Back to Journals » Psychology Research and Behavior Management » Volume 18
Discussion on the Application of Mindfulness Therapy in the Treatment of Diabetic Peripheral Neuropathy: A Narrative Review
Authors Fan Q, Yu S, Sun X, Dong Y, Chen Y, Jia L ![]()
Received 8 April 2025
Accepted for publication 29 July 2025
Published 12 August 2025 Volume 2025:18 Pages 1729—1747
DOI https://doi.org/10.2147/PRBM.S533200
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Qing Fan,1 Shuang Yu,1 Xu Sun,2 Yao Dong,3 Yao Chen,4 Lihong Jia1
1Department of Nursing, First Affiliated Hospital of Dalian Medical University, Dalian, People’s Republic of China; 2Department of Ophthalmology, The Third People’s Hospital of Dalian, Dalian, People’s Republic of China; 3Department of Obstetric, Affiliated Central Hospital of Dalian University of Technology, Dalian, People’s Republic of China; 4Department of Coronary Heart Disease, Affiliated Central Hospital of Dalian University of Technology, Dalian, People’s Republic of China
Correspondence: Lihong Jia, Email [email protected]
Abstract: Diabetic peripheral neuropathy (DPN) is one of the most common chronic complications of diabetes. It has a slow and insidious onset, mainly manifested as sensory and motor dysfunction, and increases susceptibility to psychological problems such as anxiety and depression, seriously affecting the quality of life of patients. The current treatment strategies focus on effective metabolic management and lifestyle intervention, but the results are not satisfactory. Mindfulness therapy (MBT), as a non-pharmaceutical intervention method, has gradually shown potential value in the treatment of DPN. This review incorporates studies on the two in recent years, revealing the main mechanism by which MBT affects neuropsychology. It explores the feasibility and application status of MBT in reshaping the cognitive experience of pain in patients with DPN, alleviating pain perception, improving psychological states such as anxiety and depression, and thereby enhancing the overall quality of life. In conclusion, our research provides more powerful evidence for the clinical treatment of patients with DPN by applying MBT.
Keywords: diabetic peripheral neuropathy, mindfulness-based therapy, pain management, quality of life
Introduction
Over the past thirty years, the prevalence of diabetes worldwide has significantly continued to rise, with the number of adult diabetes patients increasing to 828 million in 2022, of which approximately 148 million are in China, accounting for about 18% of the global total.1 The incidence of diabetes-related complications that follow is showing a synchronized growth trend.2 The morbidity rate of complications and comorbidities among Chinese patients with type 2 diabetes mellitus (T2DM) is at a high level, with diabetic peripheral neuropathy (DPN) being the most common chronic complication of diabetes. Epidemiological surveys show that the combined prevalence ranges from 16% to as high as 66%, highlighting its widespread occurrence,3 it is also a significant inducement of diabetic foot ulcers and disabling neuropathic pain, and in severe cases, it can lead to lower limb amputation or even death.4 DPN is related to various factors, including metabolic disorders such as the sorbitol pathway, hexosamine pathway, non-enzymatic glycosylation, and the formation of advanced glycation end products, as well as ischemia and hypoxia, mitochondrial dysfunction and damage, and oxidative stress injury. This is accompanied by the involvement of various complex factors such as metabolic inflammation, autoimmune factors, neuroregeneration disorders, and vitamin nutritional disorders, while also being influenced by the interactions of disease duration, blood sugar, body weight, and insulin resistance, collectively driving the occurrence and development of DPN, with the most common manifestations being sensory abnormalities or pain in the distal extremities.5 Current treatments for DPN have their limitations, and long-term pain and dysfunction may lead to psychological problems such as anxiety and depression, as well as seriously affecting patients’ quality of life and increasing the economic burden on patients and society.6
Mindfulness originated from the Theravada Buddhist tradition 2500 years ago and was introduced to the fields of psychotherapy and medicine in the early 1980s.7 The core idea of mindfulness, a type of awareness that leads to liberation by observing changes in the body and mind in the present moment, lies in the simple observation and complete acceptance of feelings. Its core idea focuses on immersion in the present moment, alertness, acceptance of the situation, and mental concentration.8 Mindfulness, as a psychological intervention method, is widely used in many disciplines such as psychology, psychiatry, education clinical medicine, etc. Studies have shown that mindfulness can effectively enhance individuals’ self-awareness and emotion management ability, and improve mental health;9 Particularly noteworthy is the significant efficacy in chronic pain management, cardiovascular disease prevention, cancer rehabilitation, etc, to alleviate pain and physical and mental burden of patients.10
There is relatively little literature on the relationship between mindfulness and DPN. For humans, we still cannot draw a complete conclusion. We retrieved and collected the articles on mindfulness and the application of mindfulness therapy in DPN published in the past six years through the PubMed database. We reviewed the definition of mindfulness, its development overview, the specific role of mindfulness in neuropsychology, as well as the specific mechanism and practical application of mindfulness therapy in the treatment of DPN patients. In conclusion, this study reveals the research progress of mindfulness and mindfulness therapy in DPN, providing a scientific reference for the application of mindfulness therapy in the clinical intervention of DPN patients.
Historical Evolution and Development of Mindfulness Therapy
Development and Definition of Mindfulness
Since the 1970s, the scientific research on meditation has gradually deepened. Early studies such as Herbert Benson’s “relaxation response” revealed its potential to assist in lowering blood pressure by regulating physiological mechanisms.11 Subsequently, Ainslie Meares proposed that deep relaxation might enhance the immune function to alleviate the symptoms of cancer patients.12 Rafazov Marciniak further confirmed the optimization effect of meditation on brain structure and the improvement effect on cognition.13
Based on previous research on meditation, Jon Kabat-Zinn, one of the pioneers of modern mindfulness, defined mindfulness in the early 1980s as “awareness of the present moment and acceptance of it without judgment” and emphasized that mindfulness is not just a meditation technique, but an attitude toward life that focuses on the present experience.14–17 Ultimately, a complete therapy system covering four major branches, namely Mindfulness-based Cognitive Therapy (MBCT),18 Dialectical Behavior Therapy (DBT),19 Mindfulness-based Stress Reduction Therapy (MBSR),20 and Acceptance and Commitment Therapy (ACT),21 was formed and widely applied in fields such as depression prevention, personality disorder intervention, stress relief, and mental illness treatment. The development process and definition of positive thinking meditation are shown in Figure 1.
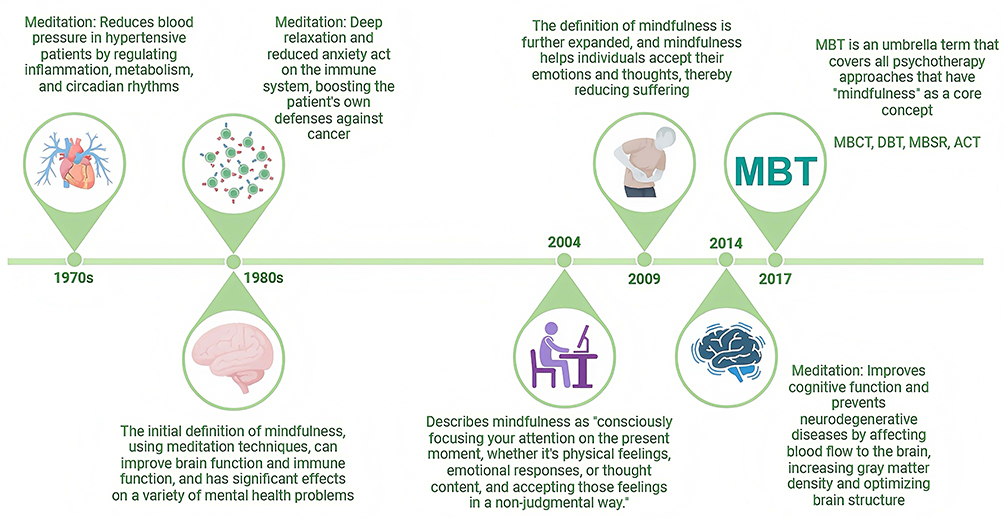 |
Figure 1 Historical Development of Mindfulness and Its Definition. |
Multiple Mechanisms of Mindfulness Therapy
Mindfulness therapy impacts neurological disorders and the management of chronic diseases by affecting multiple regions and networks of the brain in synergy with each other at four levels: neurological, physiological, psychological, and cellular, the following mechanistic components and the mechanistic diagrams are shown in Figure 2.
