Back to Journals » International Journal of Women's Health » Volume 17
Construction of a Nomogram Prediction Model for Intraoperative Shivering During Caesarean Section
Authors Liu J, Huang S, Zhang L, Du L, Xu W, Tian Q, Luo X, Zhang M
Received 28 March 2025
Accepted for publication 19 September 2025
Published 23 September 2025 Volume 2025:17 Pages 3179—3188
DOI https://doi.org/10.2147/IJWH.S531119
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Matteo Frigerio
Jinghui Liu,1,2,* Shan Huang,1,* Luwen Zhang,2 Libaihe Du,1 Wenqi Xu,1,2 Qingmi Tian,1,2 Xiaoping Luo,1 Mingyang Zhang1
1Department of Surgery and Anesthesia III, Zhongshan City People’s Hospital, Zhongshan, Guangdong, People’s Republic of China; 2School of Nursing and Health, Henan University, Kaifeng, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoping Luo, Email [email protected] Mingyang Zhang, Email [email protected]
Objective: To explore the risk factors of intraoperative shivering in cesarean section patients, construct a prediction model and evaluate its performance.
Methods: Clinical data of 260 patients undergoing cesarean section from March 2024 to January 2025 were collected, with intraoperative shivering as the primary outcome. Univariate and multivariable logistic regression analyses were performed to identify statistically significant independent risk factors. A risk prediction model was subsequently developed and visualized as a nomogram. The model’s discriminative ability, calibration, and clinical utility were evaluated.
Results: The incidence of intraoperative shivering was 32.69%. Multivariable logistic regression analysis revealed that body mass index (BMI), baseline body temperature, American Society of Anesthesiologists (ASA) classification, intraoperative fluid infusion volume, and intraoperative blood loss were independent risk factors for intraoperative shivering (P < 0.05). The area under the curve (AUC) was 0.914, with a sensitivity of 0.894, specificity of 0.823, and Youden index of 0.717, indicating good discriminative ability. The Hosmer-Lemeshow test demonstrated good calibration (χ² = 3.061, P = 0.930). Decision Curve Analysis (DCA) indicated favorable clinical applicability.
Conclusion: The nomogram model demonstrates good predictive performance, assisting clinicians in identifying high-risk parturients prone to intraoperative shivering during cesarean section. Early identification based on risk factors enables implementation of targeted interventions, thereby potentially reducing the incidence and adverse impacts of shivering. This improves maternal intraoperative comfort and perioperative outcomes.
Keywords: cesarean section, shivering, risk factors, prediction, nomogram
Introduction
Shivering is a common complication in surgical procedures, primarily caused by thermoregulatory impairment and hypothermia, manifesting as involuntary rapid contractions of skeletal muscles and bodily tremors.1 In recent years, clinical observations have shown a rising trend in the incidence of shivering among cesarean section patients, reaching as high as 30%-85%.2–5 Beyond causing significant patient discomfort and interfering with vital clinical monitoring, shivering increases oxygen consumption and is associated with elevated risks of surgical site bleeding, cardiac events, wound infections, and other complications,6 all of which may lead to adverse outcomes for both mothers and infants. The choice of anesthesia is a critical modifiable factor. Combined spinal epidural anesthesia (CSEA), widely used for cesarean delivery due to its rapid onset and reliable blockade, inherently increases susceptibility to hypothermia and shivering.7,8 Compared to general anesthesia, neuraxial techniques like CSEA impair central thermoregulation (reducing the shivering threshold) and induce profound peripheral vasodilation (promoting rapid core-to-peripheral heat redistribution).9 Furthermore, proactive warming strategies, particularly preoperative warming (prewarming), are established preventive measures. Prewarming minimizes the core-peripheral temperature gradient, mitigating redistribution hypothermia during the initial phase of neuraxial anesthesia and significantly reducing shivering incidence.10,11 Despite its efficacy, prewarming is inconsistently applied in obstetric practice.
