Back to Journals » International Journal of Women's Health » Volume 15
How Do Anxiety and Relationship Factors Influence the Application of Childbirth Education Strategies During Labor and Birth: A Bowen Family Systems Perspective
Authors Sutcliffe KL ![]() , Levett K, Dahlen HG, Newnham E, MacKay LM
, Levett K, Dahlen HG, Newnham E, MacKay LM
Received 5 December 2022
Accepted for publication 24 March 2023
Published 1 April 2023 Volume 2023:15 Pages 455—465
DOI https://doi.org/10.2147/IJWH.S399588
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Kerry L Sutcliffe,1 Kate Levett,1– 3 Hannah G Dahlen,4 Elizabeth Newnham,5 Linda M MacKay6
1School of Medicine, University of Notre Dame Australia, Sydney, NSW, Australia; 2Adjunct Fellow, NICM Health Research Institute, and THRI, Western Sydney University, Sydney, NSW, Australia; 3Honorary Fellow, Centre for Midwifery, Child and Family Health, University of Technology Sydney, Sydney, NSW, Australia; 4School of Nursing & Midwifery, Western Sydney University, Sydney, NSW, Australia; 5School of Nursing & Midwifery, University of Newcastle, Newcastle, NSW, Australia; 6School of Arts & Sciences, University of Notre Dame Australia, Sydney, NSW, Australia
Correspondence: Kerry L Sutcliffe, School of Medicine, University of Notre Dame Australia, Auburn Clinical School, 88-90 Water Street, Auburn, Sydney, NSW, 2144, Australia, Tel +61 451771723, Email [email protected]
Abstract: The effectiveness of childbirth education (CBE) has long been debated with studies showing contradictory outcomes for mothers and babies. Understanding how what is learned in CBE is translated into practice during labor and birth is an area that requires investigation as this may be a mediating factor in its effectiveness. Bowen family system theory’s concept of differentiation of self, the ability to be guided by and to act from one’s beliefs and values, is an organizing principle that may affect how relational factors affect the use and application of CBE at the time of birth. The ability to act with emotional maturity when faced with a stressor, such as childbirth, depends on an individual’s capability to separate thoughts from the more reactive feeling process. Recognizing how one’s level of differentiation interacts with the anxious responses of others may assist pregnant women and birth partners to make decisions more objectively about how they want to manage the birthing process. For the health professional, understanding the interplay of relationship variables, physiological stress, anxiety and individual reactivity may allow for the provision of more thoughtful evidence-based practice, which may increase objectivity, and aid communication and decision-making for women during birth. Bowen theory, as a comprehensive systems-based approach to understanding human functioning under stress, offers a novel approach to exploring the application of CBE during birth.
Keywords: antenatal education, Bowen family systems, anxiety, human functioning, birth partner, relationship factors
Introduction
Part of the purpose of childbirth education, according to the Australian Clinical Practice Guidelines, is to generate confidence in a woman’s ability to give birth, prepare her for the pain of labor, and support her ability to give birth without pain relief.1 A recent systematic review showed that childbirth education can reduce maternal stress, improve self-efficacy, decrease the use of epidural anesthesia and lower the rates of caesarean sections.2 However, childbirth education differs widely and trials assessing its effectiveness and the usefulness of specific components show contradictory outcomes.2–4 There is a paucity of research looking at how childbirth education strategies, such as education about the physiological birth process and teaching of non-pharmacological pain relief techniques, are translated into practice during labor and birth.5 Furthermore, the support of birth partners and care-providers can be both an enabler and a barrier to childbirth education,5 highlighting the mediating effect relationship factors may have on the effectiveness of CBE.
Shared decision-making is touted as a cornerstone of ethical care, providing opportunity for high-quality and personalized care. Despite this, Villarmea and Kelly raised questions about the effect of dynamics in the birth room that may undermine true shared decision-making.6 They state how decisions in maternity care “are framed in terms of the ‘individual’ pregnant woman not at organizational level, which is where reality operates” (p516), and that a woman’s participation in decision-making while in labor has been undermined by discriminatory narratives throughout history that suggest women are less able to reason.6 Reed reflects on the “Herstory” of birth, discussing how underlying cultural and religious beliefs in the past have resulted in the modern approach to maternity care being centered around the needs of patriarchal institutions rather than women,7 which may impact how a woman decides to manage her labor.
Furthermore, the language used by clinicians is often too complex for any non-clinically trained person to understand, is underpinned by a philosophy of medical dominance, and as identified in Newnham et al’s ethnographic study of epidurals and waterbirth is biased towards the medical management of birth.8 This in turn influences the practices of care-providers, the information that the birthing woman and her birthing support partner(s) are presented with, and the decisions and choices she makes.8 Much of the health promotion literature targets individual-level attitudes and behaviors,9 without ever taking into account the up-stream stressors such as those that may exist within the organizational culture,10 the demanding workloads of staff,11 or any fear of litigation faced by clinicians.12 Additionally, healthcare staff’s ability to provide good leadership during anxious circumstances requires a balancing of emotions and intellect.13
A woman in labor who plans to utilize childbirth education strategies is therefore subject to influences that go well beyond her individual circumstances and reflect wider systemic issues.14 It has been noted that attitudes of staff and the impact of hospital policies can negate the effects of childbirth education, with obstetric management potentially derailing any effects childbirth education may have, thus rendering it meaningless.15 There is a mistaken belief that women who attend CBE will be treated the same by maternity staff as those who do not, meaning any differences seen in research outcomes can only be attributable to the education they receive in preparation for birth. Yet additional factors, such as pressures on the maternity system in relation to personnel, resources and regulatory requirements may inhibit women having choice and control over how they manage their births, given that the maternity system remains increasingly geared towards medical interventions that attempt to manage labor.14
Research therefore needs to investigate not only women’s and birth partners’ use of childbirth education but also the care-provider’s attitudes towards it and the way it is implemented in the system. Exploring individual characteristics and relational dynamics of those present at birth, as well as at all levels of maternity care and management, provides an important opportunity to uncover barriers and enablers to improving the implementation and integration of current childbirth education.