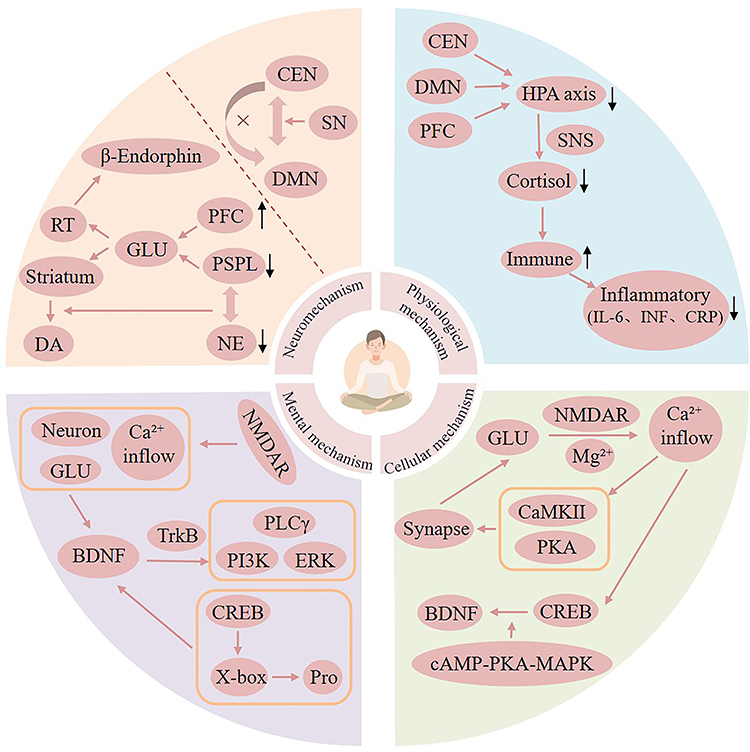 |
Figure 2 Neurological, Physiological, Psychological and Cellular Mechanisms of Mindfulness. The black upward arrow represents “up-regulation”, the black downward arrow represents “down-regulation”, and the Orange arrow represents biological processes. |
The Neuromechanism of Mindfulness (NM) Involves Three Main Network Patterns and Associated Neurotransmitters
The default mode network (DMN) is a series of regions in the parietal, frontal, and temporal lobes.22 Active in the resting state, it is thought to be related to the ability to visualize past and future events, scene construction and situational processing, language, social and emotional processing, and is associated with self-referential thinking (eg, rumination, worrying, daydreaming), Mind Wandering, and emotional introspection, and has a very complex diversity. Overactive DMN may lead to anxiety, depression, and ruminative thinking. The Central Executive Network (CEN) core brain areas include the prefrontal cortex and parietal lobe, which are involved in higher cognitive functions such as attention control, working memory, and goal-directed behavior. Key nodes of the Salience Network (SN) include the anterior insula and anterior cingulate cortex, which are responsible for detecting important stimuli (eg, emotional signals, pain) in the internal and external environments, enhancing the awareness and processing of emotional and bodily signals, and coordinating the switching between the DMN and the CEN. Bremer et al conducted an Independent component analysis and sliding time window on adults who had not received meditation after completing 31 days of mindfulness meditation training. And seed-based correlation analyses were conducted to evaluate the training-related changes in functional connections within and between networks related to mindfulness meditation.23 Their research indicated that positive thinking dynamically regulates the three network patterns by reshaping the functional connections and activity patterns of DMN, CEN, and SN to achieve cognitive and emotional balance. SN acts as a “switch” to balance DMN and CEN, and after detecting and recognizing important information, it helps individuals to choose whether to activate CEN (to focus on a task) or inhibit DMN (to reduce self-referential thinking). After detecting and recognizing important information, it helps individuals to choose whether to activate CEN (focusing on processing tasks) or inhibit DMN (reducing self-referential thinking), and the inhibition of DMN by CEN is enhanced, which reduces mental wandering; at the same time, the connection between DMN and SN is adjusted, which promotes the neutral observation of emotions rather than judgment; long-term mindfulness practice alters the connectivity strength of the three networks and the structure of the grey matter, which results in a more efficient cognitive-emotional regulation model.
The prefrontal cortex (PFC), an area involved in attention and intention, was activated during meditation.24 PFC stimulates the reticular nucleus of the thalamus (RT) via the excitatory neurotransmitter glutamate (GLU).25 At the same time, the arcuate nucleus of the medial hypothalamus is activated, increasing the production of beta-endorphins, which reduce pain and promote feelings of pleasure.26 In addition, PFC activation stimulates dopamine (DA) release in the striatum via glutamatergic synapses, contributing to relaxation, reduction of emotional responses, and withdrawal from external stimuli during meditation.27
In an extremely meditative state, the thalamus releases the inhibitory neurotransmitter gamma-aminobutyric acid (GABA) into the posterior lateral nucleus,28 this inactivates the posterior superior parietal lobe (PSPL), increasing attentional capacity and leads to diminished self-awareness or spatial boundaries. Furthermore, the inactivation of PSPL stimulates the hippocampus and amygdala via glutamate signaling,29 stimulating the parasympathetic nervous system, and causing a decrease in heart rate and blood pressure.30 Parasympathetic activation also reduces the production and distribution of norepinephrine (NE).31 Reduced NE levels further promote PSPL inactivation,32 creating a cycle, this process is likewise accompanied by lower adrenocorticotropic hormone (ACTH) levels and higher serotonin levels. Elevated serotonin will modulate the dopaminergic system and support sustained concentration during meditation.33 Notably, during meditation, the pineal gland will also be activated, increasing melatonin production and helping to relieve pain.34
Physiological Mechanism of Mindfulness
Physiological mechanisms involve stress response systems and immune and inflammatory regulation. The hypothalamic-pituitary-adrenal axis (HPA axis) and its cascade of effects are activated by organisms in the face of physiologically or psychologically stressful stimuli. This process involves the participation of corticotropin-releasing hormone (CRH), adrenocorticotropic hormone (ACTH), and cortisol (COR), respectively, and ultimately triggers the sympathetic nervous system Excitation.35 Long-term overactivation of the HPA axis may lead to health problems such as anxiety, depression, metabolic disorders, and immune dysfunction.36 Mindfulness meditation may reduce stress-induced amygdala hyperactivation by facilitating functional adjustments in the executive control of CEN and DMN, thereby decreasing the secretion of CRH, ACTH, and cortisol, slowing down the inflammatory response triggered by prolonged stress, and ameliorating chronic stress.37 Mindfulness meditation also enhances negative feedback regulation of the HPA axis by increasing the activity of the PFC, restoring homeostasis, and avoiding chronic overactivation, for instance, Wang et al conducted a multicenter randomized controlled trial and discovered the effectiveness of mindfulness training in alleviating the psychological stress of pregnant women and improving the physiological stress response function of the HPA axis.38 Down-regulated cortisol will also activate the parasympathetic nervous system, which controls the body’s immune response.39
Gamaiunova et al evaluated the effects of two mindfulness intervention methods on different stages of stress responses in different physiological systems based on a randomized controlled trial, and they found that mindfulness meditation also regulates the activity of the autonomic nervous system by activating the parasympathetic nervous system (PNS) and promoting cortisol secretion, thereby controlling the body’s immune response.40 Specifically, mindfulness meditation activates the interferon signaling system, which triggers a complex regulatory system of innate and adaptive immune responses to defend against pathogens and disease,41 reduces pro-inflammatory factors such as interleukin 6, and slows the inflammatory response associated with chronic disease. Mindfulness also reduces basal inflammation levels (eg C-reactive protein),42 but retains its acute immune response capacity.43 In addition, mindfulness affects specific immune pathways, such as the vagus nerve-mediated cholinergic anti-inflammatory pathway),43 this ultimately leads to a milder immune response and low levels of inflammatory cytokines.
Mental Mechanism of Mindfulness
Nakamura constructed a functional brain model based on dissecting the network structure of the brain and analyzing the way information is transmitted between various regions. By simulating the changes in activity in each region, it examined the impact of mindfulness meditation on information transmission in the brain. They found that mindfulness mainly through cognitive and emotional regulation, including decentering to reduce identification with negative emotions, reducing rumination, and accepting current emotions in a non-judgmental and non-confrontational way, thus enhancing emotional awareness and acceptance, and improving psychological resilience.44 As an important neurotrophic factor, BDNF has a significant effect on cognitive function and emotion regulation, and its high level is associated with strong learning ability, good memory, emotional stability, and a high sense of well-being, whereas a low level tends to lead to low mood and even depression. Mindfulness therapy promotes BDNF (brain-derived neurotrophic factor) synthesis through NMDA receptor (NMDAR) induced neuronal activation, glutamate release, and Ca²⁺ in-flow.45 At the same time, pathways involving CAMP Response Element Binding protein (CREB) and X-box binding protein will further enhance BDNF levels.46 The binding of BDNF to take on the postsynaptic membrane further activates downstream signaling cascades, including phospholipase-Cγ (PLCγ), phosphatidylinositol 3-kinase (PI3K), and the ERK pathway to improve cognitive functioning and emotional state.47 Therefore, the mindfulness mental mechanism not only directly enhances mental health but also forms a virtuous cycle by promoting BDNF synthesis and signaling, further enhancing cognitive function and emotion regulation.
Cellular Mechanisms of Mindfulness
NMDA receptor activation leads to calcium inward flow, which in turn activates kinases such as calcium calmodulin-dependent kinase II (CaMKII) and protein kinase A (PKA) to promote synaptic transmission.48 Tang et al conducted a randomized controlled trial, providing comprehensive physical and mental training to healthy college students who had no previous meditation experience or mental illness. Subsequently, behavioral measurements and proton magnetic resonance spectroscopy data collection were carried out, and it was found that mindfulness training prompts the release of glutamate from presynaptic neurons by enhancing synaptic activity.49 Glutamate binding to NMDAR unblocks the channel by magnesium ions (Mg²⁺), leading to calcium ion (Ca²⁺) inward flow.50 Ca²⁺ signaling activates the transcription factor cAMP-responsive element-binding protein (CREB) through the cAMP-PKA-MAPK pathway to promote the expression of synaptic plasticity-related genes, such as brain-derived neurotrophic factor (BDNF), to consolidate long-term memory and synaptic remodeling. Derived neurotrophic factor (BDNF), which promotes the expression of genes related to synaptic plasticity, such as brain-derived neurotrophic factor (BDNF), consolidates long-term memory and synaptic remodeling.51
Intervention Model of Mindfulness Therapy
The main modes of intervention in mindfulness therapy include individual interventions, group interventions, and integrative modes of intervention that incorporate other therapies. We have summarized the characteristics of individual intervention, group intervention and comprehensive intervention models of mindfulness (Table 1).
