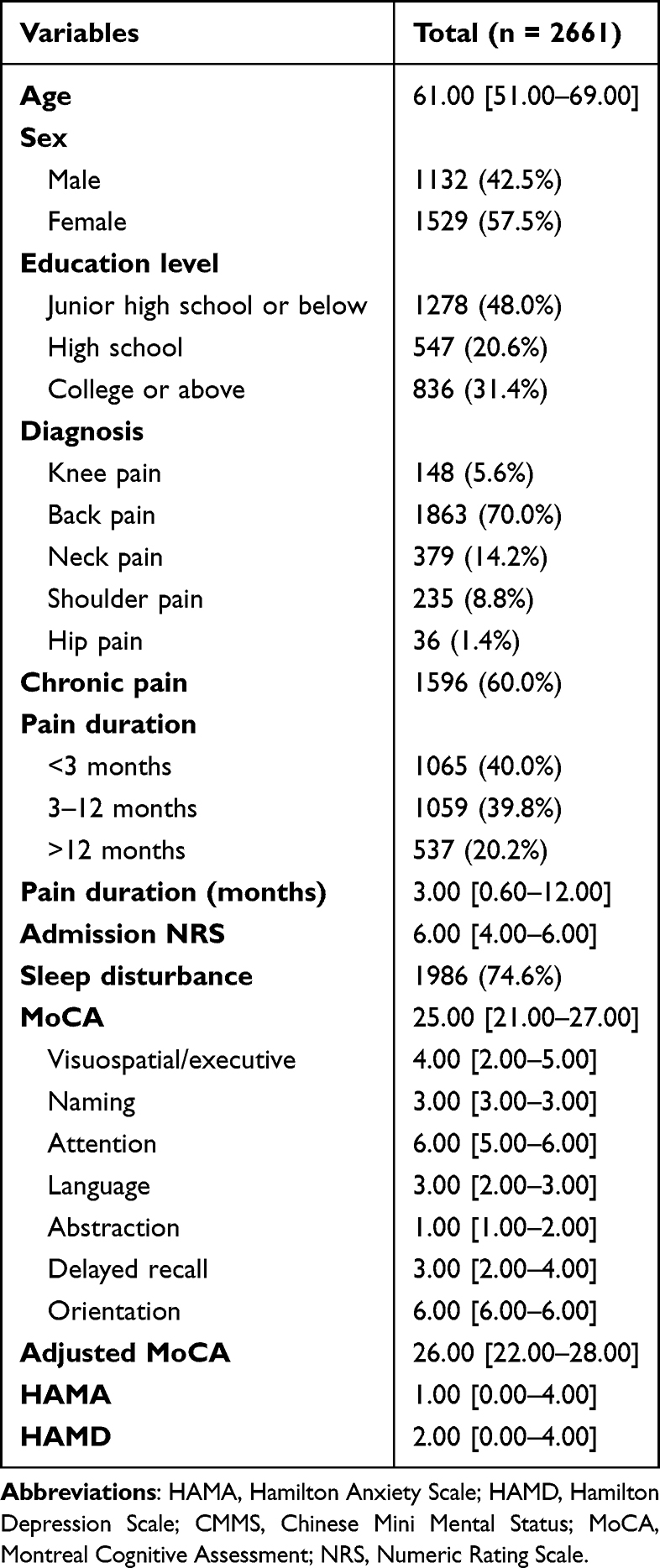 |
Table 1 Baseline Characteristics of Participants Included in the Study |
The most common pain diagnosis was back pain (70.0%), followed by neck pain (14.2%), shoulder pain (8.8%), knee pain (5.6%), and hip pain (1.4%). Chronic pain was reported by 60.0% of individuals. Regarding pain duration, 40.0% reported pain lasting < 3 months, 39.8% reported 3–12 months, and 20.2% reported > 12 months, with a median duration of 3.0 months (IQR 0.6–12.0). The median admission NRS score was 6 (IQR 4–6), and 74.6% of participants reported sleep disturbance.
The median MoCA scores was 25 (IQR 21–27), respectively. After applying the education correction, the median MoCA score was 25 (IQR 22–28). The distributions of both the unadjusted and adjusted MoCA scores are presented in Figure 1. Median HAMA and HAMD scores were 1 (IQR 0–4) and 2 (IQR 0–4).
