")
Back to Journals » International Journal of General Medicine » Volume 16
Antegrade versus Retrograde Approach for Recanalization of Ostial or Stumpless Coronary Chronic Total Occlusion
Authors Wu X, Wu M, Huang H, Liu Z, Cai J, Zhang Q, Huang H
Received 11 July 2023
Accepted for publication 30 August 2023
Published 1 September 2023 Volume 2023:16 Pages 3995—4005
DOI https://doi.org/10.2147/IJGM.S429956
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Xi Wu,* Mingxing Wu,* Haobo Huang,* Zhe Liu, Jie Cai, Qizhou Zhang, He Huang
Department of Cardiology, Xiangtan Central Hospital, Xiangtan, Hunan, 411100, People’s Republic of China
*These authors contributed equally to this work
Correspondence: He Huang, Department of Cardiology, Xiangtan Central Hospital, Xiangtan, Hunan, 411100, People’s Republic of China, Email [email protected]
Purpose: This research aimed to evaluate the procedural and in-hospital clinical outcomes of percutaneous coronary intervention (PCI) for ostial or stumpless chronic total occlusion (CTO) utilizing both the antegrade-only and retrograde approaches.
Methods: A comprehensive retrospective examination was conducted on the procedural and in-hospital clinical outcomes of 89 consecutive patients subjected to ostial or stumpless CTO PCI at our institution between April 2015 and October 2022.
Results: The antegrade-only technique demonstrated a superior technical success rate (92.0% vs 71.9%, p = 0.041) and procedural success rate (92.0% vs 68.8%, p = 0.022) in comparison to the retrograde approach (RA). The RA group presented a notably elevated Japanese-CTO (J-CTO) score relative to the antegrade-only approach group (2.45± 0.73 vs 1.64± 0.70, p < 0.001). The antegrade-only approach group manifested an increased frequency of microchannels at the proximal stump relative to the RA group (56.0% vs 10.9%, p < 0.001). In-hospital major adverse cardiac events (MACE) and in-hospital myocardial infarction (MI) were observed more prevalently in the RA group (18.8% vs 0, p = 0.003; 15.6% vs 0, p = 0.008; respectively). A J-CTO score below 2 and the manifestation of microchannels at the proximal stump were identified as predictors for successful antegrade-only approach PCI for ostial or stumpless CTO (OR: 2.79 [95% CI: 1.92– 5.03, P =0.003]; OR: 2.89 [95% CI: 1.32– 6.03, P =0.001]; respectively).
Conclusion: Relative to RA PCI for ostial or stumpless CTO, the antegrade-only approach is utilized for less complex CTO lesions and is associated with a diminished probability of in-hospital MACE.
Keywords: chronic total occlusion, percutaneous coronary intervention, intravascular ultrasound
Introduction
Recanalization of coronary chronic total occlusion (CTO) improves myocardial ischemia symptom and patient's quality of life.1,2 Notwithstanding the inherent intricacies and elevated risk of failure in percutaneous coronary intervention (PCI) for CTO, advancements in devices, experience, and techniques have led to improved success rates.3 Failure to successfully navigate the guidewire into the true lumen remains the primary reason for unsuccessful CTO PCI.4,5 Ostial or stumpless CTOs delineate a specialized category of CTOs, presenting persistent revascularization challenges,6 as it can be difficult to accurately locate the entrance of the CTO, with the guidewire often slipping into a side branch. To circumvent this, the intravascular ultrasound (IVUS) catheter may be extended to the side branch of the CTO lesion using the initially positioned first wire, and then drawn back until the IVUS visualizes the CTO cap’s entrance point.7 Maintaining the position of the IVUS provides the advantage of real-time vessel imaging, enabling the visualization of the CTO-dedicated guidewire entering the true lumen of the proximal cap.8 Additionally, the IVUS device and technique can assess the morphology of the proximal stump, helping the operator in selecting the appropriate wire and significantly improving the success rate of the second wire, ideally entering centrally.9 Comparatively, IVUS-guided CTO recanalization has manifested superior clinical outcomes and a potential diminution in major adverse cardiac events (MACE) relative to angiography-guided CTO recanalization10,11. While retrograde techniques have contributed to increased overall success rates of CTO-PCI, antegrade-only procedures have demonstrated higher technical and procedural effectiveness costs, as well as reduced in-hospital major negative cardiac event rates as compared to retrograde procedures. The present research compared the characteristics and procedural outcomes of ostial or stumpless CTO-PCI performed using the antegrade-only method versus the retrograde.
