Back to Journals » Journal of Pain Research » Volume 19
Personalized Multimodal and Opioid-Sparing Analgesia for Postoperative Pain Management: Enhancing Recovery and Addressing the Post-Discharge Gap
Authors Sezerano ML, Niyonkuru E ![]()
Received 19 January 2026
Accepted for publication 26 March 2026
Published 16 April 2026 Volume 2026:19 597049
DOI https://doi.org/10.2147/JPR.S597049
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Karina Gritsenko
Marie Louise Sezerano,1 Emery Niyonkuru2
1Department of Clinical Sciences (Pharmacy), National Institute of Public Health, Bujumbura, Burundi; 2Department of Clinical Sciences (Anesthesiology), National Institute of Public Health, Bujumbura, Burundi
Correspondence: Emery Niyonkuru, Department Clinical Sciences (Anesthesiology), National Institute of Public Health, Bujumbura, Burundi, Tel + 25768094876, Email [email protected]
Abstract: Postoperative pain remains a persistent clinical challenge affecting more than 80% of surgical patients, driving prolonged hospitalization, delayed recovery, and progression to chronic postsurgical pain. Opioid-centered analgesia, despite its historical primacy, is constrained by dependence, tolerance, opioid-induced hyperalgesia, and a critical post-discharge prescribing gap in which prescribed quantities consistently exceed actual patient consumption, perpetuating avoidable harm without proportional improvement in outcomes. Enhanced Recovery After Surgery protocols emphasize multimodal, opioid-sparing strategies combining pharmacologic agents including NSAIDs, acetaminophen, gabapentinoids, ketamine, dexmedetomidine, and intravenous lidocaine with neuraxial and peripheral nerve blocks and non-pharmacologic interventions including cognitive-behavioral therapy, physical rehabilitation, acupuncture, and digital therapeutics. Current evidence identifies NSAIDs combined with dexamethasone or regional anesthesia as delivering the greatest opioid-sparing efficacy, while emerging precision-based approaches incorporating pharmacogenomic-guided prescribing, machine learning–based pain prediction, and wearable monitoring platforms offer transformative opportunities for individualized perioperative analgesic optimization. Significant gaps persist including heterogeneity in multimodal regimen combinations, inconsistent outcome measures, limited post-discharge standardization, and insufficient long-term data on chronic postsurgical pain prevention and functional recovery across diverse surgical populations. Future research must prioritize procedure-specific, standardized, and pharmacogenomically informed multimodal protocols integrating technological innovations to optimize recovery, minimize opioid-related risks, and ensure sustainable, patient-centered perioperative pain management.
Keywords: postoperative pain, multimodal analgesia, opioid sparing, chronic postsurgical pain, regional anesthesia, pharmacogenomics, enhanced recovery after surgery, perioperative pain management, opioids exposure
Introduction
Postoperative pain is among the most prevalent and poorly resolved problems in modern surgical medicine. With over 280 million procedures performed globally each year,1 the incidence of moderate-to-severe postoperative pain ranges from 30% to 80% depending on procedure type and pain definition,2 and persists after hospital discharge in 31% to 58% of patients.3 The failure to achieve adequate analgesia carries consequences that extend far beyond subjective discomfort—driving thromboembolic events, respiratory compromise, impaired wound healing, and psychological sequelae that collectively prolong hospitalization and worsen recovery.4,5 Understood within a biopsychosocial framework,6,7 postoperative pain is not a discrete physiologic signal but a multidimensional experience, and its management demands an equally multidimensional response.
Opioids, long the default analgesic cornerstone, have proven insufficient to that task. Beyond well-established risks of dependence and opioid-induced hyperalgesia,8 up to 80% of postoperative patients experience opioid-attributable cognitive impairment, fall risk, or rehabilitative delay,9 while NSAIDs—though adjunctively useful—carry prohibitive risk profiles in elderly and comorbid populations.10 These limitations have appropriately accelerated the shift toward multimodal, opioid-sparing strategies.11
Yet the promise of multimodal analgesia10–13 has outpaced its evidence base. Of 84 conceivable pharmacologic combinations, only acetaminophen plus NSAIDs is formally recommended14—and even this pairing is not without fault: preemptive acetaminophen failed to reduce opioid consumption in total knee arthroplasty,15 and intravenous formulations add little over oral equivalents.16 Optimal agent selection, dosing, and sequencing remain undefined,17 compounded by subjective pain assessment, variable clinical practice, and inadequate structured training in modern analgesic techniques.18 In cardiac surgery specifically, multimodal regimens remain so poorly characterized that nearly 30% of patients report persistent pain at one year.19
Regional techniques, particularly peripheral nerve blocks, offer meaningful short-term opioid sparing but are constrained by rebound phenomena, technical demands, and local anesthetic systemic toxicity risk.20–25 More fundamentally, they do not reliably interrupt the progression to chronic postsurgical pain (CPSP)—a transition that is far more common than clinical practice acknowledges. Post-thoracotomy CPSP persists in 57% of patients at three months and 47% at six months;26 after lung resection and knee arthroplasty, prevalence reaches 10% and 28% respectively at three months.27 Neuropathic features, preoperative pain, anxiety, and depression independently predict this transition,28 underscoring that acute and chronic pain exist on a continuum requiring prospective, risk-stratified intervention—not reactive treatment. The economic stakes are proportionate: in 2021, chronic pain affected an estimated 65.8 million U.S. adults, imposing a total societal burden of $722.8 billion in medical costs and lost productivity;29 earlier estimates place annual costs at $560–$635 billion in 2010 dollars,30 surpassing the combined burden of heart disease, cancer, and diabetes, with direct neuropathic pain syndromes alone generating nearly $42,000 per patient in annualized expenses.31 These gaps expose the absence of an integrative synthesis that evaluates the full spectrum of pharmacologic, regional, and non-pharmacologic analgesic strategies across their mechanisms, safety limitations, and clinical interactions — with attention to long-term outcomes including chronic postsurgical pain and opioid dependence. Accordingly, this review evaluates each analgesic modality and its role within multimodal frameworks, identifies procedure-specific evidence and critical gaps, and proposes evidence-informed, opioid-sparing analgesic principles aimed at supporting durable recovery across diverse surgical populations.
Epidemiology of Opioid Use and Opioid-Related Harm in the Perioperative Context
The liberalization of opioid prescribing for noncancer pain in the 1990s marked a pivotal inflection point in the contemporary opioid crisis. Converging forces—including relaxed state prescribing regulations, the introduction of pain management standards by accrediting bodies such as The Joint Commission, the designation of pain as the “fifth vital sign,” and aggressive pharmaceutical marketing—normalized long-term opioid therapy and expanded prescribing across clinical settings.32–34 These shifts coincided with a near fourfold increase in U.S. sales of oxycodone hydrochloride and methadone hydrochloride between 1997 and 2002, during which accidental drug overdose emerged as the second leading cause of unintentional death.35 Despite representing only 5% of the global population, the United States consumed 99% of hydrocodone bitartrate and 83% of oxycodone worldwide.34 By 2010, opioid distribution reached 710 mg morphine sulfate equivalents per capita—sufficient to supply every adult with 5 mg of hydrocodone every six hours for 45 days—underscoring the extraordinary scale of opioid availability preceding the escalation of fatal overdose and heroin use across both urban and rural communities.34,35
More than two decades later, opioid-related harm remains profound. In 2023, approximately 105,000 overdose deaths occurred in the United States, nearly 80,000 (76%) involving opioids.36 Although opioid-related mortality declined modestly (4%) compared with 2022, deaths remain nearly tenfold higher than in 1999.36 Trends varied by opioid class, with reductions in deaths attributed to prescription opioids, heroin, and synthetic opioids other than methadone, including illicitly manufactured fentanyl.36
However, these aggregate improvements obscure a critical epidemiologic shift: in some jurisdictions, nearly half of overdose deaths involved concurrent opioid and stimulant use, highlighting the growing complexity of polysubstance exposure that challenges traditional opioid-centric interventions.37
Opioid-related mortality also demonstrates marked heterogeneity across settings and populations. In Illinois, analysis of 2,833 opioid overdose deaths between 2017 and 2018 revealed that most fatalities occurred outside healthcare facilities, predominantly in private residences.38 Hospital-based deaths were associated with prior overdose and bystander presence, emphasizing the importance of access to treatment, decriminalization strategies, and supervised consumption environments.38 Importantly, declining opioid prescribing alone has not translated into proportional reductions in mortality. Between 2010 and 2015, U.S. opioid prescribing fell substantially, yet overdose deaths increased by 63%.39 Among opioid-related decedents in Illinois, nearly one-third had not filled an opioid prescription in the preceding six years and were disproportionately Black, Hispanic, and urban residents.39 These individuals were more likely to die from heroin or fentanyl analogues and less likely to have diagnosed opioid use disorder or access to buprenorphine treatment, underscoring structural inequities and the limits of prescription-focused mitigation strategies.39 Within this broader epidemiologic landscape, surgical care represents a critical and underappreciated gateway to opioid exposure. Opioid use following surgery is associated with persistent use, opioid use disorder, and other serious adverse outcomes, yet postoperative opioid trajectories vary widely by procedure and patient characteristics.40 For example, patients undergoing cervical laminectomy with fusion demonstrated higher six-month opioid use than those receiving laminoplasty in a single-surgeon cohort, although this association was not replicated in national datasets, highlighting the influence of contextual and provider-level factors.41
In orthopedic populations, preoperative opioid exposure and advanced joint pathology—but not surgical technique—were the primary predictors of prolonged postoperative use.42,43 Conversely, in colorectal surgery, individualized multimodal care bundles incorporating tailored opioid regimens, scheduled gabapentinoids, and clonidine rescue reduced postoperative opioid consumption by more than two-thirds, demonstrating the modifiability of postoperative exposure when care is personalized.44 Nevertheless, high-risk procedures such as cervical discectomy and fusion continue to be associated with substantial postoperative opioid prescribing and prolonged use (Figure 1), reinforcing the need for procedure-specific and patient-specific risk mitigation strategies.45
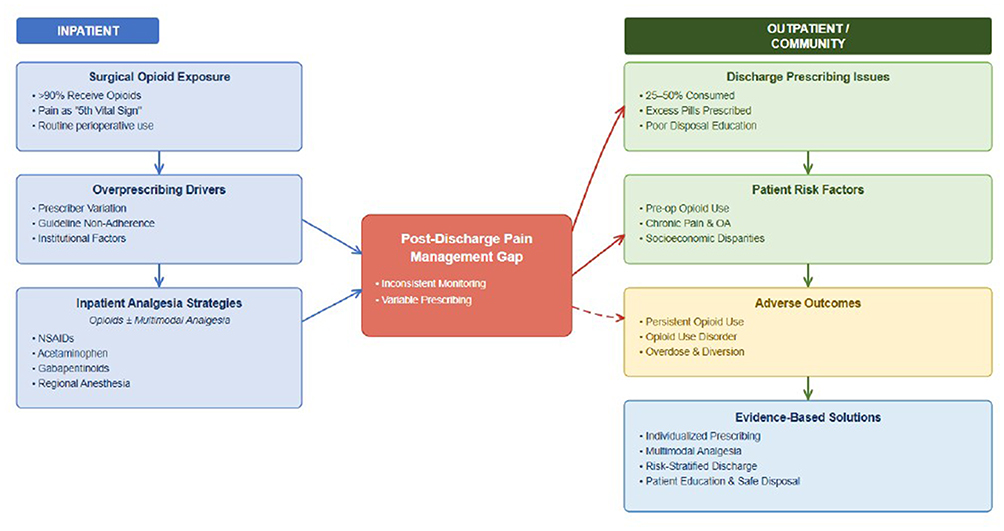










A persistent and consequential gap emerges at the point of hospital discharge. Across multiple surgical cohorts, opioid prescriptions substantially exceed actual patient consumption. In elective surgery populations, surgeons prescribed nearly twice the amount of opioids consumed, leaving large quantities of unused medication vulnerable to diversion.40 Similar patterns were observed across outpatient procedures, where fewer than one-third of prescribed opioids were used, and prescription size—not pain severity—was the strongest predictor of consumption.46 Large-scale analyses demonstrate that more than half of postoperative opioid prescriptions exceed guideline recommendations, driven predominantly by prescriber-level factors rather than patient need.47 Notably, evidence suggests that indiscriminate intraoperative opioid minimization may paradoxically worsen postoperative pain and increase persistent opioid use, underscoring the need for balance rather than elimination (Figure 1).48–50
International and post-discharge data further expose critical deficiencies in perioperative opioid stewardship. In a multinational cohort spanning 25 countries, fewer than one-third of patients were prescribed opioids at discharge; however, when opioids were prescribed, quantities exceeded consumption by more than twofold.51 Regional variation was striking: while more than three-quarters of surgical patients in the United States and Canada received opioids within one week of discharge, only 11% did so in Sweden, highlighting the absence of globally harmonized, evidence-based discharge practices.52 Even within high-performing institutions, most patients consumed less than one-third of their prescribed opioids, few received disposal instructions, and a measurable proportion of opioid-naïve patients developed persistent use months after surgery.53,54 Persistent post-surgical pain affects 10–35% of patients, highlighting critical gaps between clinical practice and patient outcomes.55 Scoping reviews confirm that post-discharge pain is often inadequately managed despite effective inpatient multimodal analgesia, revealing a critical discontinuity between hospital-based care and outpatient pain management (Figure 1).56 Notably, persistent postoperative opioid use occurs in up to 4.7% of opioid-naive adolescents.57 Post-discharge analgesia often relies on clinician experience over guidelines, leaving patients with unmet expectations, inconsistent opioid use, and anxiety.58
Enhanced Recovery After Surgery (ERAS) pathways have successfully reduced inpatient opioid use, length of stay, and early postoperative complications, particularly in orthopedic procedures.59 However, reductions in in-hospital opioid exposure do not consistently translate into optimized discharge prescribing (Figure 1). In procedure-specific contexts such as cesarean delivery, ERAS implementation reduced the proportion of patients receiving opioids at discharge, yet most patients still received opioid prescriptions, often at high daily morphine equivalent doses.60 These findings expose a persistent knowledge gap regarding post-discharge opioid exposure, long-term functional outcomes, and the optimal extension of multimodal analgesia beyond hospitalization.
Collectively, these data delineate critical unresolved epidemiologic gaps in perioperative opioid use. Existing research remains disproportionately centered on inpatient prescribing, despite mounting evidence that the greatest volume of opioid exposure occurs after hospital discharge.
Standardized, procedure-specific guidance for discharge prescribing is largely absent, contributing to wide inter-provider and inter-institutional variability. Moreover, patient-level risk factors—including prior opioid exposure, pain phenotypes, comorbid substance use, and sociodemographic determinants—are inconsistently incorporated into prescribing decisions. Finally, the disconnect between effective inpatient multimodal analgesia and largely unstructured outpatient pain management underscores a fundamental breakdown in continuity of care. Failure to address these gaps perpetuates avoidable opioid exposure without demonstrable improvement in postoperative pain outcomes, highlighting an urgent need for data-driven, perioperative-to-post-discharge analgesic frameworks.
Precision-Based Opioid Stewardship in Perioperative Pain
Opioid analgesics vary substantially in their pharmacological properties, clinical utility, and safety profiles, with important implications for postoperative pain management and public health. Despite significant advances in analgesic strategies, postoperative pain (POP) remains frequently undertreated, contributing to delayed recovery, prolonged hospitalization, and progression to chronic postsurgical pain.61 Contemporary perioperative pain management therefore requires not only effective analgesia but also careful consideration of opioid pharmacology, misuse risk, and interindividual variability in treatment response.
Tramadol provides analgesia through weak μ-opioid receptor agonism combined with inhibition of serotonin and norepinephrine reuptake. It is primarily metabolized hepatically via CYP2D6, with partial renal excretion of active metabolites.62 Epidemiologic data indicate that tramadol has a comparatively lower misuse potential than other commonly prescribed opioids. Between 2015 and 2017, tramadol accounted for approximately 4% of past-year opioid misuse, substantially lower than the 7–8% observed for hydrocodone or oxycodone after adjustment for drug availability.63 Long-term analyses from 2002 to 2014 further demonstrate a stable misuse rate of approximately 1.5%, markedly lower than hydrocodone (6%), oxycodone (4%), and alprazolam.63 Despite this favorable misuse profile, tramadol poses clinically significant risks, including serotonin syndrome, particularly in overdose, in CYP2D6 poor metabolizers with elevated parent-drug concentrations, or when co-administered with serotonergic agents such as selective serotonin reuptake inhibitors, serotonin–norepinephrine reuptake inhibitors, or tricyclic antidepressants, which may potentiate serotonergic toxicity and inhibit tramadol metabolism.62
Prescribing patterns for fentanyl have undergone notable shifts. Population-adjusted outpatient use declined by 17.9% between 2016 and 2017, exceeding reductions observed for other prescription opioids, with pronounced decreases in states implementing stringent opioid regulations.64 Nevertheless, substantial inter-state variability persists, with a reported 3.5-fold difference between Alaska and Oregon.64 In contrast, hospital-based administration of fentanyl analogs, including remifentanil and sufentanil, tripled between 2006 and 2017, raising concerns regarding substitution effects and the downstream risks of misuse and diversion.64 Clinically, fentanyl produces potent μ-opioid–mediated effects including analgesia, sedation, euphoria, respiratory depression, nausea, and urinary retention.65 Misuse or dosing errors may precipitate severe adverse events such as chest wall rigidity, respiratory compromise, hypotension, cyanosis, and life-threatening arrhythmias (Figure 1).66
Comparative perioperative research highlights important opioid-sparing opportunities. Intraoperative administration of dexmedetomidine has demonstrated superior postoperative outcomes compared with remifentanil, including reduced pain at 2 and 24 hours, lower postoperative opioid consumption, and fewer complications such as hypotension, shivering, and postoperative nausea and vomiting.67 These findings support the need for individualized intraoperative opioid titration and careful selection of adjunct medications within multimodal analgesic strategies.
Tapentadol, a newer dual-mechanism analgesic, exerts synergistic analgesic effects through μ-opioid receptor agonism and norepinephrine reuptake inhibition, with enhanced noradrenergic signaling via α2-adrenergic pathways contributing to its efficacy.68 Recommended dosing does not exceed 600 mg/day for immediate-release formulations.69 Tapentadol provides effective analgesia for acute, chronic, and neuropathic pain and is associated with reduced nausea, constipation, and withdrawal severity, as well as lower μ-receptor affinity compared with traditional opioids.69,70 Its modulation of noradrenergic neurotransmission shares functional similarities with certain antidepressant mechanisms, which may support improved tolerability and adherence in selected patient populations.69
While informed opioid selection and stewardship are essential, substantial interindividual variability in analgesic response persists. This variability is increasingly attributed to genetic polymorphisms affecting opioid metabolism, transport, and receptor signaling—most notably CYP2D6, OPRM1, CYP2C9, COMT, and ABCB1—underscoring the clinical relevance of integrating pharmacogenomics into perioperative pain management.61,71–73 Among these, CYP2D6 genotype exerts a particularly strong influence on opioid analgesic efficacy, especially for prodrug opioids such as codeine, tramadol, and hydrocodone.74–77 Following knee arthroscopy, CYP2D6 poor metabolizers demonstrate significantly attenuated tramadol analgesia, whereas ultrarapid metabolizers experience the greatest pain reduction; in contrast, variants in ABCB1 (MDR1) show no significant effect in this setting.74 Hybrid implementation–effectiveness trials further confirm the feasibility of CYP2D6-guided postoperative opioid prescribing after total joint arthroplasty, identifying approximately 20% of patients as high-risk metabolizers, increasing the use of alternative opioids, reducing overall opioid exposure, and achieving pain control comparable to usual care.75
Beyond the perioperative setting, CYP2D6 polymorphisms also significantly influence opioid effectiveness in oncology populations, where intermediate and poor metabolizers experience inadequate analgesia, higher rates of pain-related hospitalizations, and more frequent escalation to opioids such as morphine or hydromorphone.76,77 Collectively, these findings support consideration of preemptive CYP2D6 genotyping to inform opioid selection, enhance safety, and improve pain outcomes across both acute and chronic pain contexts.71,78 The marked heterogeneity in opioid pharmacology, misuse potential, and genetically mediated response highlights the necessity of an integrated, precision-based approach to perioperative pain management. Combining evidence-based opioid stewardship with pharmacogenomic insights enables more individualized analgesic planning, optimizes patient safety, and represents a critical step toward sustainable, modern perioperative analgesia.
A pragmatic, scalable strategy to reduce perioperative opioid use is to systematically offer nonopioid analgesia as the foundation of postoperative pain management. Opioid monotherapy often provides suboptimal pain relief while increasing the risk of adverse drug events, dependence, and misuse. For many patients, scheduled nonopioid agents alone are sufficient, whereas others benefit from multimodal analgesic regimens, incorporating adjunct pharmacologic therapies and regional techniques. Collectively, these approaches reduce perioperative opioid exposure, enhance analgesic quality, and accelerate functional recovery.79–82
The Table 1 summarizes contemporary perioperative multimodal analgesia strategies, aligned with recommendations from Enhanced Recovery After Surgery (ERAS), the American Society of Anesthesiologists (ASA), and PROSPECT guidelines.83–85 While not exhaustive, it provides a practical framework for implementing opioid-sparing, evidence-based analgesia across diverse surgical populations.
