Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Changes in Mood, Anxiety, and Cognition with Polycystic Ovary Syndrome Treatment: A Longitudinal, Naturalistic Study
Authors Sukhapure M, Eggleston K, Fenton A ![]() , Frampton C, Porter RJ
, Frampton C, Porter RJ ![]() , Douglas KM
, Douglas KM ![]()
Received 4 August 2022
Accepted for publication 10 November 2022
Published 15 November 2022 Volume 2022:18 Pages 2703—2712
DOI https://doi.org/10.2147/NDT.S385014
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Mayouri Sukhapure,1,2 Kate Eggleston,1,3 Anna Fenton,4,5 Christopher Frampton,1 Richard J Porter,1,3 Katie M Douglas1
1Department of Psychological Medicine, University of Otago, Christchurch, Canterbury, New Zealand; 2Centre for Healthy Brain Ageing, University of New South Wales, Sydney, New South Wales, Australia; 3Specialist Mental Health Services, Canterbury District Health Board, Christchurch, Canterbury, New Zealand; 4Department of Endocrinology, Canterbury District Health Board, Christchurch, Canterbury, New Zealand; 5Oxford Women’s Health, Christchurch, Canterbury, New Zealand
Correspondence: Katie M Douglas, Department of Psychological Medicine, University of Otago, Christchurch, PO Box 4345, Christchurch, 8140, New Zealand, Tel +64 3 3726700, Fax +64 3 3720407, Email [email protected]
Purpose: Individuals with polycystic ovary syndrome (PCOS) are at increased risk of depression and anxiety symptoms and impairment in aspects of cognitive function. However, there is little evidence regarding effects of standard treatment for PCOS on these features of the syndrome. The aim of this study was to examine the effect of 12 weeks of naturalistic treatment of PCOS, with usual medications, on depression symptoms, anxiety symptoms and cognitive function.
Patients and Methods: Thirty-three participants with PCOS received 12 weeks of individualised treatment based on clinical presentation. Changes in depression and anxiety symptoms were assessed with the self-report Hospital Anxiety and Depression Scale at baseline and 12 weeks, and cognitive function was assessed at the same time-points with a battery of tests spanning cognitive domains of verbal learning and memory, visuospatial learning and memory, psychomotor speed, attention and executive function. Outcomes were compared with a control group of 40 healthy participants.
Results: Participants with PCOS (mean age = 29.2 years; mean Body Mass Index = 27.4) were treated with a variety of medications, predominantly spironolactone (n = 22) and oral contraceptives (n = 16). Depression and anxiety symptoms improved significantly over the course of treatment, with moderate effect sizes (Cohen’s d 0.43– 0.55, p < 0.05). Effect sizes of the difference in change from that of the control group were moderate but did not reach statistical significance. Women undergoing PCOS treatment demonstrated significant improvements in aspects of cognitive function, but improvement did not differ significantly from controls and effect size changes were similar, suggesting practise effects in both groups.
Conclusion: Our study provides preliminary evidence that treatment of PCOS may be associated with improvement in psychiatric aspects of the syndrome, particularly depressive symptoms.
Keywords: androgen, depression, cognitive function, testosterone, spironolactone
Introduction
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder in premenopausal women.1 Worldwide prevalence rates are between 5% and 10% depending on the diagnostic definition used,2 and the economic impact is high, with a recent meta-analysis estimating the annual economic healthcare burden of PCOS was $8 billion in the United States.3 It is a heterogenous disorder defined by a combination of signs and symptoms of androgen excess, oligo/anovulation and polycystic ovarian morphology.4 PCOS is associated with psychiatric disorders, including mood and anxiety disorders.5–8 Moderate-to-severe depression and anxiety symptoms are increased in women with PCOS compared with control groups in cross-sectional studies,9,10 and longitudinal studies suggest increased risk of incident depression and anxiety.11 As a result, screening for depression and anxiety has been recommended as a routine part of PCOS assessment,12 and research into treatment for psychiatric aspects of PCOS has been identified as a priority.6
There is preliminary evidence of cognitive impairment in women with PCOS compared with control participants,13,14 which is unsurprising given that cognitive impairment is considered a core feature of depression.15,16 Studies of cognitive function in samples with depression consistently find a broad range of cognitive functions impaired, including verbal and visuospatial learning and memory, executive functions, and psychomotor speed.15 In anxiety disorders, impairment may still be evident across a number of domains, but can often be more circumscribed to attentional biases (to threatening stimuli) and memory dysfunction (working and episodic memory).17 As well as potential effects on cognitive function of comorbid depression and anxiety in PCOS, there are also possible direct effects of androgens on cognition.18
Very few studies have investigated the effects of treatment for PCOS on depression, anxiety, and cognitive function, and studies are small. Findings are mixed, with two studies suggesting a reduction in depression,19,20 one study finding a reduction in depression and non-significant reduction in anxiety21 and two studies showing no improvement in depression or anxiety.22,23 Difficulty in interpreting findings across these studies is also hampered by studies not including no-treatment comparison groups (or healthy control groups), and often using depression measures intended for screening depression rather than assessing sensitivity to change in depression symptoms. With regards to the effects of PCOS treatment on cognitive function, research is even more preliminary. Only one small study has demonstrated improvement in some aspects of cognitive function with PCOS treatment.24 Further research is needed in larger samples with comprehensive and simultaneous measurement of depression, anxiety and cognitive function.
This paper reports longitudinal outcomes relating to mood, anxiety and cognition from a sample of patients treated for PCOS. Cross-sectional (pre-treatment) associations between androgen levels, cognitive function, and mood and anxiety symptoms in this sample have previously been published.7 Higher free testosterone levels were significantly correlated with poorer performance on measures of psychomotor speed and visuospatial learning, even after adjustment for depression and anxiety symptoms.7 Our aim here was to examine, in a preliminary naturalistic study, whether depression, anxiety and cognitive function improved with individualised PCOS treatment, and whether there was an association between change in these outcomes. We hypothesised that depression and anxiety symptoms and cognitive function would improve with treatment, and that this improvement would be greater than that shown over the same time frame by healthy participants.
