Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
The Knowledge-Attitude-Behavior Paradox in E-Cigarette Adoption Among University Students at Northern Border University, Saudi Arabia
Authors Alenezi IN ![]() , Mersal FA
, Mersal FA ![]() , Osman Mohamed HA, El Said FG, Alanazi FJ, Abu-Negm LM
, Osman Mohamed HA, El Said FG, Alanazi FJ, Abu-Negm LM ![]() , Aboelola TH, Alrwili AG
, Aboelola TH, Alrwili AG
Received 1 November 2025
Accepted for publication 3 February 2026
Published 18 February 2026 Volume 2026:19 578360
DOI https://doi.org/10.2147/JMDH.S578360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tilakavati Karupaiah
Ibrahim Naif Alenezi,1 Fathia Ahmed Mersal,1 Heba Ahmed Osman Mohamed,2 Fathia Gamal El Said,1 Fadiyah Jadid Alanazi,1 Lobna Mohamed Abu-Negm,3 Taghreed Hussien Aboelola,1 Abdulhamid Gharib Alrwili1
1Public Health Nursing Department, Faculty of Nursing, Northern Border University, Arar, Saudi Arabia; 2Maternal and Newborn Nursing, Faculty of Nursing, Northern Border University, Arar, Saudi Arabia; 3Emergency Nursing, Faculty of Nursing, Northern Border University, Arar, Saudi Arabia
Correspondence: Fathia Ahmed Mersal, Email [email protected]
Background: The proliferation of e-cigarette use among university students presents a critical public health challenge, yet the mechanisms driving adoption in non-Western sociocultural contexts remain inadequately theorized.
Purpose: Guided by the Social Cognitive Theory and the Theory of Planned Behavior, this study investigated the prevalence and predictors of e-cigarette use among university students at Northern Border University in Saudi Arabia.
Material and Methods: A cross-sectional survey of 670 students assessed knowledge, attitudes, and usage behaviors, with predictors identified via multivariable logistic regression.
Results: The prevalence of current use was 20.6% (138/670), with a significant gender disparity where female students had lower odds of use (adjusted OR = 0.334**; 95% CI: 0.203– 0.550**). A striking knowledge-attitude-behavior paradox emerged: while 77.6% (520/670) acknowledged addiction potential, substantial gaps in knowledge about respiratory risks (only 45%, 301/670) and nicotine content (35%, 234/670) persisted. Critically, medical students, despite having superior knowledge (53.2%, 141/265 vs 28.4%, 115/405 among non-medical students), exhibited only moderately more protective attitudes (61.5% vs 78.5% disapproving). More favorable attitudes significantly predicted current use (adjusted OR = 1.040 per one-point increase**; 95% CI: 1.008– 1.073**), confirming the mediating role of attitudes.
Conclusion: These findings indicate that e-cigarette adoption is a socially embedded behavior shaped by gender norms and educational contexts, challenging information-deficit models. This underscores the necessity for theory-driven, multilevel interventions that address cognitive, affective, and normative determinants of behavior to inform culturally sensitive prevention strategies and campus policies.
Plain Language Summary: Why was the study done? E-cigarettes, or vaping, have become very popular among young people worldwide, including university students in Saudi Arabia. As traditional smoking rates fall, vaping presents new public health challenges. We conducted this study to understand what drives students to vape, looking beyond simple numbers to explore their knowledge, attitudes, and social influences.
What did the researchers do and find? We surveyed 670 university students across Saudi Arabia. We found that 1 in 5 students currently vape. A major gender difference emerged: male students were much more likely to vape than female students, likely reflecting cultural norms. A key discovery was a “knowledge-attitude gap”. Even medical students, who knew more about health risks, did not have much stronger negative opinions about vaping than their peers. Many students mistakenly believed the vapor was harmless water.
What do these results mean? Our findings show that just giving students facts about the dangers of vaping is not enough to stop them. To be effective, health programs must also address the powerful influence of friends and challenge the idea that vaping is a safe or socially acceptable activity. Interventions need to be culturally sensitive, especially considering the different social pressures on male and female students, to help them make healthier choices.
Keywords: E-cigarettes, university students, Saudi Arabia, knowledge, attitudes, practice, gender differences, prevalence, tobacco control, harm reduction
Introduction
The global tobacco control landscape has been fundamentally reshaped by the rapid proliferation of electronic nicotine delivery systems (ENDS), commonly known as e-cigarettes, which have emerged as the predominant form of nicotine consumption among youth and young adults in numerous countries.1,2 Despite substantial declines in conventional cigarette smoking over the past two decades, e-cigarettes have introduced novel public health challenges characterized by aggressive marketing, appealing flavors, and widespread misperceptions regarding their safety profile.3,4 Globally, e-cigarette users increased from 58 million in 2018 to 68 million in 2020, with adoption rates particularly pronounced among university students, who represent a critical demographic for understanding product diffusion patterns and intervention opportunities.5 Among European university students, lifetime e-cigarette use reached 43.7%, with notable gender disparities (51.3% males vs 40.5% females) reflecting both biological predispositions and sociocultural constraints on tobacco product use.5 These epidemiological trends signal an urgent need to understand the behavioral, cognitive, and social mechanisms driving e-cigarette adoption in higher education settings.
In Saudi Arabia, the nicotine consumption landscape exhibits a paradoxical trajectory: while traditional adolescent cigarette smoking rates declined from 15.9% in 2007 to 9.4% in 2022, the regulatory liberalization of e-cigarette imports in 2019 coincided with marked increases in ENDS availability and youth uptake.6,7 Recent studies among university students across various Saudi regions have documented concerning prevalence rates and patterns. Alqahtani et al8 reported a prevalence of electronic cigarette use among King Khalid University students in Abha, Aseer region, while Alahmadi and Al-Zalabani9 identified distinct patterns and factors associated with e-cigarette initiation and transition among university students in Al-Madinah City. Additionally, Alsaedi and Al-Zalabani10 demonstrated significant associations between electronic cigarette use and respiratory symptoms among university students, and Aqeeli et al11 assessed dependence and perceptions of harm and addictiveness among Saudi university students. Earlier work by Aqeeli et al12 examined awareness, knowledge, and perception of electronic cigarettes among undergraduate students in Jazan Region. University students in the Kingdom demonstrate smoking prevalence rates (17%) exceeding national averages, with pronounced gender disparities (21% males vs substantially lower female rates) that reflect intersecting cultural norms regarding masculinity, femininity, and public comportment.13 Recent Saudi surveys documented that 26.3% of individuals had used e-cigarettes at least once, while 24.7% reported familial use, indicating substantial social diffusion beyond experimental adoption.14 These patterns suggest that e-cigarettes have become embedded within the social fabric of Saudi university life, functioning not merely as nicotine delivery devices but as symbols of modernity, social sophistication, and peer group membership within evolving youth subcultures.
Understanding e-cigarette adoption requires theoretically grounded investigations of the mechanisms linking knowledge, attitudes, social influences, and behavioral outcomes. Social Cognitive Theory (SCT) posits that health behaviors emerge from dynamic, reciprocal interactions among personal factors (knowledge, risk perceptions, and self-efficacy), environmental influences (peer networks, social norms, marketing exposure, and policy contexts), and behavioral patterns (experimentation, dual use, and cessation attempts).15 Complementing SCT, the Theory of Planned Behavior (TPB) elucidates how attitudes toward vaping, subjective norms, and perceived behavioral control interact to shape behavioral intentions, which subsequently predict actual e-cigarette use.16 The Risk Perception Attitude (RPA) Framework addresses how individuals process health risk information and form behavioral intentions based on risk perceptions and efficacy beliefs.17 Collectively, these theoretical perspectives predict that e-cigarette adoption among university students constitutes a socially embedded behavior shaped by multiple, interacting determinants.
Despite growing recognition of e-cigarettes as a major public health threat among youth globally, significant knowledge gaps persist regarding adoption mechanisms in non-Western sociocultural contexts, particularly in Saudi Arabia where distinct cultural and regulatory environments shape tobacco use patterns.8–14 This study addresses these critical gaps through a comprehensive investigation at Northern Border University.
Specifically, we examined: (1) current prevalence rates of e-cigarette use across demographic subgroups, (2) the distribution and determinants of e-cigarette knowledge and risk awareness, (3) attitudes toward vaping and their relationship to usage behaviors, and (4) gender-specific patterns reflecting sociocultural norms unique to the Saudi context. We hypothesized that e-cigarette use represents a socially embedded behavior shaped by the dynamic interplay of personal factors (knowledge, attitudes), environmental influences (peer networks, gender norms), and behavioral patterns, with critical discordance between knowledge and behavior mediated by attitudes and subjective norms.