Literature studies indicate that the significant variation in the incidence of intraoperative shivering during cesarean sections suggests its association with multiple factors beyond anesthesia type and warming practices. These primarily include: patient factors (age, anxiety, pregnancy complicated by hypothyroidism, emergency admission); physiological states (pain, core temperature, mean arterial pressure (MAP); procedural aspects (duration of surgery and anesthesia, level of sensory blockade, operating room temperature, emergency surgery, transfer from delivery room, epidural labor analgesia, membrane rupture, labor status); and intraoperative management (blood loss, fluid replacement volume, lack of intraoperative heat preservation measures).2,12,13 Identifying and minimizing these risk factors, including optimizing anesthesia management and implementing targeted warming protocols, could significantly reduce shivering incidence and improve maternal and neonatal outcomes. The purpose of this study is to understand the current situation of intraoperative shivering in cesarean section patients and its risk factors, and to construct a risk prediction model. By incorporating factors such as anesthesia-related parameters, the resulting nomogram will provide a practical tool for individualized risk assessment. This will offer a crucial reference for implementing preventive strategies and ultimately reduce the occurrence of shivering during cesarean sections.
Materials and Methods
Study Design and Subjects
This study adopted a convenience sampling method to select patients undergoing cesarean section at a tertiary grade A hospital in Zhongshan City, from March 2024 to January 2025 as participants. This study protocol was approved by the hospital ethics committee (K2022-272) and registered with the China Clinical Registration Center (registration number, ChiCTR2200064965). The inclusion criteria were: (1) Age ≥18 years; (2) Patients undergoing cesarean section under CSEA; (3) Without prewarming. The exclusion criteria were: (1) Patients with comorbid severe metabolic or cardiovascular diseases; (2) Patients with major organ dysfunction; (3) Patients with coagulation disorders; and (4) Patients with preoperative shivering.
Assessment Method for Shivering
Shivering was evaluated using the Bedside Shivering Assessment Scale (BSAS): Grade 0 (no shivering), Grade 1 (mild shivering with tremors localized to the neck and/or chest), Grade 2 (moderate shivering with visible tremors involving the upper limbs, neck, and chest), and Grade 3 (severe shivering with visible tremors in both limbs and trunk).14 To ensure accurate assessment, all raters observed each patient for 2 minutes, via visual inspection and palpation of the neck, chest, arms, and legs. Each patient was independently assessed by physicians and nurses simultaneously, with raters blinded to each other’s assessments. After each assessment session, blinding was broken to establish a consensus score. Disagreements were adjudicated by adopting the majority score. In the event of a tie, each rater was asked to reassess the patient until a consensus was reached. According to this scale, patients with a BSAS score ≥ 1 were defined as having intraoperative shivering and assigned to the shivering group; those with a BSAS score of 0 were defined as having no shivering and assigned to the non-shivering group. The questionnaire used is available in Supplementary file 1.
Data Collection Tool
Based on domestic and international studies on shivering,2,12,15–17 intraoperative shivering risk factors were identified through literature review and two rounds of expert consultation, culminating in the development of the Questionnaire on Influencing Factors of Intraoperative Shivering in Cesarean Section Patients. The questionnaire includes: (1) Patient demographic data: age (years), BMI (kg/m2), gestational weeks at delivery (weeks), primipara status, history of abortion, baseline body temperature (°C), MAP (mmHg), heart rate (bpm), preoperative fasting status, preoperative pain score (points), gestational hypertension, gestational diabetes mellitus, gestational hypothyroidism, emergency admission, premature rupture of membranes, and scarred uterus. (2) Surgery-related data: operating room temperature (°C), ASA classification, anesthesia block level, implementation of active warming measures, intraoperative oxytocin use, duration of surgery (min), duration of anesthesia (min), fetal delivery time (min), intraoperative fluid volume (mL), and intraoperative blood loss (mL).
Data Collection Methods
Uniformly trained investigators preoperatively reviewed the electronic medical record (EMR) system to collect general participant demographic data. Intraoperative monitoring indicators were documented by the research team through direct observation and completed records according to real-time surgical conditions. All questionnaires were finalized upon completion of the surgery. After collecting, the data were kept by designated personnel. Data entry and verification were conducted by two people, and 5% to 10% of the maternal data were verified simultaneously during the entry process.
Sample Size Calculation
The sample size was determined using the population estimation formula for categorical variables in cross-sectional studies: n = (Z1-α/2)2 p (1-p) / d2. Parameters were defined as follows: α=0.05, Z1-α/2=1.96, p=0.5 (based on internationally reported shivering incidence in cesarean sections), and d=0.15p (15% permissible error). This yielded an initial sample size of 171 participants. To compensate for a 20% attrition rate, the adjusted sample size was calculated as 171 / (1–20%) = 214. Based on this calculation and considering clinical feasibility, 286 participants were included initially; 26 were later excluded due to incomplete data, resulting in 260 participants for final analysis.
