Back to Journals » Infection and Drug Resistance » Volume 19
Clinical Characteristics and Early Risk Factors for Severe Mycoplasma Pneumoniae Pneumonia in Hospitalized Children: A Retrospective Analysis of 417 Cases
Authors An J, Du S, Yu S, Xu L, Song Y, Dong L, Zhao S
Received 18 December 2025
Accepted for publication 19 March 2026
Published 7 April 2026 Volume 2026:19 585205
DOI https://doi.org/10.2147/IDR.S585205
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Jia An,1 Shuling Du,2 Shuping Yu,3 Ling Xu,4 Yu Song,4 Li Dong,4 Shunying Zhao1
1Department II of Respiratory Medicine, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, China National Clinical Research Center of Respiratory Disease, Beijing, 100045, People’s Republic of China; 2Pediatric Emergency, The Seventh Medical Centre, Chinese PLA General Hospital, Beijing, 100700, People’s Republic of China; 3Medical Security Cente, The Seventh Medical Centre, Chinese PLA General Hospital, Beijing, 100700, People’s Republic of China; 4Children’s Outpatient and Emergency Department, The Seventh Medical Centre, Chinese PLA General Hospital, Beijing, 100700, People’s Republic of China
Correspondence: Shunying Zhao, Department II of Respiratory Medicine, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, China National Clinical Research Center of Respiratory Disease, 56 Nanlishi Road, Xicheng District, Beijing, 100045, People’s Republic of China, Tel +8613370115009, Email [email protected] Li Dong, Children’s Outpatient and Emergency Department, The Seventh Medical Centre, Chinese PLA General Hospital, 5 Nanxincang, Dongsishitiao, Dongcheng District, Beijing, 100700, People’s Republic of China, Tel +8618614081178, Email [email protected]
Background: Mycoplasma pneumoniae pneumonia (MPP) represents a common form of community-acquired pneumonia in children, and a proportion of cases progress to severe Mycoplasma pneumoniae pneumonia (SMPP), which may result in serious complications and life-threatening outcomes. Effective indicators for early recognition of severe disease remain unclear.
Methods: This retrospective analysis included 417 hospitalized children diagnosed with MPP, comprising 210 children with SMPP and 207 children with general Mycoplasma pneumoniae pneumonia (GMPP), admitted to The Seventh Medical Centre, Chinese PLA General Hospital, from October 2023 to February 2025. Clinical information, laboratory results, and imaging findings obtained within 24 hours of admission were collected. Differences between groups were compared, and logistic regression analysis along with receiver operating characteristic (ROC) curve analysis was performed to identify risk factors and their predictive value.
Results: Children with SMPP had longer hospitalization and higher frequencies of extrapulmonary complications. Their C-reactive protein (CRP), aspartate aminotransferase (AST), alanine aminotransferase (ALT), lactate dehydrogenase (LDH), and D-dimer (DD) levels were markedly higher. Imaging findings more often demonstrated lobar pneumonia, atelectasis, and pleural effusion. Multivariate logistic regression analysis identified CRP, AST, LDH, and DD as independent risk factors for SMPP. ROC analysis indicated that LDH greater than 286.5 U/L, DD greater than 0.1965 mg/L, and AST greater than 25.05 U/L were strong predictors of SMPP.
Conclusion: The clinical and laboratory profiles of children with SMPP differed significantly from those with GMPP. CRP, AST, LDH, and DD function as important indicators for early identification and assessment of disease severity, supporting clinical decision making. Early monitoring of these parameters enables timely recognition of high-risk patients and may improve clinical management and prognosis.