Methods
Study Design and Setting
This cross-sectional observational study employed a structured electronic survey to assess e-cigarette knowledge, attitudes, and usage behaviors among university students at Northern Border University in Saudi Arabia. Data collection occurred over 9 weeks from January 27, 2025, through March 31, 2025, at Northern Border University, a large public university located in Arar, Northern Border Region, with an enrollment of 16,415 undergraduate students across diverse academic disciplines. The cross-sectional design was selected to provide contemporary prevalence estimates and identify demographic and psychosocial correlates of e-cigarette use during a critical regulatory transition period in Saudi Arabia following the 2019 liberalization of e-cigarette import policies.
Participant Eligibility and Sampling Strategy
Target Population
The study population comprised all currently enrolled undergraduate students aged ≥18 years at Northern Border University, representing approximately 16,415 eligible individuals across medical and non-medical colleges during the 2024–2025 academic year.
Inclusion Criteria
Participants were eligible if they: (1) were currently enrolled as undergraduate students at Northern Border University; (2) were aged 18 years or older at the time of survey completion; and (3) demonstrated understanding of study procedures and voluntarily accessed the survey link.
Exclusion Criteria
Students were ineligible if they: (1) were enrolled in graduate or postgraduate programs; or (2) were under 18 years of age.
Sample Size Determination
Sample size calculations were conducted a priori to ensure adequate statistical power for detecting associations between sociodemographic predictors and e-cigarette use outcomes. Using an estimated population prevalence of 50% (p = 0.50) to maximize variance, a 99% confidence level was selected (Z = 2.576) rather than the conventional 95% confidence level to provide greater precision and reduce type I error risk in this exploratory investigation of a relatively understudied population,18 and a margin of error (d) of 5%, the required sample size was calculated as:
To account for potential incomplete responses, non-response, and data quality issues, the target sample was increased by approximately 5% to 670 participants, ensuring robust statistical power (1-β = 0.80) for detecting moderate effect sizes (OR ≥ 1.5) at α = 0.01 (consistent with the 99% confidence level used for sample size calculation).
Sampling Procedure
A convenience snowball sampling technique was employed through dissemination of the electronic survey link via multiple digital channels.19 The survey link was distributed through: (1) institutional Email invitations sent to students across all colleges; (2) announcements posted on official university learning management systems (eg, Blackboard); and (3) distribution via closed WhatsApp groups affiliated with student organizations and academic departments, with prior authorization from group administrators. To enhance representativeness, initial recruitment targeted diverse academic disciplines and year levels, with subsequent participants encouraged to share the survey link with peers (snowball component). While this approach does not permit true random selection, stratification weights were retrospectively applied during analysis based on the known distribution of age, sex, and academic discipline within the university’s undergraduate population to adjust for potential sampling biases and enhance the generalizability of findings.20
Data Collection Instrument
Questionnaire Development
The survey instrument, adapted from validated tools by Hafiz et al,21 comprised five distinct sections totaling 33 items designed to comprehensively assess e-cigarette-related knowledge, attitudes, and practices alongside relevant sociodemographic characteristics.
Section A: Sociodemographic Characteristics (9 Items)
This section collected key demographic data, including: (1) age in years (continuous variable, subsequently categorized as 18–21 vs 22–25 years); (2) biological sex (male/female); (3) marital status (single/married); (4) college affiliation (medical/health sciences vs non-medical disciplines); (5) academic year; (6) grade point average; (7) residential status (on-campus/off-campus); (8) monthly household income; and (9) parental education levels.
Section B: E-Cigarette Knowledge Assessment (9 Items)
This section evaluated participants’ factual knowledge regarding e-cigarette composition, health effects, addiction potential, and regulatory status. Each item presented a declarative statement (eg, “E-cigarettes contain nicotine”, “E-cigarette aerosol is merely harmless water vapor”), with response options of “True”, “False”, or “Don’t know”. Each correct response was scored 1 point, while incorrect or “Don’t know” responses received 0 points. Total scores ranged from 0 to 9, with higher scores indicating greater knowledge. We dichotomized knowledge levels using a 75% cut-point (≥7 correct responses out of 9) based on Bloom’s taxonomy-based classification system, which defines mastery as achieving ≥75% of the maximum possible score.22,23 This threshold is widely used in knowledge-attitude-practice (KAP) research to distinguish between adequate and inadequate knowledge levels and has demonstrated utility in previous tobacco-related studies.24,25 Participants were categorized as having “Good knowledge” (≥75% correct responses; score ≥7) or “Poor knowledge” (<75% correct responses; score <7).
Section C: Attitude Toward E-Cigarettes (10 Items)
Attitudinal dimensions were assessed using a 10-item battery employing a 5-point Likert scale with anchors: 0 = “Not sure/Don’t know”, 1 = “Strongly agree”, 2 = “Agree”, 3 = “Disagree”, and 4 = “Strongly disagree”. The coding scheme assigns 0 to “Not sure/Don’t know” responses to distinguish genuine uncertainty from informed opinions, consistent with established practices in attitude measurement where neutral or uncertain responses are treated as conceptually distinct from the agree-disagree continuum.26 This approach prevents forcing respondents without formed opinions into artificial agreement or disagreement categories, thereby enhancing measurement validity.27 Items captured perceptions of relative harm (eg, “E-cigarettes are safer than conventional cigarettes”), social acceptability (eg, “E-cigarette use enhances social status”), cessation utility (eg, “E-cigarettes are effective tools for quitting smoking”), and regulatory support (eg, “E-cigarettes should be banned on university campuses”). Items were coded such that higher total attitude scores reflected more favorable (permissive) attitudes toward e-cigarettes. The total attitude score ranged from 0 to 40, with mean scores computed for classification. Applying Bloom’s cut-off thresholds,22,23 attitudes were dichotomized as follows: “Supporting attitude” (≥75% of maximum score, ie, ≥30 points, indicating permissive or favorable views) versus “Opposed attitude” (<75% of maximum score, ie, <30 points, indicating critical or unfavorable views).
Section D: E-Cigarette Use Practices (5 Items)
This section assessed lifetime e-cigarette use (“Have you ever tried an e-cigarette, even once or twice?” coded as 0 = Yes, 1 = No), age at first use (continuous variable), frequency of current use (categorized as daily, weekly, monthly, or never), primary acquisition methods (purchase from stores, online vendors, friends/family), and self-reported reasons for use (open-ended responses subsequently coded thematically as follows: curiosity, peer influence, smoking cessation, stress relief, flavor appeal). Current e-cigarette users were identified through a direct question: “Do you currently use e-cigarettes?” with response options: daily, weekly, monthly, or never. Participants selecting any frequency (daily, weekly, or monthly) were classified as current users; those selecting “never” were classified as non-users.
Section E: Conventional Cigarette Smoking History (3 Items)
Smoking history was assessed through: (1) current smoking status (“Do you currently smoke conventional cigarettes?” with response options: Yes/No); (2) lifetime cigarette exposure (“Have you ever smoked conventional cigarettes, even once or twice?” with response options: Yes/No); and (3) quit attempts among former smokers.
For analytical purposes, the variable “past smoking history” was constructed as follows: Participants were coded as having “past smoking history” (coded = 1) if they answered “Yes” to lifetime cigarette exposure, indicating any historical cigarette smoking experience (including current smokers, former smokers, and experimenters). Participants were coded as having “no past smoking history” (coded = 0) if they answered “No” to lifetime cigarette exposure, indicating never having smoked cigarettes. A small proportion (n=12, 1.8%) of participants who preferred not to answer were grouped with the “no past smoking history” category (coded = 0) to maintain analytic sample size, though this decision may introduce conservative bias.
It is important to note that this variable definition differs from conventional epidemiological classifications that typically distinguish current smokers, former smokers, and never smokers as separate categories. The current coding scheme may obscure important distinctions between these subgroups and could explain counterintuitive findings in multivariable analyses. Future investigations should employ more granular smoking history categorization to better elucidate the relationship between conventional cigarette smoking and e-cigarette use.
Psychometric Properties
The reliability and internal consistency of the instrument were rigorously evaluated before substantive analysis. For the knowledge section employing dichotomous scoring, the Kuder-Richardson Formula 20 (KR-20) coefficient was calculated to assess the reliability of binary items, yielding KR-20 = 0.78, which exceeds the minimum acceptable threshold of 0.70 and indicates satisfactory internal consistency. For the attitude section utilizing Likert-scale responses, Cronbach’s alpha was computed to evaluate scale reliability, yielding α = 0.86, demonstrating strong internal coherence and justifying the computation of composite attitude scores. Content validity was established through expert panel review involving three tobacco control specialists and two survey methodologists who evaluated item relevance, clarity, and cultural appropriateness for the Saudi Arabian context. Pilot testing with 30 students (excluded from final analyses) confirmed face validity and identified minor wording ambiguities, which were subsequently refined.
