Back to Archived Journals » Open Access Journal of Sports Medicine » Volume 16
Deciding Between ACL Reconstruction, Repair, and Conservative Treatment in Young Athletes: A Systematic Narrative Review
Authors Lewis J, Gul EH, Boden S, Nyland J ![]()
Received 29 October 2025
Accepted for publication 30 January 2026
Published 12 February 2026 Volume 2025:16 Pages 1—24
DOI https://doi.org/10.2147/OAJSM.S534937
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mark Williams
Jonathon Lewis,1 Essa H Gul,1 Stephanie Boden,2 John Nyland2
1School of Medicine, University of Louisville, Louisville, KY, USA; 2Division of Sports Medicine, Department of Orthopaedic Surgery, University of Louisville, Louisville, KY, USA
Correspondence: John Nyland, Division of Sports Medicine, Department of Orthopaedic Surgery, University of Louisville, 550 S. Jackson St., First Floor ACB, Louisville, KY, 40202, USA, Email [email protected]
Objective: The best pediatric and adolescent athlete anterior cruciate ligament (ACL) injury management method remains unknown. This systematic narrative review examined ACL reconstruction (ACLR), ACL repair, and conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option for pediatric and adolescent ACL injury management. The primary purpose was to compare failure rates, return to sport (RTS) rates, and perceived knee function.
Methods: The PubMed, ResearchGate, Google Scholar, Sage Journals, and OVID (Medline) databases were searched. The Modified Coleman Methodology Score (MCMS) assessed study methodological quality and bias risk.
Results: Fifty-six studies were included. Group 1 (ACLR) studies were published before Group 2 (ACL repair) or Group 3 (conservative brace, or rehabilitation-based therapeutic exercise intervention with a delayed ACLR option) studies (Group 1 = 2010.8 ± 9; Group 2 = 2015.9 ± 10; Group 3 = 2018.0 ± 4, p = 0.05). Group 2 displayed “good” quality (MCMS = 70.2 ± 7.9), while Group 1 (MCMS = 63.3 ± 6.8) and Group 3 (MCMS = 59.8 ± 6.4) displayed “fair” quality (p ≤ 0.03). Group 2 had more level 1 or 2 studies, and Group 1 had more level 4 studies (p = 0.007). Lysholm scores were similar (Group 1 = 94.4 ± 2.7, Group 2 = 92.1 ± 6.8, Group 3 = 95, p = 0.51). Group RTS rates were similar (Group 1 = 88.8 ± 14%, Group 2 = 94.1 ± 10%, Group 3 = 78.6 ± 21%; p = 0.22). Group 1 failure rates (7.4 ± 6.6%) were < Group 2 (17.0 ± 19%) (p = 0.02) and Group 3 (32.4 ± 18%) (p < 0.001).
Conclusion: Although ACLR had lower failure rates, neurocognitive, reactive strength, and psychological readiness assessments were underreported. The stronger methodological rigor for ACL repair studies was encouraging but long-term outcomes are lacking.
Keywords: adolescence, anterior cruciate ligament, athletic injuries, knee, pediatrics
Background
Sports-related ACL injuries are increasing among 13–17-year-old athletes,1 and the number of ACLR being performed is increasing in parallel.2 Most athletes return to sports (RTS) post-ACLR;3 however, reinjury rates are high.4 For the adolescent or pediatric athlete, an ACL tear is often more than a season-ending injury as it can lead to an identity crisis with lifelong implications. Because contemporary ACLR techniques do not fully restore native ACL function,5 and may risk growth-plate injury, alternative innervations have emerged. These include primary ACL repair6 and focused conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option.7 Each option requires careful consideration of further growth potential, reinjury risk, long-term neuromuscular and biomechanical adaptations, and early knee osteoarthritis development. Unfortunately, the best pediatric and adolescent athlete ACL injury management method remains unknown.1–7 For these reasons, a systematic narrative review was performed to examine evidence gaps surrounding ACLR, ACL repair, and conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option in pediatric and adolescent athletes. The primary study purpose was to determine which management method had the lowest failure rates, the highest RTS rates, and superior patient-reported outcome measure (PROM) perceived knee function. Secondary outcomes of interest included knee laxity, muscle strength, and functional performance test results.
Methods
This systematic narrative review was performed in alignment with the Cochrane Handbook for Systematic Reviews of Interventions, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 checklist. To minimize selection bias, two independent reviewers searched the PubMed, ResearchGate, Google Scholar, Sage Journals, and OVID (Medline) databases. The initial search was restricted to studies published between January 1, 2015–August 31, 2025. To broaden search results, this range was later expanded without date restrictions. Search terms were developed in consultation with the senior author and medical literature, incorporating standardized Medical Subject Headings (MeSH). Boolean operators “OR” and “AND” were used to combine terms across categories. Population-related terms included pediatric, adolescent, youth, young athlete, skeletally immature, and open physes. Condition terms were anterior cruciate ligament and ACL. Intervention terms included repair, primary repair, suture repair, bridge-enhanced ACL repair (BEAR) technique, reconstruction, physeal-sparing, transphyseal, conservative treatment, and non-operative. Outcome terms included arthrometer, KT-1000, Lachman, pivot-shift, goniometer, range of motion, strength, dynamometer, hop test, return to play, International Knee Documentation Committee (IKDC) score, Knee Injury and Osteoarthritis Outcome Score (KOOS), Lysholm score, and patient-reported outcome measurements (PROM).
Inclusion and Exclusion Criteria
Study eligibility was assessed using the patient/population/problem, intervention, comparison/control, and outcome (PICOS) framework. The target population was skeletally immature athletes aged 13–17 years with radiographic evidence of open physes. Interventions included ACL repair (such as the BEAR, suture, or suture anchor-based techniques), ACLR, non-surgical natural ACL healing strategies (Cross Bracing) or conservative rehabilitation therapeutic exercise-based management with a delayed ACLR option. Primary study outcomes included group RTS rates, failure rates, and PROM use and results. Secondary outcomes of interest included knee laxity (arthrometer, anterior Lachman test, pivot shift test), muscle strength/power (isokinetic or handheld dynamometry), and functional performance (single leg hop testing) test results. Eligible study designs included randomized controlled trials, cohort, and observational studies or case reports with at least five patients. Studies were excluded if non-English, unavailable in full text, if they involved multiple ligament injury surgeries, if they did not include skeletally immature patients, were solely surgical technique papers, were reviews, or consisted of solely of biomechanical or animal data.
Data Extraction
Using a standardized digital spreadsheet, two reviewers (JL, EG) independently extracted data. Variables collected included study design, participant number, age, sex distribution, skeletal maturity confirmation, growth or limb length disturbance, intervention type, comparison group, outcome measures, and follow-up duration. Discrepancies were resolved by consensus with a third reviewer (JN).
Risk of Bias and Quality Assessment
Methodological study quality and bias risk assessments were performed using the Modified Coleman Methodology Score (MCMS),8 a 100-point scale evaluating study size, follow-up, design, diagnostic clarity, intervention description, rehabilitation reporting, outcome validity, objectivity of assessments, statistical analysis, and study design suitability.
Statistical Analysis
Descriptive data analysis and group comparisons were performed using specialized software (IBM-SPSS ver. 29, Chicago, IL, USA). Where applicable, unweighted group study means with standard deviations, or frequencies were determined and statistically compared. Categorical data were compared using Chi-square or Fisher’s Exact tests. Continuous data were compared using either an independent samples t-test or a one-way ANOVA (group) and Tukey post-hoc tests. Meta-analysis elements such as group effect size determination and forest plot creation were not performed. An alpha value of p ≤ 0.05 was selected to indicate statistically significant differences. When feasible, the biological, biomechanical, physiological, or clinical rationale for observed group differences were qualitatively discussed.
Results
Methodological Quality and Bias Risk Assessment
The initial search identified 58 studies with MCMS of 60.4 ± 9.7 (fair).9–67 To better focus study analysis on the methodologically strongest studies, a MCMS cut-off threshold was established of the overall mean score minus one standard deviation. This resulted in 50 studies (Group 1: ACLR, n = 33; Group 2: ACL repair, n = 13; and Group 3: conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option (n = 4)). To better target long-term studies, a second search was performed resulting in an additional 13 studies identified that also underwent MCMS determination.68–80 This resulted in six studies being added to the review.69,70,76–79 With these additions, the study number increased to 56 with a mean MCMS of 64.6 ± 7.7 (Table 1) (Figure 1).
