Back to Journals » International Journal of Women's Health » Volume 17
Construction of a Nomogram Prediction Model for Individualized Prediction of Cervical Cancer Risk: A Retrospective Study
Authors Zhou W, Wang Y, Long H, Wang J
Received 7 June 2025
Accepted for publication 30 October 2025
Published 13 November 2025 Volume 2025:17 Pages 4435—4446
DOI https://doi.org/10.2147/IJWH.S541374
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Wenting Zhou,1– 3 Yili Wang,1– 3 Heming Long,1– 3 Jinfeng Wang1– 3
1Department of Oncology, The First Affiliated Hospital of Gannan Medical University, Ganzhou, Jiangxi, 341000, People’s Republic of China; 2Jiangxi “Flagship” Oncology Department of Synergy for Chinese and Western Medicine, Ganzhou, Jiangxi, 341000, People’s Republic of China; 3Jiangxi Provincial Unit for Clinical Key Oncology Specialty Development, Ganzhou, Jiangxi, 341000, People’s Republic of China
Correspondence: Jinfeng Wang, Department of Oncology, The First Affiliated Hospital of Gannan Medical University, No. 2201, Building 7, Zhongyang Park Shoufu, Zhanggong District, Ganzhou, Jiangxi, 341000, People’s Republic of China, Tel +8618370826061, Email [email protected]
Objective: To construct and validate a nomogram prediction model for the risk of cervical cancer.
Methods: From May 2021 to September 2023, 1234 female patients who underwent cervical cancer examinations were included in the training set and divided into a cervical cancer group (97 cases) and a non-cervical cancer group (1137 cases). In addition, 528 women who underwent cervical cancer screening between October 2023 and October 2024 were included as the validation set. Multivariate logistic regression analysis was used to identify independent risk factors. R software was used to establish a nomogram prediction model. Moreover, ROC curve analysis, the Hosmer-Lemeshow (H-L) test, calibration plots, and decision curve analysis were used to evaluate the predictive performance of the model.
Results: There was a statistically significant difference in the positivity of human papillomavirus (HPV) between the training set and the validation set (P< 0.05). Education level of junior high school or below, menarche age ≤ 14 years, first sexual intercourse age ≤ 20 years, number of sexual partners > 2, long-term use of hormonal contraceptives, number of deliveries > 2, HPV positivity, cervicitis, and systemic lupus erythematosus were independent risk factors for cervical cancer (P< 0.05). The AUCs of ROC curve for internal and external validation were 0.867 and 0.850, respectively. H-L test showed χ2=11.541 and 5.769, with P=0.173 and 0.673, respectively. The ideal curve and calibration curve had a high degree of overlap, and the nomogram model demonstrated good discrimination and calibration. In the clinical decision curve, the net benefit of the nomogram model was higher within the threshold probability range of 0.02– 0.78.
Conclusion: The Nomogram model based on nine identified factors provides a reliable tool to assist in the early detection and risk assessment of cervical cancer, which may help identify high-risk populations and guide targeted screening strategies in clinical practice.
Keywords: cervical cancer, disease risk, influencing factors, nomogram, prediction model
Introduction
According to data released by the International Agency for Research on Cancer (IARC), a specialized agency of the World Health Organization, there were approximately 660,000 new cases and 350,000 deaths from cervical cancer worldwide in 2024. In China, an estimated 150,700 new cases and 55,700 deaths from cervical cancer were reported in 2024.1,2 Cervical cancer is one of the most common cancers in women, with significant differences in the risk of developing cervical cancer among individuals. Personal medical history, economic, political, and social factors all influence the risk of cervical cancer.1 Although political factors are not direct causes of disease, they primarily influence cervical cancer outcomes at both the individual and population levels by shaping the structure of health systems, the accessibility of resources, and social norms.2 The primary etiology of cervical cancer is persistent infection with high-risk human papillomavirus (HPV), to which the vast majority of cases can be attributed.3 By the end of 2023, the cumulative HPV vaccination coverage among Chinese women aged 9–45 years had reached nearly 20%.4 At present, the cervical cancer screening rate among women of eligible age in China is 51.5%, with a coverage rate of 48.2% in rural areas, and the treatment rate approaches 90%.4 In many regions, cervical cancer is often detected only at an advanced stage. In China, approximately 50–60% of patents are diagnosed at a middle or advanced stage, where prognoses are generally poor.5 Cervical cancer progresses slowly and allows for early identification of precancerous lesions, making it one of the most preventable cancers. Early screening and treatment for cervical cancer can significantly reduce its incidence and mortality rates.6,7 Therefore, clinicians need to identify high-risk populations for cervical cancer and apply appropriate guidelines to provide medical guidance and decision-making. However, this remains challenging in clinical practice. Additionally, current studies lack sufficient exploration of cervical cancer risk factors and the early prediction of its onset. Based on this, the present study aims to analyze the relevant risk factors for cervical cancer and develop a visual nomogram prediction model for early screening of high-risk populations, providing an effective reference for reducing the clinical incidence and mortality rates of cervical cancer.