Data Analysis
Data entry was performed using EpiData 3.1 with a dual-entry protocol to ensure accuracy. Statistical analysis was conducted using SPSS 27.0 and R 4.3.2. Continuous variables, expressed as mean ± standard deviation (SD), were compared between two groups using the independent Student’s t-test or among multiple groups using one-way analysis of variance (ANOVA). Categorical variables were presented as frequency (percentage) and analyzed using the chi-square (χ²) test. Based on the significant variables identified in the univariate analysis, multivariable logistic regression analysis was performed to identify independent predictors. Multicollinearity was assessed using variance inflation factors (VIF). The nomogram prediction model for shivering risk was developed using the rms package in R 4.3.2. Internal validation of the model was performed using the Bootstrap method with 500 resamples. Model calibration (goodness-of-fit) was assessed using the Hosmer-Lemeshow test. Model discrimination was evaluated using receiver operating characteristic (ROC) curve analysis, which provided the AUC, Youden index, and optimal cutoff value. A P-value of less than 0.05 was considered statistically significant.
Results
Baseline Characteristics of Study Participants
Incidence of Intraoperative Shivering and Univariate Analysis of Risk Factors in Parturients Undergoing Cesarean Section
Of the 260 parturients who underwent cesarean delivery, intraoperative shivering occurred in 85 cases (32.69%), with the remaining 175 cases having no shivering. No statistically significant differences were observed between the two groups in age, gestational weeks at delivery, primipara status, history of abortion, MAP, heart rate, preoperative fasting status, gestational hypertension, gestational diabetes mellitus, scarred uterus, or intraoperative oxytocin use (all P > 0.05). However, statistically significant differences were identified in BMI, baseline body temperature, preoperative pain score, gestational hypothyroidism, emergency admission, premature rupture of membranes, operating room temperature, ASA classification, anesthesia block level, implementation of active warming measures, duration of surgery, duration of anesthesia, fetal delivery time, intraoperative fluid volume, and intraoperative blood loss (all P < 0.05). See Table 1.
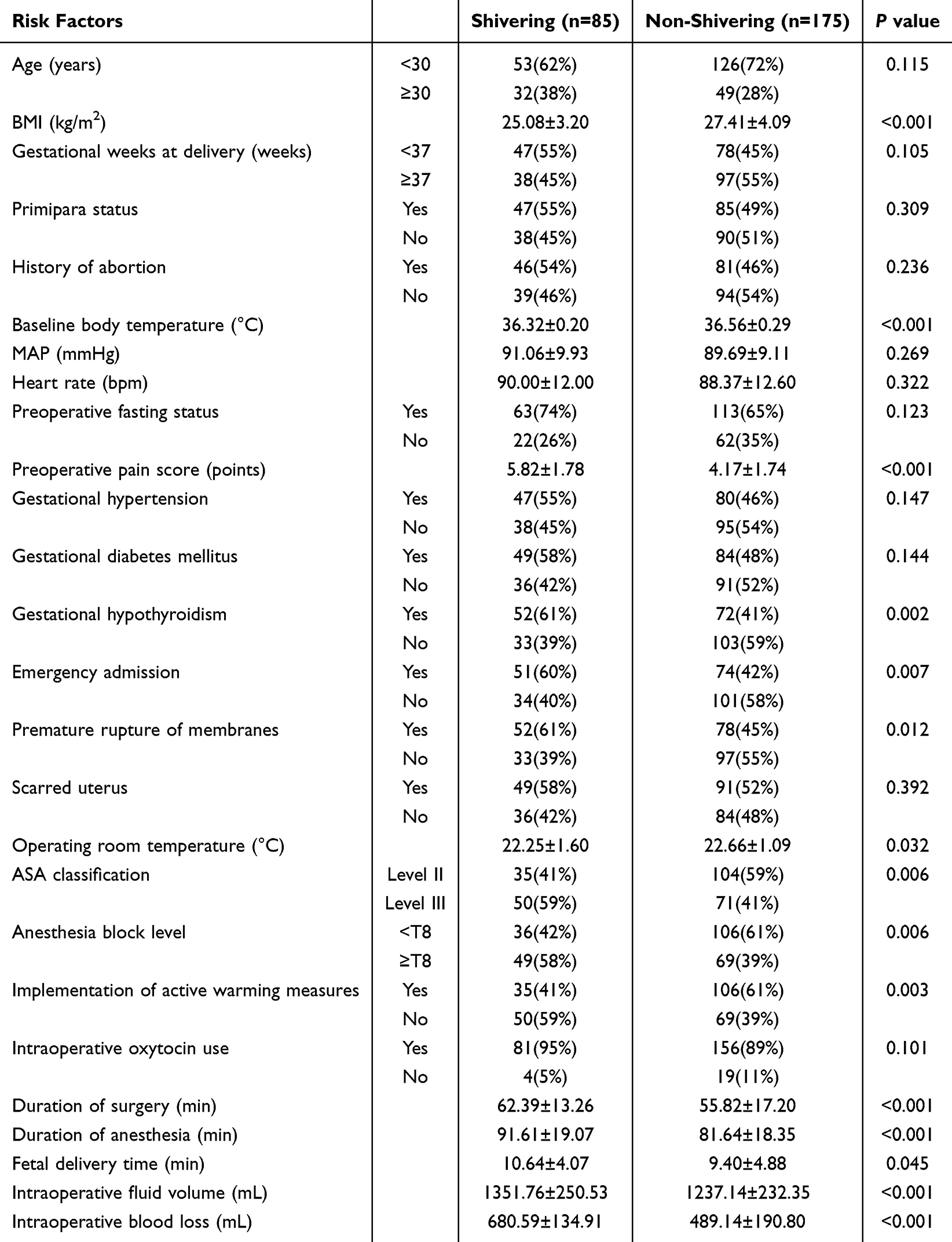 |
Table 1 Univariate Analysis of Intraoperative Shivering in Women Undergoing Cesarean Delivery [n (%), |

