Back to Journals » Cancer Management and Research » Volume 14
Nomogram to Predict Radiation Enteritis in Cervical Squamous Cell Carcinoma
Received 11 August 2022
Accepted for publication 3 November 2022
Published 25 November 2022 Volume 2022:14 Pages 3303—3311
DOI https://doi.org/10.2147/CMAR.S383909
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bilikere Dwarakanath
Jinyun Wang, Ge Hu
Department of Urogenital Oncology Radiotherapy, Hefei Cancer Hospital, Chinese Academy of Sciences, Hefei, People’s Republic of China
Correspondence: Ge Hu, Department of Urogenital Oncology Radiotherapy, Hefei Cancer Hospital, Chinese Academy of Sciences, No. 350, Shushanhu Road, Shushan District, Hefei City, Anhui Province, People’s Republic of China, Tel +86 551-65596503, Email [email protected]
Purpose: To investigate the risk factors of radiation enteritis in patients with cervical cancer after radiotherapy.
Patients and Methods: Retrospective analysis 90 cervical cancer patients receiving radiation therapy from January 2019 to May 2021 in Hefei Cancer Hospital, Chinese Academy of Sciences. The patients were divided into radiation enteritis group and control group according to the radiation enteritis, the continuous variable were analyzed by ROC to obtain the best truncation value, and univariate and multifactorial logistic regression models analyzed the independent risk factors for radiation enteritis in cervical cancer patients. Nomogram was constructed and evaluated based on independent risk factors.
Results: The radiation enteritis incidence rate was 35.56%. Univariate analysis found that hemoglobin (OR=4.25, 95% CI=1.43~13.73), albumin (OR=2.33, 95% CI=0.95~5.83), hypertension (OR=3.57, 95% CI=1.24~10.90), sigmoid colon V45(OR=0.41, 95% CI=0.15~1.03), external radiation dose (OR=0.45, 95% CI=0.18~1.08), age (OR=2.27, 95% CI=0.90~6.18), total T lymphocyte count (OR=2.4, 95% CI=0.97~6.29)(p< 0.1) are risk factors for radiation enteritis. Multivariate logistic regression analysis found that hemoglobin (p=0.001, OR=13.22, 95% CI=3.03~72.65), albumin (p=0.003, OR=6.76, 95% CI=2.08~25.67), total T lymphocyte count (p=0.015, OR=4.79, 95% CI=1.45~13.38) were independent risk factors for radiation enteritis. Based on the above predictors, a nomogram model is established, and the area under the model fit, C-index, and ROC curve indicates that the model has good prediction efficiency and differentiation.
Conclusion: Hemoglobin, albumin, and total T lymphocyte count are risk factors for radiation enteritis in cervical cancer patients under radiotherapy, the nomogram model based on the above risk factors has good predictive efficacy and can provide a reference for radiation enteritis prediction.
Keywords: cervical cancer, radiotherapy, radiation enteritis, risk factors, nomogram
Introduction
Cervical cancer is one of the most common malignancies in women,1,2 and its incidence varies significantly from country to country, mainly in developing countries.3,4 China is the largest country for cervical cancer, with about 140,000 new cases and about 30,000 deaths per year.5 The incidence of cervical cancer is age-related and begins to rise after 25 years, peaking around the age of 40 in developed countries and peaking at 55 to 69 years in developing countries. With socio-economic development, universal HPV screening, and HPV vaccination, the incidence of cervical cancer has declined.6–8 Still, cases of advanced cervical cancer remain widespread due to atypical early symptoms of cervical cancer.9,10 The primary treatment modalities for cervical cancer include surgery and radiation therapy, for locally advanced or intolerable surgery patients, concurrent chemoradiation is the best treatment, patients with medium and high-risk factors after radical hysterectomy can choose radiation therapy as an adjunctive therapy, radiation therapy is very important in the treatment of cervical cancer.11–13 Radiation enteritis (RE) is a common side effect of radiation therapy in patients with cervical cancer, the clinical manifestations are mainly abdominal pain, diarrhea, and bloody stools, and rectovaginal fistula can be seen in severe cases, which seriously affects the quality of life of patients.11,14 At present, the treatment of radiation enteritis is mainly based on symptomatic treatment, so how to effectively predict the occurrence of RE has always been the focus of clinical cervical cancer radiotherapy.
Several factors associated with an increased risk of gastrointestinal toxicity have been identified.15 Previous abdominal surgery increases the risk of radiation toxicity.16 Combining chemotherapy with radiation has been reported to increase the rate of acute intestinal toxicity.16–19 Individual patient phenotypic factors such as age and nutritional status, co-morbid disease such as hypertension and diabetes have been suggested to influence the susceptibility to radiation injury.20,21 Radiation-induced lesions are associated with infiltration of immune-inflammatory cells from the blood and/or the lymph circulation such as T-lymphocytes. Treatment factors, such as total radiation dose, dose per fraction, technique, and Organs at risk (OAR) dose also have a variable association with RE. The current means of predict RE are still far from clinical application.22 It is reported that radionuclide-labeled targeting molecules like 89Zr-labeled anti-γH2AX may be used to precisely diagnose and evaluate radiation damage.23 Moreover, some results suggest that gut microbiota can offer a set of biomarkers for prediction in RE. However, most of the predictive means are still in the experimental stage, therefore, it is very important to establish a method for rapid assessment of RE based on clinical available data.
