")
Back to Journals » International Journal of Women's Health » Volume 16
Current Situation and Mental Health of Pregnant Women During the Prevention and Control of Novel Coronavirus Infection: A Cross-Sectional Study on the Investigation of Influencing Factors
Authors Zhao J , Li Y, Guo M, Zhang G, Chen P
Received 19 October 2023
Accepted for publication 22 January 2024
Published 2 February 2024 Volume 2024:16 Pages 193—202
DOI https://doi.org/10.2147/IJWH.S445473
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Jing Zhao,1 Yan Li,1 Miao Guo,1 Guijuan Zhang,2 Ping Chen1
1Department of Gynaecology and Obstetrics, the First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China; 2Department of Gynaecology and Obstetrics, the Second Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China
Correspondence: Ping Chen, Department of Gynaecology and Obstetrics, the First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China, Tel +8613783589566, Fax +86037166262974, Email [email protected]
Background: COVID-19 is a highly contagious respiratory infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which became a global public health crisis. In the past 3 years, the COVID-19 pandemic has resulted in a dramatic increase in the occurrence of psychological symptoms such as depression, anxiety, and stress in global populations. Therefore, it is important to help pregnant women cope with major public emergencies and improve their physical and mental health.
Objective: To investigate the status and influencing factors of anxiety, insomnia, and psychological stress disorder in pregnant women with COVID-19 to provide a theoretical basis for psychological intervention in pregnant women in the case of public health emergency events.
Patients and methods: A cross-sectional survey was conducted with 435 pregnant women from multiple tertiary hospitals in Zhengzhou from November 6 to December 6, 2022. The questionnaire contents included the general information of pregnant women, insomnia scale, generalized anxiety scale, and the revised version of the Accident Impact Scale.
Results: There are 251 pregnant women with anxiety (57.7%, 95% CI: (53.0%-62.4%).There are 166 pregnant women with insomnia.(38.2%, 95% CI: 33.6%-42.7%), There are 314 pregnant women with stress disorder.(72.2%, 95% CI: 68.0%– 76.4%). During the epidemic prevention and control period, whether pregnant women had a history of adverse pregnancy had a statistically significant difference in anxiety, insomnia and stress disorders.
Conclusion and Recommendation: During the COVID-19 pandemic, pregnant women appeared to generally have anxiety, insomnia, and stress disorders. Poor pregnancy history is a protective factor for pregnant women with anxiety, insomnia, and post-traumatic stress disorder. In the case of similar public health emergencies, attention bias modification (ABM) may be a potential intervention measure to provide potentially new ideas for alleviating the psychological disorders of pregnant women during this special period.
Keywords: novel coronavirus infection, pregnancy, anxiety, insomnia, psychological stress disorder
Introduction
With the transformation of the biopsychosocial medical model, mental health of pregnant women has become a significant focus of interest in recent years. As we all know, COVID-19 is a highly contagious respiratory infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which became a global public health crisis. Since the start of the COVID-19 pandemic in December 2019 people have become increasingly prone to physical and psychological dysfunction, anxiety, and depression.1 However, pregnant women, as a special group, have special requirements given the demanding physiological process of pregnancy and childbirth, while experiencing great changes in social roles and living environment, and are hence more prone to psychological disorders such as anxiety, insomnia, and stress-related disorders. Psychological disorders of pregnant women not only harm the mother’s mental health but also have long-term adverse effects on the infant’s future development, cognition, behavior, and emotion and on the family.2 Therefore, it is important to help pregnant women cope with major public emergencies and improve their physical and mental health. Over the past three years, previous studies suggests that the COVID-19 pandemic has led to a dramatic increase in the incidence of psychological symptoms such as depression, anxiety and stress among populations worldwide. Moreover, the detection rate of anxiety and depression in China was significantly higher than that of the national epidemiological survey before the epidemic.3 However, at the beginning of the epidemic in 2019, in China, some studies investigated the current state of pregnant women’s mental state and its status Influencing factors. Among them, Jin Ying’s research is representative.4 November 2022 is a special period when COVID-19 once again broke out in the population, and there is almost no investigation on the psychological state of pregnant women in China, and this study filled the gap in this period.Thus, the objective of this study was to analyze this psychological impact on pregnant women and the factors that may influence these effects. Specifically, the objective was to investigate the status and influencing factors of anxiety, insomnia, and psychological stress disorder in pregnant women with COVID-19 to provide a theoretical basis for psychological intervention in pregnant women in the case of public health emergency events.
Methods
Study Design, Setting, and Period
A cross-sectional study of anxiety, insomnia, and psychological stress disorders among pregnant women during the COVID-19 pandemic in Zhengzhou, Henan Province, China, was conducted.
Study Population: A random sample of 20% of pregnant women who had visited the First Affiliated Hospital of Henan University of Chinese Medicine, the Second Affiliated Hospital of Zhengzhou University, the Third Affiliated Hospital of Zhengzhou University, Zhengzhou Central Hospital and Zhengzhou Maternal and Child Health Hospital were surveyed online from November 6 to December 6, 2022.
Inclusion Criteria: (i) Age ≥ 18 years; (ii) Non-use of drugs that affect sleep and mental state; (iii) Normal intelligence, and subjects’ physical condition allowed them to cooperate with the completion of the investigation; and (iv) Voluntary participation in the study.
Exclusion criteria: (i) History of mental illness or mental disorders; (ii) pregnant patients’ decision to terminate the pregnancy for any reason; (iii) serious communication barriers (eg, reading and writing and audiovisual barriers) and/or inability to correctly understand or respond to the questionnaire.