Materials and Methods
Research Population
The current research was retrospectively completed as a single-center research study involving 89 consecutive patients with 89 lesions who underwent PCI for ostial or stumpless CTO at Xiangtan Central Hospital, Xiangtan, Hunan, People’s Republic of China from April 2015 to October 2022 (Figure 1). All patients included in the study had a single native vessel CTO. The current study was carried out in accordance with the tenets mentioned in the Helsinki Declaration and was approved by the Ethical Board of Xiangtan Central Hospital. Prior to the commencement of the research, our team obtained written informed consent from each patient.
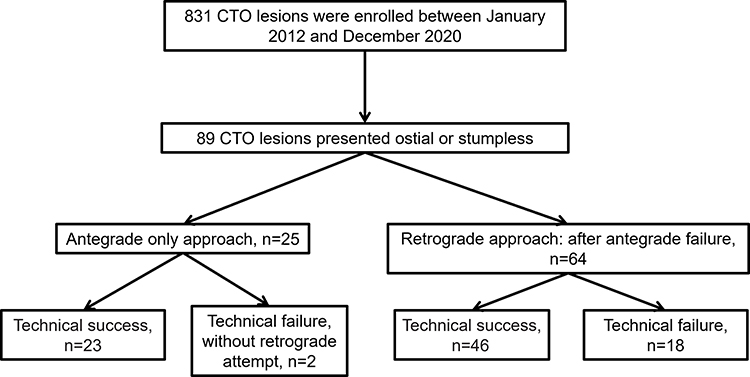 |
Figure 1 The study flow chart. Abbreviation: CTO, chronic total occlusion. |
Definition
A coronary CTO was characterized as a complete obstruction of a cardiovascular defined with thrombolysis in myocardial infarction (TIMI) grade 0 antegrade flow, exhibiting a length of manifestations or prior angiography or a history of myocardial infarction (MI) in a specific region supplied by the blocked channel,12 and with an approximate age of ≥3 months. The indication for these procedures was angina in combination with verified myocardial viability and/or ischemia within the territory supplied by the target vessel. Technical success denoted the restoration of TIMI 3 blood flow accompanied by a residual stenosis of less than 30%. Procedural success entailed technical success without incurring any MACE during the hospital stay. MACE comprised of death, MI, repeat target vessel revascularisation (TVR), cerebral vascular accident, and instances requiring pericardiocentesis or surgical repair due to tamponade. The in-hospital events were evaluated in order to detect major complications, which included any MACE events that occurred ahead of hospital discharge. A retrograde procedure was every effort to traverse the retrograde way, regardless of success. It was declared secondary when the contractor anticipated an antegrade crossing but had to divert to a retrograde approach (RA) owing to antegrade failure. RA via septal collaterals or via epicardial collaterals were at the operator’s discretion, according to the safety and feasibility of CTO’s collateral channel.
Procedure Description
A soft-tipped guidewire is carefully inserted into the neighboring side branch of the CTO, while a 40-MHz rotational IVUS catheter (Opticrosstm, Boston Scientific, America) is advanced into the side branch originating from the proximal stump site. The IVUS pullback procedure alone allows for identification and assessment of the proximal cap of the CTO. A microchannel located at proximal cap of the CTO is defined as a low echogenicity structure situated at the center of proximal cap of the CTO (Figure 2). The IVUS catheter is positioned at the CTO’s entrance, and a dedicated CTO-PCI wire is pushed into the CTO’s proximal stump using microcatheters. Additionally, we provide an algorithm for the successful crossing of the CTO (Figure 3). IVUS imaging is performed following guidewire crossing and pre-dilation using a compliant balloon ranging from 1.5 to 2.0 mm. Ultimately, balloon dilatation and stent implantation are performed following evaluation of the CTO using IVUS. There are 2 well-experienced CTO operators performed the procedures in the center and had an annual volume of more than 300 non-CTO PCIs and 80 CTO PCIs.
