Back to Journals » Journal of Pain Research » Volume 19
Comparative Effectiveness of Non-Pharmacological Interventions for Pain and Quality of Life in Women with Endometriosis: A Systematic Review and Network Meta-Analysis
Authors Zheng X ![]() , Wang Y, Li H
, Wang Y, Li H ![]() , Zhang J, Liu J, Zheng X, Zhang J
, Zhang J, Liu J, Zheng X, Zhang J ![]() , Fan G, Sun Y, Li B
, Fan G, Sun Y, Li B ![]() , Jiao J, Zuo G, Fan X, She Y
, Jiao J, Zuo G, Fan X, She Y
Received 27 October 2025
Accepted for publication 29 January 2026
Published 20 February 2026 Volume 2026:19 577080
DOI https://doi.org/10.2147/JPR.S577080
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Xiaojun Zheng,1,* Yu Wang,1,* Haiping Li,1 Juncha Zhang,1 Jun Liu,1 Xihui Zheng,1 Jie Zhang,1 Guangya Fan,1 Yi Sun,1 Bingxian Li,1 Jingyi Jiao,1 Guang Zuo,1 Xisheng Fan,1,2 Yanfen She1,2
1College of Acupuncture-Moxibustion and Tuina, Hebei University of Chinese Medicine, Shijiazhuang City, Hebei Province, People’s Republic of China; 2Hebei International Joint Research Center for Dominant Diseases in Chinese Medicine and Acupuncture, Hebei University of Chinese Medicine, Shijiazhuang City, Hebei Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xisheng Fan, College of Acupuncture-Moxibustion and Tuina & Hebei International Joint Research Center for Dominant Diseases in Chinese Medicine and Acupuncture, Hebei University of Chinese Medicine, No. 3 Xingyuan Road, Shijiazhuang City, Hebei Province, 050200, People’s Republic of China, Email [email protected] Yanfen She, College of Acupuncture-Moxibustion and Tuina & Hebei International Joint Research Center for Dominant Diseases in Chinese Medicine and Acupuncture, Hebei University of Chinese Medicine, No. 3 Xingyuan Road, Shijiazhuang City, Hebei Province, 050200, People’s Republic of China, Email [email protected]
Background: Endometriosis is a chronic gynecological disorder characterized by pain and impaired quality of life (QoL). While pharmacological and surgical options exist, their limitations necessitate complementary strategies. The comparative effectiveness of non-pharmacological interventions remains uncertain.
Objective: This network meta-analysis (NMA) aimed to evaluate and rank the efficacy of non-pharmacological therapies for pain and QoL in women with endometriosis.
Methods: We systematically searched PubMed, Embase, CENTRAL, Web of Science, and CNKI from inception to August 31, 2025. Eligible randomized controlled trials (RCTs) compared structured non-pharmacological interventions—acupuncture (ACU), exercise (EXE), nutritional supplementation (NUT), physical therapy (PHY), or psychological interventions (PSY)—against conventional care (CON). Primary outcomes were pain (overall, pelvic, dysmenorrhea) and QoL; the secondary outcome was anxiety.
Results: Thirty-three RCTs involving 2323 women were included. For overall pain, PHY (SMD = − 1.44), ACU (SMD = − 1.27), and PSY (SMD = − 1.22) were significantly superior to CON, with PHY ranking highest (SUCRA = 74.4%). ACU was most effective for pelvic pain (SMD = − 4.53; SUCRA = 99.1%), while PHY was optimal for dysmenorrhea (SMD = − 1.30; SUCRA = 82.3%). Both ACU (SMD = 4.09) and PHY (SMD = 4.18) significantly improved QoL compared to CON. No statistically significant differences were observed among interventions for anxiety.
Conclusion: Non-pharmacological interventions, particularly PHY and ACU, provide significant benefits for pain and QoL in endometriosis, with subtype-specific advantages. These findings support their integration into multimodal management pathways.
Keywords: endometriosis, non-pharmacological interventions, pain management, quality of life, network meta-analysis, randomized controlled trials
Introduction
Endometriosis is a chronic, estrogen-dependent gynecological disorder characterized by the presence of endometrial-like tissue outside the uterine cavity, most commonly on the pelvic peritoneum, ovaries, and rectovaginal septum.1 It affects approximately 10% of women of reproductive age worldwide, and the prevalence is rising as diagnostic awareness and access to medical imaging improve. By 2030, it is projected that more than 200 million women globally will be affected.2 The most debilitating manifestations of endometriosis are pain-related symptoms, including chronic pelvic pain, dysmenorrhea, and dyspareunia, which often begin early in reproductive life and persist for decades. Pain not only impairs physical functioning but also disrupts psychological well-being and social relationships, leading to substantial reductions in health-related quality of life (QoL).3 Many women also report concomitant anxiety and depressive symptoms, which amplify the negative burden of pain and reduce adherence to treatment. Together, these sequelae place endometriosis among the leading causes of gynecological morbidity and generate significant social and economic costs. Addressing pain and improving QoL are therefore central goals of endometriosis management, underscoring the importance of effective, safe, and sustainable treatment strategies.
The current therapeutic armamentarium for endometriosis includes surgical excision or ablation of ectopic lesions, hormonal therapy such as gonadotropin-releasing hormone (GnRH) analogues or combined oral contraceptives, and analgesics including non-steroidal anti-inflammatory drugs (NSAIDs).3 While these interventions can relieve symptoms and delay recurrence, they are associated with considerable limitations. Hormonal agents may cause hypoestrogenic side effects, bone mineral density loss, mood disturbances, and long-term drug dependence.4 Surgery carries risks of complications, recurrence rates approaching 40% within five years, and potential negative effects on fertility.5 Analgesics often provide only transient symptom relief and are linked to gastrointestinal and renal adverse events with chronic use.6 These shortcomings highlight the need for complementary or alternative strategies. In recent years, non-pharmacological interventions have gained attention as viable approaches for symptom relief. Such strategies, which include acupuncture and moxibustion, structured exercise programs, nutritional supplementation, physical therapy modalities, and psychological interventions, are valued for their safety profile, patient acceptability, and potential to address both physical and psychological dimensions of the disease.7
Accumulating randomized controlled trials (RCTs) have provided preliminary evidence that non-pharmacological therapies can attenuate pain and enhance QoL in women with endometriosis. For instance, acupuncture has been reported to reduce dysmenorrhea and pelvic pain through neuromodulatory and anti-inflammatory mechanisms.8 Exercise interventions have demonstrated benefits in improving pain perception and mitigating fatigue, while dietary modifications and supplementation with specific nutrients have shown promise in regulating inflammatory pathways.9 Physical therapy, including manual techniques and pelvic floor rehabilitation, may relieve musculoskeletal contributions to pelvic pain, and psychological interventions such as cognitive-behavioral therapy or mindfulness-based stress reduction can alleviate anxiety and improve coping strategies.10 However, despite these promising findings, the evidence remains fragmented. Previous pairwise meta-analyses have synthesized data on single modalities, often with inconsistent conclusions, small sample sizes, and high heterogeneity.11 Furthermore, direct head-to-head comparisons between different non-pharmacological interventions are scarce, making it unclear which strategies offer the greatest overall benefits in terms of pain reduction, QoL improvement, and anxiety relief. As a result, clinicians and patients lack evidence-based guidance to prioritize among the diverse therapeutic options available.