Materials and Methods
This study was approved by the University of Otago Human Ethics Committee (ref: H14/047) and was performed according to the principles of the Declaration of Helsinki and its later amendments. Written informed consent was obtained from all participants. The approving ethics committee deemed participants in this study (all >16 years) were of sufficient age to provide their own consent for research participation. Data were collected between June 2014 and December 2017.
Participants
Participants aged 16 to 45 years with PCOS were recruited by selective referral from two gynaecological endocrine clinics, as well as by self-referral from advertisements posted in local newspapers and social media, and from flyers posted in public places in Christchurch, New Zealand (health centres, gymnasiums, libraries). PCOS diagnosis was confirmed by a gynaecological-endocrinologist (AF) using the Rotterdam criteria.25 Control participants within the same age-range but with normal androgen levels and no physical signs of PCOS (eg, hirsutism, severe acne, ovarian cysts) were recruited by advertisement (newspapers, online, flyers in public places). Control participants were matched with PCOS participants in a pair-wise manner (within 5 years of age). Exclusion criteria were taking exogenous hormones (other than the oral contraceptive pill, OCP); psychotic disorders (eg, schizophrenia, schizoaffective disorder); neurological conditions (eg, epilepsy, multiple sclerosis); chronic medical illnesses (eg, HIV, cancer); other endocrinological abnormalities (eg, congenital adrenal hyperplasia); alcohol/substance dependence; menopause; hysterectomy; pregnancy; previous serious head injury (loss of consciousness for >1h); current infertility treatment and insufficient visual or auditory functioning for completion of cognitive tests. Individuals in both groups were not excluded for taking psychotropic medication (eg, antidepressant and anxiolytic medication).
Study Design
This is a naturalistic, parallel-group, longitudinal study, in that the treatment for PCOS was not altered from the standard clinical treatment that women would generally receive at gynaecological endocrine clinics in New Zealand. Participants with PCOS were prescribed open-label treatment as clinically indicated by their treating endocrinologist based on their individual symptom profile at baseline. Prescribing followed the recommendations in the 2018 International Guidelines on PCOS.12 Clinical and cognitive assessments were conducted at baseline and 12 weeks for PCOS and control groups. Blood samples were taken at baseline only. For the purposes of this paper, the control group was included primarily to be able to account for practice effects (eg, improved performance) on cognitive measures over time.
Clinical Assessment
Participants were screened using the brief, structured, diagnostic Mini International Neuropsychiatric Interview (MINI)26 to exclude major psychiatric illnesses and alcohol/substance use disorders. These interviews were conducted by the primary author (MS) under supervision from KMD. Body mass index (BMI) was calculated by measuring the height and weight of each participant. Mood and anxiety symptoms were measured using the self-report Hospital Anxiety and Depression Rating Scale (HADS), a 14-item scale designed to assess depression and anxiety symptoms in medical samples.27
Cognitive Assessment
Participants completed a battery of cognitive tests taking approximately 1.5 hours. Pencil-and-paper tests were administered according to standardised instructions28 and computerised tests according to their manual protocols (CogState©). The examiner (MS) was a post-graduate student (Masters in Clinical Psychology), who was trained and supervised by a clinical neuropsychologist (KMD). Cognitive tests could be categorised under one of four cognitive domains: verbal learning and memory, visuospatial learning and memory, attention and executive functioning, and psychomotor speed. See Table 1 for a summary of cognitive domains examined by each test and abbreviated test names. The National Adult Reading Test (NART),29 which involves the participant reading 50 words aloud to the examiner, was used as an estimate of verbal intelligence.
