Back to Journals » Psychology Research and Behavior Management » Volume 15
Maternal Anxiety and Its Associated Factors During the First and Second Wave of COVID-19 Pandemic in Serbia: A Cross-Sectional Study
Authors Jeličić L ![]() , Janković S, Sovilj M, Bogavac I, Drobnjak A, Dimitrijević A, Subotić M
, Janković S, Sovilj M, Bogavac I, Drobnjak A, Dimitrijević A, Subotić M
Received 1 October 2022
Accepted for publication 9 December 2022
Published 20 December 2022 Volume 2022:15 Pages 3775—3792
DOI https://doi.org/10.2147/PRBM.S391694
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Ljiljana Jeličić,1,2 Svetlana Janković,3,4 Mirjana Sovilj,2 Ivana Bogavac,1,2 Anđela Drobnjak,2 Aleksandra Dimitrijević,5,6 Miško Subotić1
1Cognitive Neuroscience Department, Research and Development Institute “Life Activities Advancement Institute”, Belgrade, Serbia; 2Department of Speech, Language and Hearing Sciences, Institute for Experimental Phonetics and Speech Pathology, Belgrade, Serbia; 3Department of Acute Perinatal Pathology, Belgrade University Medical School, Belgrade, Serbia; 4Clinic for Gynecology and Obstetrics Narodni Front Belgrade, Belgrade, Serbia; 5Department of Gynecology and Obstetrics, Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia; 6Clinic of Gynecology and Obstetrics, University Clinical Centre of Kragujevac, Kragujevac, Serbia
Correspondence: Ljiljana Jeličić, R&D Institute “Life Activities Advancement Institute”, Institute for experimental phonetics and speech pathology, G. Jovanova No. 35, Belgrade, 11000, Serbia, Tel +381 11 3208 519 ; +381 64 22 14 295, Fax +381 11 2624 168, Email [email protected]; [email protected]
Aim: The COVID 19-pandemic affects people differently, while pregnant women are among the most sensitive populations. The data about maternal mental health during the COVID-19 outbreak are in some ways consistent but also country-specific.
Purpose: The study aims to explore the impact of the COVID-19 pandemic on pregnant women’s anxiety and identify its associated factors.
Patients and Methods: This cross-sectional study included a sample of 358 pregnant women during the first and second waves of the pandemic in Serbia. An anonymous survey included basic demographic questions, pregnancy-related background questions, the question of self-reported COVID-19-related fear, State-Trait Anxiety Inventory (STAI), and Multidimensional Scale of Perceived Social Support (MSPSS).
Results: The study revealed no pregnant women with low anxiety levels measured by STAI-T and STAI-S, while the STAI-S and STAI-T scores indicated high anxiety in 32.4% and 42.7% of pregnant women, respectively. The obtained results pointed out the nonlinear dependence of state anxiety on observed associated factors and their complex interactions, including the data collecting period.
Conclusion: Our findings reveal that COVID-19 affects pregnant women’s mental health and makes it necessary for psychological monitoring and support for pregnant women, which may be reflected in their mental health but also the development of their offspring.
Keywords: maternal mental health, pregnancy, first and second wave of coronavirus, anxiety, social support, COVID-19 related fear
Introduction
In early December 2019, a new strain of coronavirus appeared in the city of Wuhan (China), after which it rapidly spread across the globe.1 The first COVID-19 case in Serbia was confirmed on March 6, 2020, and a state of emergency was declared on March 15.2 The high danger to humanity posed by the new global pandemic has led to the introduction of numerous restrictions and measures by the countries’ governments worldwide. Although these measures were implemented to protect the entire population from coronavirus, they also led to adverse effects, especially at the level of mental health, which must not be ignored. To be more precise, the global pandemic has led to adverse health impacts,3,4 including the anxiety and fear of citizens.5
Anxiety and fear are basic human emotions throughout life.6 Anxiety is a normal response described as a state with a positive and motivating influence on adaptive behavior and coping.7 On the other hand, the expressed anxiety level, which is variable in each individual, may lead to persistent, uncontrollable, excessive, and inappropriate anxiety reactions, even after the withdrawal of the stimulus.8 Fear is a normal reaction to a real or imagined threat and is considered an integral and adaptive aspect of development.9 Like anxiety, when these often adaptive states become characteristic of an individual or like traits, the resulting phenomena can become physically and psychologically destructive.10 As a result, anxiety affects physiological arousal and cognitive functions,11 with manifestation in two entities: state anxiety as a current and transient emotional state and trait anxiety as a permanent personality trait.12
Social support is the perception that others (such as family members, friends, and significant others) care about you and that you can turn to them with confidence in everyday situations or certain moments of crisis.13 The research points to social support as a protective mechanism that may relieve stress and mitigate the adverse mental health issues.14
The data about the mental health of pregnant women during the COVID-19 outbreak are in some ways consistent but also country-specific. So far, there are already some papers with clinical findings on the impact of COVID-19 on pregnancy15–17 and psychological findings related to the mental health of pregnant women.3,18–20
Mutations of the COVID-19 virus (Delta variant in the second pandemic wave) brought additional complications resulting in a severe course of the disease and increased rates of adverse obstetric outcomes in pregnant women,21 which can additionally be reflected in psychological consequences. On the other hand, vaccination which represents a significant prevention of the severe course of the disease, which may alleviate adverse physical and psychological health outcomes in pregnant women,22 may represent a significant factor influencing maternal anxiety, but it was not analyzed in the study since it was not administered in the observed data collecting periods in Serbia.
Furthermore, due to worries about fetal development, pregnant women tend to show different levels of psychological problems, among which pregnancy-related anxiety is one of the most common.23 On the other hand, pregnancy is a risk factor for COVID-19.24 More precisely, various measures conducted to protect the population from COVID-19 disease also affect pregnant women´s psychological state and represent a source of anxiety. Furthermore, specific anxiety-related distress responses during viral outbreaks and the COVID-19 pandemic have been observed.25
Numerous studies pointed out the higher anxiety levels in pregnant women during the COVID-19 pandemic.20,24,26–31 The most recent literature has shown that the prevalence of anxiety in pregnancy during COVID-19 ranges from 30.5% to 42%.31–33 On the other hand, there are countries in which the COVID-19 pandemic did not increase anxiety levels (The Netherlands)34 or have a lower prevalence of anxiety among pregnant women (Belgium) (moderate anxiety in 8.4% of pregnant women; severe anxiety in 5.2% of pregnant women.35 Such data confirm that findings related to the anxiety levels in pregnant women during the COVID-19 outbreak are not entirely consistent but rather country-specific. Possible explanations for this are, on the one hand, different measures implemented during the COVID-19 pandemic in each country (quarantine, complete or partial lockdown, overstretching of the healthcare system, emphasized hygiene measures, physical distancing, closure of companies and educational institutions, and others). On the other hand, these specificities may originate from the research methodology or sample characteristics. Furthermore, the cultural specificities of the country and its population may also lead to country-specific data.
To the best of our knowledge, no studies examine the STAI-S during the first and second pandemic waves, and limited studies have assessed mental health during the COVID-19 pandemic in Serbia,36,37 especially anxiety in pregnant women. Therefore, the present study was conducted to address this gap.
In the current study, we assessed the impact of the COVID-19 pandemic on pregnant women’s anxiety during the first and second waves of COVID-19 in Serbia. Since STAI-S examines the current state of anxiety (state anxiety), and STAI-T examines trait anxiety, we aimed to assess to what extent the data collecting period affects the maternal state anxiety. We also aimed to identify how COVID-19-related fear, social support, or certain pregnant women’s demographic characteristics are associated with pregnant women’s anxiety during the COVID-19 pandemic in Serbia.
Materials and Methods
Study Design and Participants
The cross-sectional study of pregnant women’s anxiety was conducted during the first and second waves of the COVID-19 pandemic in Serbia to determine the impact of COVID-19 on maternal anxiety and identify its associated factors. The study sample was women in the third trimester of pregnancy, who were included consecutively in the order in which they came for a regular examination during pregnancy. Participating pregnant women were recruited from the state-funded Clinic for Gynecology and Obstetrics “Narodni Front” in the Serbian capital, Belgrade. The number of births in this clinic is around 7000 per year, with pregnant women coming from all over Serbia. All pregnant women were asked to complete an anonymous self-administered questionnaire voluntarily in a pleasant atmosphere in the waiting room during a time-optimal for them. Before administering a questionnaire, participants were informed about the research’s goal: to examine the influence of COVID-19 on a woman’s mental health, which may be reflected in the child’s development. The questionnaire contained questions about socio-demographics, pregnancy-related background, perceived COVID-19 related fear, the presence of current or recent COVID-19 disease in the family and close relatives, maternal anxiety, perceived social support, maternal mental health, and personal contact information related to an e-mail address and/or mobile phone. It is emphasized that personal contact information should be written if the pregnant woman agrees to provide data on her child’s development later in the longitudinal research. All participants signed their written informed consent to participate in this study, and confidentiality of the responses was assured.
The study sample included the data collected during the first pandemic wave (from April to June 2020) and the second pandemic wave (from early June to October 2020) in Serbia. It was recruited from a larger sample collected between April 2020 and December 2020. Namely, 900 questionnaires were distributed between April 2020 and December 2020; 209 were not completed, and 187 were partially completed. After defining the inclusion and exclusion criteria, the final sample included 358 pregnant women (39.8%). The inclusion criteria for the study were: normal singleton pregnancy without complications of any kind; singleton pregnancies with the presence of hypertension, diabetes, or preterm delivery symptoms; spontaneous conception, delivering a phenotypically normal live birth. The exclusion criteria for the study were: failure to meet the inclusion criteria, infertility treatment; hospitalization; history of preeclampsia, eclampsia, autoimmune diseases, cancer, or any general chronic illnesses except hypertension or diabetes; psychiatric illnesses verified and/or treated before pregnancy; use of tranquillizers or sedatives, tobacco, alcoholic beverages, or any other type of psychoactive substances; non-acceptance of participation in the study. The exclusion criteria were in relation to the primary goal of the research, for which it was significant to reduce factors that can influence pregnant women’s anxiety, and are not related to the COVID-19 pandemic. Regarding sociodemographic characteristics, it is essential to point out a significant disproportion between participants with average, low, and high household income, concerning the small presentation of women with low or high household income. It resulted in average household income being one of the inclusion criteria.