Materials and Methods
General Data
Women undergoing cervical cancer screening who met the inclusion and exclusion criteria were divided into two groups based on screening time. A total of 1234 women screened from May 2021 to September 2023 were included in the training set for constructing the nomogram model. Among them, 97 cases were in the cervical cancer group, and 1137 cases were in the non-cervical cancer group. Additionally, 528 women screened from October 2023 to October 2024 were included in the validation set for model validation.
Inclusion criteria: ① Diagnosis of cervical cancer met the established criteria8 and was confirmed by pathological diagnosis, with multiple suspicious cervical tissue biopsies obtained under colposcopic guidance for confirmation; ② Complete case data; ③ Local residents or individuals who had lived and worked in the area for more than one year; ④ Informed consent, and the study complied with ethical standards. Exclusion criteria: ① Concurrent diagnoses of other types of malignant tumors; ② Pregnant women; ③ Presence of coagulation disorders; ④ History of invasive cervical treatments; ⑤ Severe hepatic or renal dysfunction, or autoimmune diseases. The case collection flowchart is shown in Figure 1.
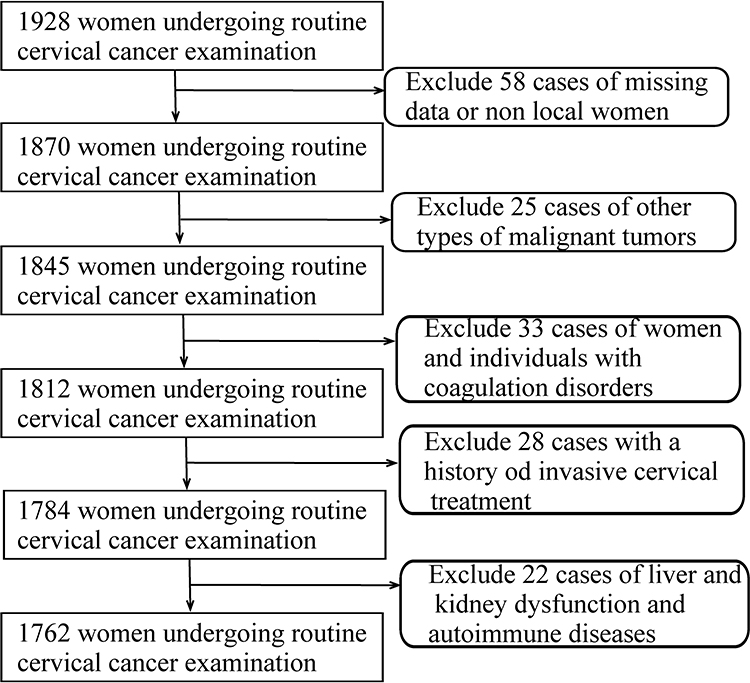 |
Figure 1 Flow chart of case collection. |
Data Collection
Patient data were obtained from the hospital’s electronic medical record system, including age, ethnicity, educational level, occupation, source of drinking water, age at menarche, age at first sexual intercourse, marital status, number of sexual partners, infrequent vulvar cleaning after intercourse (defined as failure to clean in ≥5 of 10 instances), family history of cervical cancer, smoking history (defined as continuous or cumulative smoking for ≥6 months during the lifetime), alcohol consumption history (defined as consuming on average >60 g/day of pure alcohol for men and >40 g/day for women), long-term use of hormonal contraceptives (defined as continuous use of steroid hormone contraceptives for >1 year), hypertension (defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on at least three separate occasions), diabetes (defined as 2-hour plasma glucose ≥11.1 mmol/L during an oral glucose tolerance test, or random plasma glucose ≥11.1 mmol/L in the presence of classic diabetic symptoms, including polydipsia, polyuria, polyphagia, and weight loss), number of births, genital bacterial infections, genital mycoplasma/chlamydia infections, cervicitis, arthritis, systemic lupus erythematosus, white blood cell count, lymphocyte count, platelet count, neutrophil count, and HPV positivity status.
Statistical Analysis
Statistical analyses were performed using SPSS 25.0 software. Continuous variables that conformed to a normal distribution were expressed as mean ± standard deviation ( ), and intergroup comparisons were conducted using independent-sample t-tests. Categorical variables were expressed as [n (%)], and intergroup comparisons were conducted using χ2-tests. Predictors with P < 0.05 in the univariate analysis were included in a multivariate logistic regression analysis to identify independent risk factors for cervical cancer. Based on the contribution of different predictors to cervical cancer risk in the multivariate analysis, a predictive nomogram model was constructed using the “RMS” package in R version 4.3.3. The model was internally validated using the Bootstrap method. The discriminative ability of the model was evaluated using the area under the curve (AUC) from ROC analysis. The Hosmer-Lemeshow (H-L) test and calibration curves were used to assess the agreement between predicted and observed outcomes, representing the model’s calibration. Clinical decision curves were employed to evaluate the clinical applicability of the model. A P-value < 0.05 was considered statistically significant.