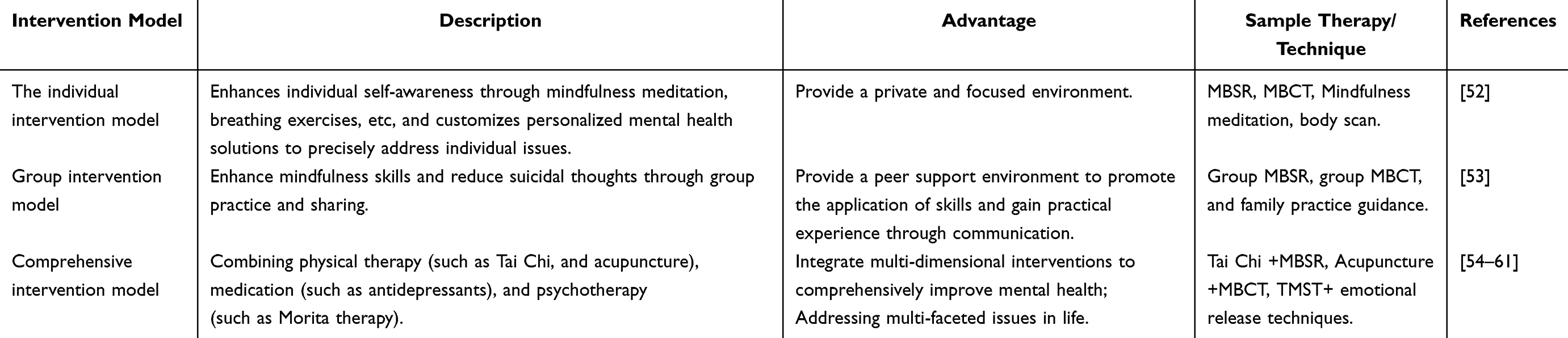 |
Table 1 Different Types of Mindfulness Methods and Their Specific Descriptions |
Individual Intervention Model
This model includes exercises such as mindfulness meditation, mindfulness of breathing, and body scanning, which can help individuals increase their awareness of their own experiences, enhance the perceived quality of their daily lives, and manage stress, emotions, and pain more effectively, which in turn improves overall mental health and quality of life.52 Individual interventions have the advantage of being personalized to an individual’s specific needs and problems, thus addressing the individual more precisely, and also providing a more private and focused environment in which the individual can understand and apply mindfulness techniques in greater depth.
Group Intervention Model
Compared to the individual intervention model, in addition to significantly increasing the individual’s level of mindfulness, it also reduces suicidal ideation also helps individuals to better understand and utilize mindfulness techniques through group practice and sharing. Researchers Annette Lloyd, Ross White, Catrin Eames, and Rebecca Crane, among others, assessed group intervention research on mindfulness-based stress reduction (MBSR) and mindfulness-based cognitive therapy (MBCT) through a narrative synthesis approach, with a particular focus on the role of home practice, and explored how to measure and enhance the quality and quantity of home practice.53 The advantage of group intervention is to provide a supportive environment so that individuals can feel the support and encouragement of their peers while practicing mindfulness, it also helps individuals to better apply mindfulness skills in their daily lives, and the communication and sharing among peers can provide more practical experience and advice.
Integrated Intervention Model
Combined with other therapies such as tai chi,54 acupuncture and moxibustion therapy,55 antidepressants,56 transcranial magnetic stimulation therapy (TMST),57 amygdala and insula retraining,58 etc, and various psychotherapies including Morita therapy,59 focused solution short-course therapy,60 memory refresher training,61 emotional release techniques,60 etc. is referred to as a combination intervention. The advantage of this intervention model is that it combines different therapies, thus addressing the psychological problems faced by the individual in a more comprehensive and effective way. A combination of interventions is usually more effective than a single therapy because it can target multiple aspects of an individual’s life, resulting in a more comprehensive improvement in the individual’s mental health.
The Practice of Mindfulness Therapy
Classical Models of Mindfulness Intervention MBSR and MBCT,62 all through a structured 8-week course. System Integration Body Scan,63 Mindful Breathing,64 Mindful Meditation65 Mindful Yoga,66 and other techniques enhance patients’ self-awareness, emotional regulation efficacy, and nonjudgmental acceptance of present-moment experiences. These intervention models have been widely validated in clinical practice and are particularly effective in relieving chronic pain, improving mood disorders (eg, depression and anxiety), and improving quality of life.67 The researchers used individualized mindfulness interventions for different groups, with children and adolescents often using a more playful and interactive form of mindfulness training,68 Interventions in the older population are more focused on improving cognitive functioning and emotional stability.69 For patients with chronic diseases (eg, diabetes, cancer), mindfulness interventions are often combined with disease management to aid in treatment by modulating stress responses, improving immune function, and promoting healthy behaviors.70
With the development of digital technology, emerging forms of mindfulness practice are rapidly gaining popularity. Mobile app-based mindfulness training provides individuals with flexible and low-threshold access to practice, while the introduction of Virtual Reality (VR) technology further enhances the immersion and depth of experience of mindfulness interventions,71 breathing new life into the practice of mindfulness. In addition, there is a growing interest in integrating the application of mindfulness with other therapies, For example, the combination of mindfulness and exercise therapy, or synergy with art therapy (eg, mindfulness painting,72 music therapy73), these cross-modal intervention strategies not only expand the application scenarios of mindfulness but also strengthen the intervention effect through multi-sensory stimulation. In the future, mindfulness practice promises a higher level of personalized intervention with the broadening and deeper application of multimodal technologies such as functional neuroimaging (fMRI),74 electroencephalography (EEG),75 and biomarker monitoring, mindfulness practice is expected to enable a higher level of personalized intervention. These technologies not only enable real-time tracking of physiological and psychological changes during mindfulness training but also provide precise data support for mechanistic research, driving mindfulness interventions toward a more scientific and precise approach rather than relying solely on experience.
The Mechanism of Mindfulness Therapy Facilitates Psychological Adjustment in DPN Patients
This article focuses on existing evidence regarding mindfulness meditation-based interventions for DPN patients and analyzes their underlying mechanisms from various perspectives, including neural activity, genetic material, and inflammatory responses, highlighting their interactions and mutual influences. The specific mechanisms are detailed as follows, with the mechanism diagram shown in Figure 3.
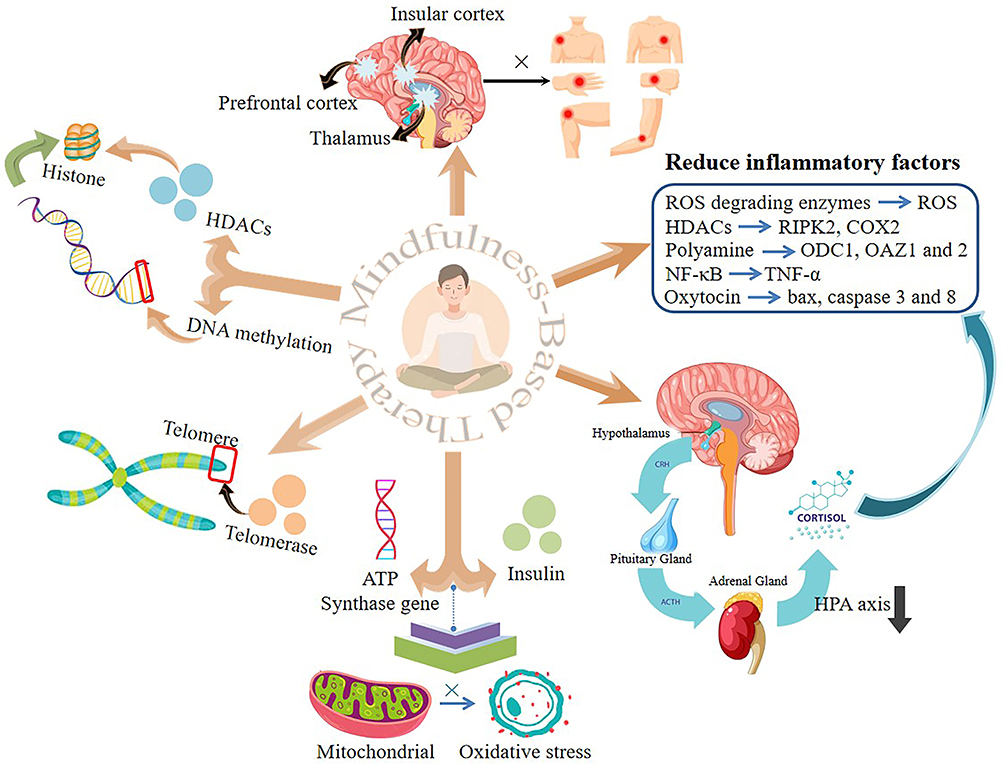 |
Figure 3 Mechanism Diagram of Mindfulness Therapy Facilitating Psychological Adjustment in DPN Patients. |
Neural Activity
Studies have found that mindfulness training can reduce activation in brain regions associated with pain, such as the insula and the anterior cingulate cortex. As a key region for pain perception and emotional processing, the insular cortex exhibits significantly reduced activity under the influence of mindfulness meditation, indicating that patients experience a diminished perception and response to pain stimuli.76 As a relay station for sensory information, the thalamus exhibits reduced neural activity, further weakening the transmission of pain signals.77 The secondary somatosensory cortex plays a crucial role in processing the cognitive and emotional aspects of pain experiences. Its reduced activity suggests that patients’ pain experiences are effectively regulated at the cognitive level.78 See Figure 3 for details.