Measures
Two scales were administered to the participants: the Spielberger State-Trait Anxiety Inventory (STAI)12 and the MSPSS.38
- Pregnant women’s anxiety was measured with the Spielberger State-Trait Anxiety Inventory (STAI), a widely used measure of general anxiety.12 The questionnaire form Y was used in our study.39 It represents a self-report measure of anxiety and has two scales: The STAI-S scale consists of 20 statements and measures transient anxiety states, ie subjective, consciously perceived feelings of anxiety, tension and concerns that change their intensity over time (state anxiety). It can be used to determine the actual anxiety intensity levels induced by stressful procedures.40 The STAI-T scale consists of 20 statements and measures relatively stable individual differences in propensity for anxiety (trait anxiety). It evaluates relatively stable aspects of “anxiety proneness”, including general states of calmness, confidence, and security.41 State and trait anxiety are evaluated on a 4-point Likert scale, from “almost never”, “sometimes”, “often” and “almost always” for the trait anxiety, and from “not at all”, “somewhat”, “moderately so”, and “very much so” for the state anxiety. The total score for each scale ranges between 20 and 80, with higher scores indicating greater anxiety levels. STAI scores are classified as “no or low anxiety” (20–30), “moderate anxiety” (31–44), and “high anxiety” (45–80). Despite this categorization, many authors use two-level cut-off points to define the low or medium/high state of state and trait anxiety.26,42,43 Three-level cut-off points which define low, intermediate or high state and trait anxiety levels were used in our study for reasons described in the literature.44,45
- Multidimensional Scale of Perceived Social Support (MSPSS) is an instrument which measures perceived support from three sources: family members, friends, and significant others.38 Pregnant women’s perception of social support was measured with the Serbian version of the MSPSS.46 This instrument has strong psychometric properties in the population of pregnant women.47 It consists of 12 items which are scored on a 7-point Likert scale ranging from “very strongly disagree” (1) to “very strongly agree” (7). The MSPSS scores range from 12 to 84. Higher total scores indicate high levels of perceived social support.
- COVID-19-related fear was assessed using a single item question, “Do you feel a fear of COVID-19 viral infection?” Participants select one of three responses: 1 - “I do not feel a fear of COVID-19 viral infection”; 2- “Sometimes, not all the time, I feel a fear of COVID-19 viral infection”; 3 - “I do feel a fear of COVID-19 viral infection”.
Statistical Analysis
Descriptive statistics were used to determine central tendencies and distributions of variables. To determine the existence of relationships between variables, we conducted a bivariate correlation analysis. One-Way ANOVA was used to compare means between variables of interest. Before any statistical test, appropriate assumptions were checked.
For STAI-S, STAI-T and MSPSS, we defined the new variables STAI-S level, STAI-T level and MSPSS level, dividing the main variables into three groups. For STAI-S and STAI-T levels, range limits are: if STAI-S/STAI-T is ≤30, Level is Low (1), if STAI-S/STAI-T is between 31 and 44, Level is Intermediate (2), and for values ≥45 Level is High (3). For MSPSS, level range limits are Low (1) ≤35; Medium (2) between 36 and 60; High (3) ≥61.
To investigate the effects of individual factors on the variables of interest and interactions between factors, we conducted Univariate General Linear Model (GLM) Analysis. Before hypothesis testing, a priori contrasts were applied and, depending on the results Post hoc test was applied. Before conducting a Univariate General Linear Model analysis, we checked the assumption of the equality of variances. Levene’s Test of Equality of Error Variances having STAI-S as a dependent variable; Education, Data collecting period (first and second pandemic wave), Number of children, Pregnancy health condition, COVID-19 related fear, Employment and COVID-19 disease in the family, as independent variables, and STAI-T, MSPSS and Maternal age as covariates revealed that the assumption of equality is violated (FSTAI-S (124, 234) = 1.597, p=0.001). To overcome this problem, we log-transformed (logarithm with base 10) STAI-S, STAI-T, MSPSS, and age and obtained new variables logSTAI-S, logSTAI-T, logMSPSS, and logage, respectively. For the Univariate GLM analysis, we used type IV sum of squares because it is appropriate for unbalanced sample with missing events.
Univariate analysis with all independent variables (Education, Data collecting period, Number of children, Pregnancy health condition, COVID-19 related fear, Employment and COVID-19 disease in the family) and covariates logSTAI-S, logMSPSS, and logage revealed that there is no statistically significant impact of Number of children nor as the main effect nor through interactions. The model was reduced by taking the following independent variables: Education, Data collecting period, COVID-19 related fear, Employment, Pregnancy health condition, and COVID-19 disease in the family.
Levene’s Test of Equality of Error Variances revealed that the assumption of equality is not violated FlogSTAI-S (74,283) = 1.250, p=0.102.
Statistical Package for the Social Sciences version 22.0 was used.
Results
Sample Characteristics
The research sample comprised 358 pregnant women with a mean age of 30.80 (SD = 6.06). One-third of the participants (n=117, 32.7%) were examined in the first data collecting period, and two-thirds (n=248, 67.3%) in the second data collecting period. None of the participants had a low level of anxiety. More than half of the participants (n=205, 57.3%) had an intermediate level of trait anxiety, while 42.7% (n=153) had a high level of trait anxiety. Regarding state anxiety, two-thirds of participants (n=242, 67.6%) had an intermediate level, while 32.4% (n=116) had a high level of state anxiety. Almost all participants (n=344, 96.1%) reported high perceived social support. Baseline sample characteristics are shown in Table 1.
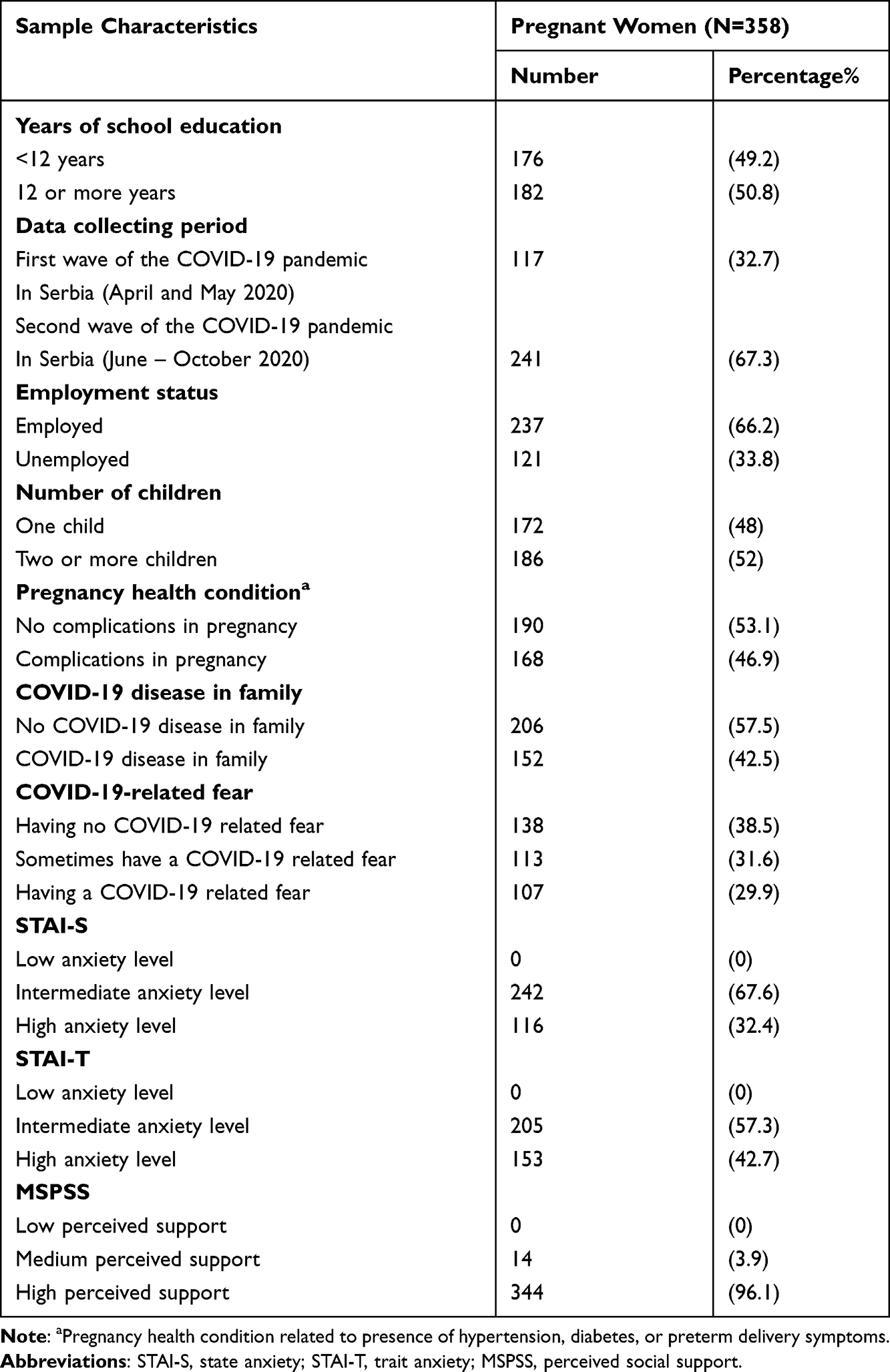 |
Table 1 Sample Characteristics (N=358) |
Descriptive statistics on maternal age, state and trait anxiety, and perceived social support are shown in Table 2. No participants had scores corresponding to low anxiety levels either on the STAI-S or STAI-T scale.