Multivariable Logistic Regression Analysis
The occurrence of intraoperative shivering in cesarean section patients was designated as the dependent variable (shivering = 1, no shivering = 0). Factors showing P < 0.05 in Table 1 were assigned as independent variables (coding details in Supplementary file 2). Variables with P < 0.05 in univariate analysis were included in the multivariable model. Results showed that BMI, baseline body temperature, ASA classification, intraoperative fluid volume, and intraoperative blood loss were independent risk factors for intraoperative shivering in cesarean section patients. Diagnostic results using the VIF method for these five variables showed that all VIF values were below 10, indicating no evidence of multicollinearity among them (see Table 2).
 |
Table 2 Multifactor Logistic Regression Analysis |
Development of the Nomogram Prediction Model
The regression equation derived from the binary logistic regression analysis was: Logit(P)=160.67 − 0.19 × BMI − 4.56 × Baseline Body Temperature + 0.91 × ASA Classification + 0.002 × Intraoperative Fluid Volume + 0.01 × Intraoperative Blood Loss. A nomogram was constructed to visualize this model, where each risk factor is represented by a calibrated axis for score assignment. The total score, calculated by summing all individual scores, corresponds to the predicted probability of intraoperative shivering occurrence. See Figure 1.
 |
Figure 1 Nomogram for predicting the risk of intraoperative shivering in women undergoing cesarean section. |
Model Predictive Performance Evaluation
Internal validation using the Bootstrap method with 500 resampling iterations was performed to assess the model. The discriminative ability of the model was evaluated via the receiver operating characteristic (ROC) curve, yielding an AUC of 0.914 (95% CI: 0.881–0.948). The optimal cutoff value of 0.318 was determined based on the maximum Youden index (0.717), with sensitivity and specificity values of 0.894 and 0.823, respectively (see Figure 2). The Hosmer-Lemeshow goodness-of-fit test (χ² = 3.061, P = 0.930 > 0.05) indicated excellent calibration of the model. DCA was conducted to evaluate overall clinical utility, demonstrating that the model’s curve consistently outperformed the extreme curves across the 0–1 threshold probability range. This suggests high net benefit and favorable safety when interventions are guided by the model’s predictions, supporting its clinical validity (see Figure 3).
