Back to Journals » Infection and Drug Resistance » Volume 19
Clinical Features and Factors Associated with Disease Severity in Acute Chikungunya Fever: A Retrospective Analysis
Authors Lin H ![]() , Xie S
, Xie S ![]() , Li K, Chen Z, Wang Y
, Li K, Chen Z, Wang Y ![]()
Received 15 October 2025
Accepted for publication 6 February 2026
Published 12 February 2026 Volume 2026:19 569624
DOI https://doi.org/10.2147/IDR.S569624
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Oliver Planz
Hanjie Lin,1,* Shan Xie,1,* Kai Li,1 Zhanqin Chen,2 Yue Wang1
1Department of Clinical Laboratory, Foshan Women and Children Hospital Affiliated to Guangdong Medical University, Foshan, Guangdong, 528000, People’s Republic of China; 2Department of Information, Foshan Women and Children Hospital Affiliated to Guangdong Medical University, Foshan, Guangdong, 528000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yue Wang, Email [email protected]
Background: Chikungunya fever has emerged as a significant public health concern in tropical and subtropical regions worldwide. Understanding the epidemiological patterns and clinical features of chikungunya virus infection is crucial for developing effective disease surveillance and management strategies.
Methods: We conducted a retrospective analysis of 311 laboratory-confirmed chikungunya fever cases presenting to a tertiary hospital in Foshan, Guangdong Province, China, from June to September 2025.
Results: The study population had a median age of 32.35 years (interquartile range: 10– 53 years), with females comprising 56.3%. Fever occurred in 85.9% of patients, with 49.2% experiencing moderate to high-grade fever. Joint symptoms were present in 76.5% of patients, with 48.6% developing moderate to severe arthralgia. Rash was a significant clinical manifestation with an incidence of 73%, of which 44.1% of patients presented with severe rash. Laboratory abnormalities included leukopenia (6.4%), lymphopenia (64.6%), and elevated C-reactive protein (66.2%). Multivariate analysis identified rash presence, joint symptoms, and younger age as factors significantly associated with moderate-severe disease presentations. However, as rash and joint symptom severity were incorporated into the severity scoring system, these associations should be interpreted as descriptive characterization rather than independent prediction.
Conclusion: This study characterizes the clinical features of acute chikungunya fever, with age-related severity differences and specific clinical and laboratory markers associated with disease severity. Rash emerges as a significant clinical manifestation associated with disease severity, highlighting its value in clinical assessment of chikungunya fever. These findings support the development of risk stratification tools and evidence-based management protocols for chikungunya fever patients.
Keywords: chikungunya fever, epidemiology, clinical features, disease severity, arboviral infection, rash
Introduction
Chikungunya fever is an increasingly important vector-borne viral infection caused by chikungunya virus (CHIKV), which belongs to the genus Alphavirus of the family Togaviridae.1,2 The disease was first described in 1952 in Tanzania, with its name derived from the Kimakonde language meaning “that which bends up,” reflecting the characteristic joint pain and postural changes experienced by infected individuals.3,4
After decades of sporadic outbreaks primarily confined to Africa and Asia, chikungunya fever has undergone significant global expansion since 2004. Major epidemics have occurred in the Indian Ocean islands, Southeast Asia, and the Americas, affecting millions of people and establishing CHIKV as a significant global public health concern.5,6 According to the World Health Organization’s Global Chikungunya Epidemiology Update (June 2025), as of December 2024, 119 countries and territories have reported local transmission of chikungunya virus. In 2024, the Region of the Americas alone reported 427,622 cases with 213 deaths, while limited data from early 2025 shows ongoing transmission in multiple regions, including over 13,000 cumulative cases in La Réunion’s outbreak that began in August 2024.7
The clinical presentation of chikungunya fever typically includes acute onset of fever, severe polyarthralgia, and myalgia, often accompanied by rash and other systemic manifestations.8,9 While traditionally considered a self-limiting illness, chikungunya infection can progress to chronic arthropathy in a substantial proportion of patients, leading to long-term disability and reduced quality of life.10–12 One study found that approximately 50% of cases progress to chronic conditions, with joint symptoms persisting for months or even years.13 Additionally, severe manifestations including neurological complications, cardiovascular involvement, and fatal outcomes have been increasingly recognized, challenging previous assumptions about the benign nature of this infection.14,15 The pathogenesis of chikungunya fever involves viral replication in target cells including fibroblasts, macrophages, and endothelial cells, triggering robust innate immune responses characterized by elevated pro-inflammatory cytokines and chemokines. The persistence of viral RNA and antigens in joint tissues has been implicated in the development of chronic arthropathy.
Despite growing recognition of chikungunya fever as a major public health problem, comprehensive epidemiological characterization remains limited in many affected regions. Recent evidence suggests a higher incidence of severe CHIKV infections and increased mortality rates than previously recognized, with studies documenting atypical and severe disease manifestations that extend beyond the traditional joint-focused symptomatology.16,17 Understanding patterns of clinical manifestations, laboratory abnormalities, and severity-related characteristics is crucial for developing effective surveillance systems, clinical management protocols, and public health intervention strategies.18,19 This study aimed to describe epidemiological and clinical features of CHIKV infection and identify factors associated with disease severity.
