Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Comparison of Percutaneous Coronary Intervention Outcomes for in-Stent vs de Novo Chronic Total Occlusions: A Meta-Analysis
Received 2 November 2025
Accepted for publication 21 March 2026
Published 15 April 2026 Volume 2026:22 576328
DOI https://doi.org/10.2147/TCRM.S576328
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Qiongya Mao,1 Lili Xie,1 Jun Wu2
1Nursing Department, Ningbo Municipal Hospital of Traditional Chinese Medicine, Affiliated to Zhejiang Chinese Medical University, Ningbo City, Zhejiang Province, 315010, People’s Republic of China; 2Department of Andrology, Ningbo Traditional Chinese Medicine Hospital, Ningbo City, Zhejiang Province, 315010, People’s Republic of China
Correspondence: Jun Wu, Department of Andrology, Ningbo Traditional Chinese Medicine Hospital, No. 819 Liyuan North Road, Haishu District, Ningbo City, Zhejiang Province, 315010, People’s Republic of China, Email [email protected]
Background: Chronic coronary total occlusion (CTO) represents a formidable challenge in interventional cardiology, occurring either within previously implanted stents (in-stent CTO) or in non-stented native vessels (de novo CTO). We aimed to compare the outcomes of percutaneous coronary intervention (PCI) between patients with in-stent and de novo CTO through a systematic review and meta-analysis.
Methods: PubMed, Embase, ScienceDirect, CENTRAL, and Google Scholar databases were searched for comparative studies published up to 20th September 20, 2025. A meta-analysis was conducted to calculate the odds ratios (OR) using a random effects model.
Results: Nineteen studies that compared 73,945 patients with in-stent CTO and 651,961 patients with de novo CTO were included. There was no statistically significant difference in technical success between the two groups (OR, 0.97; 95% CI, 0.87, 1.08; I2=0%; p=0.67). Pooled analysis of early outcomes demonstrated no statistically significant difference in the risk of all-cause mortality, major adverse cardiovascular events (MACE), myocardial infarction (MI), stent thrombosis, or tamponade between the two groups. We also noted no statistically significant differences in long-term all-cause or cardiac mortality between the two groups. However, a meta-analysis of long-term data indicated that patients with in-stent CTO have a statistically significantly increased risk of MACE, MI, and target vessel revascularization (TVR) compared to those with de novo CTO.
Conclusion: Our results indicate that in-stent CTO-PCI has success rates similar to those of de novo CTO-PCI. There was no difference in short-term adverse outcomes between the two groups; however, patients undergoing in-stent CTO PCI had an increased risk of MACE and MI, mainly driven by the significantly increased need for TVR.
Keywords: coronary artery disease, mortality, percutaneous coronary intervention, chronic total occlusion
Introduction
Chronic total occlusion (CTO) is one of the most challenging conditions in patients treated with percutaneous coronary intervention (PCI). Despite the high incidence of CTO, ranging from 18–52% among patients undergoing coronary angiography, these lesions have rarely been revascularized in the past.1 Historically, PCI for CTO has been fraught with high complication and low success rates.2 However, with the continuous advances in CTO equipment and technology, clinical outcomes have greatly improved over the past decade.3 Comprehensive evidence from large-scale meta-analyses has further substantiated that contemporary CTO-PCI can achieve high procedural success rates, and that successful revascularization is associated with significantly improved clinical outcomes and a favorable safety profile.4
In-stent CTO is defined as total occlusion that develops in a previously placed stent. According to estimates, approximately 10–16% of patients undergoing CTO-PCI have in-stent occlusion.5,6 Its pathophysiology involves neoatherosclerosis and stent thrombosis, which differ from the etiology of de novo CTO.7 In-stent CTOs are difficult to treat compared to de novo CTO because of challenges such as the inability to sustain an intrastent track across the stented vessel, difficult reentry with substent wire advancement, and poor runoff with long stented segments.7 While there have been several studies reporting outcomes of CTO-PCI,7 data on the success rates and adverse outcomes associated with in-stent CTO-PCI are scarce.7,8 It is unclear whether there is a difference in clinical outcomes among patients undergoing PCI for in-stent CTO vs de novo CTO. In a recent systematic review and meta-analysis, Mir et al9 compared the success rates and outcomes of in-stent and de novo CTO treated with PCI. However, the authors included just five studies in their review, and many of them had a small sample size. In view of new studies published in the past two years,10,11 there is a need for an updated review to present the best possible evidence to guide clinicians. In this context, the current study was designed to perform a systematic literature review and pool data from individual studies to compare the technical success and adverse outcomes of PCI between in-stent and de novo CTO patients.
Materials and Methods
The methodology of our review was based on the reporting guidelines of the PRISMA statement (Preferred Reporting Items for Systematic Reviews and Meta-Analyses).12 The review protocol was prospectively registered with PROSPERO (CRD420251153568).
Literature Search
A systematic and comprehensive search was performed using the PubMed, Embase, ScienceDirect, and CENTRAL electronic databases. Google Scholar was used to search for grey literature, but only for the first 200 results of each search query. To minimize single-reviewer bias, two authors separately explored the databases. The search limits were set from the time of inception of the databases to 20th September 20, 2025. The search terms included were “in-stent”, “restenosis”, “chronic total occlusion”, and “percutaneous coronary intervention”. Further details of the search strategy, which were common to all databases, are presented in Supplementary Table 1. After the initial search, the results were duplicated and the titles and abstracts of the remaining articles were assessed. We identified studies relevant to the review and extracted their full texts. Two reviewers independently evaluated the studies for final inclusion in the review. Any discrepancies in study selection were resolved by consensus. Finally, manual scoping of the reference lists of the included studies was performed for any missed references.
Eligibility Criteria
The inclusion criteria were framed according to the PICOS, and included population, intervention, comparison, outcomes, and study design. We included 1) studies conducted on patients undergoing PCI for CTO (Population) and 2) studies that compared patients with in-stent CTO (Intervention) and de novo CTO (Comparison). 3) Studies were to report any of the following Outcomes: Technical/Procedural success, procedural complications, MACE, mortality, myocardial infarction (MI), or target vessel revascularization (TVR). 4) The study designs eligible for inclusion were cohort, case-control, cross-sectional, controlled clinical, and randomized controlled trials.
The exclusion criteria were: 1) non-comparative studies; 2) studies not reporting relevant outcomes; and 3) non-English language studies, editorials, review articles 4) Studies reporting duplicate data. If there were two studies had overlapping data, the study with the largest sample size was included.
Data Extraction and Quality Assessment
Two authors independently extracted the following data: author details, publication year, study type, study location, sample size, demographic details, smoking status, comorbidities (diabetes mellitus, hypertension, chronic kidney disease, dyslipidemia, and peripheral artery disease), previous MI or coronary artery bypass grafting (CABG), left ventricular ejection fraction, stable angina, Japanese CTO score, vessel calcification, multivessel disease, CTO length >20 mm, details of stenting, use of drug-eluting stents (DES), trans-radial approach, intravascular ultrasound (IVUS), procedural time, fluoroscopy time, study outcomes, and follow-up.
As most studies reported technical success instead of procedural success, we designated technical success as the primary outcome of this review. Technical success was defined as residual stenosis <30% and TIMI flow grade ≥3 in all studies, except for one in which <50% residual stenosis was considered a successful procedure. Other outcomes of interest were all-cause mortality, cardiac mortality, MACE, MI, and procedural complications, such as tamponade, bleeding, and TVR. Depending on the follow-up, we classified the outcomes as early (occurring in-hospital or within 30 days) and late (occurring after at least one year of follow-up).