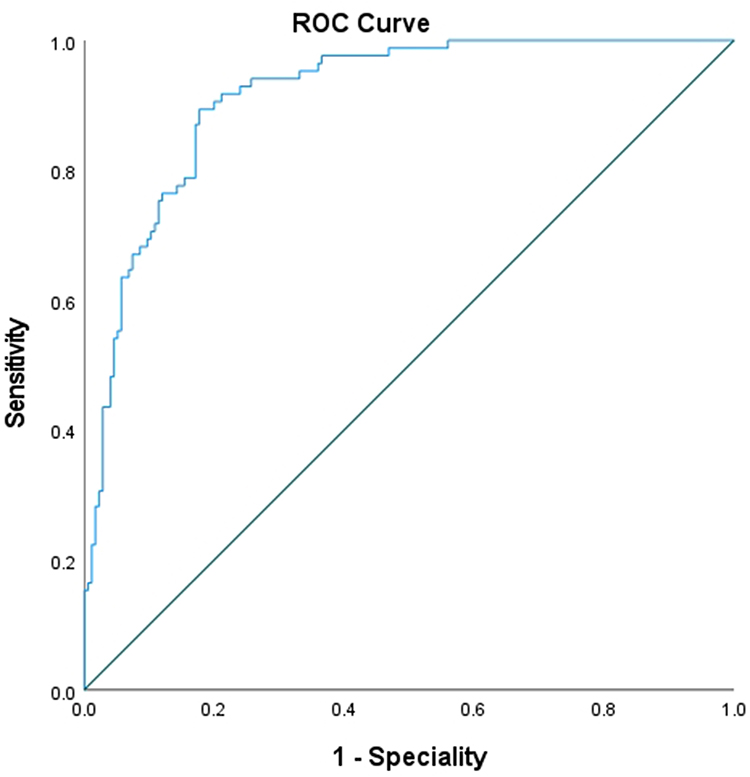 |
Figure 2 ROC curve of the predictive model for intraoperative shivering in women undergoing cesarean section. |
 |
Figure 3 DCA curve of the predictive model for intraoperative shivering in women undergoing cesarean section. |
Discussion
Shivering is a common complication during cesarean sections. Its pathophysiology remains incompletely understood. Its occurrence not only elevates intraocular and intracranial pressures but also increases oxygen consumption by 300%–400%, carbon dioxide production, catecholamine release, metabolic heat production by 600%, and metabolic rate by 400%, alongside inducing lactic acidosis.18 These effects may be particularly detrimental in patients with compromised cardiopulmonary reserve. Shivering further heightens risks of maternal cardiovascular/cerebrovascular events, fetal distress, and postoperative complications (eg, infections, pain, hemorrhage), potentially delaying wound healing and prolonging hospitalization.1,19 Establishing an intraoperative shivering risk prediction model enables proactive interventions before shivering onset, shifting from reactive to preventive management. By identifying high-risk patients for targeted interventions (eg, enhanced warming protocols, pharmacological prophylaxis), this model reduces shivering incidence and improves maternal comfort while avoiding overtreatment of low-risk populations. This approach optimizes healthcare resource allocation and alleviates clinical workload pressures.
Previous studies have demonstrated that lower maternal BMI is associated with a higher risk of hypothermia and shivering.20 This study further confirms that low BMI is an independent risk factor for intraoperative shivering during cesarean sections. The underlying mechanisms likely involve reduced adipose tissue volume and its dual physiological functions. Patients with lower BMI have diminished subcutaneous fat, which compromises thermal insulation and increases heat loss.21 Concurrently, lower adiposity is associated with reduced leptin levels; leptin deficiency suppresses sympathetic nervous activity via the hypothalamic-melanocortin pathway, diminishing thermogenic capacity.22 These dual effects collectively increase shivering risk. These findings align with studies by Desgranges et al23 and Zhang et al,24 which identified higher BMI as a protective factor against intraoperative shivering in cesarean deliveries.
This study found that patients with lower preoperative baseline body temperature had a significantly elevated risk of intraoperative shivering, attributable to multi-level pathophysiological mechanisms: (1) Compensatory imbalance in the thermoregulatory set point: Anesthesia exacerbates thermal deviation, thereby triggering the shivering reflex.25 (2) Depletion of the vasoconstrictive reserve, accelerating core-to-peripheral temperature redistribution.25 Therefore, clinical interventions should prioritize pre-warming (eg, using forced-air warming to reduce shivering incidence)26 and metabolic optimization (eg, correcting anemia or hypothyroidism).