), and intergroup comparisons were conducted using independent-sample t-tests. Categorical variables were expressed as [n (%)], and intergroup comparisons were conducted using χ2-tests. Predictors with P < 0.05 in the univariate analysis were included in a multivariate logistic regression analysis to identify independent risk factors for cervical cancer. Based on the contribution of different predictors to cervical cancer risk in the multivariate analysis, a predictive nomogram model was constructed using the “RMS” package in R version 4.3.3. The model was internally validated using the Bootstrap method. The discriminative ability of the model was evaluated using the area under the curve (AUC) from ROC analysis. The Hosmer-Lemeshow (H-L) test and calibration curves were used to assess the agreement between predicted and observed outcomes, representing the model’s calibration. Clinical decision curves were employed to evaluate the clinical applicability of the model. A P-value < 0.05 was considered statistically significant.
Results
Comparison of Data Between Training and Validation Sets
There were no statistically significant differences (P > 0.05) between the training and validation sets in terms of age, ethnicity, educational level, occupation, source of drinking water, age at menarche, age at first sexual intercourse, marital status, number of sexual partners, infrequent vulvar cleaning after intercourse, family history of cervical cancer, smoking history, alcohol consumption history, long-term use of hormonal contraceptives, hypertension, diabetes, number of births, genital bacterial infections, genital mycoplasma/chlamydia infections, cervicitis, arthritis, systemic lupus erythematosus, white blood cell count, lymphocyte count, platelet count, and neutrophil count. However, the difference in HPV positivity was statistically significant (P < 0.05). See Table 1.
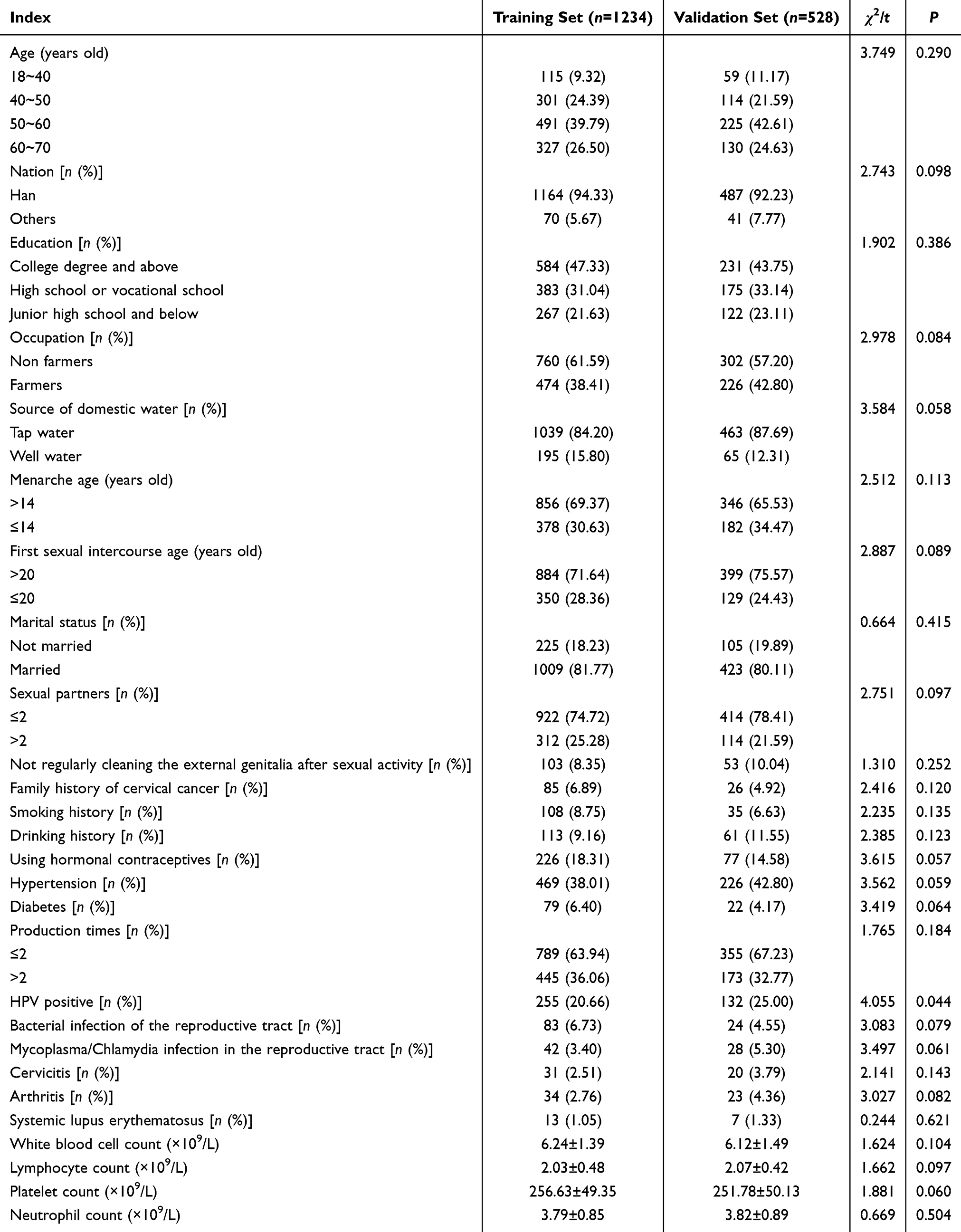 |
Table 1 Comparison of Training and Validation Set Data [n (%)/( |

Univariate Analysis of Cervical Cancer Risk in the Training Set
There were no statistically significant differences (P > 0.05) between the cervical cancer group and the non-cervical cancer group in the training set for age, ethnicity, occupation, source of drinking water, marital status, infrequent vulvar cleaning after intercourse, family history of cervical cancer, smoking history, alcohol consumption history, hypertension, diabetes, genital bacterial infections, genital mycoplasma/chlamydia infections, arthritis, white blood cell count, lymphocyte count, platelet count, and neutrophil count. However, statistically significant differences (P < 0.05) were observed for educational level, age at menarche, age at first sexual intercourse, number of sexual partners, long-term use of hormonal contraceptives, number of births, HPV positivity, cervicitis, and systemic lupus erythematosus. See Table 2.