The methodological quality of the studies was assessed using the Newcastle-Ottawa scale (NOS).13 This study was conducted by two authors independent. Disagreements were resolved by discussion. Studies were assessed for selection of study population, comparability, and outcomes, with each domain being awarded a maximum of four, two, and three points respectively. The maximum awarded was nine. Studies with nine points were considered to have a low risk of bias, seven with eight points were considered to have a moderate risk of bias, and those with scores of six and below had a high risk of bias.
Statistical Analysis
The meta-analysis was performed using “Review Manager” (RevMan, version 5.3; Nordic Cochrane Centre [Cochrane Collaboration], Copenhagen, Denmark; 2014). All dichotomous data were pooled using an inverse variance model to calculate odds ratios (OR) with 95% confidence intervals (CI). We also extracted multivariable-adjusted hazard ratios (HR) for long-term outcomes, if available, and pooled them using the generic inverse variance function of RevMan. A meta-analysis was performed only if at least three studies reported the same outcome. All meta-analyses were conducted using a random-effects model.
Heterogeneity was assessed using the I2 statistic. I2 values of 25–50% represented low heterogeneity, values of 50–75% medium heterogeneity, and values more than 75% represented substantial heterogeneity. We assessed publication bias for the primary outcome by visual inspection of funnel plots. Sensitivity analysis was performed to assess the contribution of each study to the pooled estimate by removing one study at a time and recalculating the pooled effect estimates for the remaining studies.
Results