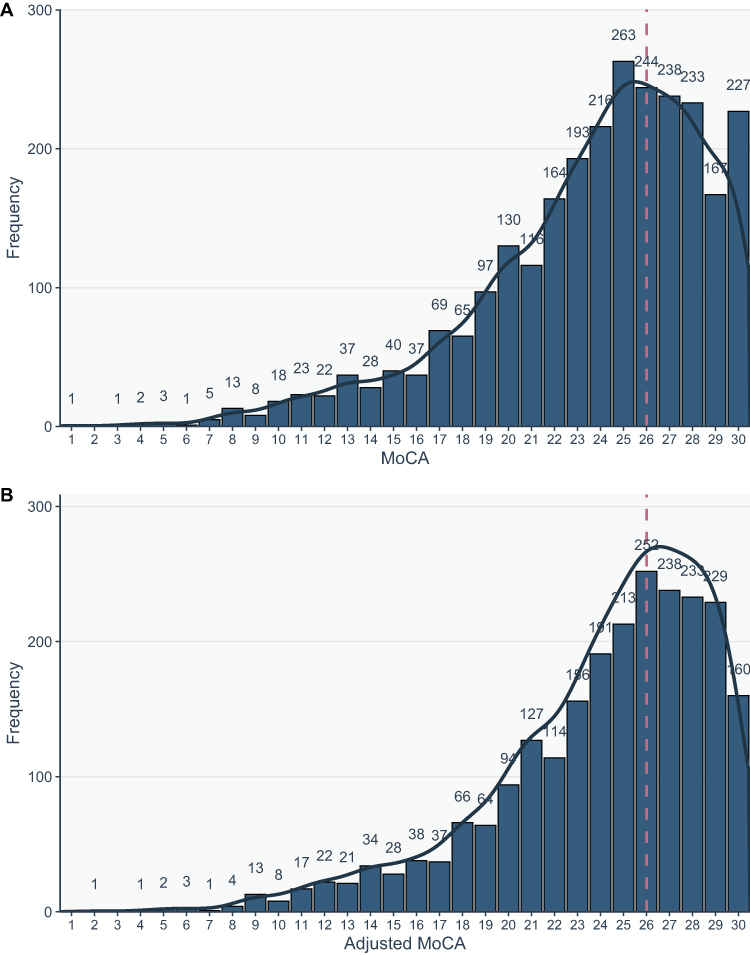 |
Figure 1 Distribution of unadjusted and education-corrected MoCA scores. (A) the distribution of unadjusted MoCA score. (B) the distribution of education-corrected MoCA score. The histogram shows the number of participants across MoCA total score levels. The black line represents the smoothed density curve of the score distribution, and the red dashed line marks the conventional cutoff of 26 points, which indicates possible mild cognitive impairment. Abbreviation: MoCA, Montreal Cognitive Assessment. |
The Association of Pain Intensity and Cognition
In the simple linear regression analysis, pain intensity was not significantly associated with the MoCA total score (β = –0.018, p = 0.773, R2 = 0.00003). After adjusting for age, sex, education, pain duration, anxiety, and depression in the multiple linear regression model, higher pain intensity was significantly associated with higher MoCA scores (β = 0.22, 95% CI [0.12, 0.33], p < 0.001) (Table 2). Age, sex, education level, and pain duration were also significant