 |
Figure 2 Intravascular ultrasound image of microchannel at proximal stump: (A) A left anterior descending artery was totally occluded. A 40-MHz IVUS catheter (Opticrosstm, Boston Scientific, America) pullback from the side branch identifies the ostium of the CTO (white arrow). (B) Microchannel (a low echogenicity structure, dotted circle) at the proximal stump (solid circle). (C and D) A left anterior descending totally occluded artery (white arrow) and without microchannel at the proximal stump (solid circle). |
 |
Figure 3 Algorithm for chronic total occlusion crossing. Abbreviations: IVUS, intravascular ultrasound; CTO, chronic total occlusion; ADR, antegrade dissection/reentry; LAST, limited antegrade subintimal tracking. |
Statistical Analysis
Variables were presented as mean ± SD, and categorical variables were expressed in percentages. For categorical variables, either the chi-square or Fisher’s exact tests were deployed, whereas for continuous determinants, the Student’s t-test was used. To identify clinical, procedural, and angiographic parameters related with technical success in antegrade-only CTO PCI, a logistic regression analysis was performed. Our multivariable analysis included parameters that exhibited a significant difference in the univariate logistic analysis. IBM SPSS Statistics 24.0 (America) was employed for every statistical evaluation. Statistical significance was determined by two-sided p-values of 0.05.
Results
Patient Characteristics
In the present investigation, 89 patients with 89 ostial or stumpless CTOs were included. Among them, 25 patients underwent an exclusive antegrade-only approach for CTO-PCI, while 64 patients underwent RA CTO-PCI. The fundamental clinical characteristics are detailed in Table 1. When comparing the antegrade-only approach group to the RA group, no statistically significant differences were observed in terms of age, age exceeding 75 years, male gender, and body mass index. The coronary artery disease (CAD) risk factors, including hypertension, diabetes mellitus, family history of CAD, and current smoking, were consistent across both groups. The incidence of comorbidities, such as a history of MI and stroke, was similar for both groups. Additionally, no significant differences were observed in left ventricular ejection fraction, blood lipid levels, clinical presentation, or the presence of multivessel disease between the two groups.
 |
Table 1 Baseline Clinical Characteristics |
CTO Characteristics
