Back to Journals » Journal of Pain Research » Volume 18
Analgesic Efficacy and Tolerability of Amitriptyline versus Mianserin in Chronic Low Back Pain: A Randomised, Double-Blind, Controlled Pilot Trial
Authors Wangnamthip S ![]() , Eiamtanasate S, Saisavoey N, Sathienluckana T, Suthisiltham L, Panchoowong S, Tipapakoon I, Euasobhon P
, Eiamtanasate S, Saisavoey N, Sathienluckana T, Suthisiltham L, Panchoowong S, Tipapakoon I, Euasobhon P ![]() , Jensen MP
, Jensen MP ![]() , Srirojanakul W
, Srirojanakul W
Received 16 September 2025
Accepted for publication 1 December 2025
Published 17 December 2025 Volume 2025:18 Pages 6829—6847
DOI https://doi.org/10.2147/JPR.S568131
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Suratsawadee Wangnamthip,1 Sarasate Eiamtanasate,1 Nattha Saisavoey,2 Thanompong Sathienluckana,3 Lucksika Suthisiltham,1 Skaorat Panchoowong,1 Isaraporn Tipapakoon,1 Pramote Euasobhon,1 Mark P Jensen,4 Wanna Srirojanakul1
1Department of Anesthesiology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand; 2Department of Psychiatry, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand; 3Faculty of Pharmacy, Siam University, Bangkok, 10160, Thailand; 4Department of Rehabilitation Medicine, University of Washington, Seattle, WA, 98195, USA
Correspondence: Sarasate Eiamtanasate, Department of Anesthesiology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok Noi, Bangkok, 10700, Thailand, Tel +66896754232, Email [email protected]
Purpose: Chronic low back pain (CLBP) is a complex, disabling condition that often necessitates multimodal treatment. Although tricyclic and tetracyclic antidepressants are recommended as adjunctive therapy, comparative efficacy data remain extremely limited.
Patients and Methods: We conducted a randomised, double-blind, controlled trial in 24 individuals with CLBP to compare the efficacy and safety of amitriptyline with mianserin. Participants received amitriptyline (n = 15) or mianserin (n = 9) for 12 weeks with titrated dosing. Pain intensity (primary outcome), adverse effects, disability, health utility, quality of life, and psychological function were recorded at baseline and at each follow-up visit.
Results: Participants in both groups reported significant within-group reductions in pain intensity from baseline to week 12. Mianserin was associated with a large effect size improvement (Cohen’s d = − 1.40; 95% CI − 2.71 to – 0.08), and amitriptyline was associated with a medium effect size improvement (d = − 0.55; 95% CI − 1.19 to 0.08). Amitriptyline significantly improved EQ-5D-5L utility scores (Δ=+0.116, p=0.008; d=0.61, 95% CI 0.14 to 1.09) but was associated with more anticholinergic effects than mianserin. Mianserin was better tolerated; only transient drowsiness was reported. Different benefits were noted in some outcome measures as a function of treatment condition: amitriptyline reduced stress by week 6, whereas mianserin lowered anxiety at weeks 6 and 12.
Conclusion: Both amitriptyline and mianserin appear to provide comparable adjunctive efficacy for CLBP. Mianserin may be more tolerable and cost-effective in resource-limited settings, although it is not yet approved for pain indications.
Keywords: amitriptyline, antidepressants, chronic low back pain, mianserin, pain management, quality of life, randomised controlled trial
Introduction
Chronic low back pain is common and may present as non-specific pain, radiculopathy (or stenosis-related) pain, referred pain from non-spinal sources, or pain arising from specific spinal pathology.1,2 The global burden and prevalence of chronic low back pain (CLBP), citing the Global Burden of Disease Study.3 Symptoms typically arise from and may be maintained by complex interactions between biological, psychological, and social factors, including occupational postures, trauma history, activities of daily living, and psychological comorbidities such as depression. Less common aetiologies include surgical complications, osteoporosis, prolonged corticosteroid use, spinal infections, trauma, and bone metastases. Identifying the specific factors that contribute to the development and maintenance of chronic low back pain in any one individual is challenging; only 5% to 15% of cases are definitively diagnosed.4
Treatment of chronic low back pain is challenging. Due to its multifactorial nature, a multidisciplinary approach is the gold standard. Treatment modalities include pharmacological interventions, physiotherapy, structured exercise, interventional pain procedures, complementary therapies, psychological counselling, surgery, lifestyle modification, patient education, and training in self-management strategies.5 Among the pharmacological options, antidepressants are favoured because they enhance noradrenergic and serotonergic signalling, thereby modulating descending pain pathways and improving mood—an important benefit given the psychological distress that often accompanies chronic pain. Tricyclic antidepressants (TCAs), particularly amitriptyline, have been shown to reliably decrease pain through central and peripheral nervous system mechanisms. Evidence demonstrates the efficacy of TCAs in a variety of chronic pain syndromes, including fibromyalgia, neuropathic pain, tension-type headache, and musculoskeletal pain.6 However, their use is limited by anticholinergic adverse effects, which can include blurred vision, photophobia in glaucoma patients, urinary retention, constipation, and dry mouth. Furthermore, prolonged TCA use has been associated with increased dementia risk in elderly patients.7,8
In clinical studies, mianserin is a well-known a tetracyclic antidepressant.9 Studies in individuals with chronic idiopathic pain have shown that 50% experienced pain reduction with mianserin, exceeding 40%.10 The preclinical evidence has shown that mianserin produced analgesic effects in animal models through α2- and β-adrenergic mechanisms.11 Moreover, mianserin has been shown to be associated with fewer anticholinergic effects and less cardiotoxicity than TCAs.12,13
Amitriptyline, a tertiary tricyclic antidepressant, exerts analgesic and antidepressant effects primarily through potent inhibition of serotonin and norepinephrine reuptake, together with antagonism at muscarinic (M1–M5), histamine H1, α1-adrenergic, and 5-HT2 receptors, as well as modulation of voltage-gated sodium and potassium channels. These multimodal actions enhance descending inhibitory pain pathways but contribute to its anticholinergic and cardiovascular adverse effects. In contrast, mianserin is a tetracyclic antidepressant with minimal reuptake inhibition; its pharmacologic profile is dominated by potent antagonism at 5-HT2A/2C, histamine H1, and α2-adrenergic receptors, leading to increased noradrenergic transmission and sedation with a lower anticholinergic burden.14–16
Effective management of chronic low back pain must balance analgesic efficacy with tolerability to optimise patients’ emotional well-being and overall quality of life. While preclinical studies suggested mianserin had analgesic effects,11 clinical trials in chronic low back pain are outdated. However, comparative evidence for antidepressants in CLBP remains limited. To our knowledge, this study is the first randomised controlled trial to compare these two antidepressants in chronic low back pain, highlighting its clinical novelty and contribution to existing evidence. Most studies are small, heterogeneous, and short in duration, and none have directly compared amitriptyline with mianserin. Antidepressants are best regarded as adjuncts that enhance descending inhibitory control and address comorbid mood and sleep disturbance rather than as stand-alone analgesics. Amitriptyline remains the most established option but is constrained by anticholinergic and cardiac adverse effects, whereas mianserin may offer improved tolerability with less well-defined analgesic efficacy. The primary aim of this study was to address this knowledge gap. Secondary aims were to compare the two drugs with respect to their adverse-effect profiles and their relative effects on physical function, health-related quality of life, and psychological function.
Materials and Methods
Study Design and Setting
This study was approved by the Institutional Review Board of the Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand (Si 256/2018). All procedures were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to enrolment. We conducted a randomised, double-blind, controlled trial at Siriraj Hospital, Bangkok, Thailand, from 4 March 2019 to 31 March 2024. The trial was registered with the Thai Clinical Trials Registry (TCTR20190303001; 03 March 2019; https://www.thaiclinicaltrials.org/show/TCTR20190303001).
Participants
Adults (≥ 18 years) with chronic low back pain were recruited from the outpatient pain clinic. Exclusion criteria were hypersensitivity to amitriptyline or mianserin, psychiatric disease, pregnancy, cardiac disease or arrhythmias, benign prostatic hypertrophy, malignancy, or planned pain procedures or surgery during the study period. As noted in the section describing the power analysis conducted to determine the sample size needed for the study, we originally sought to enroll 60 participants (30 per condition). However, we were ultimately only able to enroll 34 participants, 24 of whom completed the study.
Study Protocol and Interventions
Qualified physicians and nurses screened potential participants for study inclusion. After eligibility was confirmed, written informed consent was obtained once the study aims and procedures had been explained. Participants were then randomised (Supplementary Figure S1) to receive either amitriptyline or mianserin.
Throughout the study, participants were allowed to take breakthrough analgesia—paracetamol with codeine or tramadol—although they were asked to maintain their individual pre-study daily doses of these medications.