Against this background, network meta-analysis (NMA) offers a rigorous methodological framework that enables the integration of both direct and indirect evidence to compare multiple interventions simultaneously. By ranking the relative effectiveness of different non-pharmacological strategies, NMA allows for a more comprehensive understanding of their comparative benefits.12 The objective of this study was to apply NMA to evaluate the effectiveness of acupuncture, exercise, nutritional supplementation, physical therapy, and psychological interventions for women with endometriosis. The findings aim to generate a robust evidence base that can guide clinical decision-making, inform patient-centered care, and support the integration of non-pharmacological therapies into comprehensive management pathways for endometriosis.
Methods
PROSPERO has registered the protocol (CRD420251166535). This systematic review and network meta-analysis was conducted and reported in accordance with the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the PRISMA extension for network meta-analyses.13 The completed PRISMA checklist is provided in Supplementary 1. Because this study involved secondary analysis of published data, institutional review board approval and informed consent were not required.
Data Sources and Search Strategy
A comprehensive search was performed in PubMed, Embase, the Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, and the China National Knowledge Infrastructure (CNKI) from inception to August 31, 2025. The search strategy combined controlled vocabulary (eg, MeSH and Emtree terms) and free-text words related to endometriosis, non-pharmacological interventions (eg, “physical activity”, “exercise”, “acupuncture”, “moxibustion”, “physical therapy”, “psychological”, “mindfulness”, “nutrition”), and randomized controlled trials. Detailed search algorithms for each database are provided in Supplementary 2. Reference lists of included studies and recent systematic reviews were hand-searched to ensure completeness.
Eligibility Criteria
Eligible studies were required to meet the following criteria: (a) participants were women with a clinical or surgical diagnosis of endometriosis, regardless of stage, symptom severity, or prior treatment; (b) interventions consisted of structured non-pharmacological therapies, including but not limited to acupuncture or moxibustion, exercise programs, nutritional supplements, physical therapy modalities, and psychological or behavioral therapies; (c) comparators included usual care, conventional pharmacological treatment, sham interventions, or an alternative non-pharmacological strategy; (d) outcomes reported at least one of the prespecified endpoints of interest, namely pain symptoms, health-related quality of life, or psychological well-being; and (e) study design was restricted to randomized controlled trials, including crossover RCTs. Exclusion criteria were as follows: (a) studies combining non-pharmacological interventions with pharmacological or surgical therapies without separable data, (b) non-randomized or observational designs, (c) case reports, reviews, protocols, conference abstracts, or animal and in vitro studies, (d) trials with insufficient outcome data (eg, missing mean and standard deviation or dichotomous counts) unless adequate information could be obtained from study authors after at least four attempts over a six-week period, and (e) duplicate publications of the same trial, in which case the most complete dataset was retained. Two reviewers independently screened all titles, abstracts, and full texts, with discrepancies resolved through discussion or adjudication by a third reviewer.
Data Extraction
Eligible studies were managed in EndNote X9 to remove duplicates. Two reviewers independently extracted study characteristics (author, year, country), participant demographics (age, sample size, body mass index), details of interventions and comparators (type, dose, frequency, duration), and reported outcomes (mean ± SD, sample size per arm, or dichotomous events). For continuous outcomes reported without variance measures, standard deviations were imputed using methods recommended in the Cochrane Handbook. Change scores were calculated as post-treatment minus baseline values, with standard deviations estimated using a correlation coefficient (R = 0.5) when not reported. All extracted data were cross-checked by a senior investigator.
Risk of Bias Assessment
Two reviewers independently assessed the risk of bias for each trial using the revised Cochrane Risk of Bias tool for randomized trials (RoB 2). The following domains were evaluated: randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selective reporting.14 Each domain was judged as low risk, some concerns, or high risk. Consensus was achieved through discussion, with arbitration by a third reviewer when necessary.
Intervention Coding
Interventions were categorized into five groups: acupuncture/moxibustion (ACU), exercise interventions (EXE), nutritional supplements (NUT), physical therapy (PHY), and psychological interventions (PSY). Usual care or conventional pharmacological therapy was coded as conventional care (CON).
The included interventions within each category encompassed a range of specific modalities. Specifically, PHY included pelvic floor rehabilitation (eg, Thiele massage), energy-based laser therapy, and neuromuscular electrical stimulation; ACU included manual acupuncture, electroacupuncture, moxibustion, and auricular acupressure; PSY included cognitive-behavioral therapy, mindfulness-based stress reduction, and acceptance and commitment therapy; NUT included vitamin D, omega-3 fatty acids, and combined vitamin C/E supplements, among others. The comparator, coded as conventional care (CON), consisted of standard medical management for endometriosis, typically involving symptomatic pharmacotherapy (eg, NSAIDs, hormonal treatments), routine clinical follow-up, and no additional structured non-pharmacological interventions.
Outcomes
The primary outcomes were pain symptoms and health-related quality of life. Pain outcomes included pelvic pain, dysmenorrhea, and dyspareunia, measured using validated scales such as the Visual Analog Scale (VAS), the Numerical Rating Scale (NRS), or the McGill Pain Questionnaire. Quality of life outcomes were assessed using generic instruments (eg, SF-36, EQ-5D) or disease-specific measures (eg, Endometriosis Health Profile-30).
The secondary outcome was anxiety, measured by validated tools such as the Hospital Anxiety and Depression Scale (HADS), the Beck Anxiety Inventory (BAI), or the State-Trait Anxiety Inventory (STAI).
Statistical Analysis
All analyses were performed in Stata version 17.0 (StataCorp, College Station, TX). A frequentist random-effects network meta-analysis was conducted using the “network” and “mvmeta” packages to estimate pooled effect sizes across interventions. Standardized mean differences (SMDs) with 95% confidence intervals (CIs) were calculated for continuous outcomes. Negative SMD values indicated beneficial effects for pain and psychological symptoms, while positive SMD values indicated beneficial effects for quality of life.
Statistical heterogeneity was assessed using the I² statistic, with thresholds of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. Prediction intervals were calculated to quantify the expected range of effects in future studies. Inconsistency between direct and indirect evidence was examined using design-by-treatment interaction models and node-splitting approaches.
Treatments were ranked according to their relative effectiveness using surface under the cumulative ranking (SUCRA) probabilities, where higher SUCRA values indicate greater likelihood of being among the most effective interventions. Small-study effects and publication bias were explored using comparison-adjusted funnel plots and Egger’s regression test, with p < 0.05 indicating potential bias.15 All statistical tests were two-sided, and p values less than 0.05 were considered statistically significant.