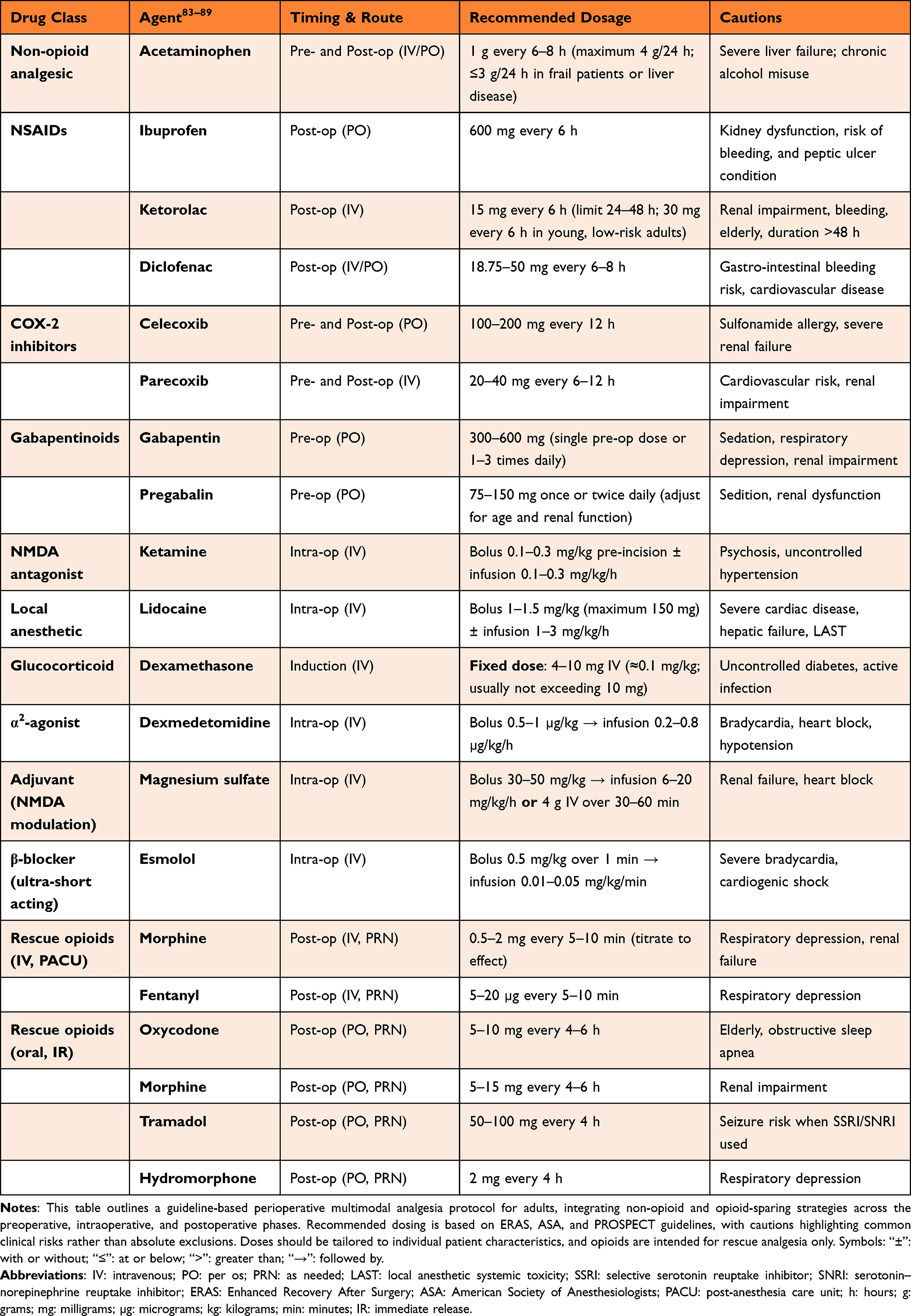 |
Table 1 Clinical Protocol for Perioperative Multimodal Pharmacological Analgesics |
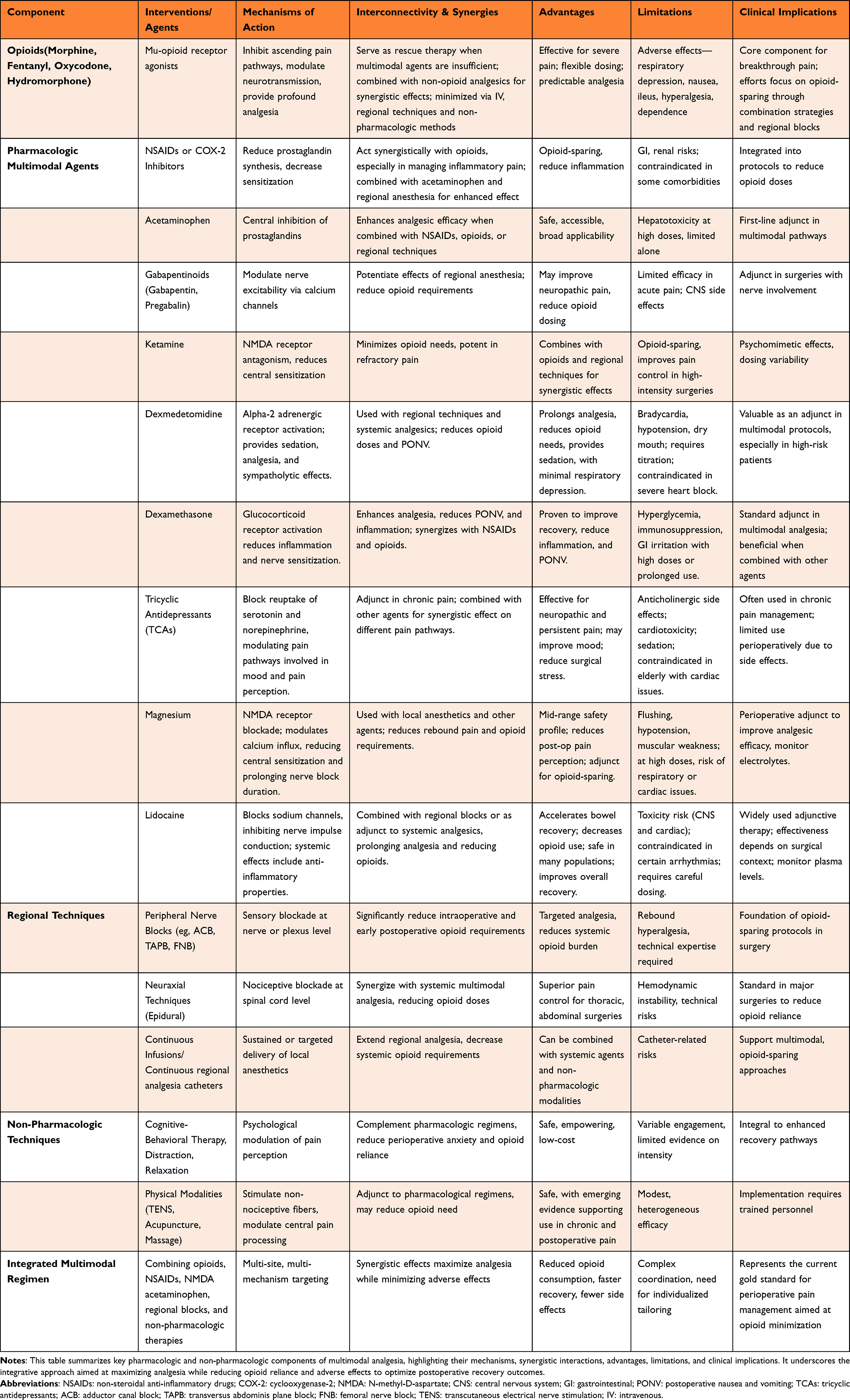 |
Table 2 Pharmacologic Multimodal Regimens: Synergistic Effects and Clinical Limitations |
Enhanced Recovery Analgesia
Opioids have traditionally been central to postoperative pain management but are associated with adverse effects—including nausea, vomiting, sedation, gastrointestinal dysmotility, respiratory depression, and immunosuppression—that can delay recovery. Enhanced Recovery After Surgery (ERAS) protocols therefore prioritize perioperative opioid minimization, reserving opioids for breakthrough pain when non-opioid strategies are insufficient. Opioid-tolerant patients represent an important exception, as scheduled opioid administration is required to prevent withdrawal. Although complete opioid avoidance is rarely feasible, ERAS pathways substantially reduce overall opioid exposure through as-needed dosing strategies (Table 1).
Multimodal analgesia, integrating pharmacologic and regional techniques targeting distinct nociceptive pathways, provides superior analgesia while enabling opioid dose reduction and limiting opioid-related adverse effects (Table 2).86 These principles underpin ERAS protocols, which incorporate non-opioid medications and regional anesthesia to accelerate recovery through additive or synergistic effects.7,87 In older adults, the American Geriatrics Society Beers Criteria identify potentially inappropriate medications; however, these are not absolute contraindications, and inappropriate substitution—such as replacing NSAIDs with opioids—should be avoided.88
Adjunctive strategies—including regional anesthesia, acetaminophen, NSAIDs, gabapentinoids, tramadol, lidocaine, and NMDA antagonists—reduce perioperative opioid requirements without increasing bleeding risk, allowing many patients to avoid postoperative opioid therapy.89 Evidence from systematic reviews and meta-analyses demonstrates that opioid-sparing multimodal analgesia reduces opioid consumption, pain scores, and ICU length of stay, including in large cardiac surgical populations, without adversely affecting mortality.79 Accordingly, ERAS protocols endorse multimodal, opioid-sparing analgesia as a cornerstone of perioperative care.84 Effective acute pain control accelerates recovery of function and quality of life, whereas inadequately treated pain may progress to chronic pain in up to 20% of patients.84 Given persistently high opioid use and the complexity of managing opioid-dependent patients, international expert consensus and professional societies advocate individualized, multimodal analgesic strategies to reduce opioid-related complications and improve outcomes.83,85
Observational and prospective studies across major surgical populations consistently demonstrate that incorporating regional anesthesia and comprehensive multimodal protocols improves postoperative pain control and reduces opioid requirements without increasing complications or length of stay.90,91 Given the avoidable risks associated with opioid-based analgesia, ERAS pathways prioritize procedure-specific, predominantly non-opioid multimodal strategies, supported by growing evidence across diverse surgical disciplines.80–82,92
Strategies for Opioid Reduction in Postoperative Pain Management
Post-operative pain impacts physical functioning, recovery, and quality of life, leading to anxiety. Effective management of pre- and postoperative pain is crucial in preventing chronic pain. Opioids are the main treatment for post-operative pain but come with unwanted side effects.25 Nearly half of spine surgery patients already take opioids pre-operatively, raising addiction concerns.93 A report published by the Academic Consortium in 2018 explored the reasons behind the widespread issue of pain management and offered scientific backing for using non-medication approaches to address pain.94 Personalized pain plans are emerging to combat this, educating patients on pain management options, addressing potential opioid dependence, and prioritizing safer medications like NSAIDs/COX-2 inhibitors (with stomach considerations) or NMDA-receptor antagonists/antiepileptics (requiring monitoring) – all considering pre-operative and post-operative effects.9,25,93
In the context of total knee arthroplasty (TKA), effective perioperative analgesia requires balancing pain control with safety. Preoperative administration of parecoxib sodium significantly lowered immediate postoperative pain (P = 0.039) without affecting surgical outcomes, complications, or analgesic consumption.95 Preoperative meloxicam improved early pain management, reduced opioid consumption by ~40%, and maintained functional recovery at three months, highlighting its potential for enhancing perioperative opioid-sparing strategies.96,97
Combination therapy with tramadol hydrochloride and acetaminophen (TRAM/APAP) outperformed NSAIDs alone, producing greater reductions in VAS pain scores and faster independent ambulation, emphasizing the value of synergistic multimodal analgesia.98 While meloxicam offers gastrointestinal advantages over non-selective NSAIDs,99 NSAID-associated risks—including transient renal impairment, platelet dysfunction, and increased cardiovascular events with long-term use—necessitate careful patient selection.97,99,100 Variations in pharmacokinetics, including fat- versus water-soluble NSAIDs, may further influence toxicity profiles in elderly and obese populations.101 Prodrug formulations, such as acemetacin, may reduce gastrointestinal side effects, but robust comparative data are lacking.102 Despite clear evidence supporting the efficacy and opioid-sparing effects of these agents, gaps remain in understanding long-term functional outcomes, optimal dosing strategies (Table 2), and individualized risk mitigation. Tailoring analgesic regimens to patient-specific factors, including comorbidities, body composition, and pharmacokinetic profiles, is essential to maximize benefit and minimize harm.102 Additionally, the search for alternatives extends beyond medications, with ongoing research on Complementary and Alternative Medicine (CAM) for pain management.103 Future studies should explore long-term safety, functional recovery, and comparative effectiveness across diverse populations to inform evidence-based multimodal perioperative pain management. Postoperative analgesia may include intravenous opioids and non-opioids—such as morphine, oxycodone, fentanyl, or bupivacaine—administered under the guidance of the surgeon and anesthetist, tailored to the patient’s pain needs after major surgery.104
Adjuvant Therapies in Multimodal Analgesia
Adjuvant analgesics while individually beneficial are most effective when integrated into a broader multimodal framework (Table 2). Their use requires cautious titration from the lowest effective dose, particularly given the delayed onset of some agents, and an adequate therapeutic trial is essential before deeming a therapy ineffective.87 Although certain adjuvants are employed for refractory pain syndromes such as back pain or temporomandibular disorders, it is important to acknowledge that evidence supporting these indications remains weak, highlighting a persistent gap in rigorous clinical data.87
Analgesic effectiveness is shaped by fundamental pharmacologic features including onset, duration, and magnitude of relief that often parallel systemic drug exposure.105 Yet despite advances in pharmacology, single-agent strategies continue to underperform in complex postoperative or geriatric pain states. This underscores the need to expand and standardize multimodal pain management approaches that integrate pharmacologic and non-pharmacologic modalities. Such comprehensive strategies have demonstrated the capacity to reduce opioid consumption, mitigate opioid-related complications, and enhance functional recovery in elderly hip-fracture patients, a population particularly vulnerable to adverse outcomes.106,107
Non-pharmacologic interventions remain underutilized despite their established safety, accessibility, and minimal risk of harm. Techniques such as breathing exercises, massage, positioning, and music therapy form a broad spectrum of cognitive–behavioral, physical, and supportive approaches.108,109 As outlined by Pölkki et al, these modalities not only complement pharmacologic therapy but empower patients, promoting self-efficacy and active engagement in pain control,109 a critical component of enhanced recovery pathways Their low cost and favorable adverse-effect profile further support their routine incorporation into perioperative practice.110–112
Current PROSPECT recommendations reflect the shift toward evidence-based multimodal regimens (Figure 2). For elective cesarean delivery under neuraxial anesthesia, intrathecal morphine (50–100 µg) or diamorphine (300 µg), combined with paracetamol/NSAIDs and IV dexamethasone, remains the cornerstone of optimized analgesia. When intrathecal opioids cannot be used, fascial plane blocks or wound infiltration provide effective alternatives, with TENS as an adjunct; opioids are relegated to rescue therapy.113 In Video-assisted Thoracoscopic Surgery, early continuation of non-opioid analgesics and the prioritization of regional techniques particularly paravertebral and erector spinae plane blocks reflect high-quality evidence favoring opioid-sparing strategies. IV dexmedetomidine is recommended when regional anesthesia is not feasible, further highlighting the move toward opioid minimization.114 Overall, synergistic multimodal analgesia protocols (MAPs) represent a critical evolution in perioperative care (Figure 2). By combining pharmacologic and non-pharmacologic strategies including regional anesthesia, acetaminophen, NSAIDs, ketamine, dexamethasone, and structured non-pharmacologic therapies MAPs consistently reduce pain severity, minimize opioid exposure, and improve postoperative recovery trajectories without increasing adverse effects (Table 2).115 Future research should focus on standardizing these multimodal pathways and identifying patient-specific predictors of response to further refine personalized analgesic care.
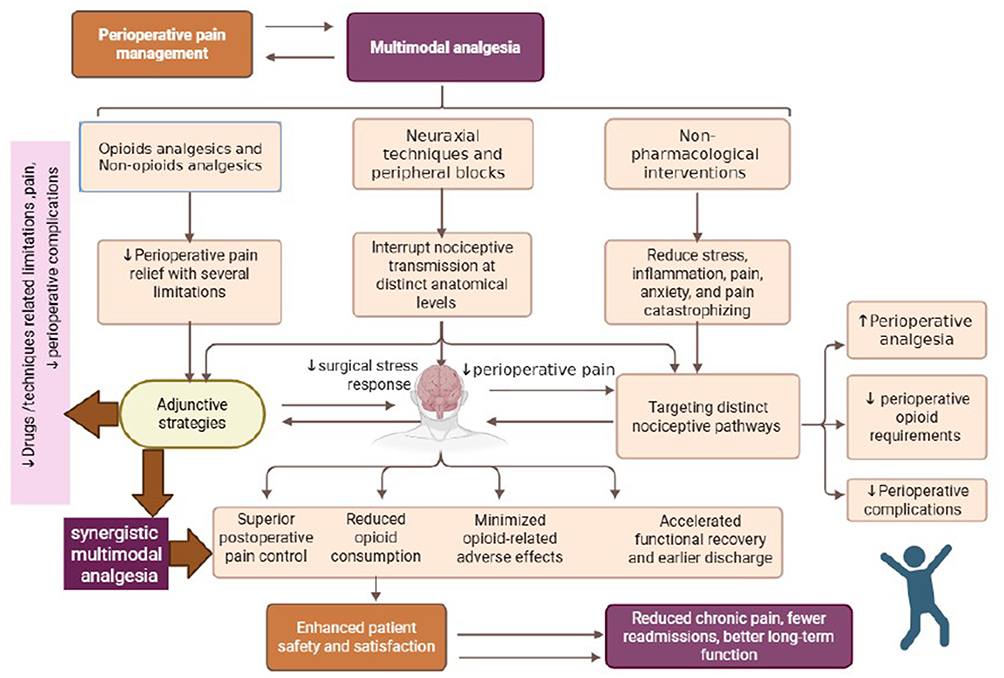 |
Figure 2 Schematic illustration of perioperative multimodal analgesia emphasizing the synergistic integration of complementary strategies to enhance analgesic efficacy, minimize treatment-related complications, and accelerate postoperative recovery, discharge, and rehabilitation. ↑: Increase, ↓: Decrease. |
Systemic Non-Opioid Analgesic
Intravenous Acetaminophen
Intravenous paracetamol and propacetamol continue to show reproducible—but not uniformly transformative—analgesic effects across surgical and acute care settings.116 Meta-analytic evidence confirms that parenteral paracetamol achieves clinically meaningful pain relief (≥50% reduction) in only about one-third of postoperative patients, with a number needed to treat of 5,116 and ED data demonstrate modest opioid-sparing benefits.117 These findings underscore paracetamol’s value but also reveal its ceiling as a foundational rather than decisive component of multimodal analgesia. Safety considerations are increasingly central. Although acetaminophen is perceived as low risk, frailty-related pharmacokinetic alterations complicate this narrative. Frail older adults experience disproportionately elevated serum concentrations and reduced clearance, far exceeding changes attributable to chronological age alone.118 This decline—driven predominantly by impaired glucuronidation with preserved sulfation positions frailty,119 rather than age, as the critical determinant of hepatotoxicity risk, which may occur even at therapeutic doses.120 Clinically, this reframes paracetamol as a drug requiring tailored dosing rather than routine administration in geriatric care.121 Hemodynamic instability following IV acetaminophen further challenges its routine use in high-acuity environments. Hypotension occurs in 10–60% of critically ill patients and demands intervention in up to 30%,122 raising concerns about unrecognized hemodynamic liability. Prospective observations reinforce this risk: over half of monitored adults experience substantial MAP reductions after infusion, with a median nadir of 64 mmHg and more than one-third requiring corrective measures.123 Experimental evidence implicates N-acetyl-p-benzoquinone imine in a Kv7.4/7.5 channel–mediated vasodilatory cascade amplified by CGRP release, offering a mechanistic explanation and a potential target for mitigation.124
Analgesic combinations containing paracetamol, such as paracetamol/codeine, can improve early postoperative pain control and reduce rescue analgesic needs relative to ibuprofen or placebo.125 Yet large-scale instrumental-variable analyses challenge assumptions about its centrality to multimodal analgesia: NSAIDs combined with dexamethasone and regional anesthesia deliver the most clinically meaningful opioid-sparing effects, whereas acetaminophen’s contribution is comparatively modest and often overstated.17 These findings compel a recalibration of multimodal protocols that currently rely heavily on acetaminophen without strong evidence of incremental benefit. Ultimately, while dual-mechanism analgesia offers an advantage in early postoperative pain control with controlled opioid exposure, substantial uncertainties persist. Optimal dosing for frail geriatric patients remains undefined, hemodynamic safety in unstable or critically ill individuals is unresolved, and long-term recovery implications are largely unexplored.126
Progress will require rigorously designed, stratified clinical trials incorporating validated frailty indices, mechanistically informed dosing frameworks, and real-time hemodynamic surveillance. Without such precision, acetaminophen’s role in personalized, opioid-sparing analgesic care will remain constrained by longstanding assumptions rather than robust evidence.
Dexmedetomidine
Growing evidence supports dexmedetomidine as a potent opioid-sparing adjunct with clinically meaningful benefits across perioperative settings. A meta-analysis demonstrated significantly reduced early postoperative pain compared with remifentanil (mean difference –0.7/10; 95% CI –1.2 to –0.2; P = 0.004) and improved 24-hour pain outcomes, reinforcing dexmedetomidine’s analgesic superiority with moderate-quality evidence.67 Beyond analgesia, dexmedetomidine prolonged time to first analgesic request, lowered postoperative morphine and rescue analgesic use, and reduced hypotension, shivering, and PONV, while maintaining comparable bradycardia rates to remifentanil.67 Standard dosing regimens (1 μg/kg bolus followed by 0.5 μg/kg/h infusion) attenuate perioperative hemodynamic stress and significantly reduce postoperative analgesic need during laparoscopic procedures.127 Its capacity to lower anesthetic and opioid requirements, diminish postoperative nausea, vomiting, delirium, and agitation, and preserve respiratory drive positions dexmedetomidine as an attractive component of opioid-free anesthesia, especially for bariatric and spine surgery.128
Mechanistically, dexmedetomidine’s analgesic, sedative, and possible antiemetic actions stem from targeted modulation of nociceptive transmission, suppression of sympathetic activation, and mitigation of hyperalgesia, with preclinical evidence supporting synergism with opioids.129 These properties translate into improved postoperative comfort, reduced anxiety, shorter hospital stay, and enhanced recovery trajectories.130 However, its expanding use must be balanced against concerns regarding hemodynamic instability. The increased risk of intraoperative bradycardia is well-documented, warranting careful patient selection and vigilant monitoring.129 Evidence from thoracoscopic lung cancer surgery further suggests that dexmedetomidine not only reduces PONV and opioid use but also accelerates functional recovery, with data supporting an optimal dose of 0.4 μg/kg/h in this population.131 Despite these promising findings, questions remain regarding its safety in high-risk cardiovascular patients, dose-response relationships, and comparative effectiveness across surgical subgroups highlighting the need for rigorously stratified future trials.
Dexamethasone
Growing evidence supports perioperative dexamethasone as a valuable adjunct within multimodal analgesia for joint arthroplasty, yet its risk–benefit profile warrants more nuanced interpretation.
Consistent reductions in postoperative pain, opioid requirements, and length of stay following TKA and THA highlight its potential to enhance recovery pathways.132–134 Notably, a single 8–10 mg intravenous dose appears sufficient for meaningful analgesic benefit, and additional dosing confers no clearly demonstrated advantage.133,135 The enhanced recovery observed with delayed postoperative dosing and adjunctive warming techniques raises the possibility that dexamethasone’s immunomodulatory and metabolic effects may influence functional outcomes beyond simple analgesia.136
However, emerging data identifying preoperative dexamethasone as an independent predictor of rebound pain (incidence 61.7%) signal an underrecognized paradox: while early analgesia improves, susceptibility to delayed hyperalgesic states may increase.135 This phenomenon challenges assumptions about corticosteroid-mediated nociceptive modulation and underscores the need to contextualize analgesic benefits within a temporal framework. Furthermore, dexamethasone’s adverse-effect profile ranging from gastrointestinal irritation to neuropsychiatric symptoms remains clinically relevant, particularly in older or frail patients.137 Current evidence supports dexamethasone as an effective perioperative adjunct, but important uncertainties persist regarding optimal timing, patient selection, and its interaction with rebound pain physiology. Future trials should incorporate mechanistic endpoints, stratify by vulnerability to hyperalgesia, and compare single versus staged dosing strategies to refine its integration into precision multimodal analgesia.
Ketamine
Ketamine has emerged as a potent multimodal analgesic with opioid-sparing properties, yet its role in perioperative pain management requires nuanced interpretation. Clinical trials demonstrate ketamine reduces postoperative pain intensity, morphine consumption, and delays rescue analgesia in cesarean sections under spinal anesthesia, indicating its value as a temporary but clinically relevant strategy.121,138 Preoperative administration under general anesthesia appears optimal, particularly for high-pain surgeries including abdominal, thoracic, orthopedic, and spinal procedures.70 Mechanistic insights suggest that ketamine’s analgesia extends beyond NMDA receptor blockade, potentially modulating emotional pain processing and influencing long-term pain perception.139 Its antidepressant effects in refractory depression, PTSD, and substance use disorders underscore its dual utility in perioperative and chronic pain settings.140 Low-dose IV infusions (<1.2 mg/kg/h) consistently demonstrate ~40% reductions in postoperative opioid consumption without major complications up to 48 hours, although optimal dosing regimens remain to be defined.141
Heterogeneity exists across populations. Pediatric studies reveal limited analgesic benefit over 72 hours, with sex differences affecting opioid use and sedation.142
Combined methadone–ketamine regimens highlight the additive potential for opioid reduction post-lumbar arthrodesis, suggesting strategic synergies in multimodal protocols.143 Systematic reviews and meta-analyses reinforce ketamine’s early analgesic efficacy and opioid-sparing impact, though sensitivity analyses indicate variability based on surgical type, dose, and timing.144,145 Clinical trials in lumbar fusion support a S-ketamine:oxycodone ratio of 1:0.75 to achieve meaningful opioid reduction without increasing adverse events.146
Despite robust analgesic effects, ketamine is not without limitations. Evidence for prolonged postoperative benefit is mixed, with variability in pediatric, minor, and major surgeries. Psychotomimetic effects, inflammatory modulation, and antidepressant outcomes offer additional mechanistic advantages, yet require careful risk–benefit consideration.147–155 Emerging public health concerns, exemplified by “Tusi” misuse, highlight the need for regulatory awareness and research caution.156 Intraoperative esketamine reduces pain, anxiety, depression, and neuroinflammatory markers, yet cognitive benefits remain unproven, reinforcing the need for targeted, individualized protocols.155 Evidence in other surgical populations is mixed. A meta-analysis of 7RCTs (748 patients) found no significant reduction in postoperative pain after breast cancer surgery, although ketamine/esketamine reduced short-term postoperative depression and dizziness without affecting recovery quality.157 In pediatric surgery, a meta-analysis of 23 randomized trials (1,996 children) showed that perioperative esketamine reduced emergence delirium, postoperative pain scores, adverse events, and PACU length of stay in tonsillectomy and adenoidectomy.158 In elderly patients undergoing lumbar spine surgery, a randomized trial (n = 90) found that low-dose esketamine reduced perioperative opioid requirements, lowered early postoperative pain scores, attenuated inflammatory cytokine responses, and improved hemodynamic stability. Postoperative respiratory depression was reduced, with no increase in psychiatric adverse effects.159 Ketamine exhibits robust analgesic and opioid-sparing effects, alongside potential mood and anti-inflammatory benefits. Nonetheless, variability in dosing, patient response, and adverse events underscores the need for cautious, evidence-driven use. Future research must clarify long-term outcomes and define optimal, multimodal analgesic strategies.