Data Collection Procedures
Electronic Survey Administration
Data were collected via a self-administered electronic questionnaire designed using Google Forms, a secure, HIPAA-compliant survey platform. The survey link was disseminated through multiple channels to maximize reach within the convenience sampling framework: (1) institutional Email invitations sent to students across all colleges; (2) announcements posted on official university learning management systems (eg, Blackboard); and (3) distribution via closed WhatsApp groups affiliated with student organizations and academic departments, with prior authorization from group administrators.
To prevent duplicate responses from the same participant across different dissemination channels, several technical measures were implemented:28 (1) Google Forms was configured to require institutional Email authentication (Northern Border University Email addresses only), which automatically restricts each authenticated account to one submission; (2) browser fingerprinting via cookies was enabled to flag potential duplicate submissions from the same device; (3) timestamp analysis was conducted to identify and remove submissions with identical or near-identical response patterns within short-time intervals; and (4) during data cleaning, responses with identical demographic profiles and response patterns were manually reviewed, with duplicates removed and only the first complete response retained for analysis. These combined measures reduced the likelihood of duplicate responses, though complete elimination cannot be guaranteed in web-based surveys.
Ethical Considerations
This study was conducted in full accordance with the ethical principles articulated in the Declaration of Helsinki (2013 revision) and received prospective approval from the Local Committee of Bioethics at Northern Border University (Protocol Number: HAP-09-A-043; Approval Date: January 27, 2025; Decision Number: 2/25/H). Additional administrative approval was secured from academic deans of participating colleges before survey dissemination.
Informed Consent
Upon accessing the survey link, eligible participants (verified as ≥18 years old and currently enrolled undergraduate students) encountered a multi-stage informed consent protocol. The electronic survey presented: (1) a detailed information sheet describing the study’s purpose, procedures, voluntary nature, potential risks/benefits, confidentiality protections, and contact information for the research team and institutional review board; (2) a mandatory verification checkbox confirming the participant was ≥18 years of age; and (3) a separate mandatory consent checkbox stating “I have read the above information and voluntarily agree to participate in this research study”. Survey questions were inaccessible until both checkboxes were affirmatively selected, ensuring informed consent was obtained after eligibility verification but before data collection. Participants were explicitly informed of their right to withdraw at any point without penalty.
Confidentiality and Data Protection
To safeguard participant privacy, no personally identifiable information (names, student identification numbers, or IP addresses) was collected. All data were stored on password-protected, encrypted servers accessible only to authorized research team members. Deidentified datasets used for statistical analysis were assigned anonymous study identification numbers, precluding linkage to individual participants. In compliance with Saudi Arabian data protection regulations and international research ethics standards, data will be securely archived for a minimum of five years post-publication before authorized destruction.
Vulnerable Populations Protections
Although university students aged 18–25 years are generally considered capable of autonomous consent, particular attention was paid to avoiding coercion. Survey distribution via multiple channels (email, learning platforms, social media) ensured no single individual could identify who did or did not participate. No course credit, grade adjustments, or monetary compensation were offered, eliminating extrinsic incentives that might compromise voluntariness.
Statistical Analysis
All analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corporation, Armonk, NY, USA). Continuous variables were summarized as mean ± SD or median (IQR), while categorical variables were reported as frequencies and percentages.
Normality of continuous variables was assessed using both Shapiro–Wilk and Kolmogorov–Smirnov tests because these tests have different sensitivity characteristics: the Shapiro–Wilk test has superior statistical power for small-to-moderate sample sizes (n<50 per group) and is more sensitive to deviations in the tails of the distribution, while the Kolmogorov–Smirnov test is more appropriate for larger samples and is less affected by tied values. Using both tests provided complementary information about distributional properties and enhanced the robustness of our assessment, particularly given the heterogeneous subgroup sample sizes in our study.29
Bivariate associations were examined using Pearson’s chi-square or Fisher’s exact test for categorical variables, Welch’s t-test for continuous variables across two groups, and Kruskal–Wallis H-test for non-normally distributed continuous variables across multiple groups, with Dunn’s test for post-hoc comparisons.
Binary logistic regression was employed to identify independent predictors of current e-cigarette use. The model included age, sex, marital status, college type, past smoking history, knowledge score, and attitude score as covariates. Model assumptions were verified through Box-Tidwell tests for linearity, variance inflation factors (<5) for multicollinearity, and the Peduzzi criterion for sample size adequacy. Results are reported as adjusted odds ratios (AOR) with 95% confidence intervals (CI). Model fit was evaluated using log-likelihood ratio test, Nagelkerke R2, and the Hosmer–Lemeshow goodness-of-fit test.
Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC-ROC) with fivefold cross-validation. Calibration was evaluated using calibration intercept and slope, Brier score, and calibration plots with observed-to-expected ratios across deciles of predicted risk.
Missing data (<2%) were handled via complete case analysis, confirmed as appropriate by Little’s MCAR test (p = 0.34). Subgroup analyses examined effect modification by sex and college type. Statistical significance was set at p < 0.01 (two-tailed) for primary analyses to maintain consistency with the 99% confidence level used in sample size determination, with Bonferroni correction applied to multiple post-hoc comparisons. The sample size provided 89% power to detect odds ratios of ≥1.5 for predictors with prevalence ≥20%.
Results
Study Population Characteristics and E-Cigarette Use Prevalence
A total of 670 university students were included in this cross-sectional analysis. The mean age was 20.50 years (SD = 1.50), with 503 participants (75.1%) aged 18–21 years and 167 participants (24.9%) aged 22–25 years. The sample comprised 385 males (57.5%) and 285 females (42.5%). Most participants were single (563 students, 84.0%), while 107 (16.0%) were married. Regarding academic enrollment, 405 students (60.4%) were enrolled in non-medical colleges, with the remainder (265 students, 39.6%) in medical programs.
Among all participants, 138 (20.6%) reported current e-cigarette use, while 532 (79.4%) were classified as non-users. Past smoking history was reported by 178 participants (26.6%). The mean e-cigarette knowledge score was 5.12 (SD = 1.45, range 1–9), and the mean attitude score was 23.40 (SD = 6.48, range 10–48).
Table 1 presents the distribution of current e-cigarette use across sociodemographic characteristics and key study variables. Percentages are calculated from row totals to facilitate comparison of e-cigarette use prevalence within each category of exposure variables (age, sex, college type, etc).
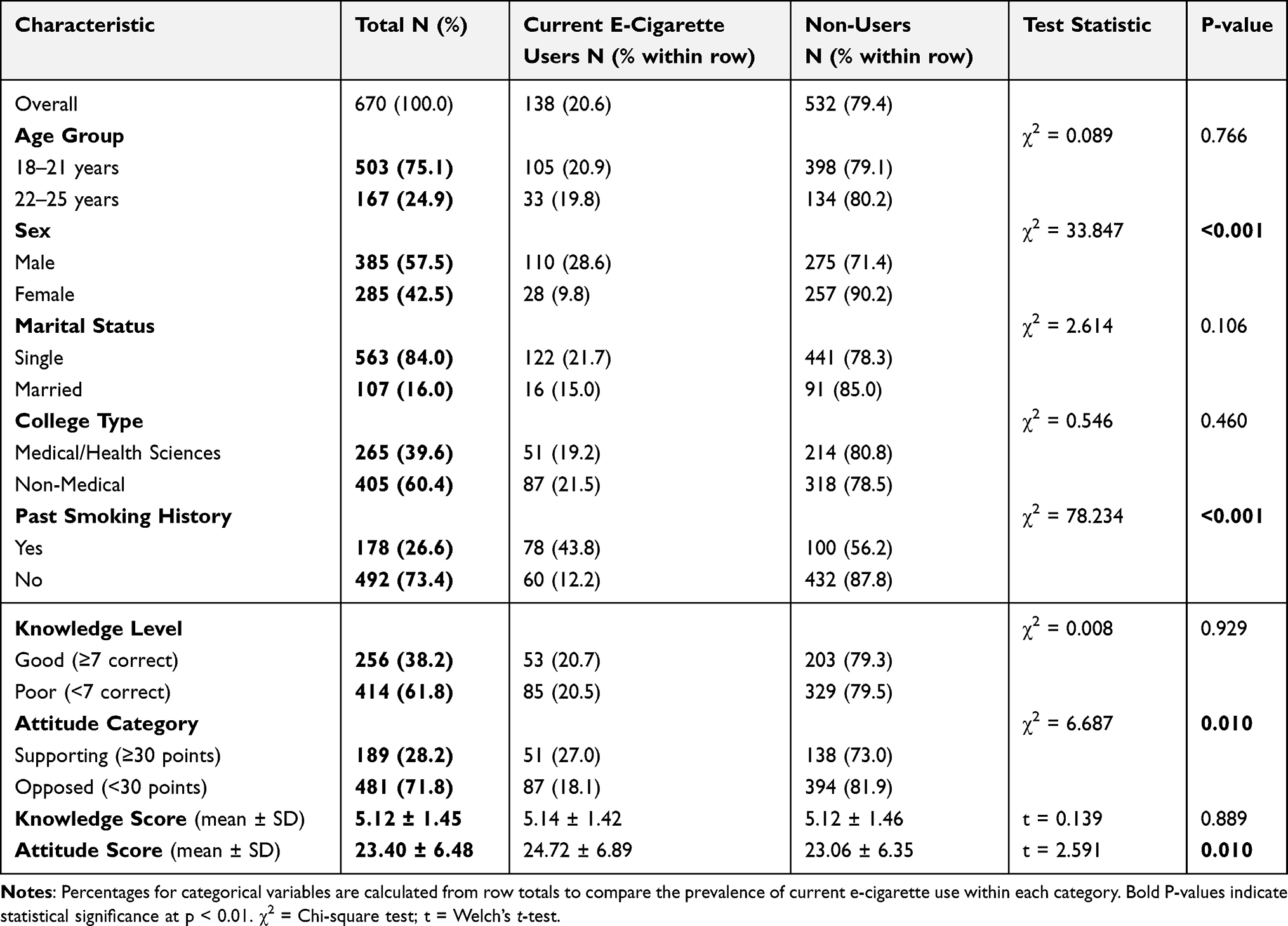 |
Table 1 Sociodemographic Characteristics and Study Variables by Current E-Cigarette Use Status (N=670) |
Multivariable Predictors of Current E-Cigarette Use
Table 2 presents the results of the binary logistic regression analysis identifying independent predictors of current e-cigarette use. After adjusting for all covariates simultaneously, three variables demonstrated statistically significant associations with current e-cigarette use.