The angiographic and interventional procedure features (Table 2). The J-CTO (Japanese-CTO) score was substantially higher in the RA group than in the antegrade-only approach group (2.45±0.73 vs 1.64±0.70, p<0.001). In comparison to the antegrade-only approach group, the incidence of J-CTO scores above 3 was notably higher in the RA group (51.6% vs 12.0, p=0.001). On the other hand, the incidence of J-CTO scores of 1 was much lower in the RA group than in the antegrade-only approach group (9.4% vs 48.0%, p<0.001), with no significant difference observed in the incidence of J-CTO scores of 2 (40.0% vs 40.6%, p=0.957). Among the components of the J-CTO score, the presence of lesion length of 20 or more (≧20) was significantly more frequent in the retrograde group than in the antegrade-only group (73.4% vs 28.0%, p<0.001).
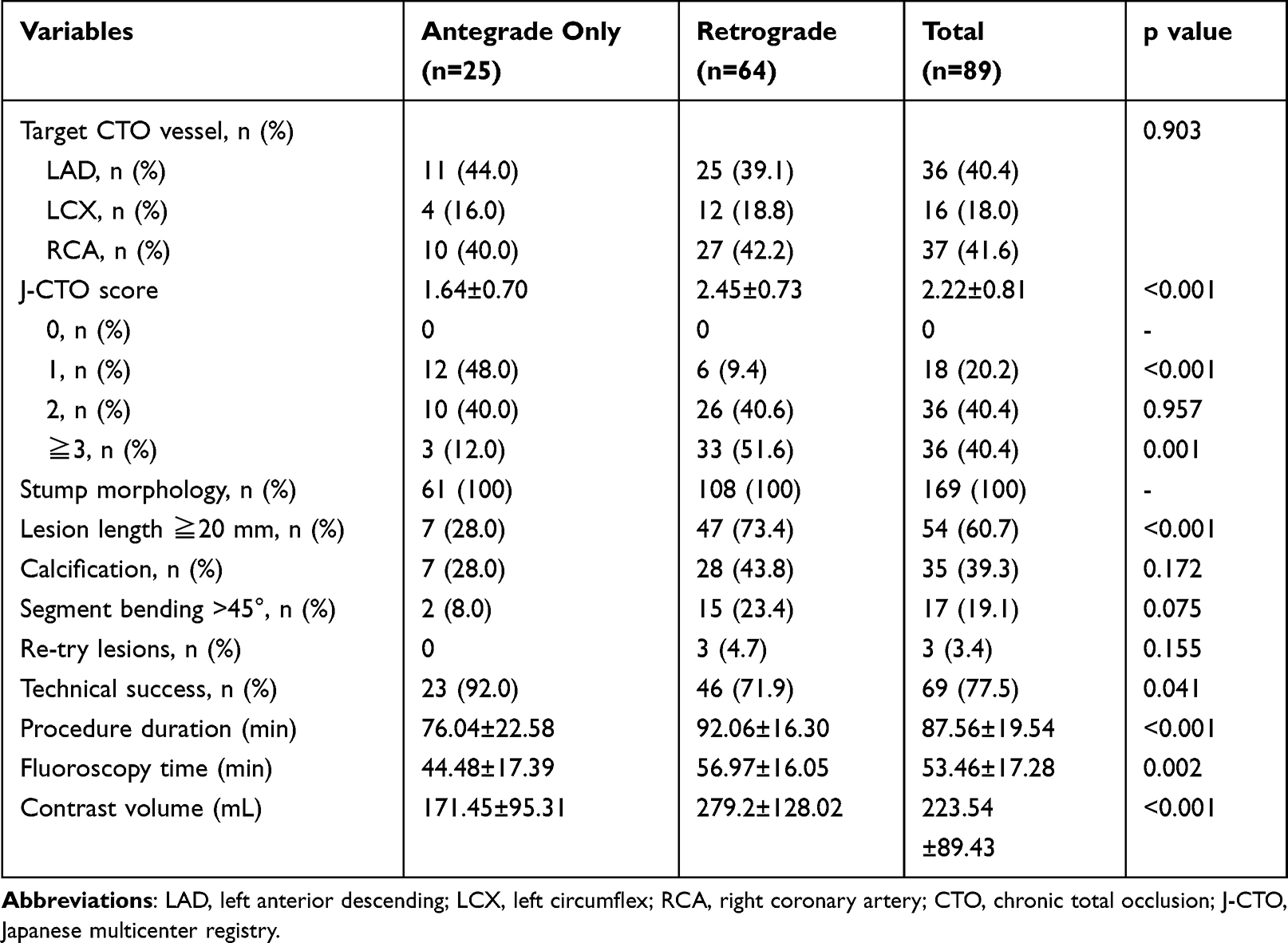 |
Table 2 Angiographic and Interventional Procedure Characteristics |
Procedural Characteristics and IVUS Findings
The technical success rates for the 89 CTOs were 77.5%. The antegrade-only approach had a success rate of 92.0%, while the RA had a success rate of 71.9% (p = 0.041). Compared to the antegrade-only approach group, the RA group had significantly longer procedure lengths, fluoroscopic times, and greater contrast volumes (92.06±16.30 vs 76.04±22.58, p<0.001; 56.97±16.05 vs 44.48±17.39, p=0.002; 171.45±95.31 vs 279.2±128.02, p<0.001, respectively) (Table 2). The antegrade-only approach group had a higher prevalence of microchannels at the proximal stump than the RA group (56.0% vs 10.9%, p<0.001) (Figure 4). Additionally, the antegrade-only approach group exhibited a higher prevalence of calcification in CTO lesion than the RA group (73.9% vs 47.8%, p=0.032). However, there were no significant differences between the two groups in terms of maximum plaque burden post-balloon pre-stenting, hematoma pre-stenting, minimum stent area (MSA) within the stent or CTO, the number of stents used, and total stent length (Table 3).
 |
Table 3 IVUS Findings in Successfully Recanalized CTO Lesions |
 |
Figure 4 Antegrade-only approach group had more microchannel at proximal stump than retrograde approach group, 56.0% (n=14) vs 10.9% (n=7), p<0.001. |
In-Hospital Outcomes and Major Adverse Cardiac Event
The in-hospital outcomes and major adverse cardiac events between the two groups are summarized in Table 4. The antegrade-only approach group had significantly higher procedural success rates than the RA group (92.0% vs 68.8%, p=0.022). The incidence of MACE in the hospital was higher in the RA group than in the antegrade-only approach group (18.8% vs 0, p=0.003). In the RA group, in-hospital MI occurred in 10 cases (15.6%, p=0.008), cerebral vascular accident in 1 case (1.6%, p=0.415), and tamponade in 1 case (1.6%, p=0.415) in RA group. Three coronary perforation (p=0.155) occurred in RA group.