In this study, we collected common clinical data of patients including general information of the patients such as age, basic disease history, hematological examination, and lymphocyte subpopulations, in order to built a nomogram model to predict the occurrence of RE during radiotherapy in cervical cancer patients.
Materials and Methods
Study Design
Retrospective analysis of 90 cervical cancer patients who received radiotherapy from January 2019 to May 2021 at Hefei Cancer Hospital, Chinese Academy of Sciences. The inclusion criteria for patients are applied: (1) All patients were pathologically diagnosed with cervical malignancy; (2) The patient’s clinical data is complete; (3) The follow-up time after radiotherapy ≥ 12 months; (4) Have not received abdominal and pelvic radiotherapy before; (5) No cognitive or communication disorders. Exclusion criteria: (1) long-term use of hormones or immunosuppressants; (2) Patients with a previous history of chronic intestinal diseases; (3) The expected survival period <6 months; (4) Participate in contemporaneous studies of other people who may have an impact on the results of the study. Patients were divided into RE groups (n=32) and control groups (n=58) according to RE, and the general clinical data of patients in both groups are detailed in Table 1.
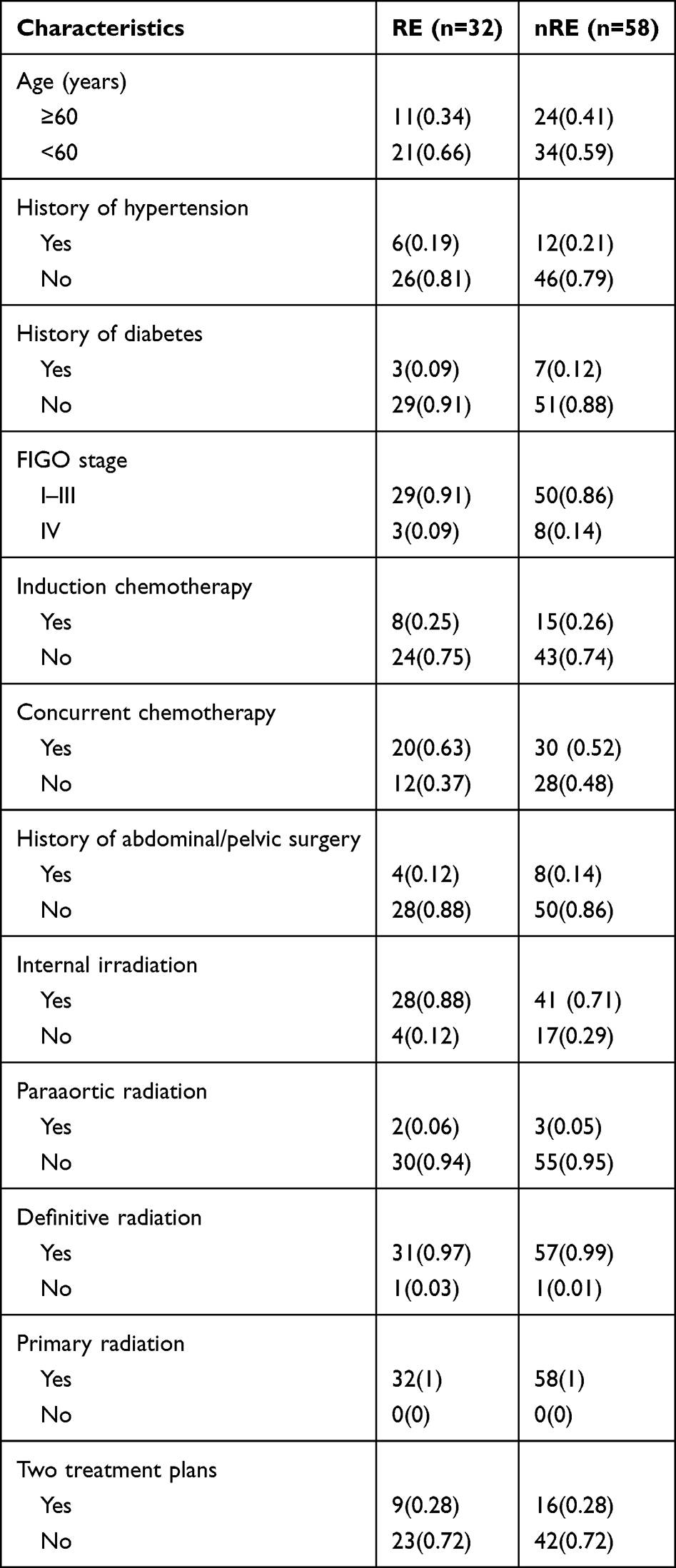 |
Table 1 The Characteristics of Patients with RE |
This study was conducted with permission by Ethics Review Committees of Hefei Cancer Hospital, Chinese Academy of Sciences. We confirm that we have obtained ethical approval to conduct the study and publish the dataset. The obtained data did not contain patient identifiers. Patient data was retrieved from our hospital database without intervention and therefore no patient consent was required, the study is exempted from informed consent, the consent waiver was approved by Ethics Review Committees of Hefei Cancer Hospital, Chinese Academy of Sciences. This study complies with the Declaration of Helsinki.
