Back to Journals » International Journal of Women's Health » Volume 18
Executive Functions Mediate Between Endometriosis Burden and Women’s Daily Life
Authors Khatib S ![]() , Hassan H, Abd Elgani S, Reiss A, Engel -Yeger B
, Hassan H, Abd Elgani S, Reiss A, Engel -Yeger B
Received 10 March 2026
Accepted for publication 16 May 2026
Published 3 June 2026 Volume 2026:18 606990
DOI https://doi.org/10.2147/IJWH.S606990
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marta Barba
Sewar Khatib,1 Haya Hassan,2 Suzan Abd Elgani,2 Ari Reiss,2 Batya Engel -Yeger1
1Department of Occupational Therapy, University of Haifa, Haifa, Israel; 2Department of Obstetrics and Gynecology, Emek Medical Center, Afula, Israel
Correspondence: Sewar Khatib, Department of occupational therapy, university of Haifa, Haifa, Israel, Tel +972-509967091, Email [email protected]
Purpose: To examine (1) group differences in executive functioning, disease burden, occupational balance and quality of life between women with endometriosis and healthy controls; (2) associations between pain-related and psychological disease burden -specifically pain catastrophizing and emotional distress- and occupational balance and quality of life; and (3) whether executive functioning mediates the relationships between disease burden and quality of life and occupational balance.
Patients and Methods: This cross-sectional correlational study included 103 women aged 18– 35 years, compromising 43 women with clinically confirmed endometriosis recruited from a specialized endometriosis clinic and 60 age-matched healthy controls. Disease burden was assessed using measures of pain severity (Visual Analog Scale – VAS), pain catastrophizing (Pain catastrophising scale -PCS), and emotional distress (Depression Anxiety Stress Scale – DASS21). Executive functioning (Barkley Deficits in Executive Functioning Scale–Short Form -BDEFS-SF), occupational balance (Occupational Balance Questionnaire – OBQ11), and quality of life (World Health Organization Quality of Life–BREF - WHOQOL-BREF). Socio-demographic and clinical characteristics were collected to characterize the study sample and inform interpretation of the findings. Mediation analyses were conducted to examine executive functioning as a mechanism linking disease burden to functional outcomes, using Hayes’ PROCESS.
Results: Compared with healthy controls, women with endometriosis reported significantly greater pain severity, pain catastrophizing, emotional distress, and executive functioning difficulties, alongside lower occupational balance and reduced quality of life (all p < 0.001). Within the endometriosis group, higher levels of pain catastrophizing and emotional distress were associated with poorer executive functioning, which in turn was associated with lower occupational balance and quality of life (all p < 0.001). Mediation analyses indicated that executive functioning fully mediated the associations between psychological disease burden and both quality of life and occupational balance, such that the direct associations between psychological disease burden and functional outcomes were no longer significant after accounting for executive functioning.
Conclusion: Executive functioning represents a central mechanism through which pain-related and psychological disease burden translate into disruptions in daily life among women with endometriosis. These findings extend symptom-based models toward a more integrative, function-oriented understanding of endometriosis and highlight executive functioning as a meaningful target for comprehensive, person-centered assessment and intervention.
Keywords: endometriosis, meta-cognition, executive functions, occupational balance, quality of life
Introduction
Endometriosis is a chronic, inflammatory gynaecological condition characterized by the presence of endometrial-like tissue outside the uterine cavity, affecting approximately 10% of women of reproductive age worldwide.1–3 The condition is commonly associated with chronic pelvic pain, dysmenorrhea, dyspareunia, infertility, fatigue, and sleep disturbances, leading to substantial physical and emotional burden.4–6
Pain represents the core symptom of endometriosis and arises from complex pathophysiological mechanisms involving inflammatory processes, altered immune responses, and changes in peripheral and central nervous system functioning.2,5,7,8 Persistent pain is often accompanied by heightened pain catastrophizing, a cognitive-emotional response characterized by rumination, magnification, and helplessness in relation to pain.9,10 High levels of pain catastrophizing have been consistently associated with greater pain intensity, emotional distress, reduced coping capacity, and poorer health outcomes, as found in chronic pain conditions, including endometriosis.9,10
Women with endometriosis frequently experience elevated levels of depression, anxiety, and stress, reflecting the cumulative psychological burden which are related to the mentioned chronic symptoms, fertility concerns, uncertainty regarding prognosis, and repeated medical interventions.4,11,12
Despite its high prevalence, endometriosis is frequently underdiagnosed, with diagnostic delays of several years being common, further exacerbating symptoms severity and psychosocial distress.1,13 This burden contributes to a marked reduction in daily function and quality of life (QoL) and increased healthcare utilization among affected women.5,12,14–17 Women with endometriosis often report difficulties maintaining consistent engagement in daily activities, roles and occupations, including challenges in intimate relationships, work and academic participation, household responsibilities, social relationships, and leisure activities.5,6,16,18–22 These functional limitations have important implications not only for individual well-being but also for societal and economic outcomes, including productivity loss and increased healthcare costs. Despite growing recognition of these consequences, research in endometriosis has predominantly focused on symptom reduction, with relatively limited attention to the mechanisms that affect coping with disease burden, translated into impairments in daily functioning.5,22
From a biopsychosocial perspective, the World Health Organization’s International Classification of Functioning, Disability and Health (ICF) framework emphasizes that health care should refer to the dynamic interactions between disease, affected body functions and structures, and people’s daily activity performance and QOL.23–25 Applied to endometriosis, this framework highlights that pain and emotional distress (body functions) may restrict daily activities, ultimately shaping QoL. Within this context, daily functioning reflects the individual’s ability to manage everyday demands, maintain balance among life roles, in work, family, and social life.23,26 Occupational balance, defined as a satisfactory distribution and harmony among daily activities, has emerged as a significant indicator of health and well-being, yet remains largely unexplored in women with endometriosis.26–28
Importantly, individuals vary considerably in how they cope with similar levels of disease burden. While some women maintain relatively stable occupational balance and functioning despite significant symptoms, others experience pronounced functional decline.29–31 This variability is related to the presence of modifiable cognitive and psychological factors that may buffer or exacerbate the impact of endometriosis on daily life.29 One such factor is executive functioning (EF), a set of higher-order cognitive processes, mainly managed by the frontal lobe,32,33 which are responsible for performing complex daily tasks, adapting to changing circumstances, and implementing effective coping strategies in the context of chronic illness.29,34 In the context of endometriosis, EF is particularly relevant because managing a chronic and fluctuating condition requires continuous self-regulation, including planning daily activities around pain, adapting to symptom variability, regulating emotional responses, and maintaining engagement in meaningful occupations despite physical and psychological burden. These ongoing demands place sustained pressure on executive processes and may contribute to variability in women’s ability to maintain daily functioning and occupational balance. Therefore, examining EF as a potential mechanism linking disease burden to functional outcomes may provide important insight into differences in QOL among women with endometriosis. EF enables individuals to regulate behaviour, emotions, and thoughts in a goal-directed manner.29,34 Core components of EF include attention, planning, organization, inhibition, initiation, cognitive flexibility, self-monitoring, and emotional regulation.26,29,34 Consistent with Barkley’s model of EFs as higher-order self-regulatory capacities that support goal-directed behaviour over time, impairments in executive functioning may undermine individuals’ ability to manage symptoms, regulating emotional responses to pain, maintaining adherence to treatment recommendations organize daily activities, and maintain function and occupational balance despite chronic disease burden.35 Whereas executive difficulties may lead to avoidance, disengagement, emotional dysregulation, and functional decline.7,36–39
Growing evidence from chronic pain research indicates that disease burden, resulting from persistent pain and emotional distress is associated with alterations in EF. Neuroimaging and behavioural studies suggest that chronic pain conditions may be linked to functional and structural changes in prefrontal brain regions implicated in cognitive control and self-regulation.7,34,36,37,40,41 In endometriosis specifically, a small but growing body of research has reported subjective cognitive complaints and objective alterations in EF as cognitive control networks, particularly among women experiencing higher pain intensity and longer disease duration.29,37 However, the current evidence base remains limited and not yet conclusive. These findings raise the possibility that executive dysfunction may represent a key mechanism linking symptom burden to impaired daily functioning and reduced quality of life in this population.
