Back to Journals » Cancer Management and Research » Volume 18

Construction and Validation of a Nomogram Prediction Model for Individualized Prediction of the Risk of Oral Infection in Patients with Nasopharyngeal Carcinoma Undergoing Radiotherapy and Chemotherapy
Authors Wang J, Ye Q, Liu C, Zhong K, Zhou W
Received 18 March 2026
Accepted for publication 5 July 2026
Published 10 July 2026 Volume 2026:18 603294
DOI https://doi.org/10.2147/CMAR.S603294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Jinfeng Wang,1– 3 Qiang Ye,4 Chunyu Liu,5 Kui Zhong,5 Wenting Zhou1– 3
1Department of Oncology, The First Affiliated Hospital of Gannan Medical University, Ganzhou, Jiangxi, 341000, People’s Republic of China; 2Jiangxi “Flagship” Oncology Department of Synergy for Chinese and Western Medicine, Ganzhou, Jiangxi, 341000, People’s Republic of China; 3Jiangxi Provincial Unit for Clinical Key Oncology Specialty Development, Ganzhou, Jiangxi, 341000, People’s Republic of China; 4Department of Oncology, Yudu County People’s Hospital, Ganzhou, Jiangxi, 341000, People’s Republic of China; 5The First Clinical Medical College, Gannan Medical University, Ganzhou, Jiangxi, 341000, People’s Republic of China
Correspondence: Wenting Zhou, Department of Oncology, The First Affiliated Hospital of Gannan Medical University, No. 2201, Building 7, Zhongyang Park Shoufu, Zhanggong District, Ganzhou, Jiangxi, 41000, People’s Republic of China, Tel +8615770705148, Email [email protected]
Objective: To establish and validate a nomogram prediction model for individualized prediction of the risk of oral infection in patients with nasopharyngeal carcinoma (NPC) undergoing radiotherapy and chemotherapy.
Methods: The clinical data of 379 NPC patients admitted to our hospital from March 2021 to March 2024 were retrospectively collected (as the training set), and the clinical data of 226 NPC patients admitted to other hospitals from April 2024 to December 2025 were also collected (as the validation set). The patients were separated into the infection group and the non-infection group based on whether they had oral infections. The clinical data of the patients were collected. LASSO-logistic regression analysis was used to identify the factors influencing the occurrence of oral infection in patients with NPC undergoing chemoradiotherapy. R software was used to construct a nomogram prediction model for the occurrence of oral infection in these patients. Bootstrap resampling was performed for internal validation. ROC curves and calibration curves were used to evaluate the discrimination and consistency of the model, respectively, while DCA was used to assess its clinical application value.
Results: The Lasso-Logistic analysis showed that age, diabetes, smoking history, oral pH value, chemotherapy cycles, history of oral infection, and ALB were the influencing factors for the occurrence of oral infections in NPC patients undergoing radiotherapy and chemotherapy (P < 0.05). The AUC of the internal validation was 0.833. The Bootstrap method indicated a C-index of 0.833. The H-L test showed χ2 = 7.638, P = 0.734. The DCA curve indicated that the model had a good positive net benefit within the probability range of 0.21~0.93. The external validation AUC was 0.886. The Bootstrap method validation showed a C-index of 0.886. The H-L test yielded χ2 = 7.764, P = 0.728. The DCA curve indicated that the model had a good positive net benefit within the probability range of 0.21~0.95.
Conclusion: Age, diabetes, smoking history, oral pH value, chemotherapy cycles, history of oral infection, and ALB are the influencing factors for the occurrence of oral infections in NPC patients undergoing radiotherapy and chemotherapy. The constructed nomogram model based on these factors is conducive to individualized prediction of oral infections in patients, and can facilitate the early identification of high-risk populations. However, as this was a retrospective study, the sample size selection and study design may have introduced potential bias.
Keywords: nasopharyngeal carcinoma, oral infection, influencing factors, nomogram
Introduction
Nasopharyngeal carcinoma (NPC) is a common type of head and neck cancer, originating mainly from the mucosal epithelial tissue of the nasopharynx. Tumor cells are primarily located at the roof and lateral walls of the nasopharyngeal cavity. Early symptoms are not obvious; however, as the disease progresses, symptoms such as blood-tinged nasal discharge and tinnitus may appear, and even facial numbness and headache may occur. Metastasis or dissemination may also develop, increasing the risk of death.1,2 Radiotherapy and chemotherapy are the main clinical treatments for NPC, which can effectively kill cancer cells and prolong patient survival. However, the adverse effects of chemotherapeutic drugs may cause acute reactions during treatment, leading to complications and reducing patients’quality of life. Oral infection is a common complication during radiotherapy and chemotherapy; it affects normal eating, increases pain perception, and compromises treatment efficacy.3,4 This is mainly because radiation can directly damage DNA and induce the ionization of water molecules, thereby generating large amounts of reactive oxygen species and free radicals. These changes impair the proliferative and reparative functions of oral mucosal epithelial stem cells, leading to mucosal congestion and ulceration, as well as loss of the integrity of the physical defense barrier. Chemotherapeutic drugs can further inhibit mucosal cell metabolism and regenerative capacity, aggravate the degree of mucosal injury, and prolong the wound-healing period. In addition, chemoradiotherapy can suppress bone marrow hematopoietic function, reduce peripheral white blood cell and lymphocyte levels, and weaken the ability of both innate and adaptive immunity to eliminate pathogens. As a result, local and systemic immune function is compromised, making the body unable to effectively resist invasion by pathogenic microorganisms in the oral cavity and thereby inducing oral infection.5,6 At present, factors associated with oral infection induced by radiotherapy and chemotherapy have not been clearly identified. Therefore, this study aims to identify factors influencing oral infection in patients to enable early targeted interventions and reduce infection risk. A nomogram model established based on clinical influencing factors can provide relatively accurate individualized predictions and intuitively estimate postoperative recurrence risk.7,8 A study showed that a nomogram model was constructed based on the risk factors for severe radiation-induced oral mucositis in patients with head and neck tumors. Smoking history, diabetes, concurrent chemotherapy, cumulative radiotherapy dose, and weight loss of ≥5% relative to body weight at admission were identified as influencing factors. The nomogram model constructed based on these factors demonstrated good predictive accuracy. This prediction model can effectively identify patients at high risk of severe oral mucositis, thereby facilitating the design of targeted interventions and improving patient management during radiotherapy.9 Accordingly, studies on nomograms for oral infection in NPC patients receiving radiotherapy and chemotherapy are limited. This study aims to develop and validate a nomogram prediction model for individualized risk prediction of oral infection in NPC patients undergoing radiotherapy and chemotherapy.