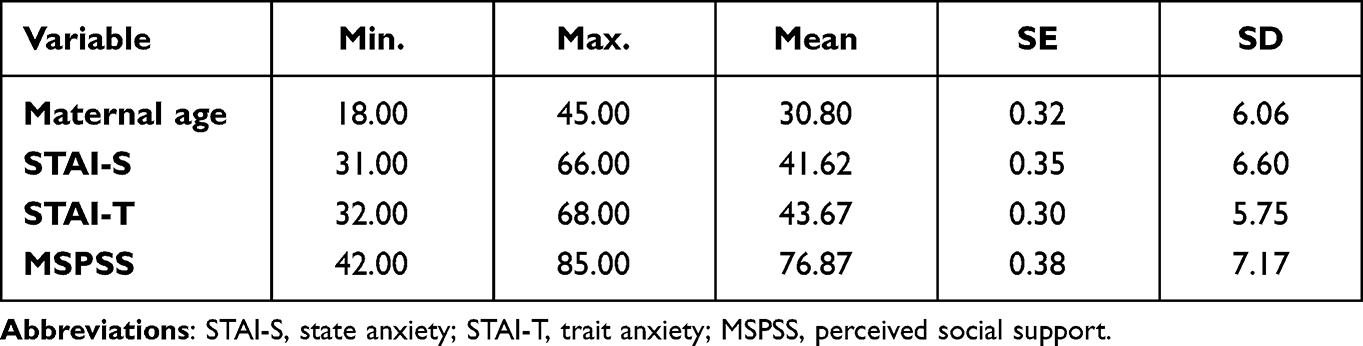 |
Table 2 Descriptive Statistics on Maternal Age, State and Trait Anxiety, and Perceived Social Support |
Mean values for maternal age, STAI-S, STAI-T, and MSPSS related to fear of COVID-19 (Table 3) show minor differences between the groups for the observed variables. One-way ANOVA revealed no statistically significant difference comparing maternal age related to the subjective attitude towards COVID-19 related fear, F(2355)=1.547, p=0.214.
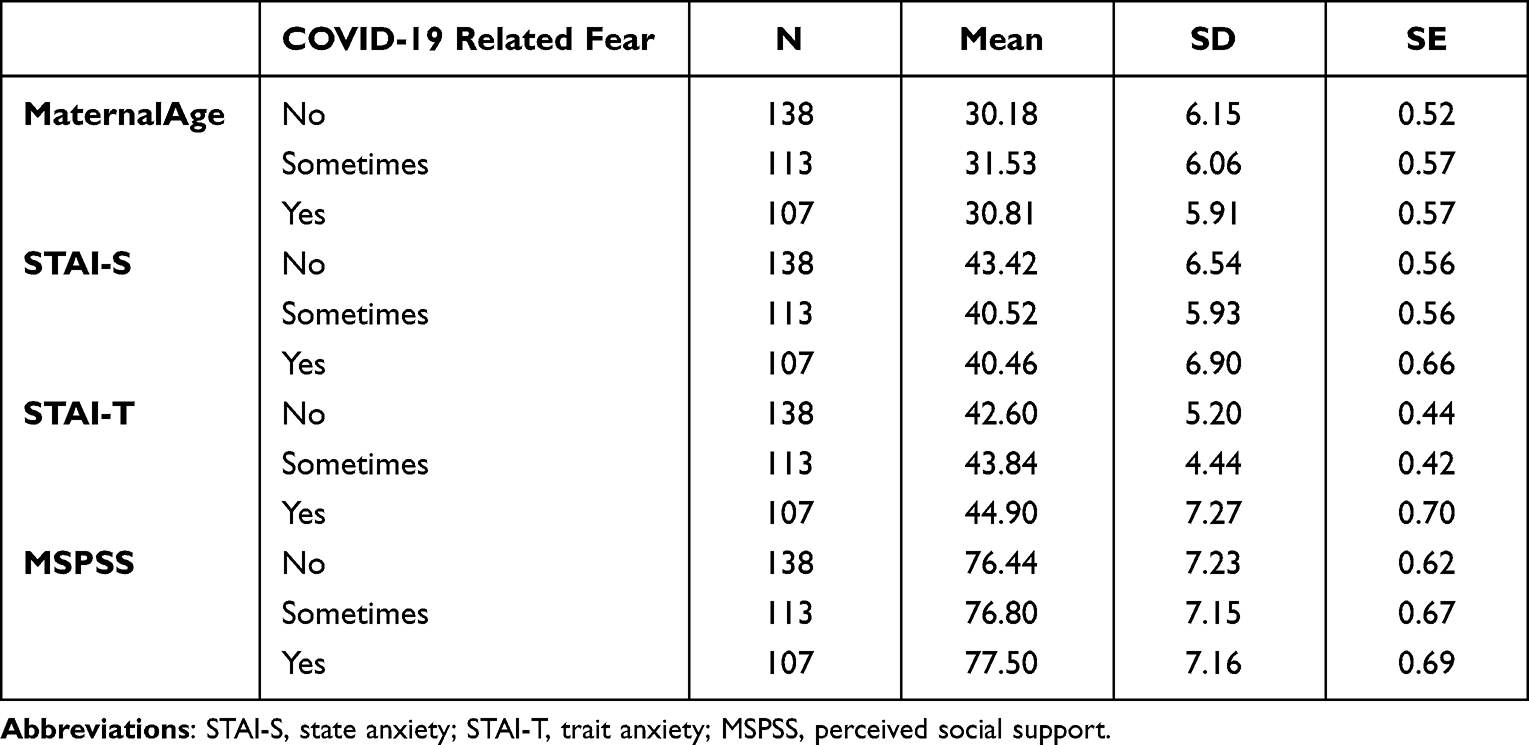 |
Table 3 Descriptive Statistics for Maternal Age, STAI-S, STAI-T and MSPSS Related to COVID-19 Related Fear |
Mean values for maternal age, STAI-T, and MSPSS related to the data collecting period show minor differences between the groups for the observed variables. One-way ANOVA revealed no statistically significant difference comparing maternal age related to the first and second pandemic waves F(1356)=1.381, p=0.241, STAI-T F(1356)=2.483, p=0.116, and there is no statistically significant difference comparing MSPSS of pregnant women related to data collecting period F(1356)=.077, p=0.781 (Table 4).
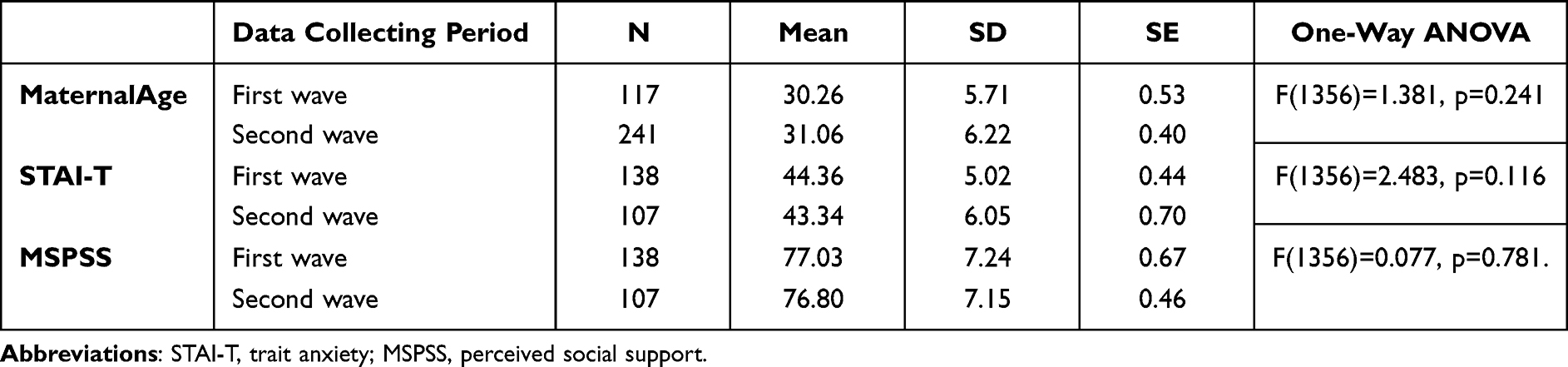 |
Table 4 Descriptive Statistics for Maternal Age, STAI-T and MSPSS Related to Data Collecting Period |
Correlation of Maternal Age, STAI-S, STAI-T, and MSPSS Scores in the First and Second Data Collecting Period
Table 5 shows the correlation between maternal age, STAI-S, STAI-T, and MSPSS scores in the first and second data collecting period. Bivariate correlation analysis revealed a statistically significant low correlation between particular parameters, some positive and some negative.
 |
Table 5 Correlation Between Maternal Age, STAI-S, STAI-T and MSPSS in the First and Second Data Collecting Period |
In the first data collecting period low negative statistically significant correlation is found between the Maternal age and STAI-S [r(117) = −0.195, p = 0.035] and Maternal age and MSPSS [r(117) = −0.229, p = 0.013].
In the second data collecting period low positive statistically significant correlation is found between STAI-S and STAI-T [r(241) = 0.274, p < 0.001] and STAI-S and MSPSS [r(241) = 0.163, p = 0.011]. Also, there is a low negative statistically significant correlation between the STAI-T and MSPSS [r(241) = −0.148, p = 0.022].