Participants already receiving antidepressants underwent a rapid or gradual tapering over 2–6 weeks, depending on the dose they were taking at enrolment. For those on large doses [amitriptyline ≥ 75 mg or mianserin ≥ 60 mg], a gradual taper was used, as slower dose reductions reduce the likelihood of withdrawal. The dose was decreased by approximately 30% every 1–2 weeks (eg, amitriptyline 75 mg → 50 mg → 35 mg → 25 mg → 18 mg → 12.5 mg → stop; mianserin 60 mg → 45 mg → 30 mg → 20 mg → 15 mg → 10 mg → stop). For the small dose [amitriptyline ≤50 mg/day or mianserin 30 mg/day], a more rapid taper was applied, the dose was reduced by ~50% each week (eg, amitriptyline 50 mg → 25 mg → 10 mg → stop; mianserin 30 mg → 15 mg → 7.5 mg → stop), followed by a 2-week washout. Doses were rounded to available tablet strengths or given on alternate days if needed, in line with established recommendations,17,18 during which tramadol or codeine remained allowable as PRN breakthrough analgesics. Baseline measures of the study outcomes were then administered. Medication adherence was monitored via pill count at each follow-up visit, and missing data for primary outcomes were handled using the last observation carried forward (LOCF) method. These procedures were included to enhance transparency and reproducibility. Participants without prior antidepressant therapy entered the trial immediately after baseline assessment, because no wash-out was required. Patients or members of the public were not involved in the design, conduct, or reporting of this trial.
Data Collection and Outcome Measures
Data were collected at baseline (T0) and at weeks 2, 6 and 12 follow-up visits (T1–T3), when participants attended the pain clinic for dose adjustment based on their reported pain levels. Nurses and research assistants recorded all data on a standardized paper case report form.
Demographic and Medical History Variables
At baseline, demographic variables (age, sex at birth) and medical history (including comorbid medical conditions) were obtained from participant interviews and medical records.
Primary Outcome
Pain intensity was the primary outcome, and assessed using the 11-point NRS (0 = “No pain” and 10 = “Worst imaginable pain”). The NRS has a great deal of evidence supporting its reliability and validity as a measure of pain intensity,19 including in individuals from Thailand.20 It is also recommended as the measure of pain intensity with the most strengths and fewest weaknesses by consensus groups.21
Secondary Outcomes
The secondary outcome domains included adverse effect severity, physical disability, health-related quality of life, and psychological function.
Adverse Effect Severity
The 11-point NRS (0–10) was used to assess the severity of medication-related adverse effects.22 Symptoms assessed included dizziness, drowsiness, nausea and vomiting, constipation, dry mouth, palpitations, blurred vision, and difficulty urinating.23 A score of 0 denoted symptom absence, and 10 indicated the worst imaginable severity of each symptom. Prior research supports the reproducibility and sensitivity of a 0–10 NRS as a measure of symptom burden.22,24
Physical Function
Physical function was assessed using the commonly used 10-item Oswestry Disability Index. For each item, respondents rated their degree of disability related to that item on a 6-point Likert scale ranging from 0 (“No disability”) to 5 (“Severe disability”). The ODI covers ten specific symptoms and areas of function assessed, including pain intensity, personal care, lifting, walking, sitting, standing, sleeping, social life, travelling, and employment or homemaking. Responses are summed and converted to a percentage score, with 0% indicating no disability and 100% indicating maximal disability.25,26 Evidence supports the reliability and validity of the ODI for assessing physical disability in individuals with chronic low back pain internationally,25 including in individuals with chronic low back in from Thailand. The Thai version of the ODI has demonstrated excellent test–retest reliability (ICC = 0.98) and good internal consistency (Cronbach’s α = 0.81) in prior studies.27,28
Health-Related Quality of Life
Health-related quality of life was assessed using the 5-item EQ-5D-5L.29,30 The EQ-5D-5L captures problem severity in five domains: mobility, self-care, usual activities, pain or discomfort, and anxiety or depression. Each item is rated on a 5-point Likert scale (1 = “No problems”; 5 = “Extreme problems or inability to perform the activity”). Responses across the five domains are combined to generate a five-digit health state profile (eg, 1-2-3-1-4). This health state was then converted into a single summary “utility score” that can range from 0 (death) to 1 (optimal health), although scores below 0 are possible when health states are perceived as worse than death. In the general Thai population, utility scores have been shown to range from –0.4 to 0.9.30 Thai validation studies have demonstrated excellent test–retest reliability (ICC ≈ 0.82) and construct validity in patients with chronic conditions.31,32
Psychological Function
The Thai version of the DASS-2133,34 was used to evaluate participants’ depression, anxiety, and stress levels. With the DASS-21, each domain is assessed with seven items that ask respondents to indicate the severity of the symptom described by the items, rated on a 4-point Likert scale on a 0 (“Did not apply to me at all”) to 3 (“Applied to me very much or most of the time”). The responses to the items are summed and then doubled to yield a final score for each domain.33 The DASS-21 has demonstrated strong reliability and validity internationally.35,36 The DASS-21 has demonstrated strong psychometric properties in Thai populations, with Cronbach’s α values of 0.86, 0.82, and 0.90 for the Depression, Anxiety, and Stress subscales, respectively, indicating good to excellent reliability, and confirmatory factor analyses supporting the expected three-factor structure.34
Randomisation, Allocation, and Blinding
After informed consent, this randomised, double-blind, controlled trial allocated participants in a 1:1 ratio to the two treatment groups. The allocation sequence used permuted blocks of variable size (4 and 6), was generated with nQuery Advisor 6.0 (Statistical Solutions, Cork, Ireland), and accommodated up to 60 participants (30 per group). Sequence concealment used sequentially numbered, opaque, sealed envelopes prepared by the Division of Pharmaceutical Services at Siriraj Hospital, which was independent of participant enrolment; identical capsules were labelled to match the randomisation numbers. All participants, outcome assessors, and treating clinicians remained blinded to group assignments throughout the study.
Sample Size Calculation
The sample size was calculated using the n4Studies program,37 assuming a continuous outcome. With a standard deviation (σ) of 0.57, an expected mean difference between groups (ε) of 0.47, and a non-inferiority margin of 0.10, a ≤10% difference in pain reduction is generally regarded as clinically trivial in analgesic research. This threshold aligns with established standards used in previous non-inferiority pain trials;38–40 we did not have adequate power to test for significant between-group differences in the primary outcome. Therefore, although formal significance testing was conducted, the primary emphasis was on estimating and interpreting treatment effects using standardized effect sizes with 95% CIs. Medium or larger effects (Cohen’s d=0.5) were considered potentially meaningful. With 30 participants per arm, the minimum detectable difference was approximately d≈0.64, indicating that this pilot study should be considered as a preliminary study that could be used for estimation and feasibility rather than for definitive hypothesis testing.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 30 (IBM Corp, Armonk, NY, USA). Categorical variables were summarised as counts and percentages and compared with Pearson’s χ2 or Fisher’s exact tests. Continuous variables were tested for normality with the Shapiro–Wilk test; because most were non-normal, results are given as medians with interquartile ranges. Between-group differences in non-normal variables were tested using the Mann–Whitney U-test.
Longitudinal outcomes were examined using generalised estimating equations assuming a normal distribution, identity link, and exchangeable correlation structure. Models included fixed factors for group, time, and the group × time interaction, as well as any baseline variables that differed significantly between groups (p <0.05; notably in this case, disc pathology), as covariates to adjust for baseline imbalance. Estimated marginal means (95% CI) were reported, with Bonferroni-adjusted pairwise comparisons were conducted to evaluate within- and between-group differences over time.
Effect sizes were computed in R (R Foundation) via RStudio. Between-group effects used Cohen’s d based on the pooled SD (unequal-variance formulation where appropriate). Within-group (baseline to post) effects used paired standardized mean change (Cohen’s d based on the SD of the paired differences), applied where noted; 95% CIs were derived from standard formulas for d (between-group) and for paired d (within-group). We interpreted d values of 0.20, 0.50, and 0.80 as small, medium, and large, respectively, and used two-sided α = 0.05 for statistical significance. No subgroup or sensitivity analyses were pre-specified or conducted. Given the limited sample and lack of power for between-group tests, we emphasised effect sizes and considered medium or larger effects as potentially meaningful.
Results
Participant Flow and Baseline Characteristics
Between 4 March 2019 and 31 March 2024, 60 candidates were screened for eligibility. Of these, 26 did not meet inclusion criteria and were excluded, due to eligibility restrictions, withdrawals, and logistical constraints, leaving 34 participants who were randomized (20 to amitriptyline and 14 to mianserin). In the amitriptyline group, three participants were lost to follow-up, including two who discontinued due to intolerable side effects, resulting in 15 completing treatment. In the mianserin group, two participants were lost to follow-up and three discontinued due to intolerable side effects, leaving 9 who completed treatment. Thus, a total of 24 participants (15 on amitriptyline and 9 on mianserin) were included in the final analysis. The CONSORT flow diagram (Figure 1) illustrates participant progress through the trial. The CONSORT flow diagram in Figure 1 shows the progress of patients throughout the trial.