Despite this relevance, the role of EFs in endometriosis has received limited empirical attention, and few studies have examined EF within an integrative model that links disease burden, daily functioning, occupational balance and QoL. Taken together, this literature suggests that EFs may play a mediating role in the relationship between endometriosis-related disease burden and women’s daily functioning and QoL.
The present study aimed to elaborate the knowledge about the role of EF in women with endometriosis and specifically examine whether EF mediates between disease burden and functional outcomes with a special attention to occupational balance and QOL.
By integrating clinical, psychological, and cognitive perspectives within the ICF framework, this study seeks to clarify mechanisms underlying functional impairment in endometriosis and to identify potential targets for intervention aimed at improving women’s daily lives beyond symptom management alone.
It was hypothesized that: (1) women with endometriosis would exhibit greater executive function deficits compared with healthy controls. (2) higher levels of endometriosis-related burden as expressed in pain intensity, pain catastrophizing, and emotional distress would significantly correlate with poorer executive functioning, reduced occupational balance and lower QoL. (3) EF would mediate between disease burden, occupational balance and QOL.
Materials and Methods
Study Design and Participants
This cross-sectional correlational study was conducted between December 2024 and December 2025 and followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Power analysis indicated that a minimum sample of 102 participants was required to detect a medium effect size (f2 = 0.25) with 90% statistical power at an alpha level of.05. The final sample included 103 participants, meeting this requirement.
The endometriosis group included 43 women aged 18–35 years with clinically confirmed endometriosis. Inclusion criteria for the endometriosis group were: (1) women aged 18–35 years; (2) a clinically confirmed diagnosis of endometriosis; and (3) ability to complete the questionnaire in Hebrew or Arabic. For the control group, inclusion criteria included women aged 18–35 years with no known diagnosis of endometriosis or other chronic conditions affecting daily functioning. Diagnosis was established based on imaging findings (transvaginal ultrasound and/or MRI), surgical confirmation (laparoscopy), and comprehensive clinical evaluation, including gynecological examination and detailed medical history (anamnestic assessment). Participants were recruited from a specialized endometriosis clinic at Emek medical center, located in Northern Israel. Diagnosis was confirmed by gynecologists specializing in endometriosis based on clinical evaluation and medical records.
The control group comprised 60 healthy women, matched by age and sociodemographic characteristics to the endometriosis group.
Exclusion criteria for both groups included the presence of severe chronic medical conditions likely to substantially affect daily functioning (eg, cancer, multiple sclerosis), diagnosed psychiatric disorders, pregnancy or the postpartum period, and a history of major surgical procedures that could bias cognitive, emotional, or functional outcomes. Participants’ sociodemographic characteristics and health status are presented in Table 1.
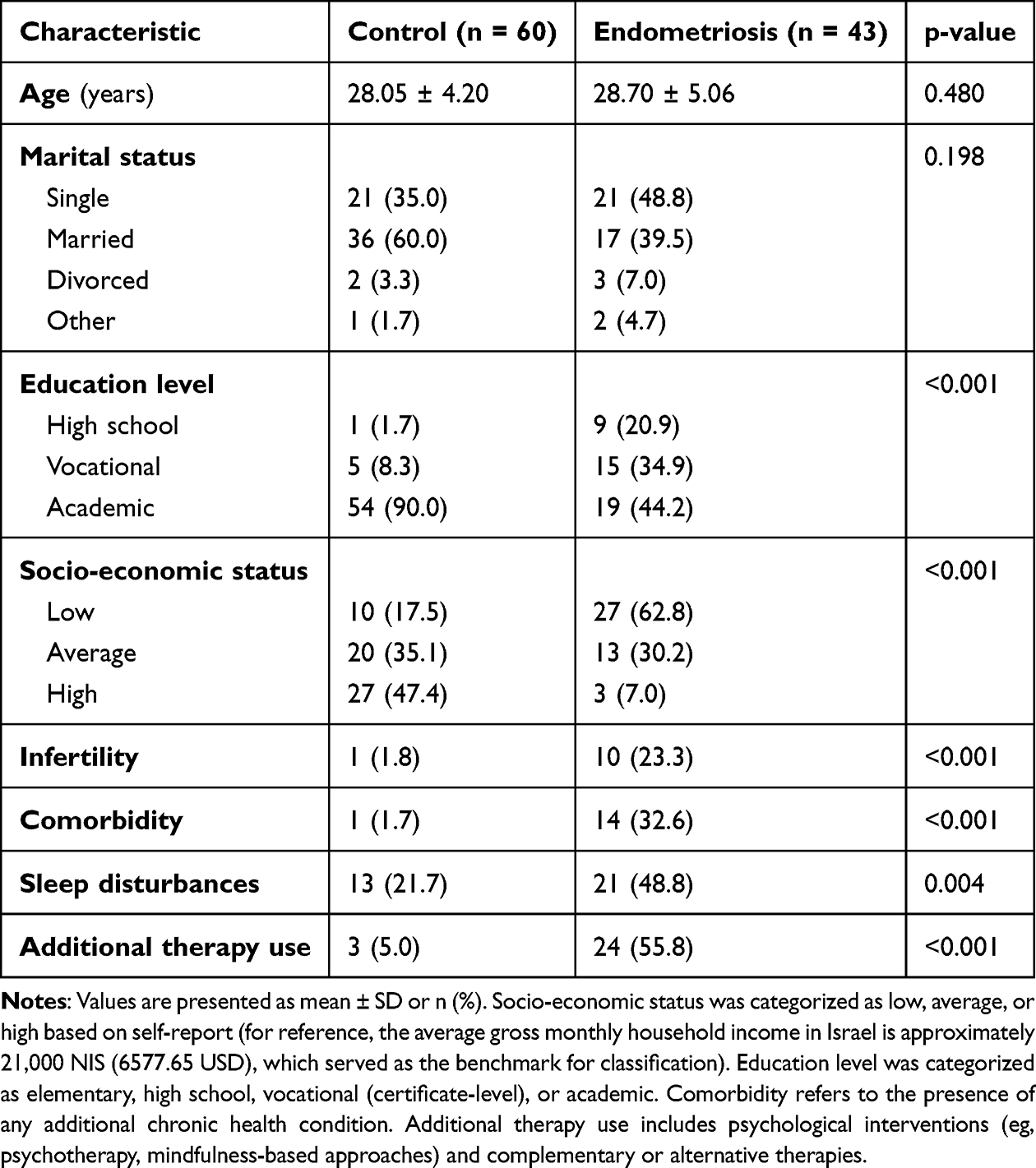 |
Table 1 Socio-Demographic and Health Related Characteristics of the Study Participants |
Procedure
The study was approved by the Institutional Review Board (IRB) of the Faculty of Social Welfare and Health Sciences at the University of Haifa, Israel (IRB approval no. 288/24), and by the Helsinki Committee of Emek Medical Center. All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the institutional and national research committees and with the Declaration of Helsinki and its later amendments. An information page preceding the questionnaire explained the study aims, confidentiality, and the voluntary nature of participation, and stated that completion of the questionnaire constituted informed consent.