Materials and Methods
General Information
In this retrospective study, the training set and external validation set were divided using an independent temporal split method at the study design stage, and Clinical data of 379 NPC patients treated at our hospital from March 2021 to March 2024 were retrospectively collected as the training set. In addition, clinical data of 226 NPC patients treated at other hospitals from April 2024 to December 2025 were collected as the validation set, and the qualifications and treatment levels of these hospitals were comparable to those of our hospital. Patients were divided into an infection group and a non-infection group based on whether oral infection occurred during radiotherapy and chemotherapy. The case flowchart is shown in Figure 1. Inclusion criteria: (1) meeting the diagnostic criteria for NPC;10 (2) first diagnosis, age ≥18 years; (3) completion of at least one cycle of radiotherapy and chemotherapy (IMRT with a nasopharyngeal dose of ≥66 Gy and concurrent radical treatment with cisplatin monotherapy were used, with radiotherapy technique, total dose, and chemotherapeutic drug type restricted to ensure a unified treatment regimen); (4) complete clinical data. Exclusion criteria: (1) other malignant tumors; (2) distant metastasis; (3) history of oral surgery; (4) hepatic or renal dysfunction (eGFR<60 mL/min/1.73m2, ALT/AST>2×ULN); (5) psychiatric disorders; (6) autoimmune diseases. This study was approved by the hospital ethics committee.
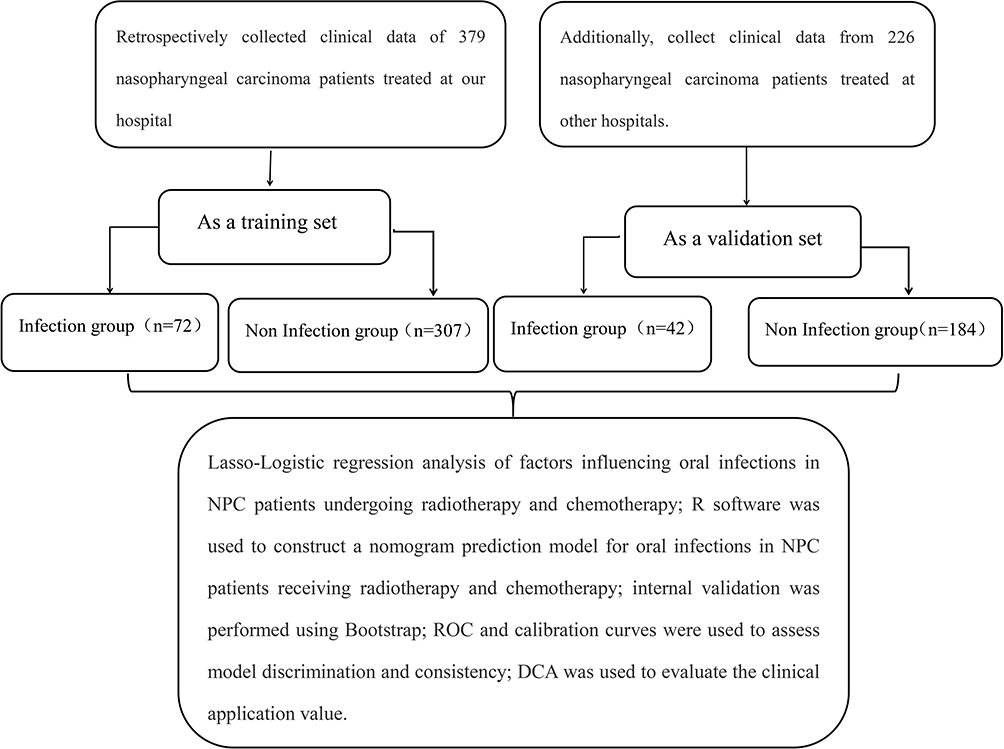 |
Figure 1 Case flow collection diagram. |
Methods
Determination of Oral Infection
According to relevant criteria,11 oral infection was diagnosed when oral mucosal ulcers or erythema were present or when local symptoms such as erosions, ulcers, white plaques, yellow-white purulent pseudomembranes, gingival redness and swelling with purulent discharge, difficulty eating, dry mouth, and burning pain were observed in the buccal mucosa, tongue, gingiva, or soft palate, and oral pathogenic microorganism testing was positive.
Clinical Data
Clinical data (Medical record data were independently and blindly extracted by two investigators and cross-checked; standardized and objective electronic data collection was used to avoid subjective recall bias; uniform outcome assessment criteria were applied to reduce misclassification bias; and strict stratified cohort splitting was performed to avoid data leakage) potentially affecting patients were retrospectively collected from the hospital electronic medical record system, including age, sex, BMI, hypertension, diabetes, smoking history, drinking history, pathological type (keratinizing squamous cell carcinoma, non-keratinizing squamous cell carcinoma), tumor stage, oral pH value, chemotherapy cycles, history of oral infection, dentures, upper respiratory tract infection, antibiotic use, use of oral mucosal protective agents, use of glycyrrhizinate disodium, oral self-cleaning habits, preventive gargling, saliva viscosity, invasive procedures, albumin (ALB), total antioxidant capacity (T-AOC), and glutathione peroxidase (GPX). Variables with a missing data rate greater than 5% were excluded to ensure the reliability and rigor of the results. For all variables with a missing data rate of <20%, multiple imputation by chained equations (MICE) was performed, generating five imputed datasets. Only variables with a missing data rate of ≥20% and an extremely high risk of data distortion were excluded, thereby maximizing the retention of study samples and reducing bias.
Statistical Analysis
SPSS 27.0 was used for data processing. Measurement data were analyzed using the t-test and expressed as ( ); count data were analyzed using the χ2-test and expressed as n (%). Lasso-Logistic regression was used to analyze factors influencing oral infection in NPC patients undergoing radiotherapy and chemotherapy. R software was used to construct a nomogram prediction model for oral infection occurrence. Bootstrap was used for internal validation. ROC and calibration curves were used to evaluate model discrimination and consistency, and DCA was used to assess clinical application value (The threshold probability refers to the critical probability used to determine whether a patient is at high risk of treatment failure and whether intensified intervention measures should be adopted, representing the trade-off criterion in clinical decision-making. Net benefit refers to the actual benefit of the model in identifying high-risk populations, which is calculated as the benefit of true positives minus the loss caused by overtreatment due to false positives). P<0.05 indicated statistical significance.
