Back to Journals » Cancer Management and Research » Volume 17

Clinical Practice and Survival Analysis of Third-Line Therapy in Patients with Metastatic Colorectal Cancer: A Single-Center Retrospective Study
Authors Li Q ![]() , Zhang X, Fan B, Yin H
, Zhang X, Fan B, Yin H ![]() , Jiang B, Xie A, Zhang X, Cui X, Li Y, Dong Y, Li J, Ma L, Sun J, Zhang B
, Jiang B, Xie A, Zhang X, Cui X, Li Y, Dong Y, Li J, Ma L, Sun J, Zhang B
Received 21 July 2025
Accepted for publication 6 December 2025
Published 27 December 2025 Volume 2025:17 Pages 3309—3320
DOI https://doi.org/10.2147/CMAR.S551664
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Yong Teng
Qizheng Li,1,2,* Xia Zhang,1,3,* Buqun Fan,1 Hang Yin,1 Bolun Jiang,1 Anqi Xie,1 Xuebing Zhang,1 Xiaonan Cui,1 Yujun Li,1 Yan Dong,1 Jia Li,1 Lu Ma,4 Jinghua Sun,5 Bin Zhang1
1The First Affiliated Hospital of Dalian Medical University, Dalian, Liaoning Province, People’s Republic of China; 2Department of Oncology, Kunshan Hospital of Traditional Chinese Medicine, Suzhou, Jiangsu Province, People’s Republic of China; 3Department of Science and Technology, Department of Thoracic Medicine, Dalian Fifth People’s Hospital, Dalian, Liaoning Province, People’s Republic of China; 4Dalian Medical University Zhongshan College, Dalian, Liaoning Province, People’s Republic of China; 5Department of Digestive Oncology, The Second Affiliated Hospital of Dalian Medical University, Dalian, Liaoning Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Zhang; Jinghua Sun, Email [email protected]; [email protected]
Background: The effectiveness of third - line treatment for metastatic colorectal cancer (mCRC) still needs enhancing. In real-world clinical practice, third-line treatment options are complex and varied. However, real-world data on third-line treatment for mCRC remains limited. Further investigation is needed into treatment patterns, the efficacy of different regimens, and their influencing factors.
Methods: This study retrospectively analyzed 229 mCRC patients receiving third-line therapy (2013– 2023). Kaplan-Meier method was used to draw the overall survival (OS) and progression-free survival (PFS) curves. With the chemotherapy group serving as the control group, the efficacy differences between third-line regimens were compared using the Log rank test. Univariate analysis was first conducted to evaluate prognostic factors, the indicators with statistical significance were analyzed by multivariate analysis using the Cox proportional hazards model.
Results: Fruquintinib plus immunotherapy achieved a median PFS of 8.8 months (95% CI: 8.6– 9.0), which was significantly longer than the 3.6 months (95% CI: 3.1– 4.1) in the chemotherapy group (p = 0.034). All 229 patients had proficient mismatch repair(pMMR) tumors or genetic testing suggestive of MSI-L/microsatellite stability(MSS). The third-line median PFS in the setting was 3.8 months, and the median OS was 13.3 months. Univariate analysis identified metastasis local treatment, RAS/BRAF mutation status, metastasis-to-PD2(defined as the second progression following first-line treatment initiation) interval, baseline CEA, and baseline CA199 as significant prognostic factors. Multivariate analysis confirmed metastasis-to-PD2 interval and baseline CA199 as independent prognostic indicators.
Conclusion: In the real-world setting, fruquintinib combined with immunotherapy was associated with benefits in third-line treatment of patients with pMMR mCRC. Shorter metastasis-to-PD2 interval and elevated baseline CA19-9 levels at the start of third-line therapy were independent poor prognostic factors.
Keywords: colorectal cancer, third-line therapy, real-world, fruquintinib, immune checkpoint inhibitors
Introduction
Data from GLOBOCAN 2020 show that colorectal cancer (CRC) has the third-highest incidence and second-highest lethality of all malignant tumours worldwide.1 In China, colorectal cancer has the third-highest incidence of malignant tumours and the fifth-highest mortality rate.2 More than 60% of patients with metastatic colorectal cancer (mCRC) receive third-line treatment after disease progression on second-line therapy.3 Immune checkpoint inhibitor therapy can be tried in patients with microsatellite instability-high/mismatch repair-deficient (MSI-H/dMMR) tumors, however, such patients represent only about 5% of the mCRC population. For the vast majority of mCRC patients, regorafenib, fruquintinib, and trifluridine/tipiracil (TAS-102) have been approved for third-line standard treatment, and third-line regimens of cetuximab ± irinotecan are also available for non-MSI-H/dMMR patients with RAS/BRAF wild-type,4 which have all shown limited benefit, although they have ameliorated the dilemma of third-line treatment of mCRC to some extent, with median OS for standard regimens ranging only from 6.4 to 9.3 months.5–9 Data are also limited regarding how the time to disease progression after first-line therapy influences outcomes in the third-line setting.
In actual clinical practice, patient management is influenced by a complex mix of factors including actual disease condition, financial status, and treatment preferences. In China, for instance, third-line treatment choices are heavily affected by drug accessibility, regional diagnostic and therapeutic preferences, as well as the financial burden of novel targeted agents such as fruquintinib. These factors result in treatment patterns that are more complex and diverse than those recommended by guidelines——such as the reintroduction/rechallenge of chemotherapeutic agents and/or targeted agents, targeted therapy ± immunotherapy, targeted combination therapy, and other kinds of combination regimens. However, data on combination regimens (eg, targeted therapy + immunotherapy) in non-MSI-H/dMMR populations remain scarce. The efficacy and side effects of these regimens also need to be further explored.
Real World Study (RWS) is a patient-centered clinical study based on actual clinical settings, which can better evaluate the treatment effects of individual patients in the clinic than RCT studies. However, there are few real-world reports on third-line treatment, further investigation is required into the treatment patterns, the differences in efficacy and side effects among various treatment regimens, as well as the factors influencing the prognosis of the third-line mCRC in the real world. Based on this, we conducted a real-world study of 229 patients with advanced metastatic colorectal cancer who received third-line treatment in the Affiliated Hospital of Dalian Medical University to assess the efficacy and safety of different third-line treatment regimens and analyse potential prognostic influencing factors, which will provide a reference for clinical treatment choices and the design of prospective clinical studies for third-line treatment of mCRC patients.This study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Dalian Medical University, and informed consent was obtained from all the study participants prior to study commencement.