Data Collection Method and Instrument
Data are collected online through the Questionnaire Star platform. The first part of all questionnaires has unified guidance and corresponding professional explanations, which are filled in anonymously by the respondents themselves. If in doubt, they can consult the professional investigators online.
The questions included: socio-demographic characteristics, and the 7-Items Generalized Anxiety Disorder Scale (GAD-7) (7 questions),5,6 insomnia severity index (ISI) (7 questions),7 and the Impact of Event Scale-Revised (IESR) (22 questions).8
Socio-Demographic Characteristics
General data mainly comprised three parts: (1) demographic sociological information such as age, education, working status, and average monthly family income; (2) Pregnancy history such as pregnancy stage, number of deliveries, adverse pregnancy history, and pregnancy complications; (3) Details related to COVID-19, such as the source of knowledge about the novel coronavirus, whether it has reappeared in the affected area, and the current prevention and control status of pregnant women. The current prevention and control status of pregnant women is divided into low risk, medium risk, high risk and very high risk according to the number of COVID-19 cases in their current region.
Operational Definitions
Generalized Anxiety Scale-7 items: The GAD-7 is a self-administered 7-item questionnaire for measuring general anxiety. Each item is scored on a 3-point Likert scale (0 = not at all to 3 = nearly every day). Scores can range from 0 to 21, with higher scores reflecting higher levels of anxiety. Cut-off intervals for anxiety include 0–4 (no anxiety), 5–9 (mild anxiety), 10–15 (moderate), and 16–21 (severe). The excellent internal consistency (Cronbach’s α = 0.92) and good test-retest reliability (intraclass correlation = 0.83) were reported.5–7
The Insomnia Severity Index (ISI) is a brief 7-item tool designed to assess the perceived severity of insomnia symptoms over the past 2 weeks. A five-point Likert scale is used to rate each item, yielding a total score ranging from 0 to 28. Higher scores indicate more severe sleep difficulties. A score of 0 to 7 indicates insomnia without significant clinical manifestations; 8–14 is classified as mild insomnia; 15–21 denotes moderate insomnia; and ≥22 denoted severe insomnia. The Cronbach’s-α coefficient of this scale is 0.843, and the retest reliability is 0.506, which has good validity and reliability, and can be used as a screening tool for insomnia.8,9
The IES-Revised (IES-R) is a 22-item self-reported questionnaire designed to assess symptoms of intrusive thoughts (8 items), avoidance (8 items), and hyperarousal (6 items) resulting from traumatic life events. The scale measures the severity with which each of the symptoms had occurred over the past 2 weeks; each item is rated on a 5-point scale using anchors between 0 (not at all) and 4 (extremely), and total scores range from 0 to 88. The cut-off intervals for indicates include 0–8 (no impact), 9–25 (mild impact), 26–43 (moderate), and 44–88 (severe). The Cronbach’s-α coefficient ranged from 0.76 to 0.89.10,11
Statistical Analysis
All the data was checked and then it was coded and entered into excel table, and it was finally exported to Statistical Package for Social Sciences (SPSS) version 25 for analysis. Frequencies, percentages, summary statistics like mean and standard deviation were examined to describe the data. Then, independent samples t-test or ANOVA were used for univariate analysis. Multifactor stepwise linear regression analysis was used. Finally level at P-value <0.05 was considered to indicate statistically significant differences.
Results
Data Recovery
In all, 458 pregnant women were randomly selected and questionnaires were distributed through an online platform. Of 458 questionnaires distributed, 435were valid, with an effective recovery rate 94.98%.
Demographic Characteristics
Overall, 167 (38.4%) pregnant women were aged <30 years, 197 (45.3%) pregnant women were aged between 30 and 34 years, and 71 (16.3%) pregnant women were aged > 35 years. Thirty (6.9%) pregnant women were educated with up to junior high school level or below, 53 (12.2%) had attained senior high school and technical secondary school education, 95 (21.8%) attained junior college education, and 257 (59.1%) held a bachelor’s degree or higher. Of all pregnant women, 101 (23.2%) did not work, 249 (57.2%) were currently employed, and 85 (19.5%) had been working during pregnancy. The average income of pregnant women was less than 4000 Chinese Yuan (CNY) in 69 (15.9%) patients, between 4000 and 8000 CNY in 196 (45.1%), between 8000 and 12,000 CNY in 107 (24.6%), and > 12,000 CNY in 63 (14.5%). Of all the pregnant women surveyed, 59 (13.6%) were in early pregnancy (≤12 weeks), 195 (44.8%) in middle pregnancy (12–28 weeks), and 181 (41.6%) in late pregnancy (≥28 weeks) (Table 1).