Keywords: clinical characteristics, inflammatory factors, Mycoplasma pneumoniae pneumonia, predictive indicators, risk factors
Introduction
Mycoplasma pneumoniae (MP) is a major pathogen responsible for community-acquired pneumonia (CAP) in children, particularly among school-age children and adolescents, with recent reports indicating a shift toward younger age groups.1–3 MP infection primarily affects the respiratory tract but may also involve multiple organ systems, presenting with diverse extrapulmonary manifestations that affect the skin, nervous system, blood, cardiovascular system, genitourinary system, and musculoskeletal system. Severe cases may develop complications such as pseudomembranous necrotizing laryngotracheobronchitis and myelin oligodendrocyte glycoprotein antibody-associated meningoencephalitis.4–7 Although most patients with Mycoplasma pneumoniae pneumonia (MPP) experience significant recovery, some progress to severe Mycoplasma pneumoniae pneumonia (SMPP), which is characterized by worsening clinical symptoms, progressive imaging abnormalities, and increased risks of mortality and complications.8
Most previous studies focused on isolated biomarkers or measurements obtained later in the disease course, limiting their applicability for early clinical decision-making at hospital admission. Lactate dehydrogenase (LDH) reflects cellular injury and immune-mediated tissue damage, whereas D-dimer indicates activation of coagulation pathways and inflammation-induced hypercoagulability-both of which have been implicated in severe MPP but remain insufficiently validated as early predictors. Early identification of high-risk patients is crucial for timely escalation of treatment, including corticosteroids or immunomodulatory therapy, to prevent irreversible pulmonary damage. Therefore, to support early identification and clinical management of SMPP, we systematically collected and compared general conditions, clinical characteristics, laboratory parameters, and chest imaging findings of patients with SMPP and general Mycoplasma pneumoniae pneumonia (GMPP). Differences between the groups were evaluated, and clinical characteristics, risk factors, and early warning indicators associated with SMPP were examined. These findings aim to provide evidence to support early diagnosis and timely intervention for SMPP, thereby reducing the occurrence of complications and long-term sequelae and improving patient prognosis.
Materials and Methods
Study Participants
This retrospective analysis included 417 children hospitalized with MPP in The Seventh Medical Centre, Chinese PLA General Hospital, from October 2023 to February 2025. Among these patients, 210 were classified as having SMPP and 207 were classified as having GMPP. The inclusion criteria were: (1) age between 3 months and 12 years; (2) diagnosis consistent with the criteria for MPP. The exclusion criteria were: (1) failure to meet inclusion criteria or incomplete clinical data; (2) patients diagnosed with congenital heart disease, pulmonary tuberculosis, bronchial foreign bodies, bronchiectasis, asthma, or metabolic disorders; and (3) children whose condition had already entered the recovery phase at the time of admission.
At our institution, cytokine testing and routine chest CT examinations were incorporated into the standardized clinical pathway for all children hospitalized with MPP.
Methods
Diagnostic Criteria for MPP
The diagnosis of MPP followed the Guidelines for Diagnosis and Treatment of Mycoplasma pneumoniae in Children (2023 Edition), which require:9 (1) acute fever, cough, and other symptoms of respiratory tract infection; (2) lung auscultation demonstrating medium to small moist rales or imaging studies demonstrating pulmonary lesions; and (3) laboratory evidence of infection with positive MP-DNA or RNA, or positive serum MP-IgM with an antibody titer of 1:160 or greater using the particle agglutination method, or a four-fold or greater increase in paired serum antibody titers during the disease course compared with earlier levels. MP-DNA or MP-RNA was tested using throat swab samples collected at admission with a Mycoplasma pneumoniae nucleic acid detection kit (Fosun Diagnostics, Shanghai, China). For children with positive nucleic acid results but a disease course longer than 5 days, serological confirmation was additionally performed using the particle agglutination method in the laboratory of our hospital.
Diagnostic Criteria for SMPP
According to the 2023 edition of the Guidelines for the Diagnosis and Treatment of Mycoplasma pneumoniae in Children, SMPP is diagnosed when any of the following criteria are met: persistent high fever of 39 °C or greater lasting 5 days or more, or fever lasting 7 days or more without reduction in peak temperature; wheezing, tachypnea, dyspnea, chest pain, or hemoptysis indicating severe pulmonary lesions or complications; extrapulmonary organ complications not meeting critical criteria; oxygen saturation of 93% or lower at rest while breathing room air; imaging studies demonstrating high-density consolidation involving more than two-thirds of a single pulmonary lobe or multiple lobes, or unilateral or bilateral diffuse bronchiolitis with bronchitis and atelectasis; or lesion progression exceeding 50% within 24 to 48 hours.9
Data Collection
Clinical information was collected for both groups, including: (1) general conditions and clinical characteristics such as age, gender, length of hospital stay, season of onset, drug resistance, and clinical manifestations; (2) laboratory examinations, including tumor necrosis factor α (TNF-α), interferon γ (IFN-γ), interleukin 2 (IL-2), interleukin 4 (IL-4), interleukin 5 (IL-5), interleukin 6 (IL-6), interleukin 17 (IL-17), immunoglobulin G (IgG), immunoglobulin M (IgM), immunoglobulin A (IgA), immunoglobulin E (IgE), white blood cell count (WBC), neutrophil count (NEU), monocyte count (MON), eosinophil count (EC), platelet count (PLT), C-reactive protein (CRP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), LDH, creatine kinase-MB isoenzyme (CK-MB), cardiac troponin I (TnI), fibrinogen (FIB), activated partial thromboplastin time (APTT), and D-dimer (DD); and (3) imaging findings from chest CT examinations (performed either at presentation in the emergency department or on the day of admission)., including infectious lesions, lobar consolidation, and the extent of pleural adhesion or thickening.