Methods
Study Design and Setting
This retrospective observational study was conducted at Foshan Women and Children Hospital Affiliated to Guangdong Medical University, a tertiary referral center in Foshan, Guangdong Province, southern China. The study analyzed laboratory-confirmed chikungunya fever cases presenting from June 2025 to September 2025, during a regional outbreak period. The study was approved by the institutional ethics committee (FSFY-MEC-2025-155, approved October 9, 2025). Chikungunya virus infection was confirmed by detection of viral RNA using reverse transcription polymerase chain reaction (RT-PCR) performed on serum samples collected during the acute febrile phase. Testing was conducted using commercially available kits according to manufacturer protocols at the hospital’s clinical laboratory. Clinical and laboratory data were collected at the time of initial presentation during the acute phase of infection. Disease severity assessment reflects acute disease status at the time of presentation, and this study does not include long-term follow-up data for assessment of chronic chikungunya disease. Data represent a single cross-sectional assessment for each patient. This study aimed to describe clinical features of acute CHIKV infection and identify factors associated with disease severity.
Study Population
The study included 311 patients with chikungunya infection confirmed by viral nucleic acid testing. Patients of all ages with confirmed chikungunya infection were eligible for inclusion. Cases with incomplete clinical documentation or uncertain diagnostic status were excluded from the analysis.
Data Collection
Clinical and laboratory data were systematically extracted from medical records using standardized data collection forms. Variables collected included demographic characteristics (age, sex), clinical manifestations (fever, joint symptoms, myalgia, headache, respiratory symptoms, rash), laboratory parameters (complete blood count, liver function tests, inflammatory markers, coagulation profile), and outcome measures.
Clinical Assessment
Clinical symptom assessment and severity grading were performed according to the “Guidelines for Diagnosis and Treatment of Chikungunya Fever (2025 Edition)” issued by the National Health Commission of People’s Republic of China.20 A standardized clinical symptom assessment system was established covering the major clinical manifestations of chikungunya fever. Fever severity was classified using a five-tier system: no fever (grade 0), low-grade fever 37–38°C (grade 1), moderate fever 38–39°C (grade 2), high fever 39–40°C (grade 3), and hyperpyrexia >40°C (grade 4). Joint symptoms were graded into four levels based on functional impact and pain intensity: asymptomatic (grade 0), mild (grade 1), moderate (grade 2), and severe (grade 3).
Rash severity assessment employed a standardized grading system based on anatomical distribution extent. This grading system evaluated rash based on the number and distribution of affected anatomical sites: no rash was rated as grade 0; rash limited to a single anatomical region (such as unilateral limb, face, or localized trunk area) was rated as grade 1 mild rash; rash involving two anatomical sites (such as bilateral upper limbs, bilateral lower limbs, or trunk combined with single limb site) was rated as grade 2 moderate rash; rash involving three or more anatomical sites, presenting widespread or generalized distribution patterns (such as all four limbs combined with trunk, or diffuse whole-body rash) was rated as grade 3 severe rash. This grading system provided clinicians with objective, reproducible criteria for assessing rash severity, facilitating accurate disease severity determination.
Other systemic symptoms including myalgia, headache, cough, and dyspnea were recorded as binary variables (present or absent), providing supplementary information for comprehensive clinical assessment.
Laboratory Analysis
Laboratory parameters analyzed included white blood cell count, lymphocyte percentage, neutrophil percentage, platelet count, neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammation index (SII), red blood cell count, hemoglobin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), C-reactive protein (CRP), and coagulation indices (PT, APTT, TT, FIB). Abnormal values were defined using standard laboratory reference ranges.
Disease Severity Assessment
The comprehensive disease severity score was calculated by summing the individual severity grades for fever (0–4 points), joint symptoms (0–3 points), and rash distribution (0–3 points). Total scores ranged from 0–10 points, with patients categorized as mild (0–2 points), moderate (3–5 points), or severe (≥6 points) disease. For analytical purposes, a binary classification comparing mild versus moderate-severe disease was adopted.
Statistical Analysis
Descriptive statistics were calculated for all variables, with continuous variables expressed as mean Chi-square tests were used for categorical comparisons when all expected cell counts were ≥5; Fisher’s exact test was used when any expected cell count was <5. Multicollinearity was assessed using variance inflation factors (VIF), with all variables showing VIF <2.5. Model fit was evaluated using the Hosmer-Lemeshow goodness-of-fit test. Given the methodological concerns regarding circular reasoning (see Limitations), we have not presented ROC analysis for predictive accuracy, as our findings should be interpreted as descriptive associations rather than a validated prediction model.
Univariate and multivariate logistic regression analyses were conducted to identify factors associated with disease severity. Variables with P-values less than 0.10 in univariate analysis were included in the multivariate model. Odds ratios (OR) with 95% confidence intervals (CI) were calculated. Statistical significance was set at P < 0.05. All analyses were performed using R statistical software version 4.3.0.
Liver function and coagulation parameters were available for a subset of patients (n=66 and n=60, respectively) based on clinical indication. Analyses involving these parameters were conducted using available-case analysis, with sample sizes clearly reported. These subset analyses should be interpreted with caution due to potential selection bias and limited statistical power.
Results
Demographic Characteristics
The study included 311 laboratory-confirmed chikungunya fever patients with demographic characteristics summarized in Table 1. The cohort was predominantly young (median age 32.35 years) with a slight female predominance (56.3%). Notably, over two-thirds of patients were under 44 years of age, reflecting the age structure of the outbreak population.