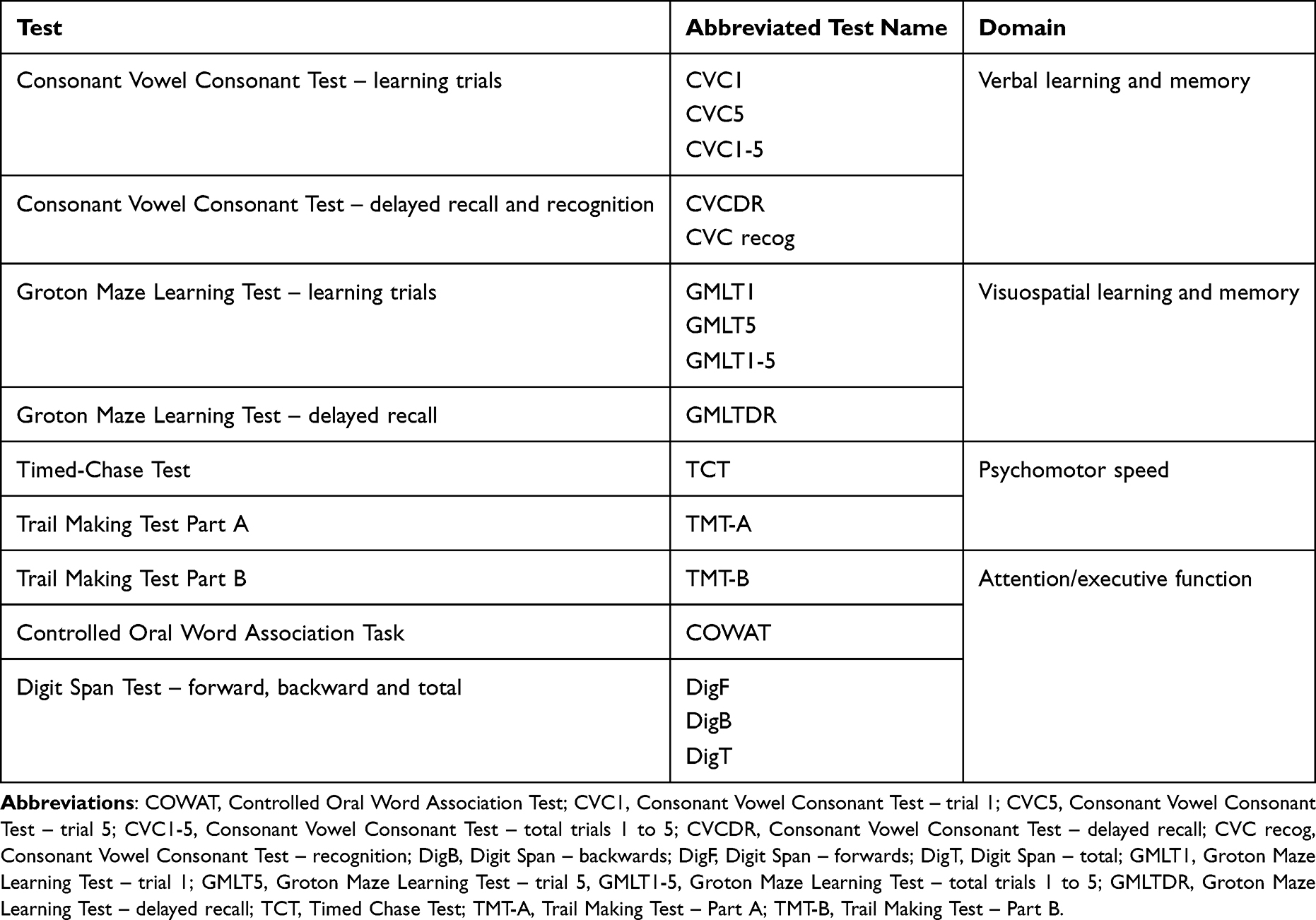 |
Table 1 Cognitive Testing Battery and Cognitive Domains |
Verbal Learning and Memory
Consonant Vowel Consonant (CVC) non-word verbal learning task:30 The CVC task includes nonsense words or “non-words”, rather than words with semantic meaning. Each non-word comprises three letters beginning and ending with a consonant, with a vowel in the middle (eg vev, fol). Pre-recorded lists of 15 non-words are played to participants through a laptop speaker and presented on the screen simultaneously with a gap of 2 seconds between each non-word. The list is presented five times, and after each presentation, the participant is asked to recall as many non-words as possible. Delayed recall is assessed after a period of 15 min. In the recognition trial, the participant is presented with 30 words, comprising 15 new non-words and 15 from the original list and asked whether they have seen the word before or not.
Visuospatial Learning and Memory
Groton Maze Learning Test (GMLT):31 On a computer screen, participants navigate through a 28-step hidden pathway, within a 10-by-10 grid of squares. The process is repeated for four successive learning trials (ie, 5 learning trials in total) and one delayed trial after 20 min. On each trial, the number of errors is recorded.
Psychomotor Speed
Timed Chase Test (TCT):31 Participants chase a moving tile around a grid of squares on the computer screen for 30s. The number of correct moves made per second is recorded.
Trail Making Test Part A (TMT-A):32 Participants connect a series of numbers, unevenly distributed on paper, in ascending order, as quickly as possible. Time taken to complete the task is recorded.
Executive Function
Controlled Oral Word Association Test (COWAT):33 Administered using the letters C-F-L (and P-R-W at follow-up). The number of words generated for each letter, in 90s, is recorded and summed for the three letters, giving a total score.
Trail Making Test Part B (TMT-B):32 Requires participants to connect a series of numbers and letters in ascending order, alternating between the two sequences (1-A, 2-B, etc), as quickly as possible. Time taken to complete the task is recorded.
Verbal Working Memory and Attention
Digit Span Test:34 Participants are read a sequence of numbers and asked to repeat the same sequence back to the examiner in order (forwards) or in reverse order (backwards). Total score (number of sequences correctly recalled) for forwards and backwards are calculated, as well as total score (forwards and backwards summed).
Biological Assessment
Blood samples were collected from all participants by a research nurse at baseline to measure biochemical markers of reproductive status (ie, total testosterone, sex hormone-binding globulin [SHBG]). Free testosterone was calculated from the measured serum levels of total testosterone and SHBG.35 Blood samples measuring hormone levels were not routinely collected at follow-up, but routine checks of biochemistry to ensure medication safety were performed. All remained within appropriate normal ranges.7
Statistical Analysis
Analyses were conducted using the IBM SPSS Statistics for Windows, version 19.36 Baseline demographic and clinical variables were compared between PCOS and control groups using independent samples t-tests. Related sample t-tests were conducted to analyse change in depression symptoms, anxiety symptoms and cognitive functioning over the course of treatment within the PCOS group. Effect sizes were calculated for differences from beginning to treatment-end (Cohen’s d). Change scores were calculated for depression symptoms, anxiety symptoms and cognitive function. Higher scores reflected improved symptoms and performance. Between-group comparisons of change were calculated using independent samples t-tests. Bivariate correlational analysis was used to assess for a relationship between change in mood and anxiety symptoms and change in cognitive function over the course of treatment in the PCOS group. A positive correlation reflected an association between improvement in symptoms and improved cognitive performance.
