Back to Journals » Cancer Management and Research » Volume 18

Complementary and Alternative Therapy Use Among Cancer Patients in Qassim: Patterns, Predictors, and Patient Perspectives
Authors Alshamsan B ![]() , Alharbi LA, Alshudukhi RI, Alaql FA, Alsweed R, Alodhaybi N
, Alharbi LA, Alshudukhi RI, Alaql FA, Alsweed R, Alodhaybi N
Received 24 September 2025
Accepted for publication 1 January 2026
Published 14 January 2026 Volume 2026:18 569861
DOI https://doi.org/10.2147/CMAR.S569861
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Chien-Feng Li
Bader Alshamsan,1 Lama Awadh Alharbi,1 Razan Ibrahim Alshudukhi,1 Fai Abdullah Alaql,1 Reema Alsweed,1 Norah Alodhaybi2
1Department of Medicine, College of Medicine, Qassim University, Buraydah, Qassim, 52571, Saudi Arabia; 2Department of Medical Oncology, Prince Faisal Cancer Center, King Fahad Specialist Hospital, Qassim Health Cluster, Buraydah, Qassim, 52366, Saudi Arabia
Correspondence: Bader Alshamsan, Email [email protected]
Purpose: Complementary and alternative medicine (CAM) is widely used by cancer patients, yet regional data from Qassim, Saudi Arabia, are lacking. This study assessed the prevalence, patterns, motivations, and predictors of CAM use among cancer patients in the region.
Methods: A cross-sectional survey was conducted at Prince Faisal Cancer Center, Qassim, between February and August 2025. Eligible adults with confirmed cancer completed a culturally adapted version of the International CAM Questionnaire. CAM modalities were classified using the NCCIH/SIO framework. Descriptive statistics summarized prevalence, types, motivations, disclosure, benefits, harms, and costs. Predictors were assessed using chi-square tests and logistic regression.
Results: Among 258 participants (mean age 51.6 ± 15.1 years; 57.4% female), 145 (56.2%) reported CAM use. Most described CAM as complementary (91.0%), with 6.2% as alternative, and 2.8% as integrative. Common modalities included spiritual/faith-based (91.0%; Qur’an recitation, 74.3%; Zamzam water, 72.2%), biologically based (66.7%; olive oil, 41.7%; honey, 34.7%), and traditional remedies (53.5%; camel milk, 22.2%; camel urine, 13.9%). The main motivation was belief in a cure (91.0%). Perceived benefits were reported by 58.6% (most often improved mood, 33.8%); adverse effects were rare (6.9%) and mild. Only 23.4% disclosed CAM use to physicians, and 7.6% delayed conventional therapy. Female sex (aOR 2.29, 95% CI 1.04– 5.01) and higher education (aOR 2.48, 95% CI 1.12– 5.18) independently predicted CAM use.
Conclusion: CAM use was highly prevalent among cancer patients in Qassim, with faith-based and traditional practices most common. Curative expectations were widespread, but disclosure to physicians was low, creating a critical communication gap. Addressing this gap requires proactive, culturally sensitive physician–patient dialogue and integration of safe, evidence-based supportive practices into cancer care.
Keywords: complementary therapies, integrative oncology, neoplasms, spiritual therapies, traditional medicine, Saudi Arabia, prevalence, patient disclosure, physician–patient communication
Introduction
Research into the use of complementary and nonconventional health practices among cancer patients has been documented since the early 1980s, when surveys first highlighted their widespread adoption.1 Historically, these practices were categorized under the term complementary and alternative medicine (CAM). Complementary practices are used alongside conventional care, whereas alternative practices replace standard treatment and are strongly discouraged due to the risks of delaying or forgoing evidence-based therapies.2–4 Over the past decade, terminology has shifted toward complementary and integrative medicine (CIM) or integrative oncology (IO), reflecting the integration of evidence-based interventions, such as acupuncture for chemotherapy-induced nausea, structured exercise, and mindfulness into routine cancer care.5–7 This distinction has been reinforced by the National Center for Complementary and Integrative Health (NCCIH) and the Society for Integrative Oncology (SIO), which recommend emphasizing integrative approaches.8,9 CAM modalities in this study included Qur’an recitation, Zamzam water, herbal and nutritional remedies, self-directed exercise, mind–body practices, and traditional remedies commonly used in the region. Participants were asked to classify the purpose of each modality as complementary (used alongside medical treatment), integrative (used with perceived clinical approval), or alternative (used in place of conventional treatment). Therapies exclusively provided as part of standard medically supervised supportive oncology care were not classified as CAM.
Globally, the use of CAM among cancer patients has increased substantially, with nearly half (51%) of patients using at least one approach; however, prevalence varies widely, from approximately 16% to over 94%, across regions and populations.10 Asian countries show a pooled prevalence of roughly 49%, ranging from 24% to 94.8% across national and cultural contexts.11 In Saudi Arabia, reported use is particularly high (53–90%) among cancer patients.12–14 Uptake is influenced by demographic, socioeconomic, clinical, and psychosocial factors, with higher use observed in women, younger patients, breast cancer cases, and those with greater education.10,15–17
According to national registry data, the age-standardized incidence rate (ASR) of all cancers in Saudi Arabia has risen substantially over the past two decades, increasing from 61.4 to 144.9 per 100,000 in males and from 59.8 to 159.1 per 100,000 in females between 2002 and 2022. During this rise in ASR, Saudi Arabia’s population expanded from approximately 22 million to over 35 million, contributing to a continuous increase in the absolute number of newly diagnosed cancer cases.18,19 During the same period, substantial economic development and expansion of the national healthcare system improved access to cancer screening and treatment services. These national patterns are reflected in the Qassim region, located in the geographic center of the Kingdom, which experiences an annual population growth rate of approximately 2.3%.20 Recent registry data indicate significant annual percentage changes (APCs) for the most common cancers in Qassim, particularly breast cancer (APC 6.0%) and colorectal cancer (APC 7.3% in men and 7.2% in women), signaling an increasing burden on oncology care.21 The region benefits from a well-developed healthcare network through the Qassim Health Cluster. It demonstrates economic stability that may influence healthcare-seeking behavior and accessibility of supportive care, including CAM. Collectively, these demographics, epidemiologic, and health system characteristics make Qassim a representative setting for examining cancer-related supportive care practices and for informing culturally appropriate integrative oncology strategies regionally and nationally.
Despite this rising cancer burden and widespread CAM use among oncology patients in Saudi Arabia, data remain limited for the Qassim region. Therefore, the primary objective of this study was to determine the prevalence and patterns of CAM use among cancer patients in Qassim. Secondary objectives included identifying predictors of CAM use, exploring patients’ motivations and attitudes, and assessing their disclosure behaviors, sources of information, and perceived benefits, risks, and satisfaction.