predictors of cognitive function. Higher HAMD scores (β = –0.12, 95% CI [–0.2, –0.05], p = 0.002) were associated with poorer cognitive performance, while HAMA scores were not significantly related to MoCA results. All VIF values were well below the strict threshold of 5 (ranging from 1.02 to 2.14), indicating that severe multicollinearity did not bias the regression estimates. In the sensitivity analysis excluding HAMA, the results remained steady (Table 3).
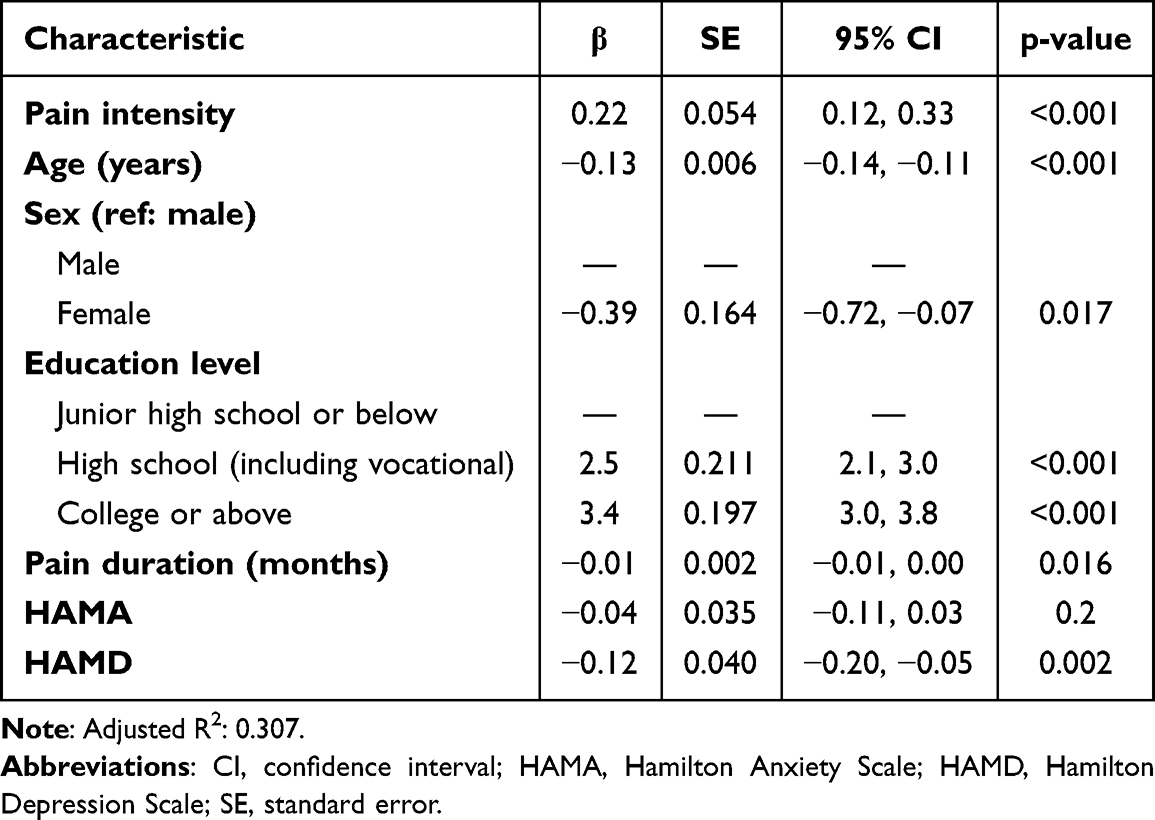 |
Table 2 Multiple Linear Regression Analysis of Pain Intensity and Cognitive Function (n = 2661) |
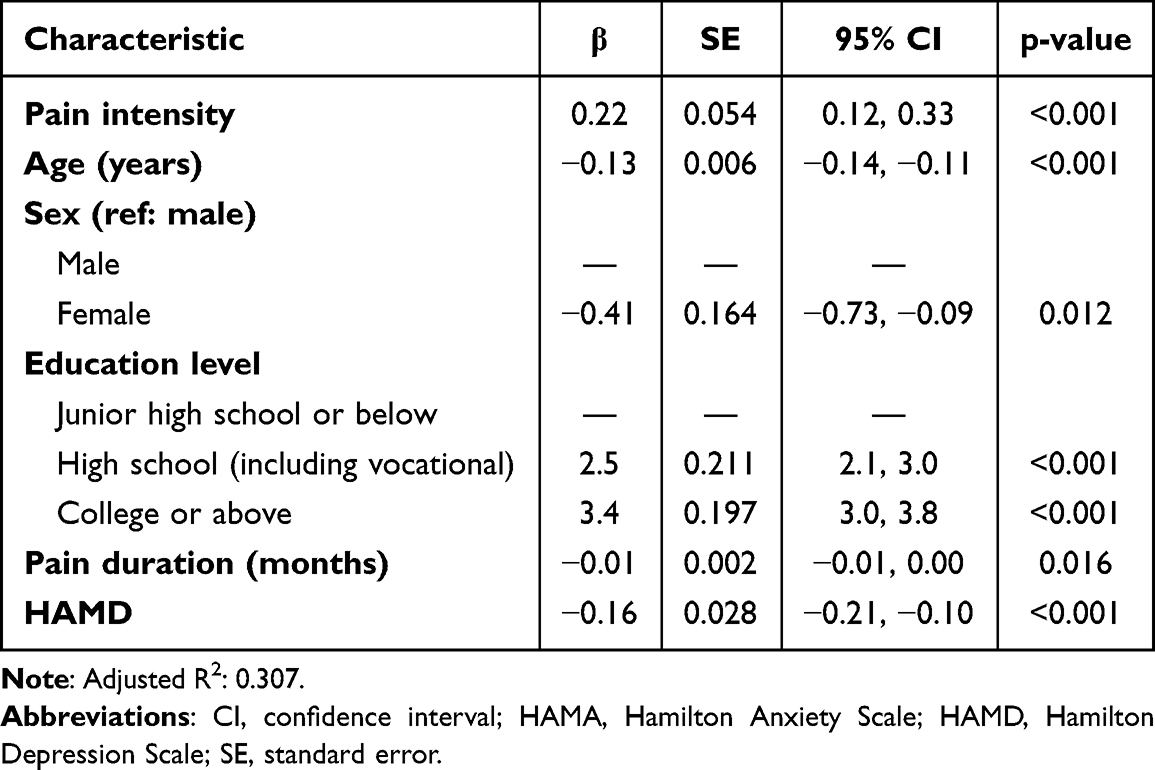 |
Table 3 Multiple Linear Regression Analysis of Pain Intensity and Cognitive Function Without Adjusting for Anxiety (n = 2661) |
In the sensitivity analysis including participants with pain duration longer than three months (n = 1596), results were generally consistent with the primary model. Higher pain intensity remained significantly associated with higher MoCA scores (β = 0.18, 95% CI [0.05, 0.32], p = 0.01) (Table 4).