Results
Eighty-one participants (40 with PCOS, 41 control participants) were recruited and completed baseline assessment. Demographic and baseline clinical characteristics are outlined in Table 2. One control participant and seven participants with PCOS were lost to follow-up. Mean age and anxiety symptoms did not differ significantly between groups. Mean baseline HADS score in PCOS completers was 12.48, reflecting a mildly symptomatic group. Participants with PCOS had significantly higher levels of depression symptoms compared with control participants and there were expected differences in BMI and free testosterone (see Table 2). Regarding ethnicity, 63% of the whole sample (PCOS and control groups combined) identified as New Zealand/European, and 6% as New Zealand Māori, with no significant differences in ethnicity distribution between PCOS and control groups (χ2 = 0.8, p = 0.1). A small number of participants were taking antidepressant (PCOS group, n = 1, control group, n = 4) and anxiolytic (PCOS group, n = 0, control group, n = 2) medications, with no changes to these medications over the 12-week study period and no significant difference between-groups in use of these medications.
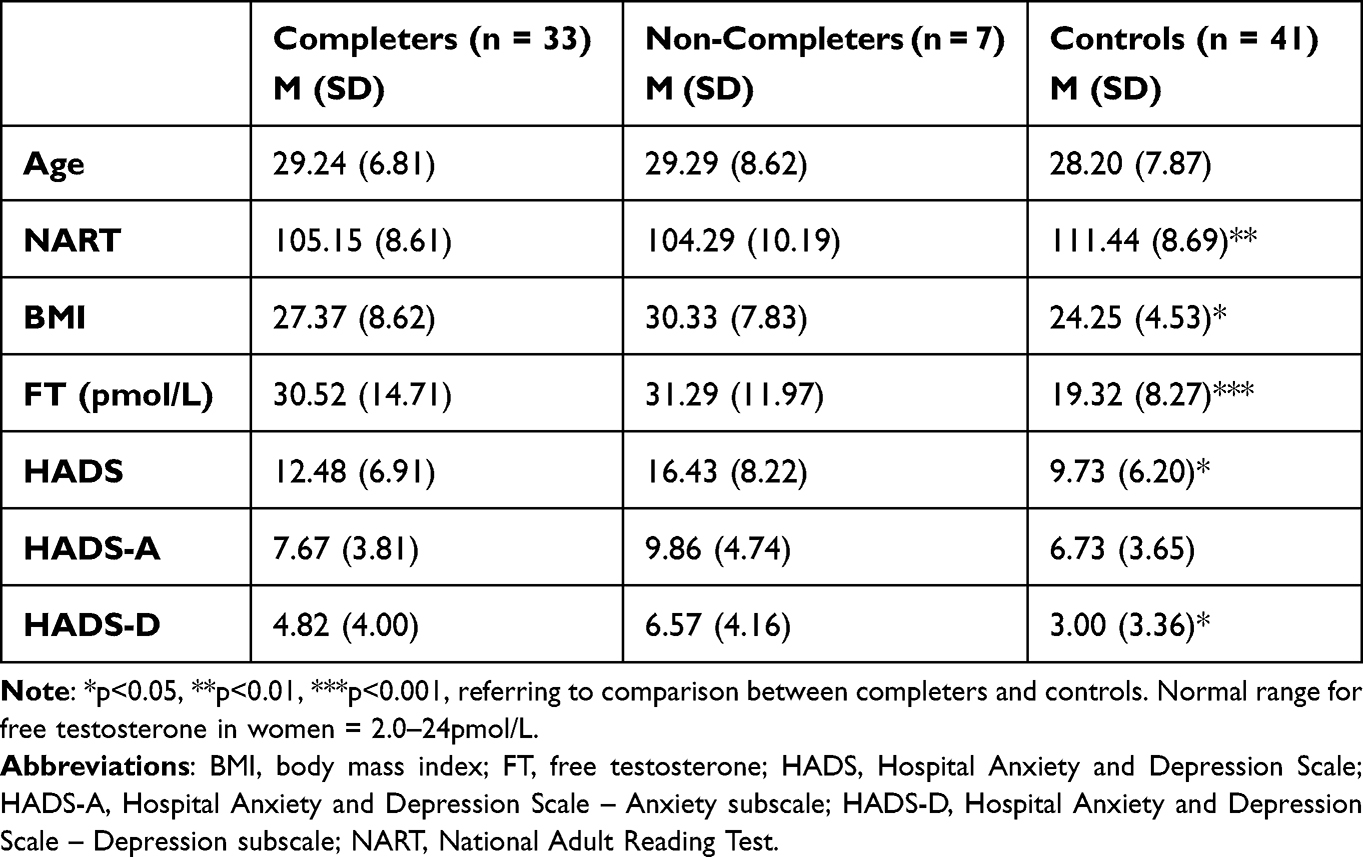 |
Table 2 Baseline Demographics and Clinical Characteristics |
Participants were treated by a gynecological endocrinologist (AF) with a variety of medications for PCOS as clinically indicated (Table 3). Participants were often started on a combination of medications (69.7%, n = 23).