After receiving ethical approval, recruitment of the endometriosis group was conducted in collaboration with the clinic’s gynecologists and nursing staff. Following routine medical examinations. Eligibility was determined by the treating gynecologists based on clinical evaluation and medical records prior to invitation to participate. For the control group, eligibility was based on self-report screening questions embedded within the online questionnaire. To minimize potential influence from treating clinicians and ensure independent participation, women who expressed interest received a neutral access code enabling them to complete the questionnaires independently at a later time. Treating physicians and clinic staff were not informed of patients’ participation decisions. The control group was recruited through social media platforms. Interested participants accessed the study via an online link and completed the same questionnaire battery as the endometriosis group. The inclusion of a control group enabled comparison of executive functioning, disease burden, and functional outcomes between women with endometriosis and healthy individuals, consistent with the study’s objectives.
Data were collected anonymously using Google Forms. No identifying information, including Email addresses, was collected or accessible to the researchers. All data were stored in accordance with institutional data protection regulations.
No financial compensation was provided to participants in either group.
Measures
Socio-demographic-health questionnaire assessing age, marital status, education level, income status, medical history, current pharmacological and non-pharmacological treatments, and infertility-related issues.
For measuring disease burden:
- Pain intensity was assessed using Visual Analog Scale (VAS), ranging from 0 (“no pain”) to 10 (“worst imaginable pain”). Participants were asked to rate their pain in two contexts: (1) current pain, referring to the level of pain experienced at the exact moment of completing the questionnaire, and (2) menstrual pain, referring to the typical level of pain experienced during their menstrual period. Higher scores indicate greater pain intensity. VAS has demonstrated good reliability and validity in the assessment of pain across clinical populations, including gynecologic and endometriosis-related pain.42,43
- The Pain Catastrophizing Scale (PCS), a 13-item self-report questionnaire measuring three cognitive–emotional components of pain catastrophizing: rumination, magnification, and helplessness. Items are rated on a 5-point Likert scale ranging from 0 (“not at all”) to 4 (“to a very great extent”), with higher scores indicating greater levels of pain catastrophizing. A total PCS score was calculated by summing all items, and subscale scores for rumination, magnification, and helplessness were computed. The PCS has demonstrated good internal consistency and construct validity in clinical pain populations, including women with gynecologic and chronic pain conditions.9,44
- Emotional distress, including symptoms of depression, anxiety, and stress, was assessed using the Depression Anxiety Stress Scale–21 (DASS-21). Items are rated on a 4-point Likert scale ranging from 0 (“did not apply to me at all”) to 3 (“applied to me very much or most of the time”). Subscale scores were calculated by summing the relevant items for each domain, with higher scores indicating greater emotional distress. In addition, a total DASS-21 score was computed by summing all 21 items to reflect overall emotional distress. The DASS-21 has demonstrated good internal consistency across its subscales, with Cronbach’s alpha coefficients typically exceeding 0.80 in clinical populations and has been shown to be suitable for assessing emotional distress and QoL–related outcomes in women with endometriosis.45–47
Executive functioning was assessed using the Barkley Deficits in Executive Functioning Scale–Short Form (BDEFS-SF), a 20-item validated self-report measure assessing five executive domains: self-management to time, self-organization/problem solving, self-restraint, self-motivation, and emotional self-regulation. Items are rated on a 4-point Likert scale ranging from 1 (“never or rarely”) to 4 (“very often”), reflecting the frequency of executive difficulties. Domain-specific scores were calculated by summing the item scores within each domain, and a total executive function score was calculated by summing all 20 items, with higher scores indicating greater executive dysfunction. The BDEFS-SF has demonstrated good internal consistency and is considered suitable for use in research across diverse populations.39,48,49
Occupational balance was assessed using the Occupational Balance Questionnaire–11 (OBQ-11).27 The questionnaire consists of 11 items rated on a 4-point Likert scale (0 = strongly disagree to 3 = strongly agree). Higher scores indicate better perceived occupational balance, reflecting greater satisfaction with the amount and variety of daily activities, including work, rest, leisure, and sleep.
QoL was assessed using the World Health Organization Quality of Life–BREF (WHOQOL-BREF), a 26-item validated self-report questionnaire assessing four domains: physical health (7 items), psychological wellbeing (6 items), social relationships (3 items), and environment (8 items). Items are rated on a 5-point Likert scale, with higher scores reflecting better perceived QoL. Domain scores were calculated by averaging the relevant items for each domain, and an overall QoL score was computed as the mean of the four domain scores. For interpretability, domain and total scores were transformed to a 0–100 scale, with higher scores indicating better perceived QoL. The WHOQOL-BREF has demonstrated good reliability and validity, including in studies of women with endometriosis.50–52
Statistical Analysis
Statistical analyses were conducted using IBM SPSS Statistics (version 27). Descriptive statistics were calculated for all study variables. Group differences between women with endometriosis and controls were examined using independent-samples t-tests for continuous variables and chi-square tests for categorical variables. Normality assumptions were tested and met. For questionnaire-based measures, T-scores were calculated for total scale scores, where applicable. Group differences in subscale scores were examined using analysis of variance (ANOVA) or multivariate analysis of variance (MANOVA), as appropriate. Pearson correlation coefficients were used to assess associations among continuous variables. To examine the mediating role of executive functions, Hayes’ PROCESS macro (Model 4) was applied. Disease burden variables were entered as independent variables, executive functioning as the mediator, and occupational balance and quality of life as outcome variables. Indirect effects were estimated using bootstrapping with 5000 samples, and mediation was considered statistically significant when the 95% confidence interval did not include zero.
Potential confounding sociodemographic variables, including age, marital status, educational level, socioeconomic status, and comorbid health conditions, were considered in the study design and analysis. Group comparability was examined descriptively, and relevant covariates were controlled for in multivariable and mediation analyses to reduce the risk of confounding. Statistical significance was set at p <0.05. Given that analyses were theory-driven and based on a priori hypotheses, no formal correction for multiple comparisons was applied. Because the online questionnaire required completion of all items before submission, there were no missing data for the primary study variables. Therefore, no imputation procedures were required.
Results
A total of 43 women with clinically confirmed endometriosis and 60 healthy controls completed the questionnaire and were included in the analyses. Because the online survey required completion of all items before submission, all participants who initiated the questionnaire completed it and were included in the final analytic sample. No participants were excluded after eligibility screening.
Participants Characteristics
Socio-demographic, clinical, and health-related characteristics of the study sample are presented in Table 1. Women with endometriosis differed from controls in educational attainment, socioeconomic status, infertility history, use of additional therapies, comorbid conditions affecting daily functioning, and sleep disturbances.
Disease Characteristics
Among women with endometriosis (n = 43), ovarian endometriosis was the most frequently reported phenotype (44.2%), followed by other or unspecified forms (32.6%), deep infiltrating endometriosis (DIE) (18.6%), and superficial endometriosis (4.7%). The mean disease duration was 8.58 ± 5.00 years.
Group differences in pain severity, pain catastrophizing, emotional distress, EFs, occupational balance, and QoL between women with endometriosis and healthy controls are summarized in Table 2.