Patients and Methods
This cross-sectional survey was conducted among cancer patients attending Prince Faisal Cancer Center (PFCC), between February 21, 2025, and August 21, 2025. PFCC is the sole comprehensive oncology referral center serving the Qassim region of Saudi Arabia. The study was approved by the Regional Research Ethics Committee, Qassim Cluster, and conducted in accordance with the Declaration of Helsinki and the guidelines of Good Clinical Practice. All participants provided written informed consent, and confidentiality was maintained throughout the study. The study adhered to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies.22
Patients were eligible if they were aged 15 years or older, had a confirmed primary cancer diagnosis, and were aware of their diagnosis. This age threshold was selected because adolescents within this age range are routinely managed in adult oncology services in Saudi Arabia. Written informed consent was obtained from participants or parents/guardians when required. Patients were excluded if they were newly diagnosed and had not yet initiated cancer therapy, had completed cancer-directed treatment more than one year earlier, or were hospitalized in palliative care units. Those with severe illnesses or cognitive impairments that prevented them from communicating were also excluded.
The sample size was calculated using OpenEpi, assuming a prevalence of 50%, a 95% confidence level, a 5% margin of error, and an eligible population diagnosed within the past 12 months. A conservative prevalence of 50% was selected because it yields the largest required sample size when the true prevalence is uncertain. Although previous Saudi studies reported CAM use estimates of 70–90% in tertiary oncology centers, these may overestimate community-level use in Qassim. Using 50% therefore minimized the risk of underpowering the study. The required sample size was 249 patients, and 350 patients were approached to account for potential nonresponse.
The survey instrument was adapted from the International CAM Questionnaire (I-CAM-Q), a validated tool widely used to assess CAM use.23 Its design was further informed by a systematic review of CAM survey methodologies in oncology24 and by studies conducted in Saudi Arabia.13,14 The questionnaire assessed prevalence of CAM use, classification of its role within the treatment plan (complementary, alternative, or integrative), healthcare providers’ reactions to disclosure, willingness to recommend CAM to others, timing of CAM use (before, during, or after conventional treatment), frequency, motivations, sources of information, perceived benefits, adverse events, costs, and satisfaction.
To ensure linguistic and cultural accuracy, the questionnaire was translated into Arabic, back-translated into English, and reviewed by bilingual oncologists and linguists. Given its multidomain structure, internal consistency statistics such as Cronbach’s α were not applicable.25,26 A pilot test was conducted with 30 cancer patients in Qassim to evaluate clarity, acceptability, and response burden, resulting in only minor wording refinements based on participant feedback. The final questionnaire was administered face-to-face by trained research staff to ensure clarity, minimize missing responses, and allow patients to seek clarification when needed. The full English version of the questionnaire is provided in Supplementary Figure 1.
The questionnaire consisted of three sections, covering eligibility screening, sociodemographic and clinical characteristics, and CAM use, attitudes, and practices. The CAM section assessed prevalence, timing, frequency, reasons for use, types of CAM, sources of information, disclosure to healthcare providers, perceived benefits, adverse events, cost, and satisfaction. Items were considered CAM when patients reported using them with the intention of complementing cancer treatment, alleviating symptoms, or improving health and well-being. CAM modalities were classified using the framework of NCCIH and SIO, with adaptation to include culturally specific practices relevant to the Saudi context. Five domains were defined: spiritual/faith-based practices, mind–body practices, biologically based practices, manipulative and body-based practices, and traditional practices. Energy therapies were not included due to cultural irrelevance within this population.
The survey included 32 predefined CAM items distributed across these five domains [faith-based (3 items), biologically based (13 items), mind–body (7 items), manipulative and body-based (3 items), and traditional remedies (6 items)]. Participants were also able to report “other” CAM modalities not listed in the questionnaire, and these were subsequently classified under the appropriate domain. In total, 47 CAM items (32 predefined and 15 additional) were analyzed. Notably, several indigenous remedies such as rusf, did al-dub’ah, and sabkha emerged through this process and were categorized under traditional practices.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics for Mac, Version 30.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize sociodemographic and clinical characteristics, as well as the prevalence and types of CAM use. Patients were categorized into three groups: adolescent/young adult (AYA, 15–39 years), older adult (OA, 40–64 years), and elderly (≥65 years). These age categories align with internationally recognized oncology standards reflecting distinct clinical and survivorship characteristics.27–29 Categorical variables were presented as frequencies and percentages, while continuous variables were expressed as means with standard deviations (SD) or medians with interquartile ranges (IQR), as appropriate. Baseline characteristics were compared between CAM users and non-users (Table 1). The chi-square test or Fisher’s exact test was applied for categorical variables, and the independent samples t-test or Mann–Whitney U-test for continuous variables, depending on normality of distribution.
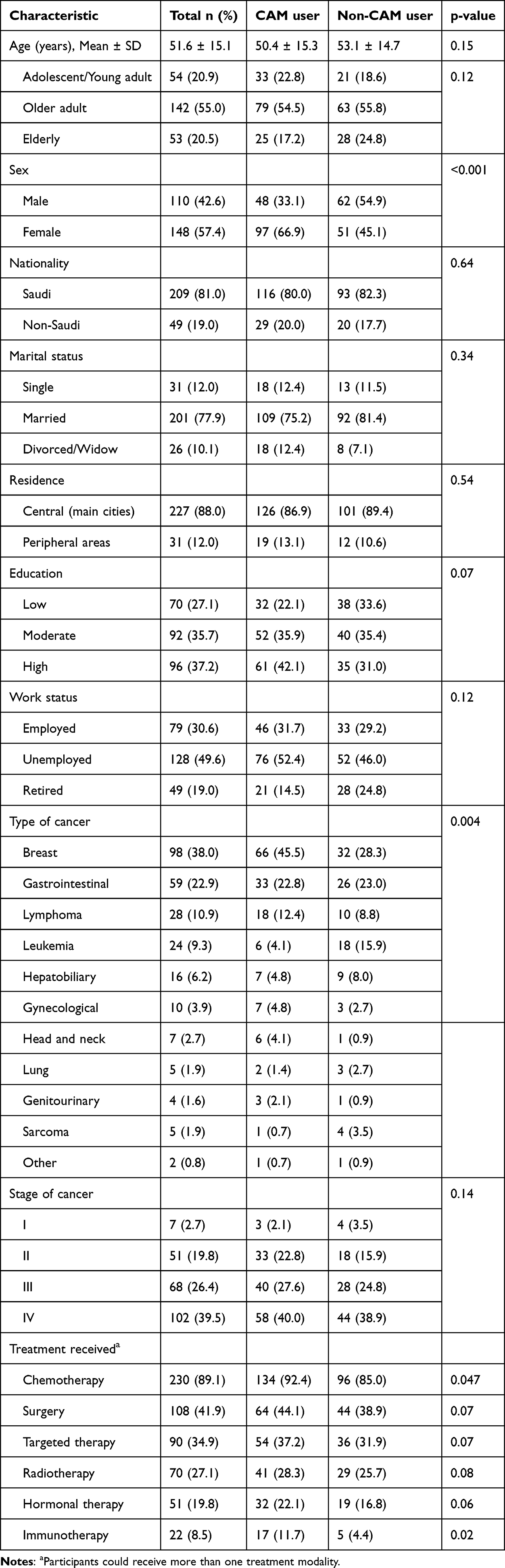 |
Table 1 Sociodemographic and Clinical Characteristics of Study Participants Stratified by CAM Use (n = 258) |
To identify predictors of CAM use, univariate logistic regression analyses were first conducted. Variables with p < 0.10 in univariate analyses were subsequently entered into a multivariable logistic regression model using the enter method, with results expressed as odds ratios (ORs) and 95% confidence intervals (CIs). A two-sided p < 0.05 was considered statistically significant.