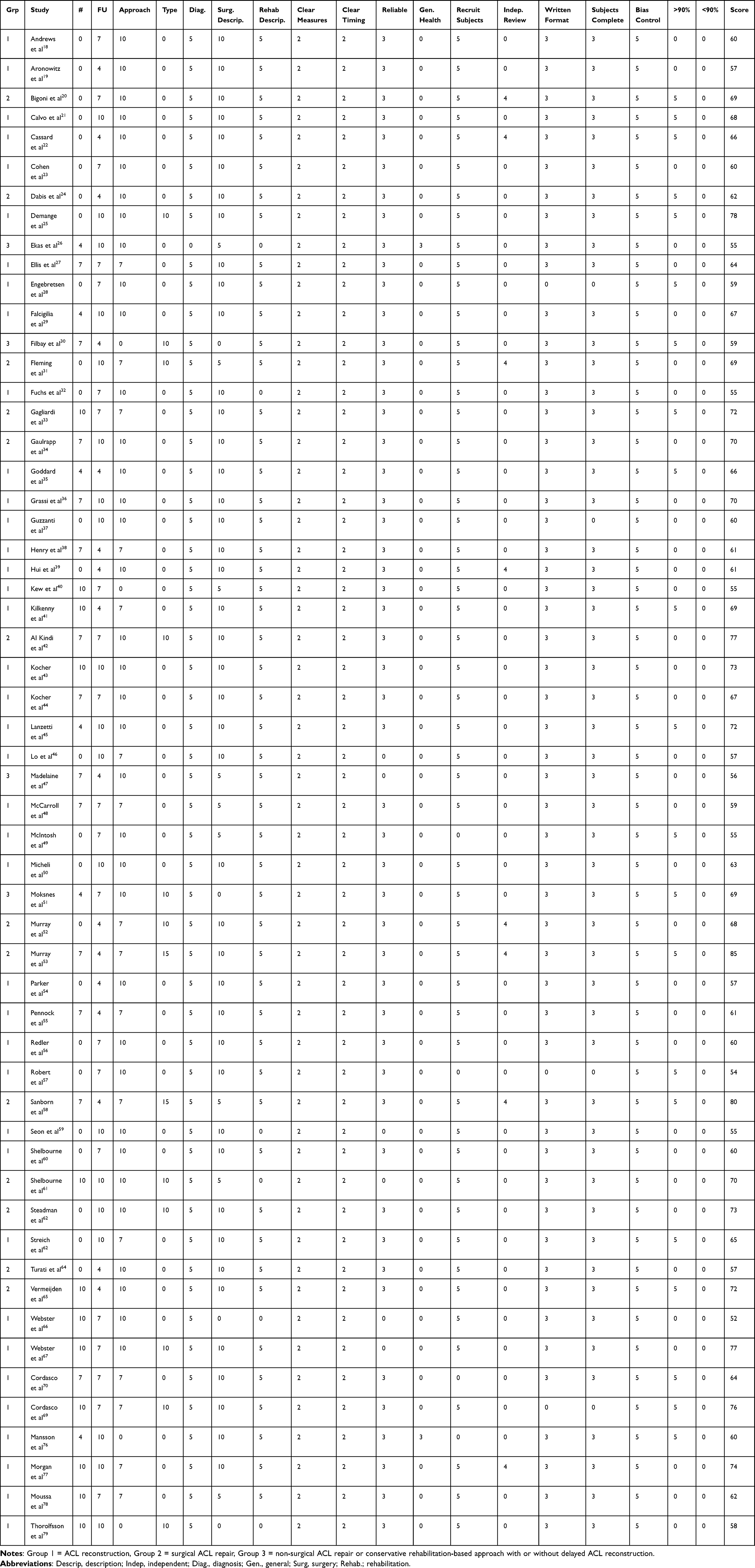 |
Table 1 Modified Coleman Methodology Scores (MCMS) |
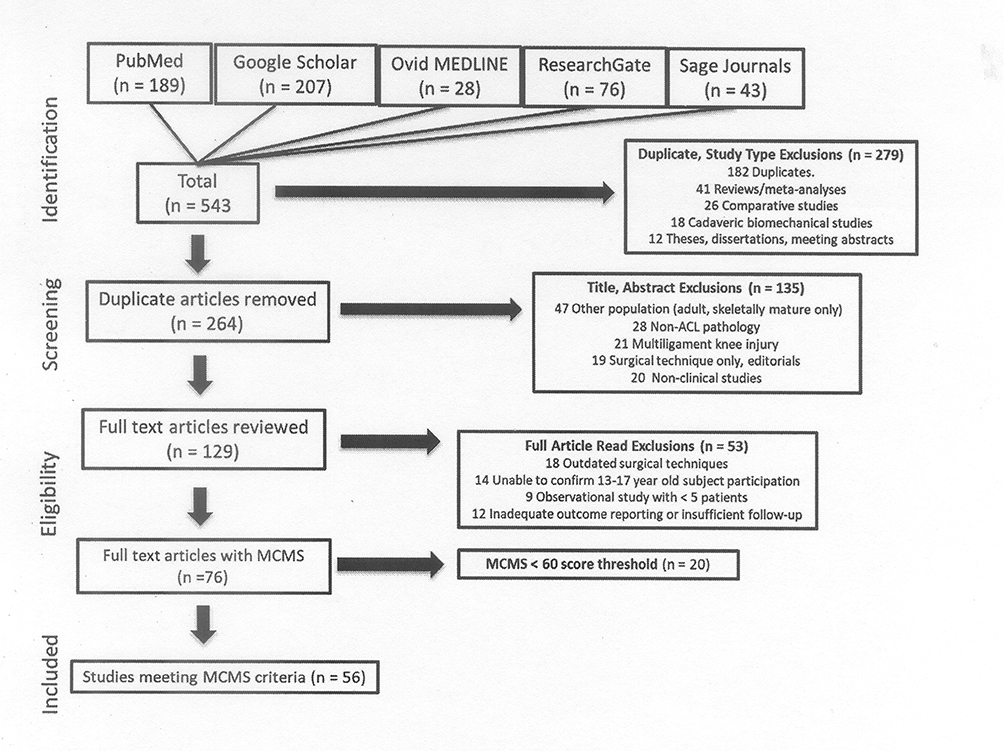 |
Figure 1 PRISMA study selection diagram. |
Group 1 (ACLR) studies were published earlier than Group 2 (ACL repair) or Group 3 (conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option) studies (Group 1 = 2010.8 ± 9; Group 2 = 2015.9 ± 10; Group 3 = 2018.0 ± 4, p = 0.05). Group 2 (ACL repair) studies had higher MCMS (70.2 ± 7.9) than Group 1 (ACLR) (63.3 ± 6.8) (P = 0.009) and Group 3 (conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option) studies (59.8 ± 6.4) (p = 0.03). Overall, Group 2 studies displayed good methodological research study quality, whereas Groups 1 and 3 were fair. Group 2 had more evidence level 1 or 2 studies (prospective) than Group 1 which had more evidence level 4 studies (retrospective) (p = 0.007). Mean patient age, sex distribution, participant numbers, and follow-up durations were comparable between groups (Table 2).
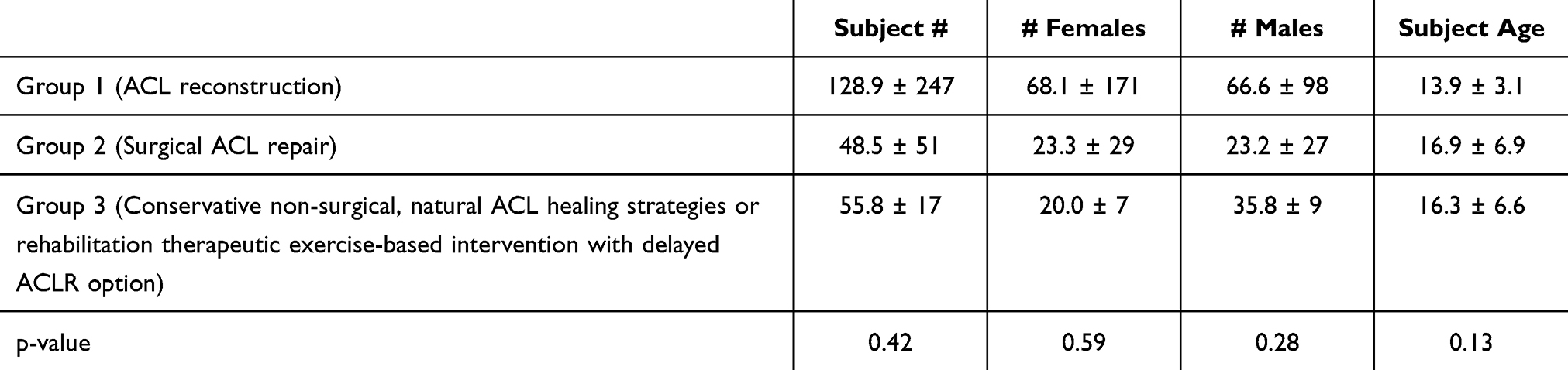 |
Table 2 Group Patient Gender and Age Demographics (Mean ± Standard Deviation) |
Group 1: ACL Reconstruction
The ACLR group surgical methods are described in Table 3. Twenty one studies used a transphyseal surgical approach,19,21,23,27,29,32,35,40,41,44,48,49,55,56,59–61,63,66,67,77 ten studies used an “over the top” surgical approach at the femur and a transphyseal approach at the tibia,18,25,29,36,38,43,45,46,50,54 two studies used either an all epiphyseal or transphyseal approach,69,78 one study used either an all epiphyseal, partial transphyseal, or complete transphyseal approach,70 two studies used an intraepiphyseal approach,22,37 and one study used the Clocheville method.57