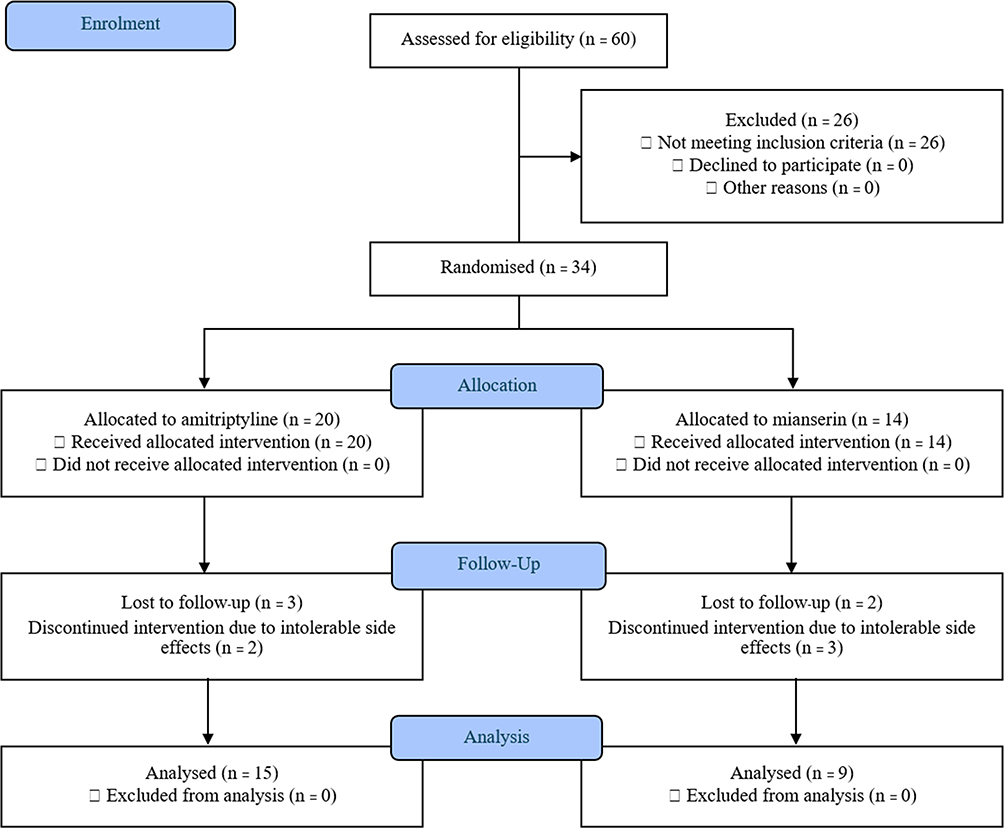 |
Figure 1 CONSORT flow diagram for the amitriptyline vs mianserin randomised, double-blind, controlled trial. Note: Numbers refer to participants unless stated otherwise; n = 34 randomised.Allocation ratio 1:1 used permuted blocks of size 4 and 6; sequence concealed with sequentially numbered, opaque, sealed envelopes prepared by an independent hospital pharmacy. |
Baseline demographic characteristics were comparable, with no significant (all p >0.05, effect sizes < medium) differences in age, birth sex, BMI, underlying medical conditions, or baseline pain intensity. More than two-thirds of participants in each group were female. However, back-pain aetiology differed significantly between groups (p = 0.021); disc pathology was more common in participants in the mianserin arm (Tables 1 and 2).
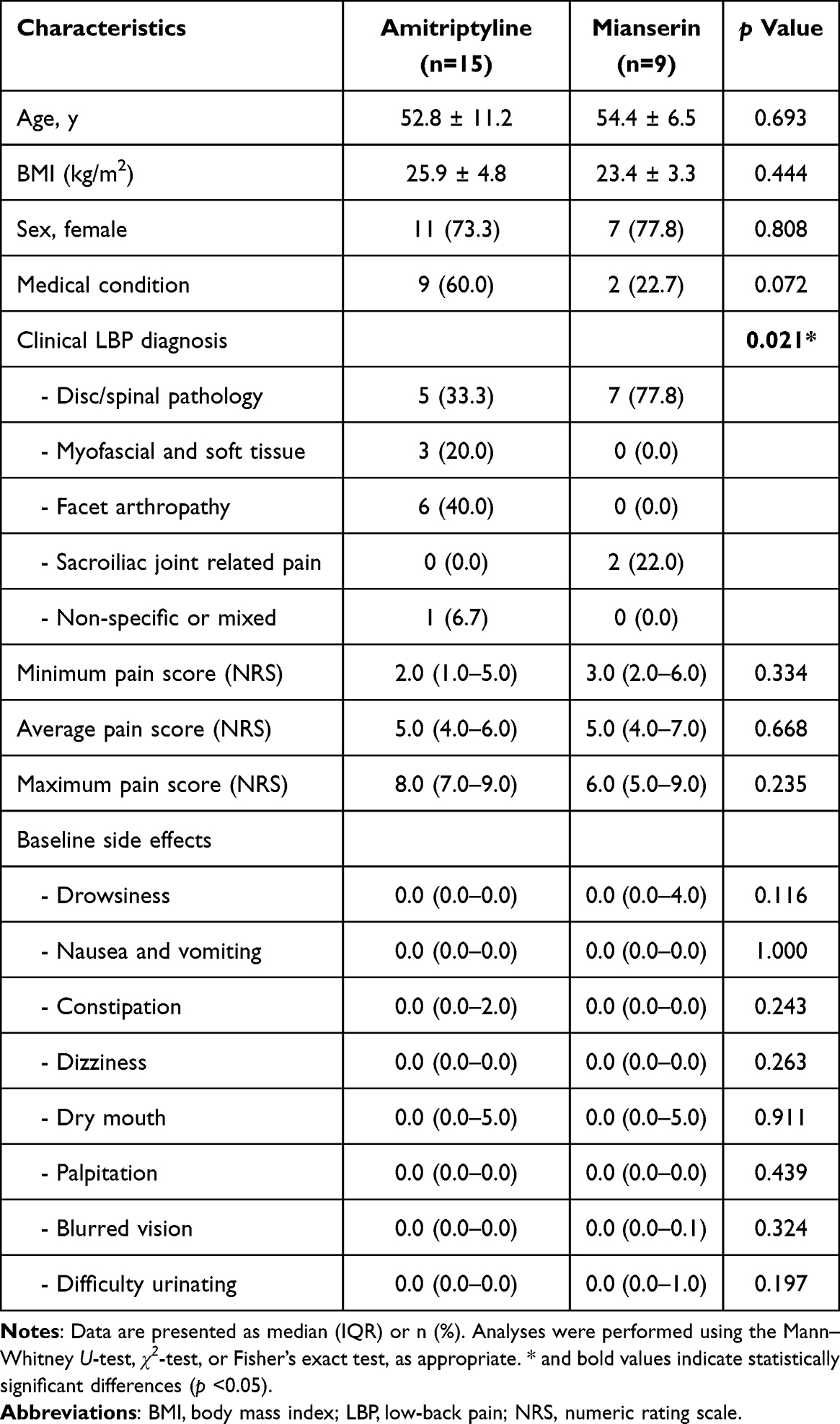 |
Table 1 Baseline Demographic and Clinical Characteristics of the Study Population |
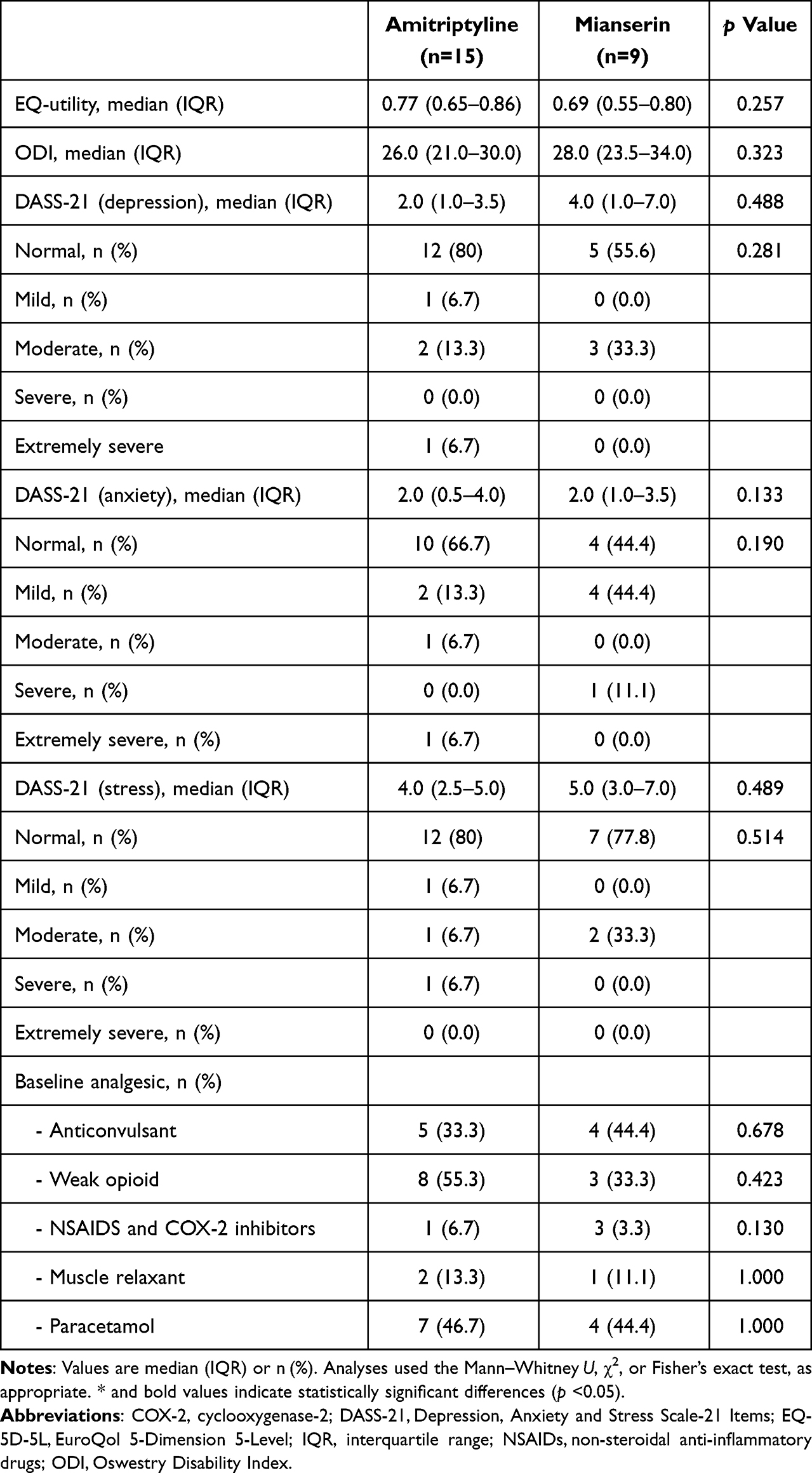 |
Table 2 Baseline Quality-of-Life, Physical-Function, Psychological-Status, and Concomitant-Analgesic Data |
Pain Reduction (Primary Outcome)
Between-Group Comparisons
GEE with Bonferroni correction, adjusted for baseline disc pathology, showed no significant difference between amitriptyline and mianserin groups at any time point (all Bonferroni-adjusted p’s ≥.302). At baseline, amitriptyline patients reported slightly lower pain (mean 4.85 vs 5.56), but this difference was not statistically significant (mean difference −0.71, 95% CI −2.25 to 0.84, p =0.372). By week 12, mean pain scores converged (3.10 for mianserin, 3.57 for amitriptyline; mean difference −0.47, 95% CI −2.32 to 1.38, p =0.618).
Between-Group Effect Size
Standardized mean differences were small and imprecise at all timepoints: baseline Cohen’s d = −0.34 (95% CI −1.05 to 0.36), week 2 Cohen’s d = 0.34 (95% CI −0.46 to 1.15), week 6 Cohen’s d = 0.22 (95% CI −0.61 to 1.05), and week 12 Cohen’s d = 0.16 (95% CI −0.73 to 1.04).
Within-Group Changes
In the amitriptyline group, pairwise comparisons (vs baseline) indicated a reduction in the amitriptyline; pain decreased from baseline (mean 4.85) to week 12 (3.57), but the difference did not reach significance (−1.28, 95% CI −2.77 to 0.21, p =0.138). Reductions at week 6 (−1.27, 95% CI −2.57 to 0.04, p =0.062) and week 2 (−0.53, 95% CI −1.61 to 0.55, p = 1.000) were also nonsignificant after Bonferroni correction. Compared with baseline to week 2 (mean change −0.53; Cohen’s d = −0.26, 95% CI −0.68 to 0.17), week 6 (−1.27; Cohen’s d = −0.60, 95% CI −1.15 to −0.06), and week 12 (−1.15; Cohen’s d = −0.55, 95% CI −1.19 to 0.08).