Results
Participant Eligibility and Characteristics
During the study period, 350 patients were approached. Forty-five were excluded because they were younger than 15 years (n=13), lacked a confirmed cancer diagnosis (n=16), or were not aware of their diagnosis (n=16). Of the 305 eligible patients, 47 declined or did not complete the questionnaire, resulting in a final analytic sample of 258 patients (84.6% response rate). The mean age was 51.6 years (SD = 15.1). Females represented 148 (57.4%) of participants, 209 (81.0%) were Saudi nationals, 201 (77.9%) were married, and 227 (88.0%) resided in urban areas. Breast cancer was the most frequent diagnosis (38.0%), followed by gastrointestinal cancers (22.9%). The majority (89.1%) received chemotherapy, while 41.9% had surgery and 34.9% targeted therapy. The detailed sociodemographic and clinical characteristics, including comparisons between CAM and non-CAM groups, are presented in Table 1. Reasons for CAM non-use are summarized in Table 2.
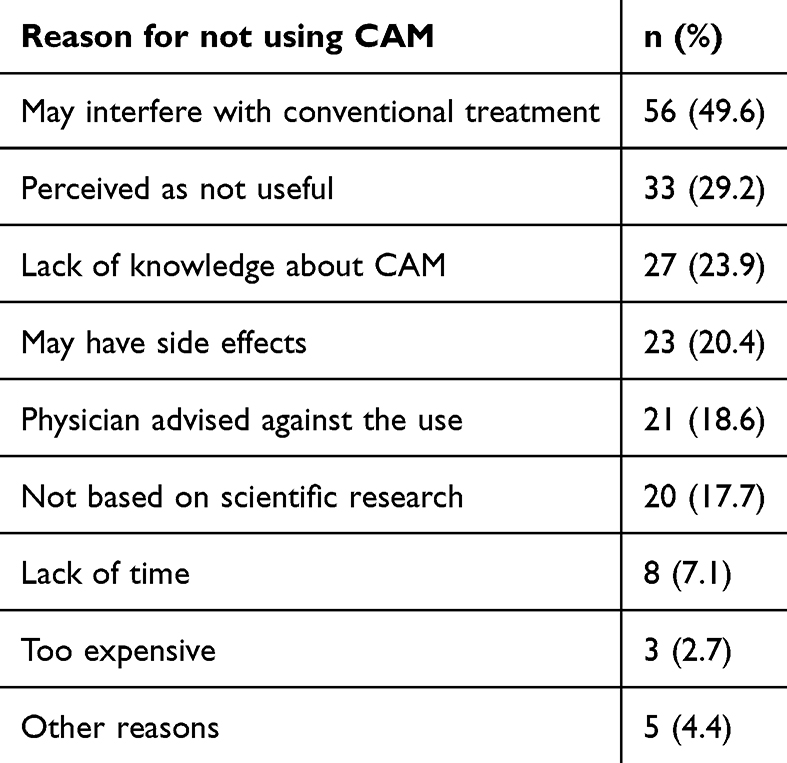 |
Table 2 Reasons for Not Using Complementary and Alternative Medicine (CAM) Among Non-Users (n = 113) |
Prevalence, Patterns, and Predictors of CAM Use
Overall, 145 (56.2%) patients reported using CAM. Most reported CAM use before treatment (57.9%) or concurrently during therapy (57.9%), while only 2.8% started after completing treatment. In terms of frequency, CAM was used daily by 92 (63.4%), weekly by 15 (10.3%), occasionally by 33 (22.8%), and only once by 5 (3.4%). Most patients considered CAM complementary (91%), with a smaller proportion describing it as alternative (6.2%) or integrative (2.8%); however, 11 (7.6%) patients reported delaying conventional treatment in favor of CAM. The most frequent sources of information were religious beliefs (49.7%, n=72) and family/friends (37.2%, n=54), followed by social media (26.9%, n=39) and cultural traditions (23.4%, n=34). Few patients cited alternative medicine practitioners (6.2%, n=9) or healthcare providers (1.4%, n=2).