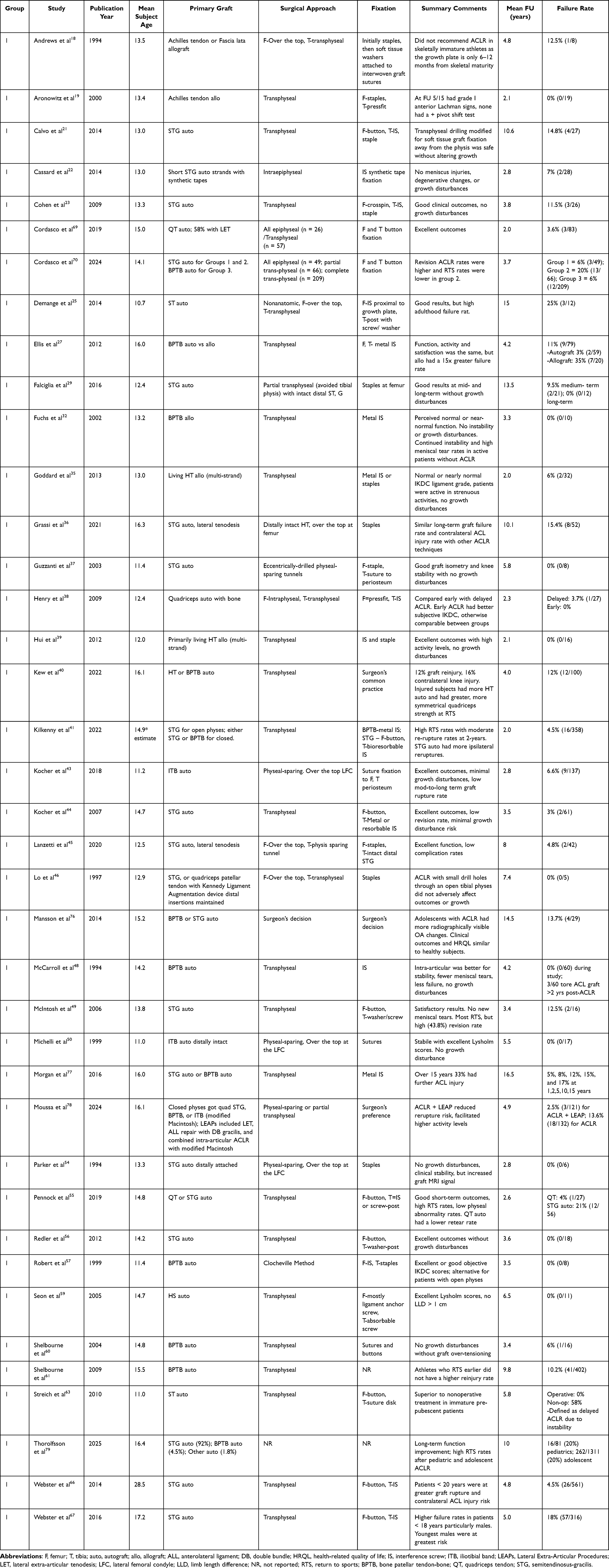 |
Table 3 ACLR Study Primary Graft, Surgical Approach, Fixation, Summary Comments, Mean Follow-Up (FU), and Failure Rate |
Group 2: ACL Repair
ACL surgical repair methods are shown in Table 4. Four studies used the BEAR technique,31,52,53,58 six studies used sutures or suture-anchor combinations,20,28,33,42,64,65 one study used the healing response technique,62 one study used four different methods,34 and one study used small diameter transphyseal tunnels with resorbable suture tape and cortical suspension button fixation.24
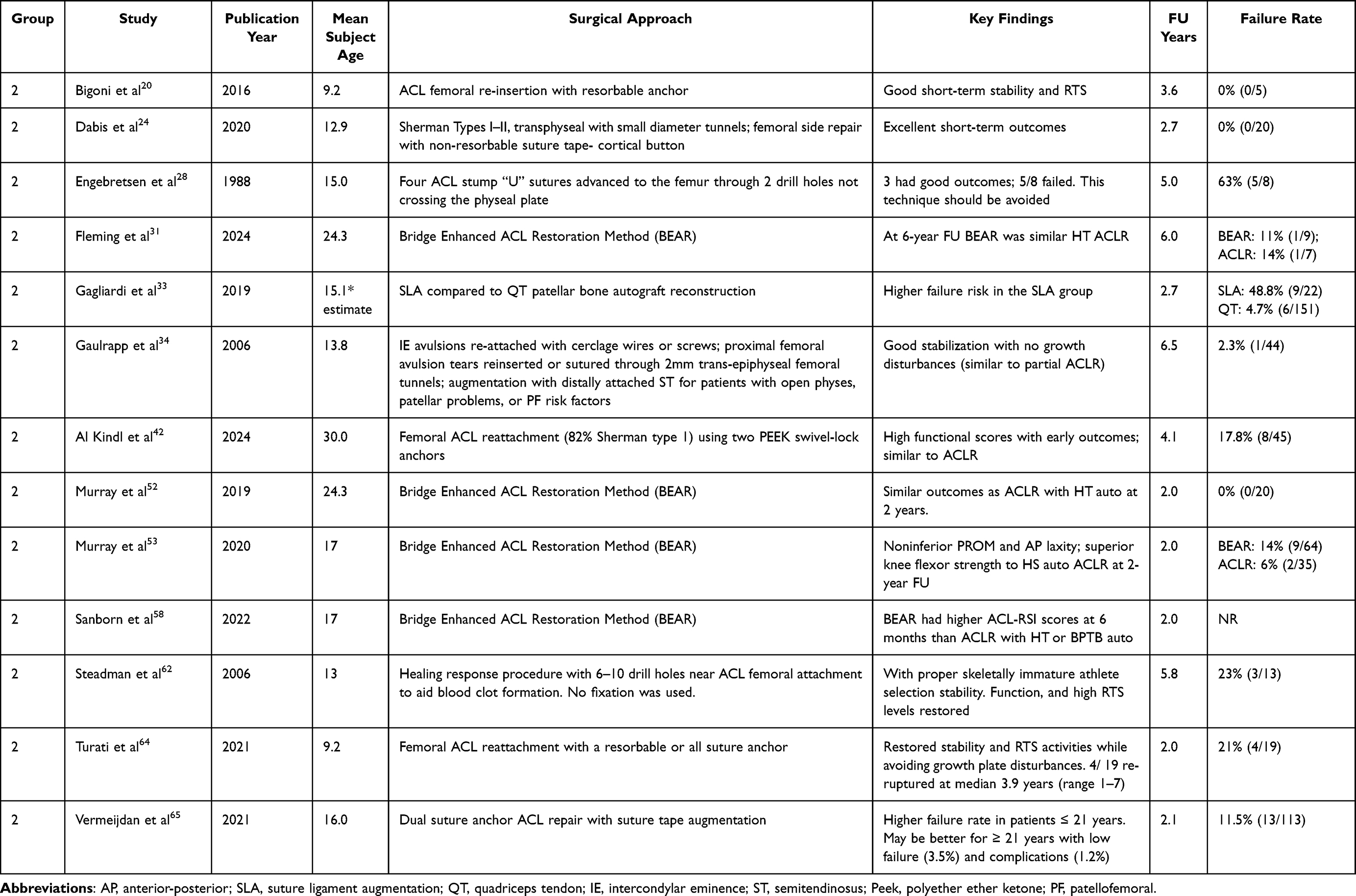 |
Table 4 Surgical ACL Repair Studies, Publication Year, Mean Subject Age, Surgical Approach, Key Findings, Follow-Up (FU), and Failure Rate |
Group 3: Conservative Brace, or Rehabilitation-Based Therapeutic Exercise Interventions with a Delayed ACLR Option
Non-surgical ACL healing strategies using Cross bracing30 and conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option26,30,47,51 are shown in Table 5.
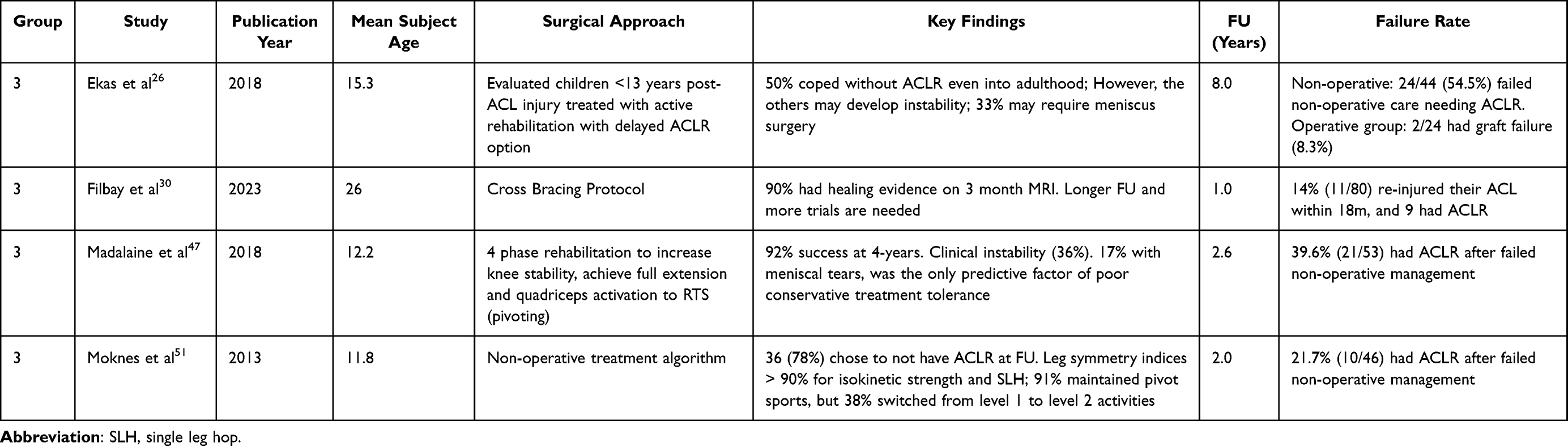 |
Table 5 Conservative Brace, or Rehabilitation-Based Therapeutic Exercise Intervention with Delayed ACLR Option Group Studies, Publication Year, Mean Subject Age, Surgical Approach, Key Findings, Follow-Up (FU), and Failure Rate |
Follow-Up
Mean final follow-up timing was comparable between groups (Group 1 = 5.6 ± 3.9 years, Group 2 = 3.6 ± 1.8 years, Group 3 = 3.4 ± 3.1 years, p = 0.12).