The results of the search strategy and the number of records for each stage are shown in Figure 1. Based on the screening criteria, 22 studies were analyzed using their full texts. Three studies reported overlapping data and were hence excluded.14–16 A total of nineteen studies were included in this systematic review and meta-analysis.7,10,11,17–32 All studies were retrospective cohort studies that reviewed data from a single institute or a multicenter registry. Four studies were multinational, whereas the others were from singular countries. Eight studies were from Asia while seven were from Western countries. The sample size of the in-stent CTO group ranged from 47 to 66,718 patients, whereas that of the de novo CTO group ranged from 94 to 586,586 patients. Further details of the demographics, comorbidities, and medical history of the included patients are presented in Table 1. The baseline angiographic and procedural details of the patients in the two groups are presented in Table 2. Ten studies reported only early outcomes while fourteen studies reported long-term outcomes. The follow-up of the studies with long-term data ranged from one to five years. Twelve studies reported outcome data for both successful and unsuccessful cases, except for Yoon et al,20 wherein adverse outcomes were reported only in successful PCI cases. In a study by Abbas et al,17 technical success was reported per CTO rather than per patient. The risk of bias assessment of the included studies is shown in Table 3. All studies were of high quality, except for five. Three studies11,25 were considered to have a moderate risk of bias, whereas two17,22,26 had a high risk of bias.
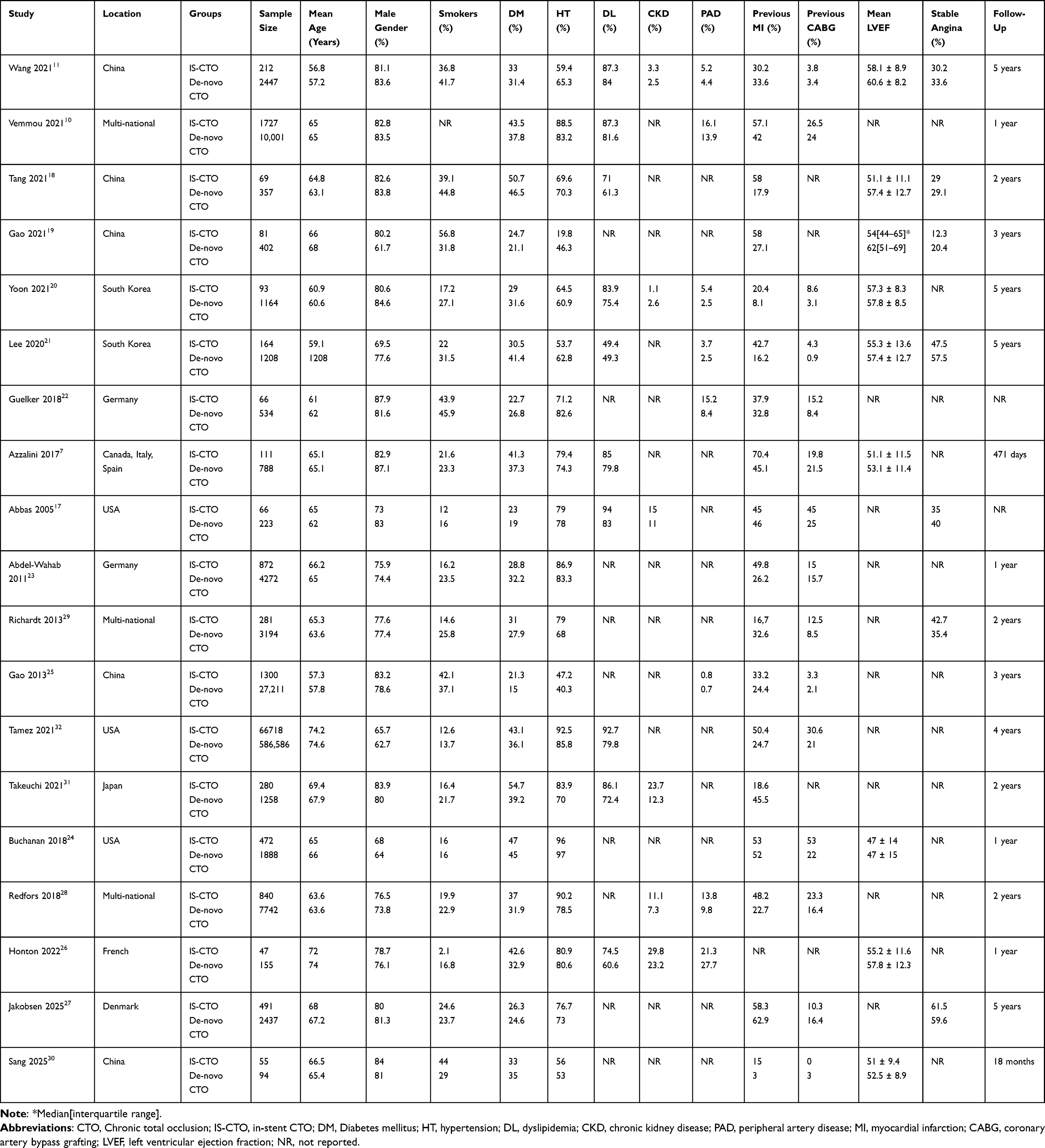 |
Table 1 Baseline Characteristics of Patients in Included Studies |
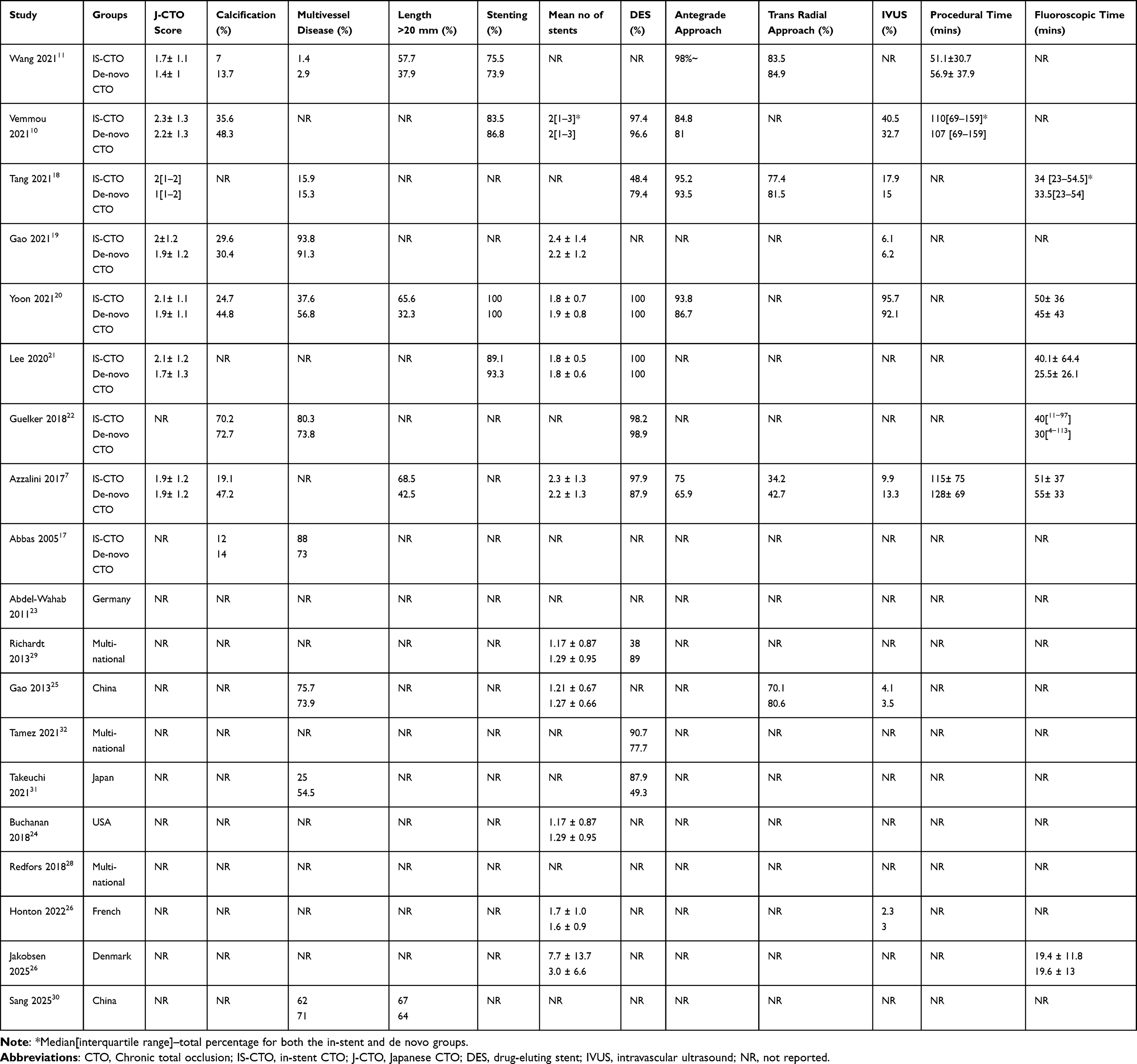 |
Table 2 Angiographic and Procedural Details From Included Studies |
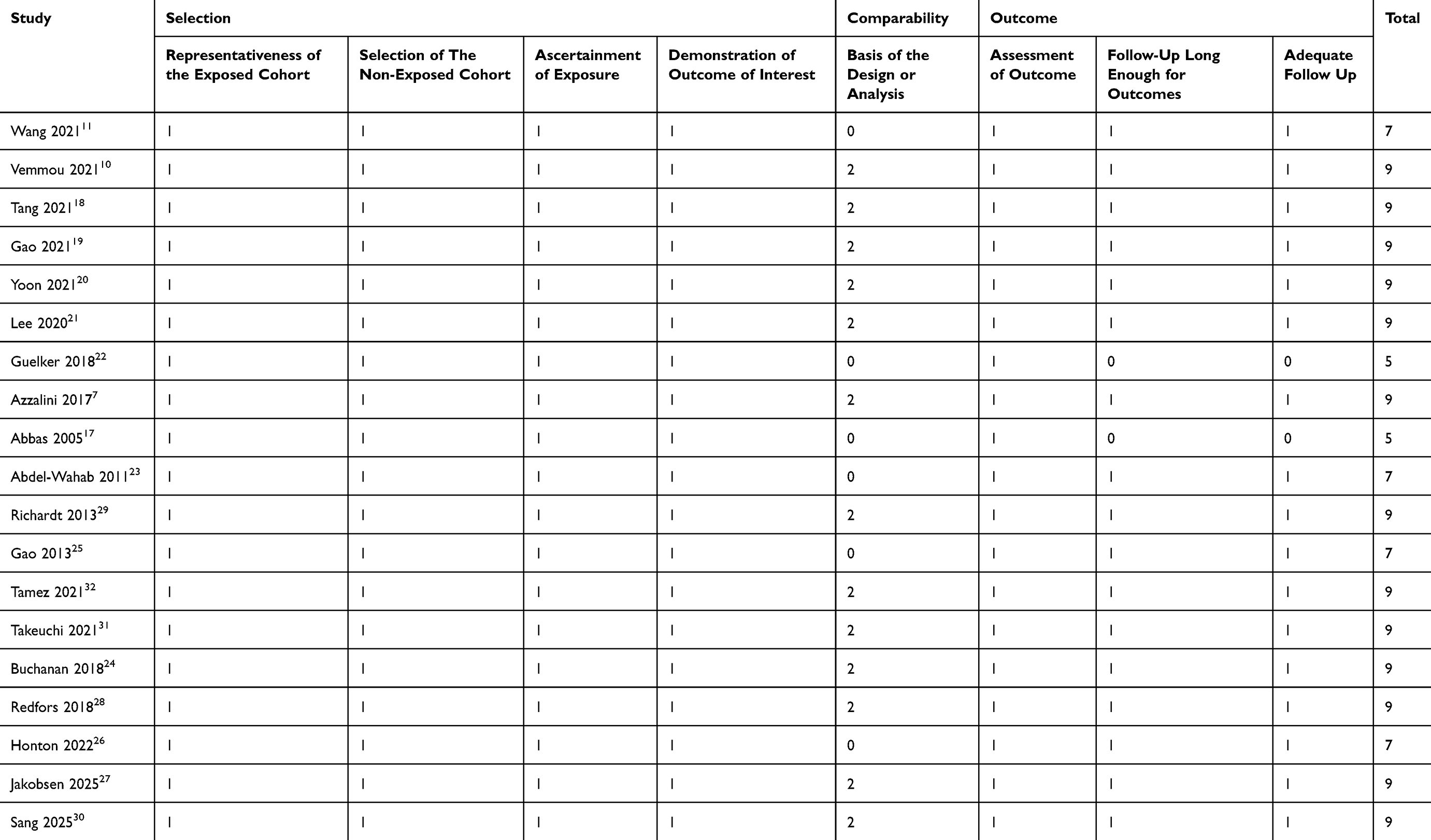 |
Table 3 Risk of Bias Analysis Based on Newcastle-Ottawa Scale |
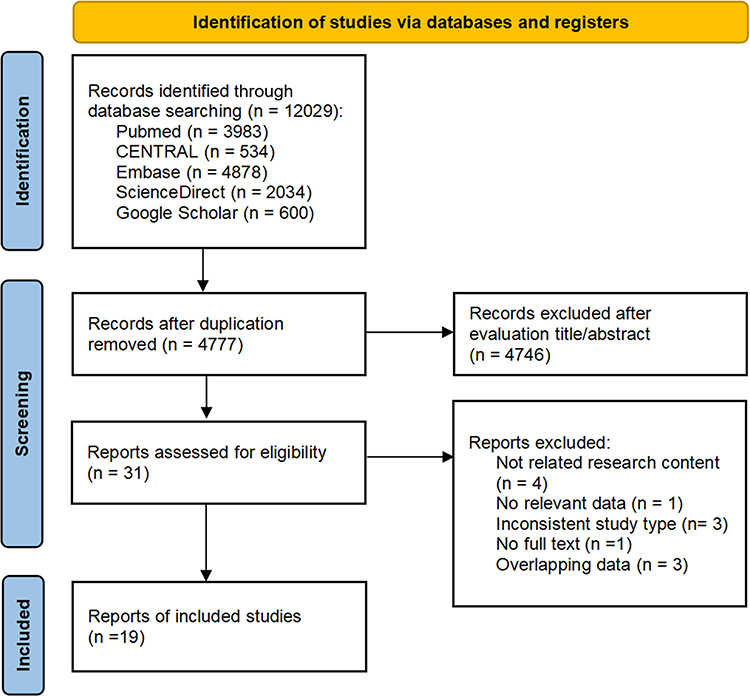 |
Figure 1 Study flow chart. |
Early Outcomes