Genetic Material
Telomere
Telomeres are located at the ends of eukaryotic chromosomes and have repetitive DNA sequences shaped like caps that protect the chromosomes. Since DNA polymerase is unable to replicate its ends, telomeres shorten with each replication, eventually leading to cellular arrest and senescence.79 Although short telomeres cause aging, telomerase re-expression prevents premature aging caused by telomerase deficiency and short telomeres.80 Telomerase is a key enzyme that reverses transcribes and synthesizes DNA to increase telomeric DNA at the ends of eukaryotic chromosomes, thus maintaining telomere lengths.81 MT promotes telomeric DNA synthesis and cell division, mitigates telomere depletion due to cell division, and interrupts telomere shortening or lengthens telomeres by enhancing telomerase activity and inducing its re-expression.82 Avoiding chromosome end problems is essential for chromosome function and regulation of cell growth and longevity.83 It has been shown that diabetic patients who develop DPN have significantly accelerated biological aging based on telomere shortening,84 Therefore effective MT might be one of the reasonable means to improve the prognosis of DPN patients, as detailed in Figure 3.
DNA Methylation
DNA methylation is an important epigenetic modification that can affect chromatin structure and function without altering the DNA sequence. DNA methylation is critical for controlling gene expression. It has been shown that low methylation levels are one of the relatively specific risk factors for DPN,85 Long-term MT methylated genes such as FKBP5, SCL6A4, NR4A2, and CLU, regulates related proteins, balances methylation status, and enhances the organism’s benefit from epigenetic regulation,86 Based on this mechanism, MBT can improve the prognostic regression of DPN patients, as detailed in Figure 3.
Acetylation
Histone deacetylases (HDACs) play a key role in the regulation of gene expression as epigenetic regulatory enzymes. They repress gene transcription by removing acetyl groups from histones, making the chromatin structure compact. The expression of HDACs is reduced after mindfulness meditation, which may lead to increased histone acetylation and loosening of chromatin structure, which in turn promotes the transcriptional activity of relevant genes. This change may contribute to the reduction of inflammatory responses, as the expression of inflammatory genes is usually negatively regulated by HDACs.87 FK228 is a deacetylation inhibitor, which has been shown to serve as a targeted therapeutic agent for DPN based on modulating the expression of nerve regeneration markers and inflammatory mediators in animals with DPN, while mindfulness meditation, likewise as a down-regulator of HDACs, would also be an effective treatment for DPN,88 see Figure 3 for details.
Inflammations
Many experimental and clinical studies have shown that prolonged low-grade inflammation plays an important role in the pathogenesis of DPN. Elevated levels of inflammatory factors such as IL-6, IL-1, tumor necrosis factor α (TNF-α), and transforming growth factor β (TNF-β) are associated with the progression of neurodegeneration in DPN, and in addition, anti-inflammatory factors such as IL-1RA and IL-10 are upregulated as a result of compensatory responses.89 Reducing the body’s inflammatory response may serve as a way to effectively treat DPN. Mindfulness may slow down the process of neurological damage by reducing pro-inflammatory factors and oxidative stress markers. The details are as follows: a) Mindfulness meditation enhances ROS-degrading enzyme activity, reduces oxidative stress indicators such as ROS and 8-hydroxy-2-deoxyguanosine, and benefits brain homeostasis,86 long-term mindfulness training reduces cortisol and salivary accumulation and boosts immune response,90 short-term meditation activates parasympathetic nerves and inhibits NF-κB and inflammatory responses by releasing acetylcholine.91 b) The pro-inflammatory genes RIPK2 and COX2, which play important roles in the inflammatory response of peripheral blood mononuclear cells (PBMC), were significantly reduced after mindfulness meditation, and this reduction may stem from the reduction in the expression of HDACs and the alteration of the overall modification of histone proteins, and may be related to the modulatory effect of mindfulness meditation on the neuroendocrine system. Endocrine system. For example, mindfulness meditation may indirectly inhibit the expression of pro-inflammatory genes by decreasing the stress response and the secretion of stress hormones, such as cortisol.92 c) Meditation inhibits the expression of genes associated with acute inflammatory responses and wound healing, such as ODC1, OAZ1, and OAZ2 in the polyamine synthesis pathway, which may imply that, in a meditative state, the body reduces its response to injury and inflammation, thereby decreasing inflammatory responses during acute wound healing.41 d) TNF-α is an important mediator of the inflammatory response, and elevated levels are associated with chronic inflammation, cardiovascular disease, and neurodegenerative disease. Meditation may reduce TNF-α production by decreasing the activation of the NF-κB pathway and decreasing the release of inflammatory signals.93 See Figure 3 for details.
Hormones
HPA Axis
Steroid regulation of the HPA axis is regulated by three main types of factors: feedback, stress, and circadian rhythms. First, glucocorticoids, as a key factor in the negative feedback regulation of the HPA axis, act on the anterior pituitary and hypothalamus to inhibit the transcription of the opioid-opiomelanocortin (Pro-opiomelanocortin (POMC)) gene and the synthesis of the mRNA for CRH and AVP as well as the secretion of the hormones, thereby decreasing the synthesis and secretion of CRH and ACTH synthesis and secretion. Secondly, stress can increase the secretion of ACTH and cortisol through central actions mediated by CRH and AVP, providing the body with a systemic defense response in response to injury. Finally, circadian rhythms lead to a marked diurnal variation in ACTH and cortisol secretion, with a peak in the early morning and a nadir in the evening.94 Dysregulation of the circadian rhythm of ACTH and cortisol secretion in DPN leads to a sustained increase in the activity of the hypothalamic-pituitary-adrenal axis activity, which is associated with most of the clinical symptoms and abnormalities in neurophysiological parameters.95
Mindfulness practice reduces the activity of the lower HPA axis by decreasing mental stress and anxiety, which reduces cortisol secretion, which in turn enhances the effects of mindfulness practice, creating a positive feedback loop. In addition, inflammatory biomarkers such as CRP, IL-6, and IL-1β, which are associated with neuroinflammation and cognitive decline,96 are also affected by HPA axis activity. Mindfulness practice reduces the activation of the HPA axis and decreases the production of inflammatory factors by decreasing mental stress,97 which may promote the maintenance or improvement of cognitive function in DPN patients. See Figure 3 for details.
Oxytocin
Oxytocin, a neuropeptide secreted in the hypothalamus, plays a key role in regulating socialization, trust, and empathy by boosting activity in areas of the brain associated with emotional and social processing, such as the prefrontal cortex and the amygdala, to enhance emotional empathy and understanding of others.98 Oxytocin increased glutathione levels by significantly decreasing plasma lipid peroxidation and increasing glutathione levels. Inhibits Bax, caspase 3, and caspase 8, thereby inhibiting inflammatory, oxidative stress, and apoptotic pathways to attenuate the deleterious effects of hyperglycemia on peripheral neurons.99 Mindfulness practice promotes oxytocin release, reduces the body’s feelings of anxiety, and enhances social connectedness, which in turn will further stimulate oxytocin production.100 See Figure 3 for details.
Metabolism
Based on mitochondrial metabolism, high levels of reactive oxygen species (ROS) are generated in response to oxidative stress driven by high glucose concentrations or lack of insulin signaling, which contributes to the development of DPN.
Mindfulness meditation significantly enhances the expression of genes related to mitochondrial function and upregulates mitochondrial ATP synthase activity, which in turn improves the efficiency of redox reactions to reduce oxidative stress, thereby buffering cellular overactivation. Mindfulness meditation also enhances mitochondrial energy production and utilization through the upregulation of insulin function, thereby evoking mitochondrial resilience, which further improves cellular adaptability and reduces stress.101 See Figure 3 for details.
Mindfulness meditation is also involved in mediating energy metabolic processes by influencing insulin secretion. Specifically, mindfulness meditation upregulates the expression of genes associated with mitochondrial ATP synthase and insulin, promoting efficient energy production and utilization, while enhancing insulin signaling and improving insulin sensitivity.102 In addition, mindfulness meditation downregulated the expression of genes associated with the NF-κB pathway, attenuated oxidative stress and inflammatory responses, and also alleviated insulin resistance, as detailed in Figure 3.
Empirical Analysis of the Effects and Challenges of Mindfulness Therapy Applied to DPN Patients
Currently, DPN management is mostly focused on the physiologic level, with less research on psychological interventions. Teixeira et al’s study on mindfulness for diabetic peripheral neuropathy, published in 2010, focused on the fact that mindfulness meditation may positively affect diabetic peripheral neuropathy through mechanisms such as increasing patients’ pain tolerance, improving sleep quality, and promoting psychological well-being, but the specific mechanisms still need to be further researched and fine-tuned.103 A 2012 study104 confirmed that the HEIDIS-study (Stress-Strain Behavioral Simulation Study) was the first to explore the effectiveness of MBSI interventions in DPN, demonstrating a trend of increasing MBSI benefits over time. The 2019 Hussain and Said study showed that mindfulness meditation reduces pain perception by guiding DPN patients to focus on the present moment, reducing fear and anxiety of pain; it also promotes relaxation, improves sleep, and enhances emotional regulation, indirectly relieving symptoms such as anxiety and depression, which are often important factors in exacerbating pain.76 A randomized controlled trial by Izgu et al in 2020 explored that a mindfulness intervention improved neuropathic pain, fatigue, and quality of life due to DPN.105 Karolina A. Rozworska et al showed that MBSR applied to DPN patients significantly improved pain and quality of life by increasing the level of mindfulness, while the effect of pain catastrophizing was not significant.106 In a 2022 study, Ximei Weng et al delved into the effects of mindfulness training combined with aerobic exercise on DPN patients in terms of neurophysiological regulation (eg, modulation of pain perception, enhancement of neural plasticity), improvement of microcirculation (increasing blood flow, promoting vascular neovascularization and repair), anti-oxidative stress (decreasing the production of oxidative stress products, increasing the activity of antioxidant enzymes), and metabolic regulation (Regulation of glucose metabolism, improvement of lipid metabolism) and other aspects, these mechanisms work together to help promote the repair and regeneration of nerve tissue, reduce pain and other symptoms, and improve the quality of life of patients. Weng et al’s study also showed that mindfulness training combined with aerobic exercise is a safe and effective treatment method, which can significantly improve the neurological function and quality of life of DPN patients, and has a broad clinical application prospect and promotion value.107 Clinical trials of mindfulness and its related therapies in DPN are summarized and detailed in Table 2.