Data Collection
All patients were treated within volumetric intensity-modulated radiotherapy equipped with Elekta Axesse linear accelerator, large-aperture CT analog positioning machine, and Beijing Kelinzhong HDR three-dimensional after-installation treatment machine. Prescription dose for external irradiation: pelvic lymphatic drainage zone 45 to 50.4 Gy, positive lymph nodes 56 to 60.2 Gy, if present in the presence of para-aortic or inguinal lymphatic drainage zone 45 Gy. The constraints of the plan was that at least 95% of the PTV received 100% of the prescription dose, and with the maximal dose in the PTV<110% of the prescription dose. Gynecological examinations were performed twice a week during treatment. If the tumor lesion regresses significantly, or the localization scan CT suggests the rectum is not satisfied emptied, we will reposition and make a new treatment plan at 15–20 times of radiotherapy. OARs need to evaluate were the bladder, small intestine, rectum, kidney, femoral head, and spinal cord. The dose constraints of the OARs were based on the Radiation Therapy Oncology Group 1203 trial guidelines as follows: bladder V45 <35%, small intestine V45 <30%, rectum V45 < 60%, kidneys V18 <20%, femoral head V30 <15%, and spinal cord max <45Gy.The internal brachytherapy treatment was guided by CT and completed three-dimensional brachytherapy under the guidance of 192Ir, 2 to 3 times per week, and the single prescription dose was 5–6Gy. The biological dose equivalent to 2Gy fractions (EQD2) was also calculated for maximum dose points for OAR, using the equation: EQD2=D×[(d+α/β)/(2+α/β)], the α/β ratio is 10Gy for HR-CTV and 3Gy for OARs. Regarding the dose-volume parameters, the D90 and D98 of the HR-CTV and the D2cc of the rectum, sigmoid colon, and bladder were calculated, recorded, and reported at every brachytherapy session. The D2cc of the rectum and sigmoid colon ≤70GyEQD2, D2cc of the bladder ≤ 90GyEQD2, when the dose constraints of the HR-CTV and OARs were not achieved simultaneously, the constraints of the OARs were prioritized. The concurrent chemotherapy regimen is cisplatin monotherapy, and the adjuvant chemotherapy is treated with paclitaxel plus platinum chemotherapy for four cycles.
Individual patient factors were collected before radiotherapy: age, smoking history, hypertension, diabetes, tumor stage, and hematological data includes ALB (albumin), HGB (hemoglobin), CD4/CD8, auxiliary/induced T cells, inhibitory/cytotoxic T cells, total B lymphocyte count, total T lymphocyte count). Treatment characteristics (radiotherapy dose, chemotherapy, small intestine V45, sigmoid colon V45, rectum V45, rectum D2cc and sigmoid colon D2cc), were collected at the end of the entire treatment.24
Patients were recorded weekly according to the Common Adverse Events Evaluation Criteria (CTCAE) 5.0 grading criteria, and the severity of RE was graded, grade 1 compared to baseline: no more than 4 increases in the frequency of stools per day; grade 2: the number of seats increased by 4–6 times/day; grade 3: the number of chairs increased by more than 6 times/day; grade 4: life-threatening patients and require urgent treatment; grade 5: causes death in the patient.
Patients were followed up by phone once a month, outpatient follow-up was once every 3 months, and the total follow-up time was 1 year after the end of radiotherapy. The study was followed up to 30 May 2022. Twenty-two patients had grade 1 RE, 7 patients developed grade 2 RE, 3 patients developed grade 3 RE, and no grade 4 or higher RE.
Statistical Analyses
SPSS 20.0 were used for statistical analysis. The counting data is represented by example(%) and uses chi-square tests. Medical statistical software is used to plot the working characteristic curve of continuous variable subjects and obtain the best truncation value, and convert the binary categorical variable according to the best truncation value. Univariate and multivariate logistic regression analysis was used to determine the influencing factors of RE in radiation therapy in patients with cervical cancer. Based on the results of multivariate logistic regression analysis, the RMS package in R version 3. 5.2 was used to draw the nomogram model and validates it to calculate consistency (C-index). The difference was statistically significant for the one-factor analysis p<0.1, and the difference was statistically significant for the multivariate logistic regression analysis p<0.05.
Results
Clinical Data Analysis of RE Group and Control Group
RE developed in 32 patients with a rate of 35.56%. For continuous clinical data (age (years), CD4/CD8, auxiliary/induced T cells, inhibitory/cytotoxic T cells, HGB(g/L), ALB(g/L), external radiation dose(Gy), total B lymphocyte count(%), total T lymphocyte count(%), small intestine V45, sigmoid colon V45, rectum V45, sigmoid colon D2cc, rectum D2cc), the ROC curve was analyzed according to whether the patient had RE, the best truncation values were 51 years, 1.19, 50.05, 29.53, 97g/L, 40.6g/L, 50Gy, 11.85, 66.78, 6.35, 69.77, 40.9, 72.09, 79.88(Table 2).
 |
Table 2 ROC Curve Analysis of Continuous Clinical Data in the Diagnosis of RE |
Factors Influencing the Occurrence of RE in Radiation Therapy in Cervical Cancer Patients
According to the truncation value obtained by the ROC curve, the results of the univariate analysis showed that HGB (OR=4.25, 95% CI=1.43~13.73), ALB (OR=2.33, 95% CI=0.95~5.83), hypertension (OR=3.57, 95% CI=1.24~10.90), sigmoid colon V45(OR=0.41, 95% CI=0.15~1.03), external radiation dose (OR=0.45, 95% CI=0.18~1.08), age (OR=2.27, 95% CI=0.90~6.18), total T lymphocyte count (OR=2.4, 95% CI=0.97~6.29)(p<0.1) are risk factors for radiation enteritis (p <0.2)(Table 3). The results of multivariate logistic regression analysis showed that HGB (p=0.001, OR=13.22, 95% CI=3.03~72.65), ALB (p=0.003, OR=6.76, 95% CI=2.08~25.67), total T lymphocyte count (p=0.015, OR=4.79, 95% CI=1.45~13.38) were independent risk factors for RE in cervical cancer patients (p<0.05)(Table 4).