Bowen theory uses systems thinking to describe the interactions taking place between people and how this impacts functioning, specifically one’s ability to act more thoughtfully, even when facing physical, emotional and relational stressors.16 The purpose of this article therefore is to explore the theoretical framework of Bowen family systems theory as a way of understanding human functioning under stress and how it influences the application of childbirth education strategies in labor. It may well be relevant to include a component of psycho-education that pertains to understanding how stress and relational variables play a part in any person’s best attempts to implement the interventions provided via CBE. What follows in this paper is an exploration of Bowen theory as a theoretical perspective to explore how and why CBE translates into practice. It focuses on Bowen theory’s main concept relating to an individual’s differentiation of self and will be followed by delving into family functioning and fusion when considering the role that others play in implementing CBE strategies.
Bowen Family Systems Theory as a Theoretical Framework
Bowen observed how humans have instinctive reactions to others that are driven by physiological and biological responses, and considered people as part of their environment rather than separate from it.17,18 As a systems-based theory of human behavior, it asserts that rather than thinking in “cause and effect” terms, individuals would benefit from identifying interrelationships in groups, not focusing on the parts alone.19 It describes family members as living under the same “emotional skin”, meaning members are interdependent due to the connectedness and reactivity between them; when there is a change in one person’s functioning, it is predictably followed by reciprocal changes in the functioning of those around them.20 The level of interdependence that families experience will differ, but it always exists to some degree.
Whilst the focus of this paper is on the family and maternity system, “Bowen family system” theory as a theoretical framework posits that all individuals are embedded within interlocking systems of influence, whether relational, professional, organizational, social, political, religious, and cultural, etc., although the most influential of these is the family. Responsiveness to others is not limited to nuclear family relationships,17 theoretically, all that is needed to create an emotional system is people spending enough time together.19 There are a number of family systems – nuclear/family of origin, maternity and Bowen – which are referred to in this paper and visually represented in Figure 1.
 |
Figure 1 A three-system approach. |
All concepts in Bowen theory are linked by the presence of, and the family’s reaction to, heightened anxiety. Level of anxiety relates to an emotional response to any threat whether real or perceived.21 When there are low levels of anxiety present, relationships appear “symptom-free”, but when tension arises symptoms of anxiety present themselves and can impede the ability of one person to function more independently. Having a baby can add additional stress and anxiety to many mothers and birth partners during pregnancy and in the lead up to birth. Situations that could generate further anxiety during labor include tension between the couple; inadequate focus on the mother’s needs; self-doubt within the mother regarding her capacity to give birth; staffing issues, staff sickness; ratios failing to include babies in staffing quotas impacting workload; dominant medical discourse over midwifery-led care and physiological approaches to birth; as well as medical emergencies. Chronic anxiety reflects a constant underlying level of worry someone feels; conversely, it may be barely felt, but is triggered by threats to relational harmony (for example, the worry about upsetting someone, not being approved of, or of meeting expectations) and the fear of what might be,17 such as how they will cope during labor or the outcome of birth. In contrast, acute anxiety manifests in moments of fear that occur at a specific time and triggers the actions of the sympathetic nervous system when the threat is a real one, and has the potential to be life-threatening or to cause harm.22 Anxiety felt by an individual whether chronic or acute, real or imagined, can then spread throughout the family system and beyond it into other relationships and systems.
High levels of anxiety in pregnant women have been linked to increased likelihood of requesting pain medication,23 prolonged labor,24 and operative births.25 With regard to fathers, research indicates that the prevalence and level of anxiety increases during the antenatal period, peaks at the time of birth before decreasing again in the postnatal period,26 and they report feeling anxious about witnessing their partner in pain during labor.27 Further to this, fathers’ experiences of maternity care services has seen them described in the qualitative literature as “not-patient and not-visitor”28 and side-lined during labor by midwives.29 Being in this interstitial and undefined space despite feeling like a partner and a parent, leaves many fathers feeling increasingly fearful and excluded.28,29 Care-providers are not exempt from anxiety either. Despite working with birth on a daily basis, and perhaps because of it, extensive research has shown that healthcare professionals are vulnerable to emotional suffering due to the empathic role they play. The high degree of empathic care that is characteristic of the midwife–woman relationship puts midwives at risk of issues such as compassion fatigue, secondary traumatic stress30 and burnout.31 This potentially risks the midwife’s own mental health and also their capacity to provide care to future birthing women. Furthermore, healthcare workers’ anxiety of the prospect of litigation has been suggested as contributing to defensive medical practice and increased interventions.32,33 When someone experiences heightened anxiety, their nervous system reacts in a way that overwhelms their capacity for objective thinking and leads to a greater likelihood of behaving in a way concordant with their fears.34 How birth partners and care-providers support the use of CBE during times of heightened emotions and how this interacts with a woman’s own response to anxious feelings is unknown.