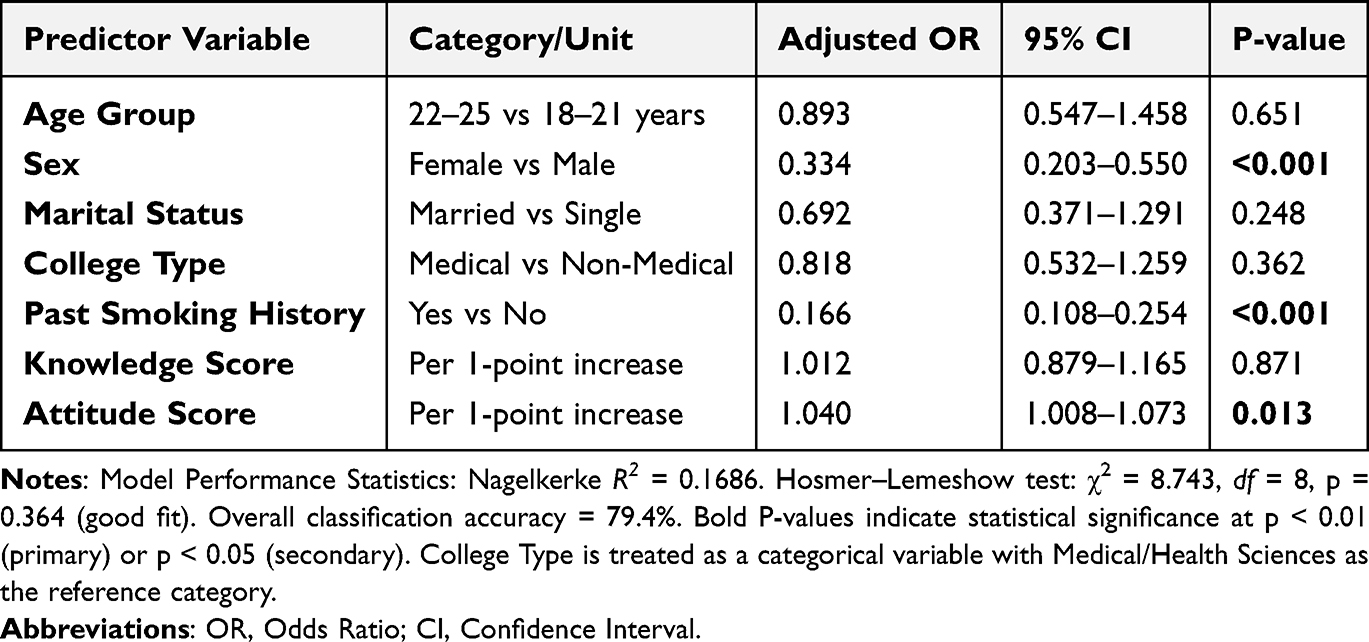 |
Table 2 Multivariable Logistic Regression Predicting Current E-Cigarette Use (N=670) |
Female sex was associated with 67% lower odds of current e-cigarette use compared with male sex (adjusted OR = 0.334, 95% CI: 0.203–0.550, P < 0.001). The variable “past smoking history” showed a counterintuitive association, with participants reporting any historical cigarette smoking experience demonstrating 83% lower odds of current e-cigarette use (adjusted OR = 0.166, 95% CI: 0.108–0.254, P < 0.001). As noted in the Methods section, this unexpected finding likely reflects the problematic variable construction wherein former smokers, current smokers, and those preferring not to answer were grouped with never smokers (coded as 0 = “No past smoking history”). This coding scheme obscures important distinctions between smoking subgroups and may produce paradoxical results.
Each one-point increase in attitude score was associated with a 4% increase in odds of current e-cigarette use (adjusted OR = 1.040, 95% CI: 1.008–1.073, P = 0.013). Age, marital status, college type, and knowledge score were not significantly associated with the outcome in the multivariable model.
Model Discrimination and Validation
Tables 3 and 4, along with Figures 1 and 2, present comprehensive model performance evaluation metrics. These analyses serve two critical purposes beyond the primary study objectives: (1) They assess the clinical utility and generalizability of the prediction model for potential application in campus-based screening programs to identify high-risk students who might benefit from targeted prevention interventions; (2) They evaluate potential overfitting and validate the robustness of our multivariable findings through internal validation techniques (cross-validation, calibration analysis), thereby strengthening confidence in the reported associations between predictors and e-cigarette use. While not primary study objectives, these validation analyses are essential for responsible reporting of prediction models in epidemiological research and provide transparency regarding the model’s strengths and limitations.
 |
Table 3 Discrimination Performance of the Prediction Model for Current E-Cigarette Use |
 |
Table 4 Calibration Performance of the Prediction Model Across Risk Deciles |
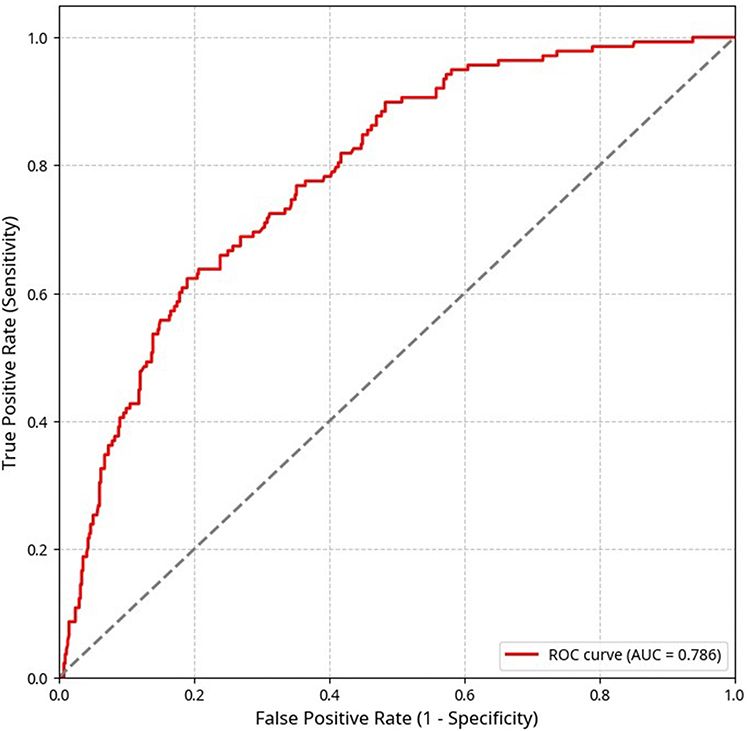 |
Figure 1 Receiver Operating Characteristic (ROC) curve showing the discrimination performance of the multivariable logistic regression model for predicting current e-cigarette use. The diagonal line represents no discrimination (AUC = 0.50). The model achieved an apparent AUC of 0.7857 and a cross-validated AUC of 0.7630, indicating acceptable-to-good discriminative ability in distinguishing current e-cigarette users from non-users. |
 |
Figure 2 Calibration plot displaying the agreement between observed and expected probabilities of current e-cigarette use across deciles of predicted risk. The diagonal line represents perfect calibration, and points close to this line indicate good agreement. Most observed-to-expected ratios fall within the acceptable range (0.5–1.5), with particularly close alignment in the higher-risk deciles. Some deviation in lower-risk deciles is expected due to smaller event counts. Overall, the plot demonstrates strong calibration across the risk spectrum, supporting the model’s reliability for probability estimation in this population. |
Model Calibration Performance
The prediction model demonstrated excellent calibration performance across multiple metrics. The Brier score of 0.1359 was substantially better than the non-informative baseline (0.1635), indicating good overall probabilistic accuracy. The calibration intercept of approximately zero (2.13 × 10−10) confirms the absence of systematic over- or under-estimation bias. The calibration slope of exactly 1.0000 indicates optimal spread of predicted probabilities without evidence of overfitting-induced overconfidence (Table 4).