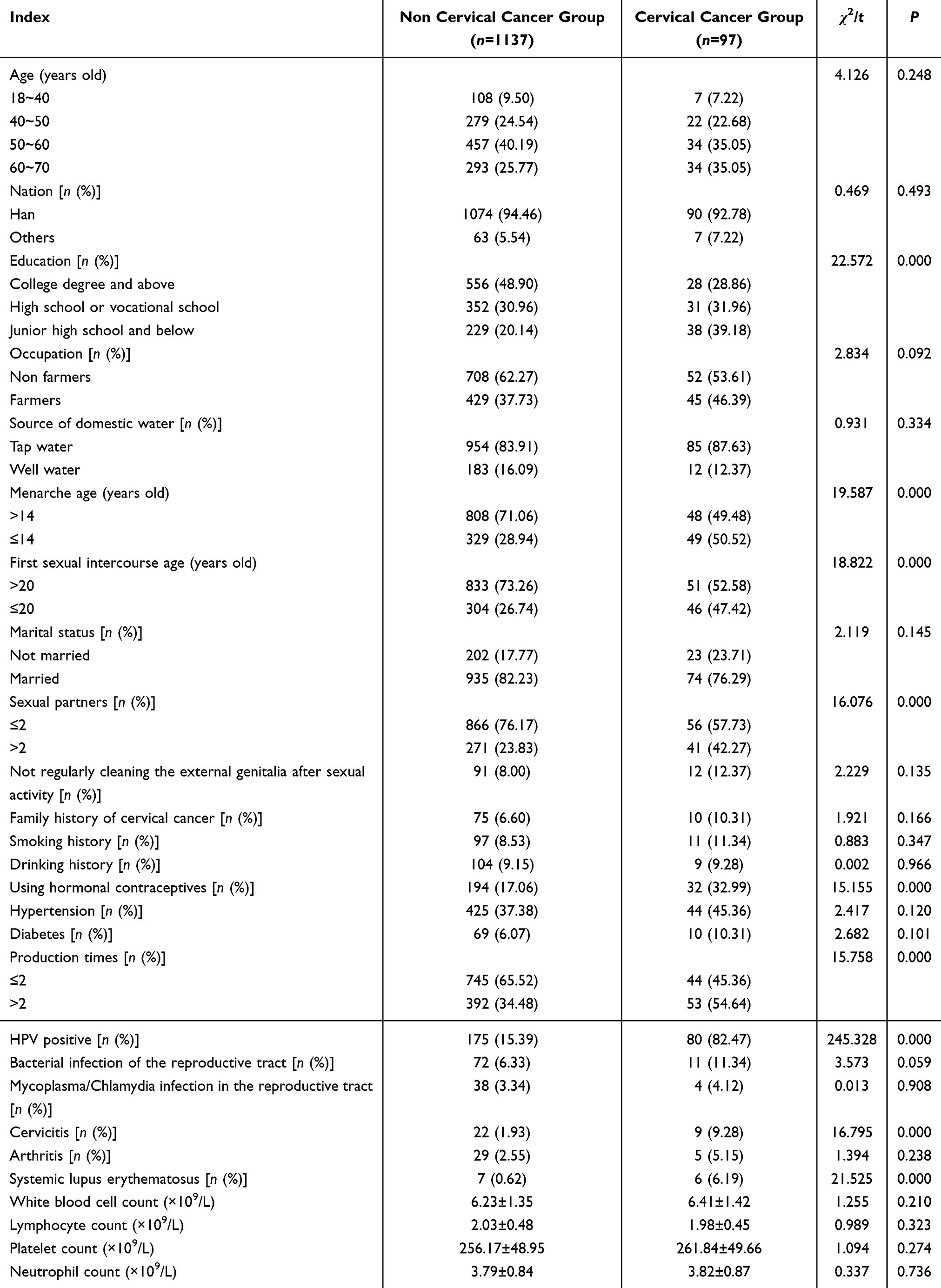 |
Table 2 Univariate Analysis of Cervical Cancer Risk in the Training Set [n (%)/ ( |

Logistic Regression Analysis
Nine indicators identified from univariate analysis were included in the multivariate logistic regression analysis. The results indicated that the following factors were independent risk factors for cervical cancer (P < 0.05): Educational level of middle school or below (OR = 3.320, 95% CI = 1.880–5.862); Age at menarche ≤14 years (OR = 2.463, 95% CI = 1.532–3.959); Age at first sexual intercourse ≤20 years (OR = 2.578, 95% CI = 1.595–4.166); Number of sexual partners >2 (OR = 2.521, 95% CI = 1.547–4.109); Long-term use of hormonal contraceptives (OR = 2.809, 95% CI = 1.658–4.758); Number of births >2 (OR = 2.021, 95% CI = 1.260–3.244); HPV positivity (OR = 7.387, 95% CI = 4.170–13.086); Cervicitis (OR = 6.368, 95% CI = 2.338–17.343); Systemic lupus erythematosus (OR = 5.347, 95% CI = 4.079–7.743). The variable assignment table is shown in Table 3, and the detailed results are shown in Table 4.