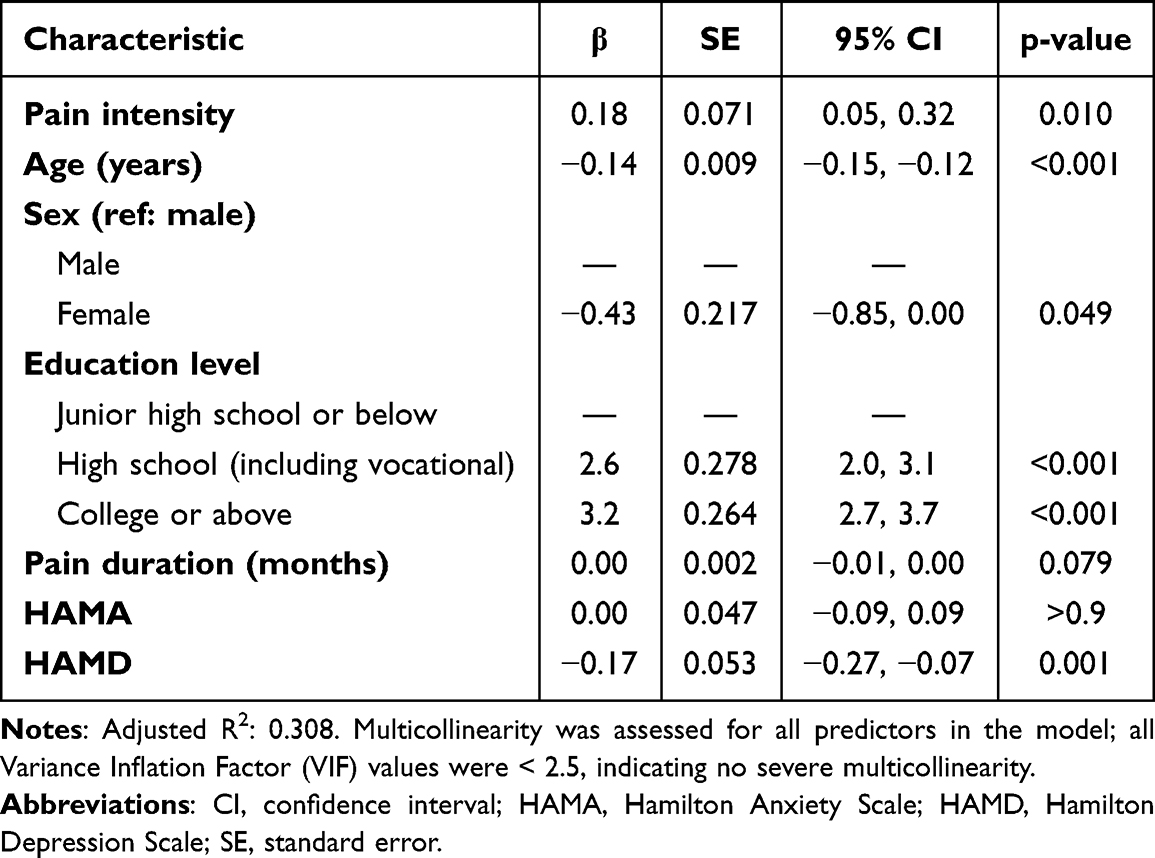 |
Table 4 Multiple Linear Regression Analysis of Pain Intensity and Cognitive Function in Participants with Pain Duration Longer Than Three months (n=1596) |
A generalized additive model (GAM) was further fitted to examine the potential nonlinear relationship between pain intensity and MoCA while adjusting for confounders (Figure 2). The smooth term for pain intensity was statistically significant (edf = 2.39, F = 8.96, p < 0.001), indicating a nonlinear association. Specifically, MoCA increased with increasing pain intensity, particularly at moderate-to-high pain levels. In the parametric component, older age (β = –0.13, p < 0.001), female gender (β = –0.39, p = 0.018), and higher HAMD (β = –0.13, p < 0.001) were independently associated with lower MoCA scores, whereas higher education levels were positively associated with cognitive performance. The model explained approximately 31% of the variance in MoCA scores (adjusted R2 = 0.31) (Table S2).