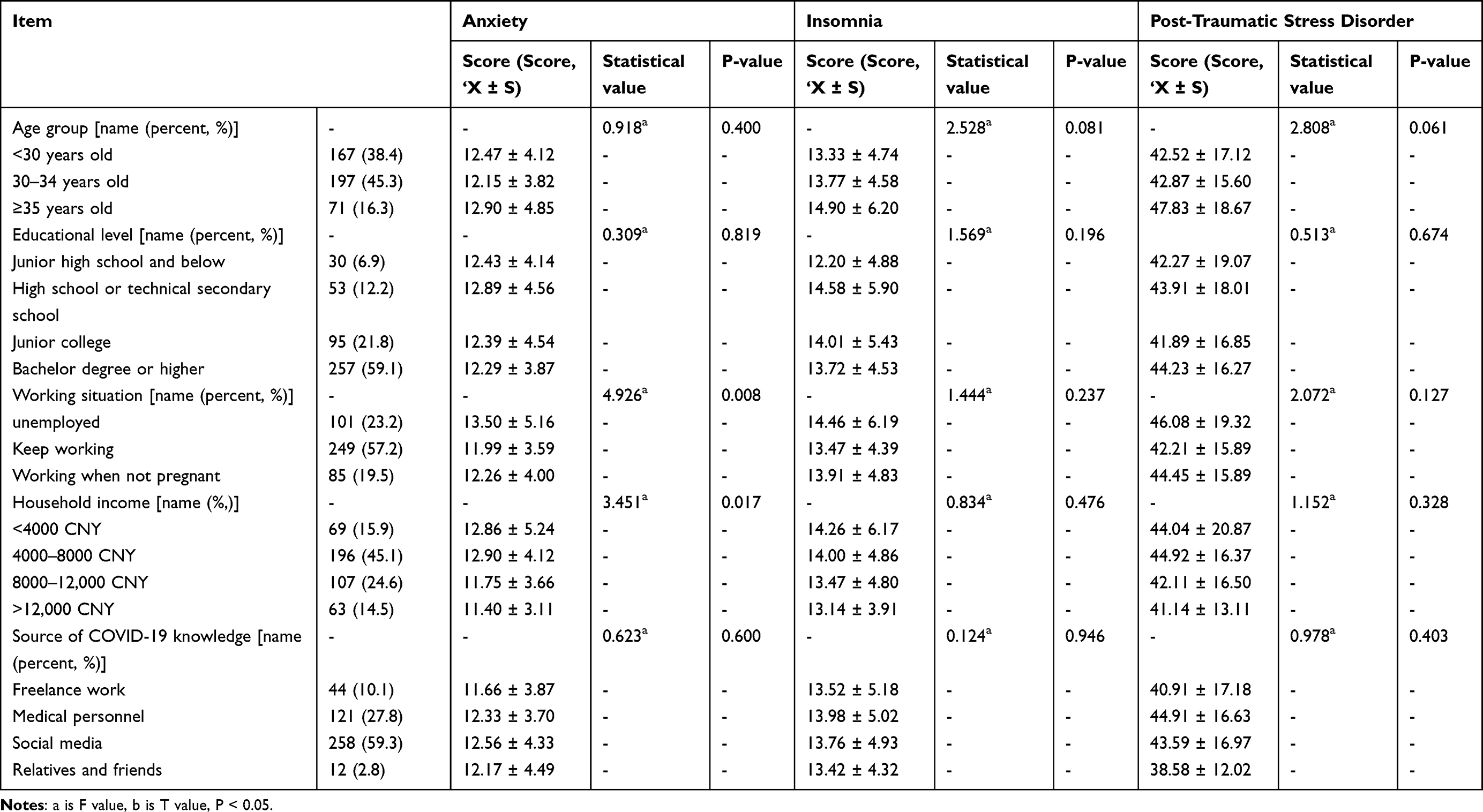 |
Table 1 Univariate Analysis of Anxiety, Insomnia, and Stress Disorder in Pregnant Women (n = 435) |
Pregnant Women Have Widespread Anxiety, Insomnia and Stress Disorder with COVID-19
The detection rates of anxiety, insomnia, and stress disorder were 57.7%, 38.2%, and 72.2%, respectively. The mean ± standard deviation of GAD-7 scores was 5.39 ± 4.12, and the overall level was close to mild anxiety. Furthermore, 251 (57.7%) patients had anxiety, of which 206 (47.4%) had mild anxiety, 29 (6.7%) had moderate anxiety, and 16 (3.7%) had severe anxiety. The mean ± standard deviation of ISI scores was 6.79 ± 4.95, and 166 (38.2%) had insomnia, among which 129 (29.7%) had mild insomnia, 31 (7.1%) had moderate insomnia, and 6 (1.4%) had severe insomnia. The mean ± standard deviation of IES-R score was 21.54 ± 16.79, and 314 (72.2%) women had stress disorder, among which 155 (35.6%) had mild disorder, 109 (25.1%) had moderate disorder, and 50 (11.5%) had severe disorder.
Single Factor Analysis of Anxiety, Insomnia, and Stress Disorder in Pregnant Women
The results of single factor analysis showed that adverse pregnancy history, pregnancy complications, whether the contacts returned from the epidemic area, current prevention and control status of pregnant women, work situation during pregnancy, and family income were influencing factors of pregnant women’s anxiety (P < 0.05). Pregnancy stage, delivery history, adverse pregnancy history, pregnancy complications, whether the contacts returned from the epidemic area, and current prevention and control status of pregnant women were the influencing factors for insomnia in pregnant women (P < 0.05). Adverse pregnancy history and pregnancy complications were the influencing factors of post-traumatic stress disorder (P < 0.05). Detailed data are presented in Tables 1 and 2.