 |
Table 4 In-Hospital Outcomes and Major Adverse Cardiac Events |
Predictors of Antegrade-Only Approach Success
Table 5 provides insights into the predictive capabilities of certain factors for the success of antegrade-only approach PCI in ostial or stumpless CTOs. A J-CTO score of less than 2 predicted the success of the antegrade-only approach in treating these CTOs (P = 0.031). Similarly, the presence of microchannels at the proximal stump indicated a 3.47-fold increased likelihood (95% CI: 1.09–8.31, P = 0.001) of successful antegrade-only approach for PCI in ostial or stumpless CTOs. Conversely, the presence of calcification within the CTO lesion was found to predict failure of the antegrade-only approach for ostial or stumpless CTO-PCI (P = 0.026). Table 6 lists the parameters included in the multivariable analysis, considering significant differences identified in the univariate logistic analysis. It is noted that a J-CTO score of less than 2 and the presence of microchannels at the proximal stump were identified as predictors for the success of antegrade-only approach in PCI for ostial or stumpless CTOs (P =0.003, P=0.001, respectively).
 |
Table 5 Univariate Analysis for Antegrade-Only Approach Technical Success |
 |
Table 6 Multivariate Predictors for Antegrade Only Approach Technical Success |
Discussion
The main findings of the current study on ostial or stumpless CTO-PCI, comparing the antegrade-only technique to the RA technique: (a) patients undergoing the antegrade-only approach for CTO-PCI exhibited lower CTO lesion complexity than those undergoing RA CTO-PCI; (b) the antegrade-only strategy for CTO-PCI showed a greater percentage of technical and procedural success, as well as a decreased risk of in-hospital MACE; (c) the determinants for achieving antegrade-only technical success in ostial or stumpless CTO-PCI were identified as J-CTO score < 2 and the presence of microchannel at the proximal stump.
The J-CTO Score for Antegrade-Only Approach in Ostial or Stumpless CTO PCI
The antegrade wiring approach is the predominant wire crossing technique in contemporary CTO-PCI, representing the final crossing strategy in over 50% of successful CTO-PCIs.13 Our current statistical research also demonstrated that the antegrade-only strategy had a greater rate of technical and procedural success than the RA group. Nevertheless, our sample size was small, which does not permit us to definitively state that the RA approach is inferior, but on the contrary, it complements the antegrade approach by addressing complex and challenging cases. However, it is worth noting that the RA group exhibited a higher complexity of CTO lesion morphology when assessed using the J-CTO score (2.45±0.73 vs 1.64±0.70, p < 0.001). This finding indicates that the successful implementation of the antegrade-only approach is correlated with the J-CTO score in ostial or stumpless CTO-PCI. The RA is frequently employed in cases involving higher J-CTO score CTO lesions. For instance, Karmpaliotis et al14 investigated 1301 cases that underwent CTO PCI and found that the retrograde group exhibited significantly greater complexity (mean J-CTO score: 3.1±1.0 vs 2.1±1.2; P<0.001) and lower technical success rates compared to the antegrade-only group (85% vs 94%; P<0.001). Similarly, Suzuki et al3 observed that among 2846 consecutive CTO-PCI procedures, the primary antegrade group had a considerably higher technical success rate than the primary retrograde group (91.0% vs 87.3%; p < 0.0001). The J-CTO scores of the primary retrograde group were much greater than those of the primary antegrade group (1.9±1.1 vs 2.4±1.1; p < 0.001). Notably, a multicentre registry conducted by Wu Eugene et al15 also demonstrated a higher technical success rate in the antegrade-only group (95.9% vs.91.2%, p = 0.03) and lower J-CTO score (2.5±1.2 vs 3.4±1.0, p<0.001). Megaly et al16 conducted an analysis of 12 observational studies involving 10,240 patients and found that CTO lesions treated with the antegrade-only approach had a lower J-CTO score (1.9 vs.2.8, p < 0.001) and were associated with a higher success rate (87.4% vs 80.9%, p <0 0.001). The OPEN-CTO registry,17 demonstrated that retrograde procedures were performed on CTOs with higher morphological complexity and J-CTO scores (2.7 vs 1.9, p <0 0.001), resulting in an overall lower technical success rate compared to antegrade-only procedures (82.4% vs 94.2%, p < 0.001). To rate the challenge of CTO-PCIs, an estimation rule centered around J-CTO scores has been devised.18 Furthermore, a hybrid algorithm for CTO-PCIs has indicated that cases involving complex morphological CTOs often prefer the RA.14
Microchannel at Proximal Stump for Antegrade-Only Approach in Ostial or Stumpless CTO PCI