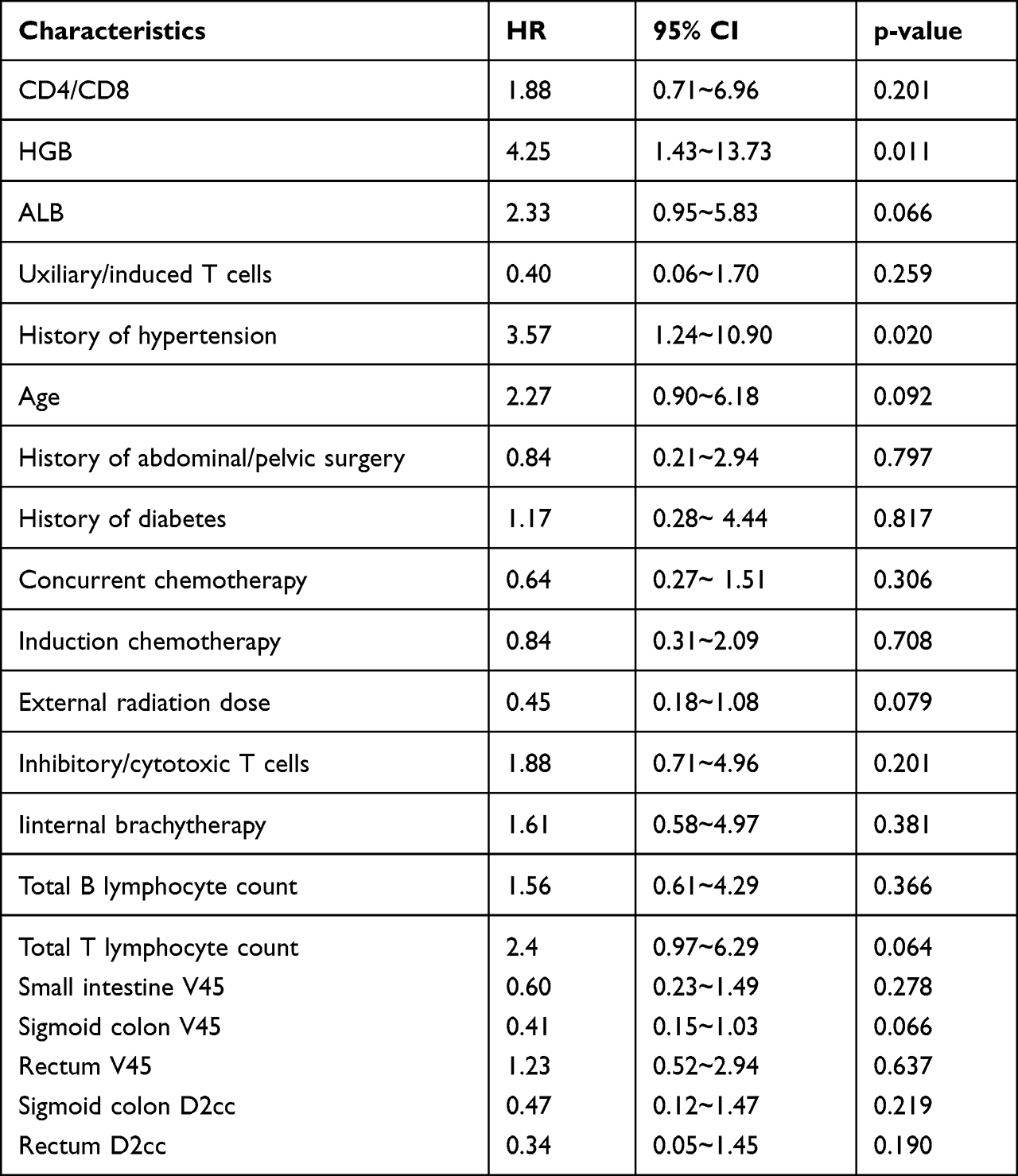 |
Table 3 Univariate Analysis of the Factors Associated with RE |
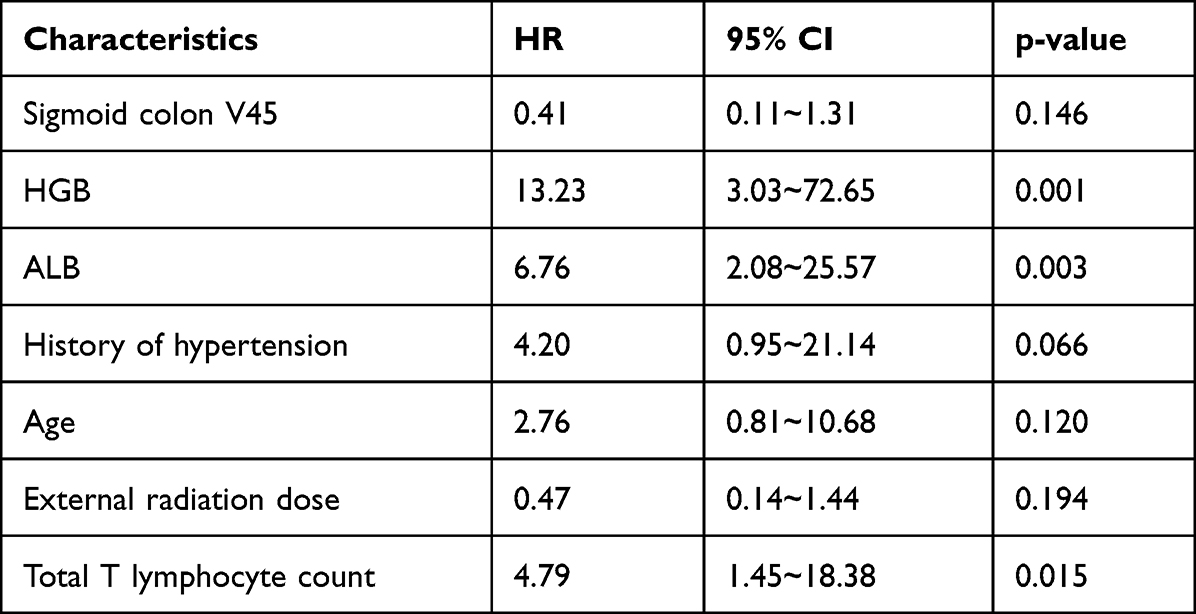 |
Table 4 Multivariate Analysis of the Factors Associated with RE |
Establishment and Evaluation of Nomogram Model
Based on the independent predictors obtained by multivariate logistic regression analysis, a risk assessment line chart model for predicting the occurrence of RE during radiation therapy in cervical cancer patients was established, and the left endpoint of each scoring line corresponded to 0 points, with a total score of 230 points (Figure 1). In this model, HGB ≤97g/L was the strongest predictor of RE occurrence (corresponding to a score of 100 points), followed by the ALB ≤40.6 g/L (75 points), total T lymphocyte count ≤66.78% (55 points).
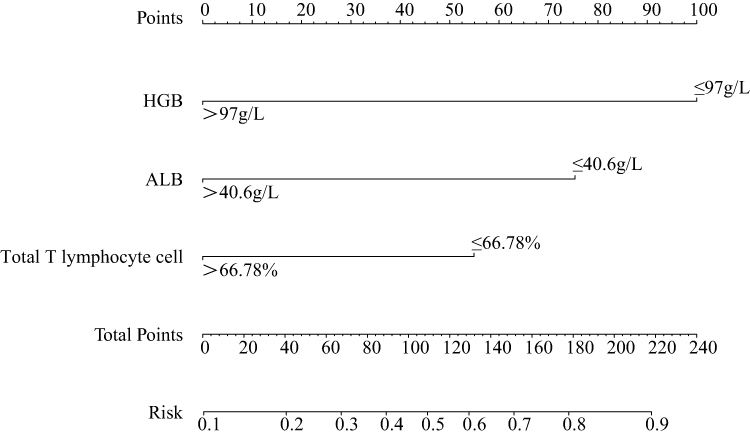 |
Figure 1 Nomogram for the individualized prediction of RE in cervical cancer patients. |
To verify the line graph model, a subject working curve ROC was established to evaluate this model (Figure 2A), which had a sensitivity of 0.79, a specificity of 0.58, and an AUC of 0.75 (95% CI: 0.72~0.81), suggesting that the predictive model had the good predictive ability. The nomogram prediction model was internally verified by the bootstrap method, the self-sampling was 1000 times, and the differentiation evaluation index C-index was 0.81 (95% CI: 0.73–0.87, p=0.038), as shown in Figure 2B. The results of the calibration graph show that the predicted probability of RE in the risk assessment line diagram model constructed in this study is more consistent with the actual possibility. The above shows that this model has a good prediction accuracy.