Univariate Analysis
Univariate GLM analysis for dependent variable logSTAI-S achievement revealed that the full linear model (Table 6) could explain 43.5% of variability F(77,280)=2.80, p<0.001, ηp2=0.435 and Observed Power=1. LogSTAI-S and LogMSPSS as the main effects have a statistically significant impact on the model. There is no statistically significant main effect of independent variables, but their effect is present through two and three way interactions (Table 6). Table 6 shows Tests of Between-Subjects Effects containing only statistically significant elements, including statistical significance, Partial Eta Square and Observed power. The literature is ambiguous on the validity of using the Observed Power in interpreting the obtained results. Having that in mind, the paper also presents those statistically significant interactions whose Observed Power is <0.8.48–50
 |
Table 6 Tests of Between-Subjects Effects Containing Only Statistically Significant Elements |
There are five two-way interactions and three three-way interactions. Education* COVID-19 disease in the family is only two-way interaction which is not an element of three-way interactions. COVID-19 related fear is the most frequently appearing independent variable in interactions (five times), followed by Data collecting period (four times).
A closer look at the interaction terms (Table 6) revealed that we could analyse the following interactions independently: Education* COVID-19 disease in the family; Education * Data collecting period * COVID-19 related fear; Employment * Data collecting period * COVID-19 related fear; COVID-19 disease in the family * Pregnancy health condition * COVID-19 related fear. The most significant contribution to the model has the interaction term Employment * Data collecting period * COVID-19 related fear (Partial eta squared=0.068).
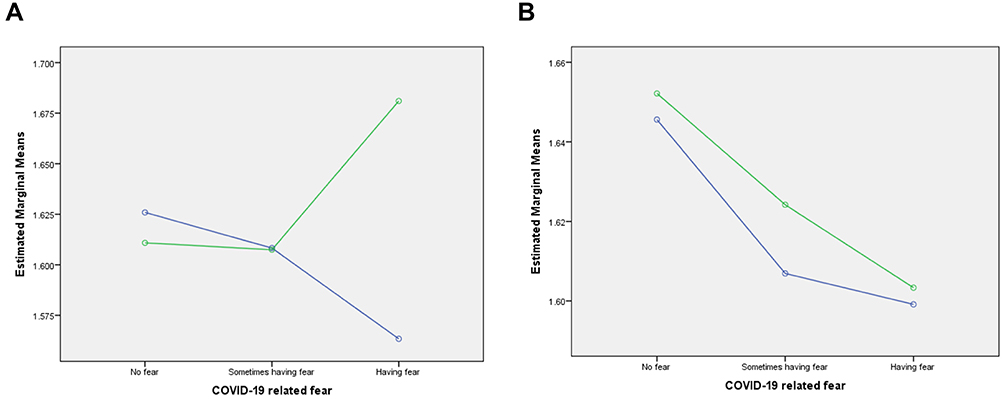
Figures 1 and 2 show the plots of estimated marginal means of dependent variable logSTAI-S for two three-way statistically significant interactions (Education * Data collecting period * COVID-19 related fear; Employment * Data collecting period * COVID-19 related fear, respectively) are presented as examples.





New grouping variables were composed for each interaction term (Table 7) to determine if there was a statistically significant difference between the mean values of groups within interaction terms. One–way ANOVA for new grouping variables was conducted.
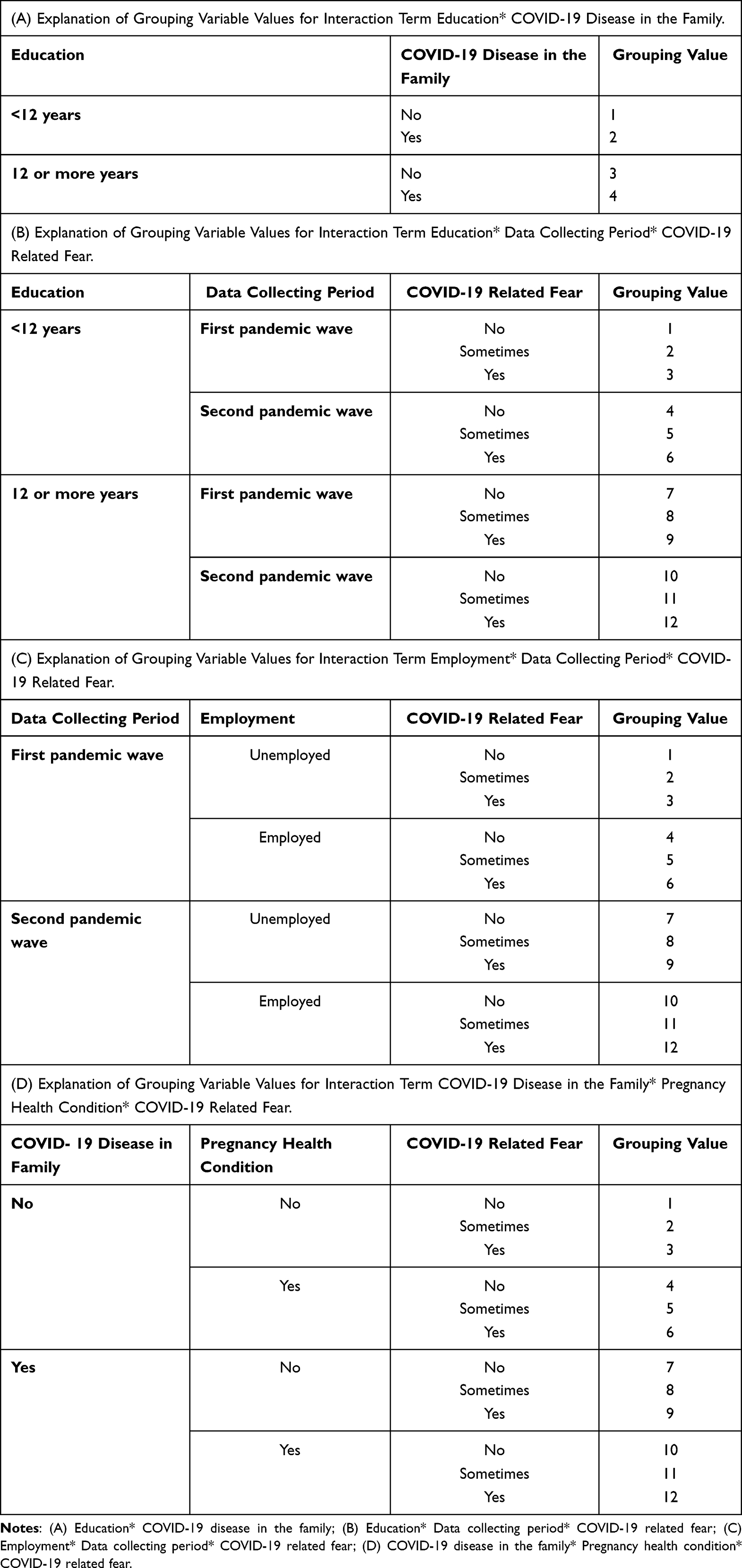 |
Table 7 Explanation of New Grouping Variables of Interaction Terms Used in One–Way ANOVA Statistical Test |
One-way ANOVA revealed no statistically significant difference between groups of interaction term Education * COVID-19 disease in the family (F(3354)=.821, p=0.483).
For interaction term Education * Data collecting period * COVID-19 related fear, we obtained a statistically significant difference between groups F(11,346)=5.592, p<0.001. (Levene’s Test of Equality of Error Variances revealed that the assumption of equality is not violated F(11,346)=1.360, p=0.190. It turns out that group 3 had the highest (mean value=1.669), and group 2 had the lowest level (mean value 1.535) of logSTAI-S. Post Hoc test with Tukey-Kramer correction revealed a statistically significant difference between group 2 and all other groups except group 5 (mean value 1.586) and group 8 (mean value 1.588). There is also a statistically significant difference between group 8 and groups 1, 3, 4 and 9 and between groups 5 and 9. An explanation of membership to the variable group is given in Table 7B.
For interaction term Data collecting period * Employment * COVID-19 related fear, we obtained a statistically significant difference between groups F(11,346)=5.009, p<0.001. (Levene’s Test of Equality of Error Variances revealed that the assumption of equality is not violated F(11,346)=1.110, p=0.352. It turns out that group 4 had the highest (mean value=1.672), and group 5 had the lowest level (mean value 1.548) of logSTAI-S. Post Hoc test with Tukey-Kramer correction revealed a statistically significant difference between group 2 and groups 3, 4 and 7 and group 3 and groups 2, 5, 8 and 9. Furthermore, there is a statistically significant difference between group 5 and groups 1, 3, 4, 7, 10 and 12. An explanation of membership to the variable group is given in Table 7C.
For interaction term COVID-19 disease in the family * Pregnancy health condition * COVID-19 related fear, we obtained a statistically significant difference between groups F(11,346)=3.570, p<0.001. (Levene’s Test of Equality of Error Variances revealed that the assumption of equality is not violated F(11,346)=1.396, p=0.172. It turns out that group 6 had the highest (mean value=1.646), and group 11 had the lowest level (mean value 1.578) of logSTAI-S. Post Hoc test with Tukey-Kramer correction revealed a statistically significant difference between group 2 and groups 1, 4 and 6 and group 6 and groups 2, 5 and 11. An explanation of membership to the variable group is given in Table 7D.
Discussion
The impact of the novel coronavirus, SARS-CoV-2, and Coronavirus Disease-2019 (COVID-19) on physiological, psychological, social, and economic status has been investigated in research on different clinical and typical human populations and from various aspects.51–55 Considering the population of pregnant women, research in the past two years revealed that they might be affected by various aspects of the COVID-19 pandemic, causing negative implications on their mental health, especially anxiety and depression.3,18,20,56 More precisely, pregnant women represent a very vulnerable group in the conditions of the COVID-19 pandemic.56
To our knowledge, limited studies have assessed maternal anxiety during the COVID-19 pandemic in Serbia.36,57,58 The present cross-sectional study examined the impact of the COVID-19-related fear, social support, or certain pregnant women’s demographic characteristics on pregnant women’s anxiety during the first and second wave of COVID-19 in Serbia.