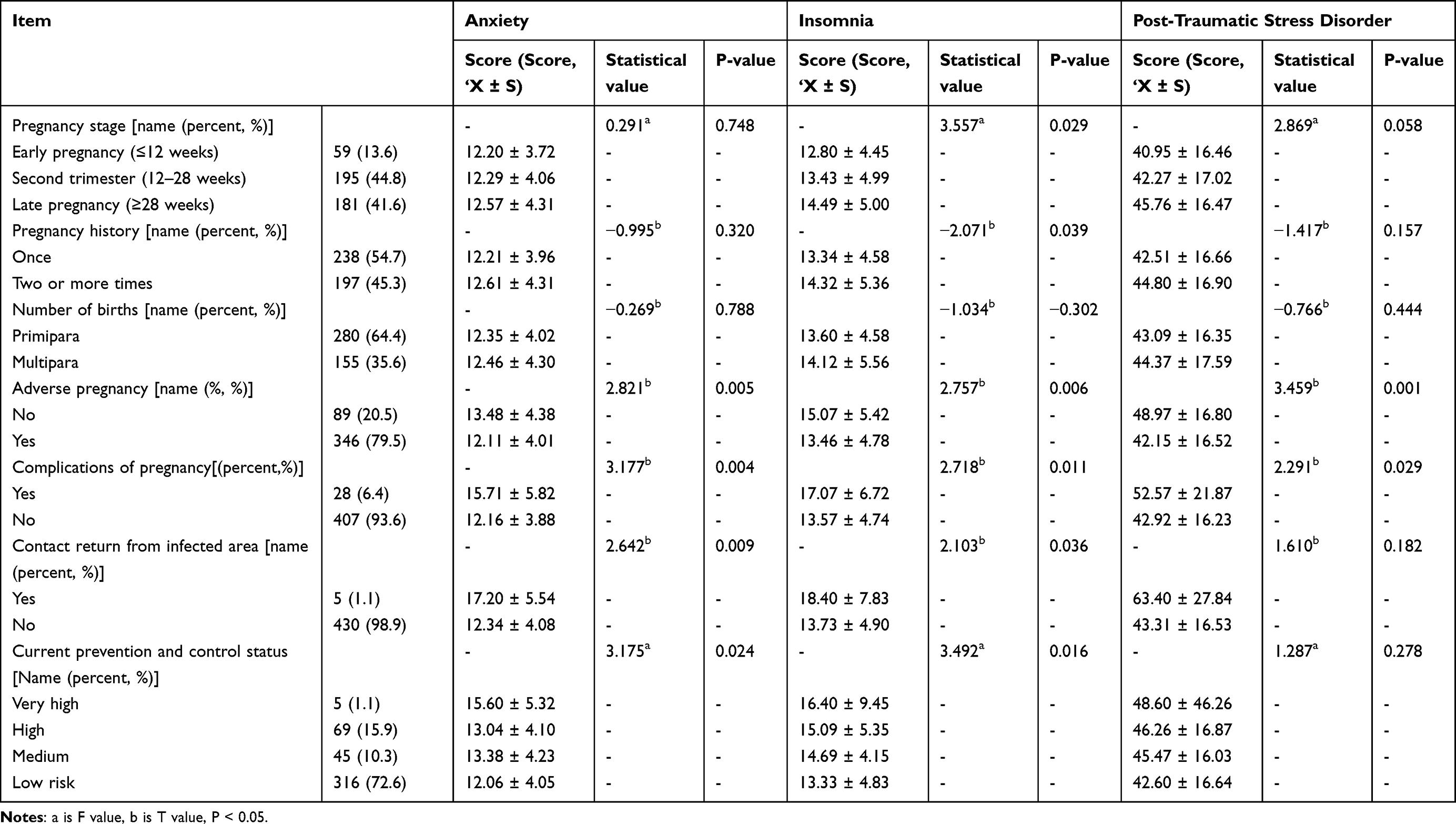 |
Table 2 Univariate Analysis of Anxiety, Insomnia, and Stress Disorder in Pregnant Women (n = 435) |
Multi-Factor Analysis of Anxiety, Insomnia, and Post-Traumatic Stress Disorder in Pregnant Women
The results of multiple step linear regression analysis showed that pregnancy complications and current prevention and control status were risk factors for anxiety in pregnant women, while adverse pregnancy history and family income were protective factors for anxiety in pregnant women (P < 0.05). Pregnancy complications, current prevention and control status, and pregnancy stage were the risk factors for insomnia in pregnant women, while adverse pregnancy history was the protective factor for insomnia (P < 0.05). The return of contacts from the epidemic area and pregnancy stage were risk factors for PTSD, while adverse pregnancy history was a protective factor for PTSD (P < 0.05). Detailed data are presented in Tables 3-5
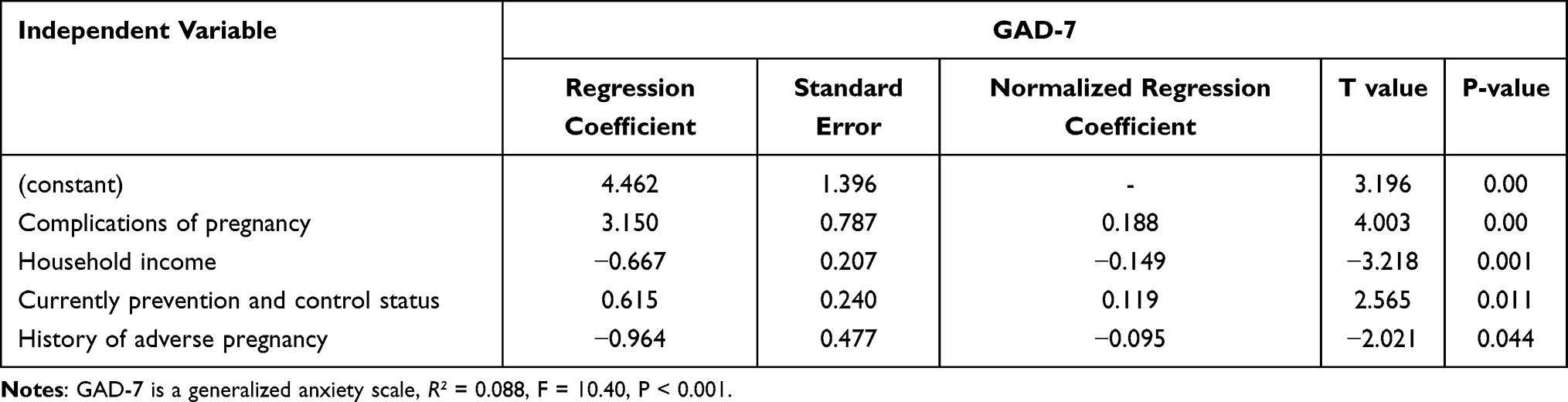 |
Table 3 Multi-Factor Analysis of Anxiety in Pregnant Women |
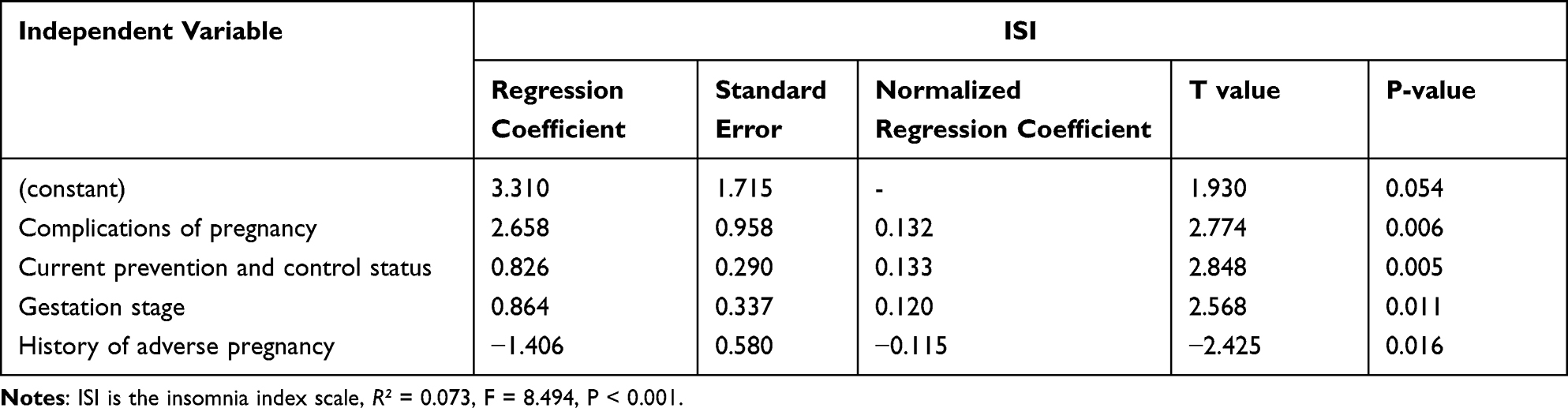 |
Table 4 Multivariate Analysis of Insomnia in Pregnant Women |
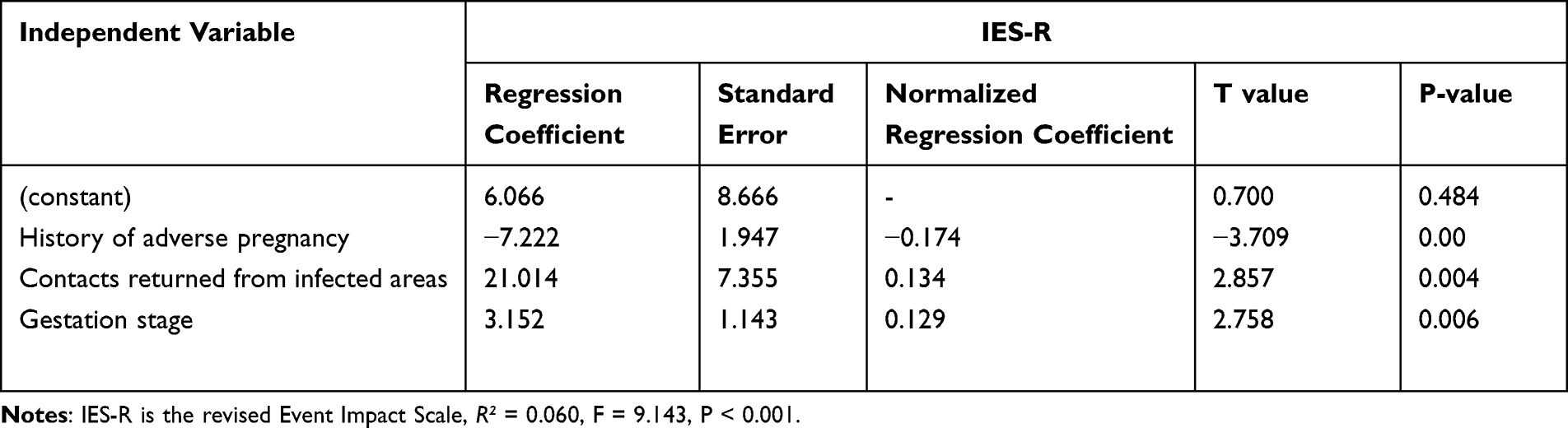 |
Table 5 Multi-Factor Analysis of Stress in Pregnant Women |
Discussion
The results of this study showed that pregnant women have widespread anxiety, insomnia and stress disorder with COVID-19. The results of this study showed that the detection rate of anxiety, insomnia, and stress disorder in pregnant women was significantly higher than that in the general population, which was consistent with the conclusions of previous studies.3,12,13 However, the detection rates of anxiety, insomnia, and stress disorders and the related average scores of pregnant women were lower than those in the early stage of COVID-19.14–16 The reasons may be as follows: Since the first outbreak of COVID-19, China has gradually improved prevention and control measures, increased epidemic prevention supplies, and rationally deployed medical resources to reduce people’s exposure risks. Second, relevant medical institutions have undertaken a variety of measures in response to the call of the state, such as setting-up Internet hospitals to provide remote health management for pregnant women’s healthcare during pregnancy, a series of disinfection and isolation measures to control the development of the epidemic in obstetric clinics and wards in a number of hospitals, while also opening a green channel for emergency and critical treatment and setting up 24-h online consultation services through relevant mini programs. At the same time, a contactless method was developed to write a prescription online and mail it to patients’ homes. Finally, the relevant media correctly guided the public through scientific prevention and control through popular science education to reduce the fear in pregnant women to an extent. These measures may alleviate the anxiety of pregnant women, insomnia, stress disorders, and other negative emotions.