Using Bowen Theory to Explore the Relational Factors Influencing the Use of CBE Strategies During Birth
The Concept of “Differentiation of Self”
Within Bowen theory, a person’s response to this heightened anxiety depends on an individual’s level of self-differentiation.13 This critical concept of “differentiation of self” is defined as the degree to which one is able to balance 1) emotional and intellectual functioning and 2) intimacy and autonomy in relationships.35 It is the capacity to separate thoughtful, goal-directed responses from emotional, reactive ones. Of note, it is the relative separation of emotional and intellectual functioning that determines differentiation of self, the two can never completely be separated from one another. It conveys a person’s ability to self-regulate and problem solve,36 the level of which determines how effectively they function in life.13 According to Bowen Theory, how an individual reacts in the face of stressors, real or imagined, reveals a more accurate level of differentiation.13 Figure 2 shows some of the main characteristics of low and high differentiation of self. Someone with lower differentiation (left of Figure 2) reacts more emotionally during anxious times, someone with higher differentiation (right of Figure 2) is more resilient during anxiety provoking events.13
 |
Figure 2 Differentiation of self: main attributes of low and high differentiated functioning. |
While Keller describes this concept for people in general, if we consider how a woman might perceive her own role during labor, a higher degree of differentiation of self is associated with a stronger internal locus of control.37 A woman with a greater level of differentiation according to Bowen Theory, would have well-developed goals, a strong internal locus of control, and a “general imperviousness to the praise or criticism of others” (Keller et al, p.41).37 Furthermore, they do not require others in order to function themselves, despite also being aware of their degree of dependence on other people. This ensures they can engage in intense relationships and have a deep respect for someone else, without feeling the need to modify their own or others’ behavior.37 Steelman examined Bowen theory’s differentiation of self and relationship factors on married women’s mental health, concluding that psychological well-being was attributable to interdependence and the perception of emotional and interactional needs being met.38 Responses to stressful events, however, have an impact on the ability of any individual to stay more thoughtful, especially when exposed to overwhelming events that persist over time. Pregnancy and the upcoming birth (and subsequent raising of a child) could be considered overwhelming. The impact of financial strain, demanding workloads, illness, abuse, past trauma, systemic racism, migration, mental health issues, the experience of isolation caused by Covid-19, family history, just to name a few stressors, will also put strain on most individuals and their families, which may well persist for years and into future generations, albeit less in conscious awareness.37
During labor, the most likely family member providing support is the woman’s chosen birth partner, which is often their significant other, but may also be a parent/sibling/friend/doula. Johannson et al identified that although most fathers want to be present at the labor and birth, they frequently articulate feeling overwhelmed and unable to support their partner39 and that mode of birth was regarded as largely unimportant to male partners.40 The recommendation for a caesarean section was readily accepted and appreciated by fathers, as it shifted responsibility for birth to the medical practitioner.40 Feelings of helplessness and frustration in partners has been reported to be reduced when pain-relief is used,41 and alternatively, other research has found that partners feel more helpful when less pain is experienced by the woman.42 While continuous labor support has been shown to reduce the need for epidurals, lower rates of caesarean rates, neonatal admissions and postpartum depression, the effect is diminished when support is provided by a person known to the birthing woman, eg, a member of her family/friendship group,43 which may indicate the ameliorating effect of the ability of the partner to respond with less anxiety in relation to the woman’s decisions. To be able to retain objective thinking and regulate themselves while sensing heightened emotions would likely aid the birth partner’s role in supporting the birthing woman. The temptation for a worried birth partner to “fix” the pain of childbirth for a laboring woman may undermine the woman’s ability to cope and embrace the childbirth experience. The increased anxiety this may cause the woman who considered herself to be coping well during labor but who has now had her capacity undermined by others perhaps suggesting pharmacological pain relief/medical interventions, may lead to compliance, withdrawal or rebellion towards them.44 Such conditions may impact the use of CBE during childbirth as a result of the birthing mother’s own reactivity to the anxious feelings/lowered functioning from birth partners present at the birth. Lower levels of differentiation may mean that more anxious birth partners have a greater inclination to adhere to care-providers who assume greater responsibility for pain-relief and birth mode.
Staff who work closely together at work may be considered to behave more like family members when stress is high. When key members of the organization are more highly differentiated, problems within it are more likely to diminish as the members recognize their contribution to the problem and solve problems in a way that enhances the functioning of other staff members.36 In contrast, staff who are less differentiated may make decisions based on an emotional response rather than thinking through the problem and focusing on the observable facts and be anxious about many aspects of their role. The degree to which a person is able to act more thoughtfully rather than reactively is influenced by the intensity of the work relationships formed, the level of acute stress that exists (eg, in hospital settings, real concerns for patient wellbeing), and wider system issues that exert pressure on an individual such that it exceeds that person’s capacity to act with more differentiation of self.45 Research by Beebe and Frische involving nurses suggested that an understanding of differentiation of self in their professional roles, can act as a useful strategy and framework for coping with internal aspects of workplace stress and maintaining an engaged workforce.46
Maternity care-providers also contend with continually changing circumstances. A woman’s labor can quickly change from a normal physiological event to an event requiring medical attention. However, as maternity staff work toward the challenge of decreasing intervention rates in childbirth, they may benefit from gaining an understanding of subtleties present in the system. Noticeable, or even subtle, changes to relationship dynamics between women, partners and staff could impact the use of information and techniques learnt in childbirth education during labor. Maternity care staff with lower levels of differentiation of self may be more likely to make decisions based on the anxiety of the moment rather than rationally thinking through the problem. Increasing anxiety will further exacerbate this, reflecting a level of reactivity that exists within the maternity system itself, and which plays out during birth. A more differentiated individual has the ability to remain emotionally contained in the middle of emotional chaos, and more able to retain their capacity to think and act more clearly, even though emotionality is heightened. If maternity staff can better understand how they function under stress and could modify their response to reduce the reactivity in the system, this could help to create a more mature work environment and reduce the anxiety felt throughout the system.