Plasma samples were prospectively collected at the time of hospital admission.10 Approximately 10 mL of peripheral blood was drawn into EDTA vacuum tubes (BD Vacutainer®) and processed within 4 hours of collection. The samples were centrifuged at 1,500 rpm (800 × g) for 10 minutes to separate plasma. The clarified plasma was then aliquoted and stored at −80°C until analysis. Cytokine levels were measured in the hospital’s clinical laboratory using the EasyMagPlex Human Cytokine 12 Plex Kit (Wellgrow Biotechnology Co., Ltd., Shenzhen, China).
Serum levels of IgG, IgM, IgA, ALT, AST, LDH, and CRP were measured using an automated biochemical analyzer (iMagic-M7; Mindray, Shenzhen, China) with corresponding commercial reagent kits.11 PLT, WBC, NEU, MON, and EC were determined using an automated hematology analyzer (XFA6000; Perlong Medical Equipment Co., China).12 FIB and APTT were assessed using an automated coagulation analyzer (Sysmex® CS-2100i).13 IgE, CK-MB, TnI, and DD were measured using a fully automated chemiluminescence immunoassay analyzer (CL-6000i; Mindray, Shenzhen, China).14
All Assays Were Performed in the Laboratory of Our Hospital
Statistical Analysis
Statistical analysis was conducted using SPSS 27.0 statistical software. Continuous variables were expressed as mean ± standard deviation ( ± s), and comparisons between groups were performed using the two-sample rank sum test. Categorical variables were reported as case numbers and percentages, with comparisons between groups conducted using the chi-square test or Fisher’s exact test. Variables that demonstrated statistical significance in univariate analysis were included in multivariate binary logistic regression analysis using forward likelihood ratio stepwise regression analysis. Receiver operating characteristic (ROC) curves were generated, and the predictive performance of each independent risk factor was assessed through the calculation of the area under the ROC curve (AUC). A p value of less than 0.05 was considered statistically significant.
± s), and comparisons between groups were performed using the two-sample rank sum test. Categorical variables were reported as case numbers and percentages, with comparisons between groups conducted using the chi-square test or Fisher’s exact test. Variables that demonstrated statistical significance in univariate analysis were included in multivariate binary logistic regression analysis using forward likelihood ratio stepwise regression analysis. Receiver operating characteristic (ROC) curves were generated, and the predictive performance of each independent risk factor was assessed through the calculation of the area under the ROC curve (AUC). A p value of less than 0.05 was considered statistically significant.
Results
Comparison of Basic Information and Clinical Characteristics Between SMPP and GMPP Groups
A total of 417 children were included, comprising 210 children in the SMPP group (103 males, 49.0%; 107 females, 51.0%) with a median age of onset of 6.17 years, and 207 children in the GMPP group (108 males, 52.2%; 99 females, 47.8%) with a median age of onset of 7.25 years. The length of hospital stay in the SMPP group was significantly longer than that in the GMPP group (11.57 days vs 8.66 days, p < 0.001). Regarding clinical manifestations, the incidence of fever (95.7% vs 87.2%, p = 0.03), cough (100.0% vs 95.2%, p = 0.01), and extrapulmonary complications (55.7% vs 0.1%, p < 0.001) was significantly higher in the SMPP group. No significant differences were observed between the groups in gender distribution, age composition, peak onset period, wheezing, or drug resistance (Table 1). The distribution of co-infecting pathogens in the SMPP and GMPP groups is shown in Figure 1.