This study demonstrated that the incidence of intraoperative shivering was 41% in ASA II patients and 59% in ASA III patients, with a progressive increase in shivering rates correlating with higher ASA classification. This trend may be attributed to the heightened anesthesia-related risks, poorer physiological status, diminished cardiovascular reserve, compromised compensatory capacity, and impaired thermoregulatory function in higher ASA classes, which collectively reduce the adaptability to perioperative stressors.27 These findings align with studies by Xiang et al28 and Dai et al.29 While this study was limited to ASA classes II and III, it is plausible that patients in higher ASA classes (eg, IV/V), with more severe systemic compromise, would face even greater shivering risks due to amplified adverse effects of surgery and anesthesia. Consequently, clinicians should tailor temperature management strategies to individual ASA class-specific profiles to prevent the occurrence of intraoperative shivering.
Substantial fluid administration during cesarean sections was identified as a critical contributor to intraoperative shivering, consistent with findings from Jin et al.16 Large-volume fluid infusion alters blood electrolyte concentrations, activates peripheral thermoreceptors, and disrupts central thermoregulatory mechanisms. If administered without adequate warming, unwarmed fluids rapidly reduce core body temperature, triggering involuntary skeletal muscle contractions and shivering. Furthermore, the exposure of body cavities during cesarean sections facilitates significant heat loss, which is exacerbated by cold fluid infusion. Additionally, excessive fluid administration may dilute coagulation factors, leading to increased surgical site bleeding and exacerbating systemic stress. Therefore, rational fluid management (eg, volume restriction combined with fluid warming protocols) is essential to reduce intraoperative shivering incidence, enhance procedural safety, and improve maternal comfort.
Intraoperative blood loss reduces circulating blood volume, leading to inadequate tissue perfusion, peripheral vasoconstriction, and hypotension. These hemodynamic changes stimulate thermoreceptors, lowering skin and peripheral tissue temperatures. Furthermore, significant blood loss necessitates increased administration of fluids or blood products, which—if inadequately warmed—exacerbate heat dissipation and core hypothermia, thereby elevating the risk of intraoperative shivering.21
In summary, BMI, basal body temperature, ASA classification, intraoperative fluid volume, and intraoperative blood loss serve as independent risk factors for shivering during cesarean sections, each contributing to the occurrence of intraoperative shivering through distinct mechanisms. Clinically, comprehensive and precise perioperative management strategies should be developed based on these factors. These strategies should focus on optimizing maternal physical status, implementing rational control of surgical procedures and fluid/blood transfusion volumes, and strengthening temperature regulation. Such multifaceted interventions will effectively reduce the incidence of intraoperative shivering during cesarean deliveries, ensure maternal surgical safety and comfort, and ultimately enhance overall healthcare quality.
This study presents several notable strengths: (1) Dual data entry verification minimized transcription errors. (2) The nomogram incorporates multifactorial predictors, providing a holistic clinical assessment tool for shivering risk. Several limitations should be acknowledged: (1) Limited sample size resulted in events per variable (EPV) less than 10, potentially affecting model stability and risking overfitting. (2) Lack of inter-rater reliability assessment (eg, Kappa statistic) for the BSAS scale, which may introduce observer bias due to its subjective nature. (3) The absence of model fit indices (eg, AIC/BIC) limits comprehensive evaluation of model quality and comparisons with alternative models. (4) Exclusive reliance on linear assumptions in logistic regression may overlook complex nonlinear relationships between predictors and outcomes. (5) Single-center design without external validation limits the generalizability of the findings to diverse populations and clinical settings. Future research should address these gaps through larger multicenter studies, incorporating nonlinear modeling techniques (eg, splines), external validation, and objective shivering monitoring technologies.
Conclusion
Based on a review of relevant literature, this study independently developed a questionnaire investigating influencing factors of intraoperative shivering in cesarean delivery patients, ensuring comprehensive inclusion of clinically relevant factors. The constructed risk prediction model for intraoperative shivering demonstrated good predictive value and high clinical applicability, providing a reference for clinicians to assess shivering risk and formulate thermal insulation measures during cesarean deliveries.
Date Sharing Statement
Research data are available from the corresponding author (Dr. Mingyang Zhang) upon reasonable request.