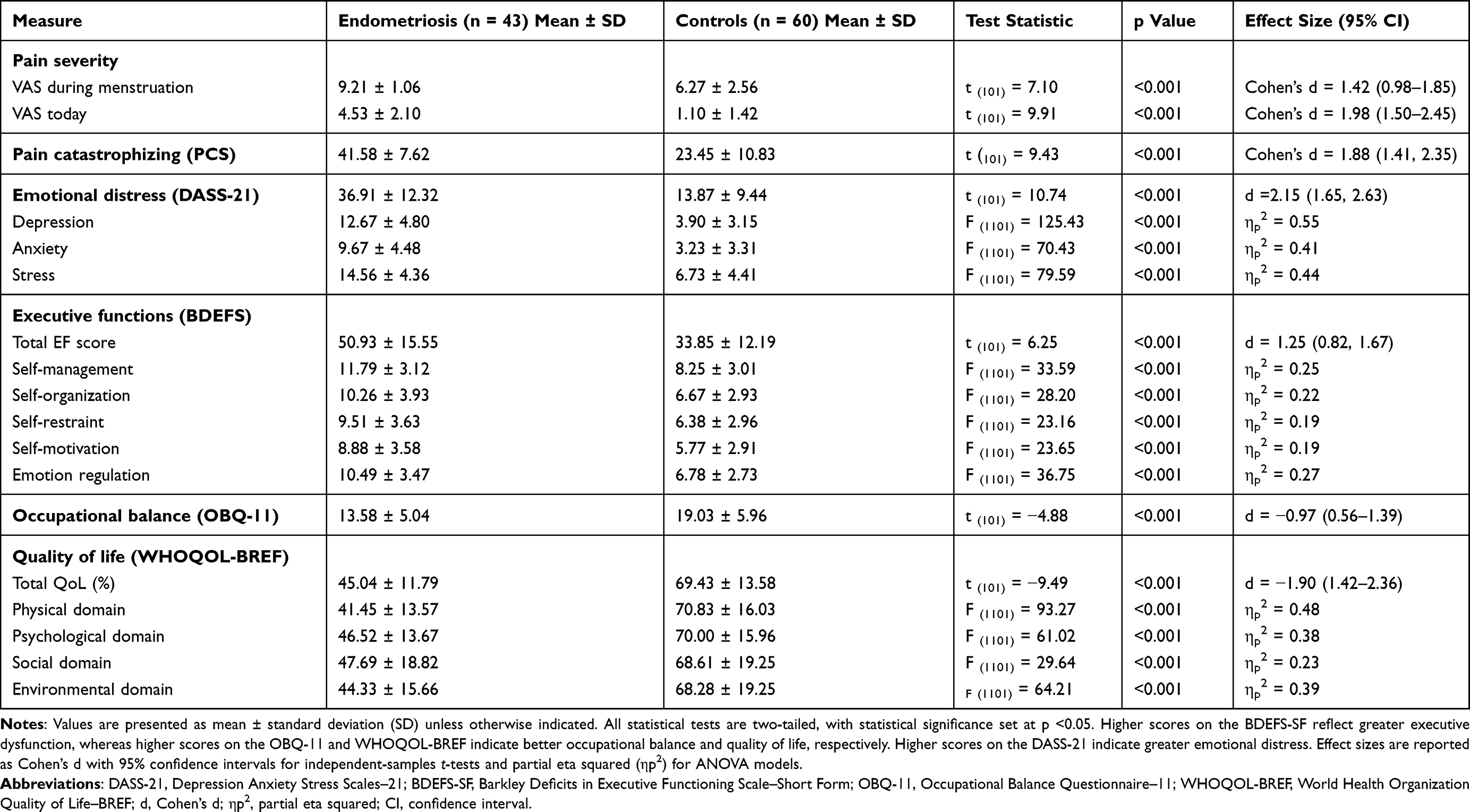 |
Table 2 Group Differences in Disease Burden, Executive Functioning, Occupational Balance, and Quality of Life Between Women with Endometriosis and Controls (Mean ± SD, Effect Sizes) |
Disease Burden
Pain Severity and Pain Catastrophizing
Women with endometriosis reported significantly higher pain severity than control participants, both during menstruation and at the time of assessment (Table 2). In addition, women with endometriosis demonstrated significantly higher levels of pain catastrophizing compared with controls. Group differences were observed across all pain catastrophizing dimensions, including rumination, magnification, and helplessness.
Emotional Distress
Women with endometriosis reported significantly higher overall emotional distress compared with healthy control participants (Table 2). Domain-specific analyses further indicated significantly higher levels of depressive symptoms, anxiety, and stress among women with endometriosis compared with controls.
Overall, women with endometriosis exhibited a substantially higher disease burden than healthy controls, characterized by greater pain severity, increased pain catastrophizing, and elevated emotional distress.
Executive Functions
Executive functioning difficulties were more prevalent among women with Endometriosis compared healthy controls (Table 2). More difficulties in EF were observed across all executive function domains.
Occupational Balance
Occupational balance was significantly lower among women with endometriosis (Table 2). Item-level analyses of the OBQ-11 showed that between-group differences were largest for items assessing the perceived number of activities during a typical week, time available for required and desired activities, satisfaction with the number of activities, and balance across activity domains, as well as satisfaction with time spent resting and recovering (Supplementary Table S1).
QoL
Women with endometriosis reported significantly lower total QoL scores compared with control participants (Table 2). Domain-specific analyses indicated significantly lower scores across all WHOQOL-BREF domains.
To further examine the study objectives regarding relationships between disease burden, EF, and functional outcomes, correlation analyses were conducted within the endometriosis group.
Correlations Between Disease Burden Variables, Executive Functioning, Occupational Balance, and QoL Within the Endometriosis Group
Pain catastrophizing and emotional distress were significantly and positively correlated with worse executive functions. Worse executive functions were significantly correlated with lower occupational balance and lower QoL. Pain catastrophizing and emotional distress were also significantly correlated with QoL. Correlations between pain catastrophizing, emotional distress, and occupational balance did not reach statistical significance (Table 3).
 |
Table 3 Pearson Correlations Among Study Variables in Women with Endometriosis (n = 43) |
EFs as a Mediator Between Pain Catastrophizing and QoL
To test the hypothesized mechanism, mediation analyses were conducted within the endometriosis group to examine whether executive functions mediated the association between pain catastrophizing (PCS total score) and quality of life (WHOQOL-BREF total score). Pain catastrophizing was significantly associated with greater executive dysfunction (B = 1.04, SE = 0.27, p <0.001). In turn, greater executive dysfunction was associated with poorer QoL after controlling for pain catastrophizing (B = −0.59, SE = 0.08, p <0.001). The direct association between pain catastrophizing and QoL was not significant when EFs were included in the model (B = −0.12, SE = 0.16, p =0.48). Bootstrapped mediation analyses revealed a significant indirect effect of pain catastrophizing on QoL through executive dysfunction (indirect effect = −0.61, 95% CI [−0.94, −0.28]), indicating that EFs fully mediated the association between pain catastrophizing and QoL. See Figure 1.
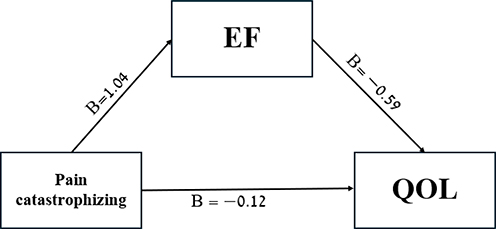 |
Figure 1 Executive functions mediate the association between pain catastrophizing and quality of life in women with endometriosis. Notes: Direct effect: B = −0.12, SE = 0.16, p =0.48. Indirect effect: B = −0.61, 95% CI [−0.94, −0.28]. |
Domain-specific mediation analyses yielded similar patterns across all WHOQOL-BREF domains, with EFs significantly mediating the associations between pain catastrophizing and physical, psychological, social, and environmental QoL (see Supplementary Table S2).