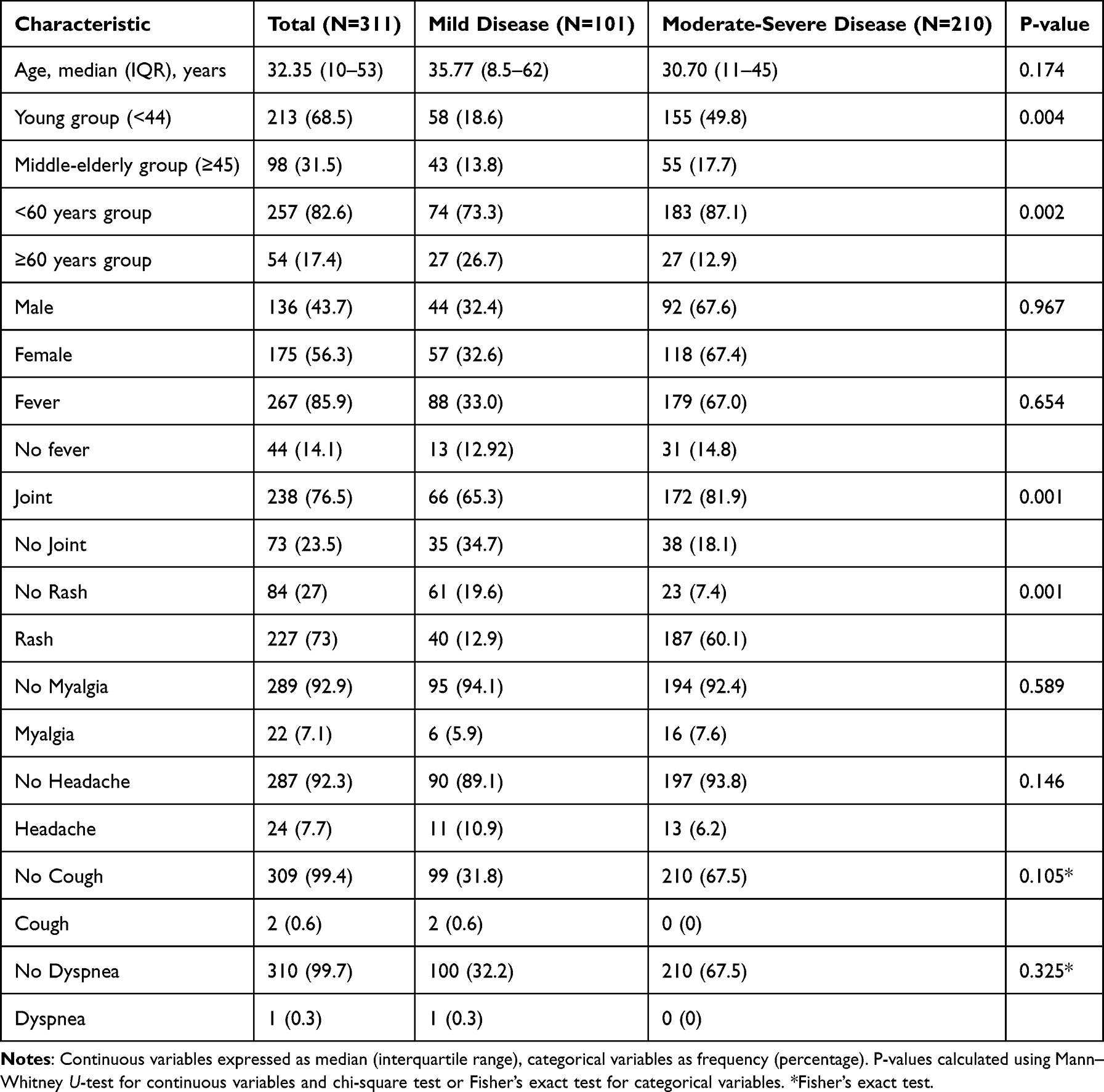 |
Table 1 Patient Demographic and Clinical Characteristics (N=311) |
Clinical Manifestations
The classic triad of chikungunya fever—fever, arthralgia, and rash—was well represented in our cohort (Table 1). Fever was nearly universal (85.9%), though most patients presented with low-to-moderate grade fever rather than hyperpyrexia. Joint symptoms and rash occurred in approximately three-quarters of patients, representing the second and third most common manifestations, respectively.
Rash demonstrated a particularly striking association with disease severity: all patients with severe rash (grade 3, involving three or more anatomical sites) were classified in the moderate-severe disease group, while no cases of severe rash occurred in the mild disease group (P=0.001) (Table S1). This strong association suggests rash extent may serve as a clinical indicator of disease severity. Systemic manifestations including myalgia (7.1%), headache (7.7%), and respiratory symptoms were relatively uncommon. The combination of fever, joint symptoms, and rash—the hallmark chikungunya syndrome—was present in 49.8% of all cases.
Laboratory Abnormalities
Laboratory findings are detailed in Table 2. The most prominent hematological abnormality was lymphopenia (64.6%), consistent with the known lymphotropism of chikungunya virus. Although leukopenia was uncommon overall (6.4%), it was significantly more frequent in moderate-severe disease compared to mild disease (8.6% vs 2.0%, P=0.026), suggesting potential utility as a severity marker.