Results
Characteristics of Included Studies
A total of 3327 records were identified through the initial electronic searches. After removal of 1816 duplicates, 1511 articles underwent title and abstract screening. Of these, 1398 were excluded, leaving 113 full-text articles assessed for eligibility. Ultimately, 33 RCTs comprising 2323 patients with endometriosis were included in the systematic review and network meta-analysis (Figure 1).16–48
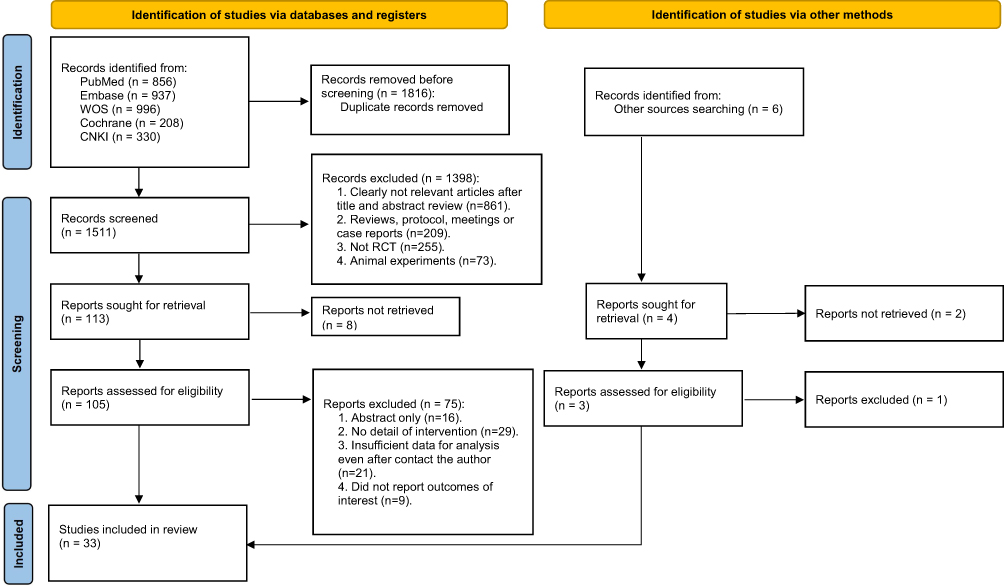 |
Figure 1 PRISMA flow diagram of study selection. |
The included trials were published between 2007 and 2025, with a median publication year of 2019. Sample sizes ranged from 18 to 200 participants, with a median of 64. The mean age of participants ranged from 17.8 to 37.6 years, with a median of 32.3 years.
With respect to interventions, 14 trials evaluated ACU, 2 evaluated EXE, 6 assessed NUT, 5 tested PHY, and 7 investigated PSY. Thirty-two trials included CON as the comparator. Detailed study characteristics are provided in Supplementary 3.
Results of Network Meta-Analysis
Pain
For pain, 21 RCTs including 1646 patients were analyzed. The network plot of direct comparisons and sample size distribution is shown in Figure 2a. According to SUCRA ranking (Figure 3a), the three most effective interventions for reducing pain were PHY (74.4%), ACU (69.8%), and PSY (65.7%), whereas CON ranked lowest (3.6%). As shown in Table 1, compared with CON, PHY (SMD = –1.44; 95% CI, –2.80 to –0.09), ACU (SMD = –1.27; 95% CI, –1.82 to –0.72), and PSY (SMD = –1.22; 95% CI, –2.11 to –0.32) significantly reduced pain scores.
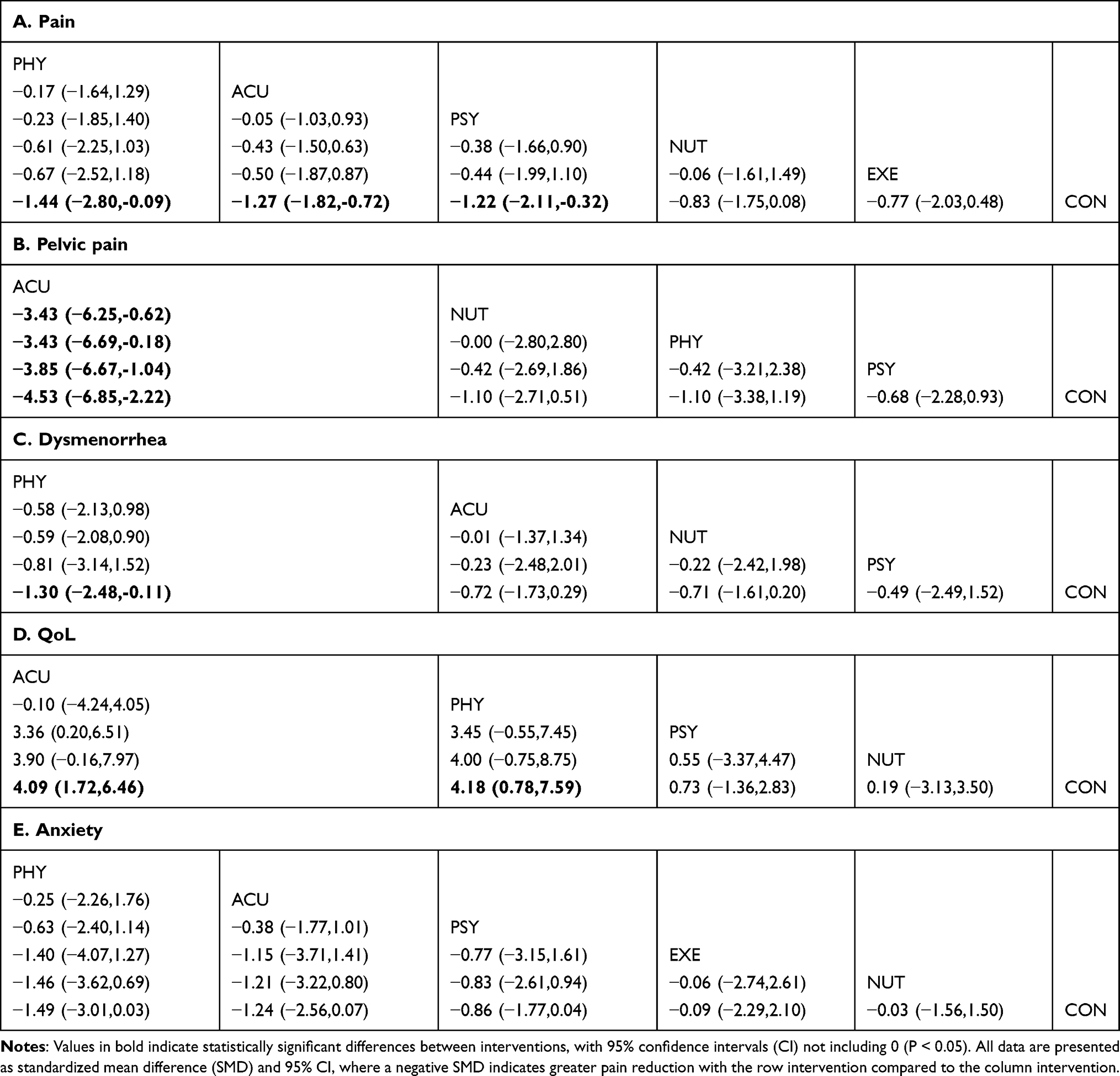 |
Table 1 League Table of Outcomes in Participants |
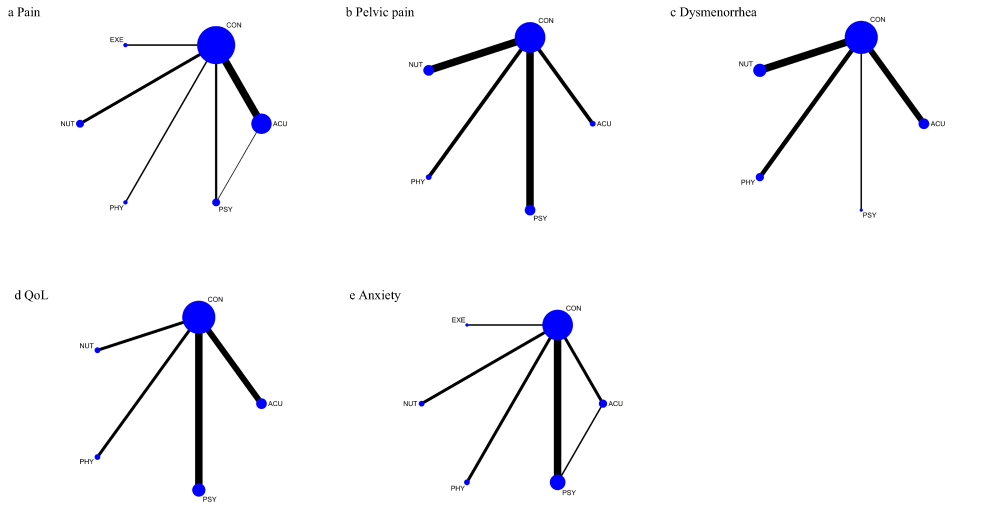 |
Figure 2 Network geometry of direct comparisons among non-pharmacological interventions for endometriosis. (a) Pain. (b) Pelvic pain. (c) Dysmenorrhea. (d) QoL. (e) Anxiety. |
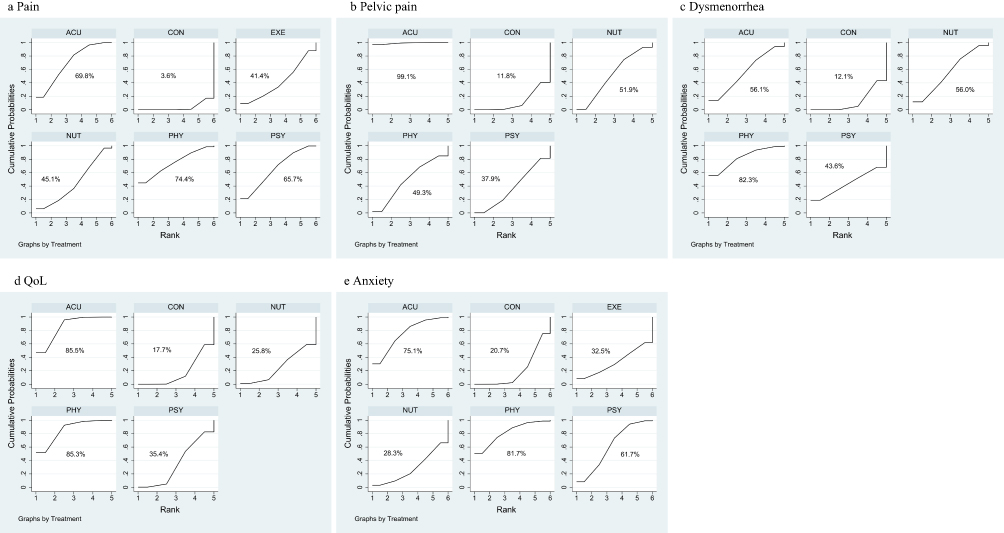 |
Figure 3 SUCRA rankings of non-pharmacological interventions for endometriosis. (a) Pain. (b) Pelvic pain. (c) Dysmenorrhea. (d) QoL. (e) Anxiety. |
Pelvic Pain
For pelvic pain, 11 RCTs with 689 patients were included. The network plot is shown in Figure 2b. Based on SUCRA values (Figure 3b), the top three interventions were ACU (99.1%), NUT (51.9%), and PHY (49.3%), with CON ranking lowest (11.8%). As summarized in Table 1, ACU significantly reduced pelvic pain compared with CON (SMD = –4.53; 95% CI, –6.85 to –2.22), PSY (SMD = –3.85; 95% CI, –6.67 to –1.04), PHY (SMD = –3.43; 95% CI, –6.69 to –0.18), and NUT (SMD = –3.43; 95% CI, –6.25 to –0.62).
Dysmenorrhea
For dysmenorrhea, 13 RCTs with 774 patients were analyzed. The network structure is illustrated in Figure 2c. SUCRA ranking (Figure 3c) indicated that PHY (82.3%), ACU (56.1%), and NUT (56.0%) were the three most effective interventions, whereas CON ranked lowest (12.1%). As shown in Table 1, PHY significantly reduced dysmenorrhea compared with CON (SMD = –1.30; 95% CI, –2.48 to –0.11).
QoL