Methods
Ethics
This study complies with the Declaration of Helsinki and was approved by the Medical Ethics Committee of the First Affiliated Hospital of Dalian Medical University, and informed consent was obtained from all the study participants prior to study commencement.
Patient Screening
The medical information, case records, and follow-up data of mCRC patients who visited the Affiliated Hospital of Dalian Medical University for third-line treatment from August 2013 to August 2023 were collected for a retrospective study. Patients who met the following criteria were included in the study: histologically or pathologically confirmed colorectal cancer patients; with definite distant metastasis confirmed by imaging, staged as IV; having undergone at least second-line treatment and failed; having at least more than one measurable metastatic lesion (with a longest diameter of at least 10mm for tumor lesions by CT or MRI, and a short-axis diameter of at least 15mm for lymph nodes); aged between 18 and 85 years. Participants were excluded if they had coexisting other cancers, unclear records of specific treatment regimens or medications for each line of treatment, unclear records of the start time of third-line treatment and the time of treatment failure (disease progression or death) with no possibility for follow-up, or if they had irregular treatment adherence.
Data Collection and Follow-up methods
Patients’ history and clinical information and data were followed up using our electronic medical record system screening and review, and telephone follow-up. When calculating third-line progression-free survival(PFS), data with poorly documented progress, if any, were calculated at the time of the last follow-up visit or the date of the remaining intervention (eg, surgery), as appropriate, and labelled as truncated. When calculating third-line overall survival (OS), if there are data from patients who are lost to follow-up during the follow-up period, the time of the last follow-up visit was taken for calculation and defined as truncated. The follow-up period was from the start of third-line treatment until 31 December 2023.
Grouping
The included patients were grouped according to their actual medication use while receiving third-line therapy, including chemotherapy (including chemotherapy alone and chemotherapy combined with cetuximab/bevacizumab targeted therapy), regorafenib monotherapy, fruquintinib monotherapy, TAS-102 monotherapy, chemotherapy combined with immunotherapy, apatinib, regorafenib combined with chemotherapy, regorafenib combined with immunotherapy, fruquintinib combined with chemotherapy, fruquintinib combined with immunotherapy, TAS-102 combined with cetuximab/bevacizumab, TAS-102 combined with fruquintinib, anlotinib, cetuximab monotherapy, cetuximab combined with vemurafenib, TAS-102 combined with chemotherapy, TAS-102 combined with regorafenib, and TAS-102 combined with immunotherapy. Chemotherapy included oxaliplatin-based regimens, irinotecan-based regimens, FOLFOXIRI, capecitabine monotherapy, raltitrexed monotherapy, and S-1 monotherapy, immunotherapy included various immune checkpoint inhibitors.
Study Endpoint
The primary study endpoint was third-line PFS, defined as the time from the start of third-line treatment to disease progression or death. The secondary study endpoint was third-line OS, defined as the time from the start of third-line treatment to death.
Criteria for Evaluating Efficacy
The treatment effect of mCRC patients was evaluated according to the RECIST 1.1 evaluation criteria, which were referred to when patients were evaluated for efficacy after each follow-up CT.
Statistical Processing
The data were statistically analysed using SPSS 25 software. Kaplan-Meier curves were used to plot the third-line OS and third-line PFS survival curves. The chemotherapy group was set as the control group, and the differences in the effects of different third-line treatment regimens on third-line OS and PFS were compared using the Log rank test. Univariate analysis of the factors influencing the prognosis and outcome of patients with metastatic colorectal cancer was performed, with variables including gender, whether the age was greater than 65 years, smoking history, primary tumour status (resected or not), location of the primary tumour (right half of the colon/left half of the colon/rectum), whether an intestinal ostomy was performed, number of metastatic sites, whether local treatment of metastasis was performed (including surgery, radiotherapy, or interventional therapy targeting metastatic lesions during the disease course), mutation status (RAS or BRAF mutant/wild-type), time from metastasis diagnosis to PD2 (defined as the second progression following first-line treatment initiation), baseline CEA (at start of third-line treatment), baseline CA199 (at start of third-line treatment), and whether bowel obstruction occurred. Indicators statistically significant on univariate analysis were analysed multivariate using Cox proportional-hazards model. Hazard ratios (HR) and corresponding 95% confidence intervals (CI) were also calculated. All statistical tests were performed with P < 0.05 as the difference was statistically significant.
Result
Clinical Characteristics and Treatment Options for Third-Line Patients
The study finally included 229 patients with mCRC, of whom 136 were male and 93 were female; their ages ranged from 24 to 85 years old, with a median age of 63 years old; 177 patients (77.3%) had undergone previous surgical resection of the primary focus; 93 patients (40.6%) had undergone local treatment of metastasis (including surgery, radiotherapy or interventional therapy); and 91 (39.7%) patients had genetic testing results that suggested a RAS/BRAF wild-type, 128 (55.9%) were RAS/BRAF mutant, and 10 (4.4%) were unknown. 229 (100%) patients had proficient mismatch repair(pMMR) tumors or genetic testing suggestive of MSI-L/microsatellite stability(MSS). The remaining clinical characteristics of the third-line patients are detailed in Table 1. In terms of treatment selection, 37.12% (85 patients) still chose chemotherapy alone or chemotherapy combined with cetuximab/bevacizumab targeted therapy; and among the guideline-recommended standard treatments (regorafenib monotherapy, fruquintinib monotherapy, or TAS-102 monotherapy), a total of 33 patients with mCRC using fruquintinib monotherapy accounted for the highest percentage. Among the 85 patients in the chemotherapy group, the specific treatment regimens have been detailed as follows: 19 patients received oxaliplatin-based regimens, 43 received irinotecan-based regimens, 2 received FOLFOXIRI, and the remaining patients were treated with regimens not based on oxaliplatin or irinotecan—specifically, 11 received S-1 monotherapy, 7 received raltitrexed monotherapy, and 3 received capecitabine monotherapy. Additionally, 48 patients in the chemotherapy group received chemotherapy combined with cetuximab/bevacizumab. The remaining treatment choices and percentages of the third-line patients are detailed in Table 2.