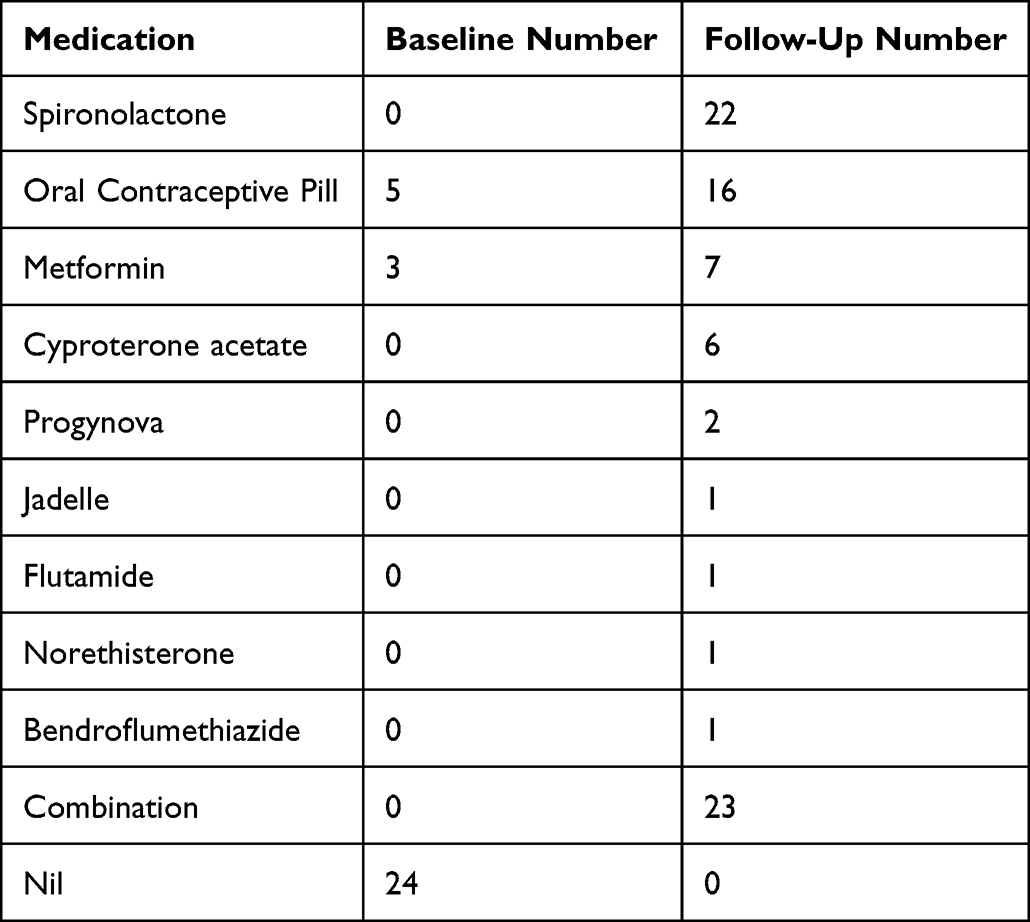 |
Table 3 Types of Polycystic Ovary Syndrome Treatments (n = 33) |
In participants with PCOS, significant reductions in depression and anxiety symptoms over the course of treatment were found (all p < 0.05), with moderate effect sizes (0.43–0.55). Although improvements in depression and anxiety symptoms differed between PCOS and control groups and were moderate in effect, the difference did not reach statistical significance (p = 0.09). There were no significant changes within the control group.
Participants undergoing treatment for PCOS demonstrated significant improvements in aspects of cognitive function with treatment, including measures of verbal learning and memory, visuospatial learning, and psychomotor speed (Table 4). Effect sizes ranged from moderate (Groton Maze Learning Test [GMLT] - total learning: d = 0.39) to large (Trail Making Test – Part A [TMT-A]: d = 0.61) to very large (Consonant Vowel Consonant Verbal Learning Test [CVC] - total learning: d = 1.29). Other aspects of cognitive function did not improve significantly. When compared with control participants, there was a significant difference in performance on the Timed Chase Test (TCT) over the course of treatment (t (71) = 2.53, p = 0.014, d = 0.59; Table 4). This was due to poorer performance in controls at follow-up. There were no other significant between-group differences in cognitive change scores.
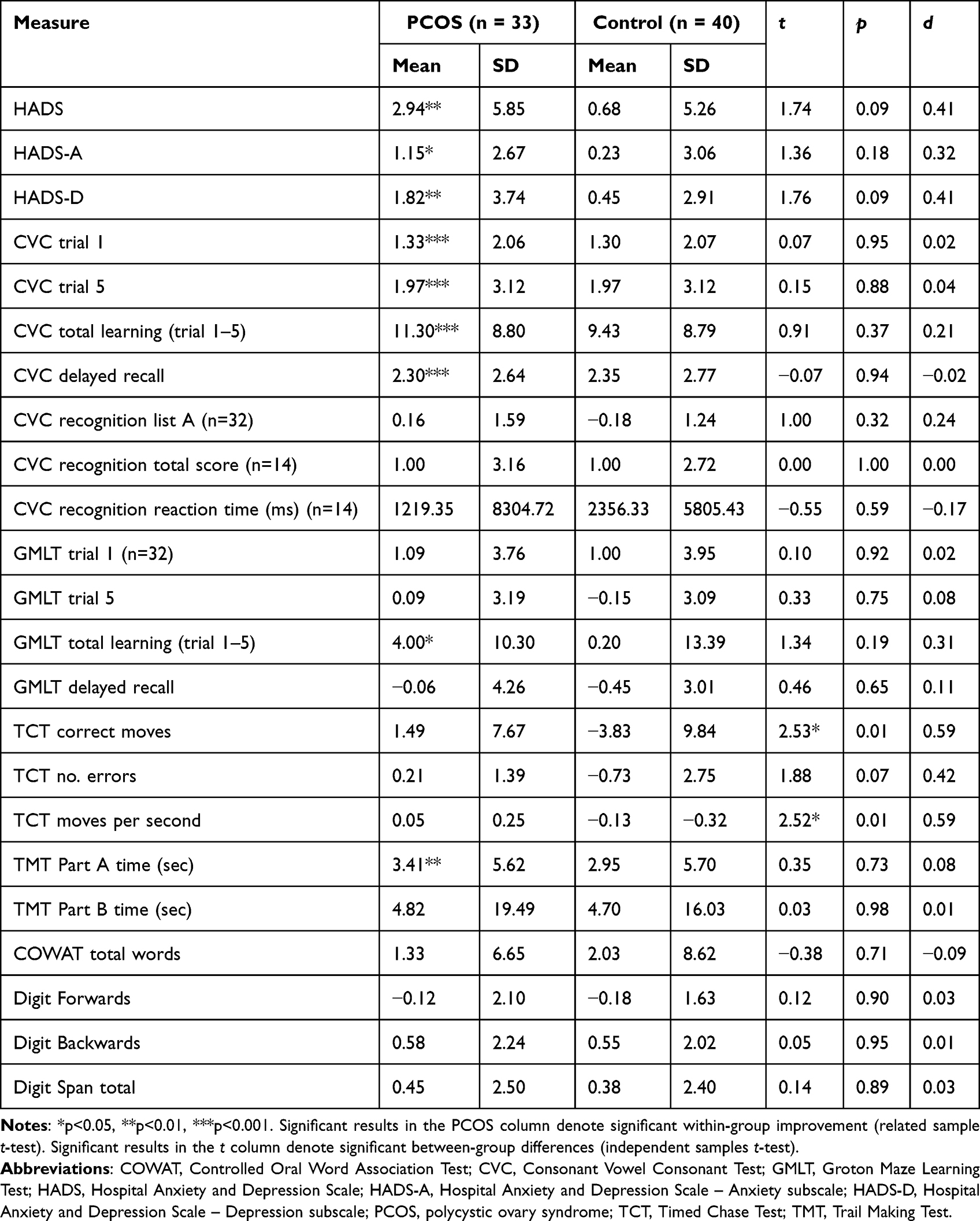 |
Table 4 Change in Depression and Anxiety Symptoms and Cognitive Function Over 12 Weeks of Treatment |
Only one significant correlation was found between change in symptoms of depression and anxiety and change in aspects of cognitive function. Specifically, reduced anxiety (HADS-A) was associated with improvement in Digit Span Forwards (r = 0.37, p = 0.04) (Supplementary Table 1).