In our analysis, the presence of microchannel at the proximal stump was more prevalent in the antegrade-only approach compared to the RA. Additionally, our study revealed that the presence of microchannels at the proximal stump serves as a positive predictor for the successful performance of ostial or stumpless percutaneous CTO-PCI. A commonly held viewpoint suggests that following the occurrence of coronary occlusion, thrombosis progresses in an upward direction towards the bifurcation of the side branch.19,20 Autopsy analyses have shown that the CTO body predominantly consists of organized thrombus with microchannels, characterized by small lumens within the CTO lesion, averaging 200µm in size, and connecting the proximal and distal caps.21 According to the antegrade loose tissue tracking concept, the wire traverses the CTO lesions by following the path of the microchannels and loose tissue.22 Based on this theory, the presence of microchannels within CTO lesions may significantly influence the success of wire crossing in CTO-PCI. The utilization of IVUS-guided wiring techniques may prove beneficial in identifying the precise entry point of occlusion in stumpless CTO cases, while also confirming the wire puncture into the microchannel at the proximal cap.
In-Hospital MACE
Several observational studies and RCT23–25 have found that effective CTO PCI is related with improved standards of life, decreased need for CABG, improved left ventricular function, and reversal remodeling of the left ventricle when compared to unsuccessful revascularization. The retrograde method is now critical in achieving high success rates, especially in complicated lesions where the antegrade approach is either technically impossible or unsuccessful.13 When compared to the antegrade-only technique in CTO-PCI, the retrograde strategy has been tied to greater rates of in-hospital MACE, target vessel revascularization, and target vessel failure.16,26,27 Our analysis also demonstrated higher rates of in-hospital MI in the RA group compared to the antegrade-only approach, suggesting that the increased occurrence of periprocedural MI may be associated with the complexity of RA CTO PCI. Furthermore, our research revealed that in-hospital MACE was more prevalent in the RA group than in the antegrade-only approach group. Consistent with the findings of the OPEN-CTO registry, the RA group exhibited higher rates of in-hospital MACE compared to the antegrade-only approach group (10.8% vs 3.3%, p < 0.001).17 A comprehensive meta-analysis found that retrograde patients had a greater likelihood of periprocedural MI, the requirement for urgent pericardiocentesis, and contrast-induced nephropathy as compared to antegrade-only cases.16 Patients in the retrograde group often present with more complex CTOs, and failed revascularization may contribute to worse in-hospital outcomes. The PROGRESS-CTO complication scores, which aid in calculating the level of periprocedural complication danger in patients going through CTO PCI, are based on eight criteria (age, gender, calcification status, stump, left ventricular ejection fraction, prior CABG, atrial fibrillation, crossing strategy). These findings indicate that the retrograde technique and blunt stump are both related with an increased risk of in-hospital MACE.28 In a recent study, it has been shown that the dual distal radial access may in fact represent an universal asset in terms of vascular safety, patient and operator ergonomics and lower radiation dose.29
Limitation
First, this was a single-center retrospective observational study with a limited number of patient. Second, some potential selection bias may have existed in patient selection. Third, only in-hospital outcomes were evaluated in this study. Fourth, the microchannel in the present study have not been validated by pathological examination. More research on substantial lesions is required to analyze the coherence between the IVUS discoveries and pathology. The longer-term impact should be evaluated in ongoing study. New forward-looking technologies and devices are hope to improve the success rate of ostial or stumpless CTO-PCI.
Conclusion
In contrast to the RA in PCI for ostial or stumpless CTO, the antegrade-only approach is employed in less complex CTO lesions and is linked to a reduced risk of in-hospital MACE and complications. Notably, a J-CTO score of less than 2 and the presence of a microchannel at the proximal stump have been identified as predictors for the successful implementation of the antegrade-only approach in PCI for ostial or stumpless CTO. More research is needed to evaluate the immediate and long-term results of ostial or stumpless CTO-PCI.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The current study was carried out in accordance with the tenets mentioned in the Helsinki Declaration and was approved by the Ethical Board of Xiangtan Central Hospital (approval number: X20201898). Prior to the commencement of the research, our team obtained written informed consent from each patient.