Magnesium
Intravenous magnesium exhibits clinically relevant opioid-sparing effects in perioperative analgesia, yet current evidence presents limitations that temper confidence in its widespread adoption. Synthesized data from 25 trials suggest reductions in 24-hour postoperative opioid consumption and improved analgesic profiles without major adverse events.160 Beyond its NMDA-receptor–mediated analgesic action, magnesium may attenuate rebound hyperalgesia, as indicated by interscalene ropivacaine studies showing modest prolongation of block duration and enhanced 24-hour pain control.161 Meta-analytic evidence further supports its role in noncardiac surgery, reporting prolonged analgesic intervals and lower morphine requirements.162 However, substantial heterogeneity, variable dosing regimens, and inconsistent reporting of magnesium-related hemodynamic effects underscore the need for caution in interpretation.163–165 Clinical use is further constrained in patients with atrioventricular conduction abnormalities, neuromuscular disorders, or renal impairment due to risks of toxicity, muscle weakness, and ECG disturbances, highlighting the importance of individualized patient assessment and monitoring.164,166 Taken together, magnesium is a promising adjunct in multimodal analgesia, but its optimal dosing, patient selection, and true impact on postoperative outcomes require rigorous, high-quality trials with standardized protocols and safety monitoring to establish evidence-based recommendations.
Gabapentinoids
Gabapentinoids have attracted considerable attention as opioid-sparing adjuncts, particularly in spinal surgery, where consistent reductions in postoperative pain and opioid-related adverse events have been observed.167 Pregabalin may offer incremental benefits over gabapentin, though conflicting reviews highlight substantial variability in effect size and clinical relevance.168 Evidence supporting gabapentin’s role in reducing catheter-related bladder discomfort (CRBD) adds a potentially meaningful secondary indication.169 Despite these advantages, accumulating safety data warrants a more conservative interpretation of their perioperative utility, especially in older, frail, or renally impaired populations. The dose-dependent interaction between gabapentinoids and opioids substantially increases the risk of oversedation and respiratory depression, particularly at preoperative doses exceeding 300 mg of gabapentin combined with >20 mg oxycodone.170
Observational and mechanistic studies further indicate increased vulnerability during laparoscopic procedures, where respiratory compromise may be masked until emergence.171 Renal elimination necessitates strict dose reduction when creatinine clearance falls below 60 mL/min.172 While randomized trials indicate gabapentin does not increase long-term opioid use compared to placebo,173 large observational datasets report heightened pulmonary risk, and small clinical trials suggest only modest analgesic benefit, highlighting a disconnect between efficacy and safety.174 Gabapentinoids also contribute to dizziness, cognitive impairment, and respiratory complications, suggesting that routine administration may be unjustified. These findings advocate for a selective, patient-specific approach, with risk stratification based on age, renal function, surgical procedure, and perioperative opioid exposure.175 Conversely, gabapentinoids emerge as a relatively effective non-opioid adjunct. Moving forward, rigorously designed trials are required to identify patient subgroups most likely to benefit, and systematically quantify respiratory and neurological risks to guide evidence-based, individualized perioperative analgesic strategies.
Lidocaine
Intravenous lidocaine represents a potent perioperative adjunct, yet its clinical adoption remains limited due to inconsistent protocols, uncertain patient selection, and variable reporting of systemic adverse effects.176 Evidence on its efficacy compared to placebo across postoperative outcomes is marked by uncertainty, as highlighted in a Cochrane review emphasizing methodological limitations and heterogeneity.177 Notably, lidocaine’s impact on pain scores beyond the initial 24-hour postoperative period appears minimal, and comparative evidence versus epidural anesthesia remains sparse, leaving its broader clinical utility unresolved.177
Perioperative studies yield mixed results: for example, systemic lidocaine during video-assisted thoracoscopic surgery (VATS) under general anesthesia did not significantly reduce postoperative pain or enhance recovery,178 whereas targeted local injections in thyroid surgery provided only modest improvements during early movement or coughing, with comparable overall analgesia.179 Dosing precision is critical. Infusions should be calculated using ideal body weight, with a maintenance rate of 1–1.5 mg/kg/h (max 120 mg/h) for ≤24 hours, and a loading dose ≤1.5 mg/kg over 10 minutes. Contraindications include patients <40 kg and concurrent local anesthetic blocks.6 Properly administered, IV lidocaine can reduce chronic postsurgical pain, early postoperative pain, and opioid consumption, particularly following abdominal and breast surgery, though optimal dosing and long-term outcomes require further investigation.176 Meta-analytic evidence demonstrates that perioperative IV lidocaine in abdominal surgery can reduce postoperative opioid use by up to 85%, accelerate gastrointestinal recovery (first flatus by 23 hours, first bowel movement by 28 hours), and shorten hospital stay by 1.1 days, without major adverse effects; however, its efficacy in other surgical populations remains uncertain.180 Mechanistic studies indicate dose-dependent effects: high doses reduce central sensitization, while low doses attenuate peripheral hyperalgesia, with analgesic effects persisting hours post-infusion.181 These findings suggest lidocaine may modulate both peripheral and spinal sensitization in neuropathic and inflammatory pain models.
While perioperative IV lidocaine may accelerate bowel recovery, decrease opioid requirements, and mitigate inflammatory responses,182 its benefit must be interpreted cautiously. Pharmacokinetic studies indicate consistent plasma levels in patients up to 86 years old, with over 90% achieving therapeutic concentrations safely, suggesting age-based dose adjustments are generally unnecessary.183 Nonetheless, heterogeneity in protocols, patient selection, and long-term outcome data necessitates further large-scale, stratified trials to clarify its efficacy, optimal dosing, and safety across diverse surgical populations.
Regional Analgesia Approaches
Regional analgesia within enhanced recovery pathways encompasses neuraxial and peripheral techniques that interrupt nociceptive transmission at distinct anatomical levels. Neuraxial approaches, including epidural analgesia and intrathecal opioids with or without adjuvants, provide dense central analgesia but require careful patient selection due to procedure- and comorbidity-specific risks. Peripheral strategies—such as paravertebral, transversus abdominis plane, brachial plexus, femoral, sciatic, and fascia iliaca blocks, as well as wound infiltration—offer targeted, opioid-sparing analgesia with reduced systemic drug exposure. These techniques may be delivered as single-injection or catheter-based interventions and can be implemented preoperatively to attenuate central sensitization or postoperatively to supplement multimodal regimens when early placement is not feasible.
Neuraxial Analgesia Within Opioid-Sparing Multimodal Strategies
Continuous epidural analgesia using local anesthetics combined with opioids, such as bupivacaine and morphine, provides meaningful improvements in postoperative pain control, particularly after major orthopedic procedures. However, within a multimodal analgesia framework, these benefits must be carefully balanced against procedure- and patient-specific risks.184 Analgesic efficacy is most pronounced during the first 18–24 postoperative hours, yet supplemental systemic opioids are frequently required, underscoring the persistent challenge of achieving sustained analgesia while minimizing opioid exposure.185,186 Traditional epidural techniques, although effective, are associated with higher complication rates in frail and cardiovascularly vulnerable patients, which has contributed to growing interest in ultrasound-guided peripheral nerve blocks as safer, opioid-sparing alternatives within multimodal strategies, despite their continued underutilization in clinical practice.9
Intrathecal morphine provides potent and prolonged analgesia and has been shown to significantly reduce postoperative opioid requirements, particularly following abdominal surgery. Nevertheless, its clinical utility is constrained by a narrow therapeutic window and an unpredictable dose–response relationship.187 Increased rates of respiratory depression and pruritus, as well as delayed respiratory compromise reported in obstetric populations, highlight safety concerns that are relevant to other high-risk surgical patients and emphasize the need for careful dosing and vigilant postoperative monitoring.188 In addition, systemic absorption of lipophilic opioids administered epidurally may contribute to gastrointestinal adverse effects, supporting consideration of local anesthetic–only neuraxial regimens in selected patients within a broader multimodal approach.187 These findings indicate that while neuraxial opioids remain an important component of perioperative analgesia,189 their use should be individualized according to surgical context, comorbid conditions, and overall risk profile.
Neuraxial analgesia, encompassing epidural and spinal techniques, contributes substantially to multimodal pain control through the use of opioids with distinct pharmacokinetic properties. Lipophilic opioids such as fentanyl and sufentanil provide rapid onset of analgesia with relatively short duration, whereas hydrophilic agents such as morphine and hydromorphone demonstrate slower onset but prolonged analgesic effects. Standard intrathecal morphine doses (0.1–0.5 mg) typically provide 6–24 hours of postoperative analgesia and reduce reliance on systemic opioids.190 Common adverse effects include nausea, vomiting, pruritus, sedation, and respiratory depression.191 Although contemporary lower-dose strategies have reduced the incidence of respiratory complications, extended-release epidural morphine (10–30 mg) has been associated with a significantly increased risk of respiratory depression (OR 5.80; 95% CI 1.05–31.93), leading to recommendations from the ASA for at least 48 hours of postoperative monitoring, particularly in high-risk populations.70,191
Postoperative opioid exposure remains associated with a broad range of adverse outcomes, including nausea, vomiting, urinary retention, sleep disturbance, respiratory depression, somnolence, dizziness, delayed recovery, and opioid-induced hyperalgesia.93 Opioid-induced hyperalgesia, particularly associated with high-dose intraoperative opioids such as remifentanil, may paradoxically increase postoperative pain, lower pain thresholds, and contribute to the development of chronic postsurgical pain.93,192 While the overall incidence of opioid misuse following surgery is relatively low (approximately 0.6%), duration of opioid therapy is a critical determinant of risk; each prescription refill is associated with a 44% increase in misuse likelihood, and each additional week of opioid use increases risk by nearly 20% (Figure 1).193 These findings reinforce the importance of neuraxial techniques as part of opioid-sparing multimodal analgesic strategies, alongside careful patient selection, ongoing assessment of analgesic efficacy, and close monitoring for adverse effects to optimize both short- and long-term postoperative outcomes.
Regional and Fascial Plane Blocks in Postoperative Pain
Regional and fascial plane blocks (FPBs) have emerged as cornerstone strategies in multimodal postoperative analgesia, yet their clinical utility must be carefully interpreted in the context of patient outcomes, procedural complexity, and risk-benefit balance. Thoracic epidural analgesia (TEA) and paravertebral blocks (PVBs) continue to demonstrate superior pain control, accelerated extubation, and reduced rescue analgesia requirements in cardiac surgery.194–196 However, the clinical adoption of TEA is limited by hemodynamic instability, risk of spinal hematoma, and potential neurologic injury, highlighting the importance of meticulous perioperative monitoring.197 Ultrasound-guided fascial plane blocks, including serratus anterior plane (SAPB) and erector spinae plane (ESPB) blocks, present safer alternatives with reduced procedural risk, yet their analgesic potency does not consistently match TEA, indicating that opioid-sparing alone may not reflect true analgesic quality.196,198 TAPB reduces perioperative opioid consumption and improves early pain scores in orthopedic and abdominal surgeries, demonstrating clear analgesic benefit in both periacetabular osteotomy and laparoscopic colorectal surgery.199,200 Nonetheless, TAPB does not consistently affect hospital stay or long-term outcomes, and superior analgesic efficacy of subarachnoid morphine must be weighed against higher adverse events.188
FNB and FICB are effective in elderly hip fracture patients, providing early analgesia and reducing opioid requirements.201–203 Evidence confirms their safety in cognitively impaired populations, although quadriceps motor blockade may increase fall risk.201,204 Comparative studies of US-guided FNB, blind FICB, and continuous FICB highlight similar analgesic outcomes, with continuous blocks offering extended opioid-sparing benefits but potentially delaying early rehabilitation.205–207 These findings underscore the trade-offs between analgesic duration, functional recovery, and procedural complexity. Thoracic, cardiac, and breast surgery pain control benefit from fascial plane blocks such as SAPB, PECS II, DPIPB, and ESPB.195,208–215 These blocks reduce opioid requirements, improve early recovery, and maintain hemodynamic stability, supporting their role as opioid-sparing adjuvants. Notably, modified S-FICB and US-FICB optimize analgesia in hip arthroplasty and hip fracture, demonstrating effective blockade of multiple target nerves.216,217 Meta-analytic evidence further corroborates FICB’s early postoperative pain reduction and decreased opioid use in total hip arthroplasty.218
Despite overall efficacy, heterogeneity persists across studies. Some blocks show comparable outcomes in intermediate-term recovery, while continuous techniques may affect early mobility.207 Moreover, the risk of motor blockade, the need for ultrasound guidance, and procedural expertise highlight practical limitations.201,204–206 Emerging evidence suggests quadratus lumborum and lumbar ESP blocks outperform standard analgesia in hip and proximal femoral surgeries, underscoring the potential for optimized, procedure-specific regional strategies.219 However, critical appraisal of FPBs also emphasizes safety and systemic considerations. LAST, though rare, poses a high-stakes complication, particularly in brachial plexus blocks, with seizures exacerbated by hypoxia, hypercapnia, and acidosis.220,221 Additionally, rebound pain and motor impairment remain notable limitations, potentially delaying rehabilitation and increasing fall risk.11,25 Nonetheless, when integrated thoughtfully within a multimodal framework, nerve blocks remain powerful adjuncts capable of improving recovery trajectories.11 These findings underscore that advanced analgesic techniques deliver significant opioid-sparing effects, superior pain control, and faster recovery.194,222 However, implementation requires balancing efficacy, safety, and functional outcomes.189,223 Future research should prioritize comparative effectiveness, long-term outcomes, and integration into multimodal analgesic protocols across varied surgical populations.
Continuous Regional Analgesia Catheters
Continuous and single-shot regional analgesic strategies demonstrate variable efficacy and resource demands, underscored by evidence from multiple surgical settings. The transmuscular quadratus lumborum block (QLB) achieved lower pain scores at rest (p = 0.036) and higher patient acceptance (p = 0.004, p = 0.006) than pre-peritoneal catheter blocks, albeit at a substantial additional cost.224 In total hip arthroplasty, continuous femoral nerve block (FNB) provided superior analgesia during movement at 6 hours (median 38 vs 67, p = 0.008) and 24 hours (median 39 vs 60, p = 0.018) compared to continuous QLB, highlighting inconsistencies in sensory blockade and suggesting procedure-specific optimization is required.225
Continuous regional and neuraxial blocks remain potent tools for severe postoperative pain, yet high failure rates—particularly with epidural catheters—limit their universal application.226 Novel applications, such as the erector spinae plane block with continuous infusion, demonstrate feasibility in enabling safe postoperative physiotherapy, illustrating how ultrasound guidance may mitigate complications.227 Dual-catheter strategies targeting popliteal and saphenous nerves enhanced analgesia, increased patient satisfaction, and reduced opioid requirements, suggesting that selective, multi-targeted approaches may improve outcomes.228 Evidence regarding adductor canal blocks (ACB) indicates that single-shot techniques provide equivalent pain relief and functional recovery to continuous ACB within the first 48 hours after total knee arthroplasty, whereas continuous ACB increases complication risks without clear analgesic superiority.229 Similarly, continuous brachial plexus blocks extend analgesia but impose high logistical and safety burdens, including infection risk, device failure, and up to 5% catheter displacement within 6 hours.230 These findings highlight the tension between theoretical analgesic advantages and practical limitations, underscoring the importance of evidence-based implementation of continuous PNBs.
Safety Considerations in Regional and Neuraxial Analgesia
Although local and regional anesthetics are cornerstone modalities for perioperative analgesia, their safety profile is constrained by dose-dependent neurotoxicity and cardiotoxicity. High doses can induce neuronal hyperexcitability, manifesting as tremors or seizures, and impair cardiac conduction, reducing contractility.231 Notably, bupivacaine, ropivacaine, and mepivacaine demonstrate preferential toxicity toward degenerated cartilage, with chondrocyte injury mediated via both necrotic and apoptotic mechanisms, a pattern not predicted by analgesic potency.232 This underscores the need to consider tissue-specific toxicity when selecting local anesthetics, particularly in degenerative joint disease. Peripheral nerve blocks carry functional trade-offs. Continuous lumbar plexus and femoral nerve blocks effectively control postoperative pain but substantially increase fall risk due to transient quadriceps weakness.233–235 Fascia iliaca compartment blocks similarly compromise muscle strength in the immediate postoperative period.207,236 Interscalene blocks present additional safety concerns, with 34% of patients in one study developing postoperative respiratory difficulties.237 Neuraxial anesthesia, while broadly safe, has rare yet severe adverse outcomes. Data from Sweden highlight that two-thirds of serious events result in permanent injury, predominantly from epidural hematomas rather than infections.197 Rebound pain following nerve blocks further complicates postoperative management.25,238 Preexisting neurologic disease markedly increases susceptibility to neuraxial complications (0.3–1.1%), far exceeding general population rates (0.001–0.07%), with serious outcomes requiring decompression occurring in <0.05%. Peripheral nerve injuries are typically transient but remain a clinical concern.197
Epidural analgesia balances efficacy with a spectrum of potential adverse effects. Local anesthetics can induce hypotension, sensory and motor deficits, and urinary retention, whereas epidural opioids add pruritus, nausea, vomiting, and respiratory depression. Technique-related risks, including post-dural puncture headache, catheter-related back pain, and epidural hematoma, emphasize the importance of procedural expertise. Concurrent anticoagulation—particularly with LMWH, unfractionated heparin, warfarin, or newer antiplatelet agents—increases hematoma risk, reinforcing the necessity for strict adherence to safety protocols.187 These data highlight that while regional anesthesia provides powerful analgesic benefit, its implementation must be individualized, integrating patient comorbidities, anticoagulation status, and tissue-specific vulnerabilities to optimize safety and outcomes.
Non-Pharmacological Pain Management(NPM)
Non-pharmacological interventions are increasingly incorporated into multimodal postoperative analgesia, yet their clinical impact remains inconsistent. Physical modalities—including TENS, acupuncture, massage, and temperature therapies—show variable efficacy.239 Large-scale observational data from 14,767 European patients revealed that 44.4% utilized at least one NPM, reporting slightly lower pain relief (68.6% ± 25.7%) than non-users (71.2% ± 27.9%, p<0.001), indicating that NPM use does not universally translate into superior analgesia.240 Evidence from 69 RCTs demonstrates nuanced outcomes. Specific acupressure decreased pain by WMD −2.09 cm on a 10-cm VAS (moderate certainty), while supervised rehabilitation paradoxically increased pain (WMD +1.06 cm). TENS reduced pain modestly (WMD −1.18 cm, low certainty), and acupressure improved function (WMD +1.51 cm). Laser therapy strongly enhanced symptom relief (OR 32.08), whereas mobilization had limited benefit (OR 7.99). Treatment satisfaction effects were generally absent.241 These findings underscore that while certain NPMs offer measurable benefits, the overall contribution to postoperative pain control is modest.103,242,243
Preoperative anxiety affects 11–80% of surgical patients and significantly influences intraoperative anesthetic dosing and postoperative analgesic requirements.244 Anxiety and pain are shaped by both biological and psychosocial factors, leading to wide interindividual variability.245 Clinical studies show that higher preoperative anxiety and pain sensitivity predict greater postoperative pain and analgesic use.246,247 Meta-analyses demonstrate that preoperative anxiety increases anesthetic (SMD 0.67) and analgesic needs (SMD 0.89), prolongs recovery and raises the risk of postoperative delirium (OR 1.90) in adults.248 These findings underscore the need for individualized anesthetic management and integrated perioperative psychological assessment.249,250
Psychological strategies—including pre- and postoperative education, cognitive behavioral therapy(CBT),239 and distraction methods—may reduce reliance on analgesics. CBT effectively mitigates postoperative anxiety and depression, particularly in older women, but its influence on pain scores is less definitive.251 Evidence for psychological preparation and acupuncture remains mixed.239,252 Techniques such as guided imagery, relaxation, hypnosis, intraoperative suggestions, and music therapy show potential, yet implementation is constrained by institutional barriers, including nurse workload, time limitations, and insufficient training.94,253 Overall, non-pharmacological strategies play a safe and valuable adjunctive role within multimodal analgesia, although heterogeneous interventions and patient populations limit generalizability and highlight the need for standardized protocols integrated with pharmacologic care. Evidence suggests that perioperative education, empathetic communication, and avoidance of nocebo language can improve pain control, reduce opioid use, and shorten hospital stay. Mindfulness and cognitive behavioral therapy support recovery, physical therapy enhances function, and modalities such as cryotherapy, acupuncture, and TENS provide modest, procedure-specific analgesic benefits.254 Despite growing evidence that psychological interventions and structured patient education can reduce perioperative pain and anxiety, their routine incorporation into anesthetic practice is variable, and their clinical impact is maximized when delivered alongside established pharmacological analgesic strategies rather than as standalone approaches.87
Pharmacist Contributions to Perioperative Pain Management
Clinical pharmacists are increasingly recognized as essential members of perioperative care teams, improving the quality, safety, and effectiveness of multimodal analgesia. Multisite quality initiatives demonstrate that pharmacist-led perioperative pain management delivers individualized analgesic strategies, mitigates opioid-related risks, and achieves high adherence to guideline-recommended practices, with strong endorsement from orthopedic and surgical teams.255–257
Integration of pharmacists into transitional perioperative care enhances continuity across surgical phases, enabling tailored analgesic planning and patient-centered interventions, which improve satisfaction among both patients and providers.256 Effective multimodal and opioid-sparing analgesia relies not only on evidence-based drug selection but also on reliable, patient-specific implementation; pharmacists facilitate this process by optimizing medication regimens, monitoring for adverse drug reactions, and supporting opioid stewardship within interdisciplinary teams.255,256
Evidence demonstrates tangible clinical benefits. Pharmacist-led perioperative pharmaceutical care in orthopedic surgery reduced postoperative pain scores and shortened hospital stay by an average of 2.3 days, without compromising breakthrough pain control or safety.258 In ambulatory surgery, pharmacist consultations decreased moderate-to-severe postoperative pain by 17% and reduced mean pain scores by 0.9 points.259 Pharmacist interventions also reduce medication errors, enhance adherence to protocols, and improve overall perioperative safety through multicomponent strategies including medication reconciliation, staff education, and patient counseling.260,261 Despite growing evidence, implementation remains inconsistent. Surveys indicate that while most pharmacists support involvement in postoperative pain management, actual engagement is limited due to a lack of standardized protocols, systematic training, and structured workflows.262 Evidence gaps persist regarding chronic disease management, development processes for interventions, and the long-term impact of pharmacist integration on patient-centered outcomes.263 Collectively, these data highlight the transformative role of clinical pharmacists in perioperative care. Their integration supports individualized, multimodal analgesia, enhances interprofessional collaboration, reduces opioid exposure, and strengthens patient safety. Structured programs and professional education are essential to maximize pharmacists’ impact, standardize care delivery, and promote sustainable, high-quality perioperative pain management.264
Personalized and Precision Multimodal Approaches to Perioperative Pain Management
Personalized Multimodal Perioperative Pain Management
Postoperative pain remains a major clinical challenge despite advances in analgesic strategies. Retrospective studies show that preoperative opioid or benzodiazepine use, smoking, and obesity increase postoperative opioid requirements, while age and sex have minimal impact.265 Evidence for preemptive opioids is limited. A Cochrane review of 20 RCTs (1,343 participants) found modest reductions in postoperative pain but no clear benefit for preventive opioids (Figure 1). Adverse events were underreported, highlighting the need for high-quality trials.266 Guidelines from the American Pain Society recommend multimodal analgesia for all surgeries, targeting multiple pain pathways and accounting for interindividual variability, including pharmacogenetic differences in opioid metabolism and pain sensitivity (Figure 3).267 Prospective studies, such as a post-cesarean cohort in Uganda, reveal gaps in care: pain peaked six hours postoperatively (median 37/100), and 32% of patients reported inadequate analgesia despite standard regimens.268 Personalized multimodal strategies improve recovery by integrating biological, psychological, and social determinants of pain. Interventions such as dynamic monitoring, virtual reality therapies, and prehabilitation reduce pain scores, opioid use, and hospital stay. AI-supported decision tools and standardized protocols have the potential to enhance these outcomes further.269







Minimally invasive procedures, including arthroscopic surgery, benefit from opioid-sparing multimodal approaches. NSAIDs, acetaminophen, gabapentinoids, and local anesthetics reduce opioid exposure while enhancing functional recovery. Randomized trials show nonopioid multimodal regimens lower pain scores (VAS, PROMIS-PI) and adverse effects compared with opioid-based therapy.270,271 Limiting opioid exposure is critical, given the U.S. overdose crisis, with 94,000 deaths in 2020. Evidence-based prescribing, procedure-specific pill counts, and standardized care pathways are essential for safe postoperative management.272 Provider knowledge impacts outcomes. In a study of 72 ICU nurses, only 21.6% applied behavioral pain scales for non-communicative patients, despite universal use of standard scales. Knowledge gaps correlated with gender, education, and prior pain training, highlighting the need for structured education and broader adoption of validated assessment tools.273 Perioperative pain management is evolving toward patient-centered, individualized care. Personalized strategies consider comorbidities, psychological status, and pain sensitivity to optimize recovery and reduce complications. Multimodal, individualized care can lower pain scores by 20–30%, opioid use by 25–40%, and hospital stay by 1–2 days.269,274
Despite over 800 primary studies and 107 systematic reviews, critical gaps remain. Evidence is limited regarding optimal patient education, nonpharmacological interventions, analgesic combinations, monitoring of treatment response, neuraxial and regional techniques, and care delivery models.275 Quality metrics are also insufficient: of 19 identified measures, only five are endorsed by the National Quality Forum. None specifically targets postoperative pain, and only three non-endorsed measures address it, highlighting a lack of standardized benchmarks.276,277
Pharmacogenomic-Guided Multimodal Analgesia
Pharmacogenomics addresses a critical gap in perioperative pain management by accounting for genetically mediated differences in pharmacokinetics, pharmacodynamics, and pain perception.71,72 Adverse drug reactions—many of which are genetically influenced—remain a major source of preventable morbidity, mortality, and healthcare expenditure, with their true burden likely underestimated due to underreporting.61 Although pharmacy-related costs account for less than 5% of total surgical expenditure, inadequately controlled postoperative pain substantially increases overall costs through prolonged hospitalization, delayed functional recovery, and progression to chronic pain, supporting the economic rationale for targeted pharmacogenomic testing in selected patient populations.61
Randomized and observational studies increasingly demonstrate that pharmacogenetic-guided multimodal analgesia is associated with reductions in postoperative pain scores and opioid consumption, particularly among patients harboring actionable genetic variants.278,279 When integrated with clinical risk stratification tools and guideline-endorsed multimodal analgesic strategies,267,280,281 pharmacogenomic-informed care represents a scalable, evidence-based pathway toward precision perioperative pain management.