Patient Reported Outcome Measures
The most used PROM for Group 1 were: the Lysholm score (n = 15),19,21,23,27,32,36,43,45,49,50,54–56,59,63 International Knee Documentation Committee (IKDC) Subjective score (n = 10),21,23,29,38,43,49,56,60,63,78 IKDC Objective score (n = 4),32,38,46,57 Cincinnati/Noyes Scoring System (n = 3),18,54,60 Knee Injury and Osteoarthritis Outcome Score (KOOS) (n = 4),36,76,78,79 Tegner Activity Scale (n = 11),21,27,36,45,49,55–57,63,76,78 Pediatric IKDC questionnaire (Pedi-IKDC) (n = 1),45 Visual Analog Scale (VAS) pain score (n = 2),36,60 the Hospital for Special Surgery Functional Activity Brief Scale (HSS Pedi-FABS) (n = 1),54 Short Form 36 (n = 1),76 EQ-5D-5L (n = 1),76 the Single Assessment Numeric Evaluation (SANE) (n = 1),55 and the ACL-Return to Sport Index (n = 1).78 For Group 2, the most frequently used PROM included the Lysholm score (n = 6),20,24,28,34,64,65 IKDC Subjective score (n = 4),20,31,58,65 Tegner Activity Scale (n = 5),20,24,28,34,64 Pedi-IKDC (n = 1),64 ACL-RSI (n = 1),58 KOOS (n = 2),24,31 SANE (n = 1),65 Cincinnati/Noyes Knee Rating (n = 1),65 and Objective IKDC score (n = 1).34 For Group 3, the most frequently used PROM were the IKDC Subjective score (n = 2),26,51 and the Lysholm score,30 KOOS51 and Knee-related Quality of Life Survey30 (each n = 1). Overall, the Lysholm score was the most used PROM with similar group scores at final follow-up: Group 1 = 94.4 ± 2.7, Group 2 = 92.1 ± 6.8, and Group 3 = 95 (p = 0.51).
Ligamentous Knee Laxity
In Group 1 (ACLR), 20 studies (51.3%, 20/39) reported anterior Lachman test results.18,19,21–23,25,29,32,37,38,44–46,50,54,56,59,60,63,76 In Group 2 (ACL repair), 6 studies (46.2%, 6/13) reported anterior Lachman test results.33,34,52,53,58,64 In Group 3 (conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option) 3 of 4 studies (75%) reported anterior Lachman test laxity26,30,47 (Table 6). Eighteen of 39 (46.2%) of ACLR group studies reported pivot shift test results.18,19,21–23,25,32,35,39,43–46,49,54,56,63,76 Graft type (p = 0.81) and bone tunnel preparation/graft placement method (p = 0.20) did not display differing pivot shift test results. Five of 13 (38.5%) ACL repair group studies reported pivot shift test results.20,31,52,53,64 In Group 3 (conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option) 3 of 4 studies (75%) reported pivot shift test results.30,47,51 Each of these studies reported greater pivot shift laxity with conservative intervention management. Using the Cross Bracing protocol, Filbay et al30 reported that 42.5% (17/40) of patients displayed a positive pivot shift test 6 months post-intervention. The ACLR group had more studies with ≥ 85% negative pivot shift test results compared to the other groups (p = 0.001).
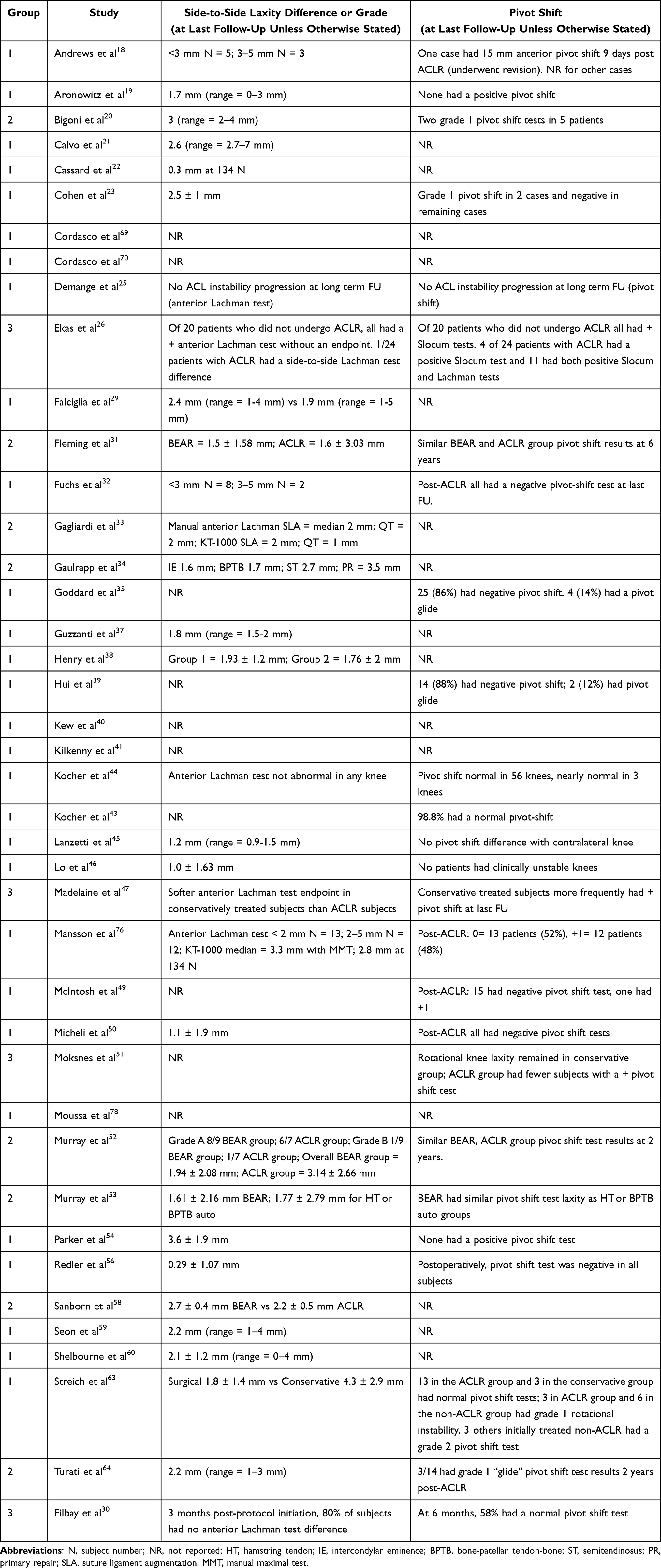 |
Table 6 Group Anterior Laxity and Pivot Shift Test Results |
Isokinetic or Handheld Dynamometry, Single Leg Hop Testing, and Return to Sport Criteria
Group isokinetic or handheld dynamometry testing, functional hop testing, RTS decision-making criteria, and outcomes are shown in Supplemental Table 1. In the ACLR group 6 studies (15.4%, 6/39)40,41,54,60,69,76 used isokinetic or instrumented handheld dynamometry to measure strength. In the ACL repair group 6 studies (46.2%, 6/13)28,31,52,53,58,65 also used isokinetic or handheld dynamometry to measure strength. In the conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option group, 2 studies (50%, 2/4)26,51 used isokinetic or handheld dynamometry to measure strength. The ACL repair and conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option groups had significantly greater isokinetic or handheld dynamometry test use frequency (p = 0.04).
In the ACLR group 7 studies (17.9%, 7/39)27,35,39,40,54,69,76 reported single leg hop testing. In the ACL repair group 6 studies (46.2%, 6/13)20,31,52,53,58,64 reported single leg hop testing. In the conservative brace, or rehabilitation-based therapeutic exercise intervention with delayed surgery option group, 2 studies (50%, 2/4)26,51 reported single leg hop testing. The ACL repair and conservative brace, or rehabilitation-based therapeutic exercise intervention with delayed surgery option groups had significantly greater single leg hop test frequency (p = 0.05). Group 1 (ACLR) had 16 studies that described at least basic RTS criteria (16/39, 41.0%).18,19,21,29,41,44,45,48,55–57,60,61,63,69,70 Group 2 (ACL repair) had 4 studies that described at least basic RTS criteria (4/13, 30.8%).24,58,62,65 Group 3 (conservative brace, or rehabilitation-based therapeutic exercise intervention with delayed surgery option) had one study that described at least basic RTS criteria (1/4, 25%).30 Groups displayed similar RTS criteria use frequency (p = 0.69).
Failure and Return to Sport Rates
Group 1 displayed lower mean reported failure rates (7.4 ± 6.6%) compared to Group 2 (17.0 ± 19%) (p = 0.02) and Group 3 (32.4 ± 18%) (p < 0.001) (Figure 2). The predominant bone tunnel preparation/graft placement method was transphyseal drilling (n = 21), followed by physeal sparing tibial tunnel drilling with over the top femoral side graft placement (n = 3) or transphyseal tibial tunnel drilling with over the top femoral side graft placement (n = 3). Failure rate differences were not observed between different bone tunnel types or over the top graft placement (p = 0.39) or for different graft types (p = 0.93). Groups did not display statistically significant RTS rate differences (Figure 3) (Table 7). Among ACLR studies, graft type (p = 0.53) and bone tunnel preparation/graft placement method (p = 0.22) did not contribute to RTS rate differences.
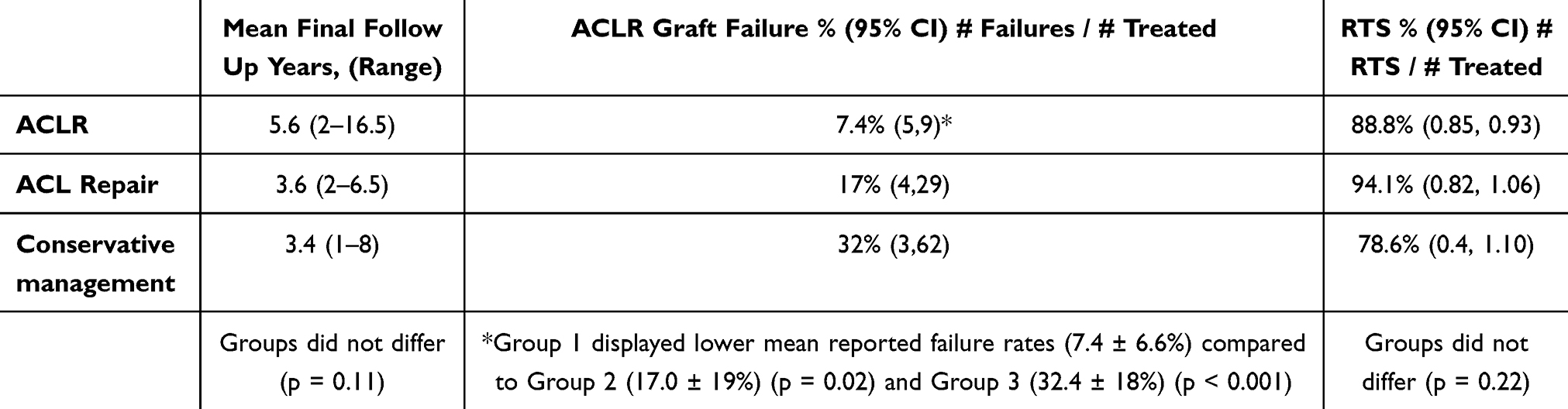 |
Table 7 Mean Group Failure and RTS Rates (Including Inclusive Comparative Study Results) |
 |
Figure 2 The ACLR group displayed lower mean reported failure rates compared to the ACL repair (p = 0.02) and to the conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option groups (p < 0.001). |
 |
Figure 3 Groups displayed similar RTS rates (p = 0.22). |
Discussion
Comparison groups had similar mean patient age, sex distribution, participants/study, and follow-up durations. Primary and secondary results and qualitative syntheses of the biological, biomechanical, physiological, or clinical rationale for observed group differences are discussed.