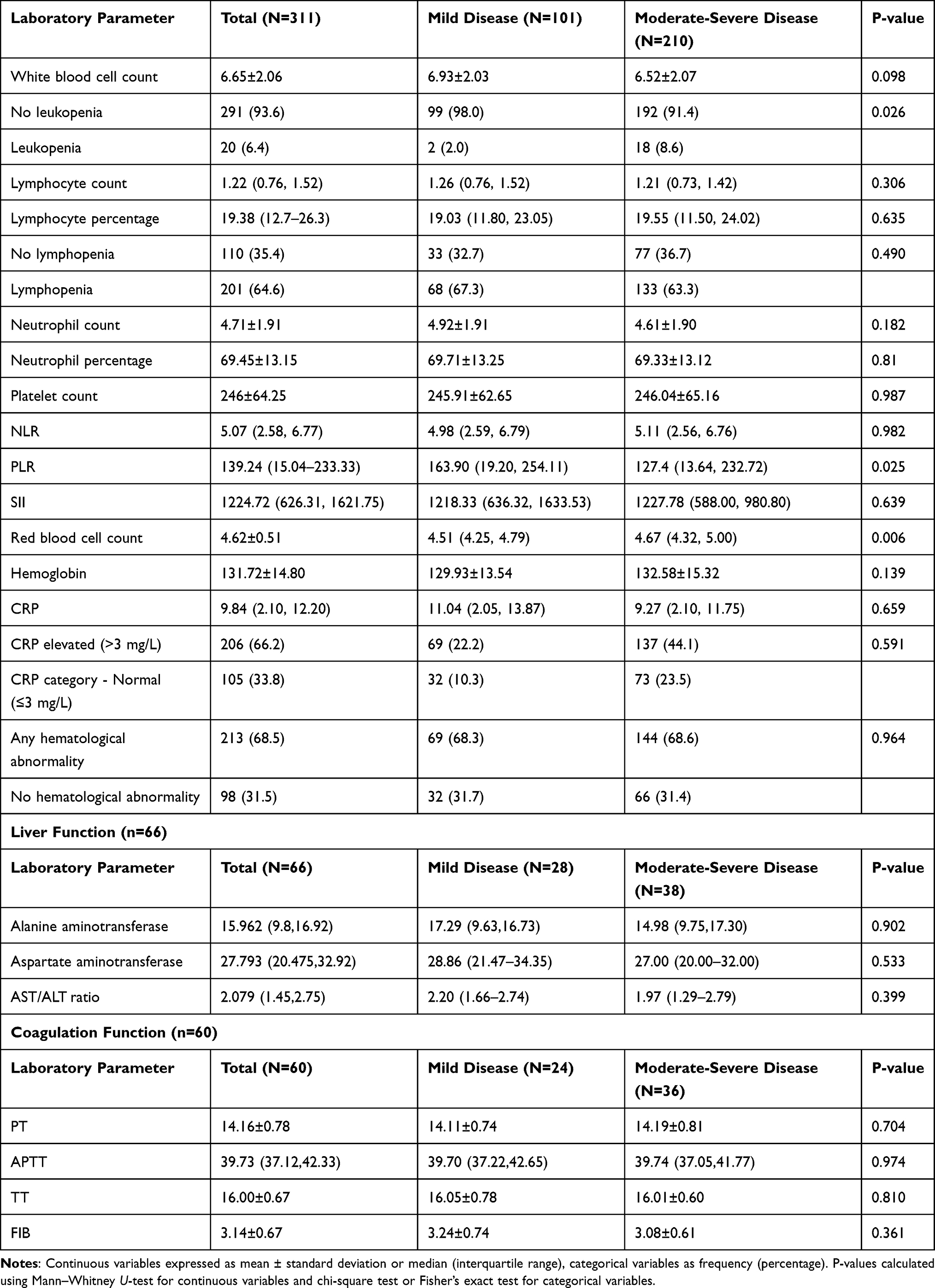 |
Table 2 Laboratory Parameters and Abnormalities Stratified by Disease Severity (N=311) |
Among inflammatory markers, C-reactive protein elevation (>3 mg/L) was observed in 66.2% of patients. The platelet-to-lymphocyte ratio (PLR) was paradoxically lower in the moderate-severe group compared to the mild group (P=0.025), a finding that warrants further investigation. Red blood cell counts were significantly higher in the moderate-severe disease group (P=0.006), possibly reflecting hemoconcentration. Liver function and coagulation parameters, available in subsets of patients (n=66 and n=60, respectively), remained largely within normal limits regardless of disease severity.
Disease Severity Analysis
Using the comprehensive severity scoring system, 32.5% of patients were classified as mild disease, 60.5% as moderate disease, and 7.1% as severe disease. For subsequent analysis, patients were dichotomized into mild (32.5%) versus moderate-severe (67.5%) disease categories. Detailed stratification of clinical features by severity grade, including fever severity, joint symptom severity, rash severity, and inflammatory marker categories, is presented in Supplementary Table S1.
Age-Related Patterns
A notable and unexpected finding was the inverse relationship between age and disease severity. Among patients under 44 years, 72.8% (155/213) developed moderate-severe disease, compared to only 56.1% (55/98) of those aged 45 years and older (P=0.004). Similarly, patients under 60 years showed higher rates of moderate-severe disease than those 60 years and older (71.2% vs 50.0%, P=0.002). This pattern contrasts with traditional understanding of chikungunya severity and may reflect differences in healthcare-seeking behavior, viral strain characteristics, or population-specific factors.