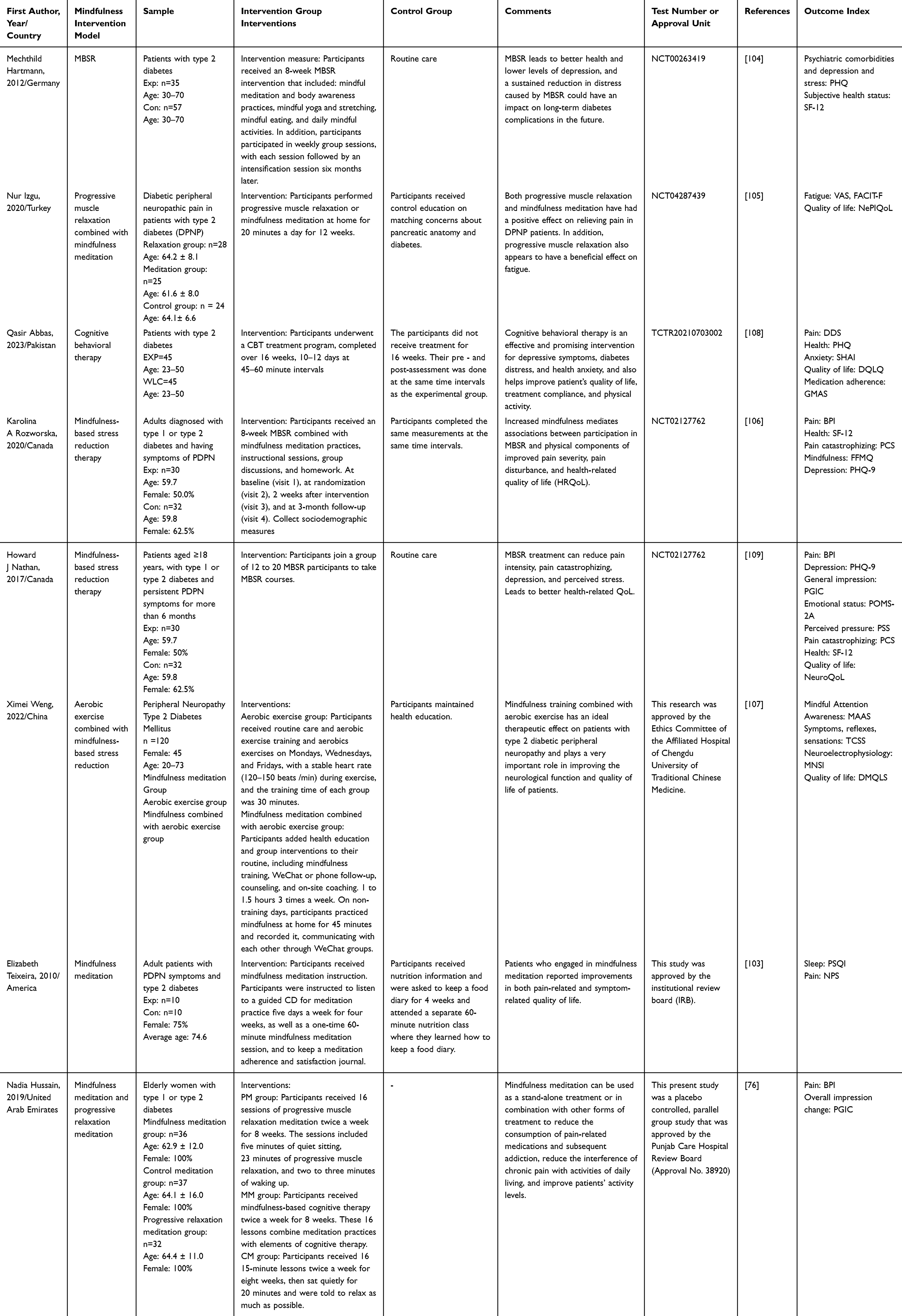 |
Table 2 The Summary of Clinical Trials of Positive Thoughts and Related Treatments in DPN |
Challenges and Future Perspectives in the Application of Mindfulness Therapy
The adaptation and localization of mindfulness in different cultural contexts has also become an important topic for future research and practice. Cross-cultural research will reveal the differences in the practice and effects of mindfulness in different cultures and provide a theoretical basis for localization and innovation.110 Combining local cultural traditions and values to develop mindfulness practices and methods suitable for local people will become an important direction for localizing mindfulness. Clinical studies have confirmed the effectiveness of short-term interventions with mindfulness therapy, but there is still a lack of validation of its effects through long-term longitudinal studies with large samples. There are also important challenges in avoiding cultural conflicts, identifying the right people, and ensuring the quality of training in mindfulness. Mindfulness therapy to meet the subjective needs of patients mainly depends on the level of the instructor, therefore, it is important to expand the faculty and balance the standardization of standardized operation and individualized application. At this stage, there is little research on the influencing factors of the effectiveness of mindfulness therapy, and further research is needed to comprehensively analyze the influencing factors. Similarly, mindfulness is an important concept in the discipline of nursing with practical applications in nurse wellness, the development and sustainability of quality of therapeutic care, and overall health promotion, and its widespread use provides strong support for improving the quality of care and promoting patient recovery as well.111 Therefore, research on the mechanism of action of mindfulness therapy, and the need for interdisciplinary research in neuroscience, psychology, physiology, sociology, education, and nursing on how it affects brain function, emotion regulation, and cognitive processes will help to reveal the deeper principles of action.112 With the development of technology, artificial intelligence, big data, smart devices, virtual reality and augmented reality and other technologies continue to progress, mindfulness therapy is gradually personalized and customized, with the help of intelligent assistive tools to provide users with instant physiological and psychological feedback, as well as immersive mindfulness experience.113 Emerging technologies such as functional near-infrared spectroscopy (fNIRS) have begun to be used for real-time monitoring of cerebral blood flow changes in mindfulness interventions, and the integration of multimodal data may reveal the precise neurobiological targets of mindfulness modulation of DPN in the future.114 It not only enhances the effectiveness and convenience of mindfulness practice but also lays a solid foundation for the popularization of mindfulness therapy. Meanwhile, a survey by Simona Racaru in 2021 revealed that caregivers have high expectations that DPN patients will benefit from psychological interventions such as mindfulness, seeing them as an effective means of augmenting medication or alternative therapies. However, the main challenge currently faced is how to effectively integrate mindfulness therapy into the traditional pain management system of care and ensure its universality. Therefore, caregivers need to delve into local resources to actively promote the benefits of mindfulness therapy to DPN patients, detail pain management interventions, and provide clear guidance. The integration of these psychotherapies into the daily care process should also be promoted when conditions permit.115 The application of mindfulness therapy in the field of DPN still faces many challenges and uncertainties, and researchers are needed to continuously explore and optimize the intervention methods, establish a more scientific and comprehensive effect assessment system, and rationally plan the intervention duration and other key parameters to promote its effective application and clinical development in the management of DPN patients. In conclusion, our study reviewed the mechanism of action, the current status of the application, and the potential challenges of mindfulness therapy in DPN. Combined with further exploration in the future, mindfulness therapy will provide new directions and opportunities for clinical decision-making in patients with DPN.
Conclusion
DPN, as a common complication of diabetes, is characterized by chronic pain and sensory dysfunction, posing significant challenges to its treatment. Our research indicates that MT, as a psychosocial intervention focused on consciousness and emotion regulation, can alleviate the symptoms of DPN by regulating pain perception, neurotransmitters, hormone levels, inflammatory responses, etc. However, the clinical integration of MT faces obstacles, including the feasibility of treatment plans, patient compliance, and effectiveness compared with drug intervention, etc. To address these gaps, future studies should further incorporate mindfulness-based assessment into the DPN care plan and enhance its role in the clinical aspects of DPN patients. In conclusion, our research provides a scientific reference direction for solving the treatment difficulties of patients with DPN.
Data Sharing Statement
All data in this study are available by contacting the corresponding author (Dr. Lihong Jia, [email protected]).
Author Contributions
All authors made a significant contribution to the work reported to varying degrees, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Zhou B, Rayner AW, Gregg EW, et al. Worldwide trends in diabetes prevalence and treatment from 1990 to 2022: a pooled analysis of 1108 population-representative studies with 141 million participants. Lancet. 2024;404:2077–2093.