EFs as a Mediator Between Pain Catastrophizing and Occupational Balance
Pain catastrophizing was significantly associated with greater executive dysfunction (B = 1.04, SE = 0.27, p <0.001). In turn, greater executive dysfunction was associated with poorer occupational balance after controlling for pain catastrophizing (B = −0.20, SE = 0.05, p <0.001). The direct association between pain catastrophizing and occupational balance was not significant when EFs were included in the model (B = 0.03, SE = 0.10, p =0.74). Bootstrapped mediation analyses revealed a significant indirect effect of pain catastrophizing on occupational balance through executive dysfunction (indirect effect = −0.21, 95% CI [−0.35, −0.07]), indicating that EFs fully mediated the association between pain catastrophizing and occupational balance. See Figure 2.
 |
Figure 2 Executive functions mediate the association between pain catastrophizing and occupational balance in women with endometriosis. Notes: Direct effect: B = 0.03, SE = 0.10, p =0.74. Indirect effect: B = −0.21, 95% CI [−0.35, −0.07]. |
EFs as a Mediator Between Emotional Distress and QoL
Mediation analyses conducted within the endometriosis group examined whether EFs mediated the association between emotional distress (DASS-21 total score) and QoL (WHOQOL-BREF total score). Higher levels of emotional distress were significantly associated with greater executive dysfunction (B = 0.95, SE = 0.13, p <0.001). In turn, greater executive dysfunction was associated with poorer QoL after controlling for emotional distress (B = −0.63, SE = 0.10, p <0.001). The direct association between emotional distress and QoL was not significant when EFs were included in the model (B = 0.02, SE = 0.13, p =0.87). Bootstrapped mediation analyses revealed a significant indirect effect of emotional distress on QoL through executive dysfunction (indirect effect = −0.60, 95% CI [−0.76, −0.28]), indicating that EFs fully mediated the association between emotional distress and QoL. As shown in Figure 3.
 |
Figure 3 Executive functions mediate the association between emotional distress and quality of life in women with endometriosis. Notes: Direct effect: B = 0.02, SE = 0.13, p =0.87. Indirect effect: B = −0.60, 95% CI [−0.76, −0.28]. |
Additional domain-specific analyses indicated that EFs significantly mediated the associations between psychological distress and social and environmental QoL, whereas mediation was not supported for the physical QoL domain (see Supplementary Table S3).
EFs as a Mediator Between Emotional Distress and Occupational Balance
Mediation analyses conducted within the endometriosis group examined whether EFs mediated the association between emotional distress and occupational balance. Higher levels of emotional distress were significantly associated with greater executive dysfunction (B = 0.95, SE = 0.13, p <0.001). Greater executive dysfunction, in turn, was associated with poorer occupational balance after controlling for emotional distress (B = −0.27, SE = 0.06, p <0.001). The direct association between emotional distress and occupational balance was attenuated and did not reach statistical significance when executive functions were included in the model (B = 0.14, SE = 0.08, p =0.081). Bootstrapped mediation analyses revealed a significant indirect effect of emotional distress on occupational balance through executive dysfunction (indirect effect = −0.26, 95% CI [−0.36, −0.08]), indicating that EFs accounted for the majority of the association between emotional distress and occupational balance. As shown in Figure 4.
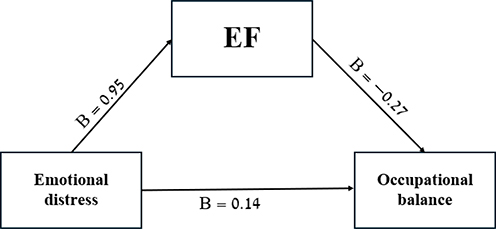 |
Figure 4 Executive functions mediate the association between emotional distress and occupational balance in women with endometriosis. Notes: Direct effect: B = 0.14, SE = 0.08, p =0.081. Indirect effect: B = −0.26, 95% CI [−0.36, −0.08]. |
Discussion
The present study examined the role of EFs in mediating between the burden of endometriosis and women’s daily life, as expressed in their occupational balance and QOL. Consistent with our hypotheses, women with endometriosis demonstrated higher levels of disease burden, including pain severity, pain catastrophizing, and emotional distress, alongside greater executive functioning difficulties, lower occupational balance, and reduced QoL compared with healthy controls. Importantly, EFs emerged as a key mechanism linking pain and psychological aspects of disease burden to functional outcomes. Specifically, EFs fully mediated the associations between pain catastrophizing and both QoL and occupational balance, as well as between emotional distress and these functional outcomes, underscoring the central role of EFs in the lived experience of endometriosis. These findings can be interpreted within a self-regulation framework, whereby persistent psychological burden may tax the cognitive resources required for effective executive control. In the context of endometriosis, elevated pain catastrophizing and emotional distress may interfere with individuals’ ability to regulate attention, plan and organize daily activities, and manage emotional responses to ongoing symptoms. As EF becomes compromised, the capacity to adapt to fluctuating pain, maintain engagement in meaningful activities, and sustain balance across daily roles may be reduced, ultimately contributing to diminished QOL. This perspective provides a functional explanation for how psychological burden is translated into everyday difficulties, highlighting EF as a critical process underlying the lived experience of endometriosis.
The correlation analyses provided important context for the mediation findings, showing that lower EFs scores were consistently associated with poorer QoL and occupational balance, whereas pain catastrophizing and emotional distress demonstrated stronger and more consistent associations with QoL than with occupational balance. This pattern supports the conceptualization of EFs as a central mechanism linking psychological disease burden to daily functioning.29,34,35
Consistent with existing models of executive functioning and self-regulation, the present findings suggest that psychological disease burden in endometriosis may compromise higher-order regulatory processes required for effective daily functioning. Pain catastrophizing and emotional distress were strongly associated with EF difficulties, which in turn were related to poorer QoL and occupational balance. Rather than exerting a direct effect on functioning, psychological burden appears to undermine EFs that play a central role in adaptive coping and everyday functioning in the context of chronic illness.29,37,39,53–59
A particularly novel contribution of the present study is the examination of occupational balance as a functional outcome in endometriosis. Women with endometriosis reported significantly lower occupational balance than controls, and EFs fully mediated the association between psychological disease burden and occupational balance. This is especially important in chronic pain conditions such as endometriosis, where daily functioning is constrained not only by symptoms severity but by the ongoing complexity of symptom unpredictability, emotional burden, and continuous self-management demands.5,53 These findings suggest that disruptions in occupational balance are closely linked to executive capacities required to coordinate daily life under conditions of chronic pain and emotional stress, rather than symptoms severity alone, highlighting EFs as a meaningful and potentially modifiable target for intervention aimed at supporting everyday functioning.53,55–59
From a gynecological and clinical perspective, it should be noted that the prevalence of reported infertility in the endometriosis group (23.3%) was lower than some estimates in the literature, which commonly range between 30% and 50%.60 This finding is likely attributable to the sample’s demographic characteristics, specifically the younger age of participants and high proportion of single women, many of whom had not yet attempted conception.
In the context of endometriosis, daily functioning is shaped by the chronic and unpredictable nature of symptoms, including cyclical pain fluctuations, fatigue, and ongoing treatment demands.2,8 Managing these challenges requires continuous monitoring of bodily signals, anticipatory planning, and repeated adjustment of daily activities, placing sustained cognitive and emotional demands on executive functioning.61,62 Consistent with the pattern of EF difficulties observed in the present study, domains related to organization, time management, emotional regulation, and sustained motivation -those most relevant to daily self-management- appear particularly challenged in the context of chronic pain. Such sustained demands may place strain on executive resources, increasing vulnerability to everyday functional difficulties.29,35,53
From an occupational perspective, occupational balance reflects the capacity to organize and sustain engagement across daily activities under changing internal and external demands.27,28 In endometriosis, symptom cyclicity, fatigue, and treatment-related side effects may disturb daily routines and role participation, placing additional strain on executive resources.2,5,15,22,26–28 The present findings suggest that occupational imbalance in endometriosis reflects not only symptom burden, but also limitations in executive capacities required to regulate, organize, and sustain everyday functioning over time. In this context, occupational balance emerges as a sensitive functional outcome through which the impact of EF difficulties becomes evident in daily life. By positioning occupational balance within an executive functioning framework, the current study extends existing endometriosis research beyond symptom-based models and underscores the importance of higher-order regulatory processes in shaping lived experience.