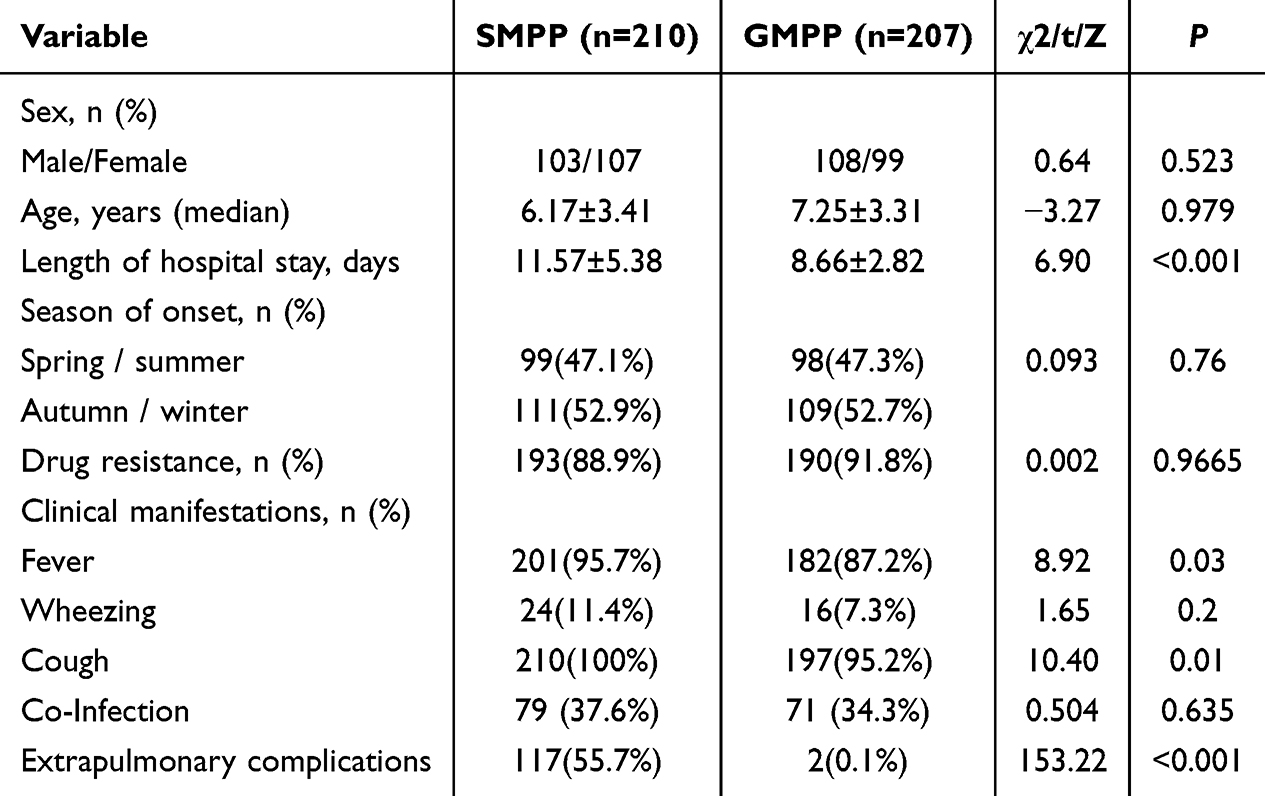 |
Table 1 Basic Information and Clinical Characteristics of Children with SMPP and GMPP |
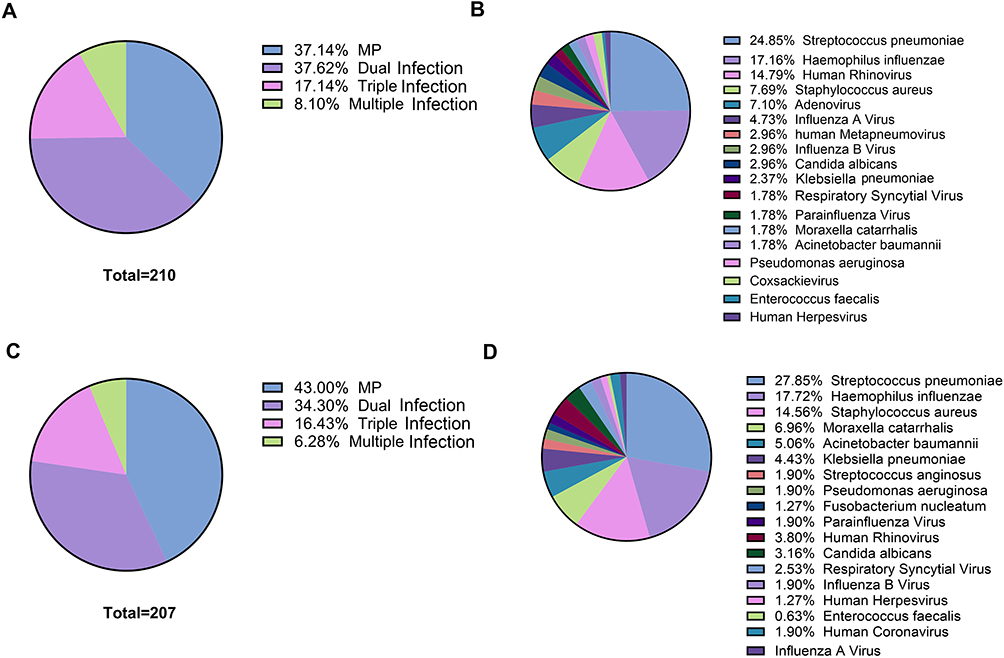 |
Figure 1 Distribution of co-infecting pathogens in the SMPP and GMPP groups. (A) Pathogen Distribution in the SMPP Group; (B) Distribution of Co-infecting Pathogens in the SMPP Group; (C) Pathogen Distribution in the GMPP Group; (D) Distribution of Co-infecting Pathogens in the GMPP Group. |
Comparison of Serum Inflammatory Cytokines and Immunoglobulin Levels Between SMPP and GMPP Groups
Compared with the GMPP group, serum levels of IFN-γ (18.87 pg/mL vs 13.26 pg/mL, p = 0.005), IL-4 (3.70 pg/mL vs 2.61 pg/mL, p = 0.045), IL-5 (2.24 pg/mL vs 1.24 pg/mL, p = 0.015), IL-6 (37.43 pg/mL vs 14.58 pg/mL, p = 0.007), and IgM (1.76 g/L vs 1.44 g/L, p < 0.001) were significantly higher in the SMPP group. Serum