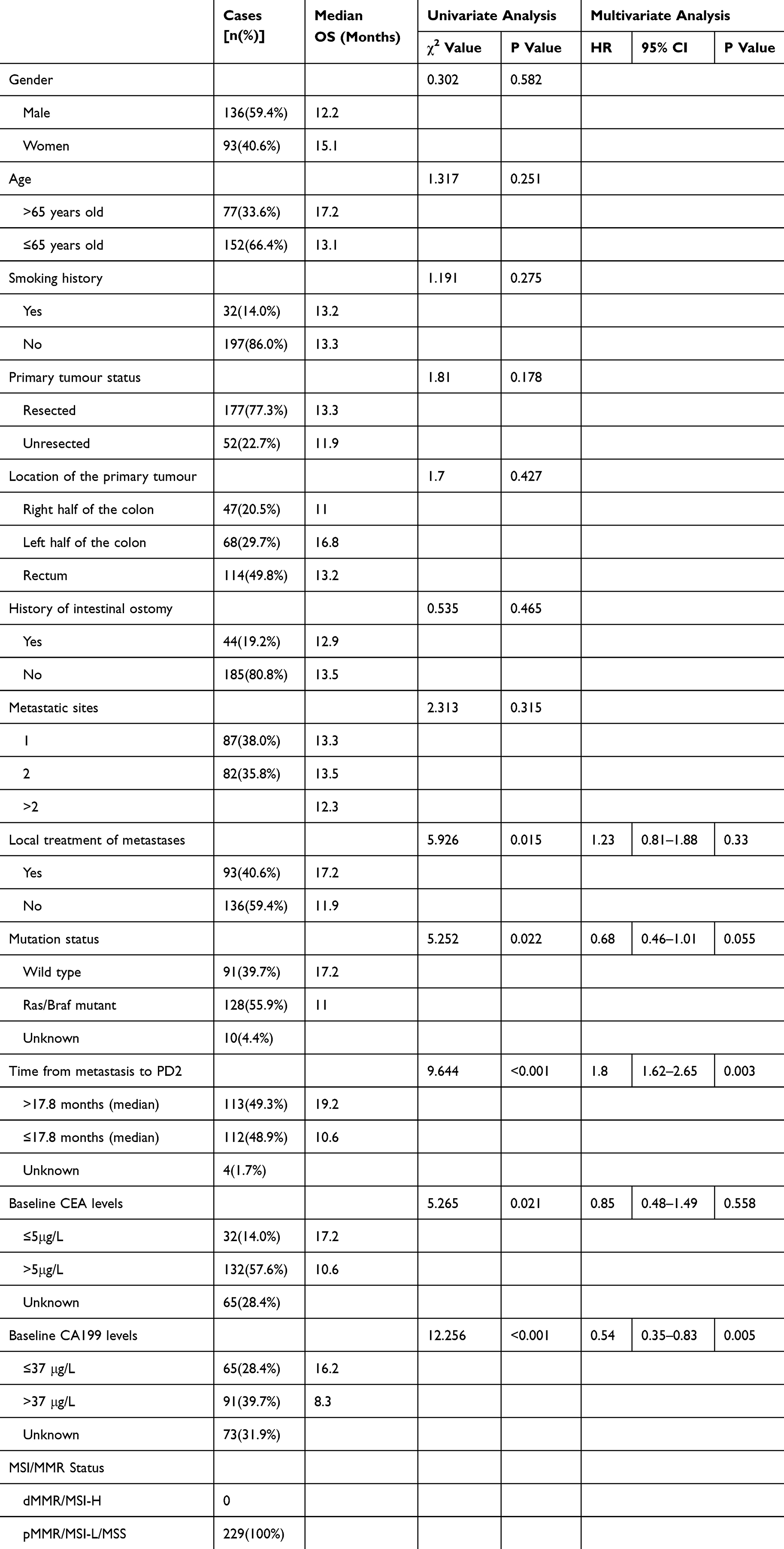 |
Table 1 Baseline Clinical Characteristics of 229 Patients and the Effect of Different Clinical Characteristics on Third-Line Survival |
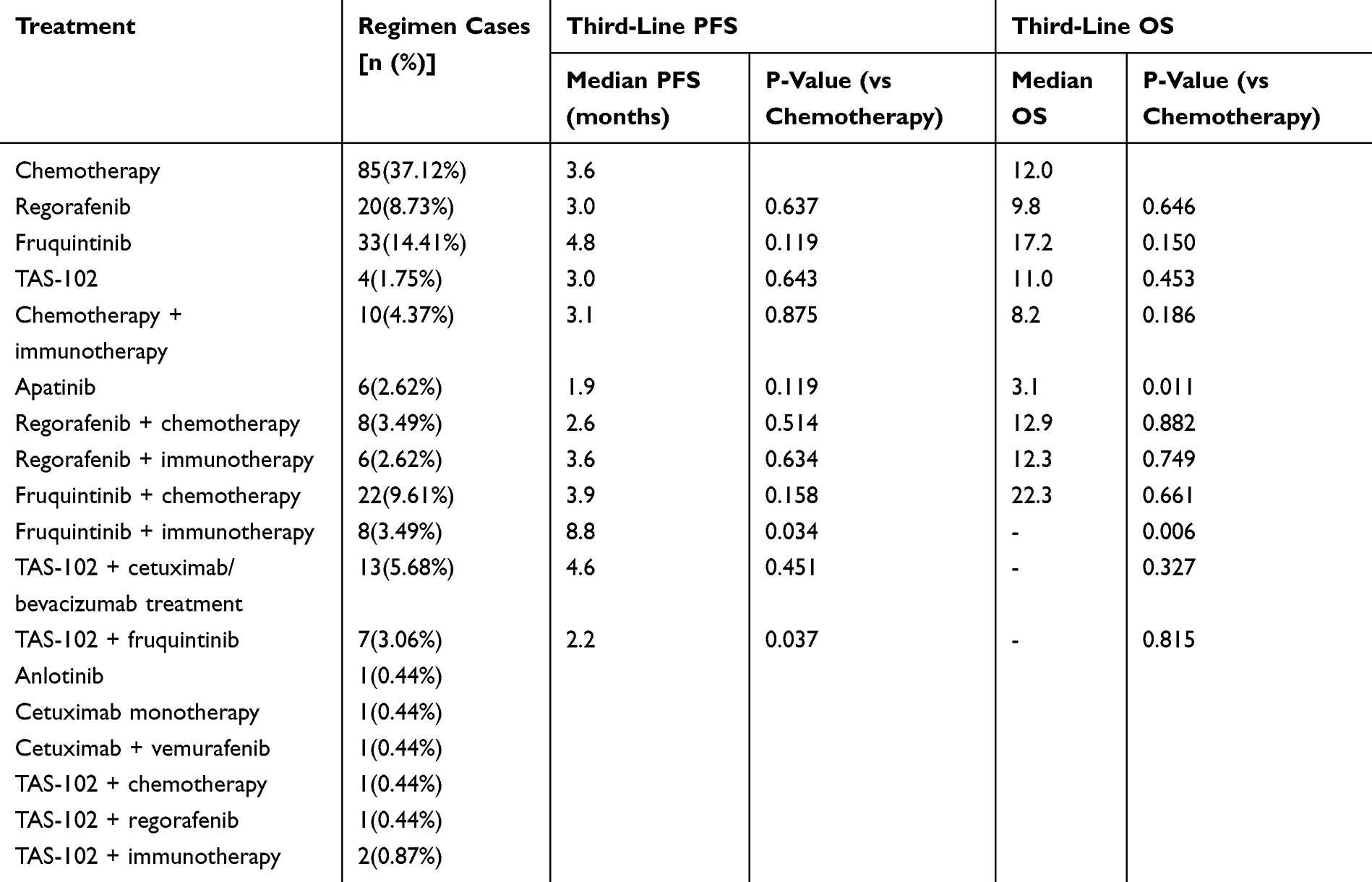 |
Table 2 Composition of Various Regimens in the Third Line of Treatment and the Efficacy of Each Regimen in Comparison to the Chemotherapy Group |
Comparison of Efficacy Among Different Third-Line Treatment Regimens
General
A total of 229 patients were enrolled in this study; by the end of follow-up, 75 patients survived, 3 were lost to follow-up, and 151 died. The third-line median PFS was 3.8 months (3.4–4.2 months); the third-line median OS was 13.3 months (9.7–16.9 months); the median follow-up time for third-line treatment was 22.7 months; and the one-year survival rate was 53.7%.
Comparison of the Primary Endpoint, Third-Line PFS
The grouping was based on the actual third-line treatment regimens of 229 patients, which included 18 treatment regimens, of which anlotinib, cetuximab monotherapy, cetuximab combined with vemurafenib, TAS-102 combined with chemotherapy, TAS-102 combined with regorafenib, and TAS-102 combined with immunotherapy were excluded from the analysis due to the small number of cases enrolled, which was not statistically significant.
A total of 12 groups of patients were finally included in the analysis, namely the chemotherapy group (including chemotherapy alone and chemotherapy combined with cetuximab/bevacizumab targeted therapy), the regorafenib monotherapy group, the fruquintinib monotherapy group, the TAS-102 monotherapy group, the chemotherapy combined with immunotherapy group, the apatinib group, the regorafenib combined with chemotherapy group, the regorafenib combined