Table 5 explains decile-based analysis revealed generally good agreement between observed and expected event rates across the risk spectrum. Most observed/expected ratios fell within the acceptable range (0.5–1.5), with the closest agreement observed in the highest risk deciles (9th and 10th deciles: 1.015 and 0.920, respectively). Some deviation was noted in the lower risk deciles, which is common and acceptable given the smaller absolute number of events in these strata. Overall, these calibration metrics support the model’s reliability for providing well-calibrated probability estimates of current e-cigarette use in this university student population.
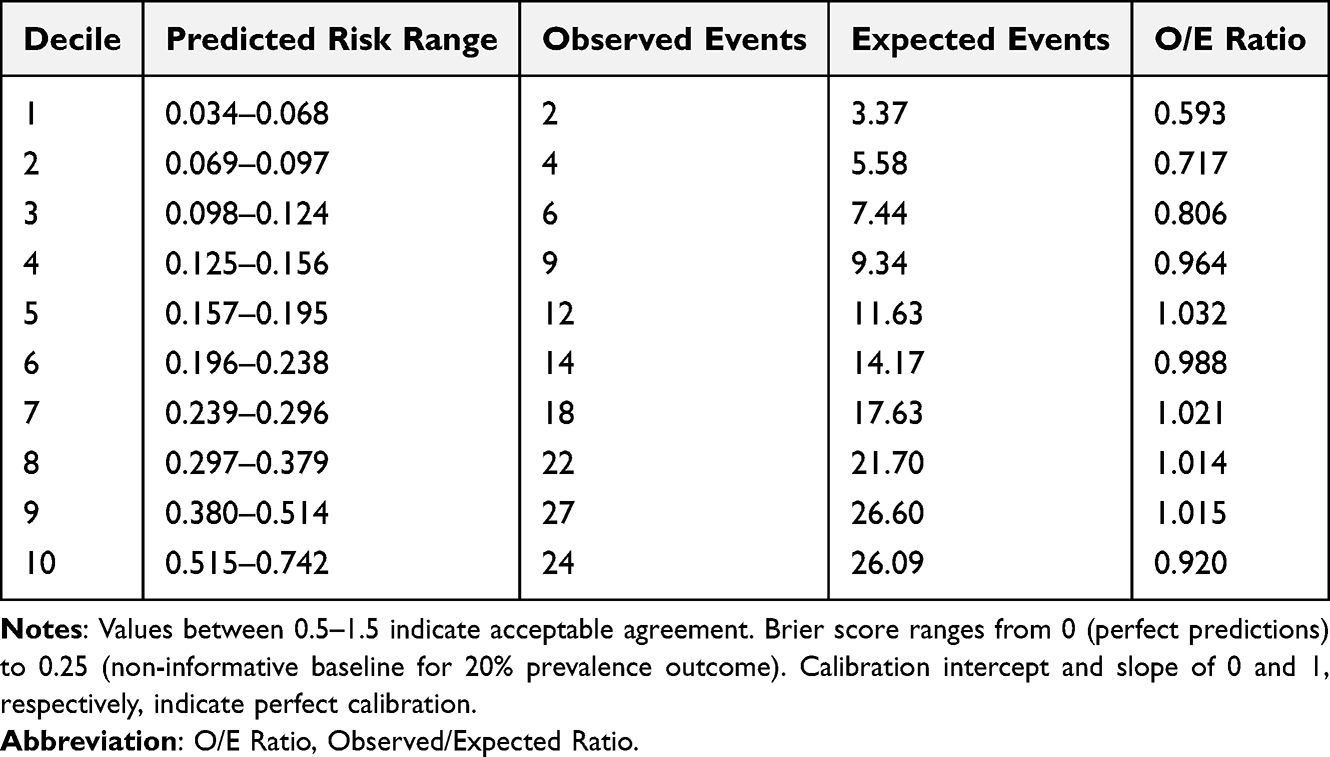 |
Table 5 Observed Vs Expected Events by Risk Decile |
E-Cigarette Knowledge Distribution
Detailed analysis of individual knowledge items revealed substantial heterogeneity in student awareness of specific e-cigarette health effects and constituents. While 77.6% (520/670) correctly recognized e-cigarettes’ addiction potential, only 45.0% (301/670) identified respiratory risks, and merely 35.0% (234/670) correctly acknowledged nicotine as a primary constituent. A particularly concerning misconception was that 55.0% (368/670) of participants incorrectly believed e-cigarette aerosol consists of “harmless water vapor”, reflecting substantial knowledge gaps despite moderate overall knowledge scores.
Stratified by academic discipline, medical/health sciences students demonstrated significantly higher overall knowledge compared to non-medical peers (mean knowledge score: 6.18 ± 1.28 vs 4.45 ± 1.31, P < 0.001). Specifically, 53.2% (141/265) of medical students achieved “good knowledge” (≥7 correct) compared to only 28.4% (115/405) of non-medical students (χ2 = 42.685, P < 0.001). However, this superior knowledge did not translate proportionally into more protective attitudes, as evidenced by the subsequent attitude analysis.
Attitude Patterns and the Knowledge-Attitude Gap
The mean attitude score was 23.40 ± 6.48 (range 10–48), with higher scores indicating more favorable (permissive) attitudes toward e-cigarettes. Overall, 28.2% (189/670) of participants demonstrated “supporting attitudes” (≥30 points), while 71.8% (481/670) held “opposed attitudes” (<30 points).
A striking knowledge-attitude-behavior paradox emerged when examining patterns across academic disciplines. Despite medical students’ significantly superior knowledge (53.2% with good knowledge vs 28.4% among non-medical students, P < 0.001), their attitudes were only moderately more protective: 61.5% (163/265) of medical students held opposed attitudes compared to 78.5% (318/405) of non-medical students (χ2 = 23.147, P < 0.001). This represents only a 17-percentage point difference in attitudes despite a 25-percentage point difference in knowledge levels, illustrating the knowledge-attitude disconnect.
Furthermore, 20.1% (135/670) of all participants endorsed the perception that “e-cigarettes are effective tools for smoking cessation”, including 16.2% (43/265) of medical students who should theoretically recognize the insufficient evidence for this claim. These findings demonstrate the gap between factual knowledge and attitudinal positioning.
Gender-Specific Patterns
Pronounced gender disparities were evident across all study outcomes. Current e-cigarette use was significantly higher among males (28.6%, 110/385) compared to females (9.8%, 28/285) (P < 0.001). Males also reported higher rates of past smoking history (38.4%, 148/385 vs 10.5%, 30/285 among females, P < 0.001).
Interestingly, no significant gender differences emerged in knowledge scores (males: 5.21 ± 1.48 vs females: 5.01 ± 1.40, P = 0.079) or attitude scores (males: 23.68 ± 6.72 vs females: 23.03 ± 6.14, P = 0.203), suggesting that gender disparities in use behavior reflect factors beyond differential awareness or risk perceptions.
Discussion
This study examined e-cigarette use prevalence, knowledge, attitudes, and predictors among 670 students at Northern Border University, Saudi Arabia. The observed prevalence of 20.6% current use, pronounced gender disparities (28.6% males vs 9.8% females), and the striking knowledge-attitude-behavior paradox documented among medical students provide important insights into the complex mechanisms driving e-cigarette adoption in Saudi university settings.
Prevalence in Regional Context
The 20.6% current use prevalence observed at Northern Border University aligns with emerging patterns across Saudi regions but reveals important geographic variations. Alqahtani et al8 reported electronic cigarette use among students at King Khalid University in Abha, Aseer region, while Alahmadi and Al-Zalabani9 documented patterns of e-cigarette initiation and transition among university students in Al-Madinah City. These regional studies collectively suggest that e-cigarette use has become widespread across Saudi universities, though prevalence rates and user profiles vary by geographic location, institutional characteristics, and local enforcement of tobacco control policies.