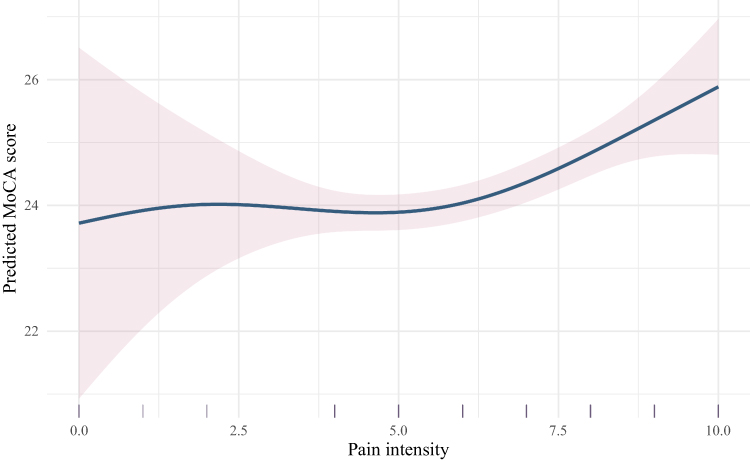 |
Figure 2 Association between pain intensity and predicted cognitive performance based on the generalized additive model (GAM). The x-axis represents pain intensity measured by the NRS, and the y-axis represents the predicted MoCA score. The solid line indicates the GAM-fitted smooth curve, and the shaded area denotes the 95% confidence interval. The rug plot on the x-axis displays the distribution of individual observations. Abbreviations: GAM, generalized additive model; MoCA, Montreal Cognitive Assessment; NRS, Numeric Rating Scale. |
Mediation Analysis
SEM revealed that baseline pain intensity was significantly associated with higher depressive symptoms (β = 0.41, p < 0.001), and depressive symptoms were negatively associated with cognitive performance (β = −0.16, p < 0.001). The statistical indirect effect of pain on cognition through depression was significant (ACME= −0.06, 95% CI [−0.09, −0.04], p < 0.001), indicating that greater pain severity was associated with poorer cognitive performance, a relationship partially explained by increased depressive symptoms. The direct effect of pain on cognition remained significant after adjusting for depression (ADE = 0.23, 95% CI [0.13, 0.34], p < 0.001), suggesting that pain is linked to cognition through additional mechanisms beyond depression. The total effect of pain on cognition was 0.17 (95% CI [0.07, 0.28], p < 0.001), of which approximately 37.7% was mediated through depressive symptoms. All paths were adjusted for age, sex, education level, and pain duration (Table 5 and Figure 3).
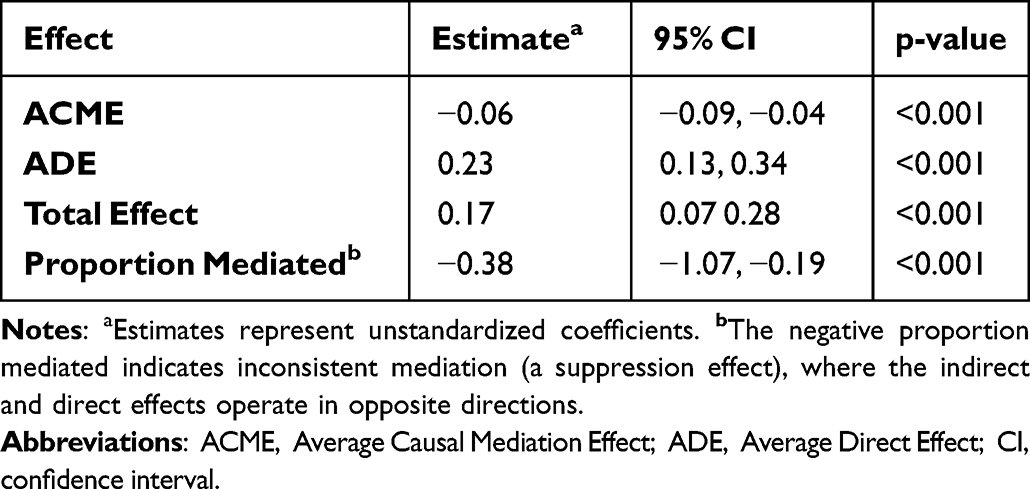 |
Table 5 Mediation Analysis of the Indirect Effect of Depression on the Relationship Between Pain and Cognition |
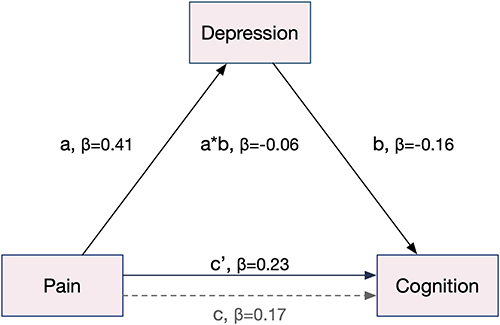 |
Figure 3 Path diagram of the mediation model testing the indirect effect of baseline pain on cognitive performance via depression. a = effect of pain intensity on depression; b = effect of depression on cognition; c = total effect of pain on cognition when the mediator is not included; c′ = direct effect of pain after adjusting for depressive symptoms. a*b represents the indirect (mediated) effect. All paths are adjusted for age, sex, education level. |
Discussion
The study is a large-scale, cross-sectional investigation into the association between pain and cognitive function. The results indicated that (1) a substantial proportion of patients with pain exhibited impaired cognitive function, as reflected by lower MoCA scores; (2) cognitive performance was associated with pain intensity, age, sex, education level, pain duration, depressive and anxiety symptoms; and (3) depressive symptoms were identified as a potential mediator in the association between pain and cognitive function.