 |
Table 3 Variable Assignment Table |
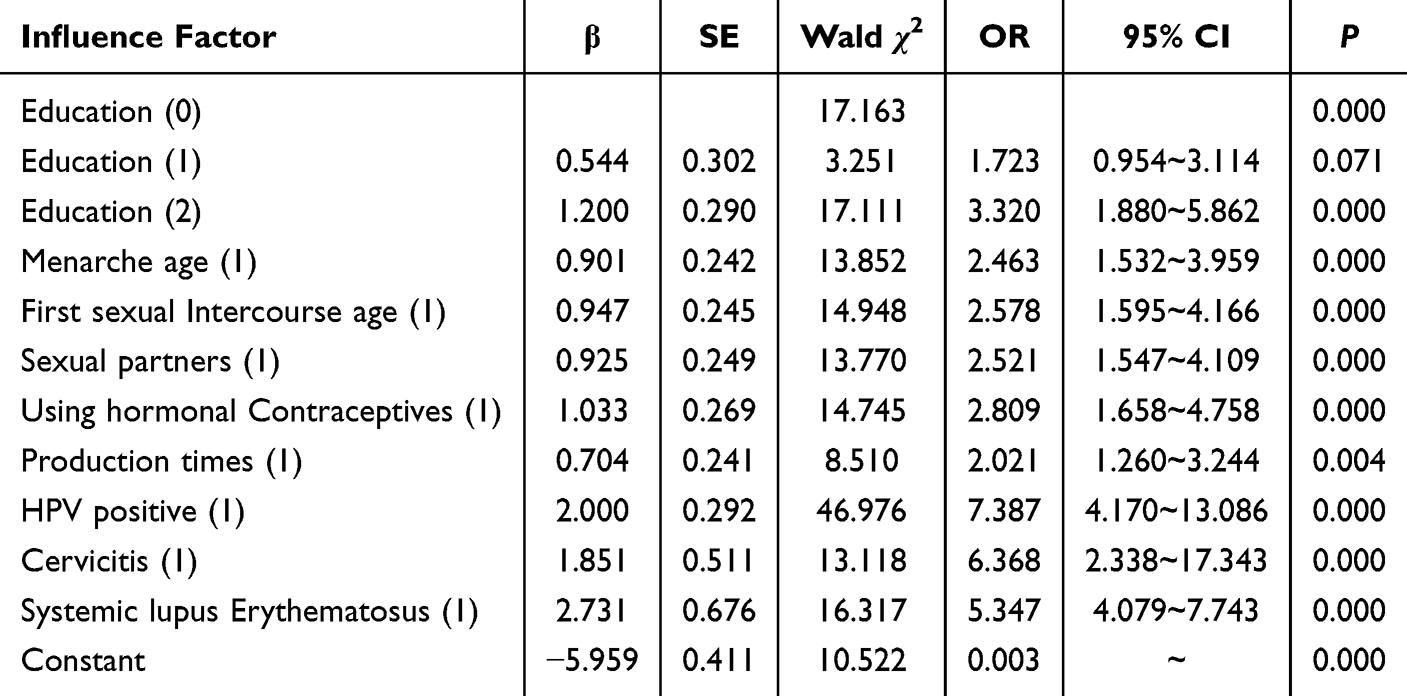 |
Table 4 Multivariate Logistic Regression Analysis of Cervical Cancer Risk |
Development of the Nomogram Prediction Model
The nomogram prediction model was developed using R software based on the nine predictive factors identified through logistic regression analysis: educational level, age at menarche, age at first sexual intercourse, number of sexual partners, long-term use of hormonal contraceptives, number of births, HPV positivity, cervicitis, and systemic lupus erythematosus. The equation for the model is: Logit (P) = −5.959 + 3.320 × Educational level + 2.463 × Age at menarche + 2.578 × Age at first sexual intercourse + 2.521 × Number of sexual partners + 2.809 × Long-term use of hormonal contraceptives + 2.021 × Number of births + 7.387 × HPV positivity + 6.368 × Cervicitis + 5.347 × Systemic lupus erythematosus. Each variable corresponds to a specific value on the score axis at the top of the model. The final total score is calculated by summing the corresponding values, which is then matched to the value on the total score axis to determine the predicted probability of cervical cancer on the probability axis at the bottom of the model. See Figure 2.