Discussion
In this preliminary study, we examined the effect of 12 weeks of naturalistic treatment of PCOS on depression symptoms, anxiety symptoms and cognitive function. Most participants received a combination of treatments, with spironolactone and OCPs the most commonly prescribed. Participants receiving treatment for PCOS showed significant improvement in depression and anxiety symptoms. Effect sizes of change compared with the control group were moderate, but this was not statistically significant. While aspects of cognitive functioning improved in the PCOS group, there was little difference from improvement in control participants – suggesting that this was largely due to practice effects. Change in cognitive function was not correlated with change in depression and anxiety symptoms, with the exception of improvement in Digit Span Forwards with reduced anxiety.
The degree of change found in depression and anxiety symptoms is similar to that seen in previous studies. For instance, a secondary analysis of a randomised controlled trial (RCT) demonstrated a significant reduction in depression prevalence in patients randomised to 16 weeks of a low-dose OCP, compared with patients receiving a lifestyle or combined intervention.21 Additionally, a small observational study found that patients with PCOS who were receiving OCPs (n = 21) were less depressed than those not receiving treatment (n = 11).19 On the other hand, a cohort study (n = 36) found OCPs were not associated with improvement in depression or anxiety symptoms over 6 months, despite improvement in hirsutism and menstrual functioning.22 These studies have some limitations, including the use of a screening instrument and the use of prescription of antidepressants as a proxy for depression and anxiety prevalence.21
While we hypothesised that improvement in depression and anxiety symptoms may relate to anti-androgenic properties of medications, alternative mechanisms may have contributed. For example, the majority of participants were started on spironolactone (n = 22, 66.7%). As well as anti-androgenic actions, spironolactone could improve mood via its action as a mineralocorticoid receptor antagonist,37 and metformin may do the same due to its anti-inflammatory effects.38,39 In this study, only 4 patients had metformin added to their treatment regime. The number was too small to analyse separately. Several previous studies have examined associations between insulin sensitisers and depression and anxiety symptoms. One RCT20 found that, compared with metformin (n = 20), pioglitazone (n = 20) was associated with improvement in depression symptoms in patients with PCOS and moderate depression. On the other hand, Marsh et al23 did not find significant improvement in depression or anxiety symptoms with metformin, but in a very small open-label (n = 7) study.
To our knowledge, the only previous study examining the effect of PCOS treatment on cognitive functioning is a small RCT comparing the effect of cyproterone acetate (CPA) + oestrogen (n = 8) with placebo (n = 11).24 While treatment caused a significant reduction in free testosterone levels, it was only associated with improved performance on a single cognitive measure (verbal fluency) amongst a battery of tests. The study did not compare change with a control group, meaning that it was unable to differentiate from change induced by normal practice effects. Our study did compare with control participants and found that there was no evidence of change compared with that which occurred in the control group, which presumably relates to practice effects.
While current PCOS guidelines suggest that comorbid psychiatric difficulties be managed following conventional treatment algorithms,12 our finding of improvement in depression and anxiety symptoms suggests that individualised PCOS treatment may have beneficial impacts on psychiatric symptoms. This suggests that treatment of PCOS may be a reasonable first-line strategy rather than starting antidepressant medications, with the attendant risk of side effects. However, our findings are preliminary and need to be taken in the context of limitations of this study, and a caveat to this conclusion is that when compared with the control group, the change was not significant.
This study had a number of limitations. First, the relatively small sample size may have limited the ability to demonstrate a significant effect of treatment given that this afforded sufficient power only to demonstrate effect size differences between the groups of 0.6. Second, difficulties demonstrating a difference between groups in change in depression and anxiety symptoms were likely contributed to by the mild levels of symptoms in the PCOS group. Mild depression symptoms may have also meant that less cognitive impairment at baseline in the PCOS group, and less cognitive change over time, was observed, although we do note that even in unmedicated samples with mild-moderate levels of depression and anxiety, significant cognitive impairment can be found.30 Third, the heterogeneous group of medications meant that we were unable to analyse the effects of each medication. In relation to this point, a small number of participants in both groups (total, n = 5) were taking psychotropic medications for depression. It is possible that these medications may have altered performance on cognitive measures in this study, although we note that changes in these medications did not occur over the 12-week period. Fourth, the study was open-label and therefore could not control for placebo effects. Fifth, the selection of patients was not at random or consecutive and therefore there may have been a source of bias in the results. However, the effect of this is likely to have been that more depressed patients were less likely to enter the study and this will have contributed to a negative result regarding mood and anxiety. Sixth, once again because of the low numbers of participants in the study, we were unable to conduct complex multivariate analyses to produce results which were controlled for all possible mediating factors. To do so would have required very large sample size.