); count data were analyzed using the χ2-test and expressed as n (%). Lasso-Logistic regression was used to analyze factors influencing oral infection in NPC patients undergoing radiotherapy and chemotherapy. R software was used to construct a nomogram prediction model for oral infection occurrence. Bootstrap was used for internal validation. ROC and calibration curves were used to evaluate model discrimination and consistency, and DCA was used to assess clinical application value (The threshold probability refers to the critical probability used to determine whether a patient is at high risk of treatment failure and whether intensified intervention measures should be adopted, representing the trade-off criterion in clinical decision-making. Net benefit refers to the actual benefit of the model in identifying high-risk populations, which is calculated as the benefit of true positives minus the loss caused by overtreatment due to false positives). P<0.05 indicated statistical significance.
Results
Comparison of Clinical Data Between Infection and Non-Infection Groups in the Training Set
Significant differences were observed between the infection group and the non-infection group in age, diabetes, smoking history, oral pH value, chemotherapy cycles, history of oral infection, antibiotic use, preventive gargling, and ALB (P<0.05). No significant differences were found in other clinical data (P>0.05). See Table 1.
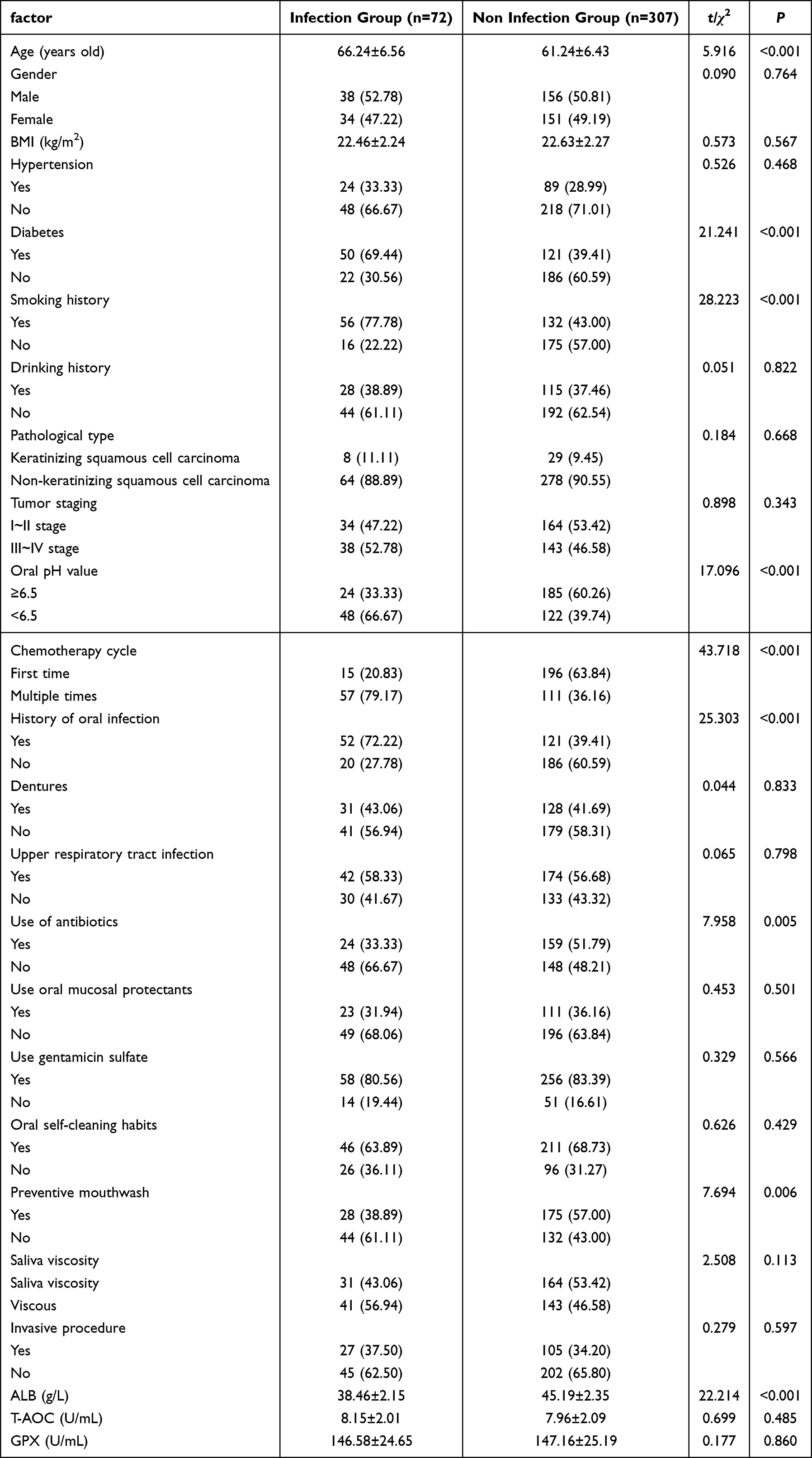 |
Table 1 Comparison of Clinical Data Between Infection and Non-Infection Groups in the Training Set |
Lasso-Logistic Regression Analysis of Factors Influencing Oral Infection in NPC Patients Undergoing Radiotherapy and Chemotherapy
Oral infection occurrence in NPC patients undergoing radiotherapy and chemotherapy (yes=1, no=0) was used as the dependent variable. Variables with P<0.05 were included as independent variables: diabetes (yes=1, no=0), smoking history (yes=1, no=0), oral pH value (≥6.5=0, <6.5=1), chemotherapy cycles (initial=0, multiple=1), history of oral infection (yes=1, no=0), antibiotic use (yes=1, no=0), preventive gargling (yes=1, no=0), age, and ALB (entered as original values). Lasso analysis was performed using R software. When λ=0.036715, seven predictive factors were selected (age, diabetes, smoking history, oral pH value, chemotherapy cycles, history of oral infection, ALB), as shown in Figure 2. Multicollinearity testing of these variables showed variance inflation factors <5, indicating no interaction among factors. Logistic regression was then performed, showing that age, diabetes, smoking history, oral pH value, chemotherapy cycles, history of oral infection, and ALB were influencing factors for oral infection in NPC patients undergoing radiotherapy and chemotherapy (P<0.05). See Table 2.