Factors Associated with Disease Severity
Results of univariate and multivariate logistic regression analyses are presented in Table 3. After adjustment for potential confounders, five factors remained significantly associated with moderate-severe disease: age <60 years, presence of joint symptoms, absence of headache, presence of rash, and leukopenia. Rash demonstrated the strongest association with moderate-severe disease (adjusted OR 19.33, 95% CI: 9.38–39.83, P=0.001). However, this finding should be interpreted with caution given that rash severity contributed to the composite severity score, creating potential circularity in the analysis. Two unexpected findings emerged: age ≥60 years appeared protective (adjusted OR 0.33, 95% CI: 0.17–0.62, P=0.001), contrasting with literature suggesting elderly patients are at higher risk; and headache presence was inversely associated with severity (adjusted OR 0.34, 95% CI: 0.13–0.90, P=0.029). These counterintuitive results may reflect the limited elderly sample size (n=54) and require validation in larger studies.
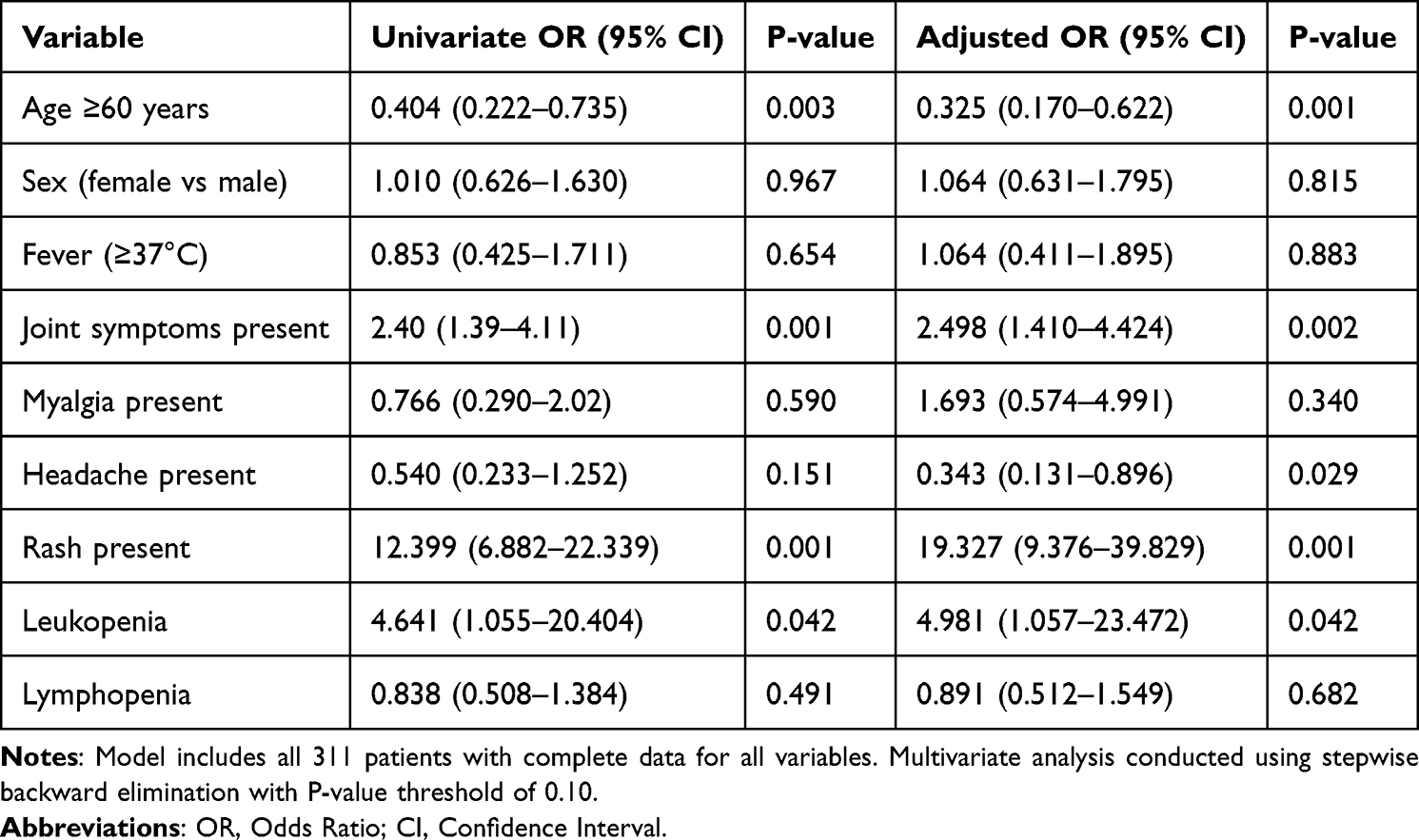 |
Table 3 Univariate and Multivariate Predictors of Moderate-Severe Disease (N=311) |
Geographic and Temporal Patterns
While specific geographic data were not systematically collected, the study population represents cases from defined endemic areas experiencing ongoing chikungunya transmission. Temporal analysis was limited by the retrospective study design, but cases appeared to cluster during periods of increased vector activity, consistent with known seasonal transmission patterns.
Discussion
This retrospective analysis of 311 laboratory-confirmed chikungunya fever cases provides comprehensive insights into the epidemiological patterns and clinical features of this increasingly important arboviral infection. The study findings demonstrate unique age-related disease severity patterns and highlight rash as a significant feature associated with disease severity, making important contributions to our understanding of chikungunya fever epidemiology and clinical management.
The demographic characteristics observed in this study, with a median age of 32.35 years and slight female predominance (56.3%), reveal unique epidemiological features of chikungunya infection in this region. Unlike previous studies demonstrating that elderly patients are at higher risk for severe disease and mortality,21–23 we observed that younger patients were more likely to develop moderate-severe disease, which may reflect differences in viral strains, population immune status, or healthcare-seeking behavior across different regions. This finding contrasts with recent evidence suggesting higher severity and mortality in elderly populations,24 highlighting the need for region-specific epidemiological assessments.