2. Harding JL, Pavkov ME, Magliano DJ, Shaw JE, Gregg EW. Global trends in diabetes complications: a review of current evidence. Diabetologia. 2019;62:3–16. doi:10.1007/s00125-018-4711-2
3. Sun J, Wang Y, Zhang X, Zhu S, He H. Prevalence of peripheral neuropathy in patients with diabetes: a systematic review and meta-analysis. Prim Care Diabetes. 2020;14:435–444. doi:10.1016/j.pcd.2019.12.005
4. Selvarajah D, Kar D, Khunti K, et al. Diabetic peripheral neuropathy: advances in diagnosis and strategies for screening and early intervention. Lancet Diabetes Endocrinol. 2019;7:938–948. doi:10.1016/S2213-8587(19)30081-6
5. Zhu J, Hu Z, Luo Y, et al. Diabetic peripheral neuropathy: pathogenetic mechanisms and treatment. Front Endocrinol. 2024;14. doi:10.3389/fendo.2023.1265372
6. Pan Q, Fei S, Zhang L, et al. How does diabetic peripheral neuropathy impact patients’ burden of illness and the economy? A retrospective study in Beijing, China. Front Public Health. 2023;11. doi:10.3389/fpubh.2023.1164536
7. Cavanna AE, Purpura G, Riva A, Nacinovich R, Seri S. The western origins of mindfulness therapy in ancient Rome. Neurol Sci. 2023;44:1861–1869. doi:10.1007/s10072-023-06651-w
8. Bunjak A, Černe M, Schölly EL. Exploring the past, present, and future of the mindfulness field: a multitechnique bibliometric review. Front Psychol. 2022;13. doi:10.3389/fpsyg.2022.792599
9. Tran MA, Vo-Thanh T, Soliman M, Ha AT, Van pham M. Could mindfulness diminish mental health disorders? The serial mediating role of self-compassion and psychological well-being. Curr Psychol. 2022;1–14. doi:10.1007/s12144-022-03421-3
10. Schuman-Olivier Z, Trombka M, Lovas DA, et al. Mindfulness and behavior change. Harv Rev Psychiatry. 2020;28:371–394. doi:10.1097/HRP.0000000000000277
11. Benson H, Beary JF, Carol MP. The relaxation response. Psychiatry. 1974;37:37–46. doi:10.1080/00332747.1974.11023785
12. Meares A. Massage as an adjunct to meditation in the psychological treatment of cancer. Aust J Physiother. 1980;26:25–26. doi:10.1016/S0004-9514(14)60799-6
13. Marciniak R, Sheardova K, Čermáková P, et al. Effect of meditation on cognitive functions in context of aging and neurodegenerative diseases. Front Behav Neurosci. 2014;8:75960. doi:10.3389/fnbeh.2014.00017
14. Germer CK. The Mindful Path to Self-Compassion. The Guilford Press; 2009.
15. Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen Hosp Psychiatry. 1982;4:33–47. doi:10.1016/0163-8343(82)90026-3
16. Davidson RJ, Kabat-Zinn J, Schumacher J, et al. Alterations in brain and immune function produced by mindfulness meditation. Psychosomatic Med. 2003;65:564–570. doi:10.1097/01.PSY.0000077505.67574.E3
17. Salmon P, Sephton S, Weissbecker I, et al. Mindfulness meditation in clinical practice. Cognit Behav Pract. 2004;11:434–446. doi:10.1016/S1077-7229(04)80060-9
18. Segal ZV, Teasdale, JD, Williams JMG.. Mindfulness-based cognitive therapy: theoretical rationale and empirical status. In Hayes SC, Follette VM, Linehan MM (editors). Mindfulness and Acceptance: Expanding the Cognitive-Behavioral Tradition. The Guilford Press; 2004:45–65.
19. Robins CJ, Chapman AL. Dialectical behavior therapy: current status, recent developments, and future directions. J Pers Disord. 2004;18:73–89. doi:10.1521/pedi.18.1.73.32771
20. Chiesa A, Serretti A. Mindfulness-based stress reduction for stress management in healthy people: a review and meta-analysis. J Altern Complementary Med. 2009;15:593–600. doi:10.1089/acm.2008.0495
21. Powers MB, Zum Vörde Sive Vörding MB, Emmelkamp PMG. Acceptance and commitment therapy: a meta-analytic review. Psychother Psychosom. 2009;78:73–80. doi:10.1159/000190790
22. Smallwood J, Bernhardt BC, Leech R, et al. The default mode network in cognition: a topographical perspective. Nat Rev Neurosci. 2021;22:503–513. doi:10.1038/s41583-021-00474-4
23. Bremer B, Wu Q, Mora Álvarez MG, et al. Mindfulness meditation increases default mode, salience, and central executive network connectivity. Sci Rep. 2022;12:13219. doi:10.1038/s41598-022-17325-6
24. Humble G, Geddes H, Baell O, et al. TMS-EEG shows mindfulness meditation is associated with a different excitation/inhibition balance in the dorsolateral prefrontal cortex. Mindfulness. 2025;16:347–365. doi:10.1007/s12671-025-02519-6
25. Wood ET, Cummings KK, Jung J, et al. Sensory over-responsivity is related to GABAergic inhibition in thalamocortical circuits. Transl Psychiatry. 2021;11:1–10. doi:10.1038/s41398-020-01154-0
26. Yousefvand S, Hamidi F. The role of ventromedial hypothalamus receptors in the central regulation of food intake. Int J Pept Res Ther. 2021;27:689–702. doi:10.1007/s10989-020-10120-9
27. Adrover MF, Shin JH, Quiroz C, et al. Prefrontal cortex-driven dopamine signals in the striatum show unique spatial and pharmacological properties. J Neurosci. 2020;40:7510–7522. doi:10.1523/JNEUROSCI.1327-20.2020
28. Grimm C, Duss SN, Privitera M, et al. Tonic and burst-like locus coeruleus stimulation distinctly shift network activity across the cortical hierarchy. Nat Neurosci. 2024;27:2167–2177. doi:10.1038/s41593-024-01755-8
29. Tang R, Friston KJ, Tang -Y-Y. Brief mindfulness meditation induces gray matter changes in a brain hub. Neural Plast. 2020;2020:8830005. doi:10.1155/2020/8830005
30. Shanks J, Ramchandra R. Angiotensin II and the cardiac parasympathetic nervous system in hypertension. Int J Mol Sci. 2021;22:12305. doi:10.3390/ijms222212305
31. Daniela M, Catalina L, Ilie O, et al. Effects of exercise training on the autonomic nervous system with a focus on anti-inflammatory and antioxidants effects. Antioxidants. 2022;11:350. doi:10.3390/antiox11020350
32. Azizi SA. Monoamines: dopamine, norepinephrine, and serotonin, beyond modulation, “switches” that alter the state of target networks. Neuroscientist. 2022;28:121–143. doi:10.1177/1073858420974336
33. Holas P, Kamińska J. Mindfulness meditation and psychedelics: potential synergies and commonalities. Pharmacol Rep. 2023;75:1398–1409. doi:10.1007/s43440-023-00551-8
34. Minich DM, Henning M, Darley C, et al. Is melatonin the “next vitamin D”?: a review of emerging science, clinical uses, safety, and dietary supplements. Nutrients. 2022;14:3934. doi:10.3390/nu14193934
35. Fan Y, Cui Y, Tang R, et al. Salivary testosterone and cortisol response in acute stress modulated by seven sessions of mindfulness meditation in young males. Stress. 2024;27:2316041. doi:10.1080/10253890.2024.2316041
36. Kivimäki M, Bartolomucci A, Kawachi I. The multiple roles of life stress in metabolic disorders. Nat Rev Endocrinol. 2023;19:10–27. doi:10.1038/s41574-022-00746-8
37. Kip E, Parr-Brownlie LC. Healthy lifestyles and wellbeing reduce neuroinflammation and prevent neurodegenerative and psychiatric disorders. Front Neurosci. 2023;17:1092537. doi:10.3389/fnins.2023.1092537
38. Wang S, Zhang C, Sun M, et al. Effectiveness of mindfulness training on pregnancy stress and the hypothalamic-pituitary-adrenal axis in women in China: a multicenter randomized controlled trial. Front Psychol. 2023;14:1073494. doi:10.3389/fpsyg.2023.1073494
39. Giunta S, Xia S, Pelliccioni G, Olivieri F. Autonomic nervous system imbalance during aging contributes to impair endogenous anti-inflammaging strategies. GeroScience. 2024;46:113–127. doi:10.1007/s11357-023-00947-7
40. Gamaiunova L, Kreibig SD, Dan-Glauser E, et al. Effects of two mindfulness based interventions on the distinct phases of the stress response across different physiological systems. Biol Psychol. 2022;172:108384. doi:10.1016/j.biopsycho.2022.108384
41. Chandran V, Bermúdez M-L, Koka M, et al. Large-scale genomic study reveals robust activation of the immune system following advanced inner engineering meditation retreat. Proc Natl Acad Sci U S A. 2021;118:e2110455118. doi:10.1073/pnas.2110455118
42. Dunn TJ, Dimolareva M. The effect of mindfulness-based interventions on immunity-related biomarkers: a comprehensive meta-analysis of randomised controlled trials. Clinic Psychol Rev. 2022;92:102124. doi:10.1016/j.cpr.2022.102124
43. Chaix R, Fagny M, Cosin-Tomás M, et al. Differential DNA methylation in experienced meditators after an intensive day of mindfulness-based practice: implications for immune-related pathways. Brain Behav Immun. 2020;84:36–44. doi:10.1016/j.bbi.2019.11.003
44. Nakamura H, Tawatsuji Y, Fang S, Matsui T. Explanation of emotion regulation mechanism of mindfulness using a brain function model. Neural Networks. 2021;138:198–214. doi:10.1016/j.neunet.2021.01.029