Technical success was reported in twelve included studies. A meta-analysis comparing 4870 patients with in-stent CTO and 49,001 patients with de novo CTO indicated no statistically significant difference in technical success between the two groups (OR, 0.97; 95% CI, 0.87, 1.08; I2=0%, p=0.67) (Figure 2). There was no evidence of publication bias on visual inspection of the funnel plot (Supplementary Figure 1). Eight studies reported the data on all-cause mortality. Pooled analysis demonstrated no statistically significant difference in the risk of early all-cause mortality between the two groups (OR, 1.06; 95% CI: 0.36, 3.08 I2=52%; p=0.07) (Figure 3). Similarly, we also noted no difference in the risk of early MACE (OR: 0.87, 95% CI: 0.66, 1.15 I2=0%, p=0.45), MI (OR: 1.09, 95% CI: 0.76, 1.57, I2=0%, p=0.52), stent thrombosis (OR: 1.27, 95% CI: 0.34, 4.79, I2=0%, p=0.72), and tamponade (OR, 1.15; 95% CI, 0.41, 3.20; I2=36%, p=0.80) between patients with in-stent CTO and de novo CTO (Figure 3). Sufficient data on the risk of cardiac death and bleeding were not available from meta-analysis studies.
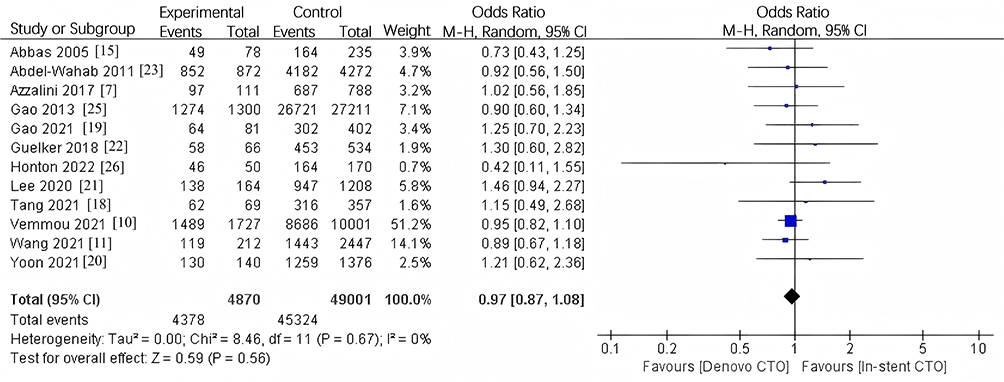 |
Figure 2 Meta-analysis of technical success between in-stent CTO and de novo CTO. Notes: blue squares represent the effect estimate (odds ratio, OR) of each individual study; the square size is proportional to the study weight in the meta-analysis; horizontal lines indicate 95% confidence intervals (CIs). The black diamond represents the pooled effect estimate with its 95% CI. The vertical line at OR = 1 indicates no difference between groups. |
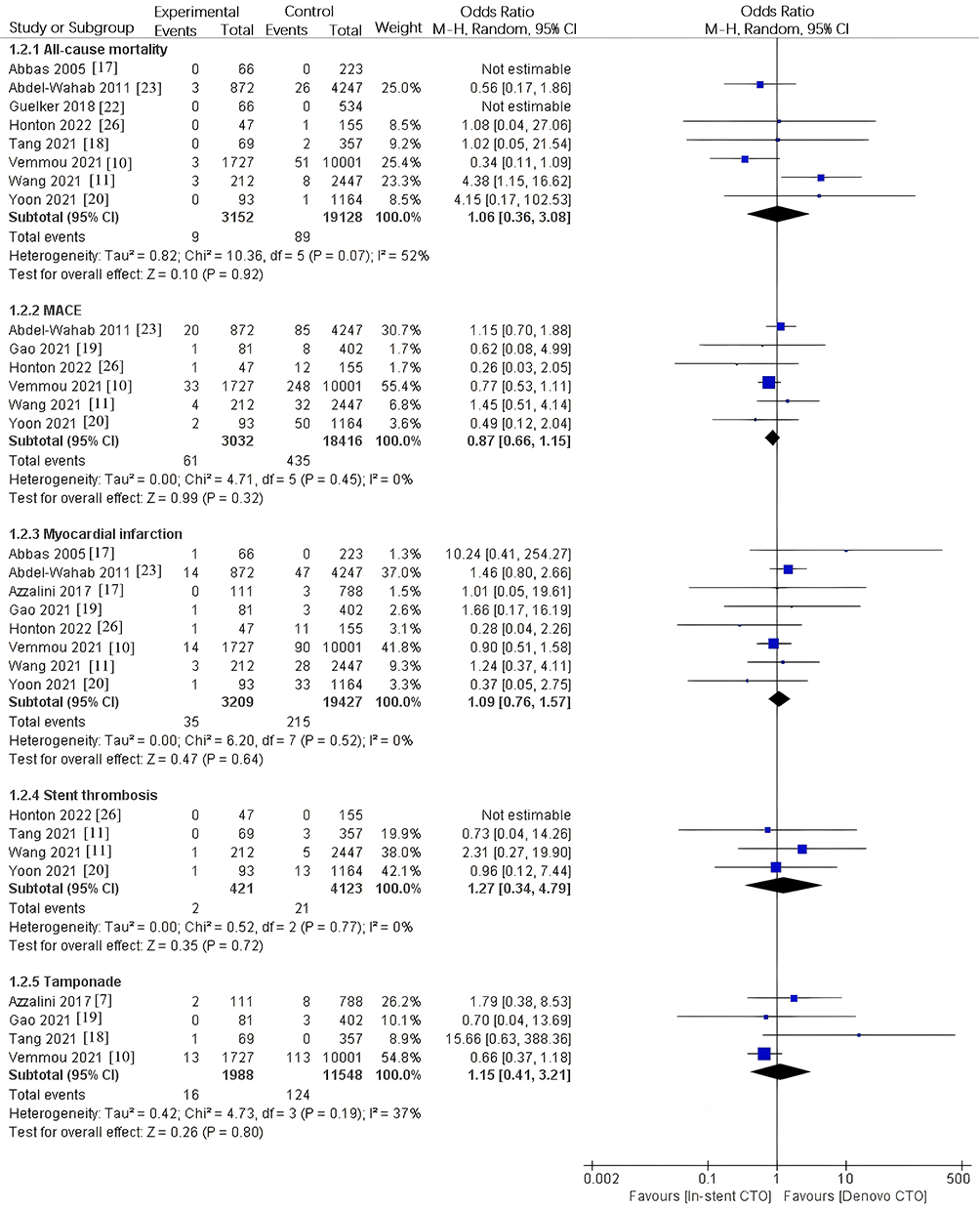 |
Figure 3 Meta-analysis of early all-cause mortality, MACE, myocardial infarction, stent thrombosis and tamponade between in-stent CTO and de novo CTO. Notes: blue squares indicate individual study ORs; square size reflects study weight; horizontal lines indicate 95% CIs. The black diamond indicates the pooled OR with 95% CI. The vertical line at OR = 1 indicates no difference. |
All of the above results were stable on sensitivity analysis, with no change in the significance of the effect size on the exclusion of any study.