Importantly, Alsaedi and Al-Zalabani10 demonstrated significant associations between electronic cigarette use and respiratory symptoms among Saudi university students, highlighting the urgent public health implications of the prevalence rates documented in our study and similar investigations. The consistency of findings across multiple Saudi regions, from the northern border region (current study) to southern regions (Abha, Jazan) and western regions (Al-Madinah), indicates that e-cigarette adoption represents a nationwide phenomenon rather than a localized trend, necessitating coordinated national prevention strategies rather than institution-specific interventions.
The Knowledge-Attitude-Behavior Paradox
The most theoretically significant finding is the knowledge-attitude-behavior paradox observed among medical students. Despite 53.2% of medical students achieving good knowledge compared to only 28.4% of non-medical peers, their attitudes were only moderately more protective (61.5% vs 78.5% opposed). This disproportionately small attitudinal difference relative to the substantial knowledge gap challenges information-deficit models underlying many health education programs.
Aqeeli et al11 similarly documented this paradox among Saudi university students, demonstrating that even individuals with high awareness of e-cigarette addictiveness frequently maintained favorable attitudes toward use. Recent evidence among medical students further corroborates this disconnect, as Hall et al12 demonstrated that nearly all medical students recognized vaping-related health risks, yet a substantial proportion reported engaging in vaping behaviors, highlighting the limited capacity of knowledge alone to drive behavioral protection.
These findings align with the Risk Perception Attitude Framework, which posits that factual knowledge proves insufficient to modify behaviors when risk perceptions are distorted by industry messaging emphasizing relative harm reduction.17 The discovery that 16.2% of medical students endorsed e-cigarettes as effective smoking cessation tools, despite pharmacological training indicating insufficient evidence for this claim, exemplifies how persuasive industry narratives can override evidence-based knowledge. Medical students’ sophisticated understanding of dose–response relationships may paradoxically enable rationalization of occasional use as minimally harmful, a phenomenon termed “calculated risk-taking” wherein advanced knowledge facilitates motivated reasoning rather than behavioral protection.30
This paradox has critical implications for intervention design: educational campaigns targeting knowledge deficits alone will prove insufficient. Effective programs must incorporate critical media literacy training to deconstruct industry marketing tactics, address normative beliefs within peer networks, and develop emotional regulation skills that reduce reliance on nicotine for stress management, particularly important given the high-pressure clinical training environment medical students navigate.31
Gender Disparities and Sociocultural Context
The profound gender disparity observed, with females demonstrating 67% lower odds of e-cigarette use, demands interpretation within Saudi Arabia’s unique sociocultural context. Critically, the absence of gender differences in knowledge or attitudes (P = 0.079 and P = 0.203, respectively) indicates that behavioral disparities stem not from differential risk awareness but from gendered opportunity structures and disclosure norms.
In conservative contexts where female tobacco use faces heightened stigmatization due to cultural expectations regarding femininity, family honor, and religious proscriptions, self-report surveys may substantially underestimate true female prevalence due to social desirability bias.32 The 9.8% female prevalence may therefore represent the lower bound of actual use. Additionally, gendered marketing strategies disproportionately target male consumers through imagery emphasizing modernity and social sophistication, while simultaneously reinforcing traditional norms discouraging female participation.33,34
These patterns underscore the necessity for gender-responsive interventions. For male students, peer-led resistance training and cultivation of alternative social frameworks not centered on vaping may prove effective. For female students, providing judgment-free support systems that acknowledge distinct social pressures and disclosure barriers represents a more appropriate approach than universal prevention messages that fail to recognize gendered constraints on behavior and reporting.
The Past Smoking History Paradox: Methodological Limitations
The counterintuitive finding that past smoking history was associated with 83% lower odds of current e-cigarette use (adjusted OR = 0.166, 95% CI: 0.108–0.254) contradicts established global evidence demonstrating positive associations between conventional smoking and e-cigarette use.35 This paradoxical result almost certainly reflects the problematic variable construction detailed in the Methods section, wherein former smokers, current smokers, and those preferring not to answer were grouped together with never smokers.
This coding scheme obscures critical distinctions between: (1) never smokers who initiate with e-cigarettes; (2) former smokers who transition to e-cigarettes; (3) current dual users; and (4) former smokers who successfully quit all nicotine products. Global research consistently documents that tobacco experimentation predisposes individuals to alternative nicotine delivery systems through both gateway mechanisms and common liability pathways involving sensation-seeking and nicotine dependence.35,36 The current findings’ contradiction of this well-established pattern underscores the variable’s measurement inadequacy rather than representing a genuine protective effect.
Future investigations must employ granular smoking history categorization, distinguishing never smokers, former smokers, current exclusive smokers, current dual users, and former users of both products. Such refined measurement would enable testing of specific hypotheses: Do e-cigarettes function primarily as initiation products for nicotine-naïve youth? As transition products for smokers attempting cessation? As long-term dual-use products? Each pathway has distinct policy implications.
Specific Knowledge Deficits and Industry Messaging
The finding that 55% of participants believed e-cigarette aerosol consists of “harmless water vapor” reflects successful industry messaging that strategically minimizes absolute health risks while emphasizing relative harm reduction compared to combustible cigarettes.3,31 This dual framing creates paradoxical risk perceptions wherein individuals acknowledge general concerns about e-cigarette safety yet dismiss specific hazards to justify personal use, a defensive processing mechanism that preserves behavioral autonomy while reducing cognitive dissonance.30
The 20.1% endorsement rate for e-cigarettes as smoking cessation tools, including among medical students, demonstrates how ambiguous regulatory messaging following Saudi Arabia’s 2019 import liberalization has created consumer confusion.22,37 When e-cigarettes are simultaneously marketed as harm-reduction tools for adult smokers and as recreational lifestyle products attractive to youth, young adults receive contradictory signals about intended use, safety, and appropriateness, a policy ambiguity that facilitates adoption among populations for whom these products were ostensibly not designed.38
Correcting these specific misconceptions requires targeted regulatory interventions: mandatory graphic health warnings, comprehensive ingredient disclosure including nicotine content in quantitative terms, and restrictions on flavored products known to appeal disproportionately to youth.39 These measures must be reinforced by enforcement of point-of-sale and online sales restrictions to reduce youth access.
Peer Influence and Campus Vape Culture
While not formally modeled in multivariable analysis, descriptive patterns and regional literature consistently identify peer influence as among the strongest proximal determinants of initiation. Al-Naimi et al40 documented substantial peer influence on smoking behaviors among students, while regional investigations identified peer smoking as the primary predictor of adolescent tobacco experimentation. These associations reflect Social Cognitive Theory’s emphasis on observational learning, imitation, and vicarious reinforcement within reference groups.15
University environments present particularly high-risk contexts due to residential proximity, shared recreational spaces, and developmental transitions involving identity exploration and peer acceptance. The emergence of “vape culture” on campuses, characterized by flavored products, discrete devices, and social media promotion, has transformed e-cigarettes from cessation tools into lifestyle accessories signaling modernity and in-group membership.41–43 Effective interventions must therefore address social normalization through comprehensive campus tobacco-free policies, peer-led resistance training, and counter-marketing campaigns on dominant social media platforms that deconstruct industry-sponsored content.44,45
Model Performance and Clinical Utility
The prediction model demonstrated acceptable discrimination (cross-validated AUC = 0.7630) and excellent calibration (Brier score = 0.1359), indicating reliable probability estimates for identifying current e-cigarette users. The low optimism value (0.0226) suggests minimal overfitting, supporting potential generalizability to similar Gulf Cooperation Council university populations. However, the modest pseudo-R2 (0.1686) indicates that measured covariates explain only approximately 17% of the variance in e-cigarette use.
This limited explanatory power underscores e-cigarette use as a multifactorial behavior involving unmeasured constructs, including personality traits (sensation-seeking, impulsivity), mental health status (anxiety, depression, stress coping), environmental exposures (parental smoking, marketing exposure, residential peer networks), and policy enforcement variations.46,47 From a clinical translation perspective, the model’s discrimination performance suggests utility for population-level risk stratification, for example, identifying high-risk demographic segments for targeted screening in campus health settings, but insufficient precision for individual-level prediction requiring higher AUC thresholds (≥0.80).48
Future model iterations incorporating behavioral variables (dual-use patterns, quit attempt history), psychological measures (risk perception scales, self-efficacy assessments), and environmental indicators (campus policy stringency, peer network density) may enhance both predictive accuracy and mechanistic understanding of adoption pathways.47
Study Limitations
Several methodological limitations warrant acknowledgment. First, the convenience snowball sampling approach, while pragmatic for reaching university students via digital platforms, precludes true random selection and may introduce selection bias favoring students with stronger opinions about e-cigarettes or greater social media engagement. Although retrospective stratification weights were applied to enhance representativeness, findings should be interpreted as specific to Northern Border University rather than generalizable to all Saudi university students.