45. Mahalakshmi AM, Ray B, Tuladhar S, et al. Impact of pharmacological and non-pharmacological modulators on dendritic spines structure and functions in brain. Cells. 2021;10:3405. doi:10.3390/cells10123405
46. Benchoula K, Parhar IS, Madhavan P, Hwa WE. CREB nuclear transcription activity as a targeting factor in the treatment of diabetes and diabetes complications. Biochem Pharmacol. 2021;188:114531. doi:10.1016/j.bcp.2021.114531
47. Schirò G, Iacono S, Ragonese P, et al. A brief overview on BDNF-trk pathway in the nervous system: a potential biomarker or possible target in treatment of multiple sclerosis? Front Neurol. 2022;13:917527. doi:10.3389/fneur.2022.917527
48. Wu E, Zhang J, Zhang J, Zhu S. Structural insights into gating mechanism and allosteric regulation of NMDA receptors. Curr Opin Neurobiol. 2023;83:102806. doi:10.1016/j.conb.2023.102806
49. Tang -Y-Y, Askari P, Choi C. Brief mindfulness training increased glutamate metabolism in the anterior cingulate cortex. Neuroreport. 2020;31:1142–1145. doi:10.1097/WNR.0000000000001527
50. Gupta S, Gupta AK, Mehan S, et al. Disruptions in cellular communication: molecular interplay between glutamate/NMDA signalling and MAPK pathways in neurological disorders. Neuroscience. 2025;569:331–353. doi:10.1016/j.neuroscience.2025.01.021
51. Wang CS, McCarthy CI, Guzikowski NJ, Kavalali ET, Monteggia LM. Brain-derived neurotrophic factor scales presynaptic calcium transients to modulate excitatory neurotransmission. Proc Natl Acad Sci U S A. 2024;121:e2303664121. doi:10.1073/pnas.2303664121
52. Michalak J, Crane C, Germer CK, et al. Principles for a responsible integration of mindfulness in individual therapy. Mindfulness. 2019;10:799–811. doi:10.1007/s12671-019-01142-6
53. Zhang H, Zhang A, Liu C, Xiao J, Wang K. A brief online mindfulness-based group intervention for psychological distress among Chinese residents during COVID-19: a pilot randomized controlled trial. Mindfulness. 2021;12:1502–1512. doi:10.1007/s12671-021-01618-4
54. Shen H, Du X, Fan Y, Dai J, Wei G-X. Interoceptive sensibility mediates anxiety changes induced by mindfulness-based tai chi chuan movement intervention. Mindfulness. 2023;14:1662–1673. doi:10.1007/s12671-023-02162-z
55. Jiayuan Z, Xiang-Zi J, Li-Na M, Jin-Wei Y, Xue Y. Effects of mindfulness-based tai chi chuan on physical performance and cognitive function among cognitive frailty older adults: a six-month follow-up of a randomized controlled trial. J Prev Alzheimers Dis. 2022;9:104–112. doi:10.14283/jpad.2021.40
56. Montero-Marin J, Maj van der Velden A, Kuyken W. Mindfulness-based cognitive therapy’s untapped potential. JAMA Psychiatry. 2024;81:1059–1060. doi:10.1001/jamapsychiatry.2024.2741
57. Gao L, Xie J, Huang T, Shang Y, Gao Z. Effects of mindfulness decompression therapy combined with transcranial magnetic stimulation in generalized anxiety disorder. Am J Transl Res. 2021;13:6827.
58. Sanabria-Mazo JP, Montero-Marin J, Feliu-Soler A, et al. Mindfulness-based program plus amygdala and insula retraining (MAIR) for the treatment of women with fibromyalgia: a pilot randomized controlled trial. J Clin Med. 2020;9:3246. doi:10.3390/jcm9103246
59. Lin Y, Hsu CC, Lin CJ, et al. Neurobiological mechanisms of dialectical behavior therapy and morita therapy, two psychotherapies inspired by zen. J Neural Transm. 2023;130:1077–1088. doi:10.1007/s00702-023-02644-3
60. Hedayati Zafarghandi S, Emamipour S, Rafiepoor A. A comparative study of the effectiveness of the solution-focused brief therapy and mindfulness-based therapy to reduce educational stress in junior high school students in Tehran. Shen J Psychol Psychiatr. 2022;9:123–135. doi:10.32598/shenakht.9.3.123
61. Jha AP, Denkova E, Zanesco AP, et al. Does mindfulness training help working memory ‘work’ better? Curr Opin Psychol. 2019;28:273–278. doi:10.1016/j.copsyc.2019.02.012
62. Ni Y, Ma L, Li J. Effects of mindfulness-based stress reduction and mindfulness-based cognitive therapy in people with diabetes: a systematic review and meta-analysis. J Nurs Scholarsh. 2020;52:379–388. doi:10.1111/jnu.12560
63. Guthrie T, Matthews JR, Chambers R, Windt J, Hohwy J. Changes in multisensory integration following brief state induction and longer-term training with body scan meditation. Mindfulness. 2022;13:1214–1231. doi:10.1007/s12671-022-01869-9
64. Komariah M, Ibrahim K, Pahria T, Rahayuwati L, Somantri I. Effect of mindfulness breathing meditation on depression, anxiety, and stress: a randomized controlled trial among university students. Healthcare. 2023;11:26. doi:10.3390/healthcare11010026
65. Galante J, Grabovac A, Wright M, et al. A framework for the empirical investigation of mindfulness meditative development. Mindfulness. 2023;14:1054–1067. doi:10.1007/s12671-023-02113-8
66. Miao C, Gao Y, Li X, et al. The effectiveness of mindfulness yoga on patients with major depressive disorder: a systematic review and meta-analysis of randomized controlled trials. BMC Complement Med Ther. 2023;23:313. doi:10.1186/s12906-023-04141-2
67. Sharma PK, Kumra R. Relationship between mindfulness, depression, anxiety and stress: mediating role of self-efficacy. Pers Individ Dif. 2022;186:111363. doi:10.1016/j.paid.2021.111363
68. Kil H, Antonacci R, Shukla S, De Luca A. Mindfulness and parenting: a meta-analysis and an exploratory meta-mediation. Mindfulness. 2021;12:2593–2612. doi:10.1007/s12671-021-01720-7
69. Kwon C-Y, Chung S-Y, Kim JW. Mindfulness meditation program for the elderly in Korea: a preliminary review for planning the program. Integrat Med Res. 2021;10:100451. doi:10.1016/j.imr.2020.100451
70. Zhang X, Tan SS, Fierloos I, et al. Evaluation design of the Social Engagement Framework for Addressing the Chronic-disease-challenge (SEFAC): a mindfulness-based intervention to promote the self-management of chronic conditions and a healthy lifestyle. BMC Public Health. 2019;19:664. doi:10.1186/s12889-019-6979-7
71. Chandrasiri A, Collett J, Fassbender E, De Foe A. A virtual reality approach to mindfulness skills training. Virtual Reality. 2020;24:143–149.
72. Liu C, Chen H, Liu C-Y, Lin R-T, Chiou W-K. Cooperative and individual mandala drawing have different effects on mindfulness, spirituality, and subjective well-being. Front Psychol. 2020;11:564430.
73. Liu H, Gao X, Hou Y. Effects of mindfulness-based stress reduction combined with music therapy on pain, anxiety, and sleep quality in patients with osteosarcoma. Braz J Psychiatry. 2019;41:540–545. doi:10.1590/1516-4446-2018-0346
74. Weder BJ. Mindfulness in the focus of the neurosciences - The contribution of neuroimaging to the understanding of mindfulness. Front Behav Neurosci. 2022;16:928522. doi:10.3389/fnbeh.2022.928522
75. Ng H-YH, Wu CW, Huang F-Y, et al. Mindfulness training associated with resting-state electroencephalograms dynamics in novice practitioners via mindful breathing and body-scan. Front Psychol. 2021;12. doi:10.3389/fpsyg.2021.748584
76. Hussain N, Said ASA. Mindfulness-based meditation versus progressive relaxation meditation: impact on chronic pain in older female patients with diabetic neuropathy. J Evid Based Complementary Altern Med. 2019;24:2515690X19876599. doi:10.1177/2515690X19876599
77. Riegner G, Posey G, Oliva V, et al. Disentangling self from pain: mindfulness meditation–induced pain relief is driven by thalamic–default mode network decoupling. Pain. 2023;164:280–291. doi:10.1097/j.pain.0000000000002731
78. Okada T, Kato D, Nomura Y, et al. Pain induces stable, active microcircuits in the somatosensory cortex that provide a therapeutic target. Sci Adv. 2021;7. doi:10.1126/sciadv.abd8261
79. Eppard M, Passos JF, Victorelli S. Telomeres, cellular senescence, and aging: past and future. Biogerontology. 2024;25:329–339. doi:10.1007/s10522-023-10085-4
80. Piñeiro-Hermida S, Autilio C, Martínez P, et al. Telomerase treatment prevents lung profibrotic pathologies associated with physiological aging. J Cell Biol. 2020;219:e202002120. doi:10.1083/jcb.202002120
81. He Y, Wang Y, Liu B, et al. Structures of telomerase at several steps of telomere repeat synthesis. Nature. 2021;593:454–459. doi:10.1038/s41586-021-03529-9
82. Smith EM, Pendlebury DF, Nandakumar J. Structural biology of telomeres and telomerase. Cell Mol Life Sci. 2020;77:61–79. doi:10.1007/s00018-019-03369-x
83. Anitha A, Thanseem I, Vasu MM, Viswambharan V, Poovathinal SA. Telomeres in neurological disorders. Adv Clin Chem. 2019;90:81–132.