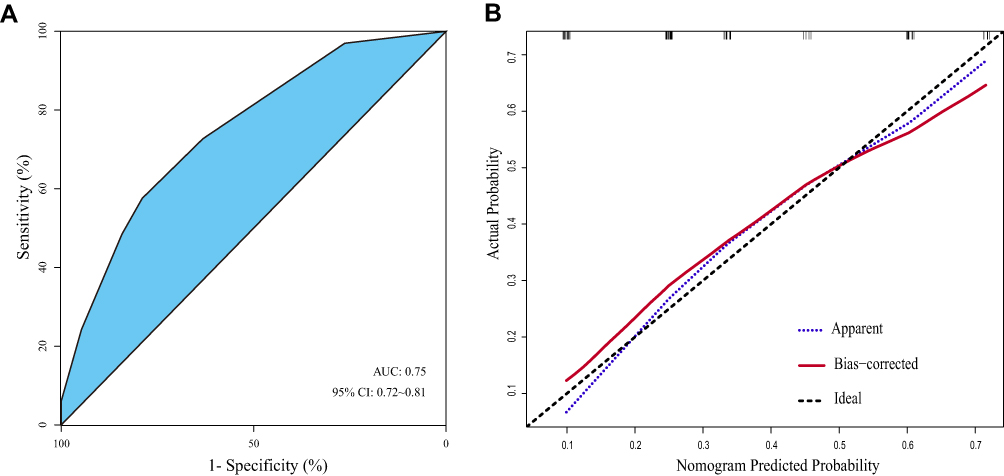 |
Figure 2 (A) ROC curve for the prediction nomogram. (B) Calibration curve showing nomogram-predicted RE probabilities compared with the actual RE. |
Discussion
Approximately 70% of patients with cervical cancer require radiation therapy during the disease,8,9,25 and RE is a nonspecific inflammatory response that is a common complication of normal intestinal tissue damaged by ionizing radiation. The adverse effects of RE on the quality of life and long-term prognosis of patients with cervical cancer radiotherapy have attracted widespread attention in the clinical. However, the mechanism of RE and the influencing factors are still unclear, and there is no standard prevention and treatment in the clinical, the prediction of RE should be strengthened clinically, and the treatment plan of patients should be adjusted according to the prediction results.26 Wang et al show that early RE was 54.3%, and late RE was 17.9% in cervical patients,27 the results of Ma et al also showed that the incidence of radiation enteritis was 27.1%, suggesting that the clinical risk of RE is relatively high.
The results of this study show that 35.56% of patients with cervical cancer develop RE during the follow-up process of 1 year after radiotherapy, which is consistent with the above study data.
Simultaneous chemoradiotherapy has been reported to increase the incidence of RE in locally advanced cervical cancer, particularly in patients with post-pelvic lymph node dissection in locally advanced cervical cancer.28 Sun et al found that postoperative adjuvant radiotherapy after rectal cancer surgery increased the risk of radiation rectal toxicity side effects. This study shows that both concurrent chemotherapy and pre-radiotherapy chemotherapy are not independent risk factors for the occurrence of RE in cervical cancer patients, and there is no significant correlation between the history of abdominal and pelvic surgery and the incidence of RE, which may be a small sample study in this study, and the sample size needs to be further expanded.29–32
Low levels of ALB, HGB, and diabetes had been reported to be associated with side effects in cancers. However, the combined analysis has not been reported. Moreover, studies on the impact of serum biochemical indexes on toxicity with radiotherapy of lymphocyte subsets for cervical cancer have not yet been reported.33 Zeng et al found serological markers such as ALB and BUN acted as risk factors for side effects in nasopharyngeal carcinoma. ALB is an acute-phase protein that positively correlates with the patients’ nutritional status.34,35 Patients undergoing cancer-related treatment often suffer from gastrointestinal reactions such as nausea and vomiting, which contributes to malnutrition. This study showed that the RE incidence of cervical cancer patients with HGB ≤97 g/L was 3.03 times that patients with HGB >97g/L, and 2.08 times in patients with ALB ≤40.6 g/L than patients with ALB >40.6 g/L, suggesting that malnutrition may be a risk factor for the development of RE in cervical cancer patients, improve the nutritional status of patients before radiotherapy can reduce the occurrence of RE in cervical cancer patients. This may be due to the low tissue repair ability of malnourished patients, ionizing radiation damage to the intestinal mucosa caused by intestinal digestive and absorption dysfunction, and then increased risk of RE in patients thus it is speculated that strengthening nutritional therapy is an effective means to reduce the risk of RE in cervical cancer patients. The multivariate logistic regression analysis showed the total T lymphocytes in patients with radiation therapy for cervical cancer were also associated with RE occurrence. This means detecting lymphocyte subsets before radiation therapy in patients with cervical cancer can assess the risk of RE to a certain extent. The results show that the percentage of dose of small bowel and rectum had no significantly contribute to the appearance of RE. Similar result in the D2cc to small bowel, sigmoid colon, and rectum from contributions of external beam irradiation plus internal brachytherapy. The possible reason for this result may due to the narrow range of different doses that were choose to use in this single institution experience, and some patients were repositioned and had a new treatment plan when they reach 15–20 times radiation treatments based on gynecological examination and bladder and rectal preparation at the first treatment plan. This may result in the OARs’ doses were not much difference in the RE group and control group patients.36,37
The nomogram visualizes the results of logistic regression or cox regression to provide a more intuitive, individualized patient risk probability. According to the size of the independent regression coefficient, the scoring criteria are formulated, and the corresponding scores are assigned to the different separate variable values. A total score can be calculated according to the assignment for other patients, and the probability of the patient’s outcome occurring is calculated. To establish a quantitative RE risk prediction model, assess the relevant risks, and identify high-risk groups of RE, this study demonstrated a nomogram prediction model of RE occurrence based on independent risk factors of RE. After statistical verification, the model has a more reliable predictive effect, suggesting that the predictive model can be applied to clinical diagnosis and treatment activities. Assuming a 48-year-old patient under poor nutritional status, ALB 32g/L, HGB 94g/L, the total score of the patient was calculated according to the nomogram model score to be 175, the corresponding risk prediction value was 0.73, indicating that the patient had a 73% probability of concurrent RE.
Our study has some limitations. This was a single-center retrospective case study with a small sample size, and the model was cross-validated only in internal populations. Therefore, expanding the sample size, carrying out multi-center research, and further revising and improving the predictive model are necessary.