Patient-Controlled Analgesia Within Personalized Pain Pathways
Patient-controlled analgesia (PCA) remains a cornerstone of acute postoperative pain management, enabling individualized, on-demand opioid delivery for surgical, trauma-related, and chronic pain in both adults and children older than five years.282 Its widespread use in perioperative care reflects its ability to reduce the analgesic “perception–delivery gap”; however, clinical outcomes are highly dependent on opioid selection, pump programming, and patient-specific factors.283 Hydromorphone and sufentanil are among the most commonly administered opioids for PCA, yet direct comparative evidence regarding their postoperative efficacy and safety remains limited, with available studies yielding inconsistent results.283 Opioid-induced pruritus—particularly frequent with morphine—often necessitates opioid rotation, with hydromorphone frequently favored because of its comparatively improved tolerability profile.284
Comparative studies demonstrate that hydromorphone- and sufentanil-based IV-PCA generally provide similar analgesic efficacy across diverse surgical contexts.285,286 Notably, in colorectal cancer surgery, hydromorphone improved mood recovery at 48–96 hours yet increased pruritus and nausea relative to sufentanil,286 underscoring the nuanced balance between analgesic benefit and tolerability. Randomized evidence further suggests that fentanyl–ketamine IV-PCA may serve as a viable alternative to thoracic epidural analgesia after minimally invasive thoracic surgery; both techniques produced comparable analgesia and adverse effect profiles, though fk-IVPCA resulted in more early postoperative demands.287 These findings highlight the growing role of multimodal PCA strategies, particularly in settings where epidural analgesia is contraindicated or technically challenging. Despite its advantages, PCA is not without risk. Sufentanil, while potent, may induce respiratory depression and thereby jeopardize postoperative safety, particularly in high-risk surgical populations.288 Moreover, many PCA-related complications including programming errors, excessive dosing, and respiratory depression stem from human factors rather than the device itself,282 highlighting the need for standardized training and monitoring.
Recent pediatric data illustrate the potential benefits of opioid-sparing PCA strategies: nalbuphine/dexmedetomidine PCIA supported superior hemodynamic stability, analgesia, sedation, and stress control compared with sufentanil/dexmedetomidine in tonsillectomy, with fewer adverse reactions.289 Age also modifies PCA pharmacodynamics: younger recipients of fentanyl PCA have higher rescue analgesic requirements—attenuated by ketorolac—whereas older adults benefit from prophylactic antiemetics such as ramosetron.290 Incorporating adjunct non-opioid analgesics (paracetamol, NSAIDs, local anesthetics, ketamine, tramadol) effectively reduces opioid consumption but demands caution in patients receiving concurrent sedatives or with renal/hepatic dysfunction due to metabolite accumulation (eg, morphine (M3G, M6G) and hydromorphone (H3G).291
Common opioid-related side effects sedation, nausea, vomiting, and pruritus typically remain manageable with dosage adjustment or supportive medication,292,293 though constipation and urinary retention warrant ongoing surveillance.293 Importantly, emerging evidence questions routine PCA use in certain low-to-moderate pain surgeries: in laparoscopic cholecystectomy, morphine PCA was associated with delayed recovery, impaired alertness, and significantly higher postoperative nausea and vomiting compared with non-PCA protocols.294 These findings suggest that reflexive postoperative PCA prescribing may be inappropriate in procedures with predictable, mild-to-moderate pain trajectories. Basal opioid infusion via IV-PCA was previously used to enhance postoperative pain control; however, it does not improve pain or sleep quality and increases opioid-related side effects.295 A meta-analysis of 796 patients showed basal IV-PCA significantly raises respiratory depression risk, leading to recommendations against its routine use.296 Despite this, basal fentanyl infusion in IV-PCA continues in practice.295 Most existing evidence comes from morphine-based IV-PCA studies with small sample sizes, highlighting the need for research on the risks and benefits specific to fentanyl’s distinct pharmacokinetics.295
PCA provides superior postoperative pain relief and patient satisfaction compared to traditional methods, allowing self-titration and immediate analgesia. Morphine is first-line; alternatives include hydromorphone and fentanyl. PCA should integrate non-opioid analgesics, with careful monitoring for sedation, respiratory status, and side effects.297 Special considerations apply for pediatric, elderly, and emergency surgery patients, emphasizing education and safety protocols.297,298 Smart pump technology enhances safety by reducing errors, but proxy use, continuous infusions, or programming mistakes pose risks. Optimizing outcomes requires standardized protocols, staff training, and a multidisciplinary approach integrating technology, clinical oversight, and procedural rigor.298
Machine Learning in Postoperative Pain Management
Recent studies have applied machine learning (ML) to personalize perioperative and postoperative pain management, enabling individualized analgesic strategies that account for patient variability in pain response and opioid effectiveness. The OPIAID algorithm leverages observational electronic health record data and causal modeling to predict optimal opioid doses based on patient characteristics, intraoperative factors, and opioid type, aiming to maximize analgesia while minimizing opioid-related adverse events.299 The Interpretable Neural Network Regression (INNER) model combines deep neural networks with traditional statistical methods to assess preoperative opioid use risk. Applied to 34,186 surgical patients, INNER generated interpretable, patient-specific risk estimates, identified key predictive factors, and supported evidence-based individualized pain management.300
In obstetric populations, ML models such as XGBoost have been used to optimize post-cesarean pain management. Among multiple models tested, XGBoost performed best, highlighting critical predictors including anesthesia type and adjunctive analgesics such as esketamine, thereby facilitating tailored analgesic protocols.301 Similarly, gradient boosting models in major abdominal surgery integrated demographic, clinical, genetic, and psychosocial variables to predict severe postoperative pain with 83.7% accuracy, enabling preemptive, personalized pain management.302 Ensemble ML approaches have also been applied in spine surgery. Stacking classifiers effectively predicted postoperative axial pain intensity in 484 patients with degenerative cervical myelopathy, achieving an AUC of 0.91, while ensemble models forecasted 1-year functional recovery (Japanese Orthopedic Association scores) in 672 patients, providing clinicians with interpretable, patient-specific insights for optimized pain management and resource allocation.303,304 Overall, ML and artificial intelligence techniques provide robust tools for objective pain assessment, identification of high-risk patients, and integration of precision analgesic strategies. Across diverse surgical populations, these approaches enhance the ability to predict pain trajectories, tailor opioid and multimodal analgesia, and improve perioperative outcomes.305
Recent studies have developed multimodal machine learning frameworks for objective postoperative pain assessment using biosignals such as ECG, EMG, EDA, and respiration. In a cohort of 25 patients, these models achieved over 80% balanced accuracy, with respiration signals most effective for low pain and EMG for high pain, demonstrating feasibility for real-world clinical monitoring.306 Similarly, automated pain assessment using galvanic skin response (GSR) in 25 non-communicative postoperative adults achieved up to 86% accuracy with random forest and k-nearest-neighbor classifiers, outperforming previous approaches.307 Despite their promise, high costs and technical complexity—including real-time monitoring, AI-driven analytics, pharmacogenomic integration, and wearable sensors—remain significant barriers to widespread adoption, particularly in low-resource healthcare settings.269
Digital and Wearable Innovations in Pain Monitoring and Management
Wearable devices and digital health technologies enable real-time monitoring, objective assessment, and personalized interventions for chronic and postoperative pain.308–315 Many studies link physiological markers with pain. Traditional models such as Random Forest and multilevel models perform reliably. Advanced models face challenges with data quality and computational demands. Integrating multimodal data and enhancing data security could improve predictive accuracy and clinical utility.308
Integration of wearables with electronic health records (EHRs), especially Epic systems, is increasing. Partnerships between start-ups and health systems have improved data capture and provider workflows. Insurance programs also incentivize wearable use. Remaining challenges include privacy, interoperability, and data overload.309 Pain assessment in children is challenging due to its subjective nature. Validated tools enable accurate postoperative pain evaluation, improving comfort and recovery.310 Parents often under-treat pain at home. Factors such as age, development, language, cultural beliefs, and biology influence management. Using multiple assessment tools with technology supports effective pediatric pain care.311 Technology-based interventions—including apps, virtual reality, and wearables—reduce postoperative pain scores in children, as shown in a meta-analysis of 14 RCTs.312
Digital therapeutics, including virtual reality and mobile applications, improve opioid-based pain management as adjuncts, demonstrating better pain scores in randomized trials. They provide opportunities to enhance patient-centered care and integrate with pharmacotherapy.316 Researchers at WashU developed an uncertainty-aware machine learning model using preoperative surveys and clinical data to predict risk, offering clinicians both probability and confidence estimates.55 However, precision perioperative medicine applies genetics, pharmacogenomics, and predictive analytics to personalize anesthetic care, optimize drug dosing, anticipate complications, and enhance pain management, thereby improving safety, recovery, and patient-centered outcomes.317
Wearables combined with ecological momentary assessment can track activity, physiological signals, and pain in real-world settings. These tools generate reproducible biosignals and clinically meaningful endpoints.313 AI and machine learning enable dynamic, patient-specific pain management. By analyzing large datasets, these systems predict pain trajectories, optimize medications, reduce side effects, and enhance recovery.314
Chronic pain often disrupts physical and cognitive function. Conventional therapies are limited and may have side effects. Neuromodulation approaches—including SCS, TENS, NMES, and AI-driven platforms like EcoAI—offer adaptive, personalized treatment. Combined with remote monitoring and closed-loop feedback, these strategies support scalable, precision-based pain management. Future work should focus on validated biomarkers and equitable implementation.315
Limitations and Safety Considerations of Systemic Analgesics
Opioids remain indispensable for controlling severe postoperative pain, yet their use is constrained by well-documented adverse effects including nausea, vomiting, constipation, and respiratory depression, with an ongoing risk of misuse even in short-term perioperative settings.318 Despite their theoretical utility, gabapentinoids such as gabapentin and pregabalin have demonstrated limited clinical efficacy in postoperative pain, with meta-analyses indicating minimal analgesic benefit and increased risks of dizziness and visual disturbances, challenging their routine use despite potential opioid-sparing properties.173,319 This highlights the need for careful patient selection and reconsideration of gabapentinoid use in standard postoperative protocols.
Esmolol, an ultra–short-acting selective β-blocker (0.5 mg/kg loading, then 5 μg/kg/min IV), is used for perioperative analgesia, possibly via central G-protein activation. It enhances pain control and hemodynamic stability while reducing opioid and anesthetic requirements, though excessive dosing can cause bradycardia and hypotension.320 A systematic review and meta-analysis of 19 placebo-controlled trials (1,028 patients) demonstrated that intraoperative esmolol reduced opioid use by 32% intraoperatively and 38.6% postoperatively, improved early postoperative pain scores, and lowered heart rate and mean arterial pressure without inducing clinically significant hypotension or bradycardia, confirming its role as an effective opioid-sparing adjunct in multimodal anesthesia.321
For dexamethasone, major gaps remain regarding its precise analgesic mechanisms, the relative roles of systemic versus perineural effects in nerve block prolongation, optimal dosing, efficacy in preventing persistent postoperative pain, and long-term safety across surgical populations.320 Rebound pain after single-shot interscalene block affects about one-third of patients. In a factorial RCT of 160 shoulder arthroscopy patients, intravenous dexamethasone reduced both pain escalation and severe rebound pain, whereas esketamine alone had no preventive effect.322 In a separate RCT of 200 patients, intravenous esketamine did not reduce rebound pain incidence (~25%) but significantly improved pain scores at 8–24 hours and enhanced intraoperative hemodynamic stability without serious adverse events.323 These findings underscore the need for further research to clarify dosing strategies, mechanisms, and long-term outcomes of these adjuncts in multimodal analgesia.
Intravenous lidocaine, while effective in specific patient subsets, carries substantial risk and demands strict dosing and monitoring protocols, limiting its broad applicability.6 Evidence indicates that combining acetaminophen with NSAIDs yields superior analgesia without amplifying adverse effects, reinforcing the central role of multimodal, non-opioid strategies.324 Non-opioid analgesics, including acetaminophen, NSAIDs, and coxibs, effectively modulate nociceptive pathways but require caution in populations with comorbidities such as renal impairment.93,121 Antidepressants, particularly tricyclic antidepressants (TCAs), may provide adjunctive benefits in pain management through modulation of serotonergic and noradrenergic systems, underscoring the interplay between pain and mood regulation.325
Multimodal analgesia has emerged as the evidence-based standard for postoperative pain management, optimizing efficacy while reducing opioid consumption and associated adverse outcomes.326 The greatest opioid-sparing effects were observed with NSAIDs combined with dexamethasone or regional anesthesia, while acetaminophen contributed less benefit.17 The findings reinforce the effectiveness of multimodal analgesia and support prioritizing NSAIDs and dexamethasone within perioperative pain management protocols.17 Multimodal postoperative analgesia combines pharmacological strategies (opioids, non-opioids, neuraxial and regional techniques, surgical-site infiltration) with non-pharmacological adjuncts such as acupuncture, music therapy, TENS, and hypnosis, which are generally safe but supported by mixed evidence.327 Although guidelines advocate individualized, preplanned multimodal analgesia, fewer than half of surgical patients achieve adequate pain control, reflecting limited high-quality evidence and suboptimal implementation.239 In primary total knee arthroplasty, evidence supports a combination of preoperative and intraoperative strategies—including paracetamol, NSAIDs, adductor canal block, local infiltration analgesia, and dexamethasone—while limiting postoperative opioid use. Certain interventions, including gabapentinoids, ketamine, and select nerve blocks, may offer minimal additional benefit and could introduce risk, reflecting the need for individualized, evidence-driven protocols.328 Importantly, opioid combination therapy has been associated with increased mortality compared to monotherapy, emphasizing the clinical imperative of judicious use.329
Local anesthetics provide potent, targeted analgesia with fewer systemic effects, and techniques such as epidural and paravertebral blocks reduce chronic postsurgical pain following thoracotomy and breast surgery.330,331 Complementary and alternative therapies are widely used but are supported by limited or variable evidence, reinforcing their role as adjuncts rather than primary strategies.332 Non-pharmacologic modalities, including physical therapy, acupuncture, electrical stimulation, cold therapy, and CBT, demonstrate potential in optimizing pain outcomes, particularly when integrated into multimodal frameworks.333
The strategic combination of opioids and non-opioids, exploiting distinct mechanisms, provides additive or synergistic analgesic effects and reduces single-agent toxicity(Figure 2).69 Safety data from MNK-155 studies indicate substantial TEAEs, though consistent with low-dose opioid/APAP regimens, highlighting the need to balance efficacy and tolerability.334 Combined oxycodone and flurbiprofen axetil therapy exemplifies effective multimodal postoperative pain control, providing both analgesic and anti-inflammatory effects.335 Certain patient populations warrant additional scrutiny. SSRIs increase bleeding risk with NSAID co-administration, mandating alternative antidepressants for high-risk individuals.336 Bariatric surgery alters drug pharmacokinetics, requiring individualized analgesic strategies; NSAIDs are contraindicated after gastric bypass due to ulceration risk, while monitoring remains critical even for sleeve gastrectomy patients.337–339
Peripheral nerve blocks remain a cornerstone in reducing perioperative opioid requirements, particularly within the first 72 hours; however, rebound hyperalgesia may paradoxically increase opioid consumption, highlighting the complexity of postoperative analgesia.11,340 Anesthetic co-adjuvants, including clonidine, dexmedetomidine, ketamine, and magnesium sulfate, offer mechanistic benefits such as improved analgesic efficacy and intraoperative hemodynamic stability, yet their clinical value is heterogeneous and procedure-dependent.165 Opioid-gabapentinoid combinations, while mitigating gastrointestinal side effects, may exacerbate CNS depression and mortality, particularly in cancer patients, underscoring the need for risk-stratified application.329 Adjunctive postoperative pain management includes physiotherapy and diverse non-pharmacological strategies that are low-cost, low-risk, and easy to implement. Although evidence is insufficient to recommend surgery-specific approaches, commonly used methods include physical modalities (TENS, acupuncture, heat/cold), physical activity, psychological or spiritual techniques (CBT, meditation), and distraction. Patient education and multidisciplinary care further enhance pain control.104 Optimizing postoperative pain depends on personalized, evidence-based multimodal analgesia integrating pharmacological, regional, and non-pharmacological strategies. Important gaps persist in evaluating optimal combinations and high-risk groups. Effective perioperative pain care requires dedicated pain teams, function-focused assessment, preoperative risk screening, shared decision-making, judicious opioid use, and standardized discharge planning to improve outcomes.254
Post-Discharge Multimodal Analgesia: Opportunities for Optimization
Despite the proliferation of ERAS protocols, most research remains confined to inpatient care, leaving post-discharge multimodal analgesia (MMA) poorly characterized.341 This gap contributes to suboptimal pain control, ongoing opioid use, and risk of chronic postsurgical pain(Figure 1). Standardization of analgesic regimens beyond the immediate postoperative period is lacking, and evidence for balancing effective pain relief with minimal opioid exposure remains limited.341,342 Heterogeneous study designs, variable protocols, and inconsistent outcome reporting further constrain interpretation and generalizability across procedures and institutions.342,343
Optimal analgesic strategies for high-risk or complex surgeries remain controversial. While neuraxial techniques, including epidurals, reliably reduce pain scores, they do not consistently affect morbidity or length of stay.344 Emerging regional techniques show promise, but few large, procedure-specific RCTs exist to establish best practices. Moreover, patient-centered outcomes—including psychosocial factors, quality of life, and long-term recovery—are rarely evaluated, limiting the understanding of multimodal analgesia’s broader impact.18,345 Post-discharge pain management is especially inconsistent. Scoping reviews identify gaps in patient education, continuity of care, individualized analgesic planning, and knowledge translation.346 High-quality studies are needed to define procedure-specific multimodal regimens, integrate non-pharmacologic adjuncts such as physical therapy and digital tools, and evaluate the long-term efficacy and safety of MMA strategies.18,347
Evidence supports certain pharmacologic components—acetaminophen, NSAIDs, and ketamine—as effective opioid-sparing agents with favorable safety profiles (Tables 1–3).348 Conversely, gabapentinoids and α2-agonists pose sedation risks, and evidence for lidocaine, corticosteroids, and other agents remains inconsistent.348 Despite widespread adoption of multimodal strategies, implementation is uneven, and postoperative pain care is often dictated by individual clinician preference rather than standardized, evidence-based protocols.18,349 Pharmacogenetics and precision medicine offer opportunities to individualize analgesic therapy, identifying high-risk patients and optimizing opioid efficacy while minimizing adverse effects.78,350–352 Although biologically plausible and supported by observational data, clinical adoption remains limited by knowledge gaps, inconsistent evidence, lack of standardized protocols, and reimbursement barriers.78,351 Genetic variability clearly affects postoperative pain outcomes, yet actionable guidance has not yet been integrated into routine clinical practice.353 Despite widespread advocacy of multimodal analgesia, structured quality measures, standardized protocols, and systematic incorporation of non-pharmacologic and digital adjuncts are lacking, limiting reproducibility and optimization of postoperative outcomes. Emerging technologies and holistic approaches show promise, but implementation evidence is sparse, highlighting a critical need for standardized frameworks, validated metrics, and high-quality trials to evaluate integration across settings.269,276 Collectively, these observations highlight critical priorities for future research: standardized post-discharge MMA protocols, robust procedure-specific RCTs, integration of psychosocial and non-pharmacologic interventions, and precision approaches incorporating pharmacogenetic and AI-driven tools to optimize pain control, minimize opioid exposure, and enhance recovery.