For QoL, 11 RCTs involving 770 patients were included. The network plot is presented in Figure 2d. According to SUCRA ranking (Figure 3d), the three most effective interventions were ACU (85.5%), PHY (85.3%), and PSY (35.4%), with CON ranking lowest (17.7%). As detailed in Table 1, ACU (SMD = 4.09; 95% CI, 1.72 to 6.46) and PHY (SMD = 4.18; 95% CI, 0.78 to 7.59) significantly improved QoL compared with CON.
Anxiety
For anxiety, 11 RCTs with 864 patients were analyzed. The network structure is shown in Figure 2e. Based on SUCRA values (Figure 3e), PHY (81.7%), ACU (75.1%), and PSY (61.7%) ranked highest, while CON ranked lowest (20.7%). However, as indicated in Table 1, no statistically significant differences were observed among the intervention groups.
Risk of Bias and Publication Bias
Of the 33 RCTs, 20 were judged to be at low overall risk of bias, while 13 were judged to raise some concerns. With respect to individual domains, the risk of bias was low in 30 trials and of some concern in 3 trials for the randomization process; low in 26 trials and of some concern in 7 trials for deviations from intended interventions; low in 22 trials and of some concern in 11 trials for missing outcome data; low in all 33 trials for outcome measurement; and low in all 33 trials for selective outcome reporting (Supplementary 4).
Potential publication bias was assessed using funnel plots (Supplementary 5). Scatter plots showed varying degrees of asymmetry, suggesting possible publication bias. Specifically, funnel plots S5A through S5E revealed some asymmetry. However, Egger’s test indicated that all outcomes had p values greater than 0.05, suggesting no strong evidence of publication bias in the overall analyses.
Discussion
This network meta-analysis synthesized evidence from 33 randomized controlled trials involving 2323 women with endometriosis to evaluate the comparative effectiveness of non-pharmacological interventions on pain and health-related quality of life. Three principal findings emerged. First, PHY, ACU, and PSY significantly alleviated overall pain, with PHY demonstrating the greatest effect and ranking highest among all interventions, while ACU and PSY also showed consistent benefits, underscoring the superiority of multiple non-pharmacological therapies over conventional care in pain control. Second, intervention-specific advantages were observed in pain subtypes: ACU was most effective for pelvic pain, significantly outperforming CON, PSY, PHY, and NUT, whereas PHY ranked highest for dysmenorrhea and achieved significant reductions compared with CON, highlighting the targeted benefits of different modalities for distinct pain dimensions. Third, ACU and PHY significantly improved quality of life compared with CON, confirming their role in promoting broader physical and psychosocial recovery, whereas no significant differences were detected among interventions for anxiety despite favorable rankings for PHY, ACU, and PSY, indicating insufficient evidence for definitive conclusions regarding mental health outcomes. Collectively, these findings suggest that non-pharmacological interventions, particularly PHY and ACU, represent effective strategies for alleviating pain and enhancing quality of life in women with endometriosis, thereby offering valuable complementary options to conventional therapies.