Pain and cognition interact bidirectionally through shared neural networks.14 While earlier literature often framed this relationship as pain universally impairing cognitive performance across memory and attention domains,15 recent evidence suggests a more complex, context-dependent interaction where cognitive engagement can also modulate pain perception.16,17 Van der Leeuw et al found that elderly adults with more severe pain or pain interference had poorer performance on memory tests and executive functioning compared to those with less pain.18 Ojeda et al demonstrated that chronic pain patients had significantly lower cognitive function scores compared to pain-free subjects, with 33.64% showing cognitive dysfunction.19 Tomey et al found that greater pain experiences interfering with daily work were independently associated with poorer cognitive performance (β = −0.074, p<0.01).20 Melum et al examined 5753 participants and found that lower pain tolerance was significantly associated with poorer performance on the 12-word immediate recall test, digit symbol coding test, and Mini-Mental State Examination.21 Also, Multiple studies demonstrated that cognitive engagement could modulate pain perception, though the direction and magnitude of this effect vary with task demands and individual characteristics. Lier et al found that cognitive distraction significantly decreased pain scores regardless of cognitive load, supporting a unidirectional effect of cognition on pain up to a certain pain threshold.17 Our results suggest that pain intensity is indeed linked to cognitive performance, even after adjusting for covariates. However, the direction and magnitude of this relationship appear to vary depending on contextual and individual factors, indicating a complex interplay between nociceptive processing and cognitive control systems. Pain–cognition relationship is complex and partly suppressed by mood and demographic factors.
Former studies also showed the relationship between pain and cognitive function is critically moderated by age, with older adults showing reduced cognitive pain modulation effectiveness that depends on preserved executive function,22 and by affective factors, as depression and anxiety consistently mediate pain-cognition interactions. Duan et al, using data from the 2018 China Health and Aging Longitudinal Study (CHARLS), found that chronic pain and depressive symptoms were significantly associated with cognitive impairment in older Chinese adults.23 After adjusting for depression scores, pain intensity was no longer directly associated with the impairment of cognitive function, but mediation analysis suggested that depressive symptoms partially mediated the relationship between pain and cognitive decline. Duan et al study mainly focused on elderly patients with an average age of 71, while our study extends this investigation to a broader adult population, albeit within a specific clinical inpatient setting rather than the general community.
In our study, the MoCA score was not associated with pain intensity in the univariate analysis. After adjusting for age, sex, education, pain duration, anxiety, and depression, multiple linear regression indicated that higher pain intensity was associated with better MoCA scores (β=0.22, p<0.001). The unstandardized coefficient (0.22) indicates that a 1-point increase in pain intensity corresponds to a 0.22-point increase on MoCA. Although statistically significant, this modest coefficient lacks clinical magnitude and should not be misinterpreted as a meaningful cognitive enhancement.
When integrating these variables into a mediation framework, depressive symptoms emerged as a significant indirect pathway linking pain to poorer cognitive outcomes. Thus, while the direct regression suggested a positive association between pain intensity and cognitive performance, the mediation model revealed an opposing indirect negative effect through mood‑related mechanisms. This divergence likely reflects a suppression effect, whereby the shared variance with age, education, and mood variables reverses the direction of the adjusted pain–cognition association.
The mediation analysis revealed a significant negative indirect effect of pain on cognition through depressive symptoms, alongside a positive direct effect. This pattern indicates inconsistent mediation (a suppression effect), where opposing pathways operate simultaneously. Beyond this statistical suppression, the counterintuitive positive direct association might be partially explained by acute alertness. Pain acts as a salient stressor triggering sympathetic nervous system arousal, which may temporarily mobilize attentional resources and slightly enhance performance on brief screening tools like the MoCA.24 Besides, current understanding posits that depression is a multifactorial and heterogeneous clinical continuum involving somatic and cognitive symptoms, sharing common neurobiological underpinnings rather than existing as discrete categories.25 Together, these findings suggest that pain exerts complex, partially competing influences on cognitive function through both direct physiological and indirect mood-related pathways. Finally, given the cross-sectional design of this study, the exact temporal sequence among pain, depressive symptoms, and cognition cannot be established; therefore, these mediation findings should be interpreted as indicative rather than causal.