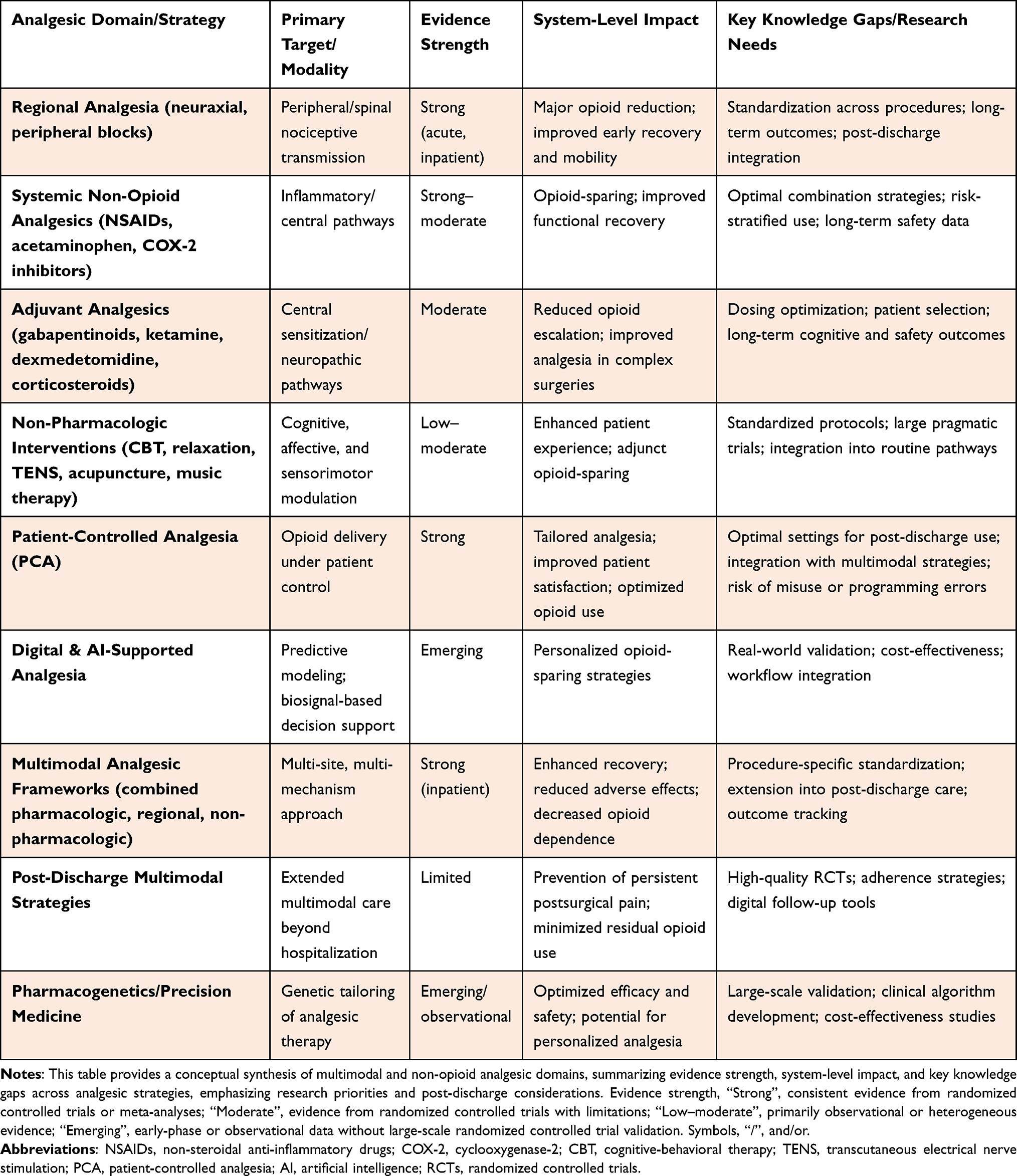 |
Table 3 Strategic Overview of Multimodal and Non-Opioid Postoperative Pain Management |
Limitations of Current Evidence and Future Directions
Despite substantial advances in perioperative pain management, critical gaps remain in the evidence base supporting multimodal analgesia. Most studies focus on inpatient care, with limited high-quality evidence addressing post-discharge pain management, leaving patients at risk for inadequate analgesia, persistent opioid use, and chronic postsurgical pain (Figure 1). Standardized, procedure-specific protocols tailored to diverse surgical populations are scarce, and long-term outcomes—such as functional recovery, quality of life, and chronic pain prevention—are insufficiently studied. Heterogeneity in study design, patient populations, outcome measures, and analgesic components further limits meta-analysis and consensus on optimal strategies. The efficacy of adjunctive agents—including,NSAIDS, gabapentinoids, ketamine, and selected non-pharmacologic interventions—remains inconsistent. Regional and neuraxial analgesic techniques, while effective, are influenced by technical variability, rebound hyperalgesia, and adverse effects. Psychological and physical modalities demonstrate variable benefits, often dependent on patient engagement and implementation fidelity.
Emerging digital and precision technologies, such as machine learning–based risk stratification, biosignal-guided pain assessment, wearable monitoring, and AI-driven decision support, provide opportunities to tailor analgesia across inpatient and post-discharge phases. However, adoption is limited by cost, technical complexity, interoperability challenges, and lack of long-term outcome data. System-level barriers—including inconsistent clinician training, underutilization of validated pain metrics, and absence of standardized quality indicators—further hinder optimal implementation.
Addressing these gaps requires high-quality, multicenter studies that evaluate post-discharge multimodal analgesia, integrate personalized and pharmacogenomic-guided strategies, and assess long-term outcomes. Evidence-informed, procedure-specific frameworks should combine pharmacologic, regional, and non-pharmacologic modalities, incorporate validated metrics, and support seamless transitions from hospital to home care. Embedding these strategies into guidelines and quality improvement initiatives is essential to enhance analgesic efficacy, reduce opioid exposure, and achieve sustainable, patient-centered perioperative pain management.
Conclusion
Achieving durable functional recovery necessitates a fundamental reorientation from opioid-dependent analgesia toward individualized, multimodal perioperative care —one that demonstrably reduces opioid consumption, mitigates adverse effects, and addresses the biopsychosocial complexity of surgical pain across the full continuum of care. Despite compelling inpatient evidence supporting this transition, critical deficiencies persist in post-discharge standardization, long-term functional recovery, and chronic postsurgical pain prevention — domains where current clinical practice remains insufficient relative to patient burden. Pharmacogenomic-guided prescribing, machine learning–based risk stratification, and wearable monitoring platforms represent promising precision-based frontiers, yet their clinical integration remains contingent upon robust validation, interoperability, and the seamless transition of data between surgical and primary care teams. Realizing the full potential of multimodal analgesia demands procedure-specific, evidence-informed protocols embedded within interdisciplinary care frameworks — bridging the persistent discontinuity between effective inpatient analgesia and the largely unstructured postoperative recovery that follows hospital discharge.
Data Sharing Statement
This study relies on published data, so availability is not applicable.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests in this work.
References
1. Liu C, Chen X, Wu S. The effect of massage therapy on pain after surgery: a comprehensive meta-analysis. ComplTherap Med. 2022;71(October):102892. doi:10.1016/j.ctim.2022.102892
2. Thiel B, Godfried MB, Koopman SJHA, et al. A multicenter analysis of registry data on postoperative orthopedic pain: a retrospective cohort study. BMC Anesthesiol. 2025;25(1):338. doi:10.1186/s12871-025-03212-w
3. Park R, Mohiuddin M, Arellano R, Pogatzki-Zahn E, Klar G, Gilron I. Prevalence of postoperative pain after hospital discharge: systematic review and meta-analysis. Pain Rep. 2023;8(3):e1075. doi:10.1097/PR9.0000000000001075
4. Carr DB, Goudas LC. Acute pain. Lancet. 1999;353(9169):2051–40. doi:10.1016/S0140-6736(99)03313-9
5. Apfelbaum JL, Gan TJ, Chen C. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. 2003:534–540. DOI:10.1213/01.ANE.0000068822.10113.9E
6. Foo I, Macfarlane AJR, Srivastava D, et al. The use of intravenous lidocaine for postoperative pain and recovery: international consensus statement on efficacy and safety. Anaesthesia. 2021;76(2):238–250. doi:10.1111/anae.15270
7. Kaye AD, Urman RD, Rappaport Y, et al. Multimodal analgesia as an essential part of enhanced recovery protocols in the ambulatory settings. J Anaesthesiol Clin Pharmacol. 2019;35(Suppl 1):S40–S45. doi:10.4103/joacp.JOACP_51_18
8. Fitzgerald A. Timefor nonaddictive relief of pain Greater insight into the biology of pain will likely identify potential drug targets.
9. Zheng J, Du L, Chen G, Zhang L, Deng X, Zhang W. Efficacy of pericapsular nerve group (PENG) block on perioperative pain management in elderly patients undergoing Hip surgical procedures: a protocol for a systematic review with meta-analysis and trial sequential analysis. BMJ open. 2023;13(1):e065304. doi:10.1136/bmjopen-2022-065304
10. Freo U. Paracetamol for Multimodal Analgesia. Pain Management. 2022;12(6):737–750. doi:10.2217/pmt-2021-0116
11. Cardwell TW, Zabala V, Mineo J, Ochner CN. The effects of perioperative peripheral nerve blocks on peri- and postoperative opioid use and pain management. American Surgeon. 2022;88(12):2842–2850. doi:10.1177/00031348211023395
12. Frauenknecht J, Kirkham KR, Jacot-Guillarmod A, Albrecht E. Analgesic impact of intra-operative opioids vs. opioid-free anaesthesia: a systematic review and meta-analysis. Anaesthesia. 2019;74(5):651–662. doi:10.1111/anae.14582
13. Stevens J, Trimboli A, Samios P, et al. A sustainable method to reduce postoperative oxycodone discharge prescribing in a metropolitan tertiary referral hospital. Anaesthesia. 2019;74(3):292–299. doi:10.1111/anae.14570
14. Mariano ER, Dickerson DM, Szokol JW, et al. A multisociety organizational consensus process to define guiding principles for acute perioperative pain management. Reg Anesth Pain Med. 2022;47(2):118–127. doi:10.1136/rapm-2021-103083
15. Wang Q, Ma T, Wang L, Zhao C, Kang P. Efficacy of adding acetaminophen to preemptive multimodal analgesia in total knee arthroplasty: a double-blinded randomized study. Orthopaedic Surgery. 2023;15(9):2283–2290. doi:10.1111/os.13780
16. Tompkins DM, DiPasquale A, Segovia M, Cohn SM. Review of intravenous acetaminophen for analgesia in the postoperative setting. The American SurgeonTM. 2021;87(11):1809–1822. doi:10.1177/0003134821989056
17. Graham LA, Illarmo S, Wren SM, Mudumbai SC, Odden MC. Optimal multimodal analgesia combinations to reduce pain and opioid use following non-cardiac surgery: an instrumental variable analysis. Reg Anesth Pain Med. 2025. doi:10.1136/rapm-2025-106720
18. Lopez BM, Lee BM, Miller MD, Ibrahim M, Vanderah TW, Riegel A. Postoperative multimodal pain management: a narrative review of current practices, clinical and educational gaps, and future directions. Front Anesthesiol. 2025;4. doi:10.3389/fanes.2025.1709252
19. Wynne R, Jedwab RM, Gjeilo KH, et al. A systematic review of multimodal analgesic effectiveness on acute postoperative pain after adult cardiac surgery. J Adv Nurs. 2025;81(5):2757–2792. doi:10.1111/jan.16688
20. Ode K, Selvaraj S, Smith AF. Monitoring regional blockade. Anaesthesia. 2017;72 Suppl 1:70–75. doi:10.1111/anae.13742
21. Bottomley T, Gadsden J, West S. The failed peripheral nerve block. BJA Educ. 2023;23(3):92–100. doi:10.1016/j.bjae.2022.12.002
22. Ko S, Jun CM, Min WK, et al. Pain relief after selective nerve root block as a predictor of postoperative functional outcome in patients with degenerative lumbar spinal stenosis patients undergoing decompressive surgery. Spine. 2022;47(9):666–671. doi:10.1097/BRS.0000000000004216
23. Sort R, Brorson S, Gögenur I, Nielsen JK, Møller AM. Rebound pain following peripheral nerve block anaesthesia in acute ankle fracture surgery: an exploratory pilot study. Acta Anaesthesiologica Scandinavica. 2019;63(3):396–402. doi:10.1111/aas.13290
24. Choi YH, Kim DH, Paik NJ, Park J. Long-term analgesic effects of peripheral nerve block in patients with central post-stroke pain: a retrospective series. Pain Practice. 2021;21(8):843–849. doi:10.1111/papr.13031
25. Luebbert E, Rosenblatt MA. Postoperative rebound pain: our current understanding about the role of regional anesthesia and multimodal approaches in prevention and treatment. Curr Pain and Headache Rep. 2023;27(9):449–454. doi:10.1007/s11916-023-01136-z
26. Bayman EO, Brennan TJ. Incidence and severity of chronic pain at 3 and 6 months after thoracotomy: meta-analysis. J Pain. 2014;15(9):887–897. doi:10.1016/j.jpain.2014.06.005
27. S Y, I H, S M, et al. Prevalence and risk factors of chronic postsurgical pain after lung cancer surgery and knee arthroplasty: a prospective multicenter cohort study in Japan. J Anesth. 2025;39(4). doi:10.1007/s00540-025-03494-x
28. Khan JS, Dana E, Xiao MZX, et al. Prevalence and risk factors for chronic postsurgical pain after thoracic surgery: a prospective cohort study. J Cardiothorac Vasc Anesth. 2024;38(2):490–498. doi:10.1053/j.jvca.2023.09.042
29. Guy GP, Miller GF, Legha JK, et al. Economic Costs of Chronic Pain-United States, 2021. Med Care. 2025;63(9):679–685. doi:10.1097/MLR.0000000000002181
30. Gaskin DJ, Richard P. The Economic Costs of Pain in the United States. In Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. National Academies Press (US); 2011 https://www.ncbi.nlm.nih.gov/books/NBK92521/.
31. Parsons B, Schaefer C, Mann R, et al. Economic and humanistic burden of post-trauma and post-surgical neuropathic pain among adults in the United States. J Pain Res. 2013;6:459–469. doi:10.2147/JPR.S44939
32. Phillips DM, Chapman CR. opioids JCAHO pain management. 2016;284(4).
33. Kozol RA, Voytovich A. Misinterpretation of the fifth vital sign. Archives of Surgery. 2007;142(5):417–419. doi:10.1001/archsurg.142.5.417
34. Manchikanti L, Helm S, Fellows B, et al. Opioid epidemic in the United States. Pain Physician. 2012;15(3):ES9–ES38. doi:10.36076/ppj.2012/15/es9
35. Engla NEW, Journal ND. New Engla Nd Journal. 2010;1981–1985
36. CDC. Understanding the opioid overdose epidemic. overdose prevention. 2025. Available from: https://www.cdc.gov/overdose-prevention/about/understanding-the-opioid-overdose-epidemic.html.
37. CDC. SUDORS dashboard: fatal drug overdose data. overdose prevention. 2025. Available from: https://www.cdc.gov/overdose-prevention/data-research/facts-stats/sudors-dashboard-fatal-overdose-data.html.
38. Feinglass J, Walker G, Khazanchi R, Rydland K, Tessier RA, Mason M. Community versus hospital opioid-related overdose deaths in illinois. Public Health Rep. 2022;137(2):291–300. doi:10.1177/0033354921994901
39. Abbasi AB, Salisbury-Afshar E, Jovanov D, et al. Health care utilization of opioid overdose decedents with no opioid analgesic prescription history. J Urban Health. 2019;96(1):38–48. doi:10.1007/s11524-018-00329-x
40. Shanahan CW, Reding O, Holmdahl I, et al. Opioid analgesic use after ambulatory surgery: a descriptive prospective cohort study of factors associated with quantities prescribed and consumed. BMJ Open. 2021;11(8):e047928. doi:10.1136/bmjopen-2020-047928
41. Shankar DS, Kim J, Bienstock DM, et al. Postoperative opioid use and prescribing patterns among patients undergoing cervical laminectomy with instrumented fusion versus cervical laminoplasty with reconstruction. Global Spine J. 2024;14(2):561–567. doi:10.1177/21925682221116825
42. Pohl NB, Narayanan R, Lee Y, et al. Postoperative opioid consumption patterns diverge between propensity matched patients undergoing traumatic and elective cervical spine fusion. Spine J. 2024;24(10):1844–1850. doi:10.1016/j.spinee.2024.06.006
43. Jildeh TR, Taylor KA, Khalil LS, et al. Risk factors for postoperative opioid use in arthroscopic meniscal surgery. Arthroscopy. 2019;35(2):575–580. doi:10.1016/j.arthro.2018.10.122
44. Gedda C, Nygren J, Garpenbeck A, Hoffström L, Thorell A, Soop M. Multimodal analgesia bundle and postoperative opioid use among patients undergoing colorectal surgery. JAMA Netw Open. 2023;6(9):e2332408. doi:10.1001/jamanetworkopen.2023.32408
45. Harris AB, Marrache M, Jami M, et al. Chronic opioid use following anterior cervical discectomy and fusion surgery for degenerative cervical pathology. Spine J. 2020;20(1):78–86. doi:10.1016/j.spinee.2019.09.011
46. Hill MV, McMahon ML, Stucke RS, Barth RJJ. Wide variation and excessive dosage of opioid prescriptions for common general surgical procedures. Annals of Surgery. 2017;265(4):709. doi:10.1097/SLA.0000000000001993
47. Zanocco K, Romanelli RJ, Meeker D, et al. Drivers of variation in opioid prescribing after common surgical procedures in a large multihospital healthcare system. J Am Coll Surg. 2024;239(3):242. doi:10.1097/XCS.0000000000001095
48. LA SCM, Liu R, Bharadwaj KM, et al. Association of intraoperative opioid administration with postoperative pain and opioid use. JAMA Surg. 2023;158(8):854–864. doi:10.1001/jamasurg.2023.2009
49. Murphy GS, Szokol JW. Intraoperative methadone in surgical patients: a review of clinical investigations. Anesthesiology. 2019;131(3):678. doi:10.1097/ALN.0000000000002755
50. Murphy GS, Avram MJ, Greenberg SB, et al. Postoperative pain and analgesic requirements in the first year after intraoperative methadone for complex spine and cardiac surgery. Anesthesiology. 2020;132(2):330. doi:10.1097/ALN.0000000000003025
51. Patterns of opioid use after surgical discharge: a multicentre, prospective cohort study in 25 countries. Anaesthesia. 2024;79(9). doi:10.1111/anae.16297
52. Colvin LA. Opioid prescribing after surgery—cause for concern? JAMA Netw Open. 2019;2(9):e1910721. doi:10.1001/jamanetworkopen.2019.10721
53. Fujii MH, Hodges AC, Russell RL, et al. Post-discharge opioid prescribing and use after common surgical procedure. J Am Coll Surg. 2018;226(6):1004–1012. doi:10.1016/j.jamcollsurg.2018.01.058
54. Beyene KA, Chan AHY, Aquite OM, et al. Postdischarge opioid use and persistent use after general surgery: a retrospective study. Surgery. 2022;172(2):602–611. doi:10.1016/j.surg.2022.02.017
55. Shaffer L. Predicting pain with machine learning. The Source. June 20, 2025. Available from: https://source.washu.edu/2025/06/predicting-pain-with-machine-learning/.
56. Walton LL, Duff E, Arora RC, McMillan DE. Surgery patients’ perspectives of their role in postoperative pain: a scoping review. Int J Nurs Stud Adv. 2023;5:100124. doi:10.1016/j.ijnsa.2023.100124
57. Bhuchakra HP, Balasubramanian S, Nair AG, et al. Personalized perioperative opioid strategies in children: focus on methadone, pharmacogenomics and prevention of persistent postoperative opioid use. Children. 2025;12(12). doi:10.3390/children12121660
58. Liang I, Youssef P, Haynes A, et al. Expectations about pain management after discharge from total Hip and knee replacement surgery: a qualitative study with patients and prescribers. Front Pain Res. 2025;6:1647020. doi:10.3389/fpain.2025.1647020
59. Ishaku Z, Koshy DI, Adamu Bala M. Enhanced recovery after surgery (eras) pathways in elective total joint arthroplasty. Cureus. 2025. doi:10.7759/cureus.91481
60. Langnas EM, Matthay ZA, Lin A, et al. Enhanced recovery after surgery protocol and postoperative opioid prescribing for cesarean delivery: an interrupted time series analysis. Perioper Med (Lond). 2021;10(1):38. doi:10.1186/s13741-021-00209-0
61. Ferreira Do Couto ML, Fonseca S, Pozza DH. Pharmacogenetic approaches in personalized medicine for postoperative pain management. Biomedicines. 2024;12(4):729. doi:10.3390/biomedicines12040729
62. Beakley BD, Kaye AM, Kaye AD. Tramadol, pharmacology, side effects, and serotonin syndrome: a review. 2015;(10):395–400.
63. Reines SA, Goldmann B, Harnett M, Lu L. Misuse of Tramadol in the United States: an Analysis of the National Survey of Drug Use and Health 2002-2017. Substance Abuse: Research and Treatment. 2020;14. doi:10.1177/1178221820930006
64. Collins LK, Pande LJ, Chung DY, Nichols SD, McCall KL, Piper BJ. Trends in the medical supply of fentanyl and fentanyl analogues: united States, 2006 to 2017. Preventive Medicine. 2019;123:95–100. doi:10.1016/j.ypmed.2019.02.017
65. DEA. Drug Fact Sheet: fentanyl. In: Drug Enforcement Administration. Vol. 2. 2022.
66. Fentanyl (injection route) - Side effects & uses. Mayo Clinic. Available from: https://www.mayoclinic.org/drugs-supplements/fentanyl-injection-route/description/drg-20075614.
67. Grape S, Kirkham KR, Frauenknecht J, Albrecht E. Intra-operative analgesia with remifentanil vs. dexmedetomidine: a systematic review and meta-analysis with trial sequential analysis. Anaesthesia. 2019;74(6):793–800. doi:10.1111/anae.14657
68. Bee LA, Bannister K, Rahman W, Dickenson AH. Mu-opioid and noradrenergic α2-adrenoceptor contributions to the effects of tapentadol on spinal electrophysiological measures of nociception in nerve-injured rats. Pain. 2011;152(1):131–139. doi:10.1016/j.pain.2010.10.004
69. Hartrick CT, Rozek RJ. Tapentadol in Pain Management. CNS Drugs. 2011;25(5):359–370. doi:10.2165/11589080-000000000-00000
70. Argoff CE. Recent management advances in acute postoperative pain. Pain Practice. 2014;14(5):477–487. doi:10.1111/papr.12108
71. Kaye AD, Garcia AJ, Hall OM, et al. Update on the pharmacogenomics of pain management. PGPM. 2019;12:125–143. doi:10.2147/PGPM.S179152
72. Aroke EN, Kittelsrud JM. A primer to pharmacogenetics of postoperative pain management. AANA J. 2019;87(2):131–137.
73. Sachtleben EP, Rooney K, Haddad H, et al. The role of pharmacogenomics in postoperative pain management. Methods Mol Biol. 2022;2547:505–526. doi:10.1007/978-1-0716-2573-6_18
74. Slanar O, Dupal P, Matouskova O, Vondrackova H, Pafko P, Perlik F. Tramadol efficacy in patients with postoperative pain in relation to CYP2D6 and MDR1 polymorphisms. Bratisl Lek Listy. 2012;113(3):152–155. doi:10.4149/bll_2012_036
75. Thomas CD, Parvataneni HK, Gray CF, et al. A hybrid implementation-effectiveness randomized trial of CYP2D6-guided postoperative pain management. Genet Med. 2021;23(4):621–628. doi:10.1038/s41436-020-01050-4
76. Reizine N, Danahey K, Schierer E, et al. Impact of CYP2D6 pharmacogenomic status on pain control among opioid-treated oncology patients. Oncologist. 2021;26(11):e2042–e2052. doi:10.1002/onco.13953
77. Cho Y, Karrison T, Jack MM, et al. Catalyzing pharmacogenomic analysis for informing pain treatment (C-PAIN): a RANDOMIZED TRIAL OF PREEMPTIVE CYP2D6 GENOTYPING IN CANCER PALLIATIVE CAre. J Pain Res. 2024;17:4187–4196. doi:10.2147/JPR.S488416
78. Cornett EM, Carroll Turpin MA, Pinner A, et al. Pharmacogenomics of pain management: the impact of specific biological polymorphisms on drugs and metabolism. Curr Oncol Rep. 2020;22(2):18. doi:10.1007/s11912-020-0865-4
79. Rauseo M, Mirabella L, Carrideo AA, et al. Opioid-sparing anesthesia in cardiac surgery: a meta-analysis. J Cardiothorac Vasc Anesth. 2025;39(11):3140–3153. doi:10.1053/j.jvca.2025.06.040
80. McEvoy MD, Raymond BL, Krige A. Opioid-sparing perioperative analgesia within enhanced recovery programs. Anesthesiol Clin. 2022;40(1):35–58. doi:10.1016/j.anclin.2021.11.001
81. Beverly A, Kaye AD, Ljungqvist O, Urman RD. Essential elements of multimodal analgesia in Enhanced Recovery After Surgery (ERAS) Guidelines. Anesthesiol Clin. 2017;35(2):e115–e143. doi:10.1016/j.anclin.2017.01.018
82. Negm EM, Younus MA, Morsy AA, et al. Opioid-sparing multimodal analgesia for post-craniotomy pain: a randomized, double-blind, placebo-controlled trial. BMC Anesth. 2025;25(1):437. doi:10.1186/s12871-025-03306-5
83. Scholars@duke publication: American society for enhanced recovery and perioperative quality initiative joint consensus statement on perioperative management of patients on preoperative opioid therapy. Available from: https://scholars.duke.edu/publication/1370075?utm_source=chatgpt.com.