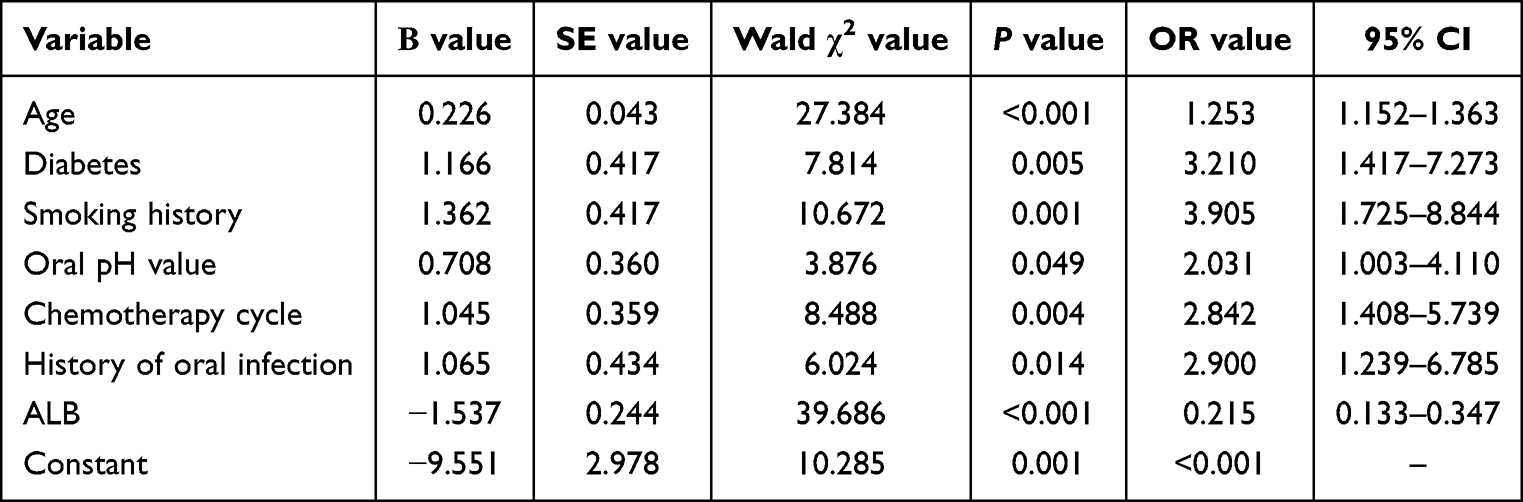 |
Table 2 Lasso-Logistic Regression Analysis of Factors Influencing Oral Infections in NPC Patients Undergoing Radiotherapy and Chemotherapy |
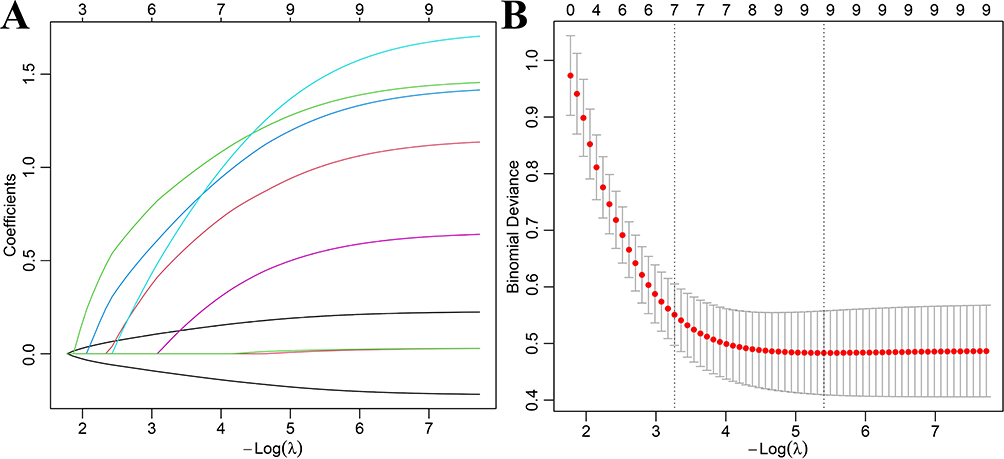 |
Figure 2 LASSO–logistic regression analysis of factors associated with oral infection in nasopharyngeal carcinoma patients undergoing chemoradiotherapy (A) Relationship diagram of Lasso regression coefficient; (B) Lasso regression 10-fold cross-validation results. |
Construction of a Nomogram Model for Oral Infection in NPC Patients Undergoing Radiotherapy and Chemotherapy
A nomogram model was constructed based on factors selected by Lasso-Logistic regression, with P=ex/(1+ex), x=−9.551+1.362×age+0.708×diabetes+1.045×smoking history+1.065×oral pH value+1.165×chemotherapy cycles+0.226×history of oral infection+1.537×ALB. The strongest predictor was ALB. By evaluating the score of each factor, the total score was used to calculate the predicted probability of oral infection occurrence in NPC patients undergoing radiotherapy and chemotherapy. Higher scores indicated higher risk of oral infection; for example, when the total score was 150, the probability of oral infection was 73%. See Figure 3.
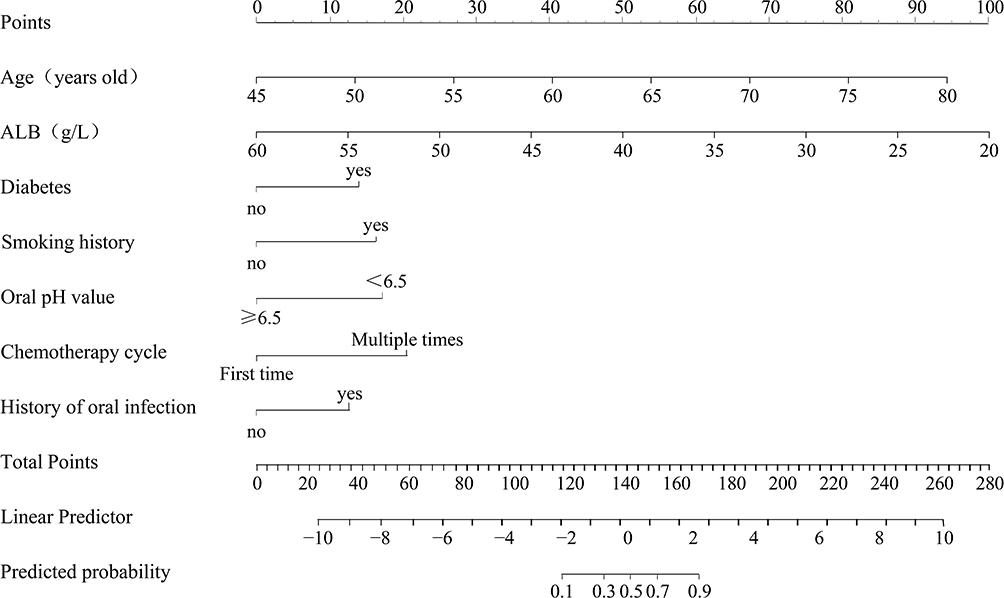 |
Figure 3 The Nomogram Model for the Occurrence of Oral Infections in NPC Patients Undergoing Radiotherapy and Chemotherapy. |
Internal Validation of the Nomogram Model for Oral Infection in NPC Patients Undergoing Radiotherapy and Chemotherapy
The AUC of the model for predicting oral infection was 0.833 (95% CI: 0.775–0.884). Internal validation using the Bootstrap method (1000 repetitions) showed a C-index of 0.833. Goodness-of-fit analysis showed an H-L test χ2=7.638, P=0.734. The predicted curve for oral infection occurrence closely matched the ideal curve, as shown in Figure 4.