Several limitations of this study should be acknowledged. First, as a single-center cross‑sectional design, the findings can only demonstrate associations between pain and cognitive performance rather than establish causal relationships. Longitudinal or intervention studies are warranted to clarify the temporal and mechanistic links among pain, depression, and cognition. Additionally, relying exclusively on an inpatient sample from a single institution inherently introduces selection bias and restricts the generalizability of our results. Second, relying on the MoCA as our sole metric for cognitive classification is a key limitation. As a brief screening tool, it provides a global estimate but cannot capture nuanced deficits across distinct cognitive domains or replace comprehensive neuropsychological testing for formal clinical diagnosis. Third, this study employed multiple linear regression to explore the continuous relationship between pain intensity and cognitive function. While this approach allows for a nuanced examination across the full spectrum of pain severity, it may be less sensitive than categorical or logistic regression models in identifying threshold or nonlinear effects. Forth, the sample included participants with various types, sites, and durations of pain without further stratification. Although this broad inclusion enhances the generalizability of the findings to the overall pain population, it may also introduce heterogeneity and reduce the stability of the associations observed. Future studies could benefit from differentiating by pain phenotype and chronicity. Fifth, a critical unresolved limitation is the absence of medication data in this inpatient pain sample. Pharmacological agents common in hospitalized patients (eg, opioids, sedatives, or analgesics) act as major unmeasured confounders that profoundly and independently influence both cognitive arousal and mood states. Finally, the mediation analysis provides preliminary evidence suggesting that depressive symptoms may partially mediate the pain–cognition relationship; however, these indirect effects should be interpreted with caution given the cross‑sectional nature of the data. Nevertheless, this finding offers a valuable direction for future longitudinal and experimental research examining the role of depression in the cognitive consequences of chronic pain.
Conclusion
This cross-sectional study identified a complex association between pain intensity and cognitive performance in hospitalized patients with pain. While higher pain intensity was associated with cognitive scores after adjustment, depressive symptoms exerted a significant negative indirect effect, indicating partially opposing pathways. These findings suggest that mood-related mechanisms may play an important role in the pain–cognition relationship. While these correlational findings may highlight the importance of addressing mood symptoms in pain management, the practical clinical impact requires further quantification through longitudinal studies.
Abbreviations
GAMs, Generalized additive models; HAMA, Hamilton Anxiety Scale; HAMD, Hamilton Depression Scale; MCI, Mild cognitive impairment; MoCA, Montreal Cognitive Assessment; NRS, Numeric Rating Scale; SEM, Structural equation modeling.
Ethics Approval and Informed Consent
This cross-sectional study was approved by the Ethics Committee of Beijing Jishuitan Hospital, Capital Medical University (Approval No. K2025-021-00). All participants received detailed information about the study and provided written informed consent before enrollment.
Consent for Publication
All authors approved consent for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Scientific and Technological Achievements and Appropriate Technology Promotion Project, Beijing Municipal Health Commission (Grant No. BHTPP2024075), Beijing Hospitals Authority Clinical medicine Development of special funding support (Grant No.ZLRK202506) and Beijing Science and Technology plan project (Grant No. Z241100007724008).
Disclosure
The authors declare no competing interest.
References
1. Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–11. doi:10.1097/j.pain.0000000000001939
2. Cho C, Deol HK, Martin LJ. Bridging the translational divide in pain research: biological, psychological and social considerations. Front Pharmacol. 2021;12:603186. doi:10.3389/fphar.2021.603186
3. Fillingim RB. Individual differences in pain: understanding the mosaic that makes pain personal. Pain. 2017;158(Suppl 1):S11–S18. doi:10.1097/j.pain.0000000000000775
4. Abd-Elsayed A, Gyorfi M. Chronic low back pain and cognitive function. Pain Pract. 2023;23(4):463–464. doi:10.1111/papr.13202
5. Galvez-Sánchez CM, Duschek S, Reyes del paso GA. A comparative analysis of cognitive deficits in rheumatoid arthritis and fibromyalgia: impact of symptoms severity and its clinical implications. Psychol Res Behav Manag. 2024;17:1399–1415. doi:10.2147/prbm.S446798
6. Chen J, Wang X, Xu Z. The relationship between chronic pain and cognitive impairment in the elderly: a review of current evidence. J Pain Res. 2023;16:2309–2319. doi:10.2147/jpr.S416253
7. Tofani PS, Máximo RO, Cochar-Soares N, et al. Does the coexistence of pain and depressive symptoms accelerate cognitive decline? Aging Mental Health. 2025;29(2):334–342. doi:10.1080/13607863.2024.2392737
8. Ding M, Xiang S, Zhang Y, et al. From chronic pain to depression: neurogenesis-driven microglial remodeling in the hippocampal dentate gyrus. Science. 2026;391(6791):eaee6177. doi:10.1126/science.aee6177
9. van Merriënboer JJ, Sweller J. Cognitive load theory in health professional education: design principles and strategies. Med Educ. 2010;44(1):85–93. doi:10.1111/j.1365-2923.2009.03498.x
10. Renz MP, Schmidt H, Drusko A, et al. Neural, psychological, and daily life evidence for a transdiagnostic process of affective dysregulation in depression and chronic widespread pain. Pain. 2025;166(12):e788–e806. doi:10.1097/j.pain.0000000000003800
11. Michaelides A, Zis P. Depression, anxiety and acute pain: links and management challenges. Postgrad Med. 2019;131(7):438–444. doi:10.1080/00325481.2019.1663705