Second, the cross-sectional design prevents causal inference regarding temporal relationships between knowledge, attitudes, and behaviors. We cannot determine whether favorable attitudes preceded e-cigarette initiation or emerged subsequently as post-hoc justifications (cognitive consonance). Longitudinal investigations tracking students from matriculation through graduation would clarify developmental trajectories and identify critical windows for intervention delivery.
Third, self-report measures are vulnerable to social desirability bias, particularly concerning stigmatized behaviors in conservative cultural contexts. Female students may systematically underreport e-cigarette use due to concerns about social sanctions and reputational consequences, potentially explaining pronounced gender disparities. Future research employing biological validation (cotinine testing) or anonymous reporting mechanisms may yield more accurate prevalence estimates among female populations.
Fourth, as extensively discussed, the problematic construction of the “past smoking history” variable obscures important distinctions between smoking subgroups, producing counterintuitive findings that contradict established literature. Future investigations must employ more granular smoking history categorization to elucidate gateway effects, dual-use patterns, and harm-reduction pathways.
Fifth, unmeasured confounders including personality traits, mental health status, family environment, marketing exposure, and peer network characteristics likely explain substantial residual variance in e-cigarette use not captured by the current model (pseudo-R2 = 0.1686). Comprehensive investigations incorporating these domains would provide more complete mechanistic understanding.
Implications for Policy and Practice
Findings suggest multilevel, theory-driven interventions addressing cognitive, affective, and normative determinants simultaneously. At the individual level, educational programs must move beyond information dissemination to incorporate critical media literacy training that deconstructs industry marketing tactics, addresses harm-reduction claim ambiguities, and develops analytical skills for evaluating product claims. For medical students specifically, case-based curricula examining e-cigarette pharmacology, clinical evidence gaps, and patient counseling strategies would leverage their advanced scientific knowledge while addressing the knowledge-attitude gap.
At the interpersonal level, peer-led interventions harnessing social influence for behavioral protection show promise. Training student leaders to model abstinence, challenge pro-vaping norms, and provide resistance skills within naturally occurring social networks may prove more effective than adult-delivered programs that students perceive as disconnected from peer culture.
At the environmental level, comprehensive campus tobacco-free policies extending to all areas without exception provide critical structural interventions that denormalize use, reduce environmental exposure, and send clear institutional messages about health priorities. These must be supported by accessible cessation resources specifically designed for young adults, including counseling services, pharmacotherapy when appropriate, and digital interventions leveraging platforms students already use.
At the regulatory level, Saudi Arabia’s evolving tobacco control landscape requires strengthening. Mandatory graphic health warnings, comprehensive ingredient disclosure, flavor restrictions, enhanced point-of-sale enforcement, and age verification for online sales represent evidence-based strategies proven effective in other jurisdictions.7 Social media counter-marketing campaigns deploying peer-generated content can challenge industry narratives on platforms where youth receive product information.
Critically, interventions must be gender-responsive, recognizing that male and female students face distinct social pressures, opportunity structures, and disclosure barriers. Universal prevention messages ignoring these gendered realities will fail to engage their intended audiences effectively.
Future Research Directions
Longitudinal cohort studies following students from matriculation through graduation would clarify the following: (1) developmental trajectories of initiation, escalation, and cessation; (2) temporal relationships between knowledge acquisition, attitude formation, and behavioral onset; (3) critical transition points when students are most vulnerable to initiation; and (4) natural history of dual use and product switching patterns. Such designs would enable causal inference currently precluded by cross-sectional data.
Mixed-methods investigations incorporating qualitative components (focus groups, in-depth interviews) would provide rich contextual understanding of decision-making processes, perceived benefits and risks, social norms within specific peer groups, and barriers to cessation that quantitative surveys cannot capture. Understanding why medical students with superior knowledge maintain favorable attitudes requires exploring their subjective rationales, perceived differences between personal and population-level risks, and cognitive strategies for managing knowledge-behavior discordance.
Intervention trials testing theory-driven, multilevel programs are urgently needed. Randomized controlled trials comparing standard educational approaches against enhanced programs incorporating critical media literacy, peer-led resistance training, and emotional regulation skills would provide evidence regarding effective intervention components. Given the knowledge-attitude gap documented among medical students, trials specifically targeting health sciences students represent a priority.
Finally, biological validation studies employing cotinine testing alongside self-report would clarify the extent of underreporting, particularly among female students in conservative contexts, providing more accurate prevalence estimates essential for resource allocation and policy planning.
Conclusion
This investigation of 670 students at Northern Border University revealed a 20.6% current e-cigarette use prevalence, with patterns consistent with regional studies across Saudi Arabia, indicating widespread adoption. The striking knowledge-attitude-behavior paradox observed among medical students, wherein superior knowledge translated into only moderately more protective attitudes, challenges information-deficit models and demonstrates that factual knowledge alone proves insufficient to shape behavior in the face of powerful social influences, industry messaging, and normative beliefs.
Pronounced gender disparities (28.6% male vs 9.8% female use) reflected sociocultural constraints rather than differential knowledge or attitudes, underscoring the necessity for gender-responsive interventions acknowledging distinct social pressures faced by male and female students. The 4% increase in e-cigarette use odds per one-point increase in favorable attitudes confirmed attitudes’ mediating role in the knowledge-behavior pathway, as predicted by the Theory of Planned Behavior.
Effective prevention requires moving beyond traditional educational campaigns toward multilevel, theory-driven interventions addressing cognitive knowledge, critical media literacy, peer norms, emotional regulation, and structural policies simultaneously. The consistency of findings across multiple Saudi regions, Northern Border, Aseer, Al-Madinah, and Jazan, indicates that coordinated national strategies rather than institution-specific approaches represent the appropriate policy response to this nationwide public health challenge.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding
This work was supported by the Deanship of Scientific Research at Northern Border University, Arar, Saudi Arabia, “NBU-FFR-2026-3326-03”. The funding body had no role in the study design, data collection and analysis, interpretation of results, manuscript writing, or the decision to submit the manuscript for publication.
Disclosure
The authors declare no conflicts of interest in this work. This research was conducted without any financial relationships with organizations that could potentially bias the outcomes, including tobacco companies, e-cigarette manufacturers, or entities with commercial interests in vaping products.
References
1. Glantz SA, Bareham DW. E-cigarettes: use, effects on smoking, risks, and policy implications. Annu Rev Public Health. 2018;39(1):215–18. doi:10.1146/annurev-publhealth-040617-013757
2. Cullen KA, Ambrose BK, Gentzke AS, Apelberg BJ, Jamal A, King BA. Notes from the field: use of electronic cigarettes and any tobacco product among middle and high school students - United States, 2011-2018. MMWR Morb Mortal Wkly Rep. 2018;67(45):1276–1277. doi:10.15585/mmwr.mm6745a5
3. Pepper JK, Ribisl KM, Brewer NT. Adolescents’ interest in trying flavoured e-cigarettes. Tob Control. 2016;25(Suppl 2):ii62–ii66. doi:10.1136/tobaccocontrol-2016-053174
4. Jackler RK, Ramamurthi D. Nicotine arms race: JUUL and the high-nicotine product market. Tob Control. 2019;28(6):623–628. doi:10.1136/tobaccocontrol-2018-054796
5. Girvalaki C, Filippidis FT, Kyriakos CN, et al. Perceptions, predictors of and motivation for waterpipe and conventional tobacco and electronic cigarette use among university students in six countries across the eastern mediterranean and European Regions. Tob Prev Cessat. 2020;6:59. doi:10.18332/tpc/127642
6. Moradi-Lakeh M, El Bcheraoui C, Tuffaha M, et al. Tobacco consumption in the Kingdom of Saudi Arabia, 2013: findings from a national survey. BMC Public Health. 2015;15(1):611. doi:10.1186/s12889-015-1902-3
7. World Health Organization. WHO report on the global tobacco epidemic 2023: protect people from tobacco smoke. Geneva: World Health Organization; 2023.