In a two-person relationship when things are calm and comfortable and anxiety is low, this would be perceived as a calm state. However, Bowen argues that this calm state does not always remain stable, even under ideal situations. A relationship involving two people, which means the anxiety cannot be displaced elsewhere, has a lower tolerance for anxiety and is more easily disturbed by emotional forces within the relationship, and relationship forces from the outside. When anxiety increases and reaches an intensely uncomfortable point, the twosome may introduce a third person into the situation, such as a confidante, to displace some anxiety.47 The third person may then absorb the anxiety that is present between the first and second person, thus reducing the anxiety between the original dyad but dispersing it onto the third. This triangle concept has a much higher tolerance for anxiety and is capable of managing more of life’s challenges.47 Figure 3 shows this process in action. For example, a birthing woman may be finding her birth partner unhelpful. Perhaps they are not as attentive as she would like them to be, or perhaps she is just getting irritated by their generally benign comments. The birthing woman says nothing to her partner, but rolls her eyes, looking at the midwife. The midwife sees this and may react to somehow relieve the pressure between the birthing woman and her partner. If this persists, and the midwife is themselves feeling stressed or anxious, their tendency to be pulled in to “fix” this tension is increased. This means that more of the original anxiety may be absorbed by the midwife.
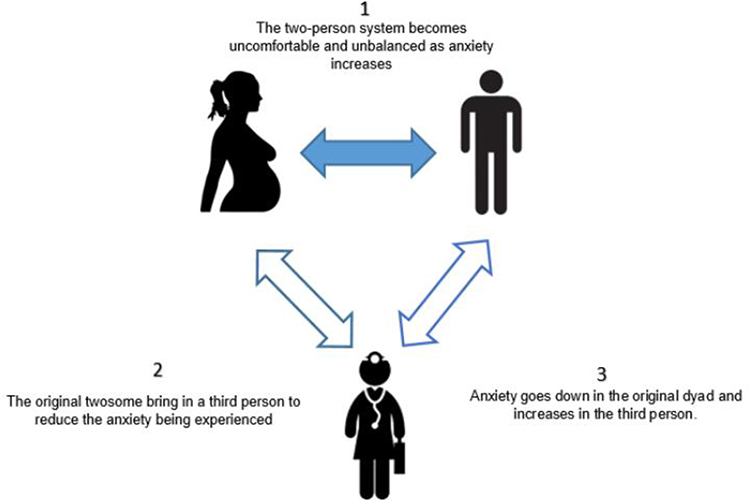 |
Figure 3 The two-person dyad creating a triangle when faced with a stressor. |
An alternative scenario is that anxiety that originates in the care-provider, could potentially cause a birth partner to feel uneasy, fearing something is wrong. The anxiousness is then felt by the birthing woman and could result in her taking up the suggestion of pharmacological pain relief or agreeing to a caesarean section to appease the situation or avoid feeling like a burden. This may have a greater impact in a system where midwives are balancing their reactions to both the woman and partner they are caring for, as well as reactions and pressures from other midwives, obstetricians and managers. A healthcare professional’s ability to not become “triangulated” into anxious work scenarios through functioning at a higher level of differentiation, has been shown by Glasscock and Hales to improve the working environment by focusing on conflict, low morale and productivity as systems issues not individual ones.13 This in turn provides staff with strategies to positively influence the functioning of the entire team.13
While the emotional intensity of a work “family” is likely different to those shared with relatives, they share some commonality, particularly in more anxious or high-stress workplaces. Emotional connectedness can exist within teams of work colleagues who seek support, reassurance and pleasure from one another’s presence. Just like in families, these connections can be intense. In the birth context, this is further complicated through maternity staff not only being emotionally connected to colleagues’ actions but also closely working with women and birth partners during the highly emotional state that accompanies childbirth, sometimes with different philosophical approaches to supporting labor. While it is not the role of maternity staff to be like a parent, it could appear akin to it, depending on the degree to which the birthing woman and her partner look to the staff for comfort and reassurance, and/or the degree to which staff provide direction beyond the scope of their role, such as insisting on implementing institutional guidelines that do not reflect evidence-based practices. Indeed, Dempsey discusses how caregivers act like a “culturally constructed symbolic attachment figure – a parent” (p.106).48 Could it be that in some circumstances, childbirth education strategies to support a physiological birth were providing adequate support to the birthing woman, but other relational factors lead to her abandoning them to alleviate anxiety elsewhere in the birth room? If so, this generates important considerations regarding how the concepts underpinning Bowen theory, specifically a person’s awareness of their level of self-differentiation, are implemented into antenatal care and childbirth education.