Addressing overall pain is clinically pivotal in endometriosis because it aggregates nociceptive, neuropathic, and centralized components into a single patient-important endpoint that guides treatment selection and longitudinal monitoring. In this network meta-analysis, three non-pharmacological modalities were associated with meaningful reductions in overall pain, with PHY achieving the most favorable ranking, followed by ACU and PSY. This pattern refines the evidence base by positioning therapist-delivered physical therapy as the leading option for global pain relief while confirming consistent benefit for acupuncture and psychologically informed care. These findings are broadly aligned with prior randomized trials and pairwise syntheses that reported pain attenuation with acupuncture and with pelvic floor–focused rehabilitation, and small to moderate benefits from cognitive-behavioral and mindfulness-based programs in chronic pelvic pain populations.24,49 Our results extend this literature by comparing modalities within a single analytical framework, which clarifies their relative performance when direct head-to-head evidence is scarce. Notably, the superiority of PHY over usual care and its lead over other non-pharmacological options on the overall pain construct has not been consistently demonstrated in earlier pairwise analyses, likely because such designs could not leverage indirect comparisons across diverse interventions.50
The apparent advantage of PHY is biologically and mechanistically plausible, particularly given the diversity of approaches encompassed within this category. Pelvic floor physiotherapy incorporating Thiele massage targets hypertonic musculature and myofascial trigger points, thereby reducing peripheral nociceptive input and improving pelvic floor coordination.27 Hydrothermal and manual regimens, such as HAMMAM baths combined with Swedish or Kessa massage, likely enhance muscle relaxation, circulation, and autonomic balance, which collectively modulate pain sensitivity.19 Energy-based modalities, including pulsed Nd: YAG laser therapy and external high-frequency hyperthermia, act through photothermal and biothermal mechanisms to downregulate prostaglandin synthesis, attenuate neurogenic inflammation, and facilitate tissue repair.17 Neuromuscular electrical stimulation may mediate somatic and visceral pain modulation through dual mechanisms: improved neuromuscular activation and the engagement of endogenous opioid and serotonergic pathways.44 Together, these multimodal components simultaneously target musculoskeletal dysfunction, neuroimmune signaling, and central sensitization, providing a plausible rationale for PHY’s superior ranking in overall pain relief. By contrast, the analgesic effects of ACU are mediated primarily through activation of endogenous opioidergic and monoaminergic systems, modulation of spinal and supraspinal gating, and suppression of inflammatory mediators, consistent with its robust but slightly less dominant performance.51 PSY interventions, including cognitive-behavioral therapy and mindfulness-based stress reduction, improve coping capacity by reducing catastrophizing, enhancing self-efficacy, and modulating the affective and cognitive dimensions of pain, thereby addressing the psychosocial amplification of symptoms.52 Collectively, the convergence of these mechanistic pathways explains the observed hierarchy, with the multimodal and contact-intensive nature of PHY conferring broad musculoskeletal and neuroplastic benefits, while ACU and PSY provide complementary contributions through neuroimmune and cognitive-affective modulation.
Endometriosis pain is phenotypically heterogeneous, encompassing cyclic dysmenorrhea driven by uterine activity and prostaglandin excess, and noncyclic pelvic pain that often reflects deep infiltrating disease, adhesions, myofascial dysfunction, neuropathic features, and central sensitization.1 Within this context, the present analysis indicates a differential pattern of benefit: ACU shows a distinct advantage for pelvic pain, whereas PHY performs best for dysmenorrhea. This hierarchy refines prior evidence that tended to aggregate pain outcomes and thereby obscured phenotype-specific effects, and it offers a pragmatic basis for tailoring treatment to the dominant pain presentation. The observed superiority of ACU for pelvic pain is congruent with trials in chronic pelvic pain populations and is biologically plausible.49 Pelvic pain in endometriosis frequently involves segmental convergence of visceral and somatic afferents, neurogenic inflammation, and sustained spinal and supraspinal facilitation. Acupuncture plausibly engages descending inhibitory pathways, augments endogenous opioidergic and monoaminergic signaling, modulates glial activity, and attenuates local inflammatory mediators, which together reduce central gain and visceral hypersensitivity.53 The distribution of deep lesions and the prominence of referred and neuropathic descriptors in pelvic pain may therefore render it particularly responsive to neuromodulatory approaches that act across spinal and supraspinal levels rather than solely at the musculoskeletal interface.54 By contrast, dysmenorrhea is characteristically cyclical and is mediated by prostaglandin-induced uterine hypercontractility, transient uterine ischemia, and nociceptor sensitization.55 The components encompassed within PHY, including pelvic floor retraining, manual myofascial release, neuromuscular stimulation, and selected energy or hydrothermal modalities, are well positioned to interrupt these mechanisms. They can decrease pelvic floor hypertonicity and guarding, improve lumbopelvic coordination, enhance local perfusion, and downregulate neurogenic inflammatory signaling, thereby reducing cramping intensity and the amplification of nociceptive input during menses.56 This mechanistic profile aligns with the preferential benefit of PHY for dysmenorrhea observed in the network analysis. These phenotype-specific effects reconcile inconsistencies across earlier single-modality reviews by showing that modalities differ not only in overall analgesic potency but also in their mechanistic match to pain subtype. For patients with predominant noncyclic pelvic pain, ACU may offer the greatest likelihood of relief through central and neuroimmune modulation, whereas for those with menses-centered cramping, PHY appears optimally suited to normalize uterine–pelvic floor dynamics and attenuate prostaglandin-related hyperalgesia.
Beyond the reduction of pain, improving health-related QoL is a central therapeutic goal in endometriosis, as the disorder profoundly disrupts physical functioning, social participation, and emotional well-being. In this network meta-analysis, ACU and PHY emerged as the most effective modalities for enhancing QoL, significantly outperforming conventional care. This finding underscores the importance of non-pharmacological interventions not only in symptom relief but also in restoring broader aspects of patient health and daily functioning. Our results are in line with previous reports showing that acupuncture can improve well-being and role functioning in women with dysmenorrhea or chronic pelvic pain, and that physiotherapy-based approaches—particularly those targeting pelvic floor dysfunction and musculoskeletal imbalances—can alleviate functional limitations and improve life quality.57,58 However, earlier evidence was fragmented, often limited to single interventions or small samples, and failed to establish a comparative ranking of modalities. By integrating direct and indirect comparisons, the present analysis provides more robust evidence that ACU and PHY confer the greatest overall benefit for QoL. ACU may modulate neuroendocrine function, reduce systemic and local inflammation, and enhance autonomic balance, thereby improving both pain control and vitality.8 PHY, through a multimodal approach that combines pelvic floor retraining, manual release, neuromuscular stimulation, and adjunctive thermal or energy-based therapies, can improve musculoskeletal coordination, circulation, and central pain modulation, leading to reductions in fatigue and disability. Together, these physiological and functional benefits extend beyond pain relief to produce meaningful gains in overall quality of life. In addition to QoL, this analysis also considered anxiety, an outcome of high relevance given the bidirectional relationship between chronic pain and psychological distress. Although PHY (SUCRA = 81.7%), ACU (75.1%), and PSY (61.7%) ranked highest, none achieved statistically significant superiority over comparators. This discrepancy may be attributed to several factors: limited trial numbers, short intervention durations insufficient to alter entrenched affective symptoms, heterogeneity in anxiety measurement tools, and the complex biopsychosocial determinants of anxiety that extend beyond pain reduction. Consequently, while the trend toward benefit is encouraging, more rigorously designed and adequately powered studies are required to clarify the role of non-pharmacological therapies in addressing psychological comorbidities in endometriosis.