Beyond the present findings, a substantial body of literature has documented the profound impact of endometriosis on QoL, highlighting persistent pain, emotional distress, and functional limitations as central features of the disease.5,12,31 Previous studies have consistently shown that pain severity and pain-related psychological processes, particularly pain catastrophizing, are strongly associated with poorer QoL, increased emotional distress, and reduced participation in daily activities among women with endometriosis.9,10 Similarly, elevated levels of depression, anxiety, and stress have been repeatedly reported and linked to worse functional and psychosocial outcomes.59,63,64 While these findings underscore the importance of psychological factors in shaping disease impact, most prior research has conceptualized these variables as either parallel correlates or direct predictors of QoL, without examining the underlying mechanisms through which psychological burden translates into impaired daily functioning.
Complementing findings within the endometriosis literature, research in chronic pain and long-term health conditions has increasingly emphasized the role of self-regulatory and executive processes in determining functional adaptation.7,29,34,41 EFs have been shown to influence pain coping, emotional regulation, adherence to treatment recommendations, and sustained engagement in goal-directed activities under conditions of chronic stress.29,35,65 Models of chronic illness adaptation suggest that persistent pain and emotional distress may erode executive control resources, thereby limiting individuals’ capacity to flexibly manage competing demands and maintain functional balance over time.54,66–68 However, despite growing recognition of these processes in broader chronic pain populations, EFs have rarely been examined as a central explanatory mechanism in endometriosis research. By explicitly testing executive functioning as a mediator linking pain catastrophizing and emotional distress to QoL and occupational balance, the present study addresses a critical gap in the literature and extends existing symptom-based models toward a more integrative, mechanism-oriented understanding of daily life disruption in endometriosis.
The present findings carry important implications for the clinical management of endometriosis, suggesting that symptoms severity alone may not fully capture the factors shaping women’s daily functioning and quality of life. Consistent with guidance from the American Society for Reproductive Medicine (ASRM) and the European Society of Human Reproduction and Embryology (ESHRE), which emphasize the chronic and multifaceted nature of endometriosis beyond pain alone,61,69 these results highlight the importance of incorporating functional and self-regulatory processes into comprehensive care. While medical treatment primarily targets pain and gynecological symptoms, women must function in real-life contexts that require planning, organization, emotional regulation, and sustained engagement across daily activities and life roles. EF difficulties may help explain why some women continue to experience substantial functional impairment despite partial pain control and why adherence to treatment recommendations and lifestyle adjustments varies. Together, these findings support a multidisciplinary approach to endometriosis care in which cognitive and psychological functioning are considered alongside gynecological treatment, and in which EFs represent a meaningful and potentially modifiable target for non-pharmacological interventions aimed at improving daily functioning, occupational balance, and QoL.
Several limitations of the present study should be acknowledged. First, the cross-sectional design precludes causal inferences regarding the temporal relationships among disease burden, executive functioning, and functional outcomes. Longitudinal studies are needed to examine how EFs evolve over the course of endometriosis and whether changes in executive functioning prospectively predict variations in occupational balance and QoL. Second, the reliance on self-report measures may introduce reporting bias and shared method variance; future research would benefit from incorporating performance-based assessments of executive functioning and objective indicators of daily functioning. Additionally, the study sample, while clinically relevant, may limit generalizability to broader populations of women with endometriosis, underscoring the need for replication in more diverse and larger samples.
Despite these limitations, the findings point to several important directions for future research and practice. Prospective and intervention studies are warranted to determine whether targeting EFs can enhance functional outcomes beyond symptoms management alone. Integrating executive functioning assessment into clinical evaluation may improve identification of women at greater risk for functional impairment and guide more personalized care. Future research should adopt a multidisciplinary framework that brings together gynecology, psychology, and occupational therapy to examine how cognitive, emotional, and physical factors interact to shape daily life in endometriosis. By incorporating EFs into diagnostic models, research designs, and therapeutic approaches, future work may advance a more comprehensive understanding of endometriosis and support the development of interventions that more effectively address the complex functional challenges experienced by affected women.
In conclusion, this study advances understanding of the functional impact of endometriosis by demonstrating that EFs represent a central pathway through which psychological disease burden shapes daily life. By showing that EFs fully mediated the associations between pain catastrophizing, emotional distress, and both QoL and occupational balance, the present findings move beyond symptom-based models toward a more integrative account of functioning in endometriosis. These results underscore the importance of higher-order self-regulatory processes in both research and clinical care and highlight EFs as a meaningful construct for understanding variability in women’s lived experiences of the disease. Incorporating executive functioning into conceptual frameworks of endometriosis may support more comprehensive, person-centred approaches to assessment and intervention that integrate cognitive, psychological, and functional perspectives, ultimately contributing to improved daily functioning and QoL for affected women.
Capsule
Executive dysfunction mediates the associations between psychological disease burden and reduced quality of life and occupational balance in women with endometriosis, highlighting executive functions as a central mechanism of daily life disruption.
Data Sharing Statement
The subjects in this study were not concomitantly involved in other randomized trials. Data regarding any of the subjects included in this study have not been previously published. The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors gratefully acknowledge the support of the Azrieli Fellows Program.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive specific external funding. Sewar Khatib is supported by a PhD scholarship from the Azrieli Fellows Program. The funding body had no role in the design of the study; collection, analysis, and interpretation of data; or in writing the manuscript.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Saunders PTK, Horne AW. Endometriosis: etiology, pathobiology, and therapeutic prospects. In: Cell. Elsevier B.V.;2021:2807–16. PubMed PMID: 34048704. doi:10.1016/j.cell.2021.04.041
2. Mińko A, Turoń-Skrzypińska A, Rył A, et al. Endometriosis—a multifaceted problem of a modern woman. Int J Environ Res Public Health. 2021;18(15). PubMed PMID: 34360470. doi:10.3390/ijerph18158177