8. Alqahtani NG, Taha AM, Aldosari RHS, et al. Prevalence, attitude, misconception, and predictors of electronic cigarette among King Khalid University students, Abha, Aseer region, Saudi Arabia. Medicine. 2025;104(16):e42229. doi:10.1097/MD.0000000000042229
9. Alahmadi SM, Al-Zalabani AH. Patterns and factors associated with e-cigarette initiation and transition among university students in Al-Madinah City, Saudi Arabia: a cross-sectional study. Healthcare. 2025;13(16):1949. doi:10.3390/healthcare13161949
10. Alsaedi MQ, Al-Zalabani AH. The association between electronic cigarette use and respiratory symptoms among university students: a cross-sectional study in Saudi Arabia. Tob Induc Dis. 2025;23(May):203454. doi:10.18332/tid/203454
11. Aqeeli A, Alsabaani AA, Alshaiban H, et al. Assessing the dependence and perceptions of the harm and addictiveness of electronic cigarettes among Saudi university students: a cross-sectional study. Healthcare. 2024;12(13):1289. doi:10.3390/healthcare12131289
12. Hall H, Feest J, Zarate S, Forde MS. Medical students’ knowledge, attitudes, and perceptions toward vaping and e‑cigarette use: an assessment of their education and preparedness. Int Med Educ. 2025;4(2):8. doi:10.3390/ime4020008
13. Almutairi KM. Culture and language differences as a barrier to provision of quality care by the health workforce in Saudi Arabia. Saudi Med J. 2015;36(4):425–431. doi:10.15537/smj.2015.4.10133
14. Saddiq HM, Mohammed AY, Alsaywid B, Zahrani A. Prevalence and determinants of cigarette smoking among undergraduate students at King Faisal University, Al-Ahsa, Eastern Province of Saudi Arabia. J Family Community Med. 2018;25(3):175–180. doi:10.4103/jfcm.JFCM_164_17
15. Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. 2001;52(1):1–26. doi:10.1146/annurev.psych.52.1.1
16. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
17. Rimal RN, Real K. Understanding the influence of perceived norms on behaviors. Commun Theory. 2003;13(2):184–203. doi:10.1111/j.1468-2885.2003.tb00288.x
18. Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;35(2):121–126. doi:10.4103/0253-7176.116232
19. Baltar F, Brunet I. Social research 2.0: virtual snowball sampling method using Facebook. Internet Res. 2012;22(1):57–74. doi:10.1108/10662241211199960
20. Kalton G. Practical methods for sampling rare and mobile populations. Proc Am Stat Assoc. 2001:5–9.
21. Hafiz N, Agha H, Alsamarrai N, Almesmari A. E-cigarettes: prevalence, perceptions and knowledge of their health effects amongst university students in the United Arab Emirates. J Environ Public Health. 2019;2019:4650267. doi:10.1155/2019/4650267
22. Bloom BS, Engelhart MD, Furst EJ, Hill WH, Krathwohl DR. Taxonomy of Educational Objectives: Handbook I—Cognitive Domain. New York, NY: David McKay; 1956.
23. Kaliyaperumal K. Guideline for conducting a knowledge, attitude and practice (KAP) study. AECS Illumination. 2004;4(1):7–9.
24. Peltzer K, Pengpid S. Knowledge, attitudes and practices regarding tuberculosis in Namibia. J Infect Dev Ctries. 2019;13(11):986–993. doi:10.3855/jidc.11564
25. Badran IG. Knowledge, attitude and practice: the three pillars of excellence and wisdom—a place in the medical profession. East Mediterr Health J. 1995;1(1):8–16. doi:10.26719/1995.1.1.8
26. Krosnick JA, Presser S. Question and questionnaire design. In: Wright JD, Marsden PV, editors. Handbook of Survey Research.
27. Johns R. Likert items and scales. Survey Question Bank: Methods Fact Sheet 1. 2010;1(1):11–28.
28. Konstan JA, Rosser BRS, Ross MW, Stanton J, Edwards WM. The story of subject naught: a cautionary but optimistic tale of internet survey research. J Comput Mediat Commun. 2005;10(2):article11. doi:10.1111/j.1083-6101.2005.tb00248.x
29. Mishra P, Pandey CM, Singh U, Gupta A, Sahu C, Keshri A. Descriptive statistics and normality tests for statistical data. Ann Card Anaesth. 2019;22(1):67–72. doi:10.4103/aca.ACA_157_18
30. Weinstein ND. Unrealistic optimism about susceptibility to health problems: conclusions from a community-wide sample. J Behav Med. 1987;10(5):481–500. doi:10.1007/BF00846146
31. Hammond D, Reid JL, Rynard VL, et al. Prevalence of vaping and smoking among adolescents in Canada, England, and the United States: repeat national cross sectional surveys. BMJ. 2019;365:l2219. doi:10.1136/bmj.l2219
32. Maziak W, Nakkash R, Bahelah R, Husseini A, Fanous N, Eissenberg T. Tobacco in the Arab world: old and new epidemics amidst policy paralysis. Health Policy Plan. 2014;29(6):784–794. doi:10.1093/heapol/czt055
33. Amos A, Greaves L, Nichter M, Bloch M. Women and tobacco: a call for including gender in tobacco control research, policy and practice. Tob Control. 2012;21(2):236–243. doi:10.1136/tobaccocontrol-2011-050280
34. Alduraywish AA, Alrasheed MM, Jahan S, et al. Smoking among adolescents in Saudi Arabia: prevalence, attitude, and its association with breakfast skipping - a cross-sectional study. Front Public Health. 2022;10:972876. doi:10.3389/fpubh.2022.972876
35. Leventhal AM, Strong DR, Kirkpatrick MG, et al. Association of electronic cigarette use with initiation of combustible tobacco product smoking in early adolescence. JAMA. 2015;314(7):700–707. doi:10.1001/jama.2015.8950
36. Bold KW, Kong G, Camenga DR, et al. Trajectories of e-cigarette and conventional cigarette use among youth. Pediatrics. 2018;141(1):e20171832. doi:10.1542/peds.2017-1832
37. Ministry of Health, Kingdom of Saudi Arabia. National tobacco control program strategic plan 2022-2030. Riyadh: Ministry of Health; 2022.
38. Kong G, Morean ME, Cavallo DA, Camenga DR, Krishnan-Sarin S. Reasons for electronic cigarette experimentation and discontinuation among adolescents and young adults. Nicotine Tob Res. 2015;17(7):847–854. doi:10.1093/ntr/ntu257
39. Henriksen L. Comprehensive tobacco marketing restrictions: promotion, packaging, price and place. Tob Control. 2012;21(2):147–153. doi:10.1136/tobaccocontrol-2011-050416
40. Al-Naimi JA, Alhomod AS, Binsaeed AA. Prevalence of smoking among secondary school students in Riyadh and its suburbs. Saudi Med J. 2010;31(4):395–399.
41. Rocha-ávila LR, Núñez-Baila MA, González-López JR. E-cigarette use among university students: a structured literature review of health risks and social determinants. Healthcare. 2025;13(17):2150. doi:10.3390/healthcare13172150
42. Biles J, Kornhaber R, Irwin P, et al. Perspectives, motivations, and experiences of adolescents and young adults using nicotine vapes: a qualitative review. Health Promot Int. 2025;40(2):daaf007. doi:10.1093/heapro/daaf007
43. Assari S, Mohammadi M, Pashmchi M, et al. I am my peers: how social ties influence e-cigarette attitudes and use among college students. Open J Psychol. 2025;15:6043. doi:10.31586/ojp.2025.6043
44. Geindreau D, Girault A, Gallopel-Morvan K. Tobacco-free university campus policies: a systematic review. J Am Coll Health. 2024;72(1):1–12. doi:10.1080/07448481.2024.2367999
45. Gnonlonfin E, Geindreau D, Gallopel-Morvan K. What are the effects of smoke-free and tobacco-free university campus policies? A systematic review. J Epidemiol Public Health. 2024;72(2):202.
46. Wills TA, Knight R, Williams RJ, Pagano I, Sargent JD. Risk factors for exclusive e-cigarette use and dual e-cigarette and cigarette use in adolescents. Addict Behav. 2015;45:190–197. doi:10.1016/j.addbeh.2015.01.004
47. Brewer NT, Chapman GB, Gibbons FX, Gerrard M, McCaul KD, Weinstein ND. Meta-analysis of the relationship between risk perception and health behavior: the example of vaccination. Health Psychol. 2007;26(2):136–145. doi:10.1037/0278-6133.26.2.136
48. Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Physicians’ Knowledge and Practices Regarding Asthma: A Cross-Sectional Study in Saudi Arabia
Dairi MS
International Journal of General Medicine 2022, 15:6671-6680
Published Date: 19 August 2022
The Prevalence of Complementary and Alternative Medications Use Among Dermatology Patients in Aseer Region, Saudi Arabia
Al-Atif HM, AL-Ghamdi HS, Alzubaidi WA, Alnaem NM, Qahtani SH
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2607-2615
Published Date: 6 December 2022
Psychiatric Nurses’ Knowledge, Attitudes, and Practice Regarding Physical Restraint in China: A Multicentre Cross-Sectional Study
Chong Y, Wang C, Zhi T, Fang S, Min H, Zhang L, Wu X, Wang Y
Journal of Multidisciplinary Healthcare 2023, 16:1475-1489
Published Date: 29 May 2023
Assessing the Knowledge, Attitudes, and Vaccination Practices Towards COVID-19 Vaccination Among Mainland Chinese Nursing Students and Interns: A Multicenter Cross-Sectional Study

Qin Z, Ye X, Liu H, Tao Y, Zheng X, Zhong Y, Chen D, Ye W, Zhan C
Infection and Drug Resistance 2023, 16:4717-4728
Published Date: 20 July 2023
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024