Rash emerged as a significant clinical manifestation of chikungunya fever, with an extremely high incidence (73%) and strong association with disease severity (OR 19.327). This finding emphasizes the importance of considering rash manifestations in clinical assessment of chikungunya fever. Our established rash grading system provides clinicians with a standardized assessment tool, facilitating early identification of disease severity and management decisions. The strong association between rash and disease severity aligns with recent studies documenting the expanding spectrum of chikungunya clinical manifestations beyond traditional joint-focused symptomatology.25 A critical methodological consideration is that rash severity was included as a component of the overall disease severity score. The high odds ratio for rash therefore partly reflects this scoring methodology rather than an independent predictive relationship. Our findings should be interpreted as characterization of the clinical phenotype of severe acute chikungunya presentations, with rash being a defining feature, rather than as identification of independent predictors for clinical risk stratification.
The clinical presentation characterized by fever rate of 85.9% and joint symptoms of 76.5% confirms the typical syndrome of chikungunya infection. Notably, respiratory symptoms showed extremely low incidence in this study (cough 0.6%, dyspnea 0.3%), which may differ from reports in other regions, suggesting geographic or viral strain-specific clinical presentation patterns. These findings are consistent with recent global epidemiological data showing variable clinical manifestations across different outbreak settings.25
Laboratory abnormality patterns revealed interesting characteristics. Compared to a study from Bangladesh reporting a leukopenia incidence of 10.4%,26 the incidence of leukopenia was relatively low (6.4%), while lymphopenia remained the most common hematological abnormality (64.6%). This pattern may reflect different disease stages, severity, or viral strain differences. Generally normal coagulation function and liver function suggest relatively mild chikungunya infection in the study population. The identification of PLR as a potential severity marker adds to the growing body of evidence on inflammatory biomarkers in arboviral infections.27
The multivariate analysis identified age <60 years, joint symptoms, and leukopenia as factors independently associated with disease severity, providing insights for clinical assessment. Notably, headache presence emerged as a protective factor (OR 0.343), a counterintuitive result that may relate to headache being relatively more common in mild disease, while in severe disease it may be masked by other prominent symptoms or subject to patient reporting bias. This finding requires further validation in larger prospective studies to determine its true significance and clinical implications.
The correlation between clinical manifestations and laboratory parameters supports the systemic nature of chikungunya fever and validates the comprehensive severity scoring approach used in this study. The difference in platelet-to-lymphocyte ratio between severity groups suggests potential value of this indicator in disease monitoring, consistent with emerging evidence on the utility of hematological ratios in arboviral disease assessment.28 While our study focused primarily on clinical features, the integration of laboratory biomarkers such as PLR and leukopenia with clinical assessment may enhance disease severity characterization. Future studies should explore combined clinical-laboratory scoring systems for improved patient stratification.
These findings have important implications for public health and clinical practice. The observed clinical diversity emphasizes the importance of symptom-based surveillance systems. These clinical patterns provide baseline data for comparison with future outbreaks and can inform evidence-based clinical management guidelines. The findings contribute to the growing recognition of chikungunya as a disease with potentially severe manifestations, challenging traditional perceptions of its benign nature.13
Several important limitations need consideration when interpreting these results. A key limitation of our severity analysis is that the comprehensive severity score incorporates rash and joint symptom severity as component variables. Therefore, the strong associations observed between these symptoms and overall severity partly reflect the scoring methodology rather than independent predictive relationships. We acknowledge that fever, joint symptoms, and rash were used both as components of the severity score and as variables in the regression analysis, which introduces circularity for these specific variables. The strong associations observed for rash (OR 19.327) and joint symptoms (OR 2.498) partly reflect this methodological limitation and should be interpreted as defining features of severe disease presentations rather than independent predictors. However, other variables analyzed—including age, headache, and leukopenia—are entirely independent of the severity score, and their significant associations with disease severity represent non-circular, clinically meaningful findings. The retrospective design inherently limits data completeness and introduces potential selection bias. The single-center nature of the study may limit generalizability to different geographic regions, populations, or healthcare settings. Additionally, lack of long-term follow-up data prevents assessment of chronic complications and recovery patterns. Quantitative viral load data were not available, precluding analysis of viremia levels as a potential severity marker.
Of particular concern are the limitations of age-related analysis. With only 54 patients (17.4%) aged ≥60 years in this study, the relatively small sample size may be insufficient to support reliable statistical inference about disease severity patterns in elderly patients. More importantly, our observation of age ≥60 years as a protective factor (OR 0.325) contradicts traditional epidemiological understanding and previous research conclusions, which typically report elderly patients being more susceptible to severe chikungunya fever. This counterintuitive finding may reflect multiple factors including differences in healthcare-seeking behavior patterns among elderly patients, variations in early disease recognition and management, or population-specific epidemiological characteristics. Therefore, conclusions regarding the relationship between age and disease severity should be interpreted cautiously and require further validation in larger multicenter studies.
The comprehensive severity scoring system and rash grading system, though systematically developed, require validation in independent populations to confirm clinical utility. The incompleteness of laboratory data (particularly liver function and coagulation tests covering only 66 and 60 patients respectively) also limits comprehensive assessment of the clinical significance of these parameters. The imbalanced age distribution, particularly the predominance of children and adolescent patients (68.5% of patients aged <44 years), may affect extrapolation of study results to populations with different age structures.