Conclusion
HGB≤97g/L, albumin ≤40.6g/L, and total T lymphocyte count≤ 66.78% are risk factors for RE in cervical cancer patients with radiotherapy. The nomogram model based on the above risk factors can effectively predict the probability of RE.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Campbell HE, Gray AM, Watson J, et al. Preferences for interventions designed to increase cervical screening uptake in non-attending young women: how findings from a discrete choice experiment compare with observed behaviours in a trial. Health Expect. 2020;23(1):202–211. doi:10.1111/hex.12992
3. Liang C, Liu P, Cui Z, et al. Effect of laparoscopic versus abdominal radical hysterectomy on major surgical complications in women with stage IA-IIB cervical cancer in China, 2004–2015. Gynecol Oncol. 2020;156(1):115–123. doi:10.1016/j.ygyno.2019.10.032
4. Cao W, Chen HD, Yu YW, et al. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020. Chin Med J. 2021;134(7):783–791. doi:10.1097/CM9.0000000000001474
5. Anyasi HI, Foss AM. A comparative analysis of cervical cancer prevention between Nigeria and Nordic countries that have experienced a decline in cervical cancer incidence. Int Health. 2021;13(4):307–317. doi:10.1093/inthealth/ihaa062
6. Arbyn M, Weiderpass E, Bruni L, et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis [published correction appears in Lancet Glob Health. 2022;10(1):e41]. Lancet Glob Health. 2020;8(2):e191–e203. doi:10.1016/S2214-109X(19)30482-6
7. Endarti D, Satibi S, Kristina SA, et al. Knowledge, perception, and acceptance of HPV vaccination and screening for cervical cancer among women in Yogyakarta Province, Indonesia. Asian Pac J Cancer Prev. 2018;19(4):1105–1111. doi:10.22034/APJCP.2018.19.4.1105
8. Shao S, Ortega-Rivera A, Ray S, et al. A scalable manufacturing approach to single dose vaccination against HPV. Vaccines. 2021;9(1):66. doi:10.3390/vaccines9010066
9. Sims TT, Klopp AH. Intensified systemic therapy regimens in combination with definitive radiation for treatment of cervical cancer. Semin Radiat Oncol. 2020;30(4):265–272. doi:10.1016/j.semradonc.2020.05.005
10. Lakomy DS, Wu J, Lombe D, et al. Immune correlates of therapy outcomes in women with cervical cancer treated with chemoradiotherapy: a systematic review. Cancer Med. 2021;10(13):4206–4220. doi:10.1002/cam4.4017
11. Loge L, Florescu C, Alves A, et al. Radiation enteritis: diagnostic and therapeutic issues. J Visc Surg. 2020;157(6):475–485. doi:10.1016/j.jviscsurg.2020.08.012
12. Vozenin-Brotons MC, Milliat F, Linard C, et al. Gene expression profile in human late radiation enteritis obtained by high-density cDNA array hybridization. Radiat Res. 2004;161(3):299–311. doi:10.1667/RR3128
13. Hale MF. Radiation enteritis: from diagnosis to management. Curr Opin Gastroenterol. 2020;36(3):208–214. doi:10.1097/MOG.0000000000000632
14. Sheng L, Hu F, Yu H, et al. Paeoniflorin inhibits ASK1-TF axis by up-regulating SOCS3 to alleviate radiation enteritis. Front Pharmacol. 2022;13:743708. doi:10.3389/fphar.2022.743708
15. Kim CW, Kim JH, Yu CS, et al. Complications after sphincter-saving resection in rectal cancer patients according to whether chemoradiotherapy is performed before or after surgery. Int J Radiat Oncol Biol Phys. 2010;78(1):156–163. doi:10.1016/j.ijrobp.2009.07.1684
16. Theis VS, Sripadam R, Ramani V, Lal S. Chronic radiation enteritis. Clin Oncol. 2010;22(1):70–83. doi:10.1016/j.clon.2009.10.003
17. Merrick GS, Butler WM, Galbreath RW, Stipetich RL, Abel LJ, Lief JH. Erectile function after permanent prostate brachytherapy. Int J Radiat Oncol Biol Phys. 2002;52(4):893–902. doi:10.1016/S0360-3016(01)02675-X
18. Pathak R, Shah SK, Hauer-Jensen M. Therapeutic potential of natural plant products and their metabolites in preventing radiation enteropathy resulting from abdominal or pelvic irradiation. Int J Radiat Biol. 2019;95(4):493–505. doi:10.1080/09553002.2018.1552374
19. Grodsky MB, Sidani SM. Radiation proctopathy. Clin Colon Rectal Surg. 2015;28(2):103–111. doi:10.1055/s-0035-1547337
20. Guipaud O, Jaillet C, Clément-Colmou K, et al. The importance of the vascular endothelial barrier in the immune-inflammatory response induced by radiotherapy. Br J Radiol. 2018;91(1089):20170762. doi:10.1259/bjr.20170762
21. Murai T, Matsuo M, Tanaka H, et al. Efficacy of herbal medicine TJ-14 for acute radiation-induced enteritis: a multi-institutional prospective Phase II trial. J Radiat Res. 2020;61(1):140–145. doi:10.1093/jrr/rrz025
22. Poty S, Mandleywala K, O’Neill E, et al. 89 Zr-PET imaging of DNA double-strand breaks for the early monitoring of response following α- and β-particle radioimmunotherapy in a mouse model of pancreatic ductal adenocarcinoma. Theranostics. 2020;10(13):5802–5814. doi:10.7150/thno.44772
23. Wang Z, Wang Q, Wang X, et al. Gut microbial dysbiosis is associated with development and progression of radiation enteritis during pelvic radiotherapy. J Cell Mol Med. 2019;23(5):3747–3756. doi:10.1111/jcmm.14289
24. Department of Health and Human Services, U.S. Common terminology criteria for adverse events (CTCAE) version 5.0[S]; 2017. Available from: http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm.