Family Functioning and Fusion
Whilst personality and environmental variables must be taken into account in terms of understanding the capacity to function more autonomously, Papero points out how families have an inherent emotional “oneness” that varies in intensity from a low level of intensity with family members exhibiting greater levels of autonomy, to a very intense connection with limited autonomy.49 The degree to which family members act more to relieve the tension of the moment, rather than be guided by their own thinking, speaks to the concept of fusion. Fusion concerns not just the degree of closeness members of a family have with one another but also individual boundaries being lost or sacrificed in the service of meeting others’ needs or wants and replaced with increased family togetherness.50 Fusion, or togetherness, transpires within personal relationships and reaches its greatest intensity in marriages,19 or arguably any romantic relationship. Family units with a more intense fusion and emotional oneness are closely connected but with tenuous relationships that can become easily strained and dysfunctional. When a member of a more fused family unit feels stressed, everyone becomes anxious. Due to the highly emotive nature of labor and the closeness of the people present, childbirth is a prime example of where this may occur. Too much fusion leads to less tolerance for disagreements with others and the less able a person is to consciously control their own life within the family system.50 The degree to which one person in a family is more “caught” in this emotional process and less able to function autonomously reflects the family’s overall capacity to navigate challenges. When there is a disagreement between family members, subtle or overt pressure may be exerted to find agreement. If this is not possible, one person may anxiously “give up self”, that is, act less from their principles about what they think is the appropriate response, and accommodate the other person, rather than risk an argument. This could manifest itself for example, in scenarios such as a woman not going to a CBE class as their partner does not want to attend, or where a woman “agrees” to their mother-in-law being at their birth of their baby despite not truly wanting this, purely to appease others and avoid additional tension. While fusion helps solve the initial problem, it ultimately adds to the anxiety in the system,19 if it is not appropriately tempered.
Fusion in and of itself is not a bad thing. Without fusion, which according to Bowen is a necessary survival response, no mother would sacrifice their individual need for sleep to get up to feed her newborn baby. Without fusion, there would be no coordinated effort by families to support new parents after the birth of a baby, or for families to pool resources to support a family member struggling to adapt to parenthood or a return to work following maternity leave. However, as a child grows and their dependency needs lessen, the capacity to build and allow for more autonomy and to be less dependent on others to help manage one’s emotional states reflects a family’s overall level of differentiation and fusion. Families with less intense fusion appear less susceptible to disturbance when faced with stressors.49 A greater ability to function under stress and pressure in a way that privileges the needs of the birthing woman (an example of a more manageable level of fusion) would be a useful attribute for a birth partner, and other support people, during labor. This may involve supporting the woman to use non-pharmacological CBE techniques to cope in labor, even if their own heightened emotional reactivity leans to a more medicalized pain relief method to be used.
From a care-provider context, work group functioning focusing on management practices and maternal outcomes in childbirth have shown large variances within hospitals.51 Staff members who share clinical work environments have been shown to influence group functioning, where changes in one team member affects other members and thereby shapes overall patient care.13 Maternity unit culture, where management practice aims to pre-empt unit challenges such as having processes to identify and address patient flow and bottlenecks in the system, has been associated with an increased risk of primary caesarean in low-risk women.51 This emphasizes how workplace culture is also an indicator of caesarean rates irrespective of clinical indication. Could it be that an over-controlling approach to maternity units by management shifts anxiety onto the birthing woman, increasing pressure for her to give birth within an artificial timeframe, which results in a system where practices supportive of a physiological birth are increasingly redundant? And to what degree does differentiation of self “protect” against such environments and conditions? For example, consider the following hypothetical example, as shown in Figure 4, of how anxiety may present and move around the system.
 |
Figure 4 A hypothetical example of anxiety moving between individuals. |
If anxious responses from management exist on a regular basis, staff may become increasingly likely to be on alert for warning signs that pressure and anxiety are mounting in the unit. Anxiety can present itself by over-relying on or over-controlling others or focusing the anxiety onto another relationship to diffuse the anxiety. As Brown states, we are “vulnerable as humans to letting our relationships act as a sedative” (p.75)50 and looking to others to appease our own anxiety. Add to this any reactivity that is present in relation to chronic non-life-threatening stressors, for example, any marital tension that exists between the couple or tensions that may be present between individual midwives and their colleagues, it is more than possible that optimal functioning is reduced. Ultimately, a lack of objective thinking in the birthing context could alter recommendations from staff, alter support from partners, and instigate a change in the use of CBE strategies and selection of pain relief management by a mother. Again, the issue of fusion and how we function in different families (personal and professional) may be important additions to CBE content that assist with prospectively considering how one aims to manage this during labor to promote continued use of CBE strategies when finding ourselves caught up in other people’s anxious responses to events.
Discussion
It is necessary for people to see they are a part of the ever-changing systems they inhabit, for if they only see a problem as existing within self or others, they are liable to miss how the system someone is part of profoundly effects their capacity for emotional resilience and objective thinking.50 Bowen theory offers a way to explore how CBE translates into practice during labor and the influence that birth partners and care-providers have on this. Bowen Theory is a way of framing the relational aspects that might be occurring at an emotional level between the mother, birth partner and the care-providers. It also explains the impact pre-existing relationship patterns have on how anxiety is experienced and the effect this has in the birth room.
As anxiety increases, this becomes a crucial time for support people to utilize the information and techniques from childbirth education which could offer ways of coping. Alternatively, we propose that partners and care-providers who negatively influence the use of childbirth education can do so more easily when a woman is looking to them for guidance under this heightened emotional state. Bowen theory argues that it becomes increasingly difficult to decipher if a fear is real or perceived as anxiety builds, which makes decision-making for a woman about how to progress with their care more difficult. The woman in labor feeling pressured to take the epidural, the birth partner who is unprepared and experiencing heightened levels of fear and overwhelm, or the staff member who feels increasingly anxious due to their perception of risk or stressors from other competing demands, are arguably more likely to adopt an approach that shifts responsibility away from themselves and onto others.