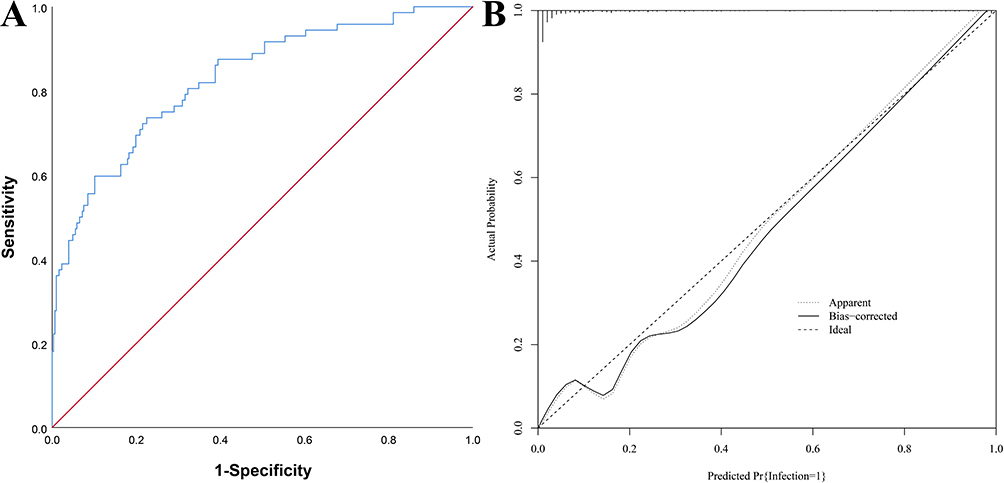 |
Figure 4 Internal validation of the nomogram model for oral infection in nasopharyngeal carcinoma patients undergoing chemoradiotherapy (A) ROC curves; (B) Calibration curves. |
Curve of the Internally Validated Nomogram Model
The DCA curve showed that within the probability range of 0.21–0.93, the model had good positive net benefit, indicating good clinical application value, as shown in Figure 5.
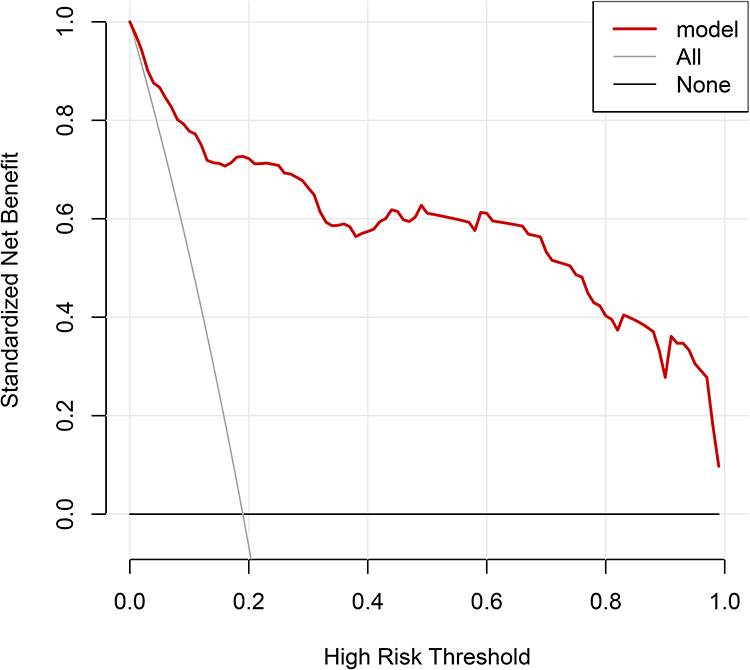 |
Figure 5 DCA curve for nomogram model (Red line: Prediction model;Vertical line: assuming all patients respond well to treatment; Dash: Assume that none of the patients’ conditions have improved). |
Comparison of Clinical Data Between Infection and Non-Infection Groups in the Validation Set
Significant differences were observed between the infection group and the non-infection group in age, diabetes, smoking history, oral pH value, chemotherapy cycles, history of oral infection, antibiotic use, preventive gargling, and ALB (P<0.05). No significant differences were found in other data (P>0.05). See Table 3.
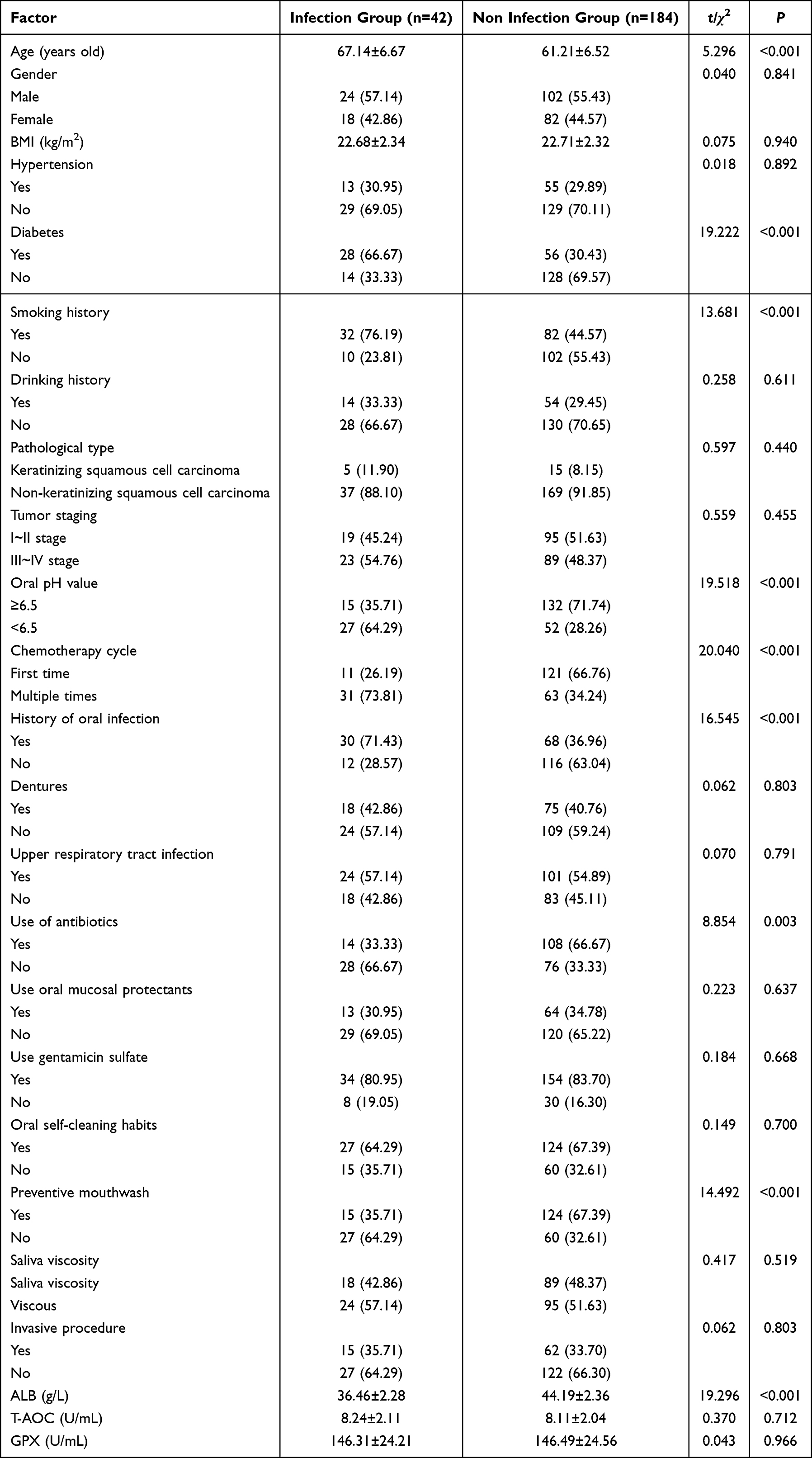 |
Table 3 Comparison of Clinical Data Between Infection and Non-Infection Groups in the Validation Set |
External Validation of the Nomogram Model for Oral Infection in NPC Patients Undergoing Radiotherapy and Chemotherapy
The AUC for predicting oral infection using the model was 0.886 (95% CI: 0.827–0.945). Bootstrap validation (1000 repetitions) showed a C-index of 0.886. Goodness-of-fit analysis showed an H-L test χ2=7.764, P=0.728. The predicted curve for oral infection closely approximated the ideal curve, as shown in Figure 6.
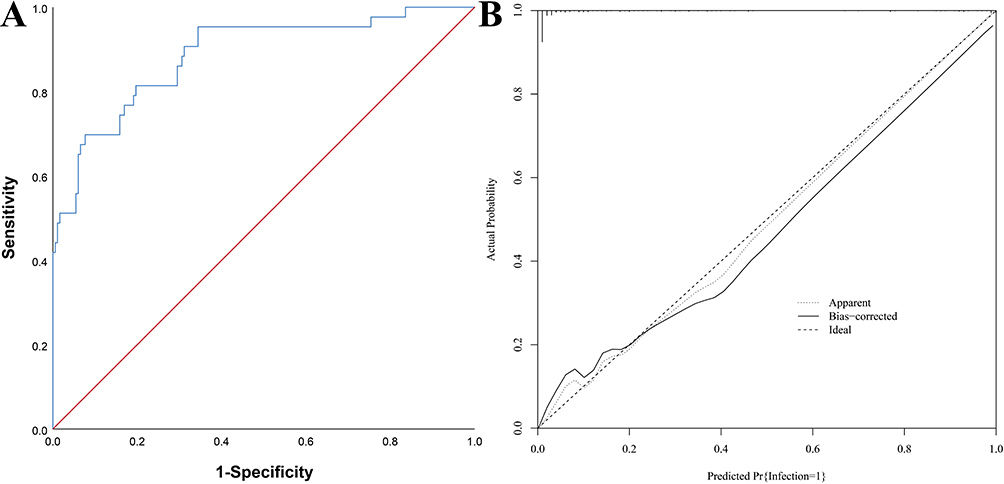 |