Research Evidence Levels
The ACL repair group displayed good methodological research study quality with higher MCMS than the ACLR or the conservative brace, or rehabilitation-based therapeutic exercise intervention with delayed ACLR option groups. The ACL repair group also had more evidence level 1 or 2 studies than the other groups, while the ACLR group had more evidence level 4 studies. This finding suggests that ACL repair studies, although lacking long-term follow-up, had methodologically stronger short-term efficacy evidence. The more recent mean publication year for this group was likely associated with stronger methodologies.
Failure Rates
The most important study finding was that the ACLR group had lower failure rates than the ACL repair, or conservative brace, or rehabilitation-based therapeutic exercise intervention with delayed ACLR option groups. The current study did not identify one particular technique that best prevented growth or alignment disturbance, minimized recurrent knee injuries, or optimized RTS outcomes. Although delaying ACLR until physeal closure increases graft options, maintaining pivot sport restrictions in young athletes can be difficult, and RTS without a functioning ACL increases secondary meniscal or articular cartilage injury risk.76 Regardless of the surgical technique or graft used, ACLR had lower failure rates than the other groups. The graft collagen scaffold may have provided superior failure resistance to ACL repair, native ACL healing, or neuromuscularly mediated knee stability responses.
Return to Sport Rates
Return to sport rates were similar between groups. This finding, however, may be obscured by the diverse ways that RTS readiness was determined. Although group differences were not statistically significant, longer final mean follow-up timing for the ACLR group may have reduced its RTS rate compared to the other groups. For up to 2 years post-ACLR or ACL repair, the contralateral, native ACL has increased metabolic activity suggesting a systemic inflammatory process.81–83 With increasing contralateral ACL injuries in high-risk young athletes after non-contact ACL injury and ACLR, more time and greater scrutiny of contralateral native ACL health might be needed in addition to more stratified RTS and return to performance decision-making criteria.84 Serial advanced imaging assessments of unilateral ACL graft and contralateral native ACL health post-ipsilateral ACL injury and ACLR may better enable re-injury (ipsilateral) or injury (contralateral) risk determination.84
Patient Reported Outcome Measures
The Lysholm Knee Scoring Scale was the most frequently used PROM with similar scores at final follow-up for ACLR = 94.4 ± 2.7; ACL repair = 92.1 ± 6.8; and for conservative brace, or rehabilitation-based therapeutic exercise intervention with delayed ACLR option = 95 (p = 0.51). These findings suggest comparable perceived sports knee function. However, survey administration timing differed between studies and the Lysholm Knee Scoring Scale was developed primarily for adults making it potentially less valid than the ACL-RSI, the Pedi-IKDC, or the HSS Pedi-FABS for adolescent or pediatric patients.
Ligamentous Knee Laxity
Conservative interventions are encouraging, but unless high pivot-dependent activities are avoided, with decreased knee stability many patients eventually develop meniscal tears and/or articular cartilage injuries.51,68 Better ACLR group pivot shift test outcomes support the lower failure rates that we report.
Isokinetic or Handheld Dynamometry Strength Testing
The ACL repair and conservative brace, or rehabilitation-based therapeutic exercise intervention with delayed ACLR option groups had more frequent isokinetic or handheld dynamometry test use than the ACLR group (p = 0.04). More frequent isolated knee strength recovery assessments in these groups suggest that RTS decision-making for these groups may have been less post-surgery time-based than for the ACLR group.
Single Leg Hop Testing
The ACL repair and conservative brace, or rehabilitation-based therapeutic exercise intervention with delayed ACLR option groups more frequently reported single leg hop test use. This finding also suggests that RTS decisions for these groups may have been less post-surgery time based than in the ACLR group.
Return to Sport Criteria
Groups had similar RTS criteria use frequencies. The best recovery path, however, may depend less on what is currently being measured and more on rehabbing athlete characteristics that to date have remained largely unappreciated (neurocognitive, reactive strength, and psychological factors).58 For obvious reasons, physical performance tests predominate RTS criteria. The lack of neurocognitive function, reactive strength, and psychological profile assessments, however, is worrisome. Incorporating these factors into future research and rehabilitation protocols would improve return to sport decision-making. Psychological factors are key recovery determinants post-ACL injury.58,66,67,85 The American Academy of Orthopaedic Surgeon guidelines86 recommend ACLR ≤ 3 months post-ACL injury. Early ACLR, however, may not provide young athletes with sufficient cognitive appraisal time to better understand recovery, or to reflect about the future role of sports in their lives.
Existing Gaps
To better determine neuromuscular system recovery post-ACL injury intervention, ACLR studies need to make greater use of both serial instrumented muscle strength dynamometry and single leg hop tests. All future studies need to better assess neurocognitive, reactive strength, and psychological factors. Advanced imaging identification of neurocognitive activation pattern locations, amplitudes, and onset timing may help clarify which intervention produces the superior short- and long-term functional outcomes that decreases both ipsilateral ACL graft re-injury or contralateral knee injury rates.87–89
With lower failure rates, ACLR is currently the gold standard for pediatric and adolescent patients who intend to return to pivoting and cutting sports. Although ACLR had lower failure rates, PROM and RTS rates were comparable between ACLR and ACL repair. Therefore, the selected intervention should be individualized based on the evidence provided by methodologically stronger study designs. For high risk, high demand young athletes who play pivoting sports and have a non-contact ACL injury family history, increased generalized joint laxity, or genu recurvatum ≥ 10°, some recent studies recommend supplemental anterolateral ligament (ALL) repair or lateral extra-articular tenodesis (LET).90 In addition to including more comprehensive health domain assessments, greater patient sample stratification by physiological age, sex, skeletal maturity level, sport type, and adolescent developmental phase will improve our understanding of which approach best facilitates more complete recovery,81 not just ACL graft healing or physical performance function restoration. Group difference interpretations should account for confounding factors such as skeletal maturity, sport-specific demands, baseline activity level, sex, and rehabilitation protocol variations, which were inconsistently reported across studies. Given that both ACL repair and conservative interventions preserve native ACL mechanoreceptors, fertile research areas include knee joint proprioceptive/kinesthetic position/alignment sense accuracy, lower extremity neuromuscular activation onset timing,88 and reactive force restoration assessments.89 Preserving native ACL mechanoreceptors may offer potential neuromuscular control and dynamic joint stability benefits; however, direct evidence for improved long-term outcomes in skeletally immature patients is limited.5,91 Serial advanced imaging may help determine which intervention most effectively reduces the systematic inflammatory responses that increase contralateral native ACL metabolic activity.84 Improved understanding of the interconnections between biological healing, mechanical stability, psychological readiness, neurocognitive, and reactive neuromuscular function should strengthen rehabilitation recovery. Well-timed, more comprehensive health domain measurements represent the next pediatric and adolescent ACL injury management frontier. Even the term RTS should evolve from simple “yes”, or “no” responses to more stratified, serial holistic health and sustainable athletic performance validations. No single intervention works best for every young athlete. Outcome success depends on effective alignment of multiple developmental, environmental, and personal factors. Reviewed studies rarely reported confounding variable differences that might have influenced recovery and reinjury risk such as rehabilitation strategies, surgical timing relative to skeletal maturity, hormonal influences (sex hormone levels), sport specialization, and socioeconomic status. To enable more meaningful intervention comparisons these factors should be reported with greater detail.
Future Directions
Rehabilitation targeting neuromuscular control and dynamic knee stability are essential not only for conservative interventions, but also post-ACLR or ACL repair. Well-designed, more comprehensive strategies can also help guide future RTS criteria development. Within motor learning of sound athletic movements lies an important opportunity to better restore and perhaps improve both physical and mental health.
Although the evidence is limited, for young active patients with Sherman grade I–II ACL tears, surgical repair may present some advantages.6,52 With ACL repair, autogenous tendon harvest for graft creation is not needed, reducing arthrogenic inhibition likelihood.91 Although early results are encouraging, fewer patients have undergone BEAR technique treatment and long-term follow-up is lacking. The conservative Cross Bracing protocol30 presents encouraging non-surgical natural ACL healing, however, evidence for its efficacy is limited, particularly for 13–17 year patients and the 3 month braced knee flexion requirement may deter compliance. Although this intervention shows promise, the case series only had one year follow-up and the failure rate at 5–18 months post-protocol was 14%.30 For some patients prolonged bracing and structured rehabilitation may also facilitate concomitant meniscal or articular cartilage injury healing, however, this data is limited, derived primarily from a small number of patient cases.