Our main findings were as follows: Most pregnant women from the sample reported high perceived social support during both data collecting periods. No pregnant women, who were examined during the first and second pandemic wave in Serbia, had low anxiety levels measured by STAI-T and STAI-S. A slightly less than one-third of the pregnant women reported a COVID-19 related fear. The study pointed out the complex dependence of state anxiety on various factors, including the data collecting period. While in the first wave, the interaction between the parameters is expressed, in the second, it is absent, and the pattern of the parameters’ influence on pregnant women’s anxiety is observed.
Perceived Social Support in Pregnant Women During the First and Second Wave of COVID-19 in Serbia
Findings from our study showed that almost all participants reported a high level of perceived social support during the first and second pandemic waves in Serbia. Also, there was no statistically significant difference comparing perceived social support of pregnant women related to the data collecting period. Before and during the COVID-19 pandemic, studies pointed out that pregnant women reported a higher level of social support than the general population.59,60 Such studies indicated that high social support plays a protective role in anxiety during pregnancy.61–63 Considering the COVID-19 pandemic, this may be explained by the fact that it imposed social isolation, due to which pregnant and postpartum women received more support from their partners and were less disturbed by external stimuli compared to the pre-COVID-19 women.64 Our study’s findings showed a high level of perceived social support in pregnant women, despite their high or intermediate anxiety levels during the first and second waves of the COVID-19 pandemic. Such findings may point to social support as a key protective factor against the adverse mental health issues caused by epidemics and natural disasters,65 especially in pregnant women.66,67 Accordingly, high perceived social support in Serbian pregnant women may be an essential coping re-source and a mechanism for maintaining psychological well-being under conditions of psychological burdens,68 as the COVID-19 pandemic is.
Also, our findings align with studies that reported increased social support during the COVID-19 pandemic perceived by pregnant women.19,69 On the contrary, it is significant to note that studies reported decreased social support for pregnant women during the COVID-19 pandemic.70–72 Based on such different findings, we noticed that the data about perceived social support in pregnant women during the COVID-19 pandemic is country-specific, similar to the data about maternal anxiety during the COVID-19. These differences can be explained and discussed from several aspects. On the one hand, the severity of lockdown measures, which vary between countries, may explain some of these differences. On the other hand, the socio-cultural peculiarities of each country also could explain this. The strong family bonding and support that pregnant women receive from their families and friends are emphasized when looking at Serbia, which was also evident in some other studies.60
Maternal Anxiety During Pregnancy During the First and Second Wave of COVID-19 in Serbia
The study revealed no pregnant women with low anxiety levels measured by STAI-T and STAI-S during the first and second pandemic waves in Serbia. Namely, the STAI-S and STAI-T scores indicated high anxiety in 32.4% and 42.7% of pregnant women, respectively. Also, there was no statistically significant difference comparing trait anxiety of pregnant women related to the first and second pandemic waves. All pregnant women were examined in the third trimester as the most sensitive period for manifesting high anxiety.73 Similar to our study results, numerous studies have been published recently, indicating an increase in anxiety symptoms in pregnant women during the COVID-19 pandemic.20,28,60,74–76 It is noticed that the data about maternal anxiety during the COVID-19 outbreak may be country-specific, pointing to the different prevalence of anxiety among pregnant women.77 Generally, the most recent systematic reviews and meta-analyses have shown that the prevalence of anxiety in pregnancy during COVID-19 ranges from 26% to 57%.31–33 Also, it was noticed that the prevalence varies to the continent and that western countries have a higher prevalence of anxiety in pregnant women (38%) than in Asian countries (7.8%),77 with similar findings for the general population as well.78
The phenomenon of increased anxiety during the COVID-19 pandemic was also observed in the general population.79 Accordingly, when analyzing the presence of elevated anxiety in the general population, Serbia has lower scores than respondents from Lebanon, Portugal, and Italy, pointing to a higher degree of resilience to psychological impacts from COVID-19 among Serbian respondents compared with those in mentioned countries.5 Comparing such findings with findings indicating elevated anxiety in pregnant women during the COVID-19 pandemic in Serbia,36,57,58 pregnant women are highlighted as a particularly vulnerable and sensitive group in the context of the COVID-19 pandemic, with higher anxiety levels compared to the general population.
In addition, the difference in anxiety levels in pregnant women during the first, second, or subsequent wave of the COVID-19 pandemic was investigated, with varying results indicating higher anxiety at the beginning of the COVID-19 pandemic and slighter decrease at the later waves and vice versa.76,80 We observed STAI-S be-cause of its variability over time.81
Correlation Between Maternal Age, STAI-S, STAI-T and MSPSS in the First and Second Collecting Period
Correlation between maternal age, STAI-S, STAI-T and MSPSS differs in the first and second collecting periods. It is evident that the relationship between STAI-S, STAI-T and MSPSS is complex and differs between the first and second pandemic waves. In the first pandemic wave, there is a negative correlation between maternal age, STAI-T and MSPSS, and for STAI-S and maternal age, it is also close to statistical significance (p=0.064). Pre-pandemic studies reported a strong correlation between age and anxiety in the general population, pointing to younger age associated with higher anxiety levels,79 which was confirmed during the COVID-19 pandemic.82 Interestingly, there is no statistically significant correlation between STAI-S and STAIT-T during the first collecting period. These findings may be further explained by the role of psychological and social changes in pregnant and postpartum women due to the burden imposed by the COVID-19 pandemic.83
In the second pandemic wave, the correlation between maternal age, STAI-T and MSPSS disappear, but a positive correlation between STAI-S and STAI-T, as well as STAI-S and MSPSS, and a negative correlation between STAI-T and MSPSS appear. Literature findings also indicate a weak positive correlation between STAI-S and STAI-T in pregnant women during the COVID-19 pandemic26 and a negative correlation between STAI-T and MSPSS.60,84 The negative correlation between higher levels of perceived social support and trait anxiety levels, which is a more expected finding in general, is in line with findings pointing to an association between higher levels of perceived social support and lower psychological symptoms in pregnant women.29,60,84 Also, considering the relation between anxiety and perceived social support, social support may have significant effects on anxiety and may be considered a potential therapeutic target for interventions in pregnant women.85 Social support has a direct negative influence on the anxiety level in pregnant women, which is consistent with previous studies.60,84 Some studies point to a small significant relationship between perceived social support and pregnant women’s anxiety during the COVID-19 pandemic.86 However, unlike the dominant studies indicating that social support was negatively linked with anxiety,87 the COVID-19 pandemic in Serbia, with all its characteristics, clearly indicates the positive relationship between the elevated state anxiety and perceived social support, as shown in our study. It can be noticed that the positive correlation between STAI-S and MSPSS is a somewhat surprising result, for the interpretation of which there is currently no sufficient amount of information. While the positive correlation between STAI-S and STAI-T observed in Serbia pregnant women during the COVID-19 pandemic has been noticed in the literature,26 and the negative correlation between trait anxiety and social support on the other side,60 the question of the weak positive correlation between state anxiety and social support is raised. A possible explanation could be the pregnant women´s prolonged period of social isolation during the second pandemic wave. This more extended isolation period, affecting pregnant women´s anxiety and family bonding relying on sociocultural peculiarities in Serbia,60 can lead to a different relationship between STAI-S and MSPSS, causing a weak positive correlation.
COVID-19 Related Fear in Pregnant Women During the First and Second Wave of COVID-19 in Serbia
Among crucial reasons that increase anxiety in pregnant women during the pandemic is the fear of COVID-19.88 Fear’s primary function is to respond to threatening situations.89 Fear to some extent has a defense mechanism leading people to comply with protective behaviors against COVID-19.90 The study results pointed to slight differences between the number of pregnant women concerning the presence of COVID-19 related fear. Although the most numerous is the group of pregnant women who reported that they have no COVID-19 related fear, the percentage of all three groups of women is approximate. Such findings align with findings indicating that individuals may respond differently to the emotional distress caused by traumatic events such as the COVID-19 pandemic.91 Also, they are not entirely in line with recent research conducted not on pregnant women, which showed that the COVID-19 pandemic might cause a significant long-lasting increase in fear,92,93 and with research pointing to a decrease in COVID-19 fear within six weeks from the pandemic outbreak.94
Univariate Analysis
None of the observed independent variables had a statistically significant influence on the model as the main effect, but statistically significant influences occurred through mutual two and three-way interactions. Data collection period appeared as a variable in three-way statistically significant interactions: Education * Data collecting period * COVID-19 related fear; Data collecting period * COVID-19 related fear * Employment. Observing the interactions between Education * COVID-19 related fear and COVID-19 related fear * Employment in the first and second collecting period, the different nature of these parameters’ influence on STAI-S can be observed. A clear interaction between the variables can be observed in the first collecting period, while there is no interaction in the second collecting period. In the second Data collection period, a certain regularity of influence of the parameters on STAI-S can be observed. Regardless of the personal level of the COVID-19 related fear, unemployed pregnant women and pregnant women with a higher level of education were more anxious than employed pregnant women and pregnant women with a lower level of education. The obtained results could be related to the fact that with time, the amount of information about the COVID-19 pandemic and its reliability enabled the formation of a clearer picture of possible risks, the course of the disease, and its consequences for certain pregnant women groups.