Figure 6 External validation of the nomogram model for oral infection in nasopharyngeal carcinoma patients undergoing chemoradiotherapy (A) ROC curves; (B) Calibration curves. |
Curve of the Externally Validated Nomogram Model
The DCA curve showed that within the probability range of 0.21–0.95, the model had good positive net benefit, indicating good clinical application value, as shown in Figure 7.
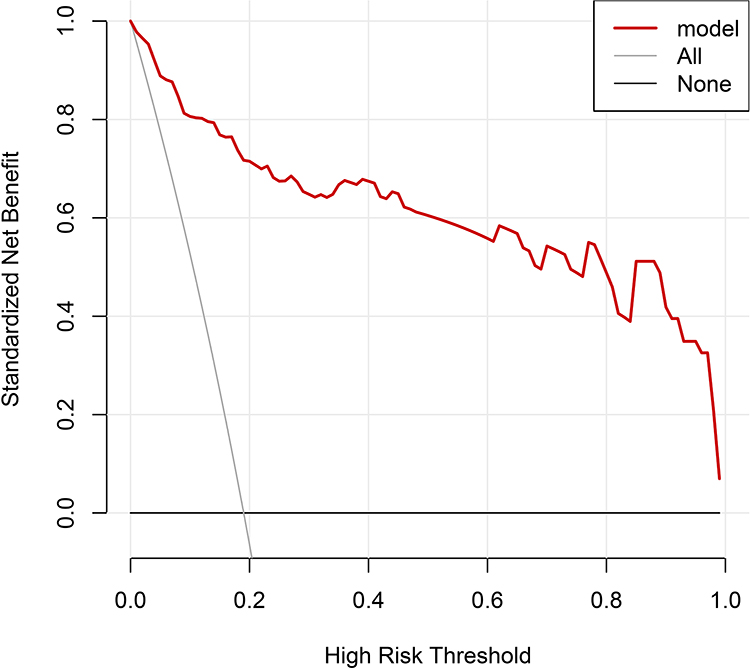 |
Figure 7 DCA curve (Red line: Prediction model; Vertical line: assuming all patients respond well to treatment; Dash: Assume that none of the patients’ conditions have improved). |
Discussion
Epidemiological data indicate that NPC ranks first among otorhinolaryngological head and neck tumors, with an annual incidence of approximately 0.7%. Early-stage disease is asymptomatic, whereas patients in the middle and late stages often present with cervical masses. Some patients have already progressed to middle or late stages at diagnosis, missing the optimal time for surgical treatment.12,13 Due to the complex anatomy of the nasopharynx, surgical treatment is challenging; thus, radiotherapy and chemotherapy are more commonly used to control disease progression. However, radiotherapy and chemotherapy impair immune function and induce acute-phase reactions, affecting chemotherapy efficacy. Radiation-induced effects also damage the oral mucosa surrounding malignant tumors, triggering oral infections, increasing mucosal fragility, reducing protective capacity, and aggravating oral infection symptoms.14–16 Therefore, accurately identifying high-risk patients and implementing timely interventions can effectively reduce recurrence risk.