On univariate analysis, CAM use was more common among females, younger patients, those with higher education, and breast cancer cases. In multivariable analysis, both female sex (OR 2.29, 95% CI 1.04–5.01, p = 0.03) and higher education (OR 2.48, 95% CI 1.12–5.18, p = 0.01) remained independent predictors. Detailed univariate and multivariable logistic regression results are presented in Table 3.
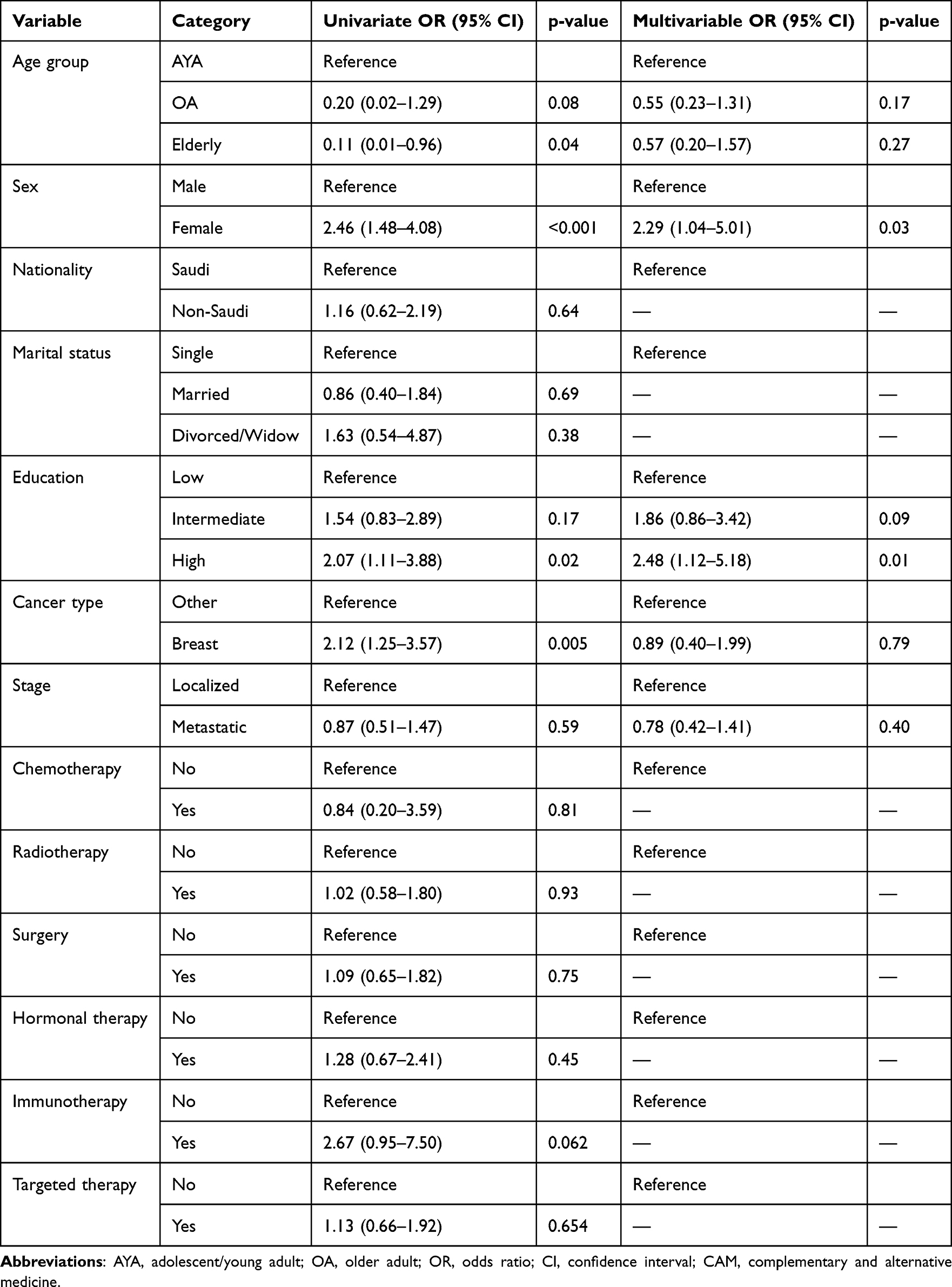 |
Table 3 Univariate and Multivariable Logistic Regression of Factors Associated with Complementary and Alternative Medicine (CAM) Use |
Types and Domains of CAM Used
Among CAM users (n=145), spiritual/faith-based practices were most common (91.0%), followed by biologically based (66.7%) and traditional remedies (53.5%). Mind-body practices (14.6%) and manipulative/body-based methods (5.6%) were less frequent; no energy-based therapies were reported. The domain distribution is shown in Figure 1. Overlap between domains was frequent (Figure 2): 32 (22.1%) patients used only spiritual/faith-based practices, 7 (4.8%) only biologically based practices, and 13 (9.0%) only traditional remedies, while 60 patients (41.4%) reported using all three domains.
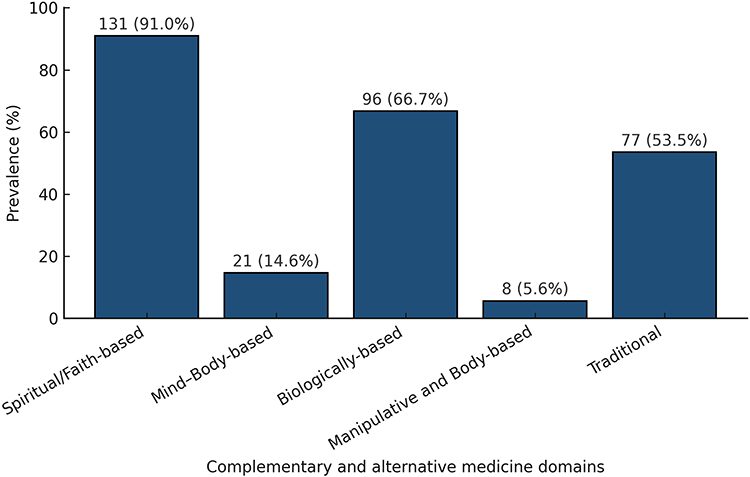 |
Figure 1 Prevalence of complementary and alternative medicine (CAM) use by domain among cancer patients in Qassim, Saudi Arabia (N = 145). |
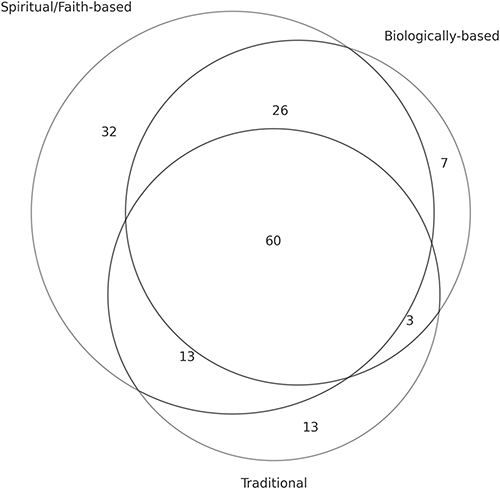 |
Figure 2 Venn diagram illustrating overlap between the three most frequently reported CAM domains: spiritual/faith-based, biologically based, and traditional remedies. |
At the item level, Qur’an recitation (74.3%), Zamzam water (72.2%), olive oil (41.7%), honey (34.7%), and black seed (27.1%) were the most frequently used items. Within traditional remedies, camel milk (22.2%) and camel urine (13.9%) were also commonly used, followed by talbinah (9.7%), whereas sabkha was rare (0.7%). Detailed item-level distributions across all domains are presented in Table 4. Beyond prevalence, the number of practices used per patient varied by domain: spiritual/faith-based (median 2, IQR 2–3; range 1–3), biologically based (median 2, IQR 1–3; range 1–6), and traditional (median 2, IQR 1–3; range 1–9). Mind–body and manipulative/body-based users typically reported a single practice (median 1; range 1–2).