Regardless of the level of education and employment, the anxiety level of pregnant women decreased as the COVID-19 related fear increased. Our data pointed to the negative trend of maternal anxiety in the second data collecting period associated with COVID-19-related fear. The relationship between fear and anxiety of COVID-19 was examined,88 and it was pointed out that there is a positive correlation between fear and anxiety (r=0.6, p=0.001). The possible causes of the difference compared to our results are different methodologies of measuring fear, different measuring time points, and different anxiety measures. It should also be considered that there are divided opinions on whether fear and anxiety are distinct phenomena. At the same time, some authors describe fear and anxiety as undistinguishable, while others define them as distinct emotions.89 Our result can be related to the literature findings indicating that fear and anxiety are not interchangeable constructs on the one hand and, on the other, that fear captured significant variance in performance that was not shared with anxiety.95
The results of ONE-way ANOVA with new grouping variables of interaction terms indicated statistically significant differences between individual subgroups within the grouping variables. Subgroups of pregnant women with min and max logSTAI-S levels can be found in both collecting periods, so it cannot be concluded that the STAI-S level is higher or lower in the first than in the second collecting period. Results indicated the intricate interconnection of the observed variables in the first collecting period and the non-linearity of the observed phenomenon that was already mentioned.
Strengths and Limitations
This research was a rare opportunity to examine pregnant women’s anxiety during the COVID-19 pandemic, which had never been present before. Since limited studies have assessed maternal anxiety during the COVID-19 pandemic in Serbia, the present study was conducted to address this gap, relying on the fact that the data about maternal anxiety during the COVID-19 outbreak may be country-specific. On the other hand, the psychological burdens which occurred in pregnant women during the COVID-19 pandemic in Serbia point to psychological support needed for pregnant and postpartum women. The study was based on a cross-sectional data collection, carried out during two data collecting periods (first and second pandemic wave), and obtained results pointed to data collecting periods as part of the interactions which affect state anxiety in pregnant women. Accordingly, the findings from this study suggest that future targeted research is warranted to investigate better insight into the examination of interrelationships or contributions to the observed interactions. It is also important to point out that the specific conditions of the COVID-19 pandemic imply the implementation of various measures and restrictions to suppress its spread, which differed from country to country. Such burdens may affect maternal anxiety and the readiness of the sample to participate in the study. Accordingly, it is necessary to be careful when comparing the results of different studies on this issue, especially studies of different countries. We can assume that this may be the global impact of the pandemic.
Conclusion
The study revealed no pregnant women with low anxiety levels measured by STAI-S and STAI-T during the first and second pandemic waves in Serbia. The STAI-S and STAI-T scores indicated high anxiety in 32.4% and 42.7% of pregnant women, respectively.
The study also pointed out the complex nonlinear dependence of state anxiety on various factors, including the data collecting period. During the COVID-19 pandemic, we did not observe the independent influence of individual variables on STAI-S, but we noticed their impact through mutual interactions. Such findings indicate the complexity of interactions and their impacts on STAI-S. There is a difference in the influence of certain parameters in the first and second pandemic waves. While in the first wave, the interaction between the parameters is expressed, in the second, it is absent, and the pattern of the parameters’ influence on pregnant women’s anxiety is observed. The obtained results suggest that timely, precise, and reliable information in the conditions of a pandemic can contribute to the formation of a clearer picture of possible risks, the course of the disease, and its consequences in certain groups of pregnant women. This would enable greater predictability of the influence of certain parameters on the anxiety of pregnant women and, thus, adequate help and support for pregnant women who, even in conditions that are not burdened by the pandemic, have a higher level of anxiety.
Abbreviations
COVID-19, Coronavirus Disease 2019 caused by SARS-CoV-2 virus; SARS-CoV-2, Severe acute respiratory syndrome coronavirus 2; STAI, State-Trait Anxiety Inventory; MSPSS, Multidimensional Scale of Perceived Social Support; STAI-S, State anxiety measure; STAI-T, Trait anxiety measure.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Clinic for Gynecology and Obstetrics “Narodni Front” in Belgrade, Serbia (No 27/2020; Date: 26. March 2020). Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Acknowledgments
LJ and MSo are working members and management committee members of COST Action CA18211: DEVoTION: Perinatal Mental Health and Birth-Related Trauma: Maximizing best practice and optimal outcomes. This paper contributes to the EU COST Action 18211: DEVoTION.
Funding
This work was partially supported by the Ministry of Education, Science and Technological Development of the Republic of Serbia within the project “Influence of psychophysiological, sociological, and cultural factors on speech and language in the child population”. This project is realized in cooperation with the Faculty of Medical Sciences, University of Kragujevac, Serbia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mohan BS, Vinod N. COVID-19: an insight into SARS-CoV2 pandemic originated at Wuhan City in Hubei Province of China. J Infect Dis Epidemiol. 2020;6(4). doi:10.23937/2474-3658/1510146
2. Stasevic-Karlicic I, Djordjevic V, Stasevic M, et al. Perspectives on mental health services during the COVID-19 epidemic in Serbia. Srp Arh Celok Lek. 2020;148(5–6):379–382. doi:10.2298/sarh200504028s
3. Usher K, Durkin J, Bhullar N. The COVID-19 pandemic and mental health impacts. Int J Ment Health Nurs. 2020;29(3):315–318. doi:10.1111/inm.12726
4. Meyerowitz-Katz GA, Bhatt S, Ratmann O, et al. Is the cure really worse than the disease? The health impacts of lockdowns during COVID-19. BMJ Global Health. 2021;6(8):e006653. doi:10.1136/bmjgh-2021-006653
5. Öcal A, Cvetković VM, Baytiyeh H, Tedim FMS, Zečević M. Public reactions to the disaster COVID-19: a comparative study in Italy, Lebanon, Portugal, and Serbia. Geomat Natural Hazards Risk. 2020;11(1):1864–1885. doi:10.1080/19475705.2020.1811405
6. Ortony A, Turner TJ. What’s basic about basic emotions? Psychol Rev. 1990;97(3):315–331. doi:10.1037/0033-295X.97.3.315
7. Tuma AH, Maser JD. Anxiety and the Anxiety Disorders. Routledge; 2019.
8. Sartori SB, Landgraf R, Singewald N. The clinical implications of mouse models of enhanced anxiety. Future Neurol. 2011;6(4):531–571. doi:10.2217/fnl.11.34
9. King NJ, Hamilton DJ, Hamilton DI, Ollendick TH. Children’s Phobias: A Behavioral Perspective. Wiley; 1988.
10. Sylvers P, LaPrairie JL, LaPrairie JL. Differences between trait fear and trait anxiety: implications for psychopathology. Clin Psychol Rev. 2011;31(1):122–137. doi:10.1016/j.cpr.2010.08.004
11. Vitasari P, Wahab MNA, Herawan T, Othman A, Sinnadurai SK. Re-test of State Trait Anxiety Inventory (STAI) among engineering students in Malaysia: reliability and validity tests. Procedia. 2011;15:3843–3848. doi:10.1016/j.sbspro.2011.04.383
12. Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. State-Trait Anxiety Inventory for Adults. Consulting Psychologists Press Inc.; 1983.
13. Taylor SE. Social support: a review. 2011.
14. Liu H, Li S, Xiao Q, Feldman M. Social support and psychological well-being under social change in urban and rural China. Soc Indic Res. 2014;119(2):979–996. doi:10.1007/s11205-013-0534-1
15. Api O, Sen C, Debska M, et al. Clinical management of coronavirus disease 2019 (COVID-19) in pregnancy: recommendations of WAPM-World Association of Perinatal Medicine. J Perinat Med. 2020;48(9):857–866. doi:10.1515/jpm-2020-0265
16. Smith V, Seo D, Warty R, et al. Maternal and neonatal outcomes associated with COVID-19 infection: a systematic review. PLoS One. 2020;15(6):e0234187. doi:10.1371/journal.pone.0234187
17. Vergara-Merino L, Meza N, Couve-Pérez C, et al. Maternal and perinatal outcomes related to COVID-19 and pregnancy: an overview of systematic reviews. Acta Obstet Gynecol Scand. 2021;100(7):1200–1218. doi:10.1111/aogs.14118
18. Motrico E, Bina R, Domínguez-Salas S, et al. Impact of the Covid-19 pandemic on perinatal mental health (Riseup-PPD-COVID-19): protocol for an international prospective cohort study. BMC Public Health. 2021;21(1):368. doi:10.1186/s12889-021-10330-w
19. Hashim M, Coussa A, Al Dhaheri AS, et al. Impact of coronavirus 2019 on mental health and lifestyle adaptations of pregnant women in the United Arab Emirates: a cross-sectional study. BMC Pregnancy Childbirth. 2021;21(1):515. doi:10.1186/s12884-021-03941-z
20. Yan H, Ding Y, Guo W. Mental health of pregnant and postpartum women during the coronavirus disease 2019 pandemic: a systematic review and meta-analysis. Syst Rev Front Psychol. 2020;11:115.
21. Sahin D, Tanacan A, Anuk AT, et al. Comparison of clinical features and perinatal outcomes between pre-variant and post-variant periods in pregnant women with SARS-CoV-2: analysis of 1935 cases. Arch Gynecol Obstet. 2022;2022:1–10.