At 6 months post-ACL repair, Sanborn et al58 reported that patients who underwent ACL repair with the BEAR technique had a mean 12.9 points higher ACL-RSI scale score (psychological readiness), which was more strongly associated with higher subjective IKDC scores (perceived sports knee function) than in patients who had ACLR with a quadrupled hamstring or bone-patellar tendon-bone autograft. Studies suggest that ACL-RSI cutoff scores of 60 and 62 are predictive of an RTS at pre-injury sports level.85,92 In the Sanborn et al58 study, the BEAR group mean ACL-RSI score was 15% > those thresholds suggesting that BEAR ACL repair may translate into better early post-ACLR psychological outcomes. Webster and Feller85 reported an ACL-RSI score of 65 as a benchmark for successful RTS 12 months post-ACLR, further supporting early psychological improvement. At 6 months post-ACLR, the mean ACL-RSI score for the BEAR group was 71.1 ± 2.9 compared to 58.2 ± 3.9 for the ACLR group. Isokinetic knee muscle strength outcomes paralleled these findings. At 6 months post-ACL repair, the BEAR group had a 10% increase in knee flexor torque (% of contralateral side) which was associated with a 2.5 point ACL-RSI score increase, while a 10% increase in knee extensor torque resulted in a 3.7 point ACL-RSI score increase. Anteroposterior knee laxity differences corresponded to decreased ACL-RSI scores in both groups (a 2 point decrease for each mm of increased laxity). These findings reinforce the interconnectedness of ligamentous joint stability, neuromuscular strength, and psychological readiness restoration, suggesting that surgical ACL repair may better support early RTS milestones. Whether or not these gains translate into sustainable mid-to-long term advantages remains to be confirmed.58
Study Limitations
This review has several limitations. With few high-level randomized controlled studies, the overall methodological quality was only fair. Many studies were retrospective increasing bias risk, limiting evidence strength and generalizability. Retrospective designs are particularly prone to recall bias and incomplete data collection, undermining reported outcome reliability. Small sample sizes also limit statistical power, potentially concealing important intervention differences. Publication bias also cannot be excluded, as studies with positive findings are more likely reported than those with neutral or negative results. The heterogeneity in patient age ranges, skeletal immaturity confirmation, surgical techniques, rehabilitation approaches, PROM use, and operational failure and RTS criteria definitions made direct comparisons difficult. Although this review targeted young patients with open physes, several contributing studies included older individuals limiting population-specific generalizability. Additionally, outcomes reporting was inconsistent with many studies relying heavily on PROM use, while others focused more on ACL graft failure rates or athlete RTS rates. Follow-up timing also varied with most studies reporting short or mid-term results. This prevented comprehensive long-term outcome assessment of ACL graft failure rates, lower extremity growth/alignment disturbances, and post-traumatic knee osteoarthritis development. Lastly, the smaller number of conservative brace, or rehabilitation-based therapeutic exercise interventions with a delayed ACLR option studies restricts the strength of conclusions. This, however, reflects the current state of the medical literature, not a definitive lack of value for any of these emerging interventions.
Conclusion
Although ACLR had lower failure rates, neurocognitive, reactive strength, and psychological readiness assessments were underreported.93 The stronger methodological rigor for ACL repair studies was encouraging but long-term outcomes are lacking.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weitz FK, Sillanpää PJ, Mattila VM. The incidence of paediatric ACL injury is increasing in Finland. Knee Surg Sports Traumatol Arthrosc. 2020;28(2):363–368. doi:10.1007/s00167-019-05553-9
2. Herzog MM, Marshall SW, Lund JL, Pate V, Mack CD, Spang JT. Incidence of anterior cruciate ligament reconstruction among adolescent females in the United States, 2002 through 2014. JAMA Pediatr. 2017;171(8):808–810. doi:10.1001/jamapediatrics.2017.0740
3. Kay J, Memon M, Marx RG, Peterson D, Simunovic N, Ayeni OR. Over 90 % of children and adolescents return to sport after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2018;26:1019–10361795. doi:10.1007/s00167-018-4830-9
4. Fones L, Kostyun RO, Cohen AD, Pace JL. Patient-reported outcomes, return-to-sport status, and reinjury rates after anterior cruciate ligament reconstruction in adolescent athletes: minimum 2-year follow-up. Orthop J Sports Med. 2020;8(11). doi:10.1177/2325967120964471
5. Nyland J, Gamble C, Franklin T, Caborn DNM. Permanent knee sensorimotor system changes following ACL injury and surgery. Knee Surg Sports Traumatol Arthrosc. 2017;25(5):1461–1474.
6. Murray MM. Optimizing outcomes of ACL surgery-Is autograft reconstruction the only reasonable option? J Orthop Res. 2021;39(9):1843–1850. PMC8387392.
7. Thoma L, Grindem H, Logerstedt D, et al. Coper classification early after ACL rupture changes with progressive neuromuscular and strength training and is associated with 2-year success: response. Am J Sports Med. 2019;47(11):NP65–NP66.
8. Angthong C, Chumchuen S, Khadsongkram A. Total ankle arthroplasty with ceramic prostheses: a systematic review of medium-term outcomes and failure rates. Hard Tissue. 2013;2(2):15. doi:10.13172/2050-2303-2-2-400
9. Arbes S, Resinger C, Vécsei V, Nau T. The functional outcome of total tears of the anterior cruciate ligament (ACL) in the skeletally immature patient. Int Orthop. 2007;31(4):471–475. doi:10.1007/s00264-006-0225-5
10. Graf BK, Lange RH, Fujisaki CK, Landry GL, Saluja RK. Anterior cruciate ligament tears in skeletally immature patients: meniscal pathology at presentation and after attempted conservative treatment. Arthroscopy. 1992;8(2):229–233. doi:10.1016/0749-8063(92)90041-9
11. Kannus P, Jarvinen M. Knee ligament injuries in adolescents. Eight year follow-up of conservative management. J Bone Joint Surg Br. 1988;70-B(5):772–776. doi:10.1302/0301-620X.70B5.3192578
12. McCarroll JR, Rettig AC, Shelbourne KD. Anterior cruciate ligament injuries in the young athlete with open physes. Am J Sports Med. 1988;16(1):44–47. doi:10.1177/036354658801600107
13. Mizuta H, Kubota K, Shiraishi M, Otsuka Y, Nagamoto N, Takagi K.The conservative treatment of complete tears of the anterior cruciate ligament in skeletally immature patients. J Bone Joint Surg Br. 1995;77(6):890–894.
14. Moore A, Rames J, McGurk K, Slone H. ACL repair of femoral osseous avulsion in a 13-year-old using suture pullout technique. Video J Sports Med. 2021;1(5):26350254211030289. doi:10.1177/26350254211030289
15. Pressman AE, Letts RM, Jarvis JG.Anterior cruciate ligament tears in children: an analysis of operative versus nonoperative treatment. J Pediatr Orthop. 1997;17(4):505–511.
16. Turati M, Benedettini E, Sugimoto D, et al. Quadriceps and hamstring muscles strength differences in adolescent and adult recreational athletes 6 months after autograft bone-patellar-tendon-bone anterior cruciate ligament reconstruction: a retrospective study. Knee. 2025;54:9–18.
17. Gebhard F, Ellermann A, Hoffmann F, Jaeger JH, Friederich NF. Multicenter-study of operative treatment of intraligamentous tears of the anterior cruciate ligament in children and adolescents: comparison of four different techniques. Knee Surg Sports Traumatol Arthrosc. 2006;14(9):797–803. doi:10.1007/s00167-006-0055-4
18. Andrews M, Noyes FR, Barber-Westin SD. Anterior cruciate ligament allograft reconstruction in the skeletally immature athlete. Am J Sports Med. 1994;22(1):48–54. doi:10.1177/036354659402200109
19. Aronowitz ER, Ganley TJ, Goode JR, Gregg JR, Meyer JS. Anterior cruciate ligament reconstruction in adolescents with open physes. Am J Sports Med. 2000;28(2):168–175. doi:10.1177/03635465000280020601
20. Bigoni M, Gaddi D, Gorla M, et al. Arthroscopic anterior cruciate ligament repair for proximal anterior cruciate ligament tears in skeletally immature patients: surgical technique and preliminary results. Knee. 2017;24(1):40–48. doi:10.1016/j.knee.2016.09.017
21. Calvo R, Figueroa D, Gili F, et al. Transphyseal anterior cruciate ligament reconstruction in patients with open physes: 10-year follow-up study. Am J Sports Med. 2015;43(2):289–294. doi:10.1177/0363546514557939
22. Cassard X, Cavaignac E, Maubisson L, Bowen M. Anterior cruciate ligament reconstruction in children with a quadrupled semitendinosus graft: preliminary results with minimum 2 years of follow-up. J Pediatr Orthop. 2014;34(1):70–77. doi:10.1097/BPO.0b013e3182a008b6
23. Cohen M, Ferretti M, Quarteiro M, et al. Transphyseal anterior cruciate ligament reconstruction in patients with open physes. Arthroscopy. 2009;25(8):831–838. doi:10.1016/j.arthro.2009.01.015
24. Dabis J, Yasen SK, Foster AJ, Pace JL, Wilson AJ. Paediatric proximal ACL tears managed with direct ACL repair is safe, effective and has excellent short-term outcomes. Knee Surg Sports Traumatol Arthrosc. 2020;28(8):2551–2556. doi:10.1007/s00167-020-05872-2
25. Demange MK, Camanho GL. Nonanatomic anterior cruciate ligament reconstruction with double-stranded semitendinosus grafts in children with open physes: minimum 15-year follow-up. Am J Sports Med. 2014;42(12):2926–2932. doi:10.1177/0363546514550981
26. Ekås GR, Moksnes H, Grindem H, Risberg MA, Engebretsen L. Coping with anterior cruciate ligament injury from childhood to maturation: a prospective case series of 44 patients with mean 8 years’ follow-up. Am J Sports Med. 2019;47(1):22–30. doi:10.1177/0363546518810750
27. Ellis HB, Matheny LM, Briggs KK, Pennock AT, Steadman JR. Outcomes and revision rate after bone-patellar tendon-bone allograft versus autograft anterior cruciate ligament reconstruction in patients aged 18 years or younger with closed physes. Arthroscopy. 2012;28(12):1819–1825. doi:10.1016/j.arthro.2012.06.016
28. Engebretsen L, Svenningsen S, Benum P. Poor results of anterior cruciate ligament repair in adolescence. Acta Orthop Scand. 1988;59(6):684–686. doi:10.3109/17453678809149425
29. Falciglia F, Panni AS, Giordano M, Aulisa AG, Guzzanti V. Anterior cruciate ligament reconstruction in adolescents (Tanner stages 2 and 3). Knee Surg Sports Traumatol Arthrosc. 2016;24(3):807–814. doi:10.1007/s00167-016-4034-0
30. Filbay SR, Dowsett M, Chaker Jomaa M, et al. Healing of acute anterior cruciate ligament rupture on MRI and outcomes following non-surgical management with the cross bracing protocol. Br J Sports Med. 2023;57(23):1490–1497.