with immunotherapy group, the fruquintinib combined with chemotherapy group, the fruquintinib combined with immunotherapy group, TAS-102 combined targeted therapy group, and TAS-102 combined fruquintinib group. Since most of the control groups in previous RCT studies were placebo groups, the chemotherapy group was set as the control group in this study for the sake of clear demonstration.
Kaplan-Meier survival analysis was applied to draw the third-line PFS survival curves and Log rank test was used to compare the groups (Figure 1), which showed that in third-line treatment, the median third-line PFS of the fruquintinib combined with immunotherapy group was 8.8 months (95% CI: 8.6–9.0), which was better than that of the chemotherapy group (3.6 months, 95% CI: 3.1–4.1), with a statistically significant difference (p=0.034); the median PFS in the TAS-102 combined with fruquintinib group was 2.2 months (95% CI: 0.1–4.3), lower than that in the chemotherapy group, with a statistically significant difference (p=0.037), and not statistically different from the median PFS of the TAS-102 monotherapy group (3.0 months, 95% CI: 0.6–5.5) (p=0.268). There was no statistically significant difference in the third-line PFS of the remaining groups compared to the chemotherapy group (Table 2).
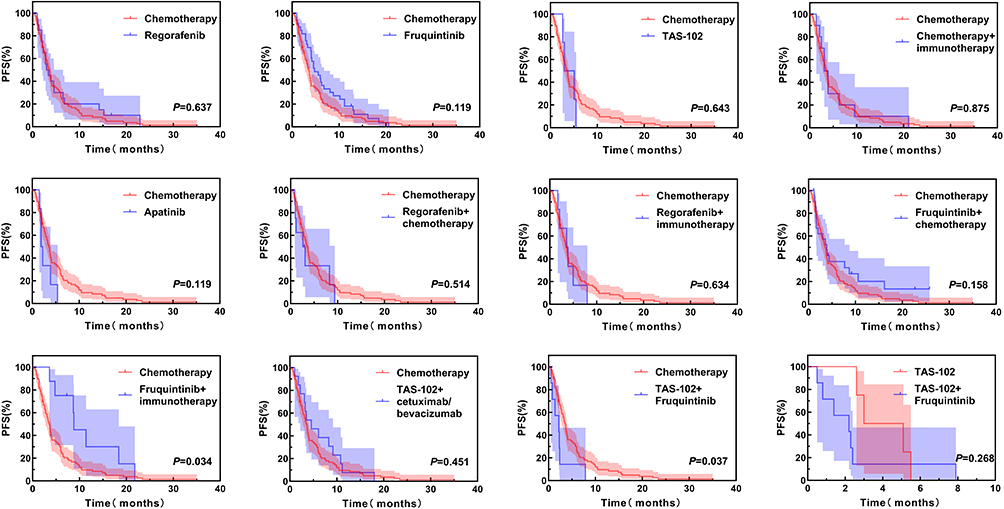 |
Figure 1 Comparison of different regimens for third-line PFS. |
Further subgroup analysis of the chemotherapy group showed that there was no statistically significant difference in median PFS between the chemotherapy-alone group (37 patients) and the chemotherapy combined with cetuximab/bevacizumab targeted therapy group (48 patients) (3.3 months [95% CI: 2.2–4.4] vs 3.7 months [95% CI: 3.1–4.3], p=0.697).