Lasso-Logistic analysis showed that age, diabetes, smoking history, oral pH value, chemotherapy cycles, history of oral infection, and ALB were influencing factors for oral infection in NPC patients undergoing radiotherapy and chemotherapy. The reasons are as follows: (1) Age is related to immune function; as age increases, immune function declines, resistance to external pathogens decreases, and radiotherapy- and chemotherapy-induced radiation further disrupts oral flora, increasing infection risk.16,17 (2) Long-term hyperglycemia leads to metabolic disorders, defects in leukocyte phagocytosis and chemotaxis, impaired resistance to pathogens, and poor control of local inflammatory responses, facilitating oral infections. Persistent hyperglycemia also provides a favorable medium for pathogen growth, accelerating bacterial proliferation and increasing infection risk.18,19 (3) Smoking increases the risk of oral infection by reducing healthy oral flora; elevated oral mucosal temperature during smoking impairs local blood circulation. Tobacco combustion releases multiple toxic byproducts that weaken host defense against pathogens. Long-term smoking inhibits epithelial cell proliferation and self-repair capacity, making mucosal reactions more likely during radiotherapy and chemotherapy.20,21 (4) Oral pH accurately reflects the oral ecological environment. Continuous radiotherapy and chemotherapy lower oral pH, alter saliva, disrupt the oral microecosystem, and create favorable conditions for fungal and pathogenic bacterial proliferation, increasing infection risk.22,23 (5) NPC patients often require periodic radiotherapy and chemotherapy. Multiple cycles have high cytotoxicity, damaging oral mucosa and impairing its barrier function. Chemotherapeutic drugs can also cause salivary gland dysfunction, reduce antibody-containing saliva secretion, weaken oral resistance to pathogens, facilitate bacterial colonization, and increase infection risk.24 (6) Patients with a history of oral infection often have poorer oral environments and hygiene habits, providing favorable conditions for pathogen growth and increasing infection risk.25 (7) ALB participates in immune function and reflects nutritional status. Long-term radiotherapy and chemotherapy increase bodily consumption, and treatment-related side effects limit nutritional intake, thereby increasing infection risk.26 Therefore, ALB levels should be closely monitored during radiotherapy and chemotherapy, and individualized dietary nursing should be implemented based on patient condition to improve nutritional status.
In this study, the AUCs for predicting oral infection in the training and validation sets were 0.833 and 0.886, respectively, with C-indices of 0.833 and 0.886, indicating good model consistency. The DCA curve threshold probabilities of 0.21–0.93 and 0.21–0.95 showed good positive net benefit, assisting clinicians in screening high-risk populations, enabling early prevention, and effectively improving patients’ quality of life.
In conclusion, age, diabetes, smoking history, oral pH value, chemotherapy cycles, history of oral infection, and ALB are influencing factors for oral infection in NPC patients undergoing radiotherapy and chemotherapy. The nomogram model constructed based on these factors facilitates individualized prediction of oral infection and early identification of high-risk populations. This study has limitations. First, this was a single-center retrospective cohort study, with a single source of cases and center-specific population baselines. Retrospective collection of electronic medical records may be prone to information bias, such as incomplete information records and mild misclassification of outcomes, which limits the generalizability of the conclusions to other medical institutions. Second, there was a potential risk of overfitting and model instability. In this study, the total number of positive oral infection events was relatively small, and the events-per-variable ratio did not reach the ideal modeling standard. Multiple predictors may easily fit random noise in the cohort, resulting in inflated effect estimates. In addition, the sample distribution of high-risk subgroups was uneven, potential confounding factors were not fully included, and the validation cohort shared a similar diagnostic and treatment environment with the modeling cohort, making it difficult to fully assess cross-center stability. Although Bootstrap correction, multiple imputation, and independent temporal external validation were used to alleviate these issues, these limitations could not be completely eliminated. Future studies should conduct multicenter, prospective, large-sample cohorts, balance population baselines, expand independent external validation sets, and further optimize and validate the model.
Research Involving Human Participants
This study was approved by the Medical Ethics Committee of The First Affiliated Hospital of Gannan Medical University (Approval No. GZ2021020016) and was conducted in accordance with the Declaration of Helsinki (1964 and its later amendments). Written informed consent was obtained from all participants prior to study commencement.
Data Sharing Statement
The original contributions presented in the study are included in the article.
Funding
There is no funding to report.
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Su ZY, Siak PY, Lwin YY, et al. Epidemiology of nasopharyngeal carcinoma: current insights and future outlook. Cancer Metastasis Rev. 2024;43(3):919–13. doi:10.1007/s10555-024-10176-9
2. Juarez-Vignon Whaley JJ, Afkhami M, Onyshchenko M, et al. Recurrent/metastatic nasopharyngeal carcinoma treatment from present to future: where are we and where are we heading? Curr Treat Options Oncol. 2023;24(9):1138–1166. doi:10.1007/s11864-023-01101-3
3. Li J, Zhu C, Zhang Y, et al. Incidence and risk factors for radiotherapy-induced oral mucositis among patients with nasopharyngeal carcinoma: a meta-analysis. Asian Nurs Res. 2023;17(2):70–82. doi:10.1016/j.anr.2023.04.002
4. Jiang R, Liu Y, Zhang H, et al. Distinctive microbiota of delayed healing of oral mucositis after radiotherapy of nasopharyngeal carcinoma. Front Cell Infect Microbiol. 2022;12:1070322. doi:10.3389/fcimb.2022.1070322
5. Li L, Huang Y, Yin J, et al. The effect of rabdosia rubescens on radiotherapy-induced oral mucositis in nasopharyngeal carcinoma patients: a phase II clinical study. Integr Cancer Ther. 2025;24:15347354251314499. doi:10.1177/15347354251314499
6. Yin J, Xie J, Lin J, et al. Evaluation of the efficacy of the anti-ulcer oral mucosal protective agent RADoralex® in the prevention and treatment of radiation-induced oral mucosal reactions induced during treatment of nasopharyngeal carcinoma. Cancer Biol Ther. 2022;23(1):27–33. doi:10.1080/15384047.2021.2013704
7. Liu K, Wang J. Developing a nomogram model and prognostic analysis of nasopharyngeal squamous cell carcinoma patients: a population-based study. J Cancer Res Clin Oncol. 2023;149(13):12165–12175. doi:10.1007/s00432-023-05120-3
8. Yan C, Tu Z, Zhang Z, et al. Institutionally validated nomogram predicting prognosis for older patients with nonmetastatic nasopharyngeal carcinoma. Future Oncol. 2022;18(15):1829–1838. doi:10.2217/fon-2021-1121
9. Wang J, Gu L, Zhi C, et al. Risk factor and prediction model development for severe radiation-induced oral mucositis in head and neck tumors. Future Oncol. 2024;20(31):2385–2395. doi:10.1080/14796694.2024.2384353
10. Saba NF, Salama JK, Beitler JJ, et al. ACR Appropriateness criteria® for nasopharyngeal carcinoma. Head Neck. 2016;38(7):979–986. doi:10.1002/hed.24423
11. Zhou H, Lu T, Guo Q, et al. Effects of oral maintenance chemotherapy and predictive value of circulating EBV DNA in metastatic nasopharyngeal carcinoma. Cancer Med. 2020;9(8):2732–2741. doi:10.1002/cam4.2926
12. Huang S, Liang Y, Liu N, et al. Predictive biomarkers for immunotherapy in nasopharyngeal carcinoma: from tumor microenvironment to macroenvironment. Front Med. 2025;19(5):721–742. doi:10.1007/s11684-025-1151-5
13. Ji J, Zhu H, Zhang M-X, et al. Individualized whole course nutrition management for nasopharyngeal carcinoma patients undergoing radiotherapy. Clin Lab. 2022;68(6). doi:10.7754/Clin.Lab.2021.210459
14. Hamzah MH, Mohamad I, Musa MY, et al. Propolis mouthwash for preventing radiotherapy-induced mucositis in patients with nasopharyngeal carcinoma. Med J Malaysia. 2022;77(4):462–467.