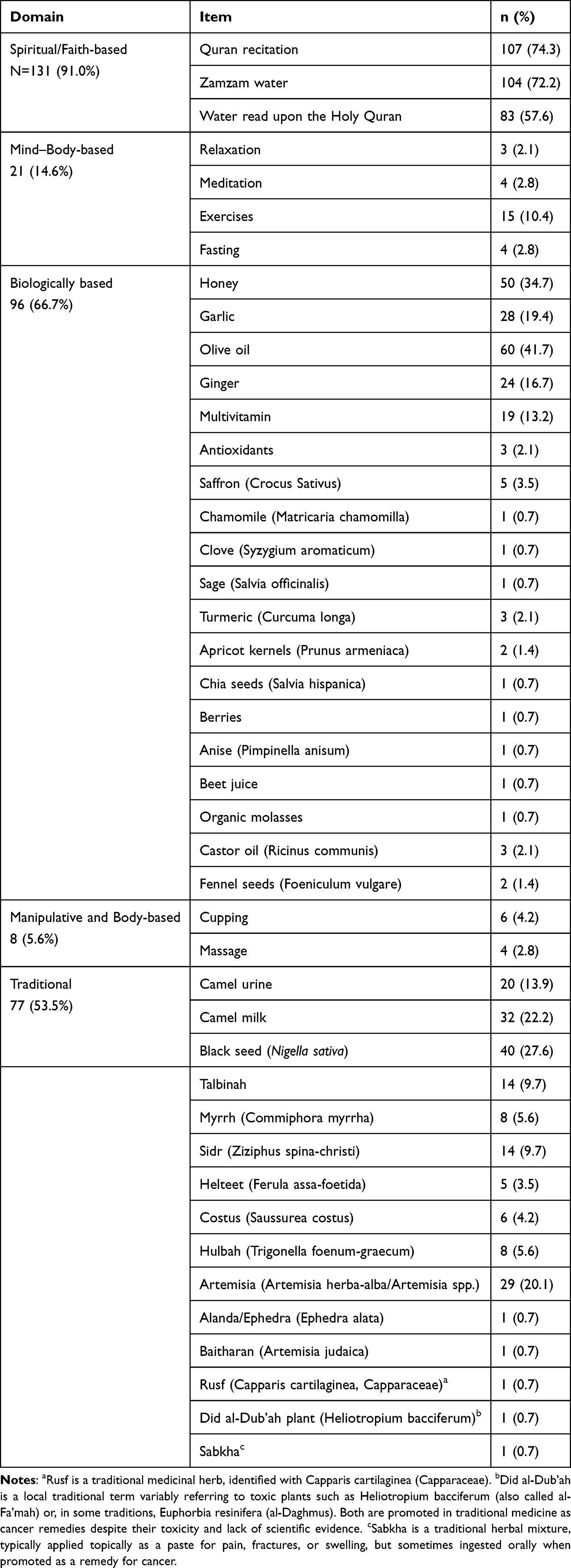 |
Table 4 Prevalence of Individual Complementary and Alternative Medicine (CAM) Items by Domain Among Cancer Patients in Qassim (N = 145) |
Motivations, Perceived Benefits, and Adverse Events
The most common motivation for CAM use was the belief that it could cure cancer (91.0%). Other reasons included boosting the immune system (22.4%), and reducing emotional distress (15.0%). The relative distribution of reasons is shown in Figure 3. Overall, 85 participants (58.6%) reported perceiving benefits from CAM, 39 (26.9%) were unsure, and 21 (14.5%) reported no benefit. The most common benefits were improved mood (33.8%), better physical health (18.6%), and pain relief (13.1%). Detailed perceived benefits are presented in Figure 4. Adverse events were infrequently reported: 10 (6.9%) participants experienced side effects such as abdominal pain, vomiting, dizziness, fatigue, or urinary retention, while 7 (4.8%) were unsure. The majority reported no adverse effects.
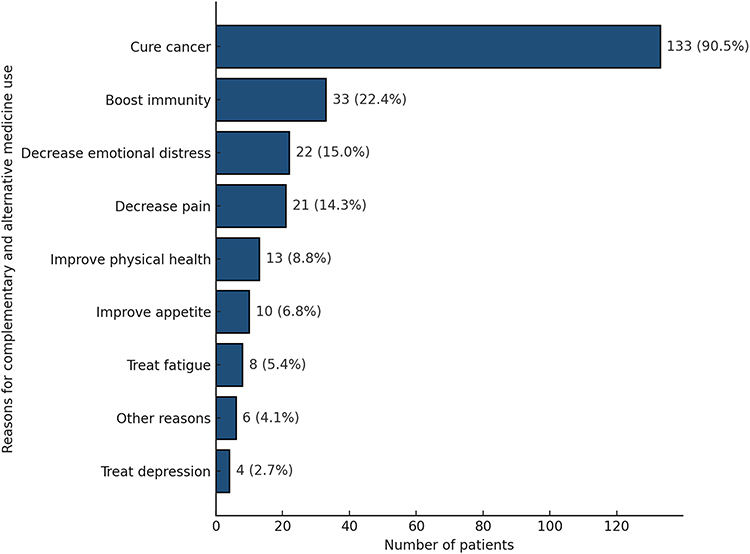 |
Figure 3 Reported reasons for complementary and alternative medicine (CAM) use among cancer patients in Qassim (N = 145). Participants could select more than one reason. Percentages are based on the total number of CAM users. “Other” reasons were reported by 6 (4.1%) patients and included managing mouth sores, fever, vomiting, infection, nausea, or dream-related concerns (one case each). |
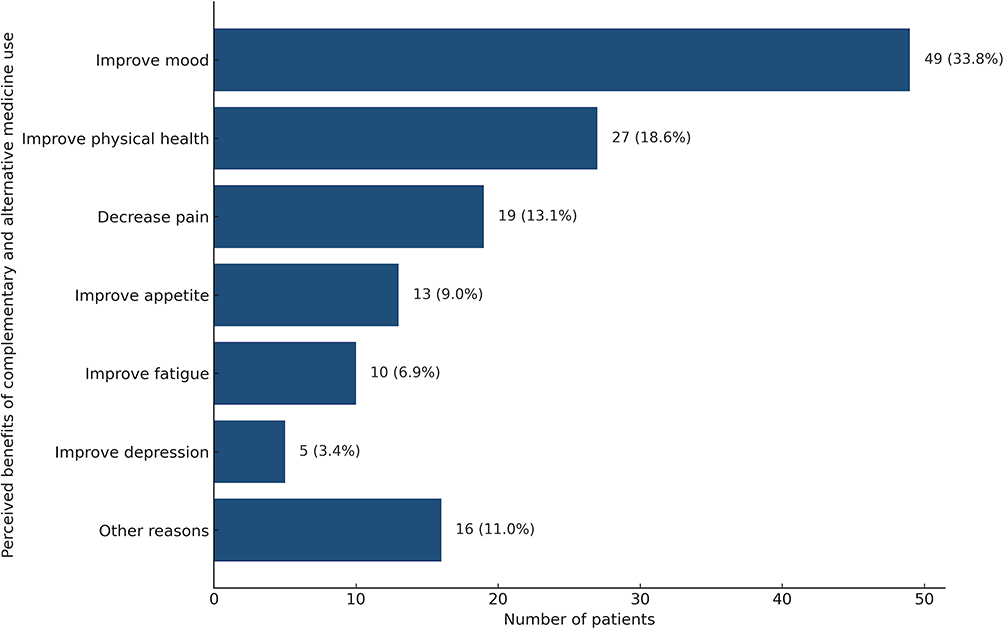 |
Figure 4 Reported perceived benefits of complementary and alternative medicine (CAM) use among cancer patients in Qassim (N = 145). Participants could select more than one benefit. “Other” responses (11.0%, N = 16) included perceived tumor shrinkage/disease control (N = 7), improved laboratory results (Hemoglobin, blood sugar; N = 3), improved immunity (N = 3), treated mouth ulcer/infection (N = 2), and relieved constipation (N = 1). |
Costs, Satisfaction, and Disclosure
Most CAM users reported low monthly costs, with 91 (62.8%) spending ≤100 Saudi Riyals (SAR), 33 (22.8%) spending 101–500 SAR, and 20 (13.8%) spending 501–1000 SAR. Satisfaction was generally high: 82 (56.6%) were very satisfied and 20 (13.8%) satisfied, though 31 (21.4%) were neutral and 11 (7.5%) dissatisfied. A large majority (73.8%) stated they would recommend CAM to others. Despite this, disclosure to healthcare providers was uncommon (23.4%). Among those who disclosed, most informed their physicians, who responded supportively in 50.0% of cases, discouragingly in 32.4%, and neutrally in 17.6%.