The results of this study show that adverse pregnancy history is a protective factor for anxiety, insomnia, and post-traumatic stress disorder in pregnant women during COVID-19, that is, women without a history of abortion during COVID-19 are more anxious than those with a history. Different from the results of previous studies, which showed that pregnant women with a history of abortion were more prone to anxiety and depression.17,18 This study showed that pregnant women with a history of adverse pregnancy during COVID-19 had lower scores on these three adverse emotions. The likely reason may be that in the non-COVID-19 epidemic, pregnant women experience excessive anxiety owing to adverse pregnancy outcomes and pay excessive attention to maternal and infant conditions, such as contractions and fetal development, which lead to a cycle of negative emotions. During the COVID-19 prevention and control, pregnant women may pay more attention to the following aspects: ①whether COVID-19 poses a risk to pregnant women; ②whether pregnant women are more likely to be infected with COVID-19 than non-pregnant women; ③ Risk of mother-to-child vertical transmission. Pregnant women may have attention bias modification (ABM) in the face of COVID-19 public events and personal events related to self-adverse pregnancy history, thus alleviating symptoms such as anxiety, insomnia, and PTSD, but this has not been reported. Attention bias modification (ABM) is the modification of selective attention to information.19 However, ABM has been proposed as an efficient, accessible psychological therapy to alleviate anxiety symptoms in previous studies.20,21, In addition, pregnant women with a history of adverse pregnancy have received corresponding psychological counseling and corresponding behavioral guidance in the process of pregnancy protection, so that they may have a certain psychological ability to resist pressure.
The results of this study indicate that pregnancy complications, low income, and late pregnancy are risk factors for pregnant women’s bad mood. This study is consistent with previous research results.4,22,23 In addition to concerns about the adverse effects of complications on pregnancy and childbirth, pregnant women are also concerned about the high risk of developing serious illness after contracting COVID-19. Pregnant women from low-income families face the burden of high costs of childbirth and childcare; hence, they tend to worry easily about the family’s economic situation and are more prone to anxiety. With respect to gestational weeks, the greater the gestational week, the higher the physiological load on the woman’s organs and the greater the psychological burden. Furthermore, with the approaching of the due date, pregnant women become increasingly worried about the health of the fetus and their own delivery process and delivery mode and are susceptible to anxiety, insomnia, stress, and other psychological effects.
The results showed that the more cases of COVID-19 in the region where pregnant women were currently living, the more likely they were to suffer from anxiety and insomnia. At the same time, this study found that returning from the epidemic area is a risk factor for PTSD in pregnant women. This study is consistent with previous research results.24–26 The COVID-19 pandemic places multiple stressors on entire populations. First, pregnant women are particularly afraid of contracting COVID-19, believing that the more cases around them, the more likely they are to get sick. Second, pregnant women are at high risk of COVID-19 complications compared with non-pregnant women. Last, it has caused illness, deaths, and strain on healthcare and economic systems. People are afraid of contracting COVID-19, have to cope with COVID-19 symptoms, physical distancing, or grieving the loss of loved ones. Pregnant women are concerned about the increased risk of their own COVID-19 infection on the one hand, and the risk of vertical mother-to-child transmission on the other hand, thus further increasing their anxiety.
In all, the negative emotions of pregnant women have a great impact on mother and child,16,27–29 and it is essential to actively seek effective intervention measures. It is worth noting that this study found that adverse pregnancy history is a protective factor for anxiety, insomnia, and PTSD in pregnant women during COVID-19, and the analysis of the causes may have corrected the attention bias. Previous studies found that the attentional bias modification training (ABMT) can alleviate depressive symptoms.30–32 However, as far as we know, there are no reports yet on the effect of attention bias correction on the negative emotions of pregnant women. According to the situation of pregnant women, actively exploring the intervention study of attention bias correction may provide some ideas for clinical research.
Regarding the study’s limitations: Similar to other survey studies, observational studies generally suffer from information bias, selection bias, and confounding bias. In this study, efforts were made to control confounding bias through two approaches: Firstly, random sampling was employed during the study design phase and the corresponding study population was carefully selected based on strict exclusion criteria. Secondly, stepwise linear regression analysis was utilized to identify influencing factors and mitigate confounding bias. This paper mainly studies the mental health status of pregnant women during the prevention and control of novel coronavirus infection. The exclusion criteria here include most women with pre-existing mental disorders, and the exclusion criteria are to optimize the model and control confounding factors.