Late Outcomes
In the pooled analysis of long-term data with variable follow-up ranging from one to five years, we noted no statistically significant difference in all-cause mortality (OR: 1.06, 95% CI: 0.90, 1.24 I2=0%, p=0.71) or cardiac mortality (OR: 1.07, 95% CI: 0.84, 1.36 I2=0%, p=0.99) between patients with in-stent CTO and de novo CTO (Figure 4). However, meta-analysis of data from five to 13 studies indicated that patients with in-stent CTO had a significantly increased risk of MACE (OR: 1.68, 95% CI: 1.16, 2.42, I2=90%, p<0.00001), MI (OR: 1.59, 95% CI: 1.21, 2.09 I2=48%, p=0.04), and TVR (OR: 1.79, 95% CI: 1.27, 2.52 I2=80%, p<0.0001) (Figure 4). All of the above results were stable on sensitivity analysis, with no change in the significance of the effect size on the exclusion of any study.
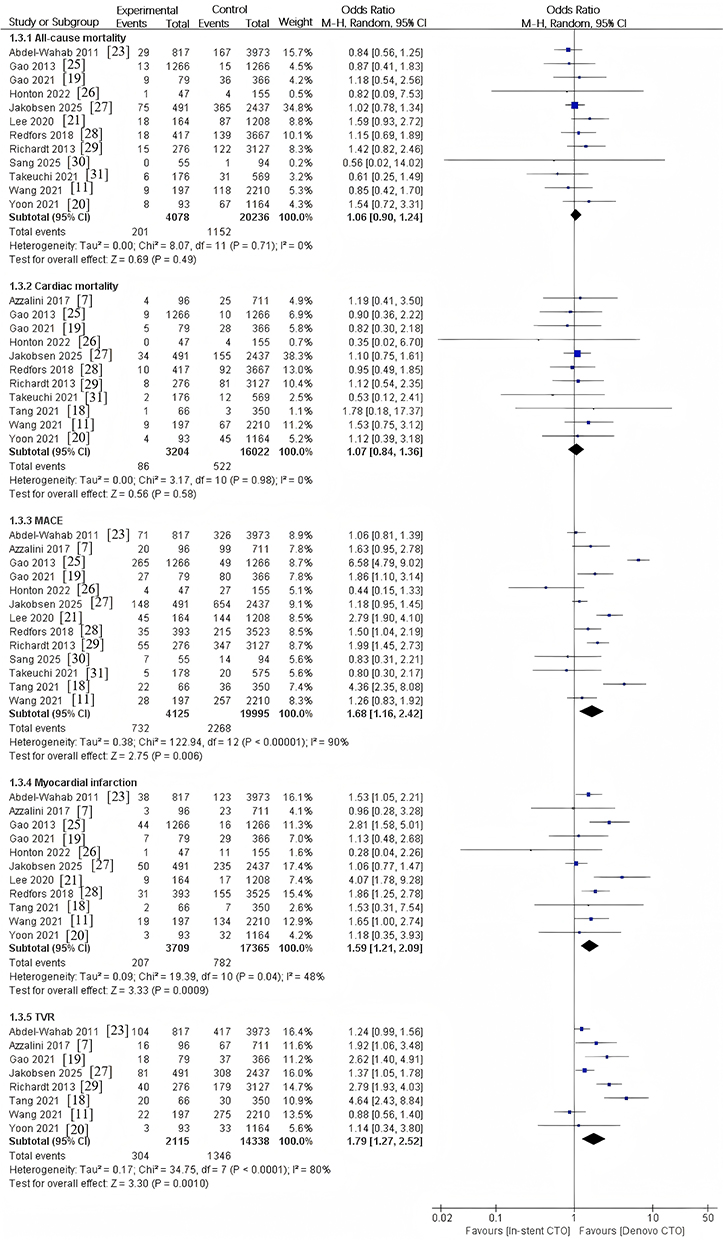 |
Figure 4 Meta-analysis of late all-cause mortality, cardiac mortality, MACE, myocardial infarction, and target vessel revascularization between in-stent CTO and de novo CTO. Notes: blue squares indicate individual study ORs; square size reflects study weight; horizontal lines indicate 95% CIs. The black diamond indicates the pooled OR with 95% CI. The vertical line at OR = 1 indicates no difference. |
Multivariable adjusted data on the long-term risk of MACE were reported in ten studies. In the pooled analysis, we noted a statistically significant increased risk of MACE in patients with in-stent CTO than in those with de novo CTO (HR: 1.54, 95% CI: 1.29, 1.84; I2=79%, p<0.00001) (Figure 5). The results of the sensitivity analysis did not change. Sufficiently adjusted data for other outcomes were not available for quantitative analysis.