Comparison of the Secondary Endpoint, Third-Line OS
Kaplan-Meier survival analysis was applied to plot the third-line OS survival curves and the Log rank test was used to compare the groups (Figure 2), the Log rank test showed that the third-line OS of the fruquintinib combination immunotherapy group was significantly better than that of the chemotherapy group (p=0.006), as 87.5% of the patients in the fruquintinib combination immunotherapy group were still alive by the follow-up cut-off date, the median OS was not reached, further comparison with the chemotherapy group showed a 1-year survival rate of 83.3% vs 49.3%, and the mean three-line OS was 39.2 months (95% CI: 29.5–49.0) vs 18.3 months (95% CI: 14.3–22.3). The median OS of the apatinib group was 3.1 months (95% CI: 0.8–5.4 months), significantly lower than 12.0 months in the chemotherapy group (95% CI: 7.7–16.3, p=0.011). There was no statistically significant difference in third-line OS in the remaining groups compared to the chemotherapy group (Table 2).
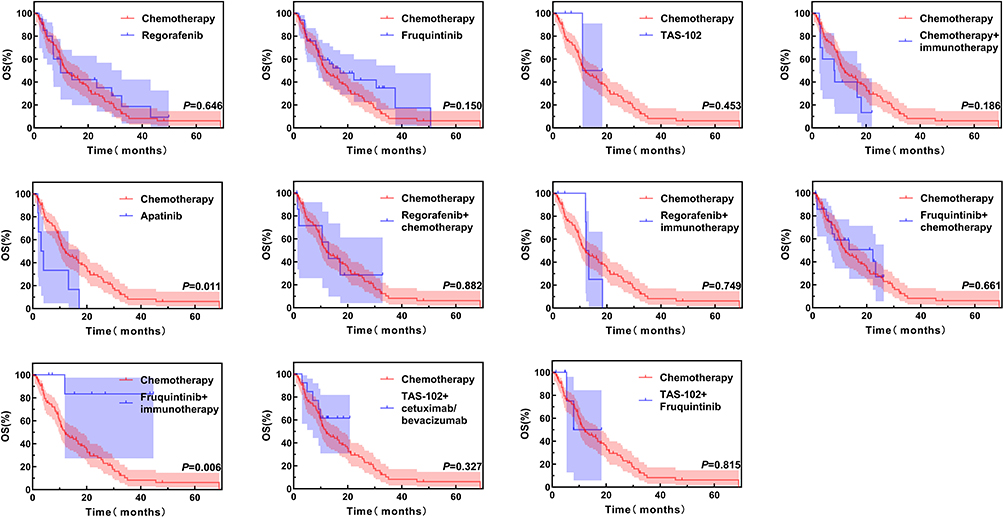 |
Figure 2 Comparison of different regimens for third-line OS. |
Impact of Different Clinical Characteristics on Survival in Third-Line Patients
Results of Univariate Analyses
Where the cut-off value for time from metastasis diagnosis to PD2 was set as the median value of the data set ie 17.8 months. Baseline CEA was defined as the CEA level at the start of third-line treatment, with serum CEA >5 μg/L as a positive criterion; baseline CA199 was defined as the CA199 level at the start of third-line treatment, with serum CA199 >37 μg/L as a positive criterion. Some cases with no information such as unknown mutation status (10 cases), unknown time from metastasis diagnosis to PD2 (4 cases), and no data on baseline CEA (65 cases) or baseline CA199 (73 cases) were excluded from the analysis.
The univariate analysis showed that factors such as whether local treatment of metastasis was performed (including surgery, radiotherapy, or interventional therapy),mutation status (RAS or BRAF mutant/wild-type), time from metastasis diagnosis to PD2, baseline CEA, and baseline CA199 were statistically significant (Table 1).
Results of Multivariate Analysis
The application of Cox regression analysis to multifactorial analysis of the clinical factors that were statistically significant in the above univariate analyses showed that time from metastasis diagnosis to PD2 and baseline CA199 were independent prognostic influences in patients with third-line mCRC (Table 1).
Discussion
Treatment options for advanced colorectal cancer in the real world are complex and varied, and for patients progressing to third-line therapy, in addition to the guideline-recommended standard third-line agents (regorafenib, fruquintinib, and TAS-102), options also include chemotherapy, targeted therapy, immunotherapy, and a variety of combination regimens. In real-life clinical practice, although most patients entering third-line therapy have already received oxaliplatin- or irinotecan-based chemotherapy, premature use of targeted therapies such as fruquintinib or regorafenib is not always preferred in patients with better physical status, and some physicians still try third-line chemotherapy. Some small-sample studies have shown that third-line chemotherapy rechallenge can provide therapeutic benefits for third-line patients.10–13 In this study, 229 mCRC patients were grouped according to their actual third-line treatment regimens, with 37.1% of patients choosing chemotherapy or chemotherapy combined with targeted therapy, the highest percentage. This is similar to a real-world study from Australia in which chemotherapy containing oxaliplatin or irinotecan had the highest percentage of third-line treatment for mCRC,14 suggesting that conventional chemotherapy continues to be an important part of third-line treatment for mCRC. This may be due, on the one hand, to the fact that some patients show better efficacy with front-line chemotherapy and therefore prefer chemotherapy as a third-line regimen; on the other hand, from a pharmacoeconomic point of view, many patients are unable to afford the newer third-line drugs such as regorafenib, thus making chemotherapy a more suitable choice.
As third-line standard agents, regorafenib, fruquintinib, and TAS-102 all have RCTs confirming their efficacy. Regorafenib, the first small molecule multi-kinase inhibitor approved for third-line treatment of mCRC, demonstrated significant improvement in median overall survival (mOS) compared to placebo (6.4 months vs 5.0 months, p=0.0052) with a favourable safety profile in the CORRECT trial.5 The CONCUR study further revealed that regorafenib showed superior efficacy in Asian-Pacific patients with advanced CRC compared to Western populations: the regorafenib group achieved a median progression-free survival (mPFS) of 3.2 months versus 1.7 months in the placebo group (P<0.001), and a mOS of 8.8 months versus 6.3 months (P<0.001).6 The FRESCO trial, evaluating fruquintinib in 416 third-line mCRC patients, reported a primary endpoint mOS of 9.30 months in the fruquintinib group versus 6.57 months in the placebo group, the secondary endpoint mPFS was 3.71 months (95% CI: 3.65–4.63) versus 1.84 months (95% CI: 1.81–1.84).7 For TAS-102, the global Phase III RECOURSE trial demonstrated that it extended mOS by 1.8 months (7.1 vs 5.3 months, P<0.001) and mPFS by 0.3 months (2.0 vs 1.7 months, P<0.001) compared to placebo in refractory mCRC patients resistant to standard second-line therapy, regardless of age, geographic origin, or KRAS status.8 The TERRA study focusing on Asian refractory mCRC patients showed mOS of 7.8 months versus 7.1 months (p=0.035) and mPFS of 2.0 months versus 1.8 months (P<0.001) for TAS-102 versus placebo, respectively.9 In our study, the overall third-line median PFS and median OS of the 229 patients were 3.8 months and 13.3 months, respectively, which are longer than the data from the aforementioned RCTs. Although potential biases inherent to a single-center study cannot be ruled out, our data may still provide a more realistic reference for survival expectations in the current real-world third-line treatment setting.