22. Şahin D, Tanaçan A, Webster SN, Tekin ÖM. Pregnancy and COVID-19: prevention, vaccination, therapy, and beyond. Turk J Med Sci. 2021;51(7):3312–3326. doi:10.3906/sag-2106-134
23. Chinchilla-Ochoa DA, Barriguete-Chávez Peón P, Farfán-Labonne BE, Garza-Morales S, Leff-Gelman PA, Flores-Ramos M. Depressive symptoms in pregnant women with high trait and state anxiety during pregnancy and postpartum. Int J Womens Health. 2019;11:257. doi:10.2147/IJWH.S194021
24. Hamzehgardeshi Z, Omidvar S, Amoli AA, Firouzbakht M. Pregnancy-related anxiety and its associated factors during COVID-19 pandemic in Iranian pregnant women: a web-based cross-sectional study. BMC Pregnancy Childbirth. 2021;21(1):208. doi:10.1186/s12884-021-03694-9
25. Asmundson GJG, Taylor S. How health anxiety influences responses to viral outbreaks like COVID-19: what all decision-makers, health authorities, and health care professionals need to know. J Anxiety Disord. 2020;71:102211. doi:10.1016/j.janxdis.2020.102211
26. Mappa I, Distefano FA, Rizzo G. Effects of coronavirus 19 pandemic on maternal anxiety during pregnancy: a prospectic observational study. J Perinat Med. 2020;48(6):545–550. doi:10.1515/jpm-2020-0182
27. Saccone G, Florio A, Aiello F, et al. Psychological impact of coronavirus disease 2019 in pregnant women. Am J Obstet Gynecol. 2020;223(2):293–295. doi:10.1016/j.ajog.2020.05.003
28. Moyer CA, Compton SD, Kaselitz E, Muzik M. Pregnancy-related anxiety during COVID-19: a nationwide survey of 2740 pregnant women. Archiv Womens Ment Health. 2020;23(6):757–765. doi:10.1007/s00737-020-01073-5
29. Lebel C, MacKinnon A, Bagshawe M, Tomfohr-Madsen L, Giesbrecht G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J Affect Disord. 2020;277:5–13. doi:10.1016/j.jad.2020.07.126
30. Durankuş F, Aksu E. Effects of the COVID-19 pandemic on anxiety and depressive symptoms in pregnant women: a preliminary study. J Matern Fetal Neonat Med. 2020;18:1–7.
31. Sun F, Zhu J, Tao H, Ma Y, Jin W. A systematic review involving 11,187 participants evaluating the impact of COVID-19 on anxiety and depression in pregnant women. J Psychosomat Obstetr Gynecol. 2021;42(2):91–99. doi:10.1080/0167482X.2020.1857360
32. Tomfohr-Madsen LM, Racine N, Giesbrecht GF, Lebel C, Madigan S. Depression and anxiety in pregnancy during COVID-19: a rapid review and meta-analysis. Psychiatry Res. 2021;300:113912. doi:10.1016/j.psychres.2021.113912
33. Fan S, Guan J, Cao L, et al. Psychological effects caused by COVID-19 pandemic on pregnant women: a systematic review with meta-analysis. Asian J Psychiatr. 2021;56:102533. doi:10.1016/j.ajp.2020.102533
34. Zilver SJM, Broekman BFP, Hendrix YM, et al. Stress, anxiety and depression in 1466 pregnant women during and before the COVID-19 pandemic: a Dutch cohort study. J Psychosomat Obstetr Gynecol. 2021;42(2):108–114. doi:10.1080/0167482X.2021.1907338
35. Ceulemans M, Hompes T, Foulon V. Mental health status of pregnant and breastfeeding women during the COVID-19 pandemic: a call for action. Int J Gynecol Obstetr. 2020;151(1):146–147. doi:10.1002/ijgo.13295
36. Tutnjević S, Lakić S. Psychological impact of the COVID-19 pandemic on pregnant women in Bosnia and Herzegovina and Serbia. 2020.
37. Stankovic M, Stojanovic A, Jelena S, Stankovic M, Shih A, Stankovic S. The Serbian experience of challenges of parenting children with autism spectrum disorders during the COVID-19 pandemic and the state of emergency with lockdown. Eur Child Adolesc Psychiatry. 2022;31(4):693–698. doi:10.1007/s00787-021-01917-0
38. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
39. Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. Priručnik za Upitnik anksioznosti kao stanja i osobine ličnosti [State-Trait Anxiety Inventory (Form Y)]. Naklada Slap; 2000.
40. Kayikcioglu O, Bilgin S, Seymenoglu G, Deveci A. State and trait anxiety scores of patients receiving intravitreal injections. Biomed Hub. 2017;2(2):1–5. doi:10.1159/000478993
41. Julian LJ. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (Hads-A). Arthritis Care Res. 2011;63(11):467–472. doi:10.1002/acr.20561
42. Özpelit ME, Özpelit E, Doğan NB, et al. Impact of anxiety level on circadian rhythm of blood pressure in hypertensive patients. Int J Clin Exp Med. 2015;8(9):16252–16258.
43. Mappa IA, Luviso MA, Distefano FA, Carbone LA, Maruotti GM, Rizzo GA. Women perception of SARS-CoV-2 vaccination during pregnancy and subsequent maternal anxiety: a prospective observational study. J Matern Fetal Neonatal Med. 2021;2021:1–4.
44. Todorovic ST, Hanna F, Boskovic K, Filipovic D, Vidovic V, Filipovic K. Motor ability and emotions in rheumatoid arthritis patients. J Neurol Neurophysiol. 2012;03(05). doi:10.4172/2155-9562.1000137
45. Candelori C, Trumello C, Babore A, Keren M, Romanelli R. The experience of premature birth for fathers: the application of the Clinical Interview for Parents of High-Risk Infants (CLIP) to an Italian sample. Front Psychol. 2015;6:1444. doi:10.3389/fpsyg.2015.01444
46. Pejičić M, Ristić M, Anđelković V. The mediating effect of cognitive emotion regulation strategies in the relationship between perceived social support and resilience in postwar youth. J Community Psychol. 2018;46(4):457–472. doi:10.1002/jcop.21951
47. Carlsson I-M, Ziegert K, Nissen E. The relationship between childbirth self-efficacy and aspects of well-being, birth interventions and birth outcomes. Midwifery. 2015;31(10):1000–1007. doi:10.1016/j.midw.2015.05.005
48. Baguley T. Understanding statistical power in the context of applied research. Appl Ergon. 2004;35(2):73–80. doi:10.1016/j.apergo.2004.01.002
49. Hoenig JM, Heisey DM. The abuse of power. Am Stat. 2001;55(1):19–24. doi:10.1198/000313001300339897
50. Onwuegbuzie AJ, Leech NL. Post hoc power: a concept whose time has come. Understand Stat. 2004;3(4):201–230. doi:10.1207/s15328031us0304_1
51. Prati G, Mancini A. The psychological impact of COVID-19 pandemic lockdowns: a review and meta-analysis of longitudinal studies and natural experiments. Psychological Med. 2021;51(2):201–211. doi:10.1017/S0033291721000015
52. Sanchez-Ramirez DC, Normand K, Zhaoyun Y, Torres-Castro R. Long-term impact of COVID-19: a systematic review of the literature and meta-analysis. Biomedicines. 2021;9(8). doi:10.3390/biomedicines9080900
53. Robinson E, Sutin AR, Daly M, Jones A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J Affect Disord. 2022;296:567–576. doi:10.1016/j.jad.2021.09.098
54. Fischer R, Bortolini T, Karl JA, et al. Rapid review and meta-meta-analysis of self-guided interventions to address anxiety, depression, and stress during COVID-19 social distancing. Syst Rev Front Psychol. 2020;11:100.