84. Recommendation-Summary-Page-_-Opioid-sparing_191229_233935.pdf. Available from: https://assets.erascardiac.org/downloads/Recommendation-Summary-Page-_-Opioid-sparing_191229_233935.pdf?utm_source=chatgpt.com.
85. Edwards DA, Hedrick TL, Jayaram J, et al. American society for enhanced recovery and perioperative quality initiative joint consensus statement on perioperative management of patients on preoperative opioid therapy. Anesth Analgesia. 2019;129(2):553. doi:10.1213/ANE.0000000000004018
86. Fabi D. Multimodal analgesia in the hip fracture patient. J Orthop Trauma. 2016;30 Suppl 1:S6–S11. doi:10.1097/BOT.0000000000000561
87.. American Geriatrics Society Panel on the Pharmacological Management of Persistent Pain in Older Persons. Pharmacological management of persistent pain in older persons. J Am Geriatr Soc. 2009;57(8):1331–1346. 10.1111/j.1532-5415.2009.02376.x.
88. American Geriatrics Society. Updated AGS beers criteria® for potentially inappropriate medication use in older adults. 2019. doi:10.1111/jgs.15767
89. Wick EC, Grant MC, Wu CL. Postoperative multimodal analgesia pain management with nonopioid analgesics and techniques: a review. JAMA Surg. 2017;152(7):691–697. doi:10.1001/jamasurg.2017.0898
90. Postoperative analgesia for upper gastrointestinal surgery: a retrospective cohort analysis | perioperative Medicine. Available from: https://link.springer.com/article/10.1186/s13741-023-00324-0?utm_source=chatgpt.com.
91. Mujukian A, Truong A, Tran H, Shane R, Fleshner P, Zaghiyan K. A standardized multimodal analgesia protocol reduces perioperative opioid use in minimally invasive colorectal surgery. J Gastrointest Surg. 2020;24(10):2286–2294. doi:10.1007/s11605-019-04385-9
92. Ashrafi AN, Yip W, Graham JN, et al. Implementation of a multimodal opioid-sparing enhanced recovery pathway for robotic-assisted radical prostatectomy. J Robot Surg. 2022;16(3):715–721. doi:10.1007/s11701-021-01268-7
93. Ghai B, Jafra A, Bhatia N, Chanana N, Bansal D, Mehta V. Opioid sparing strategies for perioperative pain management other than regional anaesthesia: a narrative review. 2022. doi:10.4103/joacp.JOACP
94. He HG, Pö T, Vehvilä Inen-Julkunen K, Pietilä AM. ISSUES AND INNOVATIONS IN NURSING PRACTICE Chinese nurses’ use of non-pharmacological methods in children’s postoperative pain relief. 2005.
95. yan BY, Chao WL, wei QW, et al. Role of parecoxib sodium in the multimodal analgesia after total knee arthroplasty: a randomized double-blinded controlled trial. Orthop Surg. 2018;10(4):321–327. doi:10.1111/os.12410
96. Shao Y, Zhao X, Zhai Y, et al. Comparison of analgesic effect, knee joint function recovery, and safety profiles between pre-operative and post-operative administrations of meloxicam in knee osteoarthritis patients who underwent total knee arthroplasty. Irish J Med Sci. 2020;189(2):535–542. doi:10.1007/s11845-019-02128-y
97. K UR, Shenoy L, Venkateswaran R. Effect of intravenous dexmedetomidine administered as bolus or as bolus-plus-infusion on subarachnoid anesthesia with hyperbaric bupivacaine. J Anaesthesiol Clin Pharmacol. 2018;34(3):46–50. doi:10.4103/joacp.JOACP
98. Mochizuki T, Yano K, Ikari K, et al. Tramadol hydrochloride/Acetaminophen combination versus non-steroidal anti-inflammatory drug for the treatment of perioperative pain after total knee arthroplasty: a prospective, randomized, open-label clinical trial. J Orthop Sci. 2016;21(5):625–629. doi:10.1016/j.jos.2016.07.011
99. Wilson SH, Wilson PR, Bridges KH, Bell LH, Clark CA. Nonopioid analgesics for the perioperative geriatric patient: a narrative review. Anesth and Analgesia. 2022;135(2):290–306. doi:10.1213/ANE.0000000000005944
100. Lee A, Cooper MG, Craig JC, Knight JF, Keneally JP. Effects of nonsteroidal anti-inflammatory drugs on postoperative renal function in adults with normal renal function. Cochrane Database Syst. Rev. 2007. doi:10.1002/14651858.CD002765.pub3
101. Fialová D, Laffon B, Marinković V, et al. Medication use in older patients and age-blind approach: narrative literature review (insufficient evidence on the efficacy and safety of drugs in older age, frequent use of PIMs and polypharmacy, and underuse of highly beneficial nonpharmacological strategies). Eur J Clin Pharmacol. 2019;75(4):451–466. doi:10.1007/s00228-018-2603-5
102. Ribeiro H, Rodrigues I, Napoleão L, et al. Non-steroidal anti-inflammatory drugs (NSAIDs), pain and aging: adjusting prescription to patient features. Biomed Pharmacother. 2022;150:112958. doi:10.1016/j.biopha.2022.112958
103. Tohol WJ, Abuejheisheh AJ, Fashafsheh I, Amro N. Using of non-pharmacological pain methods, and the perceived barriers, among nurses in critical care unit in Palestine. BMC Nursing. 2023;22(1):1–11. doi:10.1186/s12912-023-01635-9
104. Wigg D, Elson R. Management of postoperative pain. The Pharmaceutical Journal. 2022. Available from https://pharmaceutical-journal.com/article/ld/management-of-postoperative-pain.
105. Naraharisetti SB, Srour S, Xu Y, Lee DJ, hertz SH, Sahajwalla C. Effects of food on bioavailability of analgesics; resulting dosage and administration recommendations. Pain Med. 2020;21(11):2877–2892. doi:10.1093/pm/pnaa046
106. Rech MA, Griggs C, Lovett S, Motov S. Acute pain management in the emergency department: use of multimodal and non-opioid analgesic treatment strategies. The American Journal of Emergency Medicine. 2022;58:57–65. doi:10.1016/j.ajem.2022.05.022
107. Skrobik Y, Ahern S, Leblanc M, Marquis F, Awissi DK, Kavanagh BP. Protocolized intensive care unit management of analgesia, sedation, and delirium improves analgesia and subsyndromal delirium rates. Anesth Analg. 2010;111(2):451–463. doi:10.1213/ANE.0b013e3181d7e1b8
108. Caty S, Tourigny J, Koren I. Assessment and management of children’s pain in community hospitals. J Adv Nurs. 1995;22(4):638–645. doi:10.1046/j.1365-2648.1995.22040638.x
109. Pölkki T, Vehviläinen-Julkunen K, Pietilä AM. Nonpharmacological methods in relieving children’s postoperative pain: a survey on hospital nurses in Finland. Available from: https://onlinelibrary.wiley.com/doi/10.1046/j.1365-2648.2001.01777.x.
110. Felix MM Dos S, Ferreira MBG, da CLF, Barbosa MH. Relaxation therapy with guided imagery for postoperative pain management: an integrative review. Pain Manage Nurs. 2019;20(1):3–9. doi:10.1016/j.pmn.2017.10.014
111. Allred KD, Byers JF, Sole ML. The effect of music on postoperative pain and anxiety. Pain Manag Nurs. 2010;11(1):15–25. doi:10.1016/j.pmn.2008.12.002
112. Engwall M, Duppils GS. Music as a nursing intervention for postoperative pain: a systematic review. J Perianesth Nurs. 2009;24(6):370–383. doi:10.1016/j.jopan.2009.10.013
113. Roofthooft E, Joshi GP, Rawal N, Van de Velde M. PROSPECT working group* of the european society of regional anaesthesia and pain therapy and supported by the obstetric anaesthetists’ association. PROSPECT guideline for elective caesarean section: updated systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2021;76(5):665–680. doi:10.1111/anae.15339
114. Feray S, Lubach J, Joshi GP, Bonnet F, Van de Velde M, PROSPECT Working Group *of the European Society of Regional Anaesthesia and Pain Therapy. PROSPECT guidelines for video-assisted thoracoscopic surgery: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2022;77(3):311–325. doi:10.1111/anae.15609
115. Ashraf S, Andanappa A, Rani SDJ, Shrivatsam P. Multimodal analgesia strategies for optimal postoperative pain relief. Int J Clin Trials. 2025;12(2):169–175. doi:10.18203/2349-3259.ijct20251213
116. Tzortzopoulou A, Cepeda MS, Farhat T, McNicol E, Schumann R. Single dose propacetamol or IV paracetamol for postoperative pain. Cochrane Database of Systematic Reviews. 2008;(2). doi:10.1002/14651858.CD007126
117. Deutsch AB, DelBianco JD, Fagan P, et al. Evaluation of an intravenous acetaminophen protocol in the emergency department. Cureus. 2024;16(1):1–5. doi:10.7759/cureus.52934
118. Ishitsuka Y, Kondo Y, Kadowaki D. Toxicological property of acetaminophen: the dark side of a safe antipyretic/analgesic drug? Biol Pharm Bull. 2020;43(2):195–206. doi:10.1248/bpb.b19-00722
119. Wynne HA, Cope LH, Herd B, Rawlins MD, James OF, Woodhouse KW. The association of age and frailty with paracetamol conjugation in man. Age Ageing. 1990;19(6):419–424. doi:10.1093/ageing/19.6.419
120. Boudrias-Dalle E, Chen A. Acetaminophen dose considerations in frail and malnourished elderly patients: a case report of hepatotoxicity with therapeutic doses. Can J Hosp Pharm. 76(4):337–339. doi:10.4212/cjhp.3415
121. Edinoff AN, Askins D, Bobo E, et al. The emerging role of ketamine in acute postoperative pain management. Curr Pain and Headache Rep. 2023;27(9):387–397. doi:10.1007/s11916-023-01134-1
122. Maxwell EN, Johnson B, Cammilleri J, Ferreira JA. Intravenous acetaminophen–induced hypotension: a review of the current literature. Ann Pharmacother. 2019;53(10):1033–1041. doi:10.1177/1060028019849716
123. Cantais A, Schnell D, Vincent F, et al. Acetaminophen-induced changes in systemic blood pressure in critically ill patients: results of a multicenter cohort study. Critical Care Med. 2016;44(12):2192. doi:10.1097/CCM.0000000000001954
124. van der HJ, Manville RW, Hayes K, Thomsen MB, Abbott GW, Jepps TA. Acetaminophen (paracetamol) metabolites induce vasodilation and hypotension by activating kv7 potassium channels directly and indirectly. Arterioscler. Thromb. Vasc. Biol. 2020. doi:10.1161/ATVBAHA.120.313997
125. La Monaca G, Pranno N, Annibali S, et al. Comparative analgesic effects of single-dose preoperative administration of paracetamol (acetaminophen) 500 mg plus codeine 30 mg and ibuprofen 400 mg on pain after third molar surgery. J Evid Based Dent Pract. 2021;21(4):101611. doi:10.1016/j.jebdp.2021.101611
126. McLachlan AJ, Bath S, Naganathan V, et al. Clinical pharmacology of analgesic medicines in older people: impact of frailty and cognitive impairment. Br J Clin Pharmacol. 2011;71(3):351–364. doi:10.1111/j.1365-2125.2010.03847.x
127. Panchgar V, Shetti A, Sunitha H, Dhulkhed V, Nadkarni A. The effectiveness of intravenous dexmedetomidine on perioperative hemodynamics, analgesic requirement, and side effects profile in patients undergoing laparoscopic surgery under general anesthesia. Anesth Essays Res. 2017;11(1):72. doi:10.4103/0259-1162.200232
128. Davy A, Fessler J, Fischler M, Le Guen M. Dexmedetomidine and general anesthesia: a narrative literature review of its major indications for use in adults undergoing non-cardiac surgery. Minerva anestesiologica. 2017;83(12):1294–1308. doi:10.23736/S0375-9393.17.12040-7
129. Song Y, Shim JK, Song JW, Kim EK, Kwak YL. Dexmedetomidine added to an opioid-based analgesic regimen for the prevention of postoperative nausea and vomiting in highly susceptible patients. Eur. J. Anaesthesiol. 2016;33(2):75–83. doi:10.1097/EJA.0000000000000327
130. Kaye AD, Chernobylsky DJ, Thakur P, et al. Dexmedetomidine in enhanced recovery after surgery (eras) protocols for postoperative pain. Current Pain and Headache Reports. 2020;24(5). doi:10.1007/s11916-020-00853-z
131. Zhu H, Wang S, Wang R, Li B, Zhang J, Zhang W. Effect of dexmedetomidine on postoperative nausea and vomiting in female patients undergoing radical thoracoscopic lung cancer resection. Front Pharmacol. 2024;15(January):1–13. doi:10.3389/fphar.2024.1353620
132. Khan J, Ashraf RA, Bilal Shabbir HM, et al. The effect of dexamethasone on postoperative pain management in patients undergoing total knee arthroplasty: a randomized controlled trial. Cureus. 2023;15(4):1–7. doi:10.7759/cureus.37052
133. Liang S, Xing M, Jiang S, Zou W. Effect of intravenous dexamethasone on postoperative pain in patients undergoing total knee arthroplasty: a systematic review and meta-analysis. Pain Physician. 2022;25(2):E169–E188.
134. Dissanayake R, Du HN, Robertson IK, Ogden K, Wiltshire K, Mulford JS. Does dexamethasone reduce hospital readiness for discharge, pain, nausea, and early patient satisfaction in hip and knee arthroplasty? a randomized, controlled trial. J Arthroplasty. 2018;33(11):3429–3436. doi:10.1016/j.arth.2018.07.013
135. Admassie BM, Tegegne BA, Alemu WM, Getahun AB. Magnitude and severity of rebound pain after resolution of peripheral nerve block and associated factors among patients undergoes surgery at university of gondar comprehensive specialized hospital northwest, Ethiopia, 2022. Longitudinal cross-sectional st. Ann Med Surg. 2022;84:104915. doi:10.1016/j.amsu.2022.104915
136. Li F, Huang X, Liu W, Huang W, Cheng J, Yin D. Dexamethasone with aggressive warming facilitates pain reduction, reduced blood loss, and quicker recovery after total Hip arthroplasty. Scie Rep. 2023;13(1):1–11. doi:10.1038/s41598-023-47050-7
137. States U. Dexamethasone. 1–5.
138. Wang J, Xu Z, Feng Z, Ma R, Zhang X. Impact of ketamine on pain management in cesarean section: a systematic review and meta-analysis. Pain Physician. 2020;23(2):135–148. doi:10.36076/ppj.2020/23/135
139. Yang Y, Maher DP, Cohen SP. Emerging concepts on the use of ketamine for chronic pain. Expert Rev. Clin. Pharmacol. 2020;13(2):135–146. doi:10.1080/17512433.2020.1717947
140. Raymond BL, Allen BFS, Freundlich RE, et al. The IMpact of PerioperAtive KeTamine on Enhanced Recovery after Abdominal Surgery (IMPAKT ERAS): protocol for a pragmatic, randomized, double-blinded, placebo-controlled trial. BMC Anesth. 2023;23:227. doi:10.1186/s12871-023-02177-y
141. Jouguelet-Lacoste J, La Colla L, Schilling D, Chelly JE. The use of intravenous infusion or single dose of low-dose ketamine for postoperative analgesia: a review of the current literature. Pain Med. 2015;16(2):383–403. doi:10.1111/pme.12619
142. Pestieau SR, Finkel JC, Junqueira MM, et al. Prolonged perioperative infusion of low-dose ketamine does not alter opioid use after pediatric scoliosis surgery. Paediatr Anaesth. 2014;24(6):582–590. doi:10.1111/pan.12417
143. Pacreu S, Fernández Candil J, Moltó L, Carazo J, Fernández Galinski S. The perioperative combination of methadone and ketamine reduces post-operative opioid usage compared with methadone alone. Acta Anaesth Scand. 2012;56(10):1250–1256. doi:10.1111/j.1399-6576.2012.02743.x
144. Low-dose ketamine can be effective in reducing post-operative pain. Available from: https://www.cebm.ox.ac.uk/news/views/low-dose-ketamine-can-be-effective-in-reducing-post-operative-pain.
145. García-Henares JF, Moral-Munoz JA, Salazar A, Del Pozo E. Effects of ketamine on postoperative pain after remifentanil-based anesthesia for major and minor surgery in adults: a systematic review and meta-analysis. Front Pharmacol. 2018;9. 10.3389/fphar.2018.00921.
146. Brinck ECV, Virtanen T, Mäkelä S, et al. S-ketamine in patient-controlled analgesia reduces opioid consumption in a dose-dependent manner after major lumbar fusion surgery: a randomized, double-blind, placebo-controlled clinical trial. PLoS One. 2021;16(6):e0252626. doi:10.1371/journal.pone.0252626
147. Zhu J, Xie H, Zhang L, Chang L, Chen P. Efficiency and safety of ketamine for pain relief after laparoscopic cholecystectomy: a meta-analysis from randomized controlled trials. Int J Surg. 2018;49:1–9. doi:10.1016/j.ijsu.2017.11.031
148. Ketamine for acute pain management and sedation | critical care nurse | American association of critical-care nurses. Available from: https://aacnjournals.org/ccnonline/article/40/5/e26/31181/Ketamine-for-Acute-Pain-Management-and-Sedation.
149. Viderman D, Mukazhan D, Kapessova K, et al. The Impact of ketamine on outcomes in acute pain management: an umbrella review. J Clin Med. 2024;13(24). doi:10.3390/jcm13247699
150. Ahern TL, Herring AA, Anderson ES, Madia VA, Fahimi J, Frazee BW. The first 500: initial experience with widespread use of low-dose ketamine for acute pain management in the ED. Am J Emerg Med. 2015;33(2):197–201. doi:10.1016/j.ajem.2014.11.010
151. Zanos P, Moaddel R, Morris PJ, et al. Ketamine and ketamine metabolite pharmacology: insights into therapeutic mechanisms. Pharmacol Rev. 2018;70(3):621–660. doi:10.1124/pr.117.015198
152. Shaked G, Czeiger D, Dukhno O, et al. Ketamine improves survival and suppresses IL-6 and TNFalpha production in a model of Gram-negative bacterial sepsis in rats. Resuscitation. 2004;62(2):237–242. doi:10.1016/j.resuscitation.2004.02.015
153. Li S, Zhou W, Li P, Lin R. Effects of ketamine and esketamine on preventing postpartum depression after cesarean delivery: a meta-analysis. J Affect Disord. 2024;351:720–728. doi:10.1016/j.jad.2024.01.202
154. Wang X, Lin C, Lan L, Liu J. Perioperative intravenous S-ketamine for acute postoperative pain in adults: a systematic review and meta-analysis. J Clin Anesth. 2021;68:110071. doi:10.1016/j.jclinane.2020.110071
155. Lin X, Liu X, Huang H, Xu X, Zhang T, Gao J. Esketamine and neurocognitive disorders in adult surgical patients: a meta-analysis. BMC Anesthesiol. 2024;24(1):448. doi:10.1186/s12871-024-02803-3
156. Palamar JJ. Tusi: a new ketamine concoction complicating the drug landscape. Am J Drug Alcohol Abuse. 2023;49(5):546–550. doi:10.1080/00952990.2023.2207716
157. Sun X, Li C, Xu L, et al. Effect and safety of perioperative ketamine/esketamine administration on postoperative pain and depression after breast cancer surgery: a systematic review and meta-analysis. Front Pharmacol. 2025;16:1532524. doi:10.3389/fphar.2025.1532524
158. Liu J, Liu J, Sun H, et al. Effect of perioperative esketamine use on emergency delirium in children undergoing tonsillectomy and adenoidectomy: a systematic review and meta-analysis of randomized controlled trials. Front Med. 2025;12:1505408. doi:10.3389/fmed.2025.1505408
159. Hou NN, Zhang MY, Zhang YW, Wu HJ, Luo H, Yang H. Safety and efficacy of low-dose esketamine weakly opioidized anesthesia in elderly patients with lumbar spinal stenosis undergoing surgery: a prospective, double-blind randomized controlled trial. BMC Anesth. 2025;25(1):57. doi:10.1186/s12871-025-02908-3
160. Albrecht E, Kirkham KR, Liu SS, Brull R. Peri-operative intravenous administration of magnesium sulphate and postoperative pain: a meta-analysis. Anaesthesia. 2013;68(1):79–90. doi:10.1111/j.1365-2044.2012.07335.x
161. Soeding P, Morris A, Soeding A, Hoy G. Effect of intravenous magnesium on post-operative pain following Latarjet shoulder reconstruction. Shoulder and Elbow. 2024;16(1):46–52. doi:10.1177/17585732231158805
162. Ng KT, Yap JLL, Izham IN, Teoh WY, Kwok PE, Koh WJ. The effect of intravenous magnesium on postoperative morphine consumption in noncardiac surgery: a systematic review and meta-analysis with trial sequential analysis. Eur. J. Anaesthesiol. 2020;37(3):212–223. doi:10.1097/EJA.0000000000001164
163. Choi GJ, Kim YI, Koo YH, Oh HC, Kang H. Perioperative magnesium for postoperative analgesia: an umbrella review of systematic reviews and updated meta-analysis of randomized controlled trials. J Pers Med. 2021;11(12):1273. doi:10.3390/jpm11121273
164. “Oh Mg!” Magnesium: a Powerful Tool in the Perioperative Setting. ASRA Pain Medicine. Available from: https://asra.com/news-publications/asra-newsletter/newsletter-item/asra-news/2018/07/23/-oh-mg!-magnesium-a-powerful-tool-in-the-perioperative-setting.