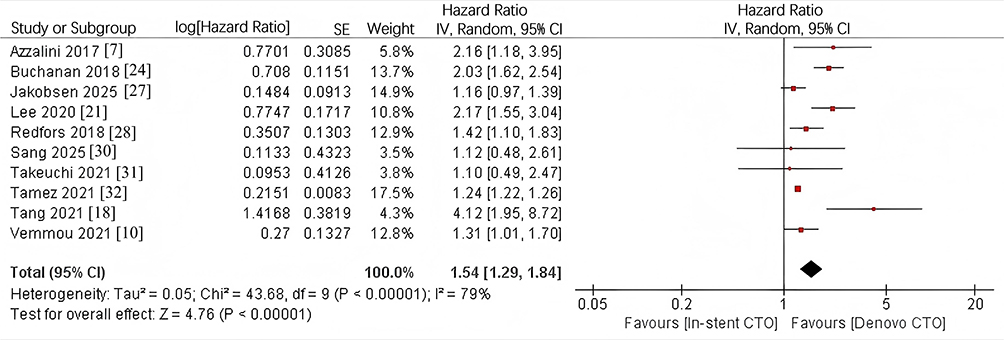 |
Figure 5 Meta-analysis of adjusted data for MACE between in-stent CTO and de novo CTO. Notes: red squares represent the adjusted effect estimate (hazard ratio, HR) from each study (log-transformed values were used for pooling); square size reflects study weight; horizontal lines indicate 95% CIs. The black diamond represents the pooled adjusted HR with 95% CI. The vertical line at HR = 1 indicates no difference. |
Discussion
According to the literature, the success rates of in-stent CTO PCI ranges widely from 56% to 98%.11,25 Several studies reporting lower success rates with in-stent CTO PCI have pointed out the inability to negotiate the wire through the CTO to the distal lumen, unsuccessful advancement of the microcatheter, or inability to completely dilate the balloon as the primary causes of failure.6,17 The struts of the previously placed stent frequently interrupt the wire or microcatheter. Subintimal tracing and wire re-entry into the true lumen is frequently complicated procedure for in-stent CTO lesions. Furthermore, even after successful negotiation, balloon expansion can be hindered by an underlying under-expanded stent. Passage of a new stent could also be complicated if the previous stent is deformed or fractured during balloon passage.6,33 Indeed, one can note that earlier studies, such as those by Abbas et al17 and Abdel-Karim et al,6 noted significantly lower success rates with in-stent CTO PCI. However, with the evolution of techniques, procedural algorithms, and operator experience, success rates have increased in recent times.34,35 In the primary analysis, we found that the technical success rates for in-stent CTO PCI and de novo CTO PCI were not significantly different (89.9% and 92.5%, respectively). The meta-analysis demonstrated an odds ratio of 0.97 with a 95% CI ranging from 0.87 to 1.08 indicating no difference between the two entities. This evidence was further strengthened by the fact that there was no heterogeneity in the analysis, and the results were stable in the sensitivity analysis.
The improved success of in-stent CTO PCI, despite having more complex lesions with higher J-scores in most studies, can be attributed to several reasons. First, there have been vast improvements in the entry techniques for in-stent CTO with antegrade dissection reentry techniques, and crossbow becoming popular in recent times.34,36 In the majority of included studies, the antegrade approach was the first choice to bypass in-stent CTO. Indeed, in several studies, the use of the antegrade approach was significantly higher for in-stent CTO vs de novo CTO.7,20 Second, IVUS is recommended for complex lesions such as in-stent CTOs.35 IVUS allows the operator to assess the characteristics of vessel plaques, measure vessel size, facilitate CTO crossing, and ensure optimal stent deployment.35 In three of the included studies.10,18,20 Lastly, despite the technical difficulties associated with the presence of the previous stent, in-stent CTO PCI can be partly easier, as the stent provides a roadmap of the target vessel.19
In the second part of our analysis, we compared the adverse outcomes between in-stent and de novo CTO-PCI. In a previous meta-analysis, Mir et al9 noted a significantly higher risk of MACE and cardiac death in patients undergoing PCI for in-stent CTOs. Importantly, data from only 464 patients with in-stent CTO were pooled in their meta-analysis. Furthermore, the review did not distinguish between early and long-term outcomes; it did not assess other important results, such as MI and TVR, nor did it pool multi-variable adjusted data. Overcoming these limitations, we noted no difference between in-stent and de novo CTO PCI for all-cause mortality, MACE, MI, stent thrombosis, and tamponade occurring in-hospital or within 30 days of the procedure. This highlights the fact that improvements in techniques and equipment have not only improved success rates but also reduced procedural complications for in-stent CTO PCI. In contrast, patients with in-stent CTOs had a significantly increased risk of MACE and MI in the long-term, which was driven by the higher incidence of TVR. As adverse outcomes after PCI can be influenced by several confounders, we performed a pooled analysis of adjusted data, which confirmed the increased risk of MACE in the in-stent CTO group.
The higher incidence of TVR after in-stent CTO PCI suggests an increased risk of restenosis and subsequent adverse events in these patients. Although the exact pathophysiological mechanism is unknown, mechanical factors such as stent under-expansion or fracture and biological factors such as neointimal hyperplasia neoatherosclerosis, which are also involved in earlier stent occlusion, could play a role.7,21 DES implantation can damage the vessel wall, leading to delayed re-endothelialization, hastened fat infiltration, and neoatherosclerosis formation.37,38 Despite improvements in vessel healing with second-generation DES, these devices still have a similar incidence of neoatherosclerosis.39 Furthermore, longer stents and multilayered stenting significantly increase the risk of restenosis owing to atypical vascular responses and thrombosis.19 Lastly, despite similar technical success rates with de novo CTO PCI, in-stent CTO may be sub-optimally revascularized, and this is an independent predictor of long-term MACE.11
Recent meta-analyses by Elbadawi et al40 and Ngonge et al41 have also explored outcomes for in-stent lesions, yet our study possesses several distinguishing features. While Elbadawi et al40 compared in-stent restenosis (ISR) with de novo lesions across a broad spectrum, they did not focus exclusively on the highly complex chronic total occlusion (CTO) subtype. Furthermore, although Ngonge et al41 specifically addressed IS-CTO, their literature search concluded earlier, missing critical high-quality data from the past two years. Our analysis, updated to September 20, 2025, incorporates the most recent evidence, including studies by Jakobsen et al27 and Sang et al30 By including 19 studies with a massive population exceeding 700,000 patients —largely driven by the inclusion of the Tamez et al32 registry —this study offers superior statistical power to detect differences in rare safety endpoints such as stent thrombosis and tamponade. Most importantly, we strictly stratified outcomes into early (≤30 days) and long-term (1–5 years), and pooled multivariable-adjusted hazard ratios to provide a more robust assessment of MACE risk by mitigating baseline clinical heterogeneity.
The substantial heterogeneity observed in our pooled analysis of late MACE and TVR (I2=90% and I2=80%, respectively) necessitates a cautious interpretation of these findings. This high variability is likely attributable to clinical heterogeneity, specifically the inconsistent follow-up durations ranging from one to five years and differences in baseline comorbidities such as diabetes and lesion complexity reflected by J-CTO scores. Furthermore, methodological differences inherent in retrospective registries—such as varying operator experience, procedural volumes, and post-PCI antiplatelet strategies—may have contributed to the observed variance. Despite this, the robustness of our results is reinforced by sensitivity analyses, which demonstrated that the exclusion of any individual study did not alter the significance of the findings. Crucially, the pooled multivariable-adjusted hazard ratio (HR: 1.54) further corroborates the increased long-term risk for in-stent CTO patients even after adjusting for potential confounders.
These results have several important clinical implications. This suggests that when guided with the appropriate equipment, the success rates of in-stent CTO PCI are not worse than those of de novo CTO PCI. Clinicians should therefore not refrain from treating these lesions because of concerns about failure. However, in-stent CTO PCI has a higher incidence of long-term adverse outcomes, which should be considered during preoperative physician-patient interactions. In addition, clinicians must recognize and execute strategies to enhance the long-term patency of vessels treated with in-stent CTOs. Aggressive antiplatelet therapies should be explored in these patients and the use of IVUS should be encouraged for stent optimization. Further research on strategies to reduce restenosis in high-risk cases could help improve the outcomes.