In the mianserin group, pairwise comparisons showed significant reductions in pain from baseline to week 12 (mean difference −2.46, 95% CI −4.20 to −0.68, p =0.002), and from baseline to week 6 (−2.45, 95% CI −4.22 to −0.68, p =0.002). Reductions at week 2 were also significant (−2.30, 95% CI −4.17 to −0.43, p =0.007). Improvements were larger and consistent across all timepoints: baseline to week 2 (−2.30; Cohen’s d = −1.03, 95% CI −1.90 to −0.16), week 6 (−2.44; Cohen’s d = −1.38, 95% CI −2.63 to −0.13), and week 12 (−2.50; Cohen’s d = −1.40, 95% CI −2.71 to −0.08). These represent large to very large effects, sustained through week 12. (Figure 2).
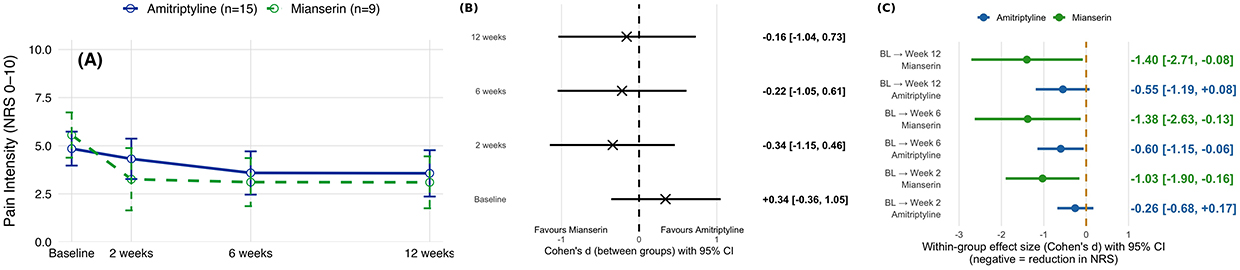 |
Figure 2 Change in numeric rating scale pain scores from baseline to week 12 Panel (A) Mean pain intensity (NRS 0–10) over time by treatment group; Points show estimated marginal means with 95% CIs plotted at baseline, week 2, week 6, and week 12. Panel (B) Between-group standardized mean differences (Cohen’s d) with 95% CIs at each time point.Panel (C) Within-group standardized mean change from baseline (Cohen’s d for paired data) with 95% Cis; Forest plots for each group show BL (baseline) to W2 (week 2), BL(baseline) to W6 (week 6), and BL (baseline) to W12 (week 12). Negative values indicate a reduction in pain. |
Adverse Effects
Sleepiness
GEE analysis adjusted for baseline disc pathology showed no significant between-group differences at any visit (all Bonferroni-adjusted p’s ≥.097). Between-group effect sizes were small to moderate (Cohen’s d −0.38 to 0.58, all 95% CIs included 0). Within groups, sleepiness increased significantly for mianserin at weeks 2 (Cohen’s d = 1.19, 95% CI 0.41 to 1.97) and 6 (Cohen’s d = 0.98, 95% CI 0.25 to 1.71), but not at week 12 (Cohen’s d = 0.31, 95% CI −0.42 to 1.04). Amitriptyline produced a progressive increase across all time points: week 2 (Cohen’s d = 0.93, 95% CI 0.19 to 1.67), week 6 (Cohen’s d = 1.23, 95% CI 0.46 to 2.00), and week 12 (Cohen’s d = 1.68, 95% CI 0.87 to 2.49).
Dry Mouth
Between-group differences were nonsignificant (GEE p’s ≥.075) after adjusting for baseline disc pathology, with effect sizes ranging from −0.21 to 0.81 (largest at week 12: Cohen’s d = 0.81, 95% CI −0.12 to 1.72). Within-arm analysis indicated significant increases only with amitriptyline, with moderate effects at weeks 2 (Cohen’s d = 0.82, 95% CI 0.06 to 1.58), 6 (Cohen’s d = 0.79, 95% CI 0.01 to 1.57), and 12 (Cohen’s d = 0.64, 95% CI −0.17 to 1.45). Mianserin showed no meaningful changes (Cohen’s d = 0.22 to −0.08, all 95% CIs crossing 0).