165. Rodríguez-Rubio L, Nava E, Del Pozo JSG, Jordán J. Influence of the perioperative administration of magnesium sulfate on the total dose of anesthetics during general anesthesia. A systematic review and meta-analysis. J. Clin. Anesth. 2017;39:129–138. doi:10.1016/j.jclinane.2017.03.038
166. Meerman M, Buijser M, van den Berg L, et al. Magnesium sulphate to prevent perioperative atrial fibrillation in cardiac surgery: a randomized clinical trial. Trials. 2024;25:540. doi:10.1186/s13063-024-08368-3
167. White PF, Tufanogullari B, Taylor J, Klein K. The effect of pregabalin on preoperative anxiety and sedation levels: a dose-ranging study. Anesthesia and Analgesia. 2009;108(4):1140–1145. doi:10.1213/ane.0b013e31818d40ce
168. Park KH, Chung NS, Chung HW, Kim TY, Lee HD. Pregabalin as an effective treatment for acute postoperative pain following spinal surgery without major side effects: protocol for a prospective, randomized controlled, double-blinded trial. Trials. 2023;24(1):1–9. doi:10.1186/s13063-023-07438-2
169. Wang YT, Xiao C, Liu H, Fu X, Ren YF, You FM. Preoperative oral gabapentin in the management of postoperative catheter-related bladder discomfort in adults: a systematic review and meta-analysis. Frontiers in Surgery. 2021;8(October). doi:10.3389/fsurg.2021.755497
170. Weingarten TN, Jacob AK, Njathi CW, Wilson GA, Sprung J. Multimodal analgesic protocol and postanesthesia respiratory depression during phase i recovery after total joint arthroplasty. Reg Anesth Pain Med. 2015;40(4):330–336. doi:10.1097/AAP.0000000000000257
171. Cavalcante AN, Sprung J, Schroeder DR, Weingarten TN. Multimodal analgesic therapy with gabapentin and its association with postoperative respiratory depression. Anesth Analg. 2017;125(1):141–146. doi:10.1213/ANE.0000000000001719
172. Fick DM, Semla TP, Steinman M, et al. American geriatrics society 2019 updated ags beers criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674–694. doi:10.1111/jgs.15767
173. Hah J, Mackey SC, Schmidt P, et al. Effect of perioperative gabapentin on postoperative pain resolution and opioid cessation in a mixed surgical cohort: a randomized clinical trial. JAMA Surg. 2018;153(4):303–312. doi:10.1001/jamasurg.2017.4915
174. Wier J, Mayfield CK, Liu KC, et al. Higher postoperative gabapentin doses are associated with pulmonary complications after total shoulder arthroplasty. JSES Int. 2025;9(5):1630–1635. doi:10.1016/j.jseint.2025.04.035
175. Patel AS, Abrecht CR, Urman RD. Gabapentinoid use in perioperative care and current controversies. Curr Pain Headache Rep. 2022;26(2):139–144. doi:10.1007/s11916-022-01012-2
176. Makwana BGM, Vohra SY, Makwana MB. Perioperative use of lidocaine infusions for chronic pain prevention: a systematic review. Eur J Cardiovas Med. 2025;15:580–586. doi:10.61336/ejcm/25-10-101
177. Nl P, Lhj E, Mw H, et al. 2018. doi:10.1002/14651858.CD009642.pub3.www.cochranelibrary.com
178. Yao Y, Jiang J, Lin W, Yu Y, Guo Y, Zheng X. Efficacy of systemic lidocaine on postoperative quality of recovery and analgesia after video-assisted thoracic surgery: a randomized controlled trial. Journal of Clinical Anesthesia. 2021;71(February):110223. doi:10.1016/j.jclinane.2021.110223
179. Gau TP, Wu SH, Huang JM, et al. Multimodal analgesia with local wound infiltration and intravenous parecoxib for thyroidectomy. Medicina. 2023;59(5):1–10. doi:10.3390/medicina59050855
180. McCarthy GC, Megalla SA, Habib AS. Impact of intravenous lidocaine infusion on postoperative analgesia and recovery from surgery: a systematic review of randomized controlled trials. Drugs. 2010;70(9):1149–1163. doi:10.2165/10898560-000000000-00000
181. Abram SE, Yaksh TL. Systemic lidocaine blocks nerve injury-induced hyperalgesia and nociceptor-driven spinal sensitization in the rat. Anesthesiology. 1994;80(2):383–391;discussion25A.
182. Baldini G. Restoration of bowel function after laparoscopic colorectal surgery: effect of intravenous lidocaine. clinicaltrials.gov; 2011. Available from: https://clinicaltrials.gov/study/NCT01155440.
183. Han M, Xia J, Zhang M, et al. Is dosage adjustment based on age necessary for intravenous lidocaine in patients undergoing general anesthesia: a prospective multi-arm comparative study. JPharmSci. 2024;113(9):2922–2932. doi:10.1016/j.xphs.2024.07.012
184. Randomized A, controlled TP, Foss NB, et al. Effect of postoperative epidural analgesia on rehabilitation and pain after hip fracture surgery. 2005(6):1197–1204.
185. Soffin EM, Wu CL. Regional and multimodal analgesia to reduce opioid use after total joint arthroplasty: a narrative review. HSS J. 2019;15(1):57–65. doi:10.1007/s11420-018-9652-2
186. Raja M, Rajaprabu R, Ialambeitlang H, Kharpran R. Comparison Of Epidural With Iliopsoas Plane Catheter Insertion For Providing Post-Operative Analgesia In Hip Surgeries. 2023:632–637. DOI:10.47009/jamp.2023.5.2.133
187. Horlocker TT, Wedel DJ, Rowlingson JC, et al. Regional Anesthesia in the patient receiving antithrombotic or thrombolytic therapy; American Society of Regional Anesthesia and Pain Medicine evidence-based guidelines (Third Edition). Regional Anesthesia and Pain Medicine. 2010;35(1):64–101. doi:10.1097/AAP.0b013e3181c15c70
188. Kanazi GE, Aouad MT, Abdallah FW, et al. The analgesic efficacy of subarachnoid morphine in comparison with ultrasound-guided transversus abdominis plane block after cesarean delivery: a randomized controlled trial. Anesth Analg. 2010;111(2):475–481. doi:10.1213/ANE.0b013e3181e30b9f
189. Marshall K, McLaughlin K. Pain management in thoracic surgery. Thorac. Surg. Clin. 2020;30(3):339–346. doi:10.1016/j.thorsurg.2020.03.001
190. Meylan N, Elia N, Lysakowski C, Tramèr MR. Benefit and risk of intrathecal morphine without local anaesthetic in patients undergoing major surgery: meta-analysis of randomized trials. Br J Anaesth. 2009;102(2):156–167. doi:10.1093/bja/aen368
191. Opioids N. Practice guidelines for the prevention, detection, and neuraxial opioid administration. Focus. 2009;(2):218–230.
192. Adams TJ, Aljohani DM, Forget P. Perioperative opioids: a narrative review contextualising new avenues to improve prescribing. Br J Anaesth. 2023;130(6):709–718. doi:10.1016/j.bja.2023.02.037
193. Brat GA, Agniel D, Beam A, et al. Postsurgical prescriptions for opioid naive patients and association with overdose and misuse: retrospective cohort study. BMJ. 2018:360. 10.1136/bmj.j5790.
194. Nagaraja P, Ragavendran S, Singh N, et al. Comparison of continuous thoracic epidural analgesia with bilateral erector spinae plane block for perioperative pain management in cardiac surgery. Ann. Card. Anaesth. 2018;21(3):323. doi:10.4103/aca.aca_16_18
195. qi CJ, lu YX, Gu H, Qing CX, Wang D. The role of serratus anterior plane block during in video-assisted thoracoscopic surgery. Pain and Ther. 2021;10(2):1051–1066. doi:10.1007/s40122-021-00322-4
196. Zhou K, Li D, Song G. Comparison of regional anesthetic techniques for postoperative analgesia after adult cardiac surgery: bayesian network meta-analysis. Front. Cardiovasc Med. 2023;10(May):1–11. doi:10.3389/fcvm.2023.1078756
197. Neal JM, Barrington MJ, Brull R, et al. The Second ASRA practice advisory on neurologic complications associated with regional anesthesia and pain medicine: executive summary 2015. Reg Anesth Pain Med. 2015;40(5):401–430. doi:10.1097/AAP.0000000000000286
198. Hamilton C, Alfille P, Mountjoy J, Bao X. Regional anesthesia and acute perioperative pain management in thoracic surgery: a narrative review. J. Thorac. Dis. 2022;14(6):2276–2296. doi:10.21037/jtd-21-1740
199. Löchel J, Janz V, Leopold VJ, Krämer M, Wassilew GI. Transversus abdominis plane block for improved early postoperative pain management after periacetabular osteotomy: a randomized clinical trial. J Clin Med. 2021;10(3):1–7. doi:10.3390/jcm10030394
200. Palareti G, Legnani C, Cosmi B, et al. Comparison between different D-Dimer cutoff values to assess the individual risk of recurrent venous thromboembolism: analysis of results obtained in the DULCIS study. Int. J. Lab. Hematol. 2016;38(1):42–49. doi:10.1111/ijlh.12426
201. Xing JG, Abdallah FW, Brull R, et al. Preoperative femoral nerve block for Hip arthroscopy. Am J Sports Med. 2015;43(11):2680–2687. doi:10.1177/0363546515602468
202. Tsai TY, Mun CK, Su YC, et al. Ultrasound-guided femoral nerve block in geriatric patients with hip fracture in the emergency department. J Clin Med. 2022;11(10). doi:10.3390/jcm11102778
203. Beaudoin FL, Haran JP, Liebmann O. A comparison of ultrasound-guided three-in-one femoral nerve block versus parenteral opioids alone for analgesia in emergency department patients with Hip fractures: a randomized controlled trial. Acad Emerg Med. 2013;20(6):584–591. doi:10.1111/acem.12154
204. Kisiangani J, Baliddawa J, Marinda P, et al. Determinants of breast cancer early detection for cues to expanded control and care: the lived experiences among women from Western Kenya. BMC Womens Health. 2018;18(1):81. doi:10.1186/s12905-018-0571-7
205. Bangshoej J, Thougaard T, Fjeldsøe-Nielsen H, Viggers S. Preoperative pain management of patients with hip fractures: blind fascia iliaca compartment block compared to ultrasound guided femoral nerve block—a randomized controlled trial. Open J Anesth. 2020;10(11):371–380. doi:10.4236/ojanes.2020.1011033
206. Beaudoin FL, Nagdev A, Merchant RC, Becker BM. Ultrasound-guided femoral nerve blocks in elderly patients with Hip fractures. Am J Emerg Med. 2010;28(1):76–81. doi:10.1016/j.ajem.2008.09.015
207. Rasappan K, Chua ITH, Tey JBL, SWL H. The continuous infusion fascia iliaca compartment block: a safe and effective analgesic modality in geriatric Hip fracture patients. Arch Orthop Trauma Surg. 2021;141(1):29–37. doi:10.1007/s00402-020-03450-2
208. Chen Y, Li Q, Liao Y, et al. Preemptive deep parasternal intercostal plane block for perioperative analgesia in coronary artery bypass grafting with sternotomy: a randomized, observer-blind, controlled study. Ann Med. 2023;55(2). doi:10.1080/07853890.2024.2302983
209. Zhang Y, Min J, Chen S. Sensory assessment and block duration of deep parasternal intercostal plane block in patients undergoing cardiac surgery: a prospective observational study. Pain and Ther. 2022;11(3):951–958. doi:10.1007/s40122-022-00403-y
210. Wong HMK, Chen PY, Tang GCC, et al. Deep parasternal intercostal plane block for intraoperative pain control in cardiac surgical patients for sternotomy: a prospective randomized controlled trial. J Cardiothorac Vasc Anesth. 2024;38(3):683–690. doi:10.1053/j.jvca.2023.11.038
211. Zhang H, Gu F, Liu Y, Wang C, Xu C. Heliyon The analgesic efficacy of paravertebral block at T11 level as a single anaesthetic technique in an older adult with severe cardiac insufficiency undergoing open complex inguinal hernia repair: a case report. Heliyon. 2023;9(4):e14962. doi:10.1016/j.heliyon.2023.e14962
212. Chai B, Wang Q, Du J, et al. Research progress on serratus anterior plane block in breast surgery: a narrative review. Pain and Ther. 2023;12(2):323–337. doi:10.1007/s40122-022-00456-z
213. Kelava M, Alfirevic A, Bustamante S, Hargrave J, Marciniak D. Regional anesthesia in cardiac surgery: an overview of fascial plane chest wall blocks. Anesth and Analg. 2020;131(1):127–135. doi:10.1213/ANE.0000000000004682
214. Chae MS, Park Y, Shim JW, et al. Clinical application of pectoralis nerve block ii for flap dissection-related pain control after robot-assisted transaxillary thyroidectomy: a preliminary retrospective cohort study. Cancers. 2022;14(17):1–11. doi:10.3390/cancers14174097
215. Ahiskalioglu A, Tulgar S, Celik M, Ozer Z, Alici HA, Aydin ME. Lumbar erector spinae plane block as a main anesthetic method for Hip surgery in high risk elderly patients: initial experience with a magnetic resonance imaging. Eurasian J Med. 2020;52(1):16–20. doi:10.5152/eurasianjmed.2020.19224
216. Zheng T, Hu B, ying ZC, yi HF, Gao F, chun ZX. Improvement of analgesic efficacy for total Hip arthroplasty by a modified ultrasound-guided supra-inguinal fascia iliaca compartment block. BMC Anesthesiol. 2021;21(1):1–8. doi:10.1186/s12871-021-01296-8
217. Chen L, Shen Y, Liu S, Cao Y, Zhu Z. Ultrasound-guided supra-inguinal fascia Iliaca compartment block for older adults admitted to the emergency department with Hip fracture: a randomized controlled, double-blind clinical trial. BMC Geriatrics. 2021;21(1):1–8. doi:10.1186/s12877-021-02646-4
218. Gao Y, Tan H, Sun R, Zhu J. Fascia iliaca compartment block reduces pain and opioid consumption after total Hip arthroplasty: a systematic review and meta-analysis. Int J Surg. 2019;65(February):70–79. doi:10.1016/j.ijsu.2019.03.014
219. Tulgar S, Kose H, Selvi O, et al. Comparison of ultrasound-guided lumbar erector spinae plane block and transmuscular quadratus lumborum block for postoperative analgesia in Hip and proximal femur surgery: a prospective randomized feasibility study. Anesthesia: Essays and Researches. 2018;12(4):825. doi:10.4103/aer.aer_142_18
220. Team MS. Local Anesthetic Toxicity. MD Searchlight. August 7, 2024. Available from: https://mdsearchlight.com/medications/local-anesthetic-toxicity/.
221. Song K, Blankenship RB, Derian A. Local Anesthetic Toxicity. StatPearls. StatPearls Publishing; 2025. Available from. http://www.ncbi.nlm.nih.gov/books/NBK499964/.
222. Chen L, Liu S, Cao Y, Yan L, Shen Y. Effect of perioperative ultrasound guided fascia iliaca compartment block in elderly adults with Hip fractures undergoing arthroplasty in spinal anesthesia—a randomized controlled trial. BMC Geriatrics. 2023;23(1):1–7. doi:10.1186/s12877-023-03786-5
223. Abadi A, Cohen R. Evaluation of an enhanced recovery after surgery protocol including parasternal intercostal nerve block in cardiac surgery requiring sternotomy. Am Surgeon. 2021;87(10):1561–1564. doi:10.1177/00031348211024638
224. Rao Kadam V, Ludbrook G, van Wijk RM, et al. Comparison of ultrasound-guided transmuscular quadratus lumborum block catheter technique with surgical pre-peritoneal catheter for postoperative analgesia in abdominal surgery: a randomised controlled trial. Anaesthesia. 2019;74(11):1381–1388. doi:10.1111/anae.14794
225. Aoyama Y, Sakura S, Abe S, Tadenuma S, Saito Y. Continuous quadratus lumborum block and femoral nerve block for total Hip arthroplasty: a randomized study. J Anesth. 2020;34(3):413–420. doi:10.1007/s00540-020-02769-9
226. Suksompong S, von Bormann S, von Bormann B. Regional catheters for postoperative pain control: review and observational data. Anesthesiol Pain Med. 2020;10(1):1–10. doi:10.5812/aapm.99745
227. McCance L, Smith EC, Moore J, Forget P. Erector spinae plane block with catheter infusion for analgesia in a patient undergoing transaxillary first rib resection. Anaesth Rep. 2022;10(2):2–5. doi:10.1002/anr3.12190
228. Jarrell K, McDonald E, Shakked R, Nicholson K, Kasper V, Raikin SM. Combined popliteal catheter with single-injection vs continuous-infusion saphenous nerve block for foot and ankle surgery. Foot and Ankle Int. 2018;39(3):332–337. doi:10.1177/1071100717744331
229. Hussain N, Brull R, Zhou S, et al. Analgesic benefits of single-shot versus continuous adductor canal block for total knee arthroplasty: a systemic review and meta-analysis of randomized trials. Reg Anesth Pain Med. 2022;48(2):49–60. doi:10.1136/rapm-2022-103756
230. Patel MA, Gadsden JC, Nedeljkovic SS, et al. Brachial plexus block with liposomal bupivacaine for shoulder surgery improves analgesia and reduces opioid consumption: results from a multicenter, randomized, double-blind, controlled trial. Pain Med. 2020;21(2):387–400. doi:10.1093/pm/pnz103
231. Barletta M, Reed R. Local anesthetics: pharmacology and special preparations. Veterinary Clinics of North America - Small Animal Practice. 2019;49(6):1109–1125. doi:10.1016/j.cvsm.2019.07.004
232. Breu A, Rosenmeier K, Kujat R, Angele P, Zink W. The cytotoxicity of bupivacaine, ropivacaine, and mepivacaine on human chondrocytes and cartilage. Anesth and Analg. 2013;117(2):514–522. doi:10.1213/ANE.0b013e31829481ed
233. Johnson RL, Kopp SL, Hebl JR, Erwin PJ, Mantilla CB. Falls and major orthopaedic surgery with peripheral nerve blockade: a systematic review and meta-analysis. Br J Anaesth. 2013;110(4):518–528. doi:10.1093/bja/aet013
234. Sharma S, Iorio R, Specht LM, Davies-Lepie S, Healy WL. Complications of femoral nerve block for total knee arthroplasty. Clin. Orthop. Relat. Res. 2010;468(1):135–140. doi:10.1007/s11999-009-1025-1
235. Elkassabany NM, Antosh S, Ahmed M, et al. The risk of falls after total knee arthroplasty with the use of a femoral nerve block versus an adductor canal block: a double-blinded randomized controlled study. Anesth and Analg. 2016;122(5):1696–1703. doi:10.1213/ANE.0000000000001237
236. Wang Q, Hu J, Zhang W, Zeng Y, Yang J, Kang P. Comparison between ultrasound-guided suprainguinal fascia iliaca block and anterior quadratus lumborum block for total hip arthroplasty: a prospective, double-blind, randomized controlled trial. J Arthroplasty. 2022;37(4):763–769. doi:10.1016/j.arth.2022.01.011
237. Xu L, Gessner D, Kou A, Kasimova K, Memtsoudis SG, Mariano ER. Rate of occurrence of respiratory complications in patients who undergo shoulder arthroplasty with a continuous interscalene brachial plexus block and associated risk factors. Reg Anesth and Pain Med. 2023;48(11):540–546. doi:10.1136/rapm-2022-104264
238. Dada O, Zacarias AG, Ongaigui C, et al. Does rebound pain after peripheral nerve block for orthopedic surgery impact postoperative analgesia and opioid consumption? A narrative review. Int. J. Environ. Res. Public Health. 2019;16(18):1–12. doi:10.3390/ijerph16183257
239. Chou R, Gordon DB, De Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American pain society, the American society of regional anesthesia and pain medicine, and the American society of anesthesiologists’ committee on regional anesthesia, executive commi. J Pain. 2016;17(2):131–157. doi:10.1016/j.jpain.2015.12.008
240. Komann M, Weinmann C, Schwenkglenks M, Meissner W. Non-pharmacological methods and post-operative pain relief: an observational study. Anesthesiology and Pain Medicine. 2019;9(2):1–7. doi:10.5812/aapm.84674
241. Qaseem A, McLean RM, O’Gurek D, Batur P, Lin K, Kansagara DL. Nonpharmacologic and pharmacologic management of acute pain from non-low back, musculoskeletal injuries in adults: a clinical guideline from the American college of physicians and American academy of family physicians. Annals of Internal Medicine. 2020;173(9):739–748. doi:10.7326/M19-3602
242. Small C, Laycock H. Acute postoperative pain management. British Journal of Surgery. 2020;107(2):e70–e80. doi:10.1002/bjs.11477
243. Gao Q, Xu Q, Zhou X, Yao Z, Yao Y. A case-control study of the effects of implementing the registered nurses association of ontario guidelines for the assessment and management of postoperative pain and the use of relaxation therapy in 312 patients with bone and soft-tissue malignancy. Med Sci Monitor. 2022;58:1–7. doi:10.12659/MSM.937496
244. Chen YYK, Soens MA, Kovacheva VP. Less stress, better success: a scoping review on the effects of anxiety on anesthetic and analgesic consumption. J Anesth. 2022;36(4):532–553. doi:10.1007/s00540-022-03081-4
245. Turk DC, Okifuji A. Assessment of patients’ reporting of pain: an integrated perspective. The Lancet. 1999;353(9166):1784–1788. doi:10.1016/S0140-6736(99)01309-4
246. Kil HK, Kim WO, Chung WY, Kim GH, Seo H, Hong JY. Preoperative anxiety and pain sensitivity are independent predictors of propofol and sevoflurane requirements in general anaesthesia. Br J Anaesth. 2012;108(1):119–125. doi:10.1093/bja/aer305
247. Pan PH, Coghill R, Houle TT, et al. Multifactorial preoperative predictors for postcesarean section pain and analgesic requirement. Anesthesiology. 2006;104(3):417. doi:10.1097/00000542-200603000-00007
248. Shebl MA, Toraih E, Shebl M, et al. Preoperative anxiety and its impact on surgical outcomes: a systematic review and meta-analysis. J Clin Transl Sci. 2025;9(1):e33. doi:10.1017/cts.2025.6
249. Attri JP, Bala N, Chatrath V. Psychiatric patient and anaesthesia. Indian J Anaesth. 2012;56(1):8–13. doi:10.4103/0019-5049.93337
250. Huyse FJ, Touw DJ, van Schijndel RS, de Lange JJ, Slaets JPJ. Psychotropic drugs and the perioperative period: a proposal for a guideline in elective surgery. Psychosomatics. 2006;47(1):8–22. doi:10.1176/appi.psy.47.1.8
251. Chen W, Sun JN, Hu ZH, Zhang Y, Chen XY, Feng S. Cognitive behavioral therapy cannot relieve postoperative pain and improve joint function after total knee arthroplasty in patients aged 70 years and older. Aging Clin. Exp. Res. 2021;33(12):3293–3302. doi:10.1007/s40520-021-01870-7
252. Powell R, Scott NW, Manyande A, et al. Psychological preparation and postoperative outcomes for adults undergoing surgery under general anaesthesia. Cochrane Database Syst. Rev. 2016;2016(5). doi:10.1002/14651858.CD008646.pub2
253. Kidanemariam BY, Elsholz T, Simel LL, Tesfamariam EH, Andemeskel YM. Utilization of non-pharmacological methods and the perceived barriers for adult postoperative pain management by the nurses at selected National Hospitals in Asmara, Eritrea. BMC Nurs. 2020;19(1):1–10. doi:10.1186/s12912-020-00492-0
254. El-Boghdadly K, Levy NA, Fawcett WJ, et al. Peri-operative pain management in adults: a multidisciplinary consensus statement from the association of anaesthetists and the British pain society. Anaesthesia. 2024;79(11):1220–1236. doi:10.1111/anae.16391
255. Schmidt K, Johnson D, Rose K, Brooks A, Dakroub B, Jorgenson T. Perioperative pain management: leveraging clinical pharmacist practitioners to improve opioid safety in veterans. Am J Health Syst Pharm. 2025;zxaf290. doi:10.1093/ajhp/zxaf290
256. Coulson EE, Kral LA. The clinical pharmacist’s role in perioperative surgical pain management. J Pain Palliat Care Pharmacother. 2020;34(3):120–126. doi:10.1080/15360288.2020.1734141
257. Nguyen HT, Pham NK, Le DT, et al. The role of clinical pharmacists in multidisciplinary teams for postoperative pain management in lumbar spine surgery: a prospective study. J Pharm Pharmacogn Res. 2025;13(5):1356–1371. doi:10.56499/jppres24.2131_13.5.1356
258. Wang R, Liu B, Feng X, et al. The effect of pharmacist-initiated perioperative multidisciplinary pharmaceutical care model and clinical pathway on pain management in patients undergoing orthopedic surgery: a before-after study. Int J Clin Pharm. 2023;45(4):929–939. doi:10.1007/s11096-023-01575-z