While these RCTs confirm that regorafenib, fruquintinib, and TAS-102 significantly improve PFS or OS compared to placebo, how efficacious they were in comparison to conventional chemotherapy needs to be further explored. Köstek et al found that regorafenib was inferior to rechallenge chemotherapy in third-line treatment (median OS: 6.6 vs 12.0 months, P<0.001).13 In our study, the chemotherapy group served as the control group to compare the efficacy of different treatment regimens. The result of our study showed that the three standard third-line agents brought considerable OS and PFS benefits, but none of them outperformed conventional chemotherapy in improving PFS or OS, which suggests that the third-line treatment options for mCRC still need to be further explored and optimised, and that multi-agent combinations may be more effective than single-agent treatments should be taken into account when designing future treatment strategies.
Immune checkpoint inhibitors have demonstrated significant anti-tumour effects in the treatment of a wide range of tumours; however, in the treatment of mCRC, their effectiveness has been largely limited to the patient population with MSI-H/dMMR. The FDA has approved nivolumab alone or in combination with ipilimumab as a later-line treatment for dMMR/MSI-H mCRC, but immunotherapy alone remains of limited efficacy in the non-dMMR/MSI-H population.15 However, progress has been made in several studies exploring immunotherapy in non-dMMR/MSI-H settings. Research from trials such as UNION, TORCH, and STELLARII has shown that short-course hypofractionated radiotherapy combined with chemotherapy and immunotherapy can improve the tumor complete response rate in patients with pMMR and/or MSS locally advanced rectal cancer (LARC).16–18 The Phase II NICHE study evaluated the efficacy and safety of immune checkpoint blockade (ICB) (nivolumab plus ipilimumab) as neoadjuvant therapy in 31 patients with early-stage pMMR colon cancer. The study found that neoadjuvant ICB was effective in some patients, with an overall pathological response rate of 26%.19 In our study, although all 229 included patients were of the pMMR/MSI-L/MSS type, 11.35% of third-line regimens still incorporated immunotherapy, reflecting clinicians’ attempts to combine it with other antineoplastic agents. Given the limited population benefiting from immunotherapy in colorectal cancer, future studies should focus on improving efficacy through combinations with other therapies (eg, targeted agents, chemotherapy, radiotherapy) and identifying predictive biomarkers, particularly for non-MSI-H/dMMR patients.
Combination therapy may enhance antitumor efficacy; for instance, the combination of targeted and immunotherapy has been shown to promote tumor-infiltrating CD8+ T lymphocytes and potentiate cancer immunotherapy when anti-angiogenic therapy is administered at appropriate doses.20 Given the limited efficacy of the current standard third-line treatment, the medical community has been prompted to actively explore various modes of combination therapy, and in this context, the Japanese REGONIVO study has attracted widespread attention, which is the first study to use a targeted therapy combined with immunotherapy regimen for refractory MSS-type mCRC. By treating CRC patients with a regimen of nivolumab in combination with regorafenib, the study observed an ORR of 36% with a median PFS of 7.9 months, a 1-year PFS of 41.8%, and a 1-year OS of 68.0%.21 Unfortunately, however, the results of the REGONIVO phase II study conducted in North America failed to replicate the stunning data from the Japanese population. Similar explorations include the phase Ib/II study of fruquintinib in combination with sintilimab for the treatment of metastatic colorectal cancer of the MSS/pMMR type, in which an ORR of 20%, a 100% disease control rate (DCR), a mPFS of 6.9 months, and a median overall survival (mOS) of 20.0 months were observed.22 Results from an open-label, single-arm, phase I/II study (APOLLON) showed that the combination of TAS-102 and panitumumab for the treatment of patients with RAS wild-type metastatic colorectal cancer resulted in a median PFS and OS of 5.8 months (95% CI 4.5–6.5) and 14.1 months (95% CI 12.2–19.3), respectively.23 Several studies have also been conducted to compare and evaluate the efficacy and safety of TAS-102 in combination with bevacizumab for the treatment of refractory mCRC. Results from C-TASK FORCE, an investigator-initiated, open-label, single-arm, multicentre, Phase 1/2 trial of TAS-102 plus bevacizumab from Japan, showed that the combination of TAS-102 with bevacizumab resulted in an mPFS of 5.6 months (95% CI:3.4–7.6) in patients with metastatic colorectal cancer who were refractory to or intolerant of standard chemotherapy.24 A Danish open-label, randomised, Phase 2 study comparing the efficacy of treatment with TAS-102 monotherapy regimen and TAS-102 in combination with bevacizumab in patients undergoing refractory therapy for metastatic colorectal cancer showed that TAS-102 in combination with bevacizumab yielded a mOS of 9.4 months and an mPFS of 4.6 months, compared to an mOS of 6.7 months and an mPFS of 2.6 months in patients treated with TAS-102 monotherapy.25 The TAS-CC3 study, a prospective, non-randomised, single-arm, multicentre, open-label Phase II trial of TAS-102 plus bevacizumab as a third-line treatment for patients with metastatic CRC resulted in an mPFS of 4.5 months (95% CI 1.8–7.1) and a median OS of 9.2 months (95% CI 5.5–12.8).26 Our study suggests that fruquintinib combined with immunotherapy may be a promising regimen, significantly improving third-line PFS and OS compared to chemotherapy, but TAS-102 combined with fruquintinib did not improve third-line PFS compared with chemotherapy and TAS-102 monotherapy. It should be noted that the current fruquintinib combined with immunotherapy group has a relatively small sample size. We look forward to including more cases in the future to further validate the efficacy of this treatment regimen.