The results of our review should be interpreted in light of the following limitations: First, we analyzed data only from retrospective studies, which are prone to selection bias. Furthermore, databases are prone to errors in record-keeping, which can alter the results. Secondly. The number of patients in the in-stent CTO group was small in several studies, which could be partly attributed to the uncommon nature of the lesion. Third, the success rate of CTO-PCI greatly depends on the operator’s experience and skill. However, this factor was not assessed in the present meta-analysis. Fourth, there were several variations in the baseline patient and lesion characteristics between the two groups which could have skewed the outcomes. Multi-variable adjusted data were presented in a limited number of studies, mostly for MACE. The lack of adjusted data for other important outcomes, such as mortality, TVR, and MI, was a significant limitation of the included studies. Finally, early and long-term data were not universally reported by all included studies, and the number of studies in the meta-analyses for adverse outcomes was lower than the total number of studies included. Moreover, the follow-up period was not consistent among the studies, ranging from one to five years, which contributed to the moderate to substantial heterogeneity observed in the meta-analysis of late clinical outcomes.
Conclusion
The results of the current meta-analysis involving 19996 patients indicated that in-stent CTO PCI has success rates similar to those of de novo CTO PCI. There was no difference in short-term adverse outcomes between the two groups; however, patients undergoing in-stent CTO PCI face a significantly higher risk of long-term MACE and MI, primarily due to an increased need for TVR. Given the substantial heterogeneity observed in late outcomes, these results should be interpreted with caution. Future large-scale prospective studies with standardized adjusted data are essential to confirm these findings and guide clinical management.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Zhejiang Province Traditional Chinese Medicine Science and Technology Program (2024ZL876).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Marechal P, Davin L, Gach O, et al. Coronary chronic total occlusion intervention: utility or futility. Expert Rev Cardiovasc Ther. 2018;16(5):361–16. doi:10.1080/14779072.2018.1459187
2. Safley DM, House JA, Rutherford BD, et al. Success rates of percutaneous coronary intervention of chronic total occlusions and long-term survival in patients with diabetes mellitus. Diab Vasc Dis Res. 2006;3(1):45–51. doi:10.3132/dvdr.2006.006
3. Creaney C, Walsh SJ. Antegrade chronic total occlusion strategies: a technical focus for 2020. Interv Cardiol. 2020;15:e08. doi:10.15420/icr.2020.05
4. Christakopoulos GE, Christopoulos G, Carlino M, et al. Meta-analysis of clinical outcomes of patients who underwent percutaneous coronary interventions for chronic total occlusions. Am J Cardiol. 2015;115(10):1367–1375. doi:10.1016/j.amjcard.2015.02.038
5. Fefer P, Knudtson ML, Cheema AN, et al. Current perspectives on coronary chronic total occlusions: the Canadian multicenter chronic total occlusions registry. J Am Coll Cardiol. 2012;59(11):991–997. doi:10.1016/j.jacc.2011.12.007
6. Abdel-Karim AR, Lombardi WB, Banerjee S, et al. Contemporary outcomes of percutaneous intervention in chronic total coronary occlusions due to in-stent restenosis. Cardiovasc Revasc Med. 2011;12(3):170–176. doi:10.1016/j.carrev.2010.08.002
7. Azzalini L, Dautov R, Ojeda S, et al. Procedural and long-term outcomes of percutaneous coronary intervention for in-stent chronic total occlusion. JACC. 2017;10(9):892–902. doi:10.1016/j.jcin.2017.01.047
8. Gong ML, Mao Y, Liu JH. Long-term outcomes of percutaneous coronary intervention for in-stent chronic total occlusion. Chin Med J. 2020;134(3):302–308. doi:10.1097/CM9.0000000000001289
9. Mir T, Ullah W, Sattar Y, et al. Outcomes of percutaneous intervention in in-stent versus de-novo chronic total occlusion: a meta-analysis. Expert Rev Cardiovasc Ther. 2020;18(11):827–833. doi:10.1080/14779072.2020.1813026
10. Vemmou E, Quadros AS, Dens JA, et al. In-stent CTO percutaneous coronary intervention: individual patient data pooled analysis of 4 multicenter registries. JACC. 2021;14(12):1308–1319. doi:10.1016/j.jcin.2021.04.003
11. Wang T, Guan H, Tian T, et al. Thirty-day and 5-year results of percutaneous coronary intervention for in-stent restenotic chronic total occlusion lesions: data from 2659 consecutive patients. Catheter Cardiovasc Interv. 2021;97 Suppl 2:1016–1024. doi:10.1002/ccd.29585
12. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):89. doi:10.1186/s13643-021-01626-4
13. Wells G, Shea B, O’Connell D, et al. The newcastle–ottawa scale (NOS) for assessing the quality of non-randomized studies in meta-analysis. 2000.
14. Christopoulos G, Karmpaliotis D, Alaswad K, et al. The efficacy of “hybrid” percutaneous coronary intervention in chronic total occlusions caused by in-stent restenosis: insights from a US multicenter registry. Catheter Cardiovasc Interv. 2014;84(4):646–651. doi:10.1002/ccd.25465
15. Lamelas P, Padilla L, Abud M, et al. In-stent chronic total occlusion angioplasty in the LATAM-CTO registry. Catheter Cardiovasc Interv. 2021;97(1):E34–e39. doi:10.1002/ccd.28937
16. Suzuki Y, Tsuchikane E, Katoh O, et al. Outcomes of percutaneous coronary interventions for chronic total occlusion performed by highly experienced japanese specialists: the first report from the japanese CTO-PCI expert registry. JACC Cardiovasc Interv. 2017;10(21):2144–2154. doi:10.1016/j.jcin.2017.06.024
17. Abbas AE, Brewington SD, Dixon SR, et al. Success, safety, and mechanisms of failure of percutaneous coronary intervention for occlusive non-drug-eluting in-stent restenosis versus native artery total occlusion. Am J Cardiol. 2005;95(12):1462–1466. doi:10.1016/j.amjcard.2005.01.098
18. Tang G, Zheng N, Yang G, et al. Procedural results and long-term outcomes of percutaneous coronary intervention for in-stent restenosis chronic total occlusion compared with de novo chronic total occlusion. Int J Gen Med. 2021;14:5749–5758. doi:10.2147/IJGM.S328332
19. Gao K, Li B-L, Zhang M, et al. Long-term outcomes of percutaneous coronary intervention for patients with in-stent chronic total occlusion versus de novo chronic total occlusion. Angiology. 2021;72(8):740–748. doi:10.1177/0003319721998575
20. Yoon YH, Lee PH, Lee S-W, et al. Clinical outcomes after percutaneous coronary intervention for in-stent chronic total occlusion. EuroIntervention. 2020;16(6):e472–e479. doi:10.4244/EIJ-D-19-00650