Ethics Approval and Informed Consent
The study complied with medical ethics standards and was reviewed by the Ethics Committee of Guangdong Provincial Zhongshan People’s Hospital (review approval number: K2022-272), and registered online at China Clinical Registration Center (registration number, ChiCTR2200064965), all methods were carried out in accordance with relevant guidelines and regulations. All participants provided informed consent, in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by a grant from the Zhongshan City Healthcare General Project 2023 (2023B1003) and Guangdong Provincial Medical Research Fund 2023 (B2023066), Zhongshan City, Guangdong Province, China.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lopez MB. Postanaesthetic shivering - from pathophysiology to prevention. Rom J Anaesth Intensive Care. 2018;25(1):73–81. doi:10.21454/rjaic.7518.251.xum
2. Qi X, Chen D, Li G, et al. Risk factors associated with intraoperative shivering during caesarean section: a prospective nested case-control study. BMC Anesthesiol. 2022;22(1):56. doi:10.1186/s12871-022-01596-7
3. Abdel-Ghaffar HS, Moeen SM. Prophylactic granisetron for post-spinal anesthesia shivering in cesarean section: a randomized controlled clinical study. Acta Anaesthesiol Scand. 2019;63(3):381–388. doi:10.1111/aas.13084
4. Sachidananda R, Basavaraj K, Shaikh SI, Umesh G, Bhat T, Arpitha B. Comparison of prophylactic intravenous magnesium sulfate with tramadol for postspinal shivering in elective cesarean section: a placebo controlled randomized double-blind pilot study. Anesth Essays Res. 2018;12(1):130–134. doi:10.4103/aer.AER_196_17
5. Lema GF, Gebremedhn EG, Gebregzi AH, Desta YT, Kassa AA. Efficacy of intravenous tramadol and low-dose ketamine in the prevention of post-spinal anesthesia shivering following cesarean section: a double-blinded, randomized control trial. Int J Womens Health. 2017;9:681–688. doi:10.2147/IJWH.S139655
6. Li L. Analysis of influencing factors and predictive modeling of postoperative shivering in patients undergoing cesarean section under epidural anesthesia. Chin J Matern Child Health Care. 2025;40(02):294–298. doi:10.19829/j.zgfybj.issn.1001-4411.2025.02.026
7. Sun J, Zheng Z, Li Y, et al. Nalbuphine versus dexmedetomidine for treatment of combined spinal-epidural post-anesthetic shivering in pregnant women undergoing cesarean section. J Int Med Res. 2019;47(9):4442–4453. doi:10.1177/0300060519865063
8. Jing C, Wang C. Combining spinal-epidural anesthesia versus single-shot spinal anesthesia for cesarean delivery: a meta-analysis of 5 randomized controlled trials. Med Sci Monit. 2019;25:2859–2867. doi:10.12659/MSM.913744
9. Kim WH, Hur M, Park SK, et al. Comparison between general, spinal, epidural, and combined spinal-epidural anesthesia for cesarean delivery: a network meta-analysis. Int J Obstet Anesth. 2019;37:5–15. doi:10.1016/j.ijoa.2018.09.012
10. Amsalu H, Zemedkun A, Regasa T, Adamu Y. Evidence-based guideline on prevention and management of shivering after spinal anesthesia in resource-limited settings: review article. Int J Gen Med. 2022;15:6985–6998. doi:10.2147/IJGM.S370439
11. Horn EP, Schroeder F, Gottschalk A, et al. Active warming during cesarean delivery. Anesth Analg. 2002;94(2):409–414. doi:10.1097/00000539-200202000-00034
12. Zhang Y, Liu J. Influencing factors of shivering during cesarean section. Med J Chin People Health. 2025;37(03):11–14.
13. Ferede YA, Aytolign HA, Mersha AT. “The magnitude and associated factors of intraoperative shivering after cesarean section delivery under Spinal anesthesia”: a cross sectional study. Ann Med Surg. 2021;72:103022. doi:10.1016/j.amsu.2021.103022
14. Badjatia N, Strongilis E, Gordon E, et al. Metabolic impact of shivering during therapeutic temperature modulation: the bedside shivering assessment scale. Stroke. 2008;39(12):3242–3247. doi:10.1161/STROKEAHA.108.523654
15. Zhang L, Ma B, Zhang J, et al. Risk factors of intraoperative shivering in puerpera undergoing cesarean section. J Clin Anesthesiol. 2022;38(08):837–840.