Building on these findings, clinicians can consider a phenotype-informed approach to selecting non-pharmacological therapies for endometriosis, guided by the relative rankings (SUCRA): For chronic pelvic pain, acupuncture (ACU) demonstrated the highest relative effectiveness (ranked first; SUCRA 99.1%). For dysmenorrhea, physical therapy (PHY) ranked highest, followed by acupuncture (ACU). For overall pain management, both physical therapy (PHY) and acupuncture (ACU) were superior to conventional care, with PHY having a slight edge in ranking. These interventions can be prioritized based on the patient’s predominant pain complaint. Psychological interventions (PSY) also showed consistent benefits for pain reduction and can be integrated to address the psychosocial dimensions of chronic pain. The current evidence base suggests that nutritional supplementation (NUT) and structured exercise (EXE) may play a more supportive role, particularly for managing comorbid symptoms such as fatigue or mood disturbance, alongside first-line therapies.
The practical value and clinical significance of this study lie in its ability to guide patient-centered and evidence-informed care in endometriosis. By establishing a comparative hierarchy of non-pharmacological interventions, this analysis provides clinicians with concrete evidence that PHY and ACU are most effective for global pain and QoL outcomes, while also highlighting the phenotype-specific advantages of ACU for pelvic pain and PHY for dysmenorrhea. These findings can inform individualized treatment strategies, allowing physicians to select interventions aligned with each patient’s predominant symptom profile, tolerance, and treatment goals. Importantly, such non-pharmacological modalities can be integrated into multimodal care pathways, reducing reliance on long-term pharmacotherapy or repeated surgery, both of which are associated with side effects, recurrence, and diminished quality of life. The results also underscore the relevance of embedding physical therapy and acupuncture into standard gynecological practice and health policy frameworks, particularly in contexts where access to pharmacological or surgical care may be limited. In this way, the study supports a paradigm shift toward broader adoption of complementary and integrative medicine strategies as core components of comprehensive endometriosis management.
This study also has several strengths and limitations that merit consideration. One strength is the comprehensive scope of evidence synthesis: by including 33 randomized trials and applying a frequentist network meta-analysis framework, this study integrated both direct and indirect comparisons to generate a coherent ranking of multiple non-pharmacological modalities. A second strength is the differentiation of outcomes by pain subtype (global pain, pelvic pain, dysmenorrhea), QoL, and anxiety, which allowed for the identification of phenotype-specific intervention effects and refined clinical applicability.
Nevertheless, several limitations must be acknowledged. First, although 33 RCTs were included, the sample size of individual trials was often modest, and some interventions (such as EXE and NUT) were represented by only a few studies, reducing statistical power and precision for those nodes. Second, the analysis was conducted at the level of broad intervention categories. While this approach allowed for a comprehensive comparison across major non-pharmacological strategies, it necessarily combines diverse sub-modalities (eg, pelvic floor therapy and laser therapy within PHY; manual acupuncture and electroacupuncture within ACU). This clinical heterogeneity may obscure the differential efficacy of specific therapeutic techniques. Future trials directly comparing standardized protocols within these categories are warranted to refine evidence-based clinical recommendations. Third, the unusually large effect sizes for select pain outcomes—most notably acupuncture for pelvic pain (SMD = −4.53; 95% CI, −6.85 to −2.22)—require cautious interpretation. These estimates may be inflated by heterogeneity in pain measurement scales (eg, Visual Analog Scale [VAS], Numerical Rating Scale [NRS], McGill Pain Questionnaire) with differing scoring criteria and sensitivity, as well as potential selective reporting of positive results in small-scale trials. While funnel plot and Egger’s test (all p > 0.05) showed no strong statistical evidence of publication bias, this risk cannot be fully excluded. Fourth, the assessment of anxiety was constrained by heterogeneous measurement tools, short follow-up durations, and underreporting in several trials, which may explain the lack of statistically significant findings despite favorable SUCRA rankings. Fifth, the robustness of our findings varies by outcome and intervention. The conclusions for ACU on pelvic pain and for PHY on overall pain and dysmenorrhea are based on a relatively larger body of evidence, though still limited by the sample sizes and heterogeneity noted above. In contrast, findings for EXE, NUT, and all interventions on anxiety are based on fewer and often smaller trials, leading to less precise estimates and greater uncertainty. These limitations indicate that while the present study provides important comparative insights, further large-scale, rigorously designed RCTs with standardized intervention protocols and longer follow-up are needed to confirm and extend these conclusions.
Conclusion
This network meta-analysis demonstrates that non-pharmacological interventions provide clinically meaningful benefits for women with endometriosis. PHY, ACU, and PSY significantly reduced overall pain, with PHY showing the greatest effect. Subtype-specific analyses revealed that ACU was most effective for pelvic pain, whereas PHY was superior for dysmenorrhea, highlighting the importance of phenotype-tailored treatment. In addition, both ACU and PHY significantly improved quality of life, confirming their broader value beyond symptom relief, while evidence for anxiety reduction remained inconclusive. These findings support the integration of PHY and ACU into multimodal care pathways as effective complementary options to conventional therapy.
Data Sharing Statement
Data are available from the first author upon reasonable request.
Acknowledgments
We thank all researchers and study participants for their contributions to this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (No. 82474395), the Hebei Province Yan Zhao Golden Talent Platform Key Talent Program (No. HJZD202505), the Hebei Provincial Department of Education Youth Fund Project (No. QN2024056) and the Graduate Innovation Fund of Hebei University of Chinese Medicine (No. XCXZZBS2025027)
Disclosure
The authors report no conflicts of interest in this work.
References
1. Becker CM, Bokor A, Heikinheimo O, et al. ESHRE guideline: endometriosis. Hum Reprod Open. 2022;2022(2):hoac009. doi:10.1093/hropen/hoac009
2. Tang WZ, Cai QY, Huang KJ, et al. The global burden of polycystic ovary syndrome, endometriosis, uterine fibroids, cervical cancer, uterine cancer, and ovarian cancer from 1990 to 2021. BMC Public Health. 2025;25(1):1774. doi:10.1186/s12889-025-22881-3
3. Horne AW, Missmer SA. Pathophysiology, diagnosis, and management of endometriosis. BMJ. 2022;379:e070750. doi:10.1136/bmj-2022-070750
4. Piriyev E, Schiermeier S, Römer T. Hormonal treatment of endometriosis: A narrative review. Pharmaceuticals. 2025;18(4):588. doi:10.3390/ph18040588
5. Zakhari A, Delpero E, McKeown S, Tomlinson G, Bougie O, Murji A. Endometriosis recurrence following post-operative hormonal suppression: a systematic review and meta-analysis. Hum Reprod Update. 2021;27(1):96–13. doi:10.1093/humupd/dmaa033
6. Lambourg E, Colvin L, Guthrie G, Walker H, Bell S. Analgesic use and associated adverse events in patients with chronic kidney disease: a systematic review and meta-analysis. Br J Anaesth. 2022;128(3):546–561.