Difficulty Urinating
No between-group differences were detected (all p’s ≥.055) after adjusting for baseline disc pathology. Between-group d values ranged from −0.41 to 0.80 (95% CIs including 0). Within-group analysis showed no change with mianserin (Cohen’s d ≈ 0.00 to −0.08). By contrast, amitriptyline showed progressive worsening, with effect sizes increasing from small at week 2 (Cohen’s d = 0.34, 95% CI −0.42 to 1.10) to large by week 12 (Cohen’s d = 1.06, 95% CI 0.22 to 1.90).
Constipation
No significant between-group differences were observed in the reporting of constipation (all p’s ≥.06; Cohen’s d’s = −0.55 to 0.03, 95% CIs including 0). Within groups, changes were nonsignificant, with small and inconsistent effects (Cohen’s d ≤ 0.3).
Other Adverse Effects
For palpitations, blurred vision, and nausea/vomiting, no significant between-group differences were detected (all GEE with disc pathology adjusted p’s >0.05). Between-group effect sizes were small to moderate but imprecise (palpitations Cohen’s d’s = 0.40 to 0.61; blurred vision Cohen’s d’s = −0.47 to −0.08; nausea/vomiting trivial, all 95% CIs included 0). Within-group analyses indicated no significant or consistent changes were observed over time.
Overall, tolerability was broadly comparable between drugs. However, amitriptyline demonstrated a modestly higher anticholinergic burden, particularly for sleepiness, dry mouth, and difficulty urinating, whereas mianserin’s profile was generally more favorable. (Figure 3).
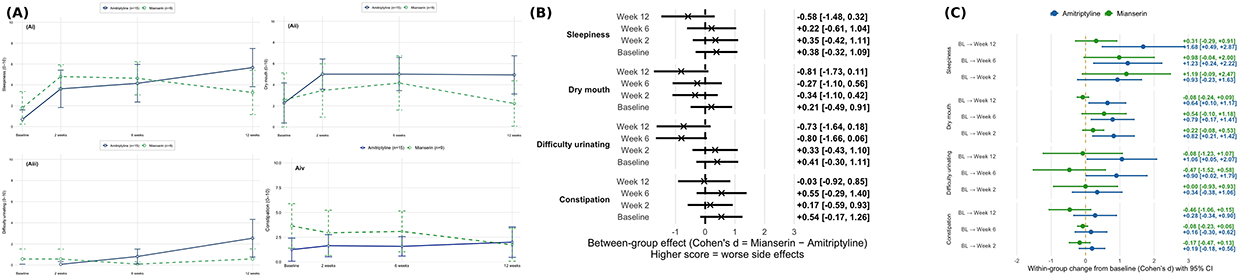 |
Figure 3 Time-course of selected anticholinergic side effects over 12 weeks Panel (Ai) Sleepiness, (Aii) Dry mouth, (Aiii) Difficulty urinating, (Aiv) Constipation. Mean scores (95% CI) analysed with generalised estimating equations; p <.05 considered significant.Panel (B) Between-group side effects (amitriptyline - mianserin). Cohen’s d with 95% CI at BL(Baseline), Weeks 2, 6, 12; Negative favors Mianserin (lower score), positive favors Amitriptyline.Panel (C) Within-group change from baseline. Cohen’s d (95% CI) for amitriptyline and mianserin at Weeks 2, 6, 12. |
Health-Related Quality of Life
Between groups, GEE pairwise comparisons adjusted by disc pathology revealed no statistically significant differences at any visit (weeks 0, 2, 6, and 12; all Bonferroni-adjusted p’s ≥.182). Between-group standardized mean differences were consistently small and imprecise (Cohen’s d =0.40, 95% CI −0.33 to 1.14 at baseline, Cohen’s d=0.32, 95% CI −0.49 to 1.33 at week 2, Cohen’s d=−0.36, 95% CI −0.52 to 1.24, and Cohen’s d=–0.40, 95% CI −0.57 to 1.33).
Within groups, both arms demonstrated progressive improvements from baseline. In amitriptyline, GEE contrasts showed a significant gain from baseline to week 12 (Δ = +0.110, p =0.009), and from baseline to week 2 (Δ = +0.084, p =0.030), corresponding to a moderate effect (Cohen’s d = 0.61, 95% CI 0.14 to 1.09). Improvements at weeks 2 and 6 were smaller and not statistically significant, with effect sizes of Cohen’s d = 0.39 (95% CI −0.01 to 0.79) and Cohen’s d = 0.49 (95% CI −0.17 to 1.15), respectively. In mianserin, GEE tests did not reach significance at any time point, but effect sizes suggested small to moderate gains: week 2 Cohen’s d = 0.53 (95% CI −0.25 to 1.30), week 6 Cohen’s d = 0.69 (95% CI −0.27 to 1.65), and week 12 Cohen’s d = 0.64 (95% CI −0.40 to 1.68). Collectively, these findings indicate within-arm improvements over time, particularly for amitriptyline, but no reliable between-group differences.
Physical Disability
Both groups showed small improvements in disability scores over 12 weeks. Without significant between-group differences after adjusting for disc pathology at any time point (weeks 0, 2, 6, 12; all Bonferroni-adjusted p ≥.354) at baseline (Cohen’s d = 0.16, 95% CI −0.54 to 0.86). Across follow-up, between-group differences were small and imprecise at week 2, Cohen’s d = −0.05, 95% CI −0.81 to 0.71, week 6, Cohen’s d = −0.05, 95% CI −0.88 to 0.77, and week 12, Cohen’s d = −0.27, 95% CI −1.16 to 0.61. Within-group standardized mean changes showed improvement from baseline in both arms (negative values reflect ODI decreases). For amitriptyline, effects were small from baseline to week 2 (Cohen’s d = −0.04, 95% CI −0.40 to 0.83), week 6 (Cohen’s d = −0.10, 95% CI −0.78 to 0.40), and week 12 (Cohen’s d = −0.25, 95% CI: −1.37 to 0.25). For mianserin, improvements were small at week 2 (Cohen’s d = −0.23, 95% CI −0.67 to 0.72) and week 6 (Cohen’s d = −0.36, 95% CI −0.90 to 0.50), with the largest change at week 12 (Cohen’s d = −0.55, 95% CI −1.20 to 0.14). (Figure 4).
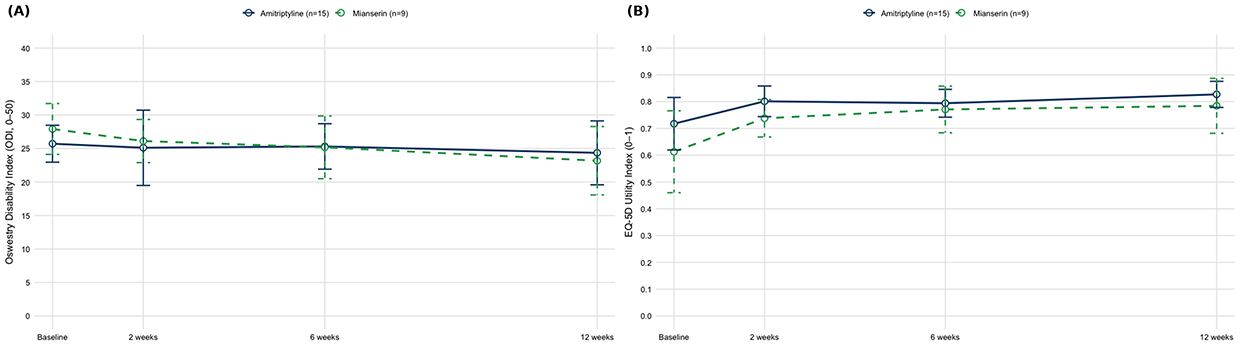 |
Figure 4 Longitudinal changes Panel (A) EQ-5D-5L utility Panel (B) ODI scores Mean (95% CI) values analysed with generalised estimating equations; p <.05 considered significant. Abbreviations: EQ 5D 5L, EuroQol Five Dimensions Five Levels; ODI, Oswestry Disability Index. |
Psychological Function
DASS21-Depression: Between groups. Bonferroni-adjusted GEE pairwise comparisons with adjusted baseline imbalance detected no differences between amitriptyline and mianserin at any visit (all p’s ≥.254): week 0 Δ=−2.05 (95% CI −5.56 to 1.47; p =0.254), week 2 Δ=−0.04 (−2.72 to 2.65; p =0.980), week 6 Δ=−0.09 (−1.74 to 1.56; p =0.980), week 12 Δ=−0.32 (−2.56 to 1.92; p =0.781). Consistently, between-group standardized effects were small and imprecise (Cohen’s d −0.48, −0.09, −0.17, −0.06 across weeks 0–12; all 95% CIs included 0).