55. Rafiq D, Batool A, Bazaz MA. Three months of COVID-19: a systematic review and meta-analysis. Rev Med Virol. 2020;30(4):e2113. doi:10.1002/rmv.2113
56. Sharifi-Heris Z, Moghasemi S, Ghamsary M, Moodi S, Ghprbani Z, Amiri-Farahani L. Perceived risk of COVID-19 acquisition and maternal mental distress. Br J Midwifery. 2021;29(3):140–149. doi:10.12968/bjom.2021.29.3.140
57. Stojanov J, Stankovic M, Zikic O, Stankovic M, Stojanov A. The risk for nonpsychotic postpartum mood and anxiety disorders during the COVID-19 pandemic. Int J Psychiatry Med. 2021;56(4):228–239. doi:10.1177/0091217420981533
58. Jeličić L, Sovilj M, Bogavac I, et al. The impact of maternal anxiety on early child development during the COVID-19 pandemic. Front Psychol. 2021;12:792053. doi:10.3389/fpsyg.2021.792053
59. Gao L-L, Sun K, Chan SW. Social support and parenting self-efficacy among Chinese women in the perinatal period. Midwifery. 2014;30(5):532–538. doi:10.1016/j.midw.2013.06.007
60. Yue C, Liu C, Wang J, et al. Association between social support and anxiety among pregnant women in the third trimester during the coronavirus disease 2019 (COVID-19) epidemic in Qingdao, China: the mediating effect of risk perception. Int J Soc Psychiatry. 2020;67(2):120–127. doi:10.1177/0020764020941567
61. Lefkovics E, Rigó J, Kovács I, et al. Effect of maternal depression and anxiety on mother’s perception of child and the protective role of social support. J Reprod Infant Psychol. 2018;36(4):434–448. doi:10.1080/02646838.2018.1475726
62. Milgrom J, Hirshler Y, Reece J, Holt C, Gemmill AW. Social support-a protective factor for depressed perinatal women? Int J Environ Res Public Health. 2019;16(8):1426. doi:10.3390/ijerph16081426
63. Nath A, Venkatesh S, Balan S, Metgud CS, Krishna M, Murthy GVS. The prevalence and determinants of pregnancy-related anxiety amongst pregnant women at less than 24 weeks of pregnancy in Bangalore, Southern India. Int J Womens Health. 2019;11:241–248. doi:10.2147/IJWH.S193306
64. Kuipers Y, Bleijenbergh R, Van den Branden L, et al. Psychological health of pregnant and postpartum women before and during the COVID-19 Pandemic. PLoS One. 2022;17(4):e0267042. doi:10.1371/journal.pone.0267042
65. Bonanno GA, Ho SMY, Chan JCK, et al. Psychological resilience and dysfunction among hospitalized survivors of the SARS epidemic in Hong Kong: a latent class approach. Health Psychol. 2008;27(5):659–667. doi:10.1037/0278-6133.27.5.659
66. Almeida M, Shrestha AD, Stojanac D, Miller LJ. The impact of the COVID-19 pandemic on women’s mental health. Archiv Womens Ment Health. 2020;23(6):741–748. doi:10.1007/s00737-020-01092-2
67. Khoury JE, Atkinson L, Bennett T, Jack SM, Gonzalez A. COVID-19 and mental health during pregnancy: the importance of cognitive appraisal and social support. J Affect Disord. 2021;282:1161–1169. doi:10.1016/j.jad.2021.01.027
68. Bruwer B, Emsley R, Kidd M, Lochner C, Seedat S. Psychometric properties of the multidimensional scale of perceived social support in youth. Compr Psychiatry. 2008;49(2):195–201. doi:10.1016/j.comppsych.2007.09.002
69. García-Fernández R, Liébana-Presa C, Marqués-Sánchez P, Martínez-Fernández MC, Calvo-Ayuso N, Hidalgo-Lopezosa P. Anxiety, stress, and social support in pregnant women in the Province of Leon during COVID-19 disease. Healthcare. 2022;10(5). doi:10.3390/healthcare10050791
70. Zhou J, Havens KL, Starnes CP, et al. Changes in social support of pregnant and postnatal mothers during the COVID-19 pandemic. Midwifery. 2021;103:103162. doi:10.1016/j.midw.2021.103162
71. Matvienko-Sikar K, Pope J, Cremin A, et al. Differences in levels of stress, social support, health behaviours, and stress-reduction strategies for women pregnant before and during the COVID-19 pandemic, and based on phases of pandemic restrictions, in Ireland. Women Birth. 2021;34(5):447–454. doi:10.1016/j.wombi.2020.10.010
72. Meaney S, Leitao S, Olander EK, Pope J, Matvienko-Sikar K. The impact of COVID-19 on pregnant womens’ experiences and perceptions of antenatal maternity care, social support, and stress-reduction strategies. Women Birth. 2022;35(3):307–316. doi:10.1016/j.wombi.2021.04.013
73. Silva MMJ, Nogueira DA, Clapis MJ, Leite E. Anxiety in pregnancy: prevalence and associated factors. Revista da Escola de Enfermagem da USP. 2017;51:e03253. doi:10.1590/s1980-220x2016048003253
74. Ayaz R, Hocaoğlu M, Günay T, Yardımcı OD, Turgut A, Karateke A. Anxiety and depression symptoms in the same pregnant women before and during the COVID-19 pandemic. J Perinat Med. 2020;48(9):965–970. doi:10.1515/jpm-2020-0380
75. Corbett GA, Milne SJ, Hehir MP, Lindow SW, O’Connell MP. Health anxiety and behavioural changes of pregnant women during the COVID-19 pandemic. Eur J Obstet Gynecol. 2020;249:96–97. doi:10.1016/j.ejogrb.2020.04.022
76. Makara-Studzińska M, Zaręba K, Kawa N, Matuszyk D. Tokophobia and anxiety in pregnant women during the SARS-CoV-2 pandemic in Poland—a prospective cross-sectional study. Int J Environ Res Public Health. 2022;19(2):714. doi:10.3390/ijerph19020714
77. Ghazanfarpour M, Bahrami F, Rashidi Fakari F, et al. Prevalence of anxiety and depression among pregnant women during the COVID-19 pandemic: a meta-analysis. J Psychosomat Obstetr Gynecol. 2021;1–12. doi:10.1080/0167482X.2021.1929162
78. Liu Y, Wang D, Xu H, et al. Public knowledge of novel coronavirus diseases 2019: a web-based national survey. Res Square. 2020. doi:10.21203/rs.3.rs-28163/v1
79. Filindassi V, Pedrini C, Sabadini C, Duradoni M, Guazzini A. Impact of COVID-19 first wave on psychological and psychosocial dimensions: a systematic review. COVID. 2022;2(3):273–340. doi:10.3390/covid2030022
80. López-Morales H, del-Valle MV, Andrés ML, Gelpi Trudo R, Canet-Juric L, Urquijo S. Longitudinal study on prenatal depression and anxiety during the COVID-19 pandemic. Archiv Womens Ment Health. 2021;24(6):1027–1036. doi:10.1007/s00737-021-01152-1
81. Floris L, Irion O, Courvoisier D. Influence of obstetrical events on satisfaction and anxiety during childbirth: a prospective longitudinal study. Psychol Health Med. 2017;22(8):969–977. doi:10.1080/13548506.2016.1258480
82. Shevlin M, McBride O, Murphy J, et al. Anxiety, depression, traumatic stress and COVID-19-related anxiety in the UK general population during the COVID-19 pandemic. BJPsych Open. 2020;6(6):
83. Fallon V, Davies SM, Silverio SA, Jackson L, De Pascalis L, Harrold JA. Psychosocial experiences of postnatal women during the COVID-19 pandemic. A UK-wide study of prevalence rates and risk factors for clinically relevant depression and anxiety. J Psychiatr Res. 2021;136:157–166. doi:10.1016/j.jpsychires.2021.01.048
84. Karimi L, Makvandi S, Mahdavian M, Khalili R. Relationship between social support and anxiety caused by COVID-19 in pregnant women. Iran J Obstetr Gynecol Infertil. 2021;23(10):9–17.
85. Harrison V, Moulds ML, Jones K. Perceived social support and prenatal wellbeing; The mediating effects of loneliness and repetitive negative thinking on anxiety and depression during the COVID-19 pandemic. Women Birth. 2022;35(3):232–241. doi:10.1016/j.wombi.2020.12.014
86. Behmard V, Bahri N, Mohammadzadeh F, Noghabi AD, Bahri N. Relationships between anxiety induced by COVID-19 and perceived social support among Iranian pregnant women. J Psychosomat Obstetr Gynecol. 2021;2021:1–8.
87. Grumi S, Provenzi L, Accorsi P, et al. Depression and anxiety in mothers who were pregnant during the COVID-19 outbreak in Northern Italy: the role of pandemic-related emotional stress and perceived social support. Original research. Front Psychiatry. 2021;12. doi:10.3389/fpsyt.2021.716488
88. Salehi L, Rahimzadeh M, Molaei E, Zaheri H, Esmaelzadeh-Saeieh S. The relationship among fear and anxiety of COVID-19, pregnancy experience, and mental health disorder in pregnant women: a structural equation model. Brain Behav. 2020;10(11):e01835. doi:10.1002/brb3.1835
89. Steimer T. The biology of fear- and anxiety-related behaviors. Dialogues Clin Neurosci. 2002;4(3):231–249. doi:10.31887/DCNS.2002.4.3/tsteimer
90. Yıldırım M, Geçer E, Akgül Ö. The impacts of vulnerability, perceived risk, and fear on preventive behaviours against COVID-19. Psychol Health Med. 2021;26(1):35–43. doi:10.1080/13548506.2020.1776891
91. Killgore WDS, Cloonan SA, Taylor EC, Dailey NS. Mental health during the first weeks of the COVID-19 pandemic in the United States. Original research. Front Psychiatry. 2021;12. doi:10.3389/fpsyt.2021.561898
92. Skoda E-M, Bäuerle A, Schweda A, et al. Severely increased generalized anxiety, but not COVID-19-related fear in individuals with mental illnesses: a population based cross-sectional study in Germany. Int J Soc Psychiatry. 2021;67(5):550–558. doi:10.1177/0020764020960773
93. Andrade EF, Pereira LJ, Oliveira AP, et al. Perceived fear of COVID-19 infection according to sex, age and occupational risk using the Brazilian version of the fear of COVID-19 scale. Death Stud. 2022;46(3):533–542. doi:10.1080/07481187.2020.1809786
94. Hetkamp M, Schweda A, Bäuerle A, et al. Sleep disturbances, fear, and generalized anxiety during the COVID-19 shut down phase in Germany: relation to infection rates, deaths, and German stock index DAX. Sleep Med. 2020;75:350–353. doi:10.1016/j.sleep.2020.08.033
95. Perkins AM, Kemp SE, Corr PJ. Fear and anxiety as separable emotions: an investigation of the revised reinforcement sensitivity theory of personality. Emotion. 2007;7(2):252. doi:10.1037/1528-3542.7.2.252
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Anxiety and Depression Among HIV-Positive and HIV-Negative Pregnant Women During COVID-19 Pandemic in Ekiti State, Southwest Nigeria
Ade-Ojo IP, Dada MU, Adeyanju TB
International Journal of General Medicine 2022, 15:4123-4130
Published Date: 16 April 2022
The Relationship Between Negative Life Events and Nonsuicidal Self-Injury Among Chinese Adolescents: A Moderated-Mediation Model
Zhang Y, Suo X, Zhang Y, Zhang S, Yang M, Qian L, Shang L, Zhang D, Xu F, Li W
Neuropsychiatric Disease and Treatment 2022, 18:2881-2890
Published Date: 14 December 2022
Factors Predicting Mental Health Among Women in Low-Income Communities of a Changing Society: A Mixed-Methods Study
Roberts LR, Sadan V, Siva R, Sathiyaseelan M, Rosalind SE, Suresh P, Montgomery SB
International Journal of Women's Health 2023, 15:381-394
Published Date: 16 March 2023
How Do Anxiety and Relationship Factors Influence the Application of Childbirth Education Strategies During Labor and Birth: A Bowen Family Systems Perspective
Sutcliffe KL, Levett K, Dahlen HG, Newnham E, MacKay LM
International Journal of Women's Health 2023, 15:455-465
Published Date: 1 April 2023
The Interconnection Between Social Support and Emotional Distress Among Individuals with Chronic Pain: A Narrative Review
Franqueiro AR, Yoon J, Crago MA, Curiel M, Wilson JM
Psychology Research and Behavior Management 2023, 16:4389-4399
Published Date: 27 October 2023