Ultimately, it becomes apparent based on Bowen theory, that as a mother becomes more anxious during childbirth, those around her become increasingly influential on what she does and how she manages her labor, particularly so for those with a lower level of differentiation and/or when stress is high. Therefore, women who are predisposed to responding more anxiously and less thoughtfully prior to pregnancy may be even more vulnerable to handing over their control in the birth. Bowen theory thus offers a way to help explain the behavior and responses of women, birth partners and care providers to the innate sensitivities that influence the behavior of individuals, and how this in turn, influences responses to distress, in self and in others, such as capacity for utilization of CBE strategies. Importantly, the use of theory-based strategies can provide frameworks for practice. Implementation of Bowen theory concepts could be incorporated into staff training and childbirth education programs as an effective health promotion strategy focused on reducing system anxiety and promoting woman-centered decision-making.
The ability to translate childbirth education into practice to support the labor process should be viewed as a systems issue as well as an individual one. The principles of Bowen theory can be directly applied to the childbirth context to provide a broader lens of the interactions taking place that influence the integration and use of childbirth education strategies. The relationships between people and the anxiety that is present during labor could help us to understand why information and techniques from childbirth education are more or less successfully applied during the birth. For partners to be able to facilitate the use of strategies aimed at supporting a physiological birth, the ability to maintain objective thinking, as opposed to getting caught up in anxious reactive responses, may help support a rite of passage rather than a rite of protection.7
To provide optimal evidence-based and personalized care, a care-provider needs to be able to give thoughtful attention to the woman and her choices, and to have the capacity to provide good leadership at times of uncertainty or medical emergency, as well as rely on evidence-based policies that support the care provided. Importantly, policies and guidelines based on current evidence are required, as these may help to alleviate anxious feelings and support midwives who may otherwise feel pressurized to promote hospital guidelines for fear of getting in trouble with managers even if such policies are outdated or non-evidence based.
Women have conveyed that a positive birth experience involves both clinically and psychologically safe births.52 Bowen Theory provides an appropriate theoretical lens to explore the birthing couple’s emotionality and reactivity under stress, and to understand how these related factors influence midwives’ responsiveness in the provision of childbirth education and its application during birth. This requires an individual who is better able to balance their emotions and intellect, or in the terms of Bowen Theory, act with greater differentiation of self.
Conclusion
Exploring what contributes to a woman abandoning the use of childbirth education techniques or information in circumstances where they had previously been working well for her, is critical to our understanding of how childbirth education is translated into practice during labor and birth. Bowen theory can provide a valuable framework to understand the difference in how people cope with similarly stressful situations. This makes for a novel application of this theory with its specific emphasis on understanding how concerns about reducing anxiety may impact an individual’s own responsiveness to other challenges. This paper has suggested relational influences that may undermine the application of childbirth education that aims to increase confidence in a woman’s ability to give birth. An understanding of these relational influences and their interplay with anxiety and stress may well be an important addition to CBE for the birthing mother, her birth partner(s) and the clinical staff committed to supporting best practice in childbirth education and its implementation.
Acknowledgments
Alongside the development of this paper, the author KS also attended training courses with The Bowen Centre (US) and The Family Systems Institute (Australia) that assisted with knowledge about Bowen Theory and the development of the ideas in this paper.
Disclosure
KLS is an independent childbirth educator and teaches expectant mothers and partners’ techniques to prepare for birth. KL is currently overseeing an RCT examining the effectiveness of a childbirth education program based on evidence-based techniques to lower the rates of caesarean section. LMM is a Bowen Family System Theory practitioner. The authors report no other conflicts of interest in this work.
References
1. Department of Health. Clinical Practice Guidelines: Pregnancy Care. Canberra: Australian Government; 2019.
2. Hong K, Hwang H, Han H, et al. Perspectives on antenatal education associated with pregnancy outcomes: systematic review and meta-analysis. Women Birth. 2021;34(3):219–230. doi:10.1016/j.wombi.2020.04.002
3. Ferguson S, Davis D, Browne J. Does antenatal education affect labour and birth? A structured review of the literature. Women Birth. 2013;26(1):5–8. doi:10.1016/j.wombi.2012.09.003
4. Gagnon A, Sandall J. Individual or group antenatal education for childbirth or parenthood, or both. Cochrane Database System Rev. 2007;2011(3):CD002869.
5. Sutcliffe K, Dahlen H, Newnham E, Levett K. “You are either with me on this or not”: a meta-ethnography of the influence birth partners and care-providers have on coping strategies learned in childbirth education and used by women during labour. Women Birth. 2023. doi:10.1016/j.wombi.2023.02.001
6. Villarmea S, Kelly B. Barriers to establishing shared decision-making in childbirth: unveiling epistemic stereotypes about women in labour. J Eval Clin Pract. 2020;26(2):515–519. doi:10.1111/jep.13375
7. Reed R. Reclaiming Childbirth as a Rite of Passage: Weaving Ancient Wisdom with Modern Knowledge. Word Witch Press; 2021.
8. Newnham E, McKellar L, Pincombe J. Towards the Humanisation of Birth: A Study of Epidural Analgesia and Hospital Birth Culture. Cham: Palgrave Macmillan US; 2018.