3. Rahmioglu N, Mortlock S, Ghiasi M, et al. The genetic basis of endometriosis and comorbidity with other pain and inflammatory conditions. Nat Genet. 2023;55(3):423–436. PubMed PMID: 36914876. doi:10.1038/s41588-023-01323-z
4. Bulletti C, Coccia ME, Battistoni S, Borini A. Endometriosis and infertility. J Assist Reprod Gen. 2010;27(8):441–447. PubMed PMID: 20574791. doi:10.1007/s10815-010-9436-1
5. Della Corte L, Di Filippo C, Gabrielli O, et al. The Burden of Endometriosis on Women’s Lifespan: A Narrative Overview on Quality of Life and Psychosocial Wellbeing. International Journal of Environmental Research and Public Health. Multidisciplinary Digital Publishing Institute (MDPI); 2020:1–17. PubMed PMID: 32610665. doi:10.3390/ijerph17134683
6. Facchin F, Buggio L, Roncella E, et al. Sleep disturbances, fatigue and psychological health in women with endometriosis: a matched pair case–control study. Reprod Biomed Online. 2021;43(6):1027–1034. doi:10.1016/j.rbmo.2021.08.011
7. Ferdek MA, Oosterman JM, Adamczyk AK, et al. Effective connectivity of beta oscillations in endometriosis-related chronic pain during rest and pain-related mental imagery. J Pain. 2019;20(12):1446–1458. doi:10.1016/j.jpain.2019.05.011
8. Vercellini P, Viganò P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol. 2014;10(5):261–275. PubMed PMID: 24366116. doi:10.1038/nrendo.2013.255
9. Allison M, Mcpeak Bsc E, Allaire C, et al. Pain catastrophizing and pain health-related quality-of-life in endometriosis. Clin J Pain. 2018;34(4):349–356. doi:10.1097/AJP.0000000000000539
10. Sewell M, Churilov L, Mooney S, Ma T, Maher P, Grover SR. Chronic pelvic pain-pain catastrophizing, pelvic pain and quality of life. Scand J Pain. 2018;18(3):441–448. PubMed PMID: 29794266. doi:10.1515/sjpain-2017-0181
11. Facchin F, Barbara G, Dridi D, et al. Mental health in women with endometriosis: searching for predictors of psychological distress. Hum Reprod. 2017;32(9):1855–1861. doi:10.1093/humrep/dex249
12. Facchin F, Barbara G, Saita E, et al. Impact of endometriosis on quality of life and mental health: pelvic pain makes the difference. J Psychosomatic Obstet Gynecol. 2015;36(4):135–141. doi:10.3109/0167482X.2015.1074173
13. Husby GK, Haugen RS, Moen MH. Diagnostic delay in women with pain and endometriosis. Acta Obstet Gynecol Scand. 2003;82(7):649–653. PubMed PMID: 12790847. doi:10.1034/j.1600-0412.2003.00168.x
14. Maulitz L, Stickeler E, Stickel S, Habel U, Tchaikovski SN, Chechko N. Endometriosis, psychiatric comorbidities and neuroimaging: estimating the odds of an endometriosis brain. In: Frontiers in Neuroendocrinology. Academic Press Inc.; 2022. PubMed PMID: 35202605. doi:10.1016/j.yfrne.2022.100988
15. Carbone MG, Campo G, Papaleo E, Marazziti D, Maremmani I. The importance of a multi-disciplinary approach to the endometriotic patients: the relationship between endometriosis and psychic vulnerability. J Clin Med. 2021;10(8):1616. doi:10.3390/jcm10081616
16. Leuenberger J, Kohl Schwartz AS, Geraedts K, et al. Living with endometriosis: comorbid pain disorders, characteristics of pain and relevance for daily life. Eur J Pain. 2022;26(5):1021–1038. doi:10.1002/ejp.1926
17. Bień A, Rzońca E, Zarajczyk M, Wilkosz K, Wdowiak A, Iwanowicz-Palus G. Quality of life in women with endometriosis: a cross-sectional survey. Qual Life Res. 2020;29(10):2669–2677. PubMed PMID: 32356276. doi:10.1007/s11136-020-02515-4
18. Lozano-Lozano M, Mundo-López A, San-Sebastian AP, et al. Limitations in activities of daily living among spanish women diagnosed with endometriosis. Am J Occup Ther. 2021;75(6). PubMed PMID: 34842913. doi:10.5014/ajot.2021.044974
19. Hållstam A, Stålnacke BM, Svensén C, Löfgren M. Living with painful endometriosis – a struggle for coherence. A qualitative study. Sex Reproduct Healthcare. 2018;17:97–102. PubMed PMID: 30193728. doi:10.1016/j.srhc.2018.06.002
20. Di Donato N, Montanari G, Benfenati A, et al. Do women with endometriosis have to worry about sex? Eur J Obstetrics Gynecol Reprod Biol. 2014;179:69–74. PubMed PMID: 24965983. doi:10.1016/j.ejogrb.2014.05.022
21. Sachs MK, Dedes I, El-Hadad S, et al. Physical activity in women with endometriosis: less or more compared with a healthy control? Int J Environ Res Public Health. 2023;20(17). PubMed PMID: 37681799. doi:10.3390/ijerph20176659
22. Mundo-López A, Ocón-Hernández O, Lozano-Lozano M, et al. Impact of symptom burden on work performance status in Spanish women diagnosed with endometriosis. Eur J Obstetrics Gynecol Reprod Biol. 2021;261:92–97. PubMed PMID: 33906026. doi:10.1016/j.ejogrb.2021.04.008
23. McDougall J, Wright V, Rosenbaum P. The ICF model of functioning and disability: incorporating quality of life and human development. Dev Neurorehabil. 2010:204–211. PubMed PMID: 20450470. doi:10.3109/17518421003620525
24. Allan CM, Campbell WN, Guptill CA, Stephenson FF, Campbell KE. A conceptual model for interprofessional education: the International Classification of Functioning, Disability and Health (ICF). J Interprof Care. 2006;20(3):235–245. PubMed PMID: 16777791. doi:10.1080/13561820600718139
25. van der Veen S, Evans N, Huisman M, Welch Saleeby P, Widdershoven G. Toward a paradigm shift in healthcare: using the International Classification of Functioning, Disability and Health (ICF) and the capability approach (CA) jointly in theory and practice. Disabil Rehabil. 2023;45(14):2382–2389. PubMed PMID: 35732595. doi:10.1080/09638288.2022.2089737
26. Boop C, Cahill SM, Davis C, et al. Occupational therapy practice framework: domain and process fourth edition. In: American Journal of Occupational Therapy. American Occupational Therapy Association, Inc; 2020:1–87. PubMed PMID: 34780625. doi:10.5014/ajot.2020.74S2001
27. Wagman P, Håkansson C. Introducing the Occupational Balance Questionnaire (OBQ). Scand J Occup Ther. 2014;21(3):227–231. PubMed PMID: 24649971. doi:10.3109/11038128.2014.900571
28. Wagman P, Håkansson C, Jonsson H. Occupational balance: a scoping review of current research and identified knowledge gaps. J Occup Sci. 2015;22(2):160–169. doi:10.1080/14427591.2014.986512
29. Hocking MC, Barnes M, Shaw C, Lochman JE, Madan-Swain A, Saeed S. Executive function and attention regulation as predictors of coping success in youth with functional abdominal pain. J Pediatr Psychol. 2011;36(1):64–73. PubMed PMID: 20592102. doi:10.1093/jpepsy/jsq056
30. Márki G, Vásárhelyi D, Rigó A, Kaló Z, Ács N, Bokor A. Challenges of and possible solutions for living with endometriosis: a qualitative study. BMC Womens Health. 2022;22(1). PubMed PMID: 35081940. doi:10.1186/s12905-022-01603-6
31. Wu YH, Lu YY, Liu KF. Factors influencing health-related quality of life in women with endometriosis: a cross-sectional study. Nurs Health Sci. 2024;26(1). PubMed PMID: 38374495. doi:10.1111/nhs.13100
32. Donald T, Stuss RTK. Principles of Frontal Lobe Function.
33. Miller EK, Cohen JD. An integrative theory of prefrontal cortex function [Internet]. Vol. 42; 2026. Available from: www.annualreviews.org.
34. Berryman C, Stanton TR, Bowering KJ, Tabor A, McFarlane A, Moseley GL. Do people with chronic pain have impaired executive function? A meta-analytical review. In: Clinical Psychology Review. Elsevier Inc.;2014:563–579. PubMed PMID: 25265056. doi:10.1016/j.cpr.2014.08.003
35. Barkley RA. Executive Functions: What They Are, How They Work, and Why They Evolved. Guilford Press; 2012:1–244.
36. Horn M, Sherman KA, Pehlivan MJ, Basson M, Lin Z, Duckworth TJ. Perceived cognitive functioning difficulties in individuals living with endometriosis. J Health Psychol. 2025. doi:10.1177/13591053251331826
37. Berryman A, MacHado L. Cognitive Functioning in Females with Endometriosis-Associated Chronic Pelvic Pain: A Literature Review. Archives of Clinical Neuropsychology. Oxford University Press; 2025:1066–1080.PubMed PMID: 39826909. doi:10.1093/arclin/acaf003
38. Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: a theoretically based approach. J Person Soc Psychol. 1989;56(2):267.