12. Hamilton M. Diagnosis and rating of anxiety. Br J Psychiatry Res. 1969;3(special issue):76–79.
13. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23(1):56–62. doi:10.1136/jnnp.23.1.56
14. Moriarty O, Finn DP. Cognition and pain. Curr Opin Support Palliat Care. 2014;8(2):130–136. doi:10.1097/spc.0000000000000054
15. Nadar MS, Jasem Z, Manee FS. The cognitive functions in adults with chronic pain: a comparative study. Pain Res Manag. 2016;2016:5719380. doi:10.1155/2016/5719380
16. Pask S, Dell’Olio M, Murtagh FEM, Boland JW. The effects of opioids on cognition in older adults with cancer and chronic noncancer pain: a systematic review. J Pain Symptom Manage. 2020;59(4):871–893.e1. doi:10.1016/j.jpainsymman.2019.10.022
17. Lier EJ, van Rijn CM, de Vries M, van Goor H, Oosterman JM. The interaction between pain and cognition: on the roles of task complexity and pain intensity. Scand J Pain. 2022;22(2):385–395. doi:10.1515/sjpain-2021-0119
18. van der Leeuw G, Eggermont LH, Shi L, et al. Pain and cognitive function among older adults living in the community. J Gerontol a Biol Sci Med Sci. 2016;71(3):398–405. doi:10.1093/gerona/glv166
19. Ojeda B, Dueñas M, Salazar A, Mico JA, Torres LM, Failde I. Factors influencing cognitive impairment in neuropathic and musculoskeletal pain and fibromyalgia. Pain Med. 2018;19(3):499–510. doi:10.1093/pm/pnx024
20. Tomey K, Greendale GA, Kravitz HM, et al. Associations between aspects of pain and cognitive performance and the contribution of depressive symptoms in mid-life women: a cross-sectional analysis. Maturitas. 2015;80(1):106–112. doi:10.1016/j.maturitas.2014.10.013
21. Melum TA, Steingrímsdóttir ÓA, Jacobsen HB, et al. Associations between cognitive test scores and pain tolerance: the Tromsø study. Scand J Pain. 2024;24(1). doi:10.1515/sjpain-2023-0082
22. Zhou S, Després O, Pebayle T, Dufour A. Age-related decline in cognitive pain modulation induced by distraction: evidence from event-related potentials. J Pain. 2015;16(9):862–872. doi:10.1016/j.jpain.2015.05.012
23. Duan W, Huang J, Huang Q, Dong B. Relationship between pain and dementia: the mediating effect of depression among Chinese elderly. Actas Esp Psiquiatr. 2024;52(2):114–121. doi:10.62641/aep.v52i2.1530
24. Meyers E, Vlaeyen JWS, van den Broeke EN, von Leupoldt A, Palmer AJ, Torta DM. The effect of high versus low cognitive load on the development of nociceptive hypersensitivity: the roles of sympathetic arousal, sex and pain-related fear. Eur J Pain. 2023;27(6):682–698. doi:10.1002/ejp.2098
25. Ng QX, Lim DY, Chee KT. Reimagining the spectrum of affective disorders. Bipolar Disord. 2020;22(6):638–639. doi:10.1111/bdi.12960
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Alleviating Excessive Worries Improves Co-Occurring Depression and Pain in Adolescent and Young Adult Cancer Patients: A Network Approach
Li W, Xu Y, Luo X, Wen Y, Ding K, Xu W, Garg S, Yang Y, Sun H
Neuropsychiatric Disease and Treatment 2022, 18:1843-1854
Published Date: 25 August 2022
Predictive Validity and Patterns of Change Over Time of the Sensitivity to Pain Traumatization Scale: A Trajectory Analysis of Patients Seen by the Transitional Pain Service Up to Two Years After Surgery
Fashler SR, Pagé MG, Svendrovski A, Flora DB, Slepian PM, Weinrib AZ, Huang A, Fiorellino J, Clarke H, Katz J
Journal of Pain Research 2022, 15:2587-2605
Published Date: 31 August 2022
Changes in Mood, Anxiety, and Cognition with Polycystic Ovary Syndrome Treatment: A Longitudinal, Naturalistic Study
Sukhapure M, Eggleston K, Fenton A, Frampton C, Porter RJ, Douglas KM
Neuropsychiatric Disease and Treatment 2022, 18:2703-2712
Published Date: 15 November 2022
Anxiety and Depression in People with Eczema or Psoriasis: A Comparison of Associations in UK Biobank and Linked Primary Care Data
Matthewman J, Mansfield KE, Hayes JF, Adesanya EI, Smith CH, Roberts A, Langan SM, Henderson AD
Clinical Epidemiology 2023, 15:891-899
Published Date: 7 August 2023
Studies on Pain Associated with Anxiety or Depression in the Last 10 Years: A Bibliometric Analysis
Zhang Q, Sun H, Xin Y, Li X, Shao X
Journal of Pain Research 2024, 17:133-149
Published Date: 5 January 2024