Discussion
This study showed that CAM use is common among cancer patients and is mainly practiced alongside conventional therapy. Faith-based practices were most common, followed by biologically based and traditional remedies. Most patients sought CAM with curative intent and perceived benefit, yet disclosure to physicians was low, and some delayed conventional therapy. Female sex and higher education were independent predictors of CAM use. These findings underscore the importance of understanding cultural context, patient motivations, demographic factors, communication challenges, and safety considerations within cancer care.
CAM use in Qassim (56.2%) aligns closely with recent estimates from Jeddah (52.9%) and is lower than the historically higher utilization reported in older Saudi cohorts (70–90%), consistent with emerging national longitudinal evidence of a gradual decline in CAM use over time.12–14,30 Among CAM users, faith-based practices were predominant (90%), reflecting the central role of religion in coping with serious illness in Saudi Arabia. These spiritually oriented approaches, such as Qur’an recitation and Zamzam water, are deeply rooted in Islamic beliefs about healing, widely regarded as safe, and provide emotional, psychological, and spiritual support.31–34 In contrast, CAM patterns in many Western settings are characterized by supplements, acupuncture, and mind–body therapies.35–38
The high prevalence of curative expectations is striking compared to Western cohorts; however, in the majority (93%), there were no treatment delays,10,39 indicating that most patients use CAM as a supportive rather than a substitutive approach. Nevertheless, a subset of patients may be at risk when using certain traditional or biologically based remedies. Some remedies, such as camel urine, lack evidence of benefit and may be harmful, while others may interact with cancer therapies, underscoring the need for routine clinical inquiry.40–43 Several biologically based and traditional products, including Artemisia species (20.1%), Ephedra (Alanda) preparations (0.7%), and other unregulated herbal mixtures, have been associated with clinically significant hepatotoxicity and cardiotoxicity in international pharmacovigilance reports.44,45 Notably, camel urine was used by 13.9% of Qassim patients, similar to national cohorts (8–15%), indicating that its use remains a persistent cultural practice rather than a region-specific phenomenon.12,14,30
Low disclosure rates mirror international patterns and reflect a critical communication gap. In our cohort, 77% of patients did not disclose their CAM use to healthcare providers, consistent with nondisclosure rates of 20% to 77% reported globally.46 A recent meta-analysis of 30 studies including 8,721 participants confirmed nondisclosure rates most often in the 40–60% range.47 Multiple factors may contribute to nondisclosure, including fears of disapproval from clinicians, perceptions that healthcare providers lack knowledge or acceptance of CAM, beliefs that spiritual practices are inherently safe and therefore do not require medical oversight, and limited consultation time.46,48,49 Physician responses to disclosure were mixed, underscoring the need for proactive, culturally sensitive dialogue to foster trust and ensure patient safety. Prior studies indicate that nearly half of patients would welcome physician inquiry into their spiritual needs, yet such discussions remain uncommon, and many patients feel their needs are unmet.50 Evidence also shows that the influence of spirituality and religiosity extends beyond patients, with oncologists’ own spiritual or religious orientations shaping not only their personal use of CAM but also their likelihood of addressing it in clinical practice.51 While our analysis highlighted female sex and higher education as independent predictors, other studies confirm that spirituality itself is also a significant predictor of CAM use, independent of religiosity.36 Taken together, these findings show that spirituality is an important part of cancer care and that both patient and physician perspectives strongly influence whether CAM is discussed, used, or integrated into treatment.
Given the high prevalence of CAM use, strong cultural and spiritual motivations, and low disclosure to physicians observed in this study, implementing an IO approach may help address patient needs while ensuring treatment safety. IO combines evidence-based mind–body practices, natural products, and lifestyle interventions with conventional therapy.52 These approaches should be tailored to the patient’s symptoms, phase of care (active treatment, survivorship, or end-of-life), available resources, and personal preferences.53 In the Saudi context, this requires acknowledging spiritual and prophetic practices while guiding patients toward safe and supportive uses of integrative therapy, discouraging unproven or harmful remedies, and addressing unrealistic expectations of cure.
These findings have direct implications for oncology policy and practice in Saudi Arabia. National guidelines should encourage routine physician inquiry into CAM use, supported by training programs that enhance cultural competence and communication skills. Integrating safe, evidence-based practices, such as structured exercise, nutrition counseling, and mindfulness, into routine cancer care may help bridge the gap between patient preferences and clinical safety, reducing reliance on unproven or potentially harmful remedies. In addition, establishing clear institutional protocols for screening, documentation, and monitoring of CAM use may support safer and more consistent integration within oncology care.
This study is, to date, the first to systematically assess CAM use among cancer patients in the Qassim region, addressing a significant gap in the Saudi oncology literature. Conducted at the sole comprehensive referral center, the sample is broadly representative of both urban and rural patients. The survey instrument was culturally adapted and extended beyond prevalence to include timing, frequency, motivations, disclosure, perceived benefits and harms, costs, and satisfaction. Face-to-face interviews conducted by trained research staff, independent of the patients’ treating teams, likely reduced social desirability bias and encouraged candid reporting of sensitive practices, including the use of camel urine, treatment delays, and nondisclosure. Limitations include the cross-sectional design, which precludes causal inference, and reliance on self-report, which may introduce recall or desirability bias. Recruitment from a single center enhances internal validity but may limit generalizability. Finally, although we categorized CAM practices using the NCCIH/SIO framework, some overlap between domains was inevitable (eg, biologically based practices with spiritual significance).
Conclusion
CAM use among cancer patients in the Qassim region is highly prevalent, at the lower end of previously reported Saudi estimates, and remains centered on spiritual and traditional practices. Unlike Western patterns, where biological and mind–body therapies tend to predominate, CAM use in Qassim is shaped primarily by faith-based and culturally rooted modalities. Persistent practices such as camel urine and unregulated herbal mixtures pose potential safety risks, and low disclosure to physicians further underscores a communication gap that may affect safe cancer care. Strengthening routine CAM screening, enhancing physician communication skills, and expanding access to evidence-based supportive therapies may improve safety, reduce treatment conflicts, and promote patient trust and satisfaction.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Regional Research Ethics Committee of the Health and Curative Programs Department, Public Health and Community Health Administration, Qassim Cluster, Qassim Province (607/46/3011) on September 25, 2024. Participants were required to provide informed consent before participating in the study, demonstrating their understanding of the study’s objectives and expressing their voluntary agreement to participate in the study. All methods were performed in accordance with relevant guidelines and regulations.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis, or interpretation; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors gratefully acknowledge Qassim University, represented by the Deanship of Graduate Studies and Scientific Research, for the financial support for this research under the number (QU-UG-2-2025-56210) during the academic year 1446 AH / 2024 AD.
Disclosure
The authors declare that the research was conducted without commercial or financial relationships that could be construed as potential conflicts of interest.
References
1. Cassileth BR, Lusk EJ, Strouse TB, Bodenheimer BJ. Contemporary unorthodox treatments in cancer medicine. Ann Intern Med. 1984;101(1):105–15. doi:10.7326/0003-4819-101-1-105
2. National Cancer Institute. Complementary and alternative medicine (CAM). [Internet]. Available from: https://www.cancer.gov/about-cancer/treatment/cam.