21. Lee SH, Cho JY, Kim JS, et al. A comparison of procedural success rate and long-term clinical outcomes between in-stent restenosis chronic total occlusion and de novo chronic total occlusion using multicenter registry data. Clin Res Cardiol. 2020;109(5):628–637. doi:10.1007/s00392-019-01550-7
22. Guelker JE, Bufe A, Blockhaus C, et al. Acute, in-hospital outcome of percutaneous coronary intervention for in-stent chronic total occlusion. Cardiovasc Revasc Med. 2019;20(11):997–1000. doi:10.1016/j.carrev.2018.12.007
23. Abdel-Wahab M, Nienaber CA, Mostafa AE, et al. Clinical outcome of percutaneous treatment of in-stent restenosis with drug-eluting stents: results from the first phase of the prospective multicentre German DES.DE registry. EuroIntervention. 2011;7(2):201–208. doi:10.4244/EIJV7I2A34
24. Buchanan KD, Torguson R, Rogers T, et al. In-stent restenosis of drug-eluting stents compared with a matched group of patients with de novo coronary artery stenosis. Am J Cardiol. 2018;121(12):1512–1518. doi:10.1016/j.amjcard.2018.02.033
25. Gao Z, Xu BO, Yang Y-J, et al. Long- T erm outcomes of Drug- E luting stent therapy for In- S tent restenosis versus de novo lesions. J Interv Cardiol. 2013;26(6):550–555. doi:10.1111/joic.12069
26. Honton B, Lipiecki J, Monségu J, et al. Mid-term outcome of de novo lesions vs. in stent restenosis treated by intravascular lithotripsy procedures: insights from the French Shock Initiative. Int J Cardiol. 2022;365:106–111. doi:10.1016/j.ijcard.2022.07.023
27. Jakobsen L, Christiansen EH, Freeman P, et al. Comparison of outcome after percutaneous coronary intervention for de novo and in-stent restenosis indications. Am J Cardiol. 2025;235:1–8. doi:10.1016/j.amjcard.2024.10.019
28. Redfors B, Généreux P, Witzenbichler B, et al. Percutaneous coronary intervention of lesions with in-stent restenosis: a report from the ADAPT-DES study. Am Heart J. 2018;197:142–149. doi:10.1016/j.ahj.2017.11.011
29. Richardt G, Leschke M, Abdel-Wahab M, et al. Clinical outcomes of the Resolute zotarolimus-eluting stent in patients with in-stent restenosis: 2-year results from a pooled analysis. JACC. 2013;6(9):905–913. doi:10.1016/j.jcin.2013.04.017
30. Sang Z, Zhao Y, Ji Q, et al. Drug-coated balloon-only strategy in de novo lesions versus in-stent restenosis for the treatment of non-ST-elevation acute coronary syndrome: a retrospective cohort study. Medicine. 2025;104(28):e43357. doi:10.1097/MD.0000000000043357
31. Takeuchi M, Dohi T, Fukase T, et al. Comparison of clinical outcomes between percutaneous coronary intervention for de novo lesions versus in-stent restenosis lesions. Cardiovasc Interv Ther. 2022;37(2):324–332. doi:10.1007/s12928-021-00792-5
32. Tamez H, Secemsky EA, Valsdottir LR, et al. Long-term outcomes of percutaneous coronary intervention for in-stent restenosis among Medicare beneficiaries. EuroIntervention. 2021;17(5):e380–e387. doi:10.4244/EIJ-D-19-01031
33. de la Torre Hernandez JM, Rumoroso JR, Subinas A, et al. Percutaneous intervention in chronic total coronary occlusions caused by in-stent restenosis: procedural results and long-term clinical outcomes in the TORO (Spanish registry of chronic TOtal occlusion secondary to an occlusive in-stent RestenOsis) multicentre registry. EuroIntervention. 2017;13(2):e219–e226. doi:10.4244/EIJ-D-16-00764
34. Danek BA, Karatasakis A, Karmpaliotis D, et al. Use of antegrade dissection re-entry in coronary chronic total occlusion percutaneous coronary intervention in a contemporary multicenter registry. Int J Cardiol. 2016;214:428–437. doi:10.1016/j.ijcard.2016.03.215
35. Huang WC, Teng H-I, Hsueh C-H, et al. Intravascular ultrasound guided wiring re-entry technique for complex chronic total occlusions. J Interv Cardiol. 2018;31(5):572–579. doi:10.1111/joic.12518
36. Wilson WM, Walsh S, Hanratty C, et al. A novel approach to the management of occlusive in-stent restenosis (ISR). EuroIntervention. 2014;9(11):1285–1293. doi:10.4244/EIJV9I11A218
37. Nakazawa G, Vorpahl M, Finn AV, et al. One step forward and two steps back with drug-eluting-stents: from preventing restenosis to causing late thrombosis and nouveau atherosclerosis. JACC Cardiovasc Imaging. 2009;2(5):625–628. doi:10.1016/j.jcmg.2009.01.011
38. Nakazawa G, Otsuka F, Nakano M, et al. The pathology of neoatherosclerosis in human coronary implants bare-metal and drug-eluting stents. J Am Coll Cardiol. 2011;57(11):1314–1322. doi:10.1016/j.jacc.2011.01.011
39. Otsuka F, Vorpahl M, Nakano M, et al. Pathology of second-generation everolimus-eluting stents versus first-generation sirolimus- and paclitaxel-eluting stents in humans. Circulation. 2014;129(2):211–223. doi:10.1161/CIRCULATIONAHA.113.001790
40. Elbadawi A, AT D, Mahana I, et al. Outcomes of percutaneous coronary intervention for in-stent restenosis versus de novo lesions: a meta-analysis. J Am Heart Assoc. 2023;12(13):e029300. doi:10.1161/JAHA.122.029300
41. AL N, Nso N, Mbome Y, et al. Comparison of percutaneous coronary intervention-related adverse cardiac outcomes in patients with in-stent vs de novo chronic total occlusion: a systematic review and meta-analysis. Curr Probl Cardiol. 2023;48(9):101797. doi:10.1016/j.cpcardiol.2023.101797
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Elevated HsCRP in Chronic Obstructive Pulmonary Disease: A Prospective Study of Long-Term Outcomes After Percutaneous Coronary Intervention
Zheng Y, Qi Y, Seery S, Yang J, Li C, Wang W, Gao J, Meng X, Shao C, Tang YD
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2517-2528
Published Date: 7 October 2022
Predictive Value of Systemic Inflammation Score for Contrast-Associated Acute Kidney Injury and Adverse Outcomes Among Patients Undergoing Elective Percutaneous Coronary Intervention
Zeng JL, Xiang YF, Zhang LW, Chen LC, Chen JH, Liang WJ, You Z, Wang CX, Lin ZJ, Lin KY, Guo Y
Journal of Inflammation Research 2023, 16:2845-2854
Published Date: 8 July 2023
Antegrade versus Retrograde Approach for Recanalization of Ostial or Stumpless Coronary Chronic Total Occlusion
Wu X, Wu M, Huang H, Liu Z, Cai J, Zhang Q, Huang H
International Journal of General Medicine 2023, 16:3995-4005
Published Date: 1 September 2023
Prognostic Value of Fibrinogen-to-Albumin Ratio in Coronary Three-Vessel Disease
Li X, Wang Z, Zhu Y, Lv H, Zhou X, Zhu H, Liu J, Guo L
Journal of Inflammation Research 2023, 16:5767-5777
Published Date: 1 December 2023
Exploring the Complementary Role of Traditional Chinese Medicine in Enhancing Percutaneous Coronary Intervention Outcomes: Mechanisms, Benefits, and Future Research Directions
Zheng S, Guo J, Wang Q
Therapeutics and Clinical Risk Management 2025, 21:1069-1083
Published Date: 10 July 2025