Multivariable analysis in this study showed that baseline CA199 and time from metastasis diagnosis to PD2 were independent prognostic factors in third-line mCRC patients.CA199, as a tumour marker, plays an important role in the prognostic assessment and diagnosis of colorectal cancer. Liu et al demonstrated that elevated preoperative CA199 levels were associated with poor long-term prognosis and shorter postoperative recurrence time in colorectal cancer patients, indicating its independent prognostic value for disease progression.27 In addition, Dong et al reported that high levels of CA199 are strongly associated with liver metastases in colorectal cancer.28 Although CA199 has limited sensitivity and specificity in early diagnosis, its diagnostic efficacy can be significantly improved when used in combination with other tumour markers, such as CEA.Zhang et al demonstrated that the diagnostic sensitivity and specificity for colorectal cancer were increased to 85.86% and 96.78%, respectively, when CEA was combined with CA199.29 Our study suggests that CA199 is an independent prognostic factor in third-line mCRC patients. With regard to the impact of time from metastasis diagnosis to PD2 on third-line OS, a shorter metastasis-to-PD2 interval, indicating shorter PFS during both first- and second-line therapies, may be associated with more aggressive tumor biology or lower sensitivity to prior antitumor treatments. Our findings are consistent with previous reports30,31 that the rate of tumour progression and the duration of first- and second-line therapy are important factors affecting survival in patients with metastatic colorectal cancer who have received a large number of treatments.
This study has several limitations. As a single-center study with long enrollment duration and multiple groups, some groups (such as fruquintinib plus immunotherapy) had small patient numbers. Additionally, the complexity of third-line treatment and challenges in follow-up led to incomplete data collection. These factors may introduce bias into the conclusions. Future real-world studies with larger sample sizes are needed to further investigate different third-line regimens for mCRC.
Conclusion
In patients with pMMR mCRC, the regimen of fruquintinib combined with immunotherapy was associated with benefit in a real-world third-line setting, whereas the combination of TAS-102 and fruquintinib did not improve third-line PFS. The interval from metastasis diagnosis to PD2 (the second progression following first-line treatment initiation) and baseline CA19-9 level at the start of third-line therapy are independent prognostic factors in third-line mCRC patients. These factors may help stratify patients for more individualized third-line treatment—shorter PD2 interval or elevated CA19-9 may indicate the need for more aggressive therapeutic strategies. These findings require further validation in future large-scale, multi-center studies.
Ethics Statement
This study complies with the Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital of Dalian Medical University (approval number: PJ-KS-KY-2024-144).
Acknowledgments
This work was supported by: Dalian Municipal Science and Technology Bureau Life and Health Guidance Program (0122023103); Hubei Chen Xiaoping Science and Technology Development Foundation Youth Science Special Fund (CXPJJH124001-2488); Beijing Medical and Healthcare Public Welfare Foundation Project (YWJKJJHKYJJ-B01-N24001); Liaoning Provincial Department of Education Basic Research Projects for Colleges and Universities (JYTMS20230599).
Author Contributions
Qizheng Li,first author; Xia Zhang, co-first author. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Zeng H, Chen W, Zheng R, et al. Changing cancer survival in China during 2003-15: a pooled analysis of 17 population-based cancer registries. Lancet Glob Health. 2018;6(5):e555–e567.
3. Tampellini M, Di Maio M, Baratelli C, et al. Treatment of Patients With Metastatic Colorectal Cancer in a Real-World Scenario: probability of Receiving Second and Further Lines of Therapy and Description of Clinical Benefit. Clin Colorectal Cancer. 2017;16(4):372–376. doi:10.1016/j.clcc.2017.03.019
4. Gebbia V, Del PS, Borsellino N, et al. Efficacy and safety of cetuximab/irinotecan in chemotherapy-refractory metastatic colorectal adenocarcinomas: a clinical practice setting, multicenter experience. Clin Colorectal Cancer. 2006;5(6):422–428. doi:10.3816/CCC.2006.n.013
5. Grothey A, Van Cutsem E, Sobrero A, et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, Phase 3 trial. Lancet. 2013;381(9863):303–312. doi:10.1016/S0140-6736(12)61900-X
6. Li J, Qin S, Xu R, et al. Regorafenib plus best supportive care versus placebo plus best supportive care in Asian patients with previously treated metastatic colorectal cancer (CONCUR): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2015;16(6):619–629. doi:10.1016/S1470-2045(15)70156-7
7. Li J, Qin S, Xu RH, et al. Effect of Fruquintinib vs Placebo on Overall Survival in Patients With Previously Treated Metastatic Colorectal Cancer: the FRESCO Randomized Clinical Trial. JAMA. 2018;319(24):2486–2496. doi:10.1001/jama.2018.7855
8. Mayer RJ, Van Cutsem E, Falcone A, et al. Randomized trial of Tas-102 for refractory metastatic colorectal cancer. N Engl J Med. 2015;372(20):1909–1919. doi:10.1056/NEJMoa1414325
9. Xu J, Kim TW, Shen L, et al. Results of a Randomised, Double-Blind, Placebo-Controlled, Phase III Trial of Trifluridine/Tipiracil (Tas-102) Monotherapy in Asian Patients With Previously Treated Metastatic Colorectal Cancer: the TERRA Study. j Clin Oncol. 2018;36(4):350–358. doi:10.1200/JCO.2017.74.3245
10. Chambers AE, Frick J, Tanner N, et al. Chemotherapy re-challenge response rate in metastatic colorectal cancer. J Gastrointest Oncol. 2018;9(4):679–686. doi:10.21037/jgo.2018.04.08
11. Suenaga M, Mizunuma N, Matsusaka S, et al. Phase II study of reintroduction of oxaliplatin for advanced colorectal cancer in patients previously treated with oxaliplatin and irinotecan: RE-OPEN study. Drug Des Devel Ther. 2015;9:3099–3108. doi:10.2147/DDDT.S85567