7. Li H, Wang X, Gao Y, et al. Acupuncture and related therapies for endometriosis: a network meta-analysis of randomized controlled trials. J Pain Res. 2024;17:3197–3216. doi:10.2147/JPR.S488343
8. Chiarle G, Allais G, Sinigaglia S, et al. Acupuncture for pain and pain-related disability in deep infiltrating endometriosis. Front Pain Res. 2024;5:1279312. doi:10.3389/fpain.2024.1279312
9. Salinas-Asensio MDM, Álvarez-Salvago F, Mundo-López A, et al. Changes in fatigue, health-related fitness, sleep quality, mental health, gastrointestinal complaints and sexual function after a multimodal supervised therapeutic exercise program in women with endometriosis unresponsive to conventional therapy: a secondary analysis of a randomized controlled trial. Eur J Obstet Gynecol Reprod Biol. 2025;312:114083. doi:10.1016/j.ejogrb.2025.114083
10. Can G, Amorim Das Virgens IP, Fehér B, et al. Physiotherapy for endometriosis-associated pelvic pain: a systematic review and meta-analysis. Pain Med. 2025;25:95–103.
11. Xie M, Qing X, Huang H, et al. The effectiveness and safety of physical activity and exercise on women with endometriosis: a systematic review and meta-analysis. PLoS One. 2025;20(2):e0317820. doi:10.1371/journal.pone.0317820
12. Leucht S, Chaimani A, Cipriani AS, Davis JM, Furukawa TA, Salanti G. Network meta-analyses should be the highest level of evidence in treatment guidelines. Eur Arch Psychiatry Clin Neurosci. 2016;266(6):477–480. doi:10.1007/s00406-016-0715-4
13. Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160.
14. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
15. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
16. Wayne PM, Kerr CE, Schnyer RN, et al. Japanese-style acupuncture for endometriosis-related pelvic pain in adolescents and young women: results of a randomized sham-controlled trial. J Pediatr Adolesc Gynecol. 2008;21(5):247–257. doi:10.1016/j.jpag.2007.07.008
17. Thabet AAE, Alshehri MA. Effect of pulsed high-intensity laser therapy on pain, adhesions, and quality of life in women having endometriosis: a randomized controlled trial. Photomed Laser Surg. 2018;36(7):363–369. doi:10.1089/pho.2017.4419
18. Rubi-Klein K, Kucera-Sliutz E, Nissel H, et al. Is acupuncture in addition to conventional medicine effective as pain treatment for endometriosis? A randomised controlled cross-over trial. Eur J Obstet Gynecol Reprod Biol. 2010;153(1):90–93. doi:10.1016/j.ejogrb.2010.06.023
19. Rodríguez-Ruiz Á, Arcos-Azubel C, Ruiz-Pérez M, et al. The benefits of an integral HAMMAM experience combining hydrotherapy and Swedish massage on pain, subjective well-being and quality of life in women with endometriosis-related chronic pelvic pain: a randomized controlled trial. Medicina. 2024;60(10). doi:10.3390/medicina60101677.
20. Nodler JL, DiVasta AD, Vitonis AF, et al. Supplementation with vitamin D or ω-3 fatty acids in adolescent girls and young women with endometriosis (SAGE): a double-blind, randomized, placebo-controlled trial. Am J Clin Nutr. 2020;112(1):229–236. doi:10.1093/ajcn/nqaa096
21. Moreira MF, Gamboa OL, Pinho Oliveira MA. A single-blind, randomized, pilot study of a brief mindfulness-based intervention for the endometriosis-related pain management. Eur J Pain. 2022;26(5):1147–1162. doi:10.1002/ejp.1939
22. Meissner K, Schweizer-Arau A, Limmer A, et al. Psychotherapy with somatosensory stimulation for endometriosis-associated pain: a randomized controlled trial. Obstet Gynecol. 2016;128(5):1134–1142. doi:10.1097/AOG.0000000000001691
23. Mehdizadehkashi A, Rokhgireh S, Tahermanesh K, Eslahi N, Minaeian S, Samimi M. The effect of vitamin D supplementation on clinical symptoms and metabolic profiles in patients with endometriosis. Gynecol Endocrinol. 2021;37(7):640–645. doi:10.1080/09513590.2021.1878138
24. Hansen KE, Brandsborg B, Kesmodel US, et al. Psychological interventions improve quality of life despite persistent pain in endometriosis: results of a 3-armed randomized controlled trial. Qual Life Res. 2023;32(6):1727–1744. doi:10.1007/s11136-023-03346-9
25. Gonçalves AV, Barros NF, Bahamondes L. The practice of hatha yoga for the treatment of pain associated with endometriosis. J Altern Complement Med. 2017;23(1):45–52. doi:10.1089/acm.2015.0343
26. Farshi N, Hasanpour S, Mirghafourvand M, Esmaeilpour K. Effect of self-care counselling on depression and anxiety in women with endometriosis: a randomized controlled trial. BMC Psychiatry. 2020;20(1):391. doi:10.1186/s12888-020-02795-7
27. Del Forno S, Arena A, Pellizzone V, et al. Assessment of levator hiatal area using 3D/4D transperineal ultrasound in women with deep infiltrating endometriosis and superficial dyspareunia treated with pelvic floor muscle physiotherapy: randomized controlled trial. Ultrasound Obstet Gynecol. 2021;57(5):726–732. doi:10.1002/uog.23590
28. Amirsalari S, Behboodi Moghadam Z, Taghizadeh Z, et al. The effect of garlic tablets on the endometriosis-related pains: a randomized placebo-controlled clinical trial. Evid Based Complement Alternat Med. 2021;2021:5547058. doi:10.1155/2021/5547058
29. Amini L, Chekini R, Nateghi MR, et al. The effect of combined Vitamin C and Vitamin E supplementation on oxidative stress markers in women with endometriosis: a randomized, triple-blind placebo-controlled clinical trial. Pain Res Manag. 2021;2021:5529741. doi:10.1155/2021/5529741
30. Almassinokiani F, Khodaverdi S, Solaymani-Dodaran M, Akbari P, Pazouki A. Effects of Vitamin D on endometriosis-related pain: a double-blind clinical trial. Med Sci Monit. 2016;22:4960–4966. doi:10.12659/MSM.901838
31. Zhao L, Wu H, Zhou X, Wang Q, Zhu W, Chen J. Effects of progressive muscular relaxation training on anxiety, depression and quality of life of endometriosis patients under gonadotrophin-releasing hormone agonist therapy. Eur J Obstet Gynecol Reprod Biol. 2012;162(2):211–215. doi:10.1016/j.ejogrb.2012.02.029
32. Lutfi M, Dalleck LC, Drummond C, et al. A single session of a digital health tool-delivered exercise intervention may provide immediate relief from pelvic pain in women with endometriosis: a pilot randomized controlled study. Int J Environ Res Public Health. 2023;20(3):1665. doi:10.3390/ijerph20031665
33. Cobellis L, Castaldi MA, Giordano V, et al. Effectiveness of the association micronized N-Palmitoylethanolamine (PEA)-transpolydatin in the treatment of chronic pelvic pain related to endometriosis after laparoscopic assessment: a pilot study. Eur J Obstet Gynecol Reprod Biol. 2011;158(1):82–86. doi:10.1016/j.ejogrb.2011.04.011
34. Jf N. Clinical study on moxibustion combined with auricular acupressure and routine therapy for dysmenorrhea caused by endometriosis. Chin J Inf Trad Chin Med. 2020;31(8):45–49.