15. Lv J, Liao S, Li B, et al. Scheduling radiotherapy for patients with nasopharyngeal carcinoma in the corresponding time window can reduce radiation-induced oral mucositis: a randomized, prospective study. Cancer Med. 2023;12(15):16032–16040. doi:10.1002/cam4.6252
16. Liu Z, Huang L, Wang H, et al. Predicting nomogram for severe oral mucositis in patients with nasopharyngeal carcinoma during intensity-modulated radiation therapy: a retrospective cohort study. Curr Oncol. 2022;30(1):219–232. doi:10.3390/curroncol30010017
17. Zou S-Q, Huang C-L, Zhang J-J, et al. Association of anti-PD-1 therapy with severe radiation-induced oral mucositis: a retrospective cohort study and validation in the CONTINUUM trial. Med. 2025;6(10):100770. doi:10.1016/j.medj.2025.100770
18. Midorikawa S, Mizukami H, Kudoh K, et al. Diabetes can increase the prevalence of EBV infection and worsen the prognosis of nasopharyngeal carcinoma. Pathology. 2023;56(1):65–74. doi:10.1016/j.pathol.2023.09.013
19. Zeng M-C, Jia Q-J, Xu J, et al. The whole-blood Epstein-Barr virus DNA can serve as a valuable molecular marker for diagnosis and prognosis prediction of nasopharyngeal carcinoma. Am J Cancer Res. 2023;13(11):5431–5442.
20. Sun X-S, Xie S-Y, Luo D-H, et al. Impact of smoking on survival in nasopharyngeal carcinoma: a cohort study with 23,325 patients diagnosed from 1990 to 2016. Radiother Oncol. 2021;162:7–17.
21. Li W, Yang C, Zhao F, et al. Combination of smoking and Epstein-Barr virus DNA is a predictor of poor prognosis for nasopharyngeal carcinoma: a long-term follow-up retrospective study. BMC Cancer. 2022;22(1):1262. doi:10.1186/s12885-022-10297-w
22. Kong -F-F, Pan G-S, Du C-R, et al. Prognostic value of circulating Epstein-Barr virus DNA level post-induction chemotherapy for patients with nasopharyngeal carcinoma: a recursive partitioning risk stratification analysis. Radiother Oncol. 2023;185:109721. doi:10.1016/j.radonc.2023.109721
23. Rose AM, Helgeson ES, Valentino KC, et al. The impact of medications on salivary flow and oral health-related quality of life in postradiation head and neck cancer patients: results of the OraRad study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2025;140(5):577–586. doi:10.1016/j.oooo.2025.06.019
24. Huang G, He H, Fan Y, et al. Induction chemoradiotherapy achieves long-term recurrence-free survival in locally advanced pulmonary lymphoepithelioma-like carcinoma: a case report and literature review. Front Immunol. 2025;16:1605900. doi:10.3389/fimmu.2025.1605900
25. Chow JCH, Lee AWM, Wong CHL, et al. Epstein-Barr virus directed screening for nasopharyngeal carcinoma in individuals with positive family history: a systematic review. Oral Oncol. 2022;133:106031. doi:10.1016/j.oraloncology.2022.106031
26. Pang H, Li S, Fu X, et al. Effect of blood oxidative stress indicators on oral mucositis in patients undergoing radiotherapy for nasopharyngeal carcinoma. Eur J Med Res. 2024;29(1):573. doi:10.1186/s40001-024-02137-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Nomogram to Identify the Optimal Candidates for Induction Chemotherapy in Advanced N-Stage Nasopharyngeal Carcinoma
Jiang YT, Chen KH, Liang ZG, Yang J, Qu S, Li L, Zhu XD
Cancer Management and Research 2022, 14:2583-2596
Published Date: 31 August 2022
Development of Prognostic Nomogram Based on Lipid Metabolic Markers and Lactate Dehydrogenase in Non-Metastatic Nasopharyngeal Carcinoma
Huang R, Chen K, Jiang Y, Li L, Zhu X
Journal of Inflammation Research 2023, 16:3093-3107
Published Date: 24 July 2023
Factors related to the occurrence of fetal birth defects and the construction of a Nomogram model
Chen X, Lin L, Zhong Q, Wu H, Zheng Z, Zhang B, Lan L
Pediatric Health, Medicine and Therapeutics 2024, 15:289-298
Published Date: 9 September 2024
Influencing Factors (History of Alcohol Consumption) and Construction of a Nomogram Prediction Model for In-Hospital Gastrointestinal Bleeding Secondary to Acute Cerebral Hemorrhage in a Certain Hospital
Ye P, Luo Y
Risk Management and Healthcare Policy 2025, 18:1557-1568
Published Date: 11 May 2025
Construction of a Nomogram Prediction Model for Individualized Prediction of the Risk of Pulmonary Fungal Infection in Lung Cancer
Lai Q, Liao K, Kuang G, Liao W, Zhang S
Infection and Drug Resistance 2025, 18:3137-3147
Published Date: 26 June 2025