16. Jin Y, Ge H, x Z, Li T. Analysis of the influencing factors of shivering during cesarean section of puerperaes. Chin J Fam Plann. 2024;32(06):
17. Wódarski B, Chutkowski R, Banasiewicz J, et al. Risk factors for shivering during caesarean section under spinal anaesthesia. A prospective observational study. Acta Anaesthesiol Scand. 2020;64(1):112–116. doi:10.1111/aas.13462
18. Tan Sook Kuan J, Musthafa QA, Abdullah FH, Sayed Masri SNN. Intraoperative phenylephrine infusion to reduce perioperative shivering in lower segment caesarean section: a randomised controlled study. Medicine. 2023;102(19):e33721. doi:10.1097/MD.0000000000033721
19. Zhong J, Xie H. Advances in nursing care for intraoperative shivering during cesarean section: a review. Chin J Gen Nurs. 2022;20(18):2498–2501.
20. Sari S, Aksoy SM, But A. The incidence of inadvertent perioperative hypothermia in patients undergoing general anesthesia and an examination of risk factors. Int J Clin Pract. 2021;75(6):e14103. doi:10.1111/ijcp.14103
21. Liao J, Wu Y, Luo L. Analysis on the occurrence of shivering in puerpera undergoing cesarean section and influencing factors. Chin Med Pharm. 2020;10(02):83–86.
22. Cheng L, Wang D. Analysis of influencing factors for postoperative hypothermia in patients undergoing general anesthesia. Henan Med Res. 2020;29(29):5428–5430.
23. Desgranges FP, Bapteste L, Riffard C, et al. Predictive factors of maternal hypothermia during Cesarean delivery: a prospective cohort study. Can J Anaesth. 2017;64(9):919–927. doi:10.1007/s12630-017-0912-2
24. Zhang Q, Sun F, Hao J, Yan W. Analysis of correlation between temperature of anterior thigh region and chills reaction in cesarean section patients and the influencing factors of chills reaction. Chin J Med. 2023;58(03):312–315.
25. Collins S, Budds M, Raines C, Hooper V. Risk factors for perioperative hypothermia: a literature review. J Perianesth Nurs. 2019;34(2):338–346. doi:10.1016/j.jopan.2018.06.003
26. Marin L, Höcker J, Esser A, Terhorst R, Sauerwald A, Schröder S. Forced-air warming and continuous core temperature monitoring with zero-heat-flux thermometry during cesarean section: a retrospective observational cohort study. Braz J Anesthesiol. 2022;72(4):484–492. doi:10.1016/j.bjane.2021.10.007
27. Li Y. Analysis on risk factors and prediction model building for intraoperative hypothermia of patients undergoing endoscopic urological surgery. Lanzhou University. 2021. doi:10.27204/d.cnki.glzhu.2021.002275
28. Xiang H, Huang L, Qian W, Zhu F, Zhang H, Lu Z. Development and application of a deep learning-based prediction model for unplanned perioperative hypothermia in patients undergoing general anesthesia. Chin J Emerg Med. 2022;31(8):1116–1120.
29. Dai Z, Zhang Y, Yi J, Huang Y. Validation of a prediction model for intraoperative hypothermia in patients receiving general anesthesia. Int J Clin Pract. 2022;2022(1):6806225. doi:10.1155/2022/6806225
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Paraspinal Muscle Degeneration: A Potential Risk Factor for New Vertebral Compression Fractures After Percutaneous Kyphoplasty
Si F, Yuan S, Zang L, Fan N, Wu Q, Wang T, Wang A
Clinical Interventions in Aging 2022, 17:1237-1248
Published Date: 13 August 2022
Incidence and Risk Factors of Cranial Nerve Palsy in Patients with Tuberculous Meningitis: A Retrospective Evaluation
Wen A, Cao WF, Liu SM, Zhou YL, Xiang ZB, Hu F, Wu LF, Cai W, Leng EL
Infection and Drug Resistance 2023, 16:829-841
Published Date: 14 February 2023
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023
Risk Factors and Prediction Nomogram of Cognitive Frailty with Diabetes in the Elderly
Deng Y, Li N, Wang Y, Xiong C, Zou X
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3175-3185
Published Date: 16 October 2023
Development and Validation of a Nomogram Model for Accurately Predicting Depression in Maintenance Hemodialysis Patients: A Multicenter Cross-Sectional Study in China
Zhou X, Zhu F
Risk Management and Healthcare Policy 2024, 17:2111-2123
Published Date: 3 September 2024