31. Fleming BC, Baranker B, Badger GJ, et al. Bridge-enhanced anterior cruciate ligament restoration: 6-year results from the first-in-human cohort study. Orthop J Sports Med. 2024;12(8):23259671241260632.
32. Fuchs R, Wheatley W, Uribe JW, Hechtman KS, Zvijac JE, Schurhoff MR. Intra-articular anterior cruciate ligament reconstruction using patellar tendon allograft in the skeletally immature patient. Arthroscopy. 2002;18(8):824–828. doi:10.1053/jars.2002.36136
33. Gagliardi AG, Carry PM, Parikh HB, Traver JL, Howell DR, Albright JC. ACL repair with suture ligament augmentation is associated with a high failure rate among adolescent patients. Am J Sports Med. 2019;47(3):560–566. doi:10.1177/0363546518825255
34. Gaulrapp HM, Haus J. Intraarticular stabilization after anterior cruciate ligament tear in children and adolescents: results 6 years after surgery. Knee Surg Sports Traumatol Arthrosc. 2006;14(5):417–424.
35. Goddard M, Bowman N, Salmon LJ, Waller A, Roe JP, Pinczewski LA. Endoscopic anterior cruciate ligament reconstruction in children using living donor hamstring tendon allografts. Am J Sports Med. 2013;41(3):567–574. doi:10.1177/0363546512473576
36. Grassi A, Pizza N, Macchiarola L, et al. Over-the-top Anterior Cruciate Ligament (ACL) reconstruction plus lateral plasty with hamstrings in high-school athletes: results at 10 years. Knee. 2021;33:226–233.
37. Guzzanti V, Falciglia F, Stanitski CL. Physeal-sparing intraarticular anterior cruciate ligament reconstruction in preadolescents. Am. J Sports Med. 2003;31(6):949–953. doi:10.1177/0363546503031006340
38. Henry J, Chotel F, Chouteau J, Fessy MH, Bérard J, Moyen B. Rupture of the anterior cruciate ligament in children: early reconstruction with open physes or delayed reconstruction to skeletal maturity? Knee. Surg Sports Traumatol Arthrosc. 2009;17(7):748–755. doi:10.1007/s00167-009-0741-0
39. Hui C, Roe J, Ferguson D, Waller A, Salmon L, Pinczewski L. Outcome of anatomic transphyseal anterior cruciate ligament reconstruction in Tanner stage 1 and 2 patients with open physes. Am J Sports Med. 2012;40(5):1093–1098. doi:10.1177/036354651243850
40. Kew ME, Bodkin S, Diduch DR, et al. Reinjury rates in adolescent patients 2 years following ACL reconstruction. J Pediatr Orthop. 2022;42(2):90–95. doi:10.1097/BPO.0000000000002031
41. Kilkenny CJ, Hurley ET, Hogan RE, et al. Return to play in paediatric & adolescent patients following anterior cruciate ligament reconstruction. Knee. 2022;37:87–94. doi:10.1016/j.knee.2022.05.013
42. Al Kindi I, Al Rawahi S, Al Ghaithi A, Al Yarubi S, Al Masakri S, Al Mutaini M. Primary ACL repair in a selected patient cohort: a prospective single cohort study. J Orthop. 2024;61:127–132. doi:10.1016/j.jor.2024.09.020
43. Kocher MS, Heyworth BE, Fabricant PD, Tepolt FA, Micheli LJ. Outcomes of physeal-sparing ACL reconstruction with iliotibial band autograft in skeletally immature prepubescent children. J Bone Joint Surg Am. 2018;100(13):1087–1094. doi:10.2106/JBJS.17.01327
44. Kocher MS, Smith JT, Zoric BJ, Lee B, Micheli LJ. Transphyseal anterior cruciate ligament reconstruction in skeletally immature pubescent adolescents. J Bone Joint Surg Am. 2007;89(12):2632–2639. doi:10.2106/JBJS.F.01560
45. Lanzetti RM, Pace V, Ciompi A, et al. Over the top anterior cruciate ligament reconstruction in patients with open physes: a long-term follow-up study. Int Orthop. 2020;44(4):771–778. doi:10.1007/s00264-020-04490-4
46. Lo IK, Kirkley A, Fowler PJ, Miniaci A. The outcome of operatively treated anterior cruciate ligament disruptions in the skeletally immature child. Arthroscopy. 1997;13(5):627–634. doi:10.1016/s0749-8063(97)90191-2
47. Madelaine A, Fournier G, Sappey-Marinier E, et al. French arthroscopic society. Conservative management of anterior cruciate ligament injury in paediatric population: about 53 patients. Orthop Traumatol Surg Res. 2018;104(8S):S169–S173. doi:10.1016/j.otsr.2018.09.001
48. McCarroll JR, Shelbourne KD, Porter DA, Rettig AC, Murray S. Patellar tendon graft reconstruction for midsubstance anterior cruciate ligament rupture in junior high school athletes. Am J Sports Med. 1994;22(4):478–484. doi:10.1177/036354659402200407
49. McIntosh AL, Dahm DL, Stuart MJ. Anterior cruciate ligament reconstruction in the skeletally immature patient. Arthroscopy. 2006;22(12):1325–1330. doi:10.1016/j.arthro.2006.07.014
50. Micheli LJ, Rask B, Gerberg L. Anterior cruciate ligament reconstruction in patients who are prepubescent. Clin Orthop Relat Res. 1999;364:40–47. doi:10.1097/00003086-199907000-00006
51. Moksnes H, Engebretsen L, Eitzen I, Risberg MA. Functional outcomes following a non-operative treatment algorithm for anterior cruciate ligament injuries in skeletally immature children 12 years and younger. A prospective cohort with 2 years follow-up. Br J Sports Med. 2013;47(8):488–494.
52. Murray MM, Kalish LA, Fleming BC, et al; BEAR Trial Team. Bridge-enhanced anterior cruciate ligament repair: two-year results of a first-in-human study. Orthop J Sports Med. 2019;7(3):2325967118824356. doi:10.1177/2325967118824356.
53. BEAR Trial Team, Murray MM, Fleming BC, Badger GJ, et al. Bridge-enhanced anterior cruciate ligament repair is not inferior to autograft anterior cruciate ligament reconstruction at 2 years: results of a prospective randomized clinical trial. Am J Sports Med. 2020;48(6):1305–1315.
54. Parker AW, Drez D, Cooper JL. Anterior cruciate ligament injuries in patients with open physes. Am J Sports Med. 1994;22(1):44–47. doi:10.1177/036354659402200108
55. Pennock AT, Johnson KP, Turk RD, et al. Transphyseal anterior cruciate ligament reconstruction in the skeletally immature: quadriceps tendon autograft versus hamstring tendon autograft. Orthop J Sports Med. 2019;7(9):2325967119872450. doi:10.1177/2325967119872450
56. Redler LH, Brafman RT, Trentacosta N, Ahmad CS. Anterior cruciate ligament reconstruction in skeletally immature patients with transphyseal tunnels. Arthroscopy. 2012;28(11):1710–1717. doi:10.1016/j.arthro.2012.04.145
57. Robert H, Bonnard C. The possibilities of using the patellar tendon in the treatment of anterior cruciate ligament tears in children. Arthroscopy. 1999;15(1):73–76.