Consent for Publication
Not applicable. No individual patient data will be reported.
Acknowledgment
We are grateful to Bo Chen for their secretarial assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no grants from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Amat-Santos IJ, Martin-Yuste V, Fernández-Díaz JA, et al. Procedural, functional and prognostic outcomes following recanalization of coronary chronic total occlusions. Results of the Iberian Registry. Rev Esp Cardiol. 2019;72(5):373–382. doi:10.1016/j.rec.2018.05.020
2. Aziz S, Stables RH, Grayson AD, Perry RA, Ramsdale DR. Percutaneous coronary intervention for chronic total occlusions: improved survival for patients with successful revascularization compared to a failed procedure. Catheterizat Cardiovasc Intervent. 2007;70(1):15–20. doi:10.1002/ccd.21092
3. Suzuki Y, Tsuchikane E, Katoh O, et al. Outcomes of percutaneous coronary interventions for chronic total occlusion performed by highly experienced Japanese specialists: the first report from the Japanese CTO-PCI Expert Registry. JACC Cardiovasc Interv. 2017;10(21):2144–2154. doi:10.1016/j.jcin.2017.06.024
4. Saito S. Different strategies of retrograde approach in coronary angioplasty for chronic total occlusion. Catheterizat Cardiovasc Intervent. 2008;71(1):8–19. doi:10.1002/ccd.21316
5. Syrseloudis D, Secco GG, Barrero EA, et al. Increase in J-CTO lesion complexity score explains the disparity between recanalisation success and evolution of chronic total occlusion strategies: insights from a single-centre 10-year experience. Heart. 2013;99(7):474–479. doi:10.1136/heartjnl-2012-303205
6. Stone GW, Colombo A, Teirstein PS, et al. Percutaneous recanalization of chronically occluded coronary arteries: procedural techniques, devices, and results. Catheterizat Cardiovasc Intervent. 2005;66(2):217–236. doi:10.1002/ccd.20489
7. Park Y, Park HS, Jang GL, et al. Intravascular ultrasound guided recanalization of stumpless chronic total occlusion. Int J Cardiol. 2011;148(2):174–178. doi:10.1016/j.ijcard.2009.10.052
8. Ryan N, Gonzalo N, Dingli P, et al. Intravascular ultrasound guidance of percutaneous coronary intervention in ostial chronic total occlusions: a description of the technique and procedural results. Int J Cardiovasc Imaging. 2017;33(6):807–813. doi:10.1007/s10554-017-1086-2
9. Mohandes M, Vinhas H, Fernández F, Moreno C, Torres M, Guarinos J. When intravascular ultrasound becomes indispensable in percutaneous coronary intervention of a chronic total occlusion. Cardiovasc Revascular Med. 2018;19(3 Pt A):292–297. doi:10.1016/j.carrev.2017.10.004
10. Shin DH, Hong SJ, Mintz GS, et al. Effects of intravascular ultrasound-guided versus angiography-guided new-generation drug-eluting stent implantation: meta-analysis with individual patient-level data from 2345 randomized patients. JACC Cardiovasc Interv. 2016;9(21):2232–2239. doi:10.1016/j.jcin.2016.07.021
11. Tian NL, Gami SK, Ye F, et al. Angiographic and clinical comparisons of intravascular ultrasound- versus angiography-guided drug-eluting stent implantation for patients with chronic total occlusion lesions: two-year results from a randomised AIR-CTO study. EuroIntervention. 2015;10(12):1409–1417. doi:10.4244/eijv10i12a245
12. Sianos G, Werner GS, Galassi AR, et al. Recanalisation of chronic total coronary occlusions: 2012 consensus document from the EuroCTO club. EuroIntervention. 2012;8(1):139–145. doi:10.4244/eijv8i1a21
13. Tajti P, Karmpaliotis D, Alaswad K, et al. The hybrid approach to chronic total occlusion percutaneous coronary intervention: update from the PROGRESS CTO Registry. JACC Cardiovasc Interv. 2018;11(14):1325–1335. doi:10.1016/j.jcin.2018.02.036