The strengths of this study are its naturalistic, individualised approach to treatment; a sample which is larger than previous studies on the effects of PCOS treatment on psychiatric outcomes; and concurrent measurement of depression, anxiety and cognitive function. Participants were comprehensively assessed, with PCOS diagnoses made by a specialist using the Rotterdam criteria, and psychiatric symptoms using a rating scale validated in medical samples. Participants underwent an intensive battery of cognitive testing allowing a number of domains of cognitive function to be examined.
Conclusion
In this novel study, symptoms of depression and anxiety reduced significantly in participants with PCOS receiving individualised treatment. While preliminary, this finding has important clinical implications and suggests that for individuals with PCOS, treatment may have beneficial effects on depression symptoms, in particular. However, given a lack of significant difference in change compared with control participants, the small sample size, and the fact that we were unable, given the sample size, to conduct more complex multivariate analysis, the results must be viewed as preliminary. Further studies of the impact of treatment on psychiatric symptoms and cognitive function in PCOS are indicated. Studies including participants with higher levels of depressive and anxiety symptoms would be of interest and may be more likely to be able to demonstrate significant improvement compared with comparator groups.
Acknowledgments
KMD was supported by a Sir Charles Hercus Health Research Fellowship from the Health Research Council of New Zealand (ref: 19/082) during completion of this paper.
Disclosure
RJP and KMD have used software provided by Scientific Brain Training Pro (SBT-Pro) for research at no cost. RJP has received support for travel to educational meetings from Servier and Lundbeck. The other authors have nothing to declare in this work.
References
1. Conway G, Dewailly D, Diamanti-Kandarakis E, et al. The polycystic ovary syndrome: a position statement from the European society of endocrinology. Eur J Endocrinol. 2014;171:P1–P29. doi:10.1530/EJE-14-0253
2. Bozdag G, Mumusoglu S, Zengin D, Karabulut E, Yildiz BO. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod. 2016;31:2841–2855. doi:10.1093/humrep/dew218
3. Riestenberg C, Jagasia A, Markovic D, Buyalos RP, Azziz R. Health care-related economic burden of polycystic ovary syndrome in the United States: pregnancy-related and long-term health consequences. J Clin Endocrinol Metab. 2022;107:575–585. doi:10.1210/clinem/dgab613
4. Ndefo UA, Eaton A, Green MR. Polycystic ovary syndrome: a review of treatment options with a focus on pharmacological approaches. Pharmacol Ther. 2013;38:336–355.
5. Brutocao C, Zaiem F, Alsawas M, Morrow AS, Murad MH, Javed A. Psychiatric disorders in women with polycystic ovary syndrome: a systematic review and meta-analysis. Endocrine. 2018;62:318–325. doi:10.1007/s12020-018-1692-3
6. Dokras A, Stener-Victorin E, Yildiz BO, et al. Androgen excess-polycystic ovary syndrome society: position statement on depression, anxiety, quality of life, and eating disorders in polycystic ovary syndrome. Fertil Steril. 2018;109:888–899. doi:10.1016/j.fertnstert.2018.01.038
7. Sukhapure M, Eggleston K, Douglas K, Fenton A, Frampton C, Porter RJ. Free testosterone is related to aspects of cognitive function in women with and without polycystic ovary syndrome. Arch Womens Ment Health. 2022;25:87–94. doi:10.1007/s00737-021-01158-9
8. Douglas KM, Fenton AJ, Eggleston K, Porter RJ. Rate of polycystic ovary syndrome in mental health disorders: a systematic review. Arch Womens Ment Health. 2022;25:9–19. doi:10.1007/s00737-021-01179-4
9. Cooney LG, Lee I, Sammel MD, Dokras A. High prevalence of moderate and severe depressive and anxiety symptoms in polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod. 2017;32:1075–1091. doi:10.1093/humrep/dex044
10. Yin X, Ji Y, Chan CLW, Chan CHY. The mental health of women with polycystic ovary syndrome: a systematic review and meta-analysis. Arch Womens Ment Health. 2021;24:11–27. doi:10.1007/s00737-020-01043-x
11. Hung J-H, Hu L-Y, Tsai S-J, et al. Risk of psychiatric disorders following polycystic ovary syndrome: a nationwide population-based cohort study. PLoS One. 2014;9:e97041. doi:10.1371/journal.pone.0097041
12. Teede HJ, Misso ML, Costello MF, et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum Reprod. 2018;33:1602–1618. doi:10.1093/humrep/dey256
13. Barnard L, Balen AH, Ferriday D, Tiplady B, Dye L. Cognitive functioning in polycystic ovary syndrome. Psychoneuroendocrinology. 2007;32:906–914. doi:10.1016/j.psyneuen.2007.06.010
14. Schattmann L, Sherwin BB. Testosterone levels and cognitive functioning in women with polycystic ovary syndrome and in healthy young women. Horm Behav. 2007;51:587–596. doi:10.1016/j.yhbeh.2007.02.007
15. Porter RJ, Robinson LJ, Malhi GS, Gallagher P. The neurocognitive profile of mood disorders–a review of the evidence and methodological issues. Bipolar Disord. 2015;17:21–40. doi:10.1111/bdi.12342
16. Douglas KM, Gallagher P, Robinson LJ, et al. Prevalence of cognitive impairment in major depression and bipolar disorder. Bipolar Disord. 2018;20:260–274. doi:10.1111/bdi.12602
17. Ferreri F, Lapp LK, Peretti CS. Current research on cognitive aspects of anxiety disorders. Curr Opin Psychiatry. 2011;24:49–54. doi:10.1097/YCO.0b013e32833f5585
18. Hamson DK, Roes MM, Galea LA. Sex hormones and cognition: neuroendocrine influences on memory and learning. Compr Physiol. 2011;6:1295–1337.