39. Barkley RA. The assessment of executive functioning using the Barkley Deficits in Executive Functioning Scales. In: Handbook of Executive Functioning. New York: Springer New York;2014:245–263. doi:10.1007/978-1-4614-8106-5_15
40. Baliki MN, Petre B, Torbey S, et al. Corticostriatal functional connectivity predicts transition to chronic back pain. Nat Neurosci. 2012;15(8):1117–1119. PubMed PMID: 22751038. doi:10.1038/nn.3153
41. Apkarian AV, Bushnell MC, Treede RD, Zubieta JK. Human brain mechanisms of pain perception and regulation in health and disease. Eur J Pain. 2005;9(4):463. PubMed PMID: 15979027. doi:10.1016/j.ejpain.2004.11.001
42. Hjermstad MJ, Fayers PM, Haugen DF, et al. Studies comparing numerical rating scales, verbal rating scales, and visual analogue scales for assessment of pain intensity in adults: a systematic literature review. J Pain Sympt Manage. 2011:1073–1093. PubMed PMID: 21621130. doi:10.1016/j.jpainsymman.2010.08.016
43. Wickström K, Edelstam G. Minimal clinically important difference for pain on the VAS scale and the relation to quality of life in women with endometriosis. Sex Reproduct Healthcare. 2017;13:35–40. PubMed PMID: 28844356. doi:10.1016/j.srhc.2017.05.004
44. Osman A, Barrios FX, Kopper BA, Hauptmann W, Jones J, O’neill E. Factor structure, reliability, and validity of the pain catastrophizing scale. J Behav Med. 1997;20(6):589–605.
45. Osman A, Wong JL, Bagge CL, Freedenthal S, Gutierrez PM, Lozano G. The Depression Anxiety Stress Scales-21 (DASS-21): further examination of dimensions, scale reliability, and correlates. J Clin Psychol. 2012;68(12):1322–1338. PubMed PMID: 22930477. doi:10.1002/jclp.21908
46. Coker AO, Coker OO, Sanni D. Psychometric properties of the 21-item Depression Anxiety Stress Scale (DASS-21). Afr Res Rev. 2018;12(2):135. doi:10.4314/afrrev.v12i2.13
47. Henry JD, Crawford JR. The short-form version of the Depression anxiety stress scales (DASS-21): construct validity and normative data in a large non-clinical sample. Br J Clin Psychol. 2005;44(2):227–239. PubMed PMID: 16004657. doi:10.1348/014466505X29657
48. Clauss K, Witte TK, Bardeen JR. Examining the factor structure and incremental validity of the Barkley Deficits in Executive Functioning Scale–short form in a community sample. J Pers Assess. 2021;103(6):777–785. doi:10.1080/00223891.2021.1887879
49. Kamradt JM, Nikolas MA, Burns GL, et al. Barkley Deficits in Executive Functioning Scale (BDEFS): validation in a large multisite college sample. Assessment. 2021;28(3):964–976. doi:10.1177/1073191119869823
50. Skevington SM, Lotfy M, O’connell KA. The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial A Report from the WHOQOL Group q. Qual Life Res. 2004;13(2):299–310.
51. Harper A, Power M. Development of the World Health Organization WHOQOL-Bref quality of life assessment. Psychological Medicine [Internet]. Cambridge University Press; 1998. Available from: https://research.tilburguniversity.edu/en/publications/5df369ff-ff7f-4bac-.
52. Hawthorne G, Herrman H, Murphy B. Interpreting the WHOQOL-Brèf: preliminary population norms and effect sizes. Soc Indic Res. 2006;77(1):37–59. doi:10.1007/s11205-005-5552-1
53. Leventhal H, Phillips LA, Burns E. The Common-Sense Model of Self-Regulation (CSM): a dynamic framework for understanding illness self-management. J Behav Med. 2016;39(6):935–946. PubMed PMID: 27515801. doi:10.1007/s10865-016-9782-2
54. Cameron LD, Leventhal H.The Self-Regulation of Health and Illness Behaviour. In: Cameron L, Leventhal H, editors.
55. Berryman C, Stanton TR, Jane Bowering K, Tabor A, McFarlane A, Lorimer Moseley G. Evidence for working memory deficits in chronic pain: a systematic review and meta-analysis. Pain. 2013;154(8):1181–1196. doi:10.1016/j.pain.2013.03.002
56. Eccleston C, Crombez G. Pain demands attention: a cognitive-affective model of the interruptive function of pain. Psychol Bull. 1999;125(3):356.
57. Snyder HR, Miyake A, Hankin BL. Advancing understanding of executive function impairments and psychopathology: bridging the gap between clinical and cognitive approaches. Front Psychol. 2015;6. PubMed PMID: 25859234. doi:10.3389/fpsyg.2015.00328
58. Katz J, Rosenbloom BN, Fashler S. Chronic Pain, psychopathology, and dsm-5 somatic symptom disorder. CanJPsychiatry [Internet]; 2015. Available from: www.TheCJP.ca.
59. Joormann J, Michael Vanderlind W. Emotion regulation in depression: the role of biased cognition and reduced cognitive control. Clin Psychol Sci. 2014;2(4):402–421. doi:10.1177/2167702614536163
60. U LRM, Chiappa V, Ceccaroni M, et al. Epidemiology of infertility in women with endometriosis. In: Best Practice and Research: Clinical Obstetrics and Gynaecology. Bailliere Tindall Ltd; 2024. PubMed PMID: 38183767. doi:10.1016/j.bpobgyn.2023.102454
61. Becker CM, Bokor A, Heikinheimo O, et al. ESHRE guideline: endometriosis. Hum Reprod Open. 2022;2022(2). doi:10.1093/hropen/hoac009
62. Stratton P, Berkley KJ. Chronic pelvic pain and endometriosis: translational evidence of the relationship and implications. Hum Reprod Update. 2011;17(3):327–346. PubMed PMID: 21106492. doi:10.1093/humupd/dmq050
63. Van Barneveld E, Manders J, Van Osch FHM, et al. Depression, anxiety, and correlating factors in endometriosis: a systematic review and meta-analysis. In: Journal of Women’s Health. Mary Ann Liebert Inc.; 2022:219–230. PubMed PMID: 34077695. doi:10.1089/jwh.2021.0021
64. Laganà AS, La Rosa VL, Rapisarda AMC, et al. Anxiety and depression in patients with endometriosis: impact and management challenges. Int J Womens Health. 2017;9:323–330. doi:10.2147/IJWH.S119729
65. McCracken LM, Vowles KE. Acceptance and commitment therapy and mindfulness for chronic pain: model, process, and progress. Am Psychologist. 2014;69(2):178–187. PubMed PMID: 24547803. doi:10.1037/a0035623
66. Karoly P, Ruehlman LS. Psychological “resilience” and its correlates in chronic pain: findings from a national community sample. Pain. 2006;123(1–2):90–97. PubMed PMID: 16563626. doi:10.1016/j.pain.2006.02.014
67. McEwen BS, Morrison JH. The brain on stress: vulnerability and plasticity of the prefrontal cortex over the life course. Neuron. 2013:16–29. PubMed PMID: 23849196. doi:10.1016/j.neuron.2013.06.028
68. Juster RP, McEwen BS, Lupien SJ. Allostatic load biomarkers of chronic stress and impact on health and cognition. Neurosci Biobehav Rev. 2010:2–16. PubMed PMID: 19822172. doi:10.1016/j.neubiorev.2009.10.002
69. Practice Committee of the American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis: a committee opinion. Fertil Steril. 2014;101(4):927–935. PubMed PMID: 24630080. doi:10.1016/j.fertnstert.2014.02.012
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Effectiveness of Non-Pharmacological Interventions for Pain and Quality of Life in Women with Endometriosis: A Systematic Review and Network Meta-Analysis
Zheng X, Wang Y, Li H, Zhang J, Liu J, Zheng X, Zhang J, Fan G, Sun Y, Li B, Jiao J, Zuo G, Fan X, She Y
Journal of Pain Research 2026, 19:577080
Published Date: 20 February 2026