14. Christopoulos G, Kandzari DE, Yeh RW, et al. Development and validation of a novel scoring system for predicting technical success of chronic total occlusion percutaneous coronary interventions: the PROGRESS CTO (Prospective Global Registry for the Study of Chronic Total Occlusion Intervention) Score. JACC Cardiovasc Interv. 2016;9(1):1–9. doi:10.1016/j.jcin.2015.09.022
15. Wu Eugene B, Tsuchikane E, Ge L, et al. Retrograde versus antegrade approach for coronary chronic total occlusion in an Algorithm-Driven Contemporary Asia-Pacific Multicentre Registry: comparison of outcomes. Heart Lung Circ. 2020;29(6):894–903. doi:10.1016/j.hlc.2019.05.188
16. Megaly M, Ali A, Saad M, et al. Outcomes with retrograde versus antegrade chronic total occlusion revascularization. Catheterizat Cardiovasc Intervent. 2020;96(5):1037–1043. doi:10.1002/ccd.28616
17. Kalra S, Doshi D, Sapontis J, et al. Outcomes of retrograde chronic total occlusion percutaneous coronary intervention: a report from the OPEN-CTO registry. Catheterizat Cardiovasc Intervent. 2021;97(6):1162–1173. doi:10.1002/ccd.29230
18. Morino Y, Abe M, Morimoto T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011;4(2):213–221. doi:10.1016/j.jcin.2010.09.024
19. Srivatsa SS, Edwards WD, Boos CM, et al. Histologic correlates of angiographic chronic total coronary artery occlusions: influence of occlusion duration on neovascular channel patterns and intimal plaque composition. J Am Coll Cardiol. 1997;29(5):955–963. doi:10.1016/s0735-1097(97)00035-1
20. Galla JM, Whitlow PL. Coronary chronic total occlusion. Cardiol Clin. 2010;28(1):71–79. doi:10.1016/j.ccl.2009.10.003
21. Katsuragawa M, Fujiwara H, Miyamae M, Sasayama S. Histologic studies in percutaneous transluminal coronary angioplasty for chronic total occlusion: comparison of tapering and abrupt types of occlusion and short and long occluded segments. J Am Coll Cardiol. 1993;21(3):604–611. doi:10.1016/0735-1097(93)90091-e
22. Sumitsuji S, Inoue K, Ochiai M, Tsuchikane E, Ikeno F. Fundamental wire technique and current standard strategy of percutaneous intervention for chronic total occlusion with histopathological insights. JACC Cardiovasc Interv. 2011;4(9):941–951. doi:10.1016/j.jcin.2011.06.011
23. Megaly M, Saad M, Tajti P, et al. Meta-analysis of the impact of successful chronic total occlusion percutaneous coronary intervention on left ventricular systolic function and reverse remodeling. J Interv Cardiol. 2018;31(5):562–571. doi:10.1111/joic.12538
24. Galassi AR, Boukhris M, Toma A, et al. Percutaneous coronary intervention of chronic total occlusions in patients with low left ventricular ejection fraction. JACC Cardiovasc Interv. 2017;10(21):2158–2170. doi:10.1016/j.jcin.2017.06.058
25. Werner GS, Martin-Yuste V, Hildick-Smith D, et al. A randomized multicentre trial to compare revascularization with optimal medical therapy for the treatment of chronic total coronary occlusions. Eur Heart J. 2018;39(26):2484–2493. doi:10.1093/eurheartj/ehy220
26. Galassi AR, Sianos G, Werner GS, et al. Retrograde recanalization of chronic total occlusions in Europe: procedural, In-hospital, and long-term outcomes from the Multicenter ERCTO Registry. J Am Coll Cardiol. 2015;65(22):2388–2400. doi:10.1016/j.jacc.2015.03.566
27. Kwon O, Lee PH, Lee SW, et al. Retrograde approach for the percutaneous recanalisation of coronary chronic total occlusions: contribution to clinical practice and long-term outcomes. EuroIntervention. 2019;15(4):e354–e361. doi:10.4244/eij-d-18-00538
28. Simsek B, Kostantinis S, Karacsonyi J, et al. Predicting periprocedural complications in chronic total occlusion percutaneous coronary intervention: the PROGRESS-CTO complication scores. JACC Cardiovasc Interv. 2022;15(14):1413–1422. doi:10.1016/j.jcin.2022.06.007
29. Achim A, Szigethy T, Olajos D, et al. Switching from proximal to distal radial artery access for coronary chronic total occlusion recanalization. Front Cardiovasc Med. 2022;9:895457. doi:10.3389/fcvm.2022.895457
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.