84. Kwiatkowska KM, Garagnani P, Bonafé M, et al. Painful diabetic neuropathy is associated with accelerated epigenetic aging. GeroScience. 2025;47:4041–4054. doi:10.1007/s11357-025-01516-w
85. Zhang -H-H, Han X, Wang M, et al. The association between genomic DNA methylation and diabetic peripheral neuropathy in patients with type 2 diabetes mellitus. J Diabetes Res. 2019;2019:2494057. doi:10.1155/2019/2494057
86. Wu C, Feng Y. Exploring the potential of mindfulness-based therapy in the prevention and treatment of neurodegenerative diseases based on molecular mechanism studies. Front Neurosci. 2023;17:1097067. doi:10.3389/fnins.2023.1097067
87. Venditti S, Verdone L, Reale A, et al. Molecules of silence: effects of meditation on gene expression and epigenetics. Front Psychol. 2020;11. doi:10.3389/fpsyg.2020.01767
88. Thakur V, Gonzalez MA, Parada M, Martinez RD, Chattopadhyay M. Role of histone deacetylase inhibitor in diabetic painful neuropathy. Mol Neurobiol. 2024;61:2283–2296. doi:10.1007/s12035-023-03701-4
89. Zheng H, Sun W, Zhang Q, et al. Proinflammatory cytokines predict the incidence of diabetic peripheral neuropathy over 5 years in Chinese type 2 diabetes patients: a prospective cohort study. EClinicalMedicine. 2021;31:100649. doi:10.1016/j.eclinm.2020.100649
90. Tang -Y-Y, Fan Y, Lu Q, et al. Long-term physical exercise and mindfulness practice in an aging population. Front Psychol. 2020;11. doi:10.3389/fpsyg.2020.00358
91. Arora R, Verma H, Banumathy N, Sharma M. The regulation of neuro-immune system by pi (parasympathetic) and SiGMA (sympathetic induction governed by meditation and asana) rhythmicity. In: Anand A, editor. Neuroscience of Yoga: Theory and Practice: Part 1. Singapore: Springer Nature; 2024:17–36. doi:10.1007/978-981-97-2851-0_2
92. Yang H-J, Koh E, Sung M-K, Kang H. Changes induced by mind–body intervention including epigenetic marks and its effects on diabetes. Int J Mol Sci. 2021;22:1317. doi:10.3390/ijms22031317
93. Bushell W, Castle R, Williams MA, et al. Meditation and yoga practices as potential adjunctive treatment of SARS-CoV-2 infection and COVID-19: a brief overview of key subjects. J Altern Complementary Med. 2020;26:547–556. doi:10.1089/acm.2020.0177
94. Androulakis IP. Circadian rhythms and the HPA axis: a systems view. WIREs Mech Dis. 2021;13:e1518. doi:10.1002/wsbm.1518
95. Guan W, Li S, Sun W, Kang Y, Li X. Endocrine characteristics and risk factors of type 2 diabetes complicated with gastrointestinal autonomic neuropathy: a single-center retrospective study. Medicine. 2023;102:e33467. doi:10.1097/MD.0000000000033467
96. Mruczyk K, Cisek-Woźniak A, Molska M, Skoczek-Rubińska A. The role of inflammatory markers in linking metabolic syndrome to cognitive decline in middle-aged women: a focus on TNF-α and IL-6. Metabolites. 2025;15:186. doi:10.3390/metabo15030186
97. Ring HZ, Kern R. Zen meditation and the neuro-immuno-endocrine axis. Health. 2024;16:1242–1249. doi:10.4236/health.2024.1612086
98. Triana-Del Rio R, Ranade S, Guardado J, et al. The modulation of emotional and social behaviors by oxytocin signaling in limbic network. Front Mol Neurosci. 2022;15. doi:10.3389/fnmol.2022.1002846
99. Erdoğan MA, Taşkıran E, Yiğittürk G, Erbaş O, Taşkıran D. The investigation of therapeutic potential of oxytocin and liraglutide on vincristine-induced neuropathy in rats. J Biochem Mol Toxicol. 2020;34:e22415. doi:10.1002/jbt.22415
100. Bellosta-Batalla M, Del Carmen Blanco‐Gandía M, Rodríguez‐Arias M, et al. Brief mindfulness session improves mood and increases salivary oxytocin in psychology students. Stress Health. 2020;36:469–477. doi:10.1002/smi.2942
101. Gomutbutra P, Srikamjak T, Sapinun L, et al. Effect of intensive weekend mindfulness-based intervention on BDNF, mitochondria function, and anxiety. A randomized, crossover clinical trial. Compr Psychoneuroendocrinol. 2022;11:100137. doi:10.1016/j.cpnec.2022.100137
102. Pascoe MC, Thompson DR, Ski CF. Meditation and endocrine health and wellbeing. Trends Endocrinol Metab. 2020;31:469–477. doi:10.1016/j.tem.2020.01.012
103. Teixeira E. The effect of mindfulness meditation on painful diabetic peripheral neuropathy in adults older than 50 years. Holist Nurs Pract. 2010;24:277. doi:10.1097/HNP.0b013e3181f1add2
104. Hartmann M, Kopf S, Kircher C, et al. Sustained effects of a mindfulness-based stress-reduction intervention in type 2 diabetic patients. Diabetes Care. 2012;35:945–947. doi:10.2337/dc11-1343
105. Izgu N, Gok Metin Z, Karadas C, et al. Progressive muscle relaxation and mindfulness meditation on neuropathic pain, fatigue, and quality of life in patients with type 2 diabetes: a randomized clinical trial. J Nurs Scholarsh. 2020;52:476–487. doi:10.1111/jnu.12580
106. Rozworska KA, Poulin PA, Carson A, Tasca GA, Nathan HJ. Mediators and moderators of change in mindfulness-based stress reduction for painful diabetic peripheral neuropathy. J Behav Med. 2020;43:297–307. doi:10.1007/s10865-019-00079-4
107. Weng X, Liao S, Wang F, Wang H, Yang L. Evaluation of mindfulness training combined with aerobic exercise on neurological function and quality of life in patients with peripheral neuropathy type 2 diabetes mellitus. Contrast Media Mol Imaging. 2022;2022:7665483. doi:10.1155/2022/7665483
108. Abbas Q, Latif S, Ayaz Habib H, et al. Cognitive behavior therapy for diabetes distress, depression, health anxiety, quality of life and treatment adherence among patients with type-II diabetes mellitus: a randomized control trial. BMC Psychiatry. 2023;23:86. doi:10.1186/s12888-023-04546-w
109. Nathan HJ, Poulin P, Wozny D, et al. Randomized trial of the effect of mindfulness-based stress reduction on pain-related disability, pain intensity, health-related quality of life, and A1C in patients with painful diabetic peripheral neuropathy. Clin Diabetes. 2017;35:294–304. doi:10.2337/cd17-0077
110. Karl JA, Prado SMM, Gračanin A, et al. The cross-cultural validity of the five-facet mindfulness questionnaire across 16 countries. Mindfulness. 2020;11:1226–1237. doi:10.1007/s12671-020-01333-6
111. White L. Mindfulness in nursing: an evolutionary concept analysis. J Adv Nurs. 2014;70:282–294. doi:10.1111/jan.12182
112. Tortella GR, Seabra AB, Padrão J, Díaz-San Juan R. Mindfulness and other simple neuroscience-based proposals to promote the learning performance and mental health of students during the COVID-19 pandemic. Brain Sci. 2021;11:552. doi:10.3390/brainsci11050552
113. Mitsea E, Drigas A, Skianis C. Digitally assisted mindfulness in training self-regulation skills for sustainable mental health: a systematic review. Behav Sci. 2023;13:1008. doi:10.3390/bs13121008
114. Adachi K, Takizawa R. Effects of an online mindfulness-based intervention on brain haemodynamics: a pilot randomized controlled trial using functional near-infrared spectroscopy. Cereb Cortex. 2024;34:bhae321. doi:10.1093/cercor/bhae321
115. Racaru S, Sturt J, Celik A. The effects of psychological interventions on diabetic peripheral neuropathy: a systematic review and meta-analysis. Pain Manag Nurs. 2021;22:302–311. doi:10.1016/j.pmn.2020.11.001
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Qualitative Study of Migraine Headache Experience in Patients with Patent Foramen Ovale Based on the Symptom Management Theory
Li M, Feng M, Li M, Wei J, Li S, Zhang N, Li Q, Song R, Li H
Patient Preference and Adherence 2025, 19:2363-2375
Published Date: 10 August 2025
Analgesic Efficacy and Tolerability of Amitriptyline versus Mianserin in Chronic Low Back Pain: A Randomised, Double-Blind, Controlled Pilot Trial
Wangnamthip S, Eiamtanasate S, Saisavoey N, Sathienluckana T, Suthisiltham L, Panchoowong S, Tipapakoon I, Euasobhon P, Jensen MP, Srirojanakul W
Journal of Pain Research 2025, 18:6829-6847
Published Date: 17 December 2025
Comparative Effectiveness of Non-Pharmacological Interventions for Pain and Quality of Life in Women with Endometriosis: A Systematic Review and Network Meta-Analysis
Zheng X, Wang Y, Li H, Zhang J, Liu J, Zheng X, Zhang J, Fan G, Sun Y, Li B, Jiao J, Zuo G, Fan X, She Y
Journal of Pain Research 2026, 19:577080
Published Date: 20 February 2026
Crisugabalin Combined with Acetyl-Levo-Carnitine for Diabetic Peripheral Neuropathic Pain: A Phase 2 Randomized Controlled Trial
Fu L, Xu N, Shang J, Yang Q, Li Y, Huang Q, Li J, Jiang H
Journal of Pain Research 2026, 19:588472
Published Date: 21 April 2026