Despite these limitations, this study provides valuable epidemiological insights into chikungunya fever presentation patterns, particularly highlighting the association between rash and disease severity. The findings contribute to the growing evidence base supporting evidence-based approaches to chikungunya fever surveillance, diagnosis, and management.
Future research directions should include prospective studies with extended follow-up periods to better characterize long-term outcomes and chronic complications. Validation of identified severity factors and the rash grading system in different populations and healthcare settings will strengthen their clinical utility. Investigation of viral genetic factors and host immune responses associated with rash manifestations and disease severity may provide additional insights into chikungunya pathogenesis. Integration of emerging diagnostic technologies and therapeutic approaches will be crucial for improving patient outcomes.29–32
Conclusions
This retrospective analysis identified rash presence, joint symptoms, age <60 years, and leukopenia as factors significantly associated with moderate-severe disease presentations at the time of clinical assessment. The high frequency of fever (85.9%), joint symptoms (76.5%), and rash (73%) confirms the characteristic clinical syndrome. The established rash grading system provides clinicians with standardized assessment tools for severity evaluation. These findings support the development of evidence-based risk stratification and clinical management protocols for chikungunya fever patients in endemic regions.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of Foshan Women and Children Hospital Affiliated to Guangdong Medical University (Approval Number: FSFY-MEC-2025-155, approved on October 9, 2025). Due to the retrospective nature of this study and the use of anonymized data, the requirement for individual informed consent was waived by the ethics committee. Patient privacy and confidentiality were maintained throughout the study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest related to this work.
References
1. Robinson MC. An epidemic of virus disease in Southern Province, Tanganyika Territory, in 1952–1953. I. Clinical Features. Trans R Soc Trop Med Hyg. 1955;49(1):28–11. doi:10.1016/0035-9203(55)90080-8
2. de Souza WM, Lecuit M, Weaver SC. Chikungunya virus and other emerging arthritogenic alphaviruses. Nat Rev Microbiol. 2025;23(9):585–601. doi:10.1038/s41579-025-01177-8
3. Zumla A, Ntoumi F, Ippolito G. Chikungunya virus disease returns to Europe: a turning point for the global arboviral landscape. Lancet. 2025;406(10506):891–894. doi:10.1016/S0140-6736(25)01458-8
4. Cohen J. A chikungunya vaccine is likely to get approved. Who will get it? Science. 2023;382(6670):503–504. doi:10.1126/science.adm6803
5. Krambrich J, Mihalič F, Gaunt MW, et al. The evolutionary and molecular history of a chikungunya virus outbreak lineage. Plos Neglect Trop Dis. 2024;18(7):e0012349. doi:10.1371/journal.pntd.0012349
6. Liu Q, Shen H, Gu L, Yuan H, Zhu W. Chikungunya virus in Europe: a retrospective epidemiology study from 2007 to 2023. Plos Neglect Trop Dis. 2025;19(3):e0012904. doi:10.1371/journal.pntd.0012904
7. World Health Organization. Chikungunya Epidemiology Update (2025). Available from: https://www.who.int/publications/m/item/chikungunya-epidemiology-update-june-2025.
8. Suhrbier A. Rheumatic manifestations of chikungunya: emerging concepts and interventions. Nat Rev Rheumatol. 2019;15(10):597–611. doi:10.1038/s41584-019-0276-9
9. Santiago RA, Bavaresco SPP, Citrangulo SG, Medronho R, Sampaio V, Costa AJL. Clinical manifestations associated with the chronic phase of chikungunya fever: a systematic review of prevalence. Plos Neglect Trop Dis. 2025;19(2):e0012810. doi:10.1371/journal.pntd.0012810
10. Amaral JK, Schoen RT, Weinblatt ME, Cândido EL. Chikungunya fever and rheumatoid arthritis: a systematic review and meta-analysis. Trop Med Infect Dis. 2025;10(2):54. doi:10.3390/tropicalmed10020054
11. Ng WH, Amaral K, Javelle E, Mahalingam S. Chronic Chikungunya Disease (Ccd): clinical insights, immunopathogenesis and therapeutic perspectives. QJM. 2024;117(7):489–494. doi:10.1093/qjmed/hcae028
12. Zaid A, Gérardin P, Taylor A, Mostafavi H, Malvy D, Mahalingam S. Review: chikungunya arthritis: implications of acute and chronic inflammation mechanisms on disease management. Arthritis Rheumatol. 2018;70(4):484–495. doi:10.1002/art.40403
13. Brito C, Falcão MB, de Albuquerque M, Cerqueira-Silva T, Teixeira MG, Franca R. Chikungunya: from hypothesis to evidence of increased severe disease and fatalities. Viruses. 2025;17(1):62. doi:10.3390/v17010062
14. Cerny T, Schwarz M, Schwarz U, Lemant J, Gérardin P, Keller E. The range of neurological complications in chikungunya fever. Neurocrit Care. 2017;27(3):447–457. doi:10.1007/s12028-017-0413-8
15. Rajapakse S, Rodrigo C, Rajapakse A. Atypical manifestations of chikungunya infection. Trans R Soc Trop Med Hyg. 2010;104(2):89–96. doi:10.1016/j.trstmh.2009.07.031
16. Lima Neto AS, Sousa GS, Nascimento OJ, Castro MC. Chikungunya-attributable deaths: a neglected outcome of a neglected disease. Plos Neglect Trop Dis. 2019;13(9):e0007575. doi:10.1371/journal.pntd.0007575
17. Mavalankar D, Shastri P, Bandyopadhyay T, Parmar J, Ramani KV. Increased mortality rate associated with chikungunya epidemic, Ahmedabad, India. Emerg Infect Dis. 2008;14(3):412–415. doi:10.3201/eid1403.070720
18. Staples JE, Breiman RF, Powers AM. Chikungunya fever: an epidemiological review of a re-emerging infectious disease. Clin Infect Dis. 2009;49(6):942–948. doi:10.1086/605496
19. Sharp TM, Keating MK, Shieh W-J, et al. Clinical characteristics, histopathology, and tissue immunolocalization of chikungunya virus antigen in fatal cases. Clin Infect Dis. 2020;73(2):e345–e54. doi:10.1093/cid/ciaa837
20. NHC. Guidelines for diagnosis and treatment of chikungunya fever (2025 Edition). 2025. Available from: https://www.nhc.gov.cn/ylyjs/gzdt/202507/c592a4f82dd7405e9be5302e4147c0c7.shtml.