Limitations
First, this study is only a cross-sectional survey on the prevention and control status of the novel COVID-19 infection, which may not fully reflect the psychological status of all pregnant women with respect to the prevention and control status. Second, the sample size of this study is not large enough, which may have had a certain impact on the results. However, given the current circumstances, such a sample size suffices to substantiate the identified issue.
Conclusion and Recommendation
Given the influence of the COVID-19 pandemic, pregnant women seemed to generally have anxiety, insomnia, and stress disorders. Poor pregnancy history is a protective factor for pregnant women with anxiety, insomnia, and post-traumatic stress disorder. In the case of similar public health emergencies, attention bias modification (ABM) may be a potential intervention measure to provide potentially new ideas for alleviating the psychological disorders of pregnant women during this special period.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Considerations and Consent to Participate
Ethical clearance was obtained from the First Affiliated Hospital to Henan University of Chinese Medicine. All participants were informed about the purpose, benefits, risks, confidentiality of information, and voluntary nature of participation in the study. The respondents were notified that they had the right to refuse or stop at any point of the data collection. Personal identifiers were not included in the written questionnaires to ensure participants’ confidentiality. The research was funded by the Special Research Project of Traditional Chinese Medicine in Henan Province.
Acknowledgments
We are thankful to the data collectors and the pregnant women who participated in the data collection through Questionnaire Star and for their willingness to participate in the study. We would like to express our deepest gratitude to the First Affiliated Hospital to Henan University of Chinese Medicine for giving us financial support and South. The research was funded by a special study of Traditional Chinese Medicine in Henan Province. I confirm all participants provided informed consent, in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the reported work in terms of conception, study design, execution, acquisition of data, analysis, and interpretation; took part in drafting, revising and critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The project was supported by the program from Special research project of Traditional Chinese Medicine (No.20-21ZY2022).
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Li XL, Yu HG, Yang WQ, et al. Depression and anxiety among quarantined people, community workers, medical staff, and general population in the early stage of COVID-19 epidemic. Front Psychol. 2021;12:638985. doi:10.3389/fpsyg.2021.638985
2. Mancuso RA, Schetter CD, Rini CM, et al. Maternal prenatal anxiety and corticotropin-releasing hormone associated with timing of delivery. Psychosom Med. 2004;66(5):762–769. doi:10.1097/01.psy.0000138284.70670.d5
3. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
4. Ying J, Qingge L, Suwen F, et al. Status and influencing factors of anxiety and psychological stress disorder in pregnant women under novel coronavirus pneumonia. Chin J Nurs. 2020;55:SI.
5. Zhong QY, Gelaye B, Zaslavsky AM, et al. Diagnostic Validity of the Generalized Anxiety Disorder - 7 (GAD-7) among Pregnant Women. PLoS One. 2015;10(4):e0125096. doi:10.1371/journal.pone.0125096
6. Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
7. Hong Y, Lee J, Lee HJ, et al. Resilience and Work-Related Stress May Affect Depressive Symptoms in Nursing Professionals during the COVID-19 Pandemic Era. Psychiatry Invest. 2021;18(4):357–363. doi:10.30773/pi.2021.0019
8. Ong JC, Manber R, Segal Z, et al. A randomized controlled trial of mindfulness meditation for chronic insomnia. Sleep. 2014;37(9):1553–1563. doi:10.5665/sleep.4010
9. Chung KF, Kan KK, Yeung WF. Assessing insomnia in adolescents: comparison of Insomnia Severity Index, Athens Insomnia Scale and Sleep Quality Index. Sleep Med. 2011;12(5):463–470. doi:10.1016/j.sleep.2010.09.019
10. Feinstein A, Owen J, Blair N. A hazardous profession: war, journalists, and psychopathology. Am. J Psychiatry. 2002;159(9):1570–1575.
11. Wu KK. Chan KS. The development of the Chinese version of Impact of Event Scale–Revised (CIES-R). Soc. Psychiatry Psychiatr Epidemiol. 2003;38(2):94–98. doi:10.1007/s00127-003-0611-x
12. Shi L, Lu ZA, Que JY, et al. Prevalence of and risk factors associated with mental health symptoms among the general population in China during the coronavirus disease 2019 pandemic. JAMA Network Open. 2020;3(7):e2014053. doi:10.1001/jamanetworkopen.2020.14053
13. Gizzi G, Mazzeschi C, Delvecchio E, et al. Possible stress-neuroendocrine system-psychological symptoms relationship in pregnant women during the COVID-19 pandemic. Int J Environ Res Public Health. 2022;19(18):11497. doi:10.3390/ijerph191811497
14. Abahussain E, Al-Otaibi M, Al-Humaidi K, et al. Pregnancy complications in pandemics: is pregnancy-related anxiety a possible physiological risk factor? Int J Environ Res Public Health. 2022;19(19):12119. doi:10.3390/ijerph191912119
15. Yan H, Ding Y, Guo W, et al. Mental Health of Pregnant and Postpartum Women During the Coronavirus Disease 2019 Pandemic: a Systematic Review and Meta-Analysis. Front Psychol. 2020;11(11):617001. doi:10.3389/fpsyg.2020.617001
16. Medjedović Marcinko V, Marcinko D, Dordević V, et al. Anxiety and depression in pregnant women with previous history of spontaneous abortion. Coll Antropol. 2011;35(1):225–228.