Within groups. Neither arm showed a statistically significant change from baseline after Bonferroni correction (all p’s ≥.435), amitriptyline showed smaller changes (Baseline to week 2: +0.11; baseline to 6: −1.33; Baseline to week 12: −0.23), with small effect sizes (Cohen’s d ≈+0.03, −0.53, −0.47; CIs crossed 0). Mianserin exhibited larger numerical declines (Baseline to week 2: −1.90; Baseline to week 6: −3.29; Baseline to week 12: −2.83) with corresponding small to moderate, imprecise effect sizes (Cohen’s d=−0.40, 95% CI −1.14 to 0.35, Cohen’s d=−0.85, 95% CI: −2.12 to 0.42, and Cohen’s d=−0.66, 95% CI −1.97 to 0.65).
DASS-21 Anxiety: Between groups. Bonferroni-adjusted GEE pairwise comparisons, adjusted for baseline disc pathology, showed no differences between groups at any visit (all p’s ≥.20): baseline Δ = −0.19 (95% CI −3.00 to 2.63; p =0.897), week 2 Δ = 1.38 (−1.80 to 4.55; p =0.395), week 6 Δ = −0.83 (−3.30 to 2.96; p =0.443), and week 12 Δ = 1.51 (−0.85 to 3.87; p =0.209). Consistently, between-group effect sizes were small and imprecise: baseline Cohen’s d=−0.15, 95% CI −0.88 to 0.58, week 2 Cohen’s d=0.23, 95% CI −0.58 to 1.04, week 6 d=0.11, 95% CI −0.76, 0.99, week 12 d=0.46, 95% CI −0.53 to 1.46.
Within groups, amitriptyline showed a transient increase at week 2 vs baseline, but there were no significant differences at any visits (p’s ≥.282). Standardized changes for amitriptyline were small and imprecise from baseline to week 2, Cohen’s d=0.11, 95% CI −0.10 to 0.31; baseline to week 6, Cohen’s d=−0.15, 95% CI −0.51 to 0.21; from baseline to week 12, Cohen’s d=−0.21, 95% CI −0.57 to 0.15. While mianserin, anxiety decreased significantly from baseline at week 6 (Δ=−1.50; 95% CI −2.98 to −0.01; p =0.047; Cohen’s d = −0.74, 95% CI −1.44 to −0.05) and at week 12 (Δ=−2.31; −3.83 to −0.80; p <0.001; Cohen’s d=−1.49, 95% CI −2.59 to −0.38. The week-2 decline was smaller and not significant (Δ≈−0.96; Cohen’s d=−0.44, 95% CI −1.10 to 0.22).
DASS-21 Stress. Bonferroni-adjusted GEE, adjusting for baseline disc pathology, showed no between-group differences at weeks 0, 2, 6, or 12 (all p’s ≥.484). Between-group standardized effects were small at baseline and week 2, Cohen’s d=−0.27 (95% CI −1.00 to 0.46) and Cohen’s d=−0.14 (95% CI −0.31 to 0.03) and were moderate at weeks 6–12 (week 6 Cohen’s d=−0.68, 95% CI −1.09 to −0.26; week 12 Cohen’s d=−0.45, 95% CI −0.85 to −0.06).
Within groups, amitriptyline produced a significant reduction at week 6 vs baseline (Δ=−2.23, p =0.001), which was not maintained at week 12 (Δ=−1.65, p =0.123). In the mianserin, stress scores declined numerically at weeks 2, 6, and 12 (Δ=−2.00, −2.04, −2.18; all p’s =0.394 to 1.000), with small–moderate and imprecise within-arm effect sizes (week 2 Cohen’s d=−0.48, 95% CI −1.10 to 0.13; week 6 Cohen’s d=−0.55, 95% CI −1.27 to 0.17; week 12 Cohen’s d=−0.61, 95% CI −1.60 to 0.38) (Figure 5).
 |
Figure 5 Trajectory of DASS-21 across 12 weeks Panel (A) Depression scores Panel (B) Anxiety scores Panel (C) Stress scores Mean (95% CI) values analysed with generalised estimating equations; p <.05 considered significant. Abbreviations: DASS 21, Depression, Anxiety, and Stress Scale–21 Items. |
Discussion
Chronic low back pain is common worldwide and a leading cause of disability, undermining quality of life and straining healthcare systems. To our knowledge, this is the first randomized controlled trial directly comparing mianserin with amitriptyline for chronic low back pain, highlighting the clinical novelty and relevance of this work. Pharmacological treatment remains central to pain relief and functional gain; however, drug choice is complicated by heterogeneous efficacy and differing adverse-effect profiles. This study expands the evidence base by comparing amitriptyline and mianserin—two agents with distinct mechanisms of action—to identify effective yet tolerable options for chronic low back pain.9,41
This randomised, double-blind, controlled trial compared the efficacy and tolerability of amitriptyline and mianserin over a 12-week period. We evaluated pain reduction, adverse effects, functional outcomes, quality of life, and psychological symptoms. Both drugs appeared to produce meaningful improvements across outcomes, yet most between-group differences were non-significant.
Pain and Functional Outcomes
Both groups showed progressive pain reductions over 12 weeks; although the between-group differences were not statistically significant, within-group improvements were clinically meaningful. Because patients with psychiatric disorders were excluded, our findings suggest that both groups showed progressive pain reductions over 12 weeks; however, because the study did not include a placebo arm, we cannot exclude regression to the mean or other nonspecific effects as explanations for these improvements. Thus, while the within-group reductions were clinically notable, caution is warranted in interpreting these findings as evidence of direct analgesic efficacy of mianserin or amitriptyline independent of mood modulation. Mianserin was associated with early, sustained pain reduction from week 2 onwards at 10 mg/day, achieving maximal benefit at 30 mg/day. Although evidence for mianserin’s analgesic efficacy in chronic low back pain is limited, standard regimens are usually 30–60 mg/day, taken at bedtime. Mianserin’s analgesic mechanism may involve antagonism at 5-HT2A, 5-HT2C, and 5-HT3 receptors in dorsal horn neurons, together with possible agonism at opioid receptors.14,42–44 However, some clinical trials in idiopathic and neuropathic pain populations have not demonstrated significant analgesic effects within this dosage range.45
Amitriptyline was associated with significant analgesia once the dose reached 25 mg/day, consistent with recommended titration ranges and tolerability constraints. Clinical practice and research favour low-dose amitriptyline, 25–50 mg/day, for chronic low back pain. Although doses up to 150 mg/day have been studied, lower doses usually offer the best efficacy–tolerability balance.6 In the present study, functional gains paralleled analgesia. The baseline ODI scores of 25.8 in the amitriptyline group and 27.8 in the mianserin group (each indicating moderate disability) improved marginally to 24.5 and 23.1, respectively, in week 12. These changes did not meet the threshold for clinically meaningful improvement, typically defined as ≥ 10 points on the 0–50 scale.25,46 Nevertheless, both agents were associated with analgesic and functional benefits, supporting their potential role as adjunctive therapy for chronic musculoskeletal pain.
Quality of Life
The EQ-5D-5L utility scores rose steadily in both groups, surpassing the minimal clinically important difference (0.034);47 amitriptyline maintained marginally higher values at every visit. Although no significant between-group differences appeared, amitriptyline improved significantly from baseline to week 12, signalling greater impact on health-related quality of life. These gains align with the findings from previous studies, linking TCAs to improved well-being and sleep in chronic pain populations.48
Adverse Effects and Tolerability
Adverse effects were generally mild to moderate, consistent with the established safety profiles of both medications. Sedation and dry mouth were more prominent with amitriptyline, showing significant increases at multiple time points.49 Mianserin demonstrated better tolerability overall, although drowsiness increased at weeks 2 and 6. However, drowsiness usually lessens once the dose reaches 60 mg/day. Low doses act mainly as antihistamines, whereas higher doses block α2-adrenergic receptors, raise noradrenaline, and become activating.14,42 Importantly, no serious adverse events occurred with either medication. Mianserin exhibits little anticholinergic activity because it binds weakly to muscarinic receptors.50 Withdrawals therefore stemmed from tolerability, not safety, underscoring the need to individualise therapy according to comorbidities and patient preference.
Psychological Outcomes
Psychological symptoms, as measured by DASS-21, improved modestly: amitriptyline lowered stress by week 6, while mianserin reduced anxiety at weeks 6 and 12. Neither group showed significant changes in depression scores. The small overall mood change probably reflects the cohort’s normal–to–mild baseline scores.