12. Amatu A, Mauri G, Tosi F, et al. Efficacy of Retreatment with Oxaliplatin-Based Regimens in Metastatic Colorectal Cancer Patients: the RETROX-CRC Retrospective Study. Cancers (Basel). 2022;14(5):1197. doi:10.3390/cancers14051197
13. Köstek O, Hacıoğlu MB, Sakin A, et al. Regorafenib or rechallenge chemotherapy: which is more effective in the third-line treatment of metastatic colorectal cancer? Cancer Chemother Pharmacol. 2019;83(1):115–122. doi:10.1007/s00280-018-3713-6
14. Min ST, Roohullah A, Tognela A, et al. Patient demographics and management landscape of metastatic colorectal cancer in the third-line setting: real- world data in an australian population. Asia Pac J Clin Oncol. 2022;18(2):e56–e63. doi:10.1111/ajco.13553
15. Chalabi M, Fanchi LF, Dijkstra KK, et al. Neoadjuvant immunotherapy leads to pathological responses in MMR-proficient and MMR-deficient early-stage colon cancers. Nat Med. 2020;26(4):566–576. doi:10.1038/s41591-020-0805-8
16. Xia F, Wang Y, Wang H, et al. Randomized phase II trial of immunotherapy⁃based total neoadjuvant therapy for proficient mismatch repair or microsatellite stable locally advanced rectal cancer (TORCH)[J]. J Clin Oncol. 2024;42(28):
17. Lin ZY, Zhang P, Chi P, et al. Neoadjuvant short⁃course radiotherapy followed by camrelizumab and chemotherapy in locally advanced rectal cancer (UNION): early outcomes of a multicenter randomized phase III trial[J]. Ann Oncol. 2024;35(10):
18. Zhang W, Tang Y, Wei L, et al. Preoperative short⁃course radiotherapy followed by chemotherapy and PD⁃1 inhibitor administration for locally advanced rectal cancer: a study protocol of a randomized phase II/III trial (STELLAR II study)[J]. Colorectal Dis. 2024;26(9):1732–1740. doi:10.1111/codi.17090
19. Tan PB, Verschoor YL, van den Berg JG, et al. Neoadjuvant immunotherapy in mismatch-repair-proficient colon cancers. Nature. 2025. doi:10.1038/s41586-025-09679-4
20. Huang Y, Stylianopoulos T, Duda DG, et al. Benefits of vascular normalization are dose and time dependent-letter[J]. Cancer Res. 2013;73(23):7144–7146. doi:10.1158/0008-5472.CAN-13-1989
21. Fukuoka S, Hara H, Takahashi N, et al. Regorafenib Plus Nivolumab in Patients With Advanced Gastric or Colorectal Cancer: an Open-Label, Dose- Escalation, and Dose-Expansion Phase Ib Trial (REGONIVO, EPOC1603). J Clin Oncol. 2020;38(18):2053–2061.
22. Guo Y, Zhang W, Ying J, et al. Phase 1b/2 trial of fruquintinib plus sintilimab in treating advanced solid tumours: the dose-escalation and metastatic colorectal cancer cohort in the dose-expansion phases. Eur J Cancer. 2023;181:26–37. doi:10.1016/j.ejca.2022.12.004
23. Kato T, Kagawa Y, Kuboki Y, et al. Safety and efficacy of panitumumab in combination with trifluridine/tipiracil for pre-treated patients with unresectable, metastatic colorectal cancer with wild-type RAS: the phase 1/2 APOLLON study. Int J Clin Oncol. 2021;26(7):1238–1247. doi:10.1007/s10147-021-01902-2
24. Kuboki Y, Nishina T, Shinozaki E, et al. Tas-102 plus bevacizumab for patients with metastatic colorectal cancer refractory to standard therapies (C- TASK FORCE): an investigator-initiated, open-label, single-arm, multicentre, phase 1/2 study. Lancet Oncol. 2017;18(9):1172–1181. doi:10.1016/S1470-2045(17)30425-4
25. Pfeiffer P, Yilmaz M, Möller S, et al. Tas-102 with or without bevacizumab in patients with chemorefractory metastatic colorectal cancer: an investigator-initiated, open-label, randomised, phase 2 trial. Lancet Oncol. 2020;21(3):412–420. doi:10.1016/S1470-2045(19)30827-7
26. Yoshida Y, Yamada T, Kamiyama H, et al. Combination of Tas-102 and bevacizumab as third-line treatment for metastatic colorectal cancer: the TAS-CC3 study. Int J Clin Oncol. 2021;26(1):111–117.
27. Jm L, Wang YY, W LIU, et al. Preoperative CA199: a competitive predictor of recurrence in patients with colorectal cancer liver metastases after hepatectomy. Int J Colorectal Dis. 2021;36(4):767–778.
28. Dong H, Tang J, Li LH, et al. Serum carbohydrate antigen 19-9 as an indicator of liver metastasis in colorectal carcinoma cases. Asian Pac J Cancer Prev. 2013;14(2):909–913. doi:10.7314/APJCP.2013.14.2.909
29. Zhang P, Wen X, Feng G, et al. Multiplexed cytokine profiling of serum for detection of colorectal cancer. Future Oncol. 2013;9(7):1017–1027. doi:10.2217/fon.13.71
30. Skuja E, Gerina-Berzina A, Hegmane A, Zvirbule Z, Vecvagare E, Purkalne G. Duration of previous treatment as a prognostic factor in metastatic colorectal cancer treated with trifluridine/tipiracil. Mol Clin Oncol. 2018;8(5):699–702. doi:10.3892/mco.2018.1600
31. Adenis A, de la Fouchardiere C, Paule B, et al. Survival, safety, and prognostic factors for outcome with Regorafenib in patients with metastatic colorectal cancer refractory to standard therapies: results from a multicenter study (REBECCA) nested within a compassionate use programme. BMC Cancer. 2016;16(1):412. doi:10.1186/s12885-016-2440-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Immune Checkpoint Inhibitor-Based Combination Therapy for Colorectal Cancer: An Overview
Li J, Xu X
International Journal of General Medicine 2023, 16:1527-1540
Published Date: 26 April 2023
Integration of scRNA-Seq and Bulk RNA-Seq Identifies Circadian Rhythm Disruption-Related Genes Associated with Prognosis and Drug Resistance in Colorectal Cancer Patients
Tao Y, Li J, Pan J, Wang Q, Ke RW, Yuan D, Wu H, Cao Y, Zhao L
ImmunoTargets and Therapy 2025, 14:475-489
Published Date: 11 April 2025
Advances in the Use of Immune Checkpoint Inhibitors for Colorectal Cancer Treatment
Li J, Fu T, Wen Z, Liang J, Qiu Y, Li K, Yang J, Tong Y, Cai H
OncoTargets and Therapy 2025, 18:1159-1168
Published Date: 15 October 2025
Mechanisms and Emerging Strategies to Overcome Immunotherapy Resistance in Cold Tumours of Colorectal Cancer
Zhu X, Ge B, Wen L
OncoTargets and Therapy 2026, 19:621109
Published Date: 15 June 2026