 |
Figure 2 Nomogram prediction model. |
Evaluation of Discrimination and Calibration in the Training and Validation Sets
The AUC of the ROC curve for internal validation was 0.867 (95% CI: 0.834–0.901), while the AUC for external validation was 0.850 (95% CI: 0.814–0.885), indicating good discrimination of the nomogram model. See Figure 3. The H-L test for internal validation yielded a P-value of 0.173 > 0.05 with χ2 = 11.541, and the H-L test for external validation yielded a P-value of 0.673 > 0.05 with χ2 = 5.769. The high degree of overlap between the ideal curve and the calibration curve suggests that the nomogram model has good calibration. See Figure 4.
 |
Figure 3 ROC curve of cervical cancer risk ((A) Internal verification; (B) External Verification). |
 |
Figure 4 Calibration curve of cervical cancer risk ((A) Internal verification; (B) External Verification). |
Evaluation of Clinical Utility of the Nomogram Prediction Model
The horizontal axis represents the threshold probability, and the vertical axis represents net benefit. The All line represents the net benefit when all individuals are considered to have cervical cancer risk and receive clinical intervention, while the None line represents the net benefit when no individuals are considered to have cervical cancer risk and no clinical intervention is conducted. The results showed that when the threshold probability ranged from 0.02 to 0.78, the nomogram prediction model yielded higher net benefits. The model line was located in the upper-right region relative to the All and None lines, indicating that the model has high clinical utility. See Figure 5.
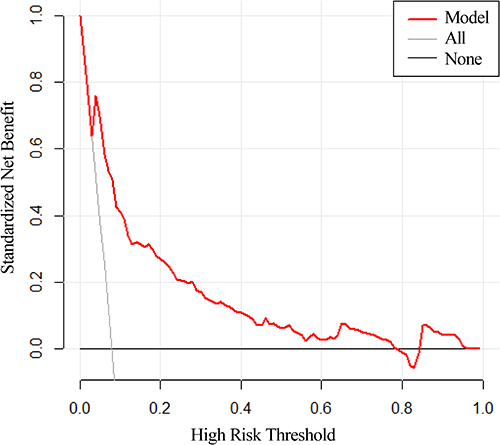 |
Figure 5 Clinical decision curve of cervical cancer risk. |
Discussion
Identifying high-risk cervical cancer patients and implementing individualized treatment strategies to improve prognosis remains a challenge for clinicians. This study found significant differences between cervical cancer and non-cervical cancer patients in terms of educational level, age at menarche, age at first sexual intercourse, number of sexual partners, long-term use of hormonal contraceptives, number of births, HPV positivity, cervicitis, and systemic lupus erythematosus. Multivariate analysis confirmed these factors as independent risk factors for cervical cancer. A nomogram model integrating these independent risk factors demonstrated high predictive performance.
Previous studies have identified low socioeconomic status or low educational levels as risk factors for cervical cancer,9,10 consistent with our findings. Women with lower educational levels often have poorer healthcare awareness and less knowledge about cervical diseases, which may delay medical care and increase exposure to harmful factors, thereby raising their risk of cervical cancer. Evidence indicates that women with an earlier age at menarche are at higher risk of cervical cancer, possibly due to prolonged exposure to hormones such as estrogen and progesterone during their lifetime.11 In this study, the younger the age at first sexual intercourse, the higher the risk of cervical cancer. Similarly, a study in China found that women who began sexual activity before the age of 19 had an increased risk of HPV infection, with an OR of 1.51.12 This may be because the reproductive tract in women aged 20 and below is not fully mature, making early sexual activity more likely to cause cervical damage and atypical hyperplasia of cervical squamous epithelium, thereby increasing cervical cancer risk. Studies conducted in the United States, China, and Tunisia have shown a significant association between having two or more sexual partners and HPV infection.13,14 A prior analysis reported that the odds ratios (ORs) for cervical cancer incidence significantly increased to 1.36, 1.93, and 2.24 for women using oral contraceptives for 2–5 years, >5 years, and >10 years, respectively.15 This study similarly found that long-term use of hormonal contraceptives is an independent risk factor for cervical cancer. This is likely because long-term contraceptive use affects hormonal secretion levels in women, increasing estrogen and progesterone levels, which indirectly contribute to cervical cancer development. In this study, a higher number of births and HPV positivity were associated with an increased risk of cervical cancer. Zhao et al16 similarly identified the number of deliveries, HPV infection, and genital infections as risk factors for cervical cancer. Their study suggested that women with a higher number of deliveries experience elevated estrogen levels during pregnancy, and frequent deliveries cause greater stimulation and potential infection of the cervix, increasing cervical cancer risk. HPV infection is currently considered one of the most critical factors in the development of cervical cancer and precancerous lesions. Most cervical cancer patients have HPV infections, and HPV DNA integrates into host DNA, enabling uncontrolled replication that may lead to carcinogenesis.17 Cervicitis contributes to cervical cancer risk primarily because prolonged inflammation weakens the body’s ability to resist pathogenic bacteria, making it more susceptible to cervical cancer upon exposure to such pathogens.18 Systemic lupus erythematosus (SLE) increases the risk of cervical cancer by causing immune system dysregulation, which promotes persistent HPV infection and subsequent cervical cancer progression.19