Clinical Implications
The study findings support either amitriptyline or mianserin as adjunctive therapy, demonstrating comparable efficacy for pain intensity, functional status, and quality of life. Although amitriptyline modestly boosts EQ-5D utility, it’s use is also associated with more anticholinergic side effects, including drowsiness, dry mouth, palpitations, and urinary retention. Conversely, mianserin is better tolerated, especially in individuals sensitive to anticholinergic effects. Despite lacking regulatory approval for chronic pain, mianserin’s favourable profile—lower anticholinergic burden and low cost—makes it a viable off-label option. It is especially useful in resource-limited settings or for older, delirious, or cardiovascular-compromised individuals. The randomised, double-blind, controlled design strengthens internal validity and reliability. Results also endorse monitoring analgesia at low doses—mianserin 10–30 mg/day and amitriptyline 25 mg/day. Within the limits of this small, short-term study, mianserin demonstrated comparable efficacy and tolerability to amitriptyline, suggesting it may be considered a potential option in settings where tricyclic antidepressants are contraindicated or unavailable. Additional research in studies using larger sample sizes is needed to test this possibility.
Study Limitations
This study has several limitations. First, the small sample size may limit generalisability and increase type II error risk when detecting between-group differences. Second, the 12-week follow-up period may not fully capture long-term efficacy or sustainability of pain relief. Third, although the study was double-blinded, reliance on self-reported measures introduces potential reporting bias. Additional research using available objective measures of outcomes (eg, actigraphy as a potential measure of pain’s impact on function) is needed to evaluate the potential bias introduced by self-report in the outcomes studied. Fourth, although participant recruitment spanned five years, the study followed a standardized protocol, consistent eligibility criteria, and identical data collection methods throughout the study period. Therefore, the potential impact of time-related confounding is likely to be minimal. Finally, the absence of objective functional assessments or biomarkers limits mechanistic interpretation of treatment effects. Future research to test hypotheses regarding the mechanisms of the effects of mianserin on pain would be useful.
Future Directions
As noted previously, future research should build on this study’s results by conducting a larger, adequately powered trial. Based on our observed effect sizes, a sample of approximately 100–150 participants would likely be sufficient to detect a medium between-group effect with sufficient power and allowing for attrition. A multicenter design spanning pain clinics and primary care would make recruitment feasible. Larger and more diverse cohorts would improve generalisability and help determine optimal dosing for chronic low back pain. Including a placebo/usual-care arm would help distinguish true drug effects from regression to the mean. Comparative studies involving other antidepressants, including nortriptyline and serotonin and norepinephrine reuptake inhibitors, alongside non-pharmacological interventions, could place the benefits and risks of amitriptyline and mianserin into a sharper clinical context. A longer follow-up would clarify the long-term efficacy, safety profiles, and tolerability of amitriptyline and mianserin, offering a much-needed contribution to the chronic low back pain literature. Finally, elucidating the mechanisms behind efficacy and adverse-effect differences could guide the development of more targeted chronic-pain therapies.
Conclusions
Amitriptyline and mianserin were both associated with clinically meaningful improvements in pain intensity, disability, and health-related quality of life (EQ-5D utility). In the amitriptyline group, pain scores decreased by 1.28 points (26%), approaching the minimal clinically important difference (MCID) of 1.5 points, while mianserin achieved a 2.46-point (44%) reduction, exceeding this threshold. Amitriptyline yielded a statistically significant improvement in utility scores, but with a higher incidence of anticholinergic side effects consistent with its pharmacological profile. Mianserin demonstrated similar functional and analgesic benefits, with a lower anticholinergic burden and better tolerability. Secondary outcomes, including sleep quality and psychological function, improved in both groups, supporting the multidimensional benefits of antidepressant therapy in CLBP. Although direct cost comparisons are limited, generic mianserin is usually more affordable in resource-constrained settings, making it a viable alternative in developing countries with limited pharmaceutical budgets.51,52 However, because aplastic anaemia and agranulocytosis have been sometimes (but rarely) reported with mianserin,53 cautious use and complete blood-count monitoring are advised during the first 3 months of treatment. Finally, given the small sample size and single-centre design, these findings should be interpreted as preliminary and hypothesis-generating, reinforcing the trial’s pilot nature; additional research with larger sample sizes is needed to determine the reliability of the current findings.
Data Sharing Statement
De-identified participant data, the data dictionary, and statistical code is available from the corresponding author on reasonable request. Access will begin 6 months after publication and continue for up to 5 years for research consistent with the approved study protocol.
Acknowledgments
We gratefully acknowledge the individuals who were willing to participate in this study. We also thank Ms. Natsupa Wiriyakulsit, Ms. Nattaya Bunwatsana, and Ms.Sunsanee Mali‑ong for their assistance with data collection. We also thank Dr. Chulalak Komoltri and Dr. Orawan Supapueng, Division of Clinical Epidemiology, Department of Research and Development, Faculty of Medicine Siriraj Hospital, for their assistance with the statistical analysis. Finally, we are grateful to Ms. Janravee Laurujisawat for her nursing care and data entry, and for their general support of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Routine to Research Division, Faculty of Medicine Siriraj Hospital, Mahidol University (reference IO R016132038), and by the Chalermprakiat Foundation, Faculty of Medicine Siriraj Hospital, Mahidol University.
Disclosure
All authors declare no personal or professional conflicts of interest related to the topic of this paper. They received no financial support from the companies that produce or distribute the drugs evaluated in this study.
References
1. Last AR, Hulbert K. Chronic low back pain: evaluation and management. Am Fam Physician. 2009;79(12):1067–1074.
2. Nicol V, Verdaguer C, Daste C, et al. Chronic low back pain: a narrative review of recent international guidelines for diagnosis and conservative treatment. J Clin Med. 2023;12(4):1685. doi:10.3390/jcm12041685
3. Ferreira ML, de Luca K, Haile LM. Global, regional, and national burden of low back pain, 1990-2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease study 2021. Lancet Rheumatol. 2023;5(6):e316–e329. doi:10.1016/S2665-9913(23)00098-X
4. Verbunt JA, Smeets RJ, Wittink HM. Cause or effect? Deconditioning and chronic low back pain. Pain. 2010;149(3):428–430. doi:10.1016/j.pain.2010.01.020
5. Urits I, Burshtein A, Sharma M, et al. Low back pain, a comprehensive review: pathophysiology, diagnosis, and treatment. Curr Pain Headache Rep. 2019;23(3):23. doi:10.1007/s11916-019-0757-1
6. Urquhart DM, Wluka AE, van Tulder M, et al. Efficacy of low-dose amitriptyline for chronic low back pain: a randomized clinical trial. JAMA Intern Med. 2018;178(11):1474–1481. doi:10.1001/jamainternmed.2018.4222
7. van den Driest JJ, Bierma-Zeinstra SMA, Bindels PJE, Schiphof D. Amitriptyline for musculoskeletal complaints: a systematic review. Fam Pract. 2017;34(2):138–146. doi:10.1093/fampra/cmw134
8. Gray SL, Anderson ML, Dublin S, et al. Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med. 2015;175(3):401–407. doi:10.1001/jamainternmed.2014.7663
9. Shami M, Elliott HL, Kelman AW, Whiting B. The pharmacokinetics of mianserin. Br J Clin Pharmacol. 1983;15(suppl 2):313S–322S. doi:10.1111/j.1365-2125.1983.tb05880.x
10. Loldrup D, Langemark M, Hansen HJ, Olesen J, Bech P. Clomipramine and mianserin in chronic idiopathic pain syndrome. A placebo-controlled study. Psychopharmacology. 1989;99(1):1–7. doi:10.1007/BF00634443
11. Bravo L, Llorca-Torralba M, Berrocoso E, Micó JA. Monoamines as drug targets in chronic pain: focusing on neuropathic pain. Front Neurosci. 2019;13:1268. doi:10.3389/fnins.2019.01268
12. Wakeling A. Efficacy and side effects of mianserin, a tetracyclic antidepressant. Postgrad Med J. 1983;59(690):229–231. doi:10.1136/pgmj.59.690.229
13. Peet M, Behagel H. Mianserin: a decade of scientific development. Br J Clin Pharmacol. 1978;5(suppl 1):5S–9S. doi:10.1111/j.1365-2125.1978.tb04567.x
14. Marshall RJ. The pharmacology of mianserin—an update. Br J Clin Pharmacol. 1983;15(suppl 2):263S–268S. doi:10.1111/j.1365-2125.1983.tb05874.x
15. Richelson E. Pharmacology of antidepressants—characteristics of the ideal drug. Mayo Clin Proc. 1994;69(11):1069–1081. doi:10.1016/s0025-6196(12)61375-5
16. Tatsumi M, Groshan K, Blakely RD, Richelson E. Pharmacological profile of antidepressants and related compounds at human monoamine transporters. Eur J Pharmacol. 1997;340(2–3):249–258. doi:10.1016/S0014-2999(97)01393-9
17. Royal College of Psychiatrists. Stopping antidepressants. Royal College of Psychiatrists. https://www.rcpsych.ac.uk/mental-health/treatments-and-wellbeing/stopping-antidepressants.