17. He L, Wang T, Xu H, et al. Prevalence of depression and anxiety in women with recurrent pregnancy loss and the associated risk factors. Arch Gynecol Obstet. 2019;300(4):1061–1066. doi:10.1007/s00404-019-05264-z
18. Pan DN, Wang Y, Lei Z, et al. The altered early components and the decisive later process underlying attention bias modification in social anxiety: evidence from event-related potentials. Soc Cogn Affect Neurosci. 2019;14(12):1307–1316. doi:10.1093/scan/nsz098
19. Macleod C, Mathews A. Cognitive bias modification approaches to anxiety. Annu Rev Clin Psychol. 2012;8:189–217. doi:10.1146/annurev-clinpsy-032511-143052
20. Kajdy A, Sys D, Pokropek A, et al. Risk factors for anxiety and depression among pregnant women during the COVID-19 pandemic: results of a web-based multinational cross-sectional study. Int J Gynaecol Obstet. 2023;160(1):167–186. doi:10.1002/ijgo.14388
21. Lowther H, Newman E, et al. Attention bias modification (ABM) as a treatment for child and adolescent anxiety: a systematic review. J Affective Disorders. 2014;168:125–135. doi:10.1016/j.jad.2014.06.051
22. Chen WP, Peng W, Zhang Y, et al. Anxiety and depression among perinatal women during the long-term normal prevention of COVID-19 pandemic period in China: a cross-sectional study. BMC Psychiatry. 2023;23(1):451. doi:10.1186/s12888-023-04930-6
23. Yu YH, Zhu XH, Xu HL, et al. Prevalence of depression symptoms and its influencing factors among pregnant women in late pregnancy in urban areas of Hengyang City, Hunan Province, China: a cross-sectional study. BMJ Open. 2020;10(9):e038511–e038511. doi:10.1136/bmjopen-2020-038511
24. Liu CH, Erdei C, Mittal L. Risk factors for depression, anxiety, and PTSD symptoms in perinatal women during the COVID-19 Pandemic. Psychiatry Res. 2021;295:113552. doi:10.1016/j.psychres.2020.113552
25. Kokou-Kpolou CK, Megalakaki O, Laimou D, Kousouri M. Insomnia during COVID-19 pandemic and lockdown: prevalence, severity, and associated risk factors in French population. Psychiatry Res. 2020;290:113128. doi:10.1016/j.psychres.2020.113128
26. Puertas-Gonzalez JA, Mariño-Narvaez C, Isabel Peralta-Ramírez M, et al. The psychological impact of the COVID-19 pandemic on pregnant women. Psychiatry Research-Neuroimaging. 2021;301:113978. doi:10.1016/j.psychres.2021.113978
27. Christian LM. Physiological reactivity to psychological stress in human pregnancy: current knowledge and future directions. Prog Neurobiol. 2012;99(2):106–116. doi:10.1016/j.pneurobio.2012.07.003
28. Ostlund BD, Vlisides-Henry RD, Crowell SE, et al. Intergenerational transmission of emotion dysregulation: part II. Developmental origins of newborn neurobehavior. Dev Psychopathol. 2019;31(3):833–846. doi:10.1017/S0954579419000440
29. Adamson B, Letourneau N, Lebel C, et al. Prenatal maternal anxiety and children’s brain structure and function: a systematic review of neuroimaging studies. Dev Psychopathol. 2019;31(3):833–846.
30. Mastikhina L, Dobson K. Biased attention retraining in dysphoria: a failure to replicate. Cogn Emot. 2017;31(3):625–631. doi:10.1080/02699931.2015.1136270
31. Li G, Cai X, Yang Q, et al. A review of attentional bias modification trainings for depression. CNS Neurosci Ther. 2023;29(3):789–803. doi:10.1111/cns.14022
32. Dennis-Tiwary TA, Denefrio S, Gelber S. Salutary effects of an attention bias modification mobile application on biobehavioral measures of stress and anxiety during pregnancy. Biol Psychol. 2017;127:148–156. doi:10.1016/j.biopsycho.2017.05.003
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Anxiety and Depression Among HIV-Positive and HIV-Negative Pregnant Women During COVID-19 Pandemic in Ekiti State, Southwest Nigeria
Ade-Ojo IP, Dada MU, Adeyanju TB
International Journal of General Medicine 2022, 15:4123-4130
Published Date: 16 April 2022
RETRACTED ARTICLE: Psychotherapy and Follow-Up in Health Care Workers After the COVID-19 Epidemic: A Single Center’s Experience
Chen H, Ma Q, Du B, Huang Y, Zhu SG, Li SL, Geng DQ, Xu XS
Psychology Research and Behavior Management 2022, 15:2245-2258
Published Date: 18 August 2022
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Maternal Anxiety and Its Associated Factors During the First and Second Wave of COVID-19 Pandemic in Serbia: A Cross-Sectional Study
Jeličić L, Janković S, Sovilj M, Bogavac I, Drobnjak A, Dimitrijević A, Subotić M
Psychology Research and Behavior Management 2022, 15:3775-3792
Published Date: 20 December 2022
How Do Anxiety and Relationship Factors Influence the Application of Childbirth Education Strategies During Labor and Birth: A Bowen Family Systems Perspective
Sutcliffe KL, Levett K, Dahlen HG, Newnham E, MacKay LM
International Journal of Women's Health 2023, 15:455-465
Published Date: 1 April 2023