9. Vallance D, LaMontagne A, Keegel T. Protecting and promoting mental health in the workplace: developing a systems approach to job stress. Health Promot J Austr. 2007;18(3):221–228. doi:10.1071/HE07221
10. Levett K, Dahlen H. Perspective: childbirth education in Australia: have we lost our way? Women Birth. 2019;32(4):291–293. doi:10.1016/j.wombi.2018.05.007
11. Levett K, Coughlan S, Longridge S, et al. Be well: a systems-based wellness intervention using mindfulness in the workplace – a case study. J Manag Organ. 2019;25(5):613–634. doi:10.1017/jmo.2017.41
12. Shaw D, Guise JM, Shah N, et al. Drivers of maternity care in high-income countries: can health systems support woman-centred care? Lancet. 2016;388(10057):2282–2295. doi:10.1016/S0140-6736(16)31527-6
13. Glasscock F, Hales A. Bowen’s family systems theory: a useful approach for a nurse administrator’s practice. J Nurs Adm. 1998;28(6):37–42. doi:10.1097/00005110-199806000-00008
14. Levett K, Sutcliffe K, Dahlen H. Childbirth Education - Is it a lost opportunity for change? Int J Birth Parent Educ. 2020;7(2):3–4.
15. Shearer M. Effects of prenatal education depend on the attitudes and practices of obstetric caregivers. Birth. 1990;17(2):73–74. doi:10.1111/j.1523-536X.1990.tb00700.x
16. Kerr M. Bowen Theory’s Secrets: Revealing the Hidden Life of Families.
17. Kerr M, Bowen M. Family Evaluation: An Approach Based on Bowen Theory.
18. Bowen M. Family Therapy in Clinical Practice. Jason Aronson; 1993.
19. Gilbert R. The Eight Concepts of Bowen Theory. Falls Church, Va: Leading Systems Press; 2006.
20. The Bowen Center. Introduction to the eight concepts; 2021. Available from: https://www.thebowencenter.org/introduction-eight-concepts.
21. Titelman P. Differentiation of Self Bowen Family Systems Theory Perspectives. New York: Routledge; 2014.
22. LeDoux J, Pine D. Using neuroscience to help understand fear and anxiety: a two-system framework. Am J Psychiatry. 2016;173(11):1083–1093. doi:10.1176/appi.ajp.2016.16030353
23. Andersson L, Sundstrom-Poromaa I, Wulff M, Astrom M, Bixo M. Implications of antenatal depression and anxiety for obstetric outcome. Obstet Gynecol. 2004;104(3):467–476. doi:10.1097/01.AOG.0000135277.04565.e9
24. Reck C, Zimmer K, Dubber S, Zipser B, Schlehe B, Gawlik S. The influence of general anxiety and childbirth-specific anxiety on birth outcome. Archiv Women’s Mental Health. 2013;16(5):363–369. doi:10.1007/s00737-013-0344-0
25. Alder J, Fink N, Bitzer J, Hosli I, Holzgreve W. Depression and anxiety during pregnancy: a risk factor for obstetric, fetal and neonatal outcome? A critical review of the literature. J Mater Fet Neonatal Med. 2009;20(3):189–209. doi:10.1080/14767050701209560
26. Philpott L, Savage E, FitzGerald S, Leahy-Warren P. Anxiety in fathers in the perinatal period: a systematic review. Midwifery. 2019;76:54–101. doi:10.1016/j.midw.2019.05.013
27. Bohren M, Berger B, Munthe-Kaas H, Tuncalp O. Perceptions and experiences of labour companionship: a qualitative evidence synthesis. Cochrane Database System Rev. 2019;2019(7):CD012449. doi:10.1002/14651858.CD012449.pub2
28. Steen M, Downe S, Bamford N, Edozien L. Not-patient and not-visitor: a metasynthesis fathers’ encounters with pregnancy, birth and maternity care. Midwifery. 2012;28(4):362–371. doi:10.1016/j.midw.2011.06.009
29. Eggermont K, Beeckman D, Van Hecke A, Delbaere I, Verhaeghe S. Needs of fathers during labour and childbirth: a cross-sectional study. Women Birth. 2017;30(4):e188–e197. doi:10.1016/j.wombi.2016.12.001
30. Leinweber J, Rowe H. The costs of ‘being with the woman’: secondary traumatic stress in midwifery. Midwifery. 2010;26(1):76–87. doi:10.1016/j.midw.2008.04.003
31. Creedy D, Sidebotham M, Gamble J, Pallant J, Fenwick J. Prevalence of burnout, depression, anxiety and stress in Australian midwives: a cross-sectional survey. BMC Pregnancy Childbirth. 2017;17(1):13. doi:10.1186/s12884-016-1212-5
32. Prosen M, Krajnc M. Perspectives and experiences of healthcare professionals regarding the medicalisation of pregnancy and childbirth. Women Birth. 2019;32(2):e173–e181. doi:10.1016/j.wombi.2018.06.018
33. Zwelling E. The Emergence of High-Tech Birthing. J Obstet Gynecol Neonatal Nurs. 2008;37(1):85–93. doi:10.1111/j.1552-6909.2007.00211.x
34. Cooper J, Yu M, Brown T. Occupational therapy theory and school-based filial therapy: intervention rationale and formulation. Can J Occupat Ther. 2022;89(1):62–71. doi:10.1177/00084174211056588
35. Titelman P. Differentiation of Self: Bowen Family Systems Theory Perspectives. New York, NY: Routledge; 2015.
36. Collier C, Villareal III P. Family unit functioning questionnaire: development and initial validation. Austr N Z J Fam Ther. 2022;43(2):223–242. doi:10.1002/anzf.1491
37. Keller M, Noone R. Handbook of Bowen Family Systems Theory and Research Methods: A Systems Model for Family Research.