18. National Institute for Health and Care Excellence. NG222: Depression in adults: treatment and management. Published 2022. https://www.nice.org.uk/guidance/ng222
19. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: visual analog scale for Pain (VAS Pain), numeric rating scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res (Hoboken). 2011;63(suppl 11):S240–S252. doi:10.1002/acr.20543
20. Atisook R, Euasobhon P, Saengsanon A, Jensen MP. Validity and utility of four pain intensity measures for use in international research. J Pain Res. 2021;14:1129–1139. doi:10.2147/JPR.S303305
21. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1–2):9–19. doi:10.1016/j.pain.2004.09.012
22. Hjermstad MJ, Fayers PM, Haugen DF, et al. Studies comparing numerical rating scales, verbal rating scales, and visual analogue scales for assessment of pain intensity in adults: a systematic literature review. J Pain Symptom Manage. 2011;41(6):1073–1093. doi:10.1016/j.jpainsymman.2010.08.016
23. Rheker J, Rief W, Doering BK, Winkler A. Assessment of adverse events in clinical drug trials: identifying amitriptyline’s placebo- and baseline-controlled side effects. Exp Clin Psychopharmacol. 2018;26(3):320–326. doi:10.1037/pha0000194
24. Jensen MP, Karoly P. Self-report scales and procedures for assessing pain in adults. In: Turk DC, Melzack R, eds. Handbook of Pain Assessment.
25. Fairbank JC, Pynsent PB. The oswestry disability index. Spine. 2000;25(22):2940–2952. doi:10.1097/00007632-200011150-00017
26. Mehra A, Baker D, Disney S, Pynsent PB. Oswestry Disability Index scoring made easy. Ann R Coll Surg Engl. 2008;90(6):497–499. doi:10.1308/003588408X300984
27. Sakulsriprasert P, Vachalathiti R, Vongsirinavarat M, Kantasorn J. Cross-cultural adaptation of modified Oswestry Low Back Pain Disability Questionnaire to Thai and its reliability. J Med Assoc Thai. 2006;89(10):1694–1701.
28. Sanjaroensuttikul N. The Oswestry low back pain disability questionnaire (version 1.0) Thai version. J Med Assoc Thai. 2007;90(7):1417–1422.
29. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727–1736. doi:10.1007/s11136-011-9903-x
30. Pattanaphesaj J, Thavorncharoensap M, Ramos-Goñi JM, Tongsiri S, Ingsrisawang L, Teerawattananon Y. The EQ-5D-5L Valuation study in Thailand. Expert Rev Pharmacoecon Outcomes Res. 2018;18(5):551–558. doi:10.1080/14737167.2018.1494574
31. Sakthong P, Sonsa-Ardjit N, Sukarnjanaset P, Munpan W. Psychometric properties of the EQ-5D-5L in Thai patients with chronic diseases. Qual Life Res. 2015;24(12):3015–3022. doi:10.1007/s11136-015-1038-z
32. Sonsa-ardjit N, Sakthong P. Reliability and validity of the Thai version of EQ-5D-5L questionnaire on patients with chronic disease. Chula Med J. 2015;59(5):489–501. doi:10.58837/CHULA.CMJ.59.5.2
33. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335–343. doi:10.1016/0005-7967(94)00075-U
34. Oei TP, Sawang S, Goh YW, Mukhtar F. Using the depression anxiety stress scale 21 (DASS-21) across cultures. Int J Psychol. 2013;48(6):1018–1029. doi:10.1080/00207594.2012.755535
35. Lee J, Lee EH, Moon SH. Systematic review of the measurement properties of the Depression Anxiety Stress scales-21 by applying updated COSMIN methodology. Qual Life Res. 2019;28(9):2325–2339. doi:10.1007/s11136-019-02177-x
36. Dwight AR, Briesch AM, Hoffman JA, Rutt C. Systematic review of the psychometric evidence supporting use of the Depression Anxiety Stress scales, Short Form (DASS-21) with youth Child Youth Care Forum. 2024;53(5):1235–1250. doi:10.1007/s10566-024-09795-8
37. Ngamjarus C. n4Studies: sample size calculation for an epidemiological study on a smart device. Siriraj Med J. 2016;68(3):160–170.
38. Dworkin RH, Turk DC, Wyrwich KW, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J Pain. 2008;9(2):105–121. doi:10.1016/j.jpain.2007.09.005
39. Shanthanna H, Joshi GP. Noninferiority trials in acute pain research: a valid approach or a slippery slope? Br J Anaesth. 2024;132(5):1027–1032. doi:10.1016/j.bja.2024.01.019
40. Moore RA, Moore OA, Derry S, Peloso PM, Gammaitoni AR, Wang H. Responder analysis for pain relief and numbers needed to treat in a meta-analysis of etoricoxib osteoarthritis trials: bridging a gap between clinical trials and clinical practice. Ann Rheum Dis. 2010;69(2):374–379. doi:10.1136/ard.2009.107805
41. Thour A, Marwaha RA.Amitriptyline. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537225/?.
42. Pinder RM. Mianserin: pharmacological and clinical correlates. Nord J Psychiatry. 1991;45(sup24):13–26. doi:10.3109/08039489109096678
43. Olianas MC, Dedoni S, Onali P. The atypical antidepressant mianserin exhibits agonist activity at κ-opioid receptors. Br J Pharmacol. 2012;167(6):1329–1341. doi:10.1111/j.1476-5381.2012.02078.x
44. Schreiber S, Backer MM, Kaufman JP, Pick CG. Interaction between the tetracyclic antidepressant mianserin HCl and opioid receptors. Eur Neuropsychopharmacol. 1998;8(4):297–302. doi:10.1016/s0924-977X(97)00088-6
45. Onghena P, De Cuyper H, Van Houdenhove B, Verstraeten D. Mianserin and chronic pain: a double-blind placebo-controlled process and outcome study. Acta Psychiatr Scand. 1993;88(3):198–204. doi:10.1111/j.1600-0447.1993.tb03439.x
46. Lauridsen HH, Hartvigsen J, Manniche C, Korsholm L, Grunnet-Nilsson N. Responsiveness and minimal clinically important difference for pain and disability instruments in low back pain patients. BMC Musculoskeletal Disorders. 2006;7(1):82. doi:10.1186/1471-2474-7-82
47. Siriwardana AN, Hoffman AT, Morton RL, Smyth B, Brown MA. Estimating a Minimal Important Difference for the EQ-5D-5L utility index in dialysis patients. Value Health. 2024;27(4):469–477. doi:10.1016/j.jval.2024.01.011
48. Häuser W, Wolfe F, Tölle T, Üçeyler N, Sommer C. The role of antidepressants in the management of fibromyalgia syndrome: a systematic review and meta-analysis. CNS Drugs. 2012;26(4):297–307. doi:10.2165/11598970-000000000-00000
49. Riediger C, Schuster T, Barlinn K, Maier S, Weitz J, Siepmann T. Adverse effects of antidepressants for chronic pain: a systematic review and meta-analysis. Front Neurol. 2017;8:307. doi:10.3389/fneur.2017.00307
50. Richelson E, Nelson A. Antagonism by antidepressants of neurotransmitter receptors of normal human brain in vitro. J Pharmacol Exp Ther. 1984;230(1):94–102.
51. Srivastava D, McGuire A. Analysis of prices paid by low-income countries - how price sensitive is government demand for medicines? BMC Public Health. 2014;14:767. doi:10.1186/1471-2458-14-767
52. Mulcahy AW, Schwam D, Lovejoy SL. International Prescription Drug Price Comparisons: Estimates Using 2022 data. Rand Health Q. 2024;11(3):5.
53. Adams PC, Robinson A, Reid MM, Vishu MC, Livingston M. Blood dyscrasias and mianserin. Postgrad Med J. 1983;59(687):31–33. doi:10.1136/pgmj.59.687.31
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Qualitative Study of Migraine Headache Experience in Patients with Patent Foramen Ovale Based on the Symptom Management Theory
Li M, Feng M, Li M, Wei J, Li S, Zhang N, Li Q, Song R, Li H
Patient Preference and Adherence 2025, 19:2363-2375
Published Date: 10 August 2025
Discussion on the Application of Mindfulness Therapy in the Treatment of Diabetic Peripheral Neuropathy: A Narrative Review
Fan Q, Yu S, Sun X, Dong Y, Chen Y, Jia L
Psychology Research and Behavior Management 2025, 18:1729-1747
Published Date: 12 August 2025
Comparative Effectiveness of Non-Pharmacological Interventions for Pain and Quality of Life in Women with Endometriosis: A Systematic Review and Network Meta-Analysis
Zheng X, Wang Y, Li H, Zhang J, Liu J, Zheng X, Zhang J, Fan G, Sun Y, Li B, Jiao J, Zuo G, Fan X, She Y
Journal of Pain Research 2026, 19:577080
Published Date: 20 February 2026