21. Silva Junior G, Pinto JR, Mota RMS, Pires Neto R, Daher EDF. Risk factors for death among patients with chikungunya virus infection during the outbreak in Northeast Brazil, 2016–2017. Trans R Soc Trop Med Hyg. 2018;113(4):221–226. doi:10.1093/trstmh/try127
22. Godaert L, Cofais C, Hequet F, et al. Adaptation of who definitions of clinical forms of chikungunya virus infection for the elderly. Am J Trop Med Hyg. 2021;104(1):106–109. doi:10.4269/ajtmh.20-0761
23. Godaert L, Dramé M, Roubaud-Baudron C. Emerging viruses in older population Chikungunya, West Nile fever and Dengue. Aging Clin Exp Res. 2021;33(3):723–727. doi:10.1007/s40520-019-01389-y
24. Cerqueira-Silva T, Pescarini JM, Cardim LL, et al. Risk of death following chikungunya virus disease in the 100 Million Brazilian Cohort, 2015–18: a matched cohort study and self-controlled case series. Lancet Infect Dis. 2024;24(5):504–513. doi:10.1016/S1473-3099(23)00739-9
25. Costa LB, Barreto F, Barreto MCA, et al. Epidemiology and economic burden of chikungunya: a systematic literature review. Trop Med Infect Dis. 2023;8(6):301. doi:10.3390/tropicalmed8060301
26. Rahman MM, Been Sayed SJ, Moniruzzaman M, et al. Clinical and laboratory characteristics of an acute chikungunya outbreak in Bangladesh in 2017. Am J Trop Med Hyg. 2019;100(2):405–410. doi:10.4269/ajtmh.18-0636
27. Böer L, Junqueira I, Nascimento T, Guilarde A, Féres V, Alcântara K. Monocyte-lymphocyte, neutrophil-lymphocyte, and platelet-lymphocyte ratios as inflammatory biomarkers of clinical dengue severity. Biosci J. 2024;40:e40038. doi:10.14393/BJ-v40n0a2024-67413
28. Russell CD, Parajuli A, Gale HJ, et al. The utility of peripheral blood leucocyte ratios as biomarkers in infectious diseases: a systematic review and meta-analysis. J Infect. 2019;78(5):339–348. doi:10.1016/j.jinf.2019.02.006
29. Jin J, Simmons G. Antiviral functions of monoclonal antibodies against chikungunya virus. Viruses. 2019;11(4):305. doi:10.3390/v11040305
30. August A, Attarwala HZ, Himansu S, et al. A Phase 1 trial of lipid-encapsulated mRNA encoding a monoclonal antibody with neutralizing activity against Chikungunya virus. Nature Med. 2021;27(12):2224–2233. doi:10.1038/s41591-021-01573-6
31. Silva S, Magalhães J, Matthews Q, et al. Development and field validation of a reverse transcription loop-mediated isothermal amplification assay (Rt-Lamp) for the rapid detection of chikungunya virus in patient and mosquito samples. Clin Microbiol Infect. 2024;30(6):810–815. doi:10.1016/j.cmi.2024.03.004
32. Bartholomeeusen K, Daniel M, LaBeaud DA, et al. Chikungunya Fever. Nat Rev Dis Primers. 2023;9(1):17. doi:10.1038/s41572-023-00429-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiological and Antimicrobial Resistant Patterns, and Molecular Mechanisms of Carbapenem-Resistant Klebsiella pneumoniae Infections in ICU Patients
Lu F, Zhang L, Ji J, Xu Y, Wang B, Xia J
Infection and Drug Resistance 2023, 16:2813-2827
Published Date: 9 May 2023
Epidemiological and Clinical Characteristics of Measles in Jinan, Shandong Province, China, from 1991 to 2022
Wang XY, Zhang XJ, Xia X, Chang SZ, Wu AZ
International Journal of General Medicine 2023, 16:2305-2312
Published Date: 6 June 2023
Acute Clinical Features and Persistence of Joint Pain in Probable Cases of Chikungunya Fever in Eritrea
Frezgi O, Berhane A, Ghebrewelde G, Tekie H, Kiflezgi T, Mohamedsied A, Tekie Y, Asrat MM, Gebrejesus T
Open Access Rheumatology: Research and Reviews 2025, 17:13-24
Published Date: 1 February 2025