38. Steelman J. Relationship dynamics: understanding married women’s mental health. Adv Nurs Sci. 2007;30(2):151–158. doi:10.1097/01.ANS.0000271105.42043.65
39. Johansson M, Fenwick J, Premberg A. A meta-synthesis of fathers’ experiences of their partner’s labour and the birth of their baby. Midwifery. 2015;31(1):9–18. doi:10.1016/j.midw.2014.05.005
40. Johansson M, Hildingsson I, Fenwick J. “As long as they are safe – birth mode does not matter’ Swedish fathers” experiences of decision-making around caesarean section. Women Birth. 2014;27(3):208–213. doi:10.1016/j.wombi.2014.03.003
41. Hendrix M, Pavlova M, Nieuwenhuijze M, Severens J, Nijhuis J. Differences in preferences for obstetric care between nulliparae and their partners in the Netherlands: a discrete-choice experiment. J Psychosom Obstet Gynaecol. 2010;31(4):243–251. doi:10.3109/0167482X.2010.527400
42. Capogna G, Camorcia M, Stirparo S. Expectant fathers’ experience during labor with or without epidural analgesia. Int J Obstet Anesth. 2006;16(2):110–115. doi:10.1016/j.ijoa.2006.08.009
43. Bohren M, Hofmeyr GJ, Sakala C, Fukuzawa R, Cuthebert A. Continuous support for women during childbirth. Cochrane Database System Rev. 2017. doi:10.1002/14651858.CD003766.pub6
44. Papero D, Frost R, Havstad L, Noone R. Natural Systems Thinking and the Human Family. Systems. 2018;6(2):19. doi:10.3390/systems6020019
45. Comella P. Observing emotional functioning in human relationships systems: lesson from murray Bowen’s writings. In: Bregman OC, White CM, editors. Bringing Systems Thinking to Life: Expanding the Horizons of Bowen Family Systems Thinking. Taylor and Francis: New York; 2011.
46. Beebe R, Frisch N. Development of the Differentiation of Self and Role Inventory for Nurses (DSRI-RN): a tool to measure internal dimensions of workplace stress. Nurs Outlook. 2009;57(5):240–245. doi:10.1016/j.outlook.2009.04.001
47. Bowen M. Family Therapy in Clinical Practice. New York: J. Aronson; 1985.
48. Dempsey R. Beyond the Birth Plan. Melbourne: Boathouse Press; 2020.
49. Papero D. Trauma and the family: a systems‐oriented approach. Austr N Z J Fam Ther. 2017;38(4):582–594. doi:10.1002/anzf.1269
50. Brown J. Growing Yourself Up: How to Bring Your Best to All of Life’s Relationships. Exisle Publishing; 2017.
51. Plough A, Galvin G, Li Z, et al. Relationship between labor and delivery unit management practices and maternal outcomes. Obstet Gynecol. 2017;130(2):358–365. doi:10.1097/AOG.0000000000002128
52. Downe S, Finlayson K, Oladapo O, et al. What matters to women during childbirth: a systematic qualitative review. PLoS One. 2018;13(4):e0194906. doi:10.1371/journal.pone.0194906
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Anxiety and Depression Among HIV-Positive and HIV-Negative Pregnant Women During COVID-19 Pandemic in Ekiti State, Southwest Nigeria
Ade-Ojo IP, Dada MU, Adeyanju TB
International Journal of General Medicine 2022, 15:4123-4130
Published Date: 16 April 2022
Maternal Anxiety and Its Associated Factors During the First and Second Wave of COVID-19 Pandemic in Serbia: A Cross-Sectional Study
Jeličić L, Janković S, Sovilj M, Bogavac I, Drobnjak A, Dimitrijević A, Subotić M
Psychology Research and Behavior Management 2022, 15:3775-3792
Published Date: 20 December 2022
Assessment of Levels of Anxiety and Fear of Covid-19 in a Population of Pregnant Women in Spain
Muñoz-Vela FJ, Fernández-Carrasco FJ, Gómez-Salgado J, Allande-Cussó R, Marques Monteiro Dias Mendes IM, Martins Teixeira-da-Costa EI, Vázquez-Lara JM, Fagundo-Rivera J, Rodríguez-Díaz L
Psychology Research and Behavior Management 2023, 16:4665-4676
Published Date: 16 November 2023
Current Situation and Mental Health of Pregnant Women During the Prevention and Control of Novel Coronavirus Infection: A Cross-Sectional Study on the Investigation of Influencing Factors
Zhao J, Li Y, Guo M, Zhang G, Chen P
International Journal of Women's Health 2024, 16:193-202
Published Date: 2 February 2024
Sleep Quality and Its Predictors Among Pregnant Women in Jordan: A Cross-Sectional Study
Alasmer Z, Nazzal MS, Mohamed Z, Al-Jaber A, Ali R, Alshar F, Ababneh EM, Alshdaifat E, Kanaan SF
International Journal of Women's Health 2025, 17:1285-1296
Published Date: 7 May 2025