259. Barat E, Chenailler C, Gillibert A, et al. Impact of clinical pharmacist consultations on postoperative pain in ambulatory surgery. Int. J. Environ. Res. Public Health. 2023;20(5). doi:10.3390/ijerph20053967
260. Naseralallah L, Koraysh S, Alasmar M, Aboujabal B. The role of pharmacists in mitigating medication errors in the perioperative setting: a systematic review. Syst Rev. 2025;14(1):12. doi:10.1186/s13643-024-02710-1
261. Naseralallah L, Koraysh S, Aboujabal B, Alasmar M. Interventions and impact of pharmacist-delivered services in perioperative setting on clinically important outcomes: a systematic review and meta-analysis. Ther Adv Drug Saf. 2024;15:20420986241260169. doi:10.1177/20420986241260169
262. Lu J, Chen M, He G, Chen B, Wang R. Evaluating clinical pharmacists’ involvement in postoperative acute pain services: a multicenter survey in Guangdong Province, China. Front Pharmacol. 2023;14:1283071. doi:10.3389/fphar.2023.1283071
263. Naseralallah L, Koraysh S, Alasmar M, Aboujabal B. Effect of pharmacist care on clinical outcomes and therapy optimization in perioperative settings: a systematic review. Am J Health Syst Pharm. 2024;82(1):44–73. doi:10.1093/ajhp/zxae177
264. Hyland SJ, Brockhaus KK, Vincent WR, et al. Perioperative pain management and opioid stewardship: a practical guide. Healthcare. 2021;9(3). doi:10.3390/healthcare9030333
265. Cryar KA, Hereford T, Edwards PK, Siegel E, Barnes CL, Mears SC. Preoperative smoking and narcotic, benzodiazepine, and tramadol use are risk factors for narcotic use after hip and knee arthroplasty. J Arthroplasty. 2018;33(9):2774–2779. doi:10.1016/j.arth.2018.03.066
266. Doleman B, Leonardi-Bee J, Heinink TP, Bhattacharjee D, Lund JN, Williams JP. Pre-emptive and preventive opioids for postoperative pain in adults undergoing all types of surgery. Cochrane Database Syst Rev. 2018;12(12):CD012624. doi:10.1002/14651858.CD012624.pub2
267. Manworren RCB. Multimodal pain management and the future of a personalized medicine approach to pain. AORN J. 2015;101(3):308–314;quiz315–318. doi:10.1016/j.aorn.2014.12.009
268. Kintu A, Abdulla S, Lubikire A, et al. Postoperative pain after cesarean section: assessment and management in a tertiary hospital in a low-income country. BMC Health Serv Res. 2019;19(1):68. doi:10.1186/s12913-019-3911-x
269. Xu J, Liu X, Zhao J, et al. Comprehensive review on personalized pain assessment and multimodal interventions for postoperative recovery optimization. J Pain Res. 2025;18:2791–2804. doi:10.2147/JPR.S516249
270. Juma SL, Ma J, Rasmussen JL, et al. Nonopioid pain protocols vs. opioid analgesia for postoperative pain control following arthroscopic surgeries: a literature review. Cureus. 2025;17(5):e83357. doi:10.7759/cureus.83357
271. Jildeh TR, Abbas MJ, Hasan L, Moutzouros V, Okoroha KR. Multimodal nonopioid pain protocol provides better or equivalent pain control compared to opioid analgesia following arthroscopic rotator cuff surgery: a prospective randomized controlled trial. Arthroscopy. 2022;38(4):1077–1085. doi:10.1016/j.arthro.2021.11.028
272. Akelman MR, Kim ST, Waterman BR. Editorial commentary: multimodal, opioid-free pain management after rotator cuff repair may be safe and effective, and decreases the risk of drug abuse. Arthroscopy. 2022;38(4):1086–1088. doi:10.1016/j.arthro.2022.01.040
273. Kara H, Çamlı DÇ. From knowledge to practice, intensive care nurses’ pain management behaviors in Turkey: a cross sectional study. BMC Nurs. 2025;24(1):1469. doi:10.1186/s12912-025-04107-4
274. Kim MK, Kang H. Personalized perioperative pain management: a narrative review. Ewha Med J. 2025;48(4):e62. doi:10.12771/emj.2025.00773
275. Gordon DB, de Leon-Casasola OA, Wu CL, Sluka KA, Brennan TJ, Chou R. Research gaps in practice guidelines for acute postoperative pain management in adults: findings from a review of the evidence for an American pain society clinical practice guideline. J Pain. 2016;17(2):158–166. doi:10.1016/j.jpain.2015.10.023
276. Joseph JM, Gori D, Curtin C, et al. Gaps in standardized postoperative pain management quality measures: a systematic review. Surgery. 2022;171(2):453–458. doi:10.1016/j.surg.2021.08.004
277. Snell A, Lobaina D, Densley S, et al. Disparities in postoperative pain management: a scoping review of prescription practices and social determinants of health. Pharmacy. 2025;13(2):34. doi:10.3390/pharmacy13020034
278. Hamilton WG, Gargiulo JM, Parks NL. Using pharmacogenetics to structure individual pain management protocols in total knee arthroplasty. Bone Joint J. 2020;102-B(6_Supple_A):73–78. doi:10.1302/0301-620X.102B6.BJJ-2019-1539.R1
279. Hamilton WG, Gargiulo JM, Reynolds TR, Parks NL. Prospective randomized study using pharmacogenetics to customize postoperative pain medication following hip and knee arthroplasty. J Arthroplasty. 2022;37(6S):S76–S81. doi:10.1016/j.arth.2022.02.037
280. Aroke EN, McMullan SP, Woodfin KO, Richey R, Doss J, Wilbanks BA. A practical approach to acute postoperative pain management in chronic pain patients. J Perianesth Nurs. 2020;35(6):564–573. doi:10.1016/j.jopan.2020.03.002
281. Johnson ZD, Connors SW, Christian Z, et al. Development and internal validation of the postoperative analgesic intake needs score: a predictive model for post-operative narcotic requirement after spine surgery. Global Spine J. 2023;13(8):2135–2143. doi:10.1177/21925682211072490
282. Motamed C. Clinical update on patient-controlled analgesia for acute postoperative pain. Pharmacy. 2022;10(1):22. doi:10.3390/pharmacy10010022
283. Nie ZB, Li ZH, Lu B, Guo YY, Zhang R. Hydromorphone vs sufentanil in patient-controlled analgesia for postoperative pain management. Medicine. 2022;101(3):e28615. doi:10.1097/MD.0000000000028615
284. DiGiusto M, Bhalla T, Martin D, Foerschler D, Jones MJ, Tobias JD. Patient-controlled analgesia in the pediatric population: morphine versus hydromorphone. J Pain Res. 2014;7:471–475. doi:10.2147/JPR.S64497
285. Pan Y, Wang Y, Lie D, et al. Effectiveness of analgesia with hydromorphone hydrochloride for postoperative pain following surgical repair of structural congenital malformations in children: a randomized controlled trial. BMC Anesth. 2021;21(1):192. doi:10.1186/s12871-021-01412-8
286. Yang Y, Wu J, Li H, et al. Prospective investigation of intravenous patient-controlled analgesia with hydromorphone or sufentanil: impact on mood, opioid adverse effects, and recovery. BMC Anesthe. 2018;18:37. doi:10.1186/s12871-018-0500-1
287. Tseng WC, Lin WL, Lai HC, Huang TW, Chen PH, Wu ZF. Fentanyl-based intravenous patient-controlled analgesia with low dose of ketamine is not inferior to thoracic epidural analgesia for acute post-thoracotomy pain following video-assisted thoracic surgery: a randomized controlled study. Medicine. 2019;98(28):e16403. doi:10.1097/MD.0000000000016403
288. Zhou Y, Huang JX, Lu XH, Zhang YF, Zhang W. Patient-controlled intravenous analgesia for non-small cell lung cancer patient after thoracotomy. J Cancer Res Ther. 2015;11 Suppl 1:C128–130. doi:10.4103/0973-1482.163870
289. Jia Y, Zhou R, Li Z, et al. Analgesic Effects and safety of dexmedetomidine added to nalbuphine or sufentanil patient-controlled intravenous analgesia for children after tonsillectomy adenoidectomy. Front Pharmacol. 2022;13:908212. doi:10.3389/fphar.2022.908212
290. Koh J, Lee J, Kim SY, Choi S, Han D. Postoperative pain and intravenous patient-controlled analgesia-related adverse effects in young and elderly patients. Medicine. 2015;94:e2008. doi:10.1097/MD.0000000000002008
291. Anaesthesia and pain management: patient controlled analgesia PCA. Available from: https://www.rch.org.au/anaes/pain_management/Patient_Controlled_Analgesia_PCA/.
292. Patient-controlled analgesia pumps. March 22, 2024. Available from: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/patientcontrolled-analgesia-pumps.
293. Patient Controlled Analgesia (PCA) | vancouver Coastal Health. Available from: https://www.vch.ca/en/patients-and-visitors/patient-guides/patient-guide-anesthesia/patient-controlled-analgesia-pca.
294. Sinha S, Munikrishnan V, Montgomery J, Mitchell SJ. The impact of patient-controlled analgesia on laparoscopic cholecystectomy. Ann R Coll Surg Engl. 2025. doi:10.1308/003588407X183337
295. Jung H, Lee KH, Jeong Y, et al. Effect of fentanyl-based intravenous patient-controlled analgesia with and without basal infusion on postoperative opioid consumption and opioid-related side effects: a retrospective cohort study. JPR. 2020;13:3095–3106. doi:10.2147/JPR.S281041
296. George JA, Lin EE, Hanna MN, et al. The effect of intravenous opioid patient-controlled analgesia with and without background infusion on respiratory depression: a meta-analysis. J Opioid Manag. 2010;6(1):47–54. doi:10.5055/jom.2010.0004
297. What is the role of Patient-Controlled Analgesia (PCA) in acute pain management? November 9, 2025. Available from:. https://droracle.ai/articles/496266/what-is-the-role-of-patient-controlled-analgesia-pca-in.
298. Investigación RS. An evaluation of patient-controlled analgesia. effectiveness, safety, and patient satisfaction in postoperative pain management. ▷ RSI - Revista Sanitaria de Investigación.
299. Andersena JV, Karlsen APH, Olsen MH, Pedersen NK. Causal machine learning for patient-level intraoperative opioid dose prediction from electronic health records. arXiv. doi:10.48550/arXiv.2508.09059
300. Sun Y, Kang J, Brummett C, Li Y. Individualized risk assessment of preoperative opioid use by interpretable neural network regression. arXiv. doi:10.48550/arXiv.2205.08370
301. Lv S, Sun N, Hao C, Li J, Li Y. Development and validation of machine learning models for predicting post-cesarean pain and individualized pain management strategies: a multicenter study. BMC Anesthesiol. 2025;25(1):170. doi:10.1186/s12871-025-03034-w
302. Oladipupo AA, Akinola MM, Omogbolahan US. Predictive model for post-operative pain management in saudi arabian patients undergoing major abdominal surgery. J Adv Med Med Res. 2025;2(1):44. doi:10.4103/ATMR.ATMR_9_25
303. Chu X, Song J, Wang J, Kang H. A stacking ensemble machine learning model for predicting postoperative axial pain intensity in patients with degenerative cervical myelopathy. Sci Rep. 2025;15(1):9954. doi:10.1038/s41598-025-94755-y
304. Cai Z, Sun Q, Li C, Xu J, Jiang B. Machine-learning-based prediction by stacking ensemble strategy for surgical outcomes in patients with degenerative cervical myelopathy. J Orthop Surg Res. 2024;19(1):539. doi:10.1186/s13018-024-05004-3
305. Fan B. Artificial Intelligence in Pain Management. In: Xia M, Jiang H editors. Artificial Intelligence in Anesthesiology. Springer Nature; 2023:79–84. doi:10.1007/978-981-99-5925-9_9.
306. Subramanian A, Cao R, Naeini EK, et al. Multimodal pain recognition in postoperative patients: machine learning approach. JMIR Form Res. 2025;9:e67969. doi:10.2196/67969
307. Aqajari SAH, Cao R, Kasaeyan Naeini E, et al. Pain assessment tool with electrodermal activity for postoperative patients: method validation study. JMIR mHealth uHealth. 2021;9(5):e25258. doi:10.2196/25258
308. Ayena JC, Bouayed A, Ben Arous M, et al. Predicting chronic pain using wearable devices: a scoping review of sensor capabilities, data security, and standards compliance. Front Digit Health. 2025;7:1581285. doi:10.3389/fdgth.2025.1581285
309. Dinh-Le C, Chuang R, Chokshi S, Mann D. Wearable health technology and electronic health record integration: scoping review and future directions. JMIR mHealth uHealth. 2019;7(9):e12861. doi:10.2196/12861
310. Zieliński J, Morawska-Kochman M, Zatoński T. Pain assessment and management in children in the postoperative period: a review of the most commonly used postoperative pain assessment tools, new diagnostic methods and the latest guidelines for postoperative pain therapy in children. Adv Clin Exp Med. 2020;29(3):365–374. doi:10.17219/acem/112600
311. Makhlouf MM, Garibay ER, Jenkins BN, Kain ZN, Fortier MA. Postoperative pain: factors and tools to improve pain management in children. Pain Manag. 2019;9(4):389–397. doi:10.2217/pmt-2018-0079
312. Düzgün MV, Özdemir C, Işler A, Karazeybek E. Technology-based interventions for pain in children undergoing surgery: a systematic review and meta-analysis. Int J Nurs Pract. 2025;31(1):e13322. doi:10.1111/ijn.13322
313. Wearable devices: current status and opportunities in pain assessment and management. Available from: http://ouci.dntb.gov.ua/en/works/leqrgjEl/?utm_source=chatgpt.com.
314. Reena Han DNL. The application of machine learning and artificial intelligence in patient controlled analgesia - towards personalized pain management. Eur. J. Med. Res Clin Trials. 2024;6(1). doi:10.17303/ejmrc.2024.6.104
315. Green M, Hayley A, Gunnersen JM, et al. Transforming chronic pain management: integrating neuromodulation with advanced technologies to tackle cognitive dysfunction – a narrative review. J Pain Res. 2025;18:2497–2507. doi:10.2147/JPR.S514285
316. Giravi HY, Biskupiak Z, Tyler LS, Bulaj G. Adjunct digital interventions improve opioid-based pain management: impact of virtual reality and mobile applications on patient-centered pharmacy care. Front Digit Health. 2022;4. doi:10.3389/fdgth.2022.884047
317. Belani KG. Precision medicine and the expanding perioperative role by anaesthesiologists. Indian J Anaesth. 2025;69(8):745–747. doi:10.4103/ija.ija_581_25
318. Pain medicines after surgery. Mayo Clinic. Available from: https://www.mayoclinic.org/tests-procedures/anesthesia/in-depth/pain-medications/art-20046452.
319. Verret M, Lauzier F, Zarychanski R, et al. Perioperative Use of gabapentinoids for the management of postoperative acute pain: a systematic review and meta-analysis. Anesthesiology. 2020;133(2):265. doi:10.1097/ALN.0000000000003428
320. Themes UFO. Perioperative pain management. Anesthesia Key. 2017. Available from: https://aneskey.com/perioperative-pain-management-3/.
321. da S NED, de Lara FST, Abreu SN, et al. Esmolol as an adjunct in multimodal anesthesia: a systematic review and meta-analysis of its opioid-sparing and analgesic effects. Anesth Analg. 2025. doi:10.1213/ANE.0000000000007787
322. Yao J, Wang C, Szmuk P, et al. Dexamethasone, but not esketamine, reduces rebound pain after interscalene nerve block: a randomized factorial trial. Drug Des Devel Ther. 2025;19:11511–11523. doi:10.2147/DDDT.S569175
323. Chen J, Pan Z, Zheng J. Effect of intravenous esketamine on rebound pain following single-shot brachial plexus block in patients undergoing shoulder arthroscopic surgery: a prospective, randomized, placebo-controlled study. J Pain Res. 2025;18:5235–5248. doi:10.2147/JPR.S533774
324. Moore PA, Hersh EV. Combining ibuprofen and Acetaminophen for acute pain management after third-molar extractions: translating clinical research to dental practice. J Am Dent Assoc. 2013;144(8):898–908. doi:10.14219/jada.archive.2013.0207
325. Bonilla-Jaime H, Sánchez-Salcedo JA, Estevez-Cabrera MM, Molina-Jiménez T, Cortes-Altamirano JL, Alfaro-Rodríguez A. Depression and Pain: use of Antidepressants. Curr Neuropharmacol. 2021;20(2):384–402. doi:10.2174/1570159x19666210609161447
326. V BJ, Robbins CE, Mehio AK, Aghazadeh M, Talmo CT. Pharmacologic pain management before and after total joint replacement of the hip and knee. Clin in Geriatric Med. 2012;28(3):459–470. doi:10.1016/j.cger.2012.05.004
327. Tan M, Law LSC, Gan TJ. Optimizing pain management to facilitate enhanced recovery after surgery pathways. Can J Anaesth. 2015;62(2):203–218. doi:10.1007/s12630-014-0275-x
328. Lavand’homme PM, Kehlet H, Rawal N, Joshi GP. Pain management after total knee arthroplasty: procedure specific postoperative pain managemenT recommendations. Eur J Anaesthesiol. 2022;39(9):743–757. doi:10.1097/EJA.0000000000001691
329. Hahn J, Jo Y, Yoo SH, Shin J, Yu YM, Ah YM. Risk of major adverse events associated with gabapentinoid and opioid combination therapy: a systematic review and meta-analysis. Front Pharmacol. 2022;13. doi:10.3389/fphar.2022.1009950
330. Jipa M, Isac S, Klimko A, et al. Opioid-sparing analgesia impacts the perioperative anesthetic management in major abdominal surgery. Medicina. 2022;58(4):1–10. doi:10.3390/medicina58040487
331. Thapa P, Euasobhon P. Chronic postsurgical pain: current evidence for prevention and management. Korean Journal of Pain. 2018;31(3):155–173. doi:10.3344/kjp.2018.31.3.155
332. Bakker CJ, Wise KL, Williams BR, Swiontkowski MF. Complementary and alternative medicine for postoperative pain: a systematic review. J Bone Joint Surg. 2020;102(1 Suppl):36–46. doi:10.2106/JBJS.19.01439
333. Prabhakar NK, Chadwick AL, Nwaneshiudu C, et al. Management of postoperative pain in patients following spine surgery: a narrative review. Int J General Med. 2022;15(May):4535–4549. doi:10.2147/IJGM.S292698
334. Zheng Y, Kostenbader K, Barrett T, et al. Tolerability of biphasic-release hydrocodone bitartrate/acetaminophen tablets (mnk-155): a phase iii, multicenter, open-label study in patients with osteoarthritis or chronic low back pain. Clin Ther. 2015;37(6):1235–1247. doi:10.1016/j.clinthera.2015.03.019
335. Xiang X, Yuan X, Lian Y, Fang J, Wu Y. Effect of oxycodone hydrochloride combined with flurbiprofen axetil for intravenous patient-controlled analgesia in lower abdominal patients. Med. 2018;97(7):e9911. doi:10.1097/MD.0000000000009911
336. Bixby AL, VandenBerg A, Bostwick JR. Clinical management of bleeding risk with antidepressants. Ann Pharmacother. 2019;53(2):186–194. doi:10.1177/1060028018794005
337. Angeles PC, Robertsen I, Seeberg LT, et al. The influence of bariatric surgery on oral drug bioavailability in patients with obesity: a systematic review. Obes Rev. 2019;20(9):1299–1311. doi:10.1111/obr.12869
338. Leonie. Pain relief after sleeve gastrectomy: is ibuprofen ok? dr peter hamer. 2025. Available from: https://www.drpeterhamer.com.au/ibuprofen-after-sleeve-gastrectomy/.
339. Porat D, Dahan A. Pharmacokinetics after bariatric surgery: adverse effects and drug safety issues in bariatric patients. Expert Rev Clin Pharmacol. 2025;18(3):101–108. doi:10.1080/17512433.2025.2462093
340. Dada O, Gonzalez Zacarias A, Ongaigui C, et al. Does rebound pain after peripheral nerve block for orthopedic surgery impact postoperative analgesia and opioid consumption? a narrative review. Int J Environ Res Public Health. 2019;16(18):3257. doi:10.3390/ijerph16183257
341. Rajput K, Shergill S, Chow RM, Vadivelu N, Kaye AD. Enhanced recovery after surgery: opioid sparing strategies after discharge: a review. Curr Pain Headache Rep. 2022;26(2):93–102. doi:10.1007/s11916-022-01009-x
342. Greer N, Sultan S, Shaukat A, et al. SUMMARY AND DISCUSSION. In: Enhanced Recovery After Surgery (ERAS) Programs for Patients Undergoing Colorectal Surgery [Internet]. Department of Veterans Affairs (US); 2017. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519369/.
343. Paton F, Chambers D, Wilson P, et al. Effectiveness and implementation of enhanced recovery after surgery programmes: a rapid evidence synthesis. BMJ Open. 2014;4(7):e005015. doi:10.1136/bmjopen-2014-005015
344. Hughes MJ, Ventham NT, McNally S, Harrison E, Wigmore S. Analgesia after open abdominal surgery in the setting of enhanced recovery surgery: a systematic review and meta-analysis. JAMA Surg. 2014;149(12):1224–1230. doi:10.1001/jamasurg.2014.210
345. Cheung CK, Adeola JO, Beutler SS, Urman RD. Postoperative pain management in enhanced recovery pathways. J Pain Res. 2022;15:123–135. doi:10.2147/JPR.S231774
346. JXC K, de Vos M, Kojic K, et al. Healthcare delivery gaps in pain management within the first 3 months after discharge from inpatient noncardiac surgeries: a scoping review. Br J Anaesth. 2023;131(5):925–936. doi:10.1016/j.bja.2023.08.006
347. Jiang W, Qin Y, Chen L. Bibliometric analysis of multimodal analgesia research in the perioperative period: trends, contributions, and emerging areas (2013–2023). Front Med. 2025;12:1573112. doi:10.3389/fmed.2025.1573112
348. Scholars@duke publication: perioperative multimodal pain management: an evidence-based update. Available from: https://scholars.duke.edu/publication/1442477?utm_source=chatgpt.com.
349. Kincaid S, How J, Agrawal DK. Multimodal analgesia in the perioperative period of major surgeries: an in-depth analysis. Anesth Crit Care. 2025;7(3):68–76.
350. Pharmacogenetics: a path to better pain management. Rxight. October 24, 2024. Available from: https://www.rxight.com/news/pain-management.
351. da SIM, Plaza-Díaz A, Ruiz-Ramos J, et al. The role of pharmacogenetic biomarkers in pain. Biomedicines. 2025;13(8). doi:10.3390/biomedicines13081935
352. Branford R, Droney J, Ross JR. Opioid genetics: the key to personalized pain control? Clin Genet. 2012;82(4):301–310. doi:10.1111/j.1399-0004.2012.01923.x
353. Groot JAN, Harmsze AM, van Dongen EHPA, Knibbe CAJ, van Oud-Alblas HJB. Pharmacogenetics in perioperative care: understanding the impact of genetic variants on patient management. J Clin Anesth. 2026;108:112064. doi:10.1016/j.jclinane.2025.112064
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of a Non-Opioid Multimodal Analgesia Protocol with Opioid-Based Patient-Controlled Analgesia for Pain Control Following Robot-Assisted Radical Prostatectomy: A Randomized, Non-Inferiority Trial
Lee JE, Oh J, Lee JN, Ri HS, Lee CS, Yeo J
Journal of Pain Research 2023, 16:563-572
Published Date: 18 February 2023
Oliceridine for the Management of Moderate to Severe Acute Postoperative Pain: A Narrative Review
Daksla N, Wang A, Jin Z, Gupta A, Bergese SD
Drug Design, Development and Therapy 2023, 17:875-886
Published Date: 22 March 2023
Review of the Current Situation of Postoperative Pain and Causes of Inadequate Pain Management in Africa
Gao L, Mu H, Lin Y, Wen Q, Gao P
Journal of Pain Research 2023, 16:1767-1778
Published Date: 29 May 2023
Comparative Effectiveness of Non-Pharmacological Interventions for Pain and Quality of Life in Women with Endometriosis: A Systematic Review and Network Meta-Analysis
Zheng X, Wang Y, Li H, Zhang J, Liu J, Zheng X, Zhang J, Fan G, Sun Y, Li B, Jiao J, Zuo G, Fan X, She Y
Journal of Pain Research 2026, 19:577080
Published Date: 20 February 2026