25. Cao DD, Xu HL, Xu M, et al. Therapeutic role of glutamine in management of radiation enteritis: a meta-analysis of 13 randomized controlled trials. Oncotarget. 2017;8(18):30595–30605. doi:10.18632/oncotarget.15741
26. Wang Y, Kong W, Lv N, et al. Incidence of radiation enteritis in cervical cancer patients treated with definitive radiotherapy versus adjuvant radiotherapy. J Cancer Res Ther. 2018;14(8):S120–S124. doi:10.4103/0973-1482.163762
27. Ma S, Zhang T, Jiang L, et al. Impact of bladder volume on treatment planning and clinical outcomes of radiotherapy for patients with cervical cancer. Cancer Manag Res. 2019;11:7171–7181. doi:10.2147/CMAR.S214371
28. Sun Myint A, Mukhopadhyay T, Ramani VS, et al. Can increasing the dose of radiation by HDR brachytherapy boost following pre operative chemoradiotherapy for advanced rectal cancer improve surgical outcomes? Colorectal Dis. 2010;12(Suppl 2):30–36. doi:10.1111/j.1463-1318.2010.02322.x
29. Du XJ, Tang LL, Mao YP, et al. The pretreatment albumin to globulin ratio has predictive value for long-term mortality in nasopharyngeal carcinoma. PLoS One. 2014;9(4):e94473. doi:10.1371/journal.pone.0094473
30. Carvalho B, Lopes RG, Linhares P, et al. Hypertension and proteinuria as clinical biomarkers of response to bevacizumab in glioblastoma patients. J Neurooncol. 2020;147(1):109–116. doi:10.1007/s11060-020-03404-z
31. Wang C, Fu G, Ji F, et al. Perioperative risk factors for radial forearm-free flap complications. J Craniofac Surg. 2020;31(2):381–384. doi:10.1097/SCS.0000000000006035
32. Veldwijk MR, Seibold P, Botma A, et al. Association of CD4+ radiation-induced lymphocyte apoptosis with fibrosis and telangiectasia after radiotherapy in 272 breast cancer patients with >10-year follow-up. Clin Cancer Res. 2019;25(2):562–572. doi:10.1158/1078-0432.CCR-18-0777
33. Zeng X, Liu G, Pan Y, et al. Prognostic value of clinical biochemistry-based indexes in nasopharyngeal carcinoma. Front Oncol. 2020;10:146. doi:10.3389/fonc.2020.00146
34. Rock CL, Doyle C, Demark-Wahnefried W, et al. Nutrition and physical activity guidelines for cancer survivors [published correction appears in CA Cancer J Clin. 2013 May;63(3):215]. CA Cancer J Clin. 2012;62(4):243–274. doi:10.3322/caac.21142
35. Inglis JE, Lin PJ, Kerns SL, et al. Nutritional interventions for treating cancer-related fatigue: a qualitative review. Nutr Cancer. 2019;71(1):21–40. doi:10.1080/01635581.2018.1513046
36. Mazouni C, Rouzier R, Ledu R, et al. Development and internal validation of a nomogram to predict macrosomia. Ultrasound Obstet Gynecol. 2007;29(5):544–549. doi:10.1002/uog.3999
37. Liu K, Huang G, Chang P, et al. Construction and validation of a nomogram for predicting cancer-specific survival in hepatocellular carcinoma patients. Sci Rep. 2020;10(1):21376. doi:10.1038/s41598-020-78545-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Model That Predicts the Risk of Diabetic Nephropathy in Type 2 Diabetes Mellitus Patients: A Cross-Sectional Study
Yang J, Jiang S
International Journal of General Medicine 2022, 15:5089-5101
Published Date: 20 May 2022
Paraspinal Muscle Degeneration: A Potential Risk Factor for New Vertebral Compression Fractures After Percutaneous Kyphoplasty
Si F, Yuan S, Zang L, Fan N, Wu Q, Wang T, Wang A
Clinical Interventions in Aging 2022, 17:1237-1248
Published Date: 13 August 2022
Tracking Epidemiological Characteristics and Risk Factors of Multi-Drug Resistant Bacteria in Intensive Care Units
Wu C, Lu J, Ruan L, Yao J
Infection and Drug Resistance 2023, 16:1499-1509
Published Date: 15 March 2023
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023
A Novel Scoring System to Predict Acute Radiation Enteritis Recovery in Cervical Cancer Patients Undergoing Concurrent Chemoradiotherapy: A Southwest China Cohort Study
Zeng C, Ji J, Huang Y, Peng Y, Zhang X, Yang Z, Guo Z
International Journal of General Medicine 2024, 17:5907-5919
Published Date: 9 December 2024