58. Sanborn RM, Badger GJ, Yen YM, et al. Psychological readiness to return to sport at 6 months is higher after bridge-enhanced ACL restoration than autograft ACL reconstruction: results of a prospective randomized clinical trial. Orthop J Sports Med. 2022;10(2):23259671211070542. doi:10.1177/23259671211070542
59. Seon JK, Song EK, Yoon TR, Park SJ. Transphyseal reconstruction of the anterior cruciate ligament using hamstring autograft in skeletally immature adolescents. J Korean Med Sci. 2005;20(6):1034–1038. doi:10.3346/jkms.2005.20.6.1034
60. Shelbourne KD, Gray T, Wiley BV. Results of transphyseal anterior cruciate ligament reconstruction using patellar tendon autograft in tanner stage 3 or 4 adolescents with clearly open growth plates. Am J Sports Med. 2004;32(5):1218–1222. doi:10.1177/0363546503262169
61. Shelbourne KD, Sullivan AN, Bohard K, Gray T, Urch SE. Return to basketball and soccer after anterior cruciate ligament reconstruction in competitive school-aged athletes. Sports Health. 2009;1(3):236–241. doi:10.1177/1941738109334275
62. Steadman JR, Cameron-Donaldson ML, Briggs KK, Rodkey WG. A minimally invasive technique (“healing response”) to treat proximal ACL injuries in skeletally immature athletes. J Knee Surg. 2006;19(1):8–13. doi:10.1055/s-0030-1248070
63. Streich NA, Barié A, Gotterbarm T, Keil M, Schmitt H. Transphyseal reconstruction of the anterior cruciate ligament in prepubescent athletes. Knee Surg Sports Traumatol Arthrosc. 2010;18(11):1481–1486. doi:10.1007/s00167-010-1057-9
64. Turati M, Rigamonti L, Zanchi N, et al. An arthroscopic repair technique for proximal anterior cruciate tears in children to restore active function and avoid growth disturbances. Knee Surg Sports Traumatol Arthrosc. 2021;29(11):3689–3696. doi:10.1007/s00167-020-06367-w
65. Vermeijden HD, Yang XA, van der List JP, DiFelice GS. Role of age on success of arthroscopic primary repair of proximal anterior cruciate ligament tears. Arthroscopy. 2021;37(4):1194–1201. doi:10.1016/j.arthro.2020.11.024
66. Webster KE, Feller JA, Leigh WB, Richmond AK. Younger patients are at increased risk for graft rupture and contralateral injury after anterior cruciate ligament reconstruction. Am J Sports Med. 2014;42(3):641–647. doi:10.1177/0363546513517540
67. Webster KE, Feller JA. Exploring the high reinjury rate in younger patients undergoing anterior cruciate ligament reconstruction. Am J Sports Med. 2016;44(11):2827–2832. doi:10.1177/0363546516651845
68. Anderson AF, Anderson CN. Correlation of meniscal and articular cartilage injuries in children and adolescents with timing of anterior cruciate ligament reconstruction. Am J Sports Med. 2015;43(2):275–281. doi:10.1177/0363546514559912
69. Cordasco FA, Black SR, Price M, et al. Return to sport and reoperation rates in patients under the age of 20 after primary anterior cruciate ligament reconstruction: risk profile comparing 3 patient groups predicated upon skeletal age. Am J Sports Med. 2019;47(3):628–639. doi:10.1177/0363546518819217
70. Cordasco FA, Hidalgo Perea S, Uppstrom TJ, et al. Quadriceps tendon anterior cruciate ligament reconstruction in skeletally immature patients: 3-year clinical and patient-reported outcomes. Am J Sports Med. 2024;52(9):2230–2236. doi:10.1177/03635465241255641
71. Dai B, Butler RJ, Garrett WE, Queen RM. Anterior cruciate ligament reconstruction in adolescent patients: limb asymmetry and functional knee bracing. Am J Sports Med. 2012;40(12):2756–2763. doi:10.1177/0363546512460837
72. DeFrancesco CJ, Striano BM, Bram JT, Baldwin KD, Ganley TJ. An in-depth analysis of graft rupture and contralateral anterior cruciate ligament rupture rates after pediatric anterior cruciate ligament reconstruction. Am J Sports Med. 2020;48(10):2395–2400. doi:10.1177/0363546520935437
73. Gagliardi AG, Carry PM, Parikh HB, Albright JC. Outcomes of quadriceps tendon with patellar bone block anterior cruciate ligament reconstruction in adolescent patients with a minimum 2-year follow-up. Am J Sports Med. 2020;48(1):93–98. doi:10.1177/0363546519885371
74. Guzzanti V, Falciglia F, Stanitski CL. Preoperative evaluation and anterior cruciate ligament reconstruction technique for skeletally immature patients in Tanner stages 2 and 3. Am J Sports Med. 2003;31(6):941–948. doi:10.1177/03635465030310063301
75. Larson CM, Heikes CS, Ellingson CI, et al. Allograft and autograft transphyseal anterior cruciate ligament reconstruction in skeletally immature patients: outcomes and complications. Arthroscopy. 2016;32(5):860–867. doi:10.1016/j.arthro.2015.10.014
76. Månsson O, Sernert N, Rostgard-Christensen L, Kartus J. Long-term clinical and radiographic results after delayed anterior cruciate ligament reconstruction in adolescents. Am J Sports Med. 2015;43(1):138–145. doi:10.1177/0363546514555673
77. Morgan MD, Salmon LJ, Waller A, Roe JP, Pinczewski LA. Fifteen-year survival of endoscopic anterior cruciate ligament reconstruction in patients aged 18 years and younger. Am J Sports Med. 2016;44(2):384–392. doi:10.1177/0363546515623032
78. Moussa MK, Lefèvre N, Valentin E, et al. Impact of lateral extra-articular procedure augmentation on rerupture risk and tegner activity scale outcomes in adolescent anterior cruciate ligament: a matched comparative study with a minimum 2-year follow-up. Am J Sports Med. 2024;52(4):892–901. doi:10.1177/03635465231223703
79. Thorolfsson B, Winkler PW, Piussi R, et al. The chance to become an elite athlete after pediatric and adolescent anterior cruciate ligament reconstruction. Am J Sports Med. 2025;53(5):1027–1033. doi:10.1177/03635465251320415
80. Zwolski C, Schmitt LC, Quatman-Yates C, Thomas S, Hewett TE, Paterno MV. The influence of quadriceps strength asymmetry on patient-reported function at time of return to sport after anterior cruciate ligament reconstruction. Am J Sports Med. 2015;43(9):2242–2249. doi:10.1177/0363546515591258
81. Magnussen RA, Binzel K, Zhang J, et al. ACL graft metabolic activity assessed by 18FDG PET-MRI. Knee. 2017;24(4):792–797. doi:10.1016/j.knee.2017.04.008
82. Kiapour AM, Flannery SW, Murray MM, et al. Regional differences in anterior cruciate ligament signal intensity after surgical treatment. Am J Sports Med. 2021;49(14):3833–3841. doi:10.1177/03635465211047554
83. Zdanowicz U, Ciszkowska-łysoń B, Paśnik M, et al. Evaluation of ACL graft remodeling and prediction of graft insufficiency in sequenced MRI—two-year follow-up. Appl Sci. 2021;11(11):5278. doi:10.3390/app11115278
84. Marturano JE, Xylas JF, Sridharan GV, Georgakoudi I, Kuo CK. Lysyl oxidase-mediated collagen crosslinks may be assessed as markers of the functional properties of tendon tissue formation. Acta Biomater. 2014;10(3):1370–1379. doi:10.1016/j.actbio.2013.11.024
85. Webster KE, Feller JA. Development and validation of a short version of the anterior cruciate ligament return to sport after injury (ACL-RSI) Scale. Orthop J Sports Med. 2018;6(4):2325967118763763. doi:10.1177/2325967118763763
86. American Academy of Orthopaedic Surgeons management of anterior cruciate ligament injuries evidence-based clinical practice guideline. Available from: www.aaos.org/aclcpg.
87. Grooms DR, Chaput M, Simon JE, Criss CR, Myer GD, Diekfuss JA. Combining neurocognitive and functional tests to improve return-to-sport decisions following ACL reconstruction. J Orthop Sports Phys Ther. 2023;53(8):415–419. doi:10.2519/jospt.2023.11489
88. Chmielewski T, Obermeier M, Meierbachtol A, et al. Advanced neuromuscular training differentially changes performance on visuomotor reaction tests and single-leg hop tests in patients with ACL reconstruction. Int J Sports Phys Ther. 2024;19(11):1324–1332. doi:10.26603/001c.124807
89. Angelozzi M, Madama M, Corsica C, et al. Rate of force development as an adjunctive outcome measure for return-to-sport decisions after anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 2012;42(9):772–780. doi:10.2519/jospt.2012.3780
90. Getgood AMJ, Bryant DM, Litchfield R, et al. Lateral extra-articular tenodesis reduces failure of hamstring tendon autograft anterior cruciate ligament reconstruction: 2-year outcomes from the STABILITY study randomized clinical trial. Am J Sports Med. 2020;48(2):285–297. doi:10.1177/0363546519896333
91. Le Guen A, Bérard E, Ben-Roummane H, et al. Clinical SANTI classification of arthrogenic muscle inhibition has an excellent inter-rater and intra-rater reliability in preoperative and post-operative anterior cruciate ligament rupture. Knee Surg Sports Traumatol Arthrosc. 2025;33(7):2397–2404. doi:10.1002/ksa.12586
92. Sadeqi M, Klouche S, Bohu Y, Herman S, Lefevre N, Gerometta A. Progression of the psychological ACL-RSI score and return to sport after anterior cruciate ligament reconstruction: a prospective 2-year follow-up study from the French prospective anterior cruciate ligament reconstruction cohort study (FAST). Orthop J Sports Med. 2018;6(12):2325967118812819. doi:10.1177/2325967118812819
93. Farrey T. Let’s start treating knee injuries like brain injuries. Time. Available from: https://time.com/6294837/knee-injuries-acl-soccer-world-cup/.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Recurrent Hepatocellular Carcinoma: Patterns, Detection, Staging and Treatment
Papaconstantinou D, Tsilimigras DI, Pawlik TM
Journal of Hepatocellular Carcinoma 2022, 9:947-957
Published Date: 3 September 2022
Breast Cancer Management in the Era of Covid-19; Key Issues, Contemporary Strategies, and Future Implications
Prodhan ASU, Islam DZ, Khandker SS, Jamiruddin MR, Abdullah A, Godman B, Opanga S, Kumar S, Sharma P, Adnan N, Pisana A, Haque M
Breast Cancer: Targets and Therapy 2023, 15:51-89
Published Date: 27 January 2023
Survival in Lung Cancer in the Nordic Countries Through A Half Century
Tichanek F, Försti A, Hemminki O, Hemminki A, Hemminki K
Clinical Epidemiology 2023, 15:503-510
Published Date: 1 May 2023
Refractory Folliculitis Decalvans Treatment Success with a Novel Surgical Excision Approach Using Guarded High-Tension Sutures
Umar S, Waterman A, Ton D, Shitabata P
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2381-2390
Published Date: 1 September 2023
Management Strategies for Pediatric Moderate-to-Severe Plaque Psoriasis: Spotlight on Biologics
Ruggiero A, Portarapillo A, Megna M, Patruno C, Napolitano M
Pediatric Health, Medicine and Therapeutics 2023, 14:435-451
Published Date: 14 November 2023