35. Fang LNX, Li HJ, Zhang RP, Xu GL. Application of moxibustion combined with auricular acupressure in patients with endometriosis-associated dysmenorrhea. Qilu Nurs J. 2024;30(23):139–141.
36. Sun Q. Clinical study on Bo’s abdominal acupuncture plus infrared therapy for dysmenorrhea due to endometriosis. Shenzhen J Integr Trad Chin West Med. 2012;22:80–83.
37. Liu YL, Yang GG, Yang LJ. Clinical observation of electro-acupuncture combined with TDP for endometriosis dysmenorrhea. J Clin Acupuncture Moxibustion. 2013;29(4):72–74.
38. Sun ZL, Jin YB. Clinical observation of otopuncture for algomenorrhea caused by endometriosis: a report of 32 cases. Zhejiang J Integr Trad West Med. 2007;17(12):738–740.
39. Du J, Wu D, Yu ZH, Huang SY, Liu KL, Cong HF. Therapeutic effect and mechanism of red-hot filiform needling combined with needle-warming moxibustion for dysmenorrhea in cold-coagulation blood-stasis endometriosis. J Clin Acupuncture Moxibustion. 2025;41(4):45–49.
40. Sun KF, He MR, Ou YF, et al. Clinical study of electro-acupuncture for EMs dysmenorrhea based on the VEGF/VEGFR pathway. J Clin Acupuncture Moxibustion. 2021;37:11–16.
41. Niu XX, Niu Q, Luo XM. Clinical observation of moxibustion and herbal therapy for dysmenorrhea in 61 endometriosis patients. Lishizhen Med Mat Medica Res. 2000;25(4):878–879.
42. Wang B, Su XN, Qin LH, Han RG, Yan X, Ni CP. Effect of cognitive behavioral intervention on infertile patients with endometriosis undergoing IVF-ET. Chin J Fam Plan. 2019;27:423–426.
43. Chen YY. Therapeutic effect of extracorporeal high-frequency hyperthermia instrument on dysmenorrhea caused by endometriosis. China Med Device Inform. 2023;29(18):136–138.
44. Qu Y. Effect of neuromuscular electrical stimulation on pain associated with endometriosis. Contemp Med. 2022;28(18):125–127.
45. Sun KF, He MR, Ou YF, et al. Clinical observation of acupuncture for endometriosis dysmenorrhea of cold-coagulation blood-stasis pattern. J Liaoning Univ Trad Chin Med. 2021;23(10):100–104.
46. Chen M, Zhang H, Li J. Acupuncture combined with acupoint sticking for endometriosis dysmenorrhea. Chin Acupuncture Moxibustion. 2010;30(9):728.
47. Shen Q, Lu J. Clinical observation of acupuncture-moxibustion for endometriosis. Shanghai J Acupuncture Moxibustion. 2017;36(6):711–714.
48. Li XY. Effect of mindfulness training on marital quality in young endometriosis patients. Heilongjiang J Trad Chinese Med. 2019;48(2):38–41.
49. Lin KY, Chang YC, Lu WC, Kotha P, Chen YH, Tu CH. Analgesic efficacy of acupuncture on chronic pelvic pain: a systemic review and meta-analysis study. Healthcare. 2023;11(6). doi:10.3390/healthcare11060830
50. Starzec-Proserpio M, Frawley H, Bø K, Morin M. Effectiveness of nonpharmacological conservative therapies for chronic pelvic pain in women: a systematic review and meta-analysis. Am J Obstet Gynecol. 2025;232(1):42–71. doi:10.1016/j.ajog.2024.08.006
51. Zhang Q, Zhou M, Huo M, et al. Mechanisms of acupuncture-electroacupuncture on inflammatory pain. Mol Pain. 2023;19:17448069231202882. doi:10.1177/17448069231202882
52. Windgassen S, Moss-Morris R, Chilcot J, Sibelli A, Goldsmith K, Chalder T. The journey between brain and gut: a systematic review of psychological mechanisms of treatment effect in irritable bowel syndrome. Br J Health Psychol. 2017;22(4):701–736. doi:10.1111/bjhp.12250
53. Lv Q, Wu F, Gan X, et al. The involvement of descending pain inhibitory system in electroacupuncture-induced analgesia. Front Integr Neurosci. 2019;13:38. doi:10.3389/fnint.2019.00038
54. Hao D, Yurter A, Chu R, et al. Neuromodulation for management of chronic pelvic pain: a comprehensive review. Pain Ther. 2022;11(4):1137–1177.
55. Kirsch E, Rahman S, Kerolus K, et al. Dysmenorrhea, a narrative review of therapeutic options. J Pain Res. 2024;17:2657–2666. doi:10.2147/JPR.S459584
56. Grinberg K, Weissman-Fogel I, Lowenstein L, Abramov L, Granot M. How does myofascial physical therapy attenuate pain in chronic pelvic pain syndrome? Pain Res Manag. 2019;2019:6091257. doi:10.1155/2019/6091257
57. Su Y, Ji R, Zheng X, et al. Efficacy and safety of acupuncture-related therapies in symptomatic endometriosis: a systematic review and network meta-analysis. Arch Gynecol Obstet. 2025;311(3):697–714. doi:10.1007/s00404-025-07979-8
58. Bittelbrunn CC, de Fraga R, Martins C, et al. Pelvic floor physical therapy and mindfulness: approaches for chronic pelvic pain in women-a systematic review and meta-analysis. Arch Gynecol Obstet. 2023;307(3):663–672. doi:10.1007/s00404-022-06514-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Qualitative Study of Migraine Headache Experience in Patients with Patent Foramen Ovale Based on the Symptom Management Theory
Li M, Feng M, Li M, Wei J, Li S, Zhang N, Li Q, Song R, Li H
Patient Preference and Adherence 2025, 19:2363-2375
Published Date: 10 August 2025
Discussion on the Application of Mindfulness Therapy in the Treatment of Diabetic Peripheral Neuropathy: A Narrative Review
Fan Q, Yu S, Sun X, Dong Y, Chen Y, Jia L
Psychology Research and Behavior Management 2025, 18:1729-1747
Published Date: 12 August 2025
Analgesic Efficacy and Tolerability of Amitriptyline versus Mianserin in Chronic Low Back Pain: A Randomised, Double-Blind, Controlled Pilot Trial
Wangnamthip S, Eiamtanasate S, Saisavoey N, Sathienluckana T, Suthisiltham L, Panchoowong S, Tipapakoon I, Euasobhon P, Jensen MP, Srirojanakul W
Journal of Pain Research 2025, 18:6829-6847
Published Date: 17 December 2025
Personalized Multimodal and Opioid-Sparing Analgesia for Postoperative Pain Management: Enhancing Recovery and Addressing the Post-Discharge Gap
Sezerano ML, Niyonkuru E
Journal of Pain Research 2026, 19:597049
Published Date: 16 April 2026
Executive Functions Mediate Between Endometriosis Burden and Women’s Daily Life
Khatib S, Hassan H, Abd Elgani S, Reiss A, Engel -Yeger B
International Journal of Women's Health 2026, 18:606990
Published Date: 3 June 2026