3. National Center for Complementary and Integrative Health. Complementary, alternative, or integrative health: what’s in a name? [Internet]. Available from: https://www.nccih.nih.gov/health/complementary-alternative-or-integrative-health-whats-in-a-name.
4. Mujar NMM, Dahlui M, Emran NA, et al. Complementary and alternative medicine use and delays in presentation and diagnosis of breast cancer patients in public hospitals in Malaysia. PLoS One. 2017;12(4):e0176394. doi:10.1371/journal.pone.0176394
5. Witt CM, Balneaves LG, Cardoso MJ, et al. A comprehensive definition for integrative oncology. J Natl Cancer Inst Monogr. 2017;2017(52):3–8. doi:10.1093/jncimonographs/lgx012
6. Latte-Naor S, Mao JJ. Putting integrative oncology into practice: concepts and approaches. J Oncol Pract. 2019;15(1):7–14. doi:10.1200/JOP.18.00562
7. Yan Y, López-Alcalde J, Zhang L, Siebenhüner AR, Witt CM, Barth J. Acupuncture for the prevention of chemotherapy-induced nausea and vomiting in cancer patients: a systematic review and meta-analysis. Cancer Med. 2023;12(11):12504–12517. doi:10.1002/cam4.5962
8. National Center for Complementary and Integrative Health. NCCIH homepage [Internet]. Available from: https://www.nccih.nih.gov/.
9. Society for Integrative Oncology. Society homepage [Internet]. Available from: https://integrativeonc.org/.
10. Keene MR, Heslop IM, Sabesan SS, Glass BD. Complementary and alternative medicine use in cancer: a systematic review. Complement Ther Clin Pract. 2019;35:33–47. doi:10.1016/j.ctcp.2019.01.004
11. Choi S, Karki Kunwor S, Im H, et al. Traditional and complementary medicine use among cancer patients in Asian countries: a systematic review and meta-analysis. Cancers. 2024;16(18):3130. doi:10.3390/cancers16183130
12. Almouaalamy NA, Banjar LA, Alshaikh HM, Altowairqi JM, Alharbi NM, Alghamdi WA. The prevalence and pattern of complementary and alternative medicine use among cancer patients in a tertiary oncology center: a cross-sectional study. Ann Med Surg Lond. 2023;85(11):5420–5427. doi:10.1097/MS9.0000000000001315
13. Jazieh AR, Al Sudairy R, Abulkhair O, et al. Use of complementary and alternative medicine by patients with cancer in Saudi Arabia. J Altern Complement Med. 2012;18(11):1045–1049. doi:10.1089/acm.2011.0266
14. Abuelgasim KA, Alsharhan Y, Alenzi T, Alhazzani A, Ali YZ, Jazieh AR. The use of complementary and alternative medicine by patients with cancer: a cross-sectional survey in Saudi Arabia. BMC Complement Altern Med. 2018;18(1):88. doi:10.1186/s12906-018-2150-8
15. Hutten RJ, Weil CR, Barney BM, et al. Complementary and alternative medicine exposure in oncology (CAMEO) study: a multi-institutional cross-sectional analysis of patients receiving cancer treatment. J Clin Oncol. 2022;40(16_suppl):e18739. doi:10.1200/JCO.2022.40.16_suppl.e18739
16. Emami SAH, Khajeh-Mehrizi A, Safaee-Nodehi SR, Dabiri MR, Emami SAM. Complementary and alternative medicine among adult cancer patients: a cross-sectional study. Holist Nurs Pract. 2025;39(2):80–85. doi:10.1097/HNP.0000000000000665
17. Stöcker A, Mehnert-Theuerkauf A, Hinz A, Ernst J. Utilization of complementary and alternative medicine (CAM) by women with breast cancer or gynecological cancer. PLoS One. 2023;18(5):e0285718. doi:10.1371/journal.pone.0285718
18. General Authority for Statistics (GaStat). Central department of statistics and information (CDSI) homepage [Internet]. Riaydh. Available from: https://www.stats.gov.sa/en/home.
19. Saudi Cancer Registry. Annual reports [Internet]. Riyadh: Ministry of Health, Saudi Cancer Registry. Available from: https://shc.gov.sa/en/NCC/Activities/Pages/NewAR.aspx.
20. Qassim Municipality. Qassim municipality official site [Internet]. Qassim: Qassim Municipality. Available from: https://www.qassim.gov.sa.
21. Alshamsan B.Trends of cancer incidence in Qassim Region, a descriptive analysis of data from the Saudi Cancer registry 2002-2016. Int J Health Sci. 2022;16(5):21–31.
22. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. STROBE initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–808. doi:10.1136/bmj.39335.541782.AD
23. Quandt SA, Verhoef MJ, Arcury TA, et al. Development of an international questionnaire to measure use of complementary and alternative medicine (I-CAM-Q). J Altern Complement Med. 2009;15(4):331–339. doi:10.1089/acm.2008.0521
24. Horneber M, Bueschel G, Dennert G, Less D, Ritter E, Zwahlen M. How many cancer patients use complementary and alternative medicine: a systematic review and metaanalysis. Integr Cancer Ther. 2012;11(3):187–203. doi:10.1177/1534735411423920
25. Streiner DL. Starting at the beginning: an introduction to coefficient alpha and internal consistency. J Pers Assess. 2003;80(1):99–103. doi:10.1207/S15327752JPA8001
26. Sijtsma K. On the use, the misuse, and the very limited usefulness of Cronbach’s alpha. Psychometrika. 2009;74(1):107–120. doi:10.1007/s11336-008-9101-0
27. Bergerot CD, Temin S, Verduzco-Aguirre HC, et al. Geriatric assessment: ASCO global guideline. JCO Glob Oncol. 2025;11(11):e2500276. doi:10.1200/GO-25-00276
28. Ferrari A, Stark D, Peccatori FA, et al. Adolescents and young adults (AYA) with cancer: a position paper from the AYA working group of the European society for medical oncology (ESMO) and the European society for paediatric oncology (SIOPE). ESMO Open. 2021;6(2):100096. doi:10.1016/j.esmoop.2021.100096
29. Li W, Liang H, Wang W, et al. Global cancer statistics for adolescents and young adults: population based study. J Hematol Oncol. 2024;17(1):99. doi:10.1186/s13045-024-01623-9
30. Jazieh AR, Abuelgasim KA, Ardah HI, Alkaiyat M, Da’ar OB. The trends of complementary alternative medicine use among cancer patients. BMC Complement Med Ther. 2021;21(1):92. doi:10.1186/s12906-021-03338-7
31. Alrawi SN, Fetters MD. Traditional arabic & islamic medicine: a conceptual model for clinicians and researchers. Glob J Health Sci. 2012;4(3):164–169. doi:10.5539/gjhs.v4n3p164
32. Omar A, Dramce G, Lakic D, Cavaco A. Exploring muslims’ health-related behaviours in Portugal: any impact on quotidian community pharmacy practice? Pharmacy. 2022;10(3):55. doi:10.3390/pharmacy10030055