A predictive model was constructed based on the above influencing factors and was visualized as a nomogram. The ROC curve analysis results for both the training and validation sets in this study yielded AUC values >0.8, indicating that the nomogram model effectively distinguishes between high-risk and low-risk women for cervical cancer. In the consistency and calibration tests, the calibration curve showed a good fit, with P-values >0.05, suggesting high consistency between the predicted probabilities of high cervical cancer risk and the actual outcomes. This demonstrates a high level of predictive accuracy. Additionally, clinical decision curve analysis revealed that the nomogram constructed in this study has the potential for actual prediction and treatment, thereby providing a certain net benefit. However, it still requires further improvement and validation, with more factors incorporated to enhance the applicability of the model. This study visualized the logistic regression equation results in the form of a nomogram, making the model more intuitive and convenient for calculation, thereby facilitating its practical application in clinical settings.20–22 For patients with predicted probabilities close to or above 0.5, early interventions can be implemented based on factors such as long-term use of hormonal contraceptives, the number of births, and HPV positivity. The nomogram developed in this study can be applied in the following ways: ① Improving screening efficiency and accuracy, and optimizing the allocation of medical resources: by providing precise risk prediction for women and offering stratified management recommendations, it can assist clinicians in determining which populations require more frequent follow-up or more aggressive interventions (eg, colposcopic biopsy), and which populations may extend screening intervals to avoid overtreatment. ② Assisting clinical decision-making and promoting personalized medicine: supporting clinicians in determining the feasibility of fertility-preserving procedures such as cervical conization.
However, this study has inherent limitations that require further investigation. First, the retrospective study design and relatively limited sample size restrict the generalizability and applicability of the findings, which also resulted in a relatively high incidence of cervical cancer in this study. In the future, the enrollment period should be extended to further clarify the incidence. Second, although the study aimed to integrate a comprehensive set of influencing factors, certain inflammation- and nutrition-related biomarkers associated with the risk of cervical cancer were not fully included. Third, the study lacks external validation from other centers, and future collaboration with other hospitals is needed to externally validate the effectiveness of the nomogram. Fourth, as a cross-sectional study, patients with cervical cancer were already diagnosed at the time of enrollment, making it impossible to clarify their precancerous conditions. Further prospective, multi-center studies are needed to verify the effectiveness of the nomogram in improving cervical cancer screening rates and to clarify the precancerous conditions of enrolled patients.
Conclusion
In summary, the nomogram model developed in this study demonstrated acceptable calibration, discrimination, and clinical utility. Nevertheless, given the single-center and retrospective design, the model requires further external validation, refinement, and integration of additional diagnostic data. With future improvement, this tool has the potential to serve as a practical instrument for predicting and evaluating cervical cancer risk in clinical settings. For individuals identified as high-risk, targeted strategies may be implemented to enhance screening awareness, including online and offline health education, population-specific communication, and promotion of HPV vaccination. From a public health perspective, policy support and resource allocation—such as incorporating screening into essential health services, providing free or subsidized screening, exploring subsidized HPV vaccination programs, and strengthening the linkage between screening and diagnosis/treatment—will be essential to maximize the model’s effectiveness and clinical applicability.
Data Sharing Statement
The original contributions presented in this study are included in the article.
Ethics Approval
The study involving human participants was reviewed and approved by the Ethics Committee of The First Affiliated Hospital of Gannan Medical University (No. LLSC-2022071502) and was in accordance with the 1964 Helsinki Declaration. Written informed consent was obtained from all patients prior to participation.
Consent for Publication
All authors provided consent for publication.
Funding
There is no funding to report.