19. Rasgon NL, Rao RC, Hwang S, et al. Depression in women with polycystic ovary syndrome: clinical and biochemical correlates. J Affect Disord. 2003;74:299–304. doi:10.1016/S0165-0327(02)00117-9
20. Kashani L, Omidvar T, Farazmand B, et al. Does pioglitazone improve depression through insulin-sensitization? Results of a randomized double-blind metformin-controlled trial in patients with polycystic ovarian syndrome and comorbid depression. Psychoneuroendocrinology. 2013;38:767–776.
21. Dokras A, Sarwer DB, Allison KC, et al. Weight loss and lowering androgens predict improvements in health-related quality of life in women with PCOS. J Clin Endocrinol Metab. 2016;101:2966–2974. doi:10.1210/jc.2016-1896
22. Cinar N, Harmanci A, Demir B, Yildiz BO. Effect of an oral contraceptive on emotional distress, anxiety and depression of women with polycystic ovary syndrome: a prospective study. Hum Reprod. 2012;27:1840–1845. doi:10.1093/humrep/des113
23. Marsh CA, Berent-Spillson A, Love T, et al. Functional neuroimaging of emotional processing in women with polycystic ovary syndrome: a case-control pilot study. Fertil Steril. 2013;100(200–7):e1. doi:10.1016/j.fertnstert.2013.02.054
24. Schattmann L, Sherwin BB. Effects of the pharmacologic manipulation of testosterone on cognitive functioning in women with polycystic ovary syndrome: a randomized, placebo-controlled treatment study. Horm Behav. 2007;51:579–586. doi:10.1016/j.yhbeh.2007.02.002
25. Eshre TR; ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2004;81:19–25.
26. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):22–33; quiz 4–57.
27. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67:361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
28. Lezak M. Neuropsychological Assessment. USA: Oxford University Press; 2004.
29. Nelson HE, Willison J. National Adult Reading Test (NART). Nfer-Nelson Windsor; 1991.
30. Bourke C, Porter RJ, Carter JD, et al. Comparison of neuropsychological functioning and emotional processing in major depression and social anxiety disorder subjects, and matched healthy controls. Aust N Z J Psychiatry. 2012;46:972–981. doi:10.1177/0004867412451502
31. Snyder PJ, Jackson CE, Piskulic D, Olver J, Norman T, Maruff P. Spatial working memory and problem solving in schizophrenia: the effect of symptom stabilization with atypical antipsychotic medication. Psychiatry Res. 2008;160:316–326. doi:10.1016/j.psychres.2007.07.011
32. Delis DC, Kaplan E, Kramer JH. Delis-Kaplan Executive Function System (D-KEFS). San Antonio, Texas: The Psychological Corporation; 2001.
33. Benton AL, Hamsher K. Multilingual Aphasia Examination. Iowa City: AJA Associates; 1989.
34. Wechsler D. Wechsler Adult Intelligence Scale (WAIS-IV).
35. Vermeulen A, Verdonck L, Kaufman JM. A critical evaluation of simple methods for the estimation of free testosterone in serum. J Clin Endocrinol Metab. 1999;84:3666–3672. doi:10.1210/jcem.84.10.6079
36. IBM Corp. IBM SPSS Statistics for Windows.
37. von Werne Baes C, de Carvalho Tofoli SM, Martins CMS, Juruena MF. Assessment of the hypothalamic–pituitary–adrenal axis activity: glucocorticoid receptor and mineralocorticoid receptor function in depression with early life stress–a systematic review. Acta Neuropsychiatr. 2012;24:4–15. doi:10.1111/j.1601-5215.2011.00610.x
38. Abdallah MS, Mosalam EM, Zidan A-A-A, et al. The antidiabetic metformin as an adjunct to antidepressants in patients with major depressive disorder: a proof-of-concept, randomized, double-blind, placebo-controlled trial. Neurotherapeutics. 2020;17:1897–1906. doi:10.1007/s13311-020-00878-7
39. AlHussain F, AlRuthia Y, Al-Mandeel H, et al. Metformin improves the depression symptoms of women with polycystic ovary syndrome in a lifestyle modification program. Patient Prefer Adherence. 2020;14:737. doi:10.2147/PPA.S244273
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Comprehensive Review and Androgen Deprivation Therapy and Its Impact on Alzheimer’s Disease Risk in Older Men with Prostate Cancer
Singh M, Agarwal V, Pancham P, Jindal D, Agarwal S, Rai SN, Singh SK, Gupta V
Degenerative Neurological and Neuromuscular Disease 2024, 14:33-46
Published Date: 17 May 2024
Association Between Sleep Quality and Cognitive Function in Patients with Hypertension in Rural Areas of Shanxi Province, China: The Chain Mediating Role of Anxiety and Depression
Li S, Liang R, Liu J, Sun W, Wang J, Li S, Zhao S, Niu Q, Yu H, Zhang H, Qin X, Bai R, Li Y
Psychology Research and Behavior Management 2026, 19:593258
Published Date: 7 April 2026
Depressive Symptoms as a Potential Mediator in the Association Between Pain and Cognitive Function: A Cross-Sectional Study
Gao S, Feng M, Zhou H, Tao Y, Feng L, Xi Y, Guo H, Nangong J, Yang Y, Zhou Y
Journal of Pain Research 2026, 19:595453
Published Date: 3 June 2026