33. Araz A, Harlak H, Meşe G. Factors related to regular use of complementary/alternative medicine in Turkey. Complement Ther Med. 2009;17(5–6):309–315. doi:10.1016/j.ctim.2009.09.002
34. Alrowais NA, Alyousefi NA. The prevalence extent of complementary and alternative medicine (CAM) use among Saudis. Saudi Pharm J. 2017;25(3):306–318. doi:10.1016/j.jsps.2016.09.009
35. Sanford NN, Sher DJ, Ahn C, Aizer AA, Mahal BA. Prevalence and nondisclosure of complementary and alternative medicine use in patients with cancer and cancer survivors in the United States. JAMA Oncol. 2019;5(5):735–737. doi:10.1001/jamaoncol.2019.0349
36. Dufter SA, Hübner J, Ahmadi E, Zomorodbakhsch B. Traits of cancer patients and CAM usage. J Cancer Res Clin Oncol. 2021;147(12):3685–3692. doi:10.1007/s00432-021-03605-7
37. Berretta M, Della Pepa C, Tralongo P, et al. Use of complementary and alternative medicine (CAM) in cancer patients: an Italian multicenter survey. Oncotarget. 2017;8(15):24401–24414. doi:10.18632/oncotarget.14224
38. Källman M, Bergström S, Carlsson T, et al. Use of CAM among cancer patients: results of a regional survey in Sweden. BMC Complement Altern Med. 2023;23(1):51. doi:10.1186/s12906-023-23876-2
39. Kasprzycka K, Kurzawa M, Kucharz M, et al. Complementary and alternative medicine use in hospitalized cancer patients: study from Silesia, Poland. Int J Environ Res Public Health. 2022;19(3):1333. doi:10.3390/ijerph190311600
40. Lee RT, Kwon N, Wu J, et al. Prevalence of potential interactions of medications, including herbs and supplements, before, during, and after chemotherapy in patients with breast and prostate cancer. Cancer. 2021;127(11):1827–1835. doi:10.1002/cncr.33324
41. Bazrafshani MS, Pardakhty A, Kalantari-Khandani B, et al. The prevalence and predictors of herb-drug interactions among Iranian cancer patients during chemotherapy courses. BMC Complement Med Ther. 2023;23(1):41. doi:10.1186/s12906-023-03869-1
42. Fasinu PS, Rapp GK. Herbal interaction with chemotherapeutic drugs: a focus on clinically significant findings. Front Oncol. 2019;9:1356. doi:10.3389/fonc.2019.01356
43. Al Zahrani A, Alfakeeh A, Alghareeb W, et al. Use of camel urine is of no benefit to cancer patients: observational study and literature review. East Mediterr Health J. 2023;29(8):657–663. doi:10.26719/emhj.23.050
44. Teschke R, Zhang L, Long H, et al. Traditional Chinese Medicine and herbal hepatotoxicity: a tabular compilation of reported cases. Ann Hepatol. 2015;14(1):7–19. doi:10.1016/S1665-2681(19)30796-3
45. Jităreanu A, Trifan A, Vieriu M, Caba I, Mârțu I, Agoroaei L. Current trends in toxicity assessment of herbal medicines: a narrative review. Processes. 2023;11(1):83. doi:10.3390/pr11010083
46. Davis EL, Oh B, Butow PN, Mullan BA, Clarke S. Cancer patient disclosure and patient–doctor communication of complementary and alternative medicine use: a systematic review. Oncologist. 2012;17(11):1475–1481. doi:10.1634/theoncologist.2012-0223
47. Akeeb AA, King SM, Olaku O, White JD. Communication between cancer patients and physicians about complementary and alternative medicine: a systematic review. J Integr Complement Med. 2023;29(2):80–98. doi:10.1089/jicm.2022.0516
48. Arthur K, Belliard JC, Hardin SB, Knecht K, Chen CS, Montgomery S. Reasons to use and disclose use of complementary medicine use - an insight from cancer patients. Cancer Clin Oncol. 2013;2(2):81–92. doi:10.5539/cco.v2n2p81
49. Kristoffersen AE, Nilsen JV, Stub T, et al. Use of complementary and alternative medicine in the context of cancer; prevalence, reasons for use, disclosure, information received, risks and benefits reported by people with cancer in Norway. BMC Complement Med Ther. 2022;22(1):202. doi:10.1186/s12906-022-03606-0
50. Astrow AB, Kwok G, Sharma RK, Fromer N, Smith D. Just what are spiritual needs of cancer patients? An empirical study in a diverse population [Internet]. Available from: https://www.asco.org/abstracts-presentations/ABSTRACT164936.
51. Powers-James C, Alvarez A, Milbury K, et al. The influence of spirituality and religiosity on US oncologists’ personal use of and clinical practices regarding complementary and alternative medicine. Integr Cancer Ther. 2020;19:1534735420945769. doi:10.1177/1534735420945769
52. Gowin K, Muminovic M, Zick SM, Lee RT, Lacchetti C, Mehta A. Integrative therapies in cancer care: an update on the guidelines. Am Soc Clin Oncol Educ Book. 2024;44(3):e3882048. doi:10.1200/EDBK_431554
53. Atreya CE, Leach H, Asiimwe E, et al. Integrative oncology: incorporating evidence-based approaches for patients with GI cancers. Am Soc Clin Oncol Educ Book. 2025;45(1):e4205302. doi:10.1200/EDBK_471734
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Prevalence of Complementary and Alternative Medications Use Among Dermatology Patients in Aseer Region, Saudi Arabia
Al-Atif HM, AL-Ghamdi HS, Alzubaidi WA, Alnaem NM, Qahtani SH
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2607-2615
Published Date: 6 December 2022
Complementary and Alternative Medicine to Treat Fibromyalgia Symptoms. A Systematic Review
Badanta B, Álvarez-Pérez I, Bonilla Sierra P, González-Cano-Caballero M, Lucchetti G, de Diego-Cordero R
Journal of Pain Research 2024, 17:1709-1723
Published Date: 10 May 2024
The Prevalence of Sleep Disorders in People with Type 2 Diabetes and Obesity in Saudi Arabia: A Cross-Sectional Study
AL-asiri IS, Almatrafi FG, Al-thagafi SD, AlQarni AM, Aljubran HJ, Aljamaan AK, Al-Zahrani N
Diabetes, Metabolic Syndrome and Obesity 2024, 17:2075-2083
Published Date: 20 May 2024
Nationwide Prevalence of Hepatocellular Carcinoma in Saudi Arabia: A Population-Based Analysis for 2021
De Vol EB, Bazarbashi S, Aseafan M, Aleid HS, Alnajem A, Alqahtani SA, Alqahtani A
Journal of Hepatocellular Carcinoma 2025, 12:3063-3076
Published Date: 30 December 2025
The Knowledge-Attitude-Behavior Paradox in E-Cigarette Adoption Among University Students at Northern Border University, Saudi Arabia
Alenezi IN, Mersal FA, Osman Mohamed HA, El Said FG, Alanazi FJ, Abu-Negm LM, Aboelola TH, Alrwili AG
Journal of Multidisciplinary Healthcare 2026, 19:578360
Published Date: 18 February 2026