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Gold RS, Williams M, Wainstein HM. Cervical cancer screening in high-risk patients: clinical challenges in primary care. Cleve Clin J Med. 2024;91(11):693–703. doi:10.3949/ccjm.91a.24023
2. Farajimakin O. Barriers to cervical cancer screening: a systematic review. Cureus. 2024;16(7):e65555. doi:10.7759/cureus.65555
3. Włoszek E, Krupa K, Skrok E, et al. HPV and cervical cancer-biology, prevention, and treatment updates. Curr Oncol. 2025;32(3):122. doi:10.3390/curroncol32030122
4. Zhao C, Zhao Y, Li J, et al. Opportunities and challenges for human papillomavirus vaccination in China. Hum Vaccin Immunother. 2024;20(1):2329450. doi:10.1080/21645515.2024.2329450
5. Galicia-Carmona T, Arango-Bravo EA, Coronel-Martínez JA, et al. Advanced, recurrent, and persistent cervical cancer management: in the era of immunotherapy. Front Oncol. 2024;14:1392639. doi:10.3389/fonc.2024.1392639
6. Swanson AA, Pantanowitz L. The evolution of cervical cancer screening. J Am Soc Cytopathol. 2024;13(1):10–15. doi:10.1016/j.jasc.2023.09.007
7. Wang M, Huang K, Wong MCS, et al. Global cervical cancer incidence by histological subtype and implications for screening methods. J Epidemiol Glob Health. 2024;14(1):94–101. doi:10.1007/s44197-023-00172-7
8. Abu-Rustum NR, Yashar CM, Bean S, et al. NCCN guidelines insights: cervical cancer, version 1.2020. J Natl Compr Canc Netw. 2020;18(6):660–666. doi:10.6004/jnccn.2020.0027
9. Wakwoya EB, Gemechu KS, Dasa TT. Knowledge of cervical cancer and associated factors among women attending public health facilities in eastern ethiopia. Cancer Manag Res. 2020;12:10103–10111. doi:10.2147/CMAR.S262314
10. Nang DW, Tukirinawe H, Okello M, et al. Prevalence of high-risk human papillomavirus infection and associated factors among women of reproductive age attending a rural teaching hospital in western Uganda. BMC Womens Health. 2023;23(1):209. doi:10.1186/s12905-023-02342-y
11. Okyere J, Ayebeng C, Dickson KS. Early age at menarche and history of sexually transmitted infections significantly predict cervical cancer screening uptake among women aged 25–49 years: evidence from the 2021 Côte d’Ivoire demographic and health survey. BMC Health Serv Res. 2024;24(1):423. doi:10.1186/s12913-024-10881-9
12. Yang D, Zhang J, Cui X, et al. Risk factors associated with human papillomavirus infection, cervical cancer, and precancerous lesions in large-scale population screening. Front Microbiol. 2022;13:914516. doi:10.3389/fmicb.2022.914516
13. Ardhaoui M, Letaief H, Ennaifer E, et al. The prevalence, genotype distribution and risk factors of human Papillomavirus in Tunisia: a National-Based Study. Viruses. 2022;14(10):2175. doi:10.3390/v14102175
14. Yang H, Xie Y, Guan R, et al. Factors affecting HPV infection in U.S. and Beijing females: a modeling study. Front Public Health. 2022;10:1052210. doi:10.3389/fpubh.2022.1052210
15. Asthana S, Busa V, Labani S. Oral contraceptives use and risk of cervical cancer-A systematic review & meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2020;247:163–175. doi:10.1016/j.ejogrb.2020.02.014
16. Zhao M, Gu R-Y, Ding S-R, et al. Risk factors of cervical cancer among ethnic minorities in Yunnan Province, China: a case-control study. Eur J Cancer Prev. 2022;31(3):287–292. doi:10.1097/CEJ.0000000000000704
17. Molina MA, Steenbergen RDM, Pumpe A, et al. HPV integration and cervical cancer: a failed evolutionary viral trait. Trends Mol Med. 2024;30(9):890–902. doi:10.1016/j.molmed.2024.05.009
18. Sahasrabuddhe VV. Cervical cancer: precursors and prevention. Hematol Oncol Clin North Am. 2024;38(4):771–781. doi:10.1016/j.hoc.2024.03.005
19. Chen Y, Wu X, Liu L. Association between systemic lupus erythematosus and risk of cervical atypia: a meta-analysis. Lupus. 2021;30(13):2075–2088. doi:10.1177/09612033211048129
20. Wang S, Zhao M, Gao Z, et al. A survival nomogram involving nutritional-inflammatory indicators for cervical cancer patients receiving adjuvant radiotherapy. J Cancer. 2024;15(17):5773–5785. doi:10.7150/jca.100564
21. Gu Z, Yang C, Zhang K, et al. Development and validation of a nomogram for predicting sever cancer-related fatigue in patients with cervical cancer. BMC Cancer. 2024;24(1):492. doi:10.1186/s12885-024-12258-x
22. Guo Q, Gao Y, Lin Y, et al. A nomogram of preoperative indicators predicting lymph vascular space invasion in cervical cancer. Arch Gynecol Obstet. 2024;309(5):2079–2087. doi:10.1007/s00404-024-07385-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predicting the Risk of Unplanned Readmission at 30 Days After PCI: Development and Validation of a New Predictive Nomogram
Xu W, Tu H, Xiong X, Peng Y, Cheng T
Clinical Interventions in Aging 2022, 17:1013-1023
Published Date: 5 July 2022
Development and Validation of a Nomogram for Predicting 28-Day Mortality on Admission in Elderly Patients with Severe Community-Acquired Pneumonia
Song Y, Wang X, Lang K, Wei T, Luo J, Song Y, Yang D
Journal of Inflammation Research 2022, 15:4149-4158
Published Date: 21 July 2022
Development and Validation of a Prediction Model for Chronic Post-Surgical Pain After Thoracic Surgery in Elderly Patients: A Retrospective Cohort Study
Wu XD, Zeng FF, Yu XX, Yang PP, Wu JP, Xv P, Wang HT, Pei YM
Journal of Pain Research 2022, 15:3079-3091
Published Date: 29 September 2022
Nomogram to Predict Radiation Enteritis in Cervical Squamous Cell Carcinoma
Wang J, Hu G
Cancer Management and Research 2022, 14:3303-3311
Published Date: 25 November 2022
Influencing Factors of New-Onset Atrial Fibrillation in Sepsis Patients and Construction of a Nomogram Prediction Model: Based on LASSO Regression
Tang J, Ou W, Han B, Wen W
International Journal of General Medicine 2026, 19:565434
Published Date: 22 January 2026