levels of TNF-α (2.99 pg/mL vs 4.20 pg/mL, p < 0.001) and IgE (194.4 g/L vs 222.6 g/L, p = 0.032) were significantly lower in the SMPP group. No significant differences were identified between the groups in IL-2, IL-17, IgG, or IgA levels (Table 2).
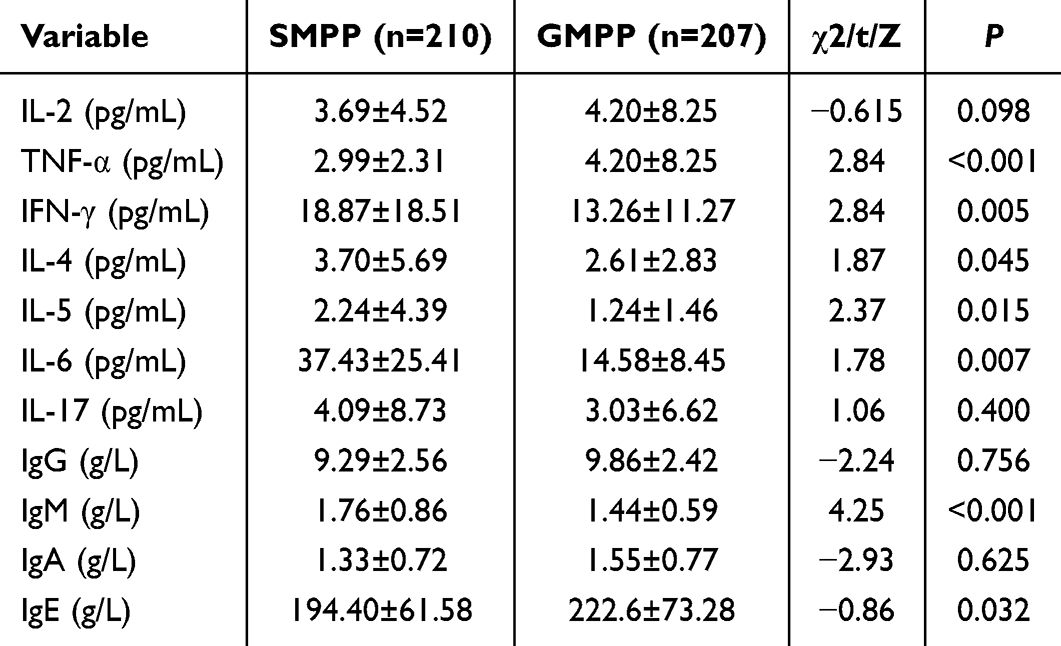 |
Table 2 Serum Inflammatory Cytokine and Immunoglobulin Levels in Children with SMPP and GMP |
Comparison of Laboratory Test results Between SMPP and GMPP Groups
Compared with the GMPP group, the SMPP group demonstrated significantly higher levels or activities of CRP (15.38 mg/L vs 10.71 mg/L, p = 0.026), AST (37.48 U/L vs 22.22 U/L, p = 0.002), ALT (25.14 U/L vs 13.16 U/L, p < 0.001), LDH (376.49 U/L vs 246.27 U/L, p < 0.001), CK-MB (23.21 U/L vs 17.79 U/L, p < 0.001), TnI (2.00 μg/L vs 1.22 μg/L, p < 0.001), APTT (33.02 s vs 33.68 s, p = 0.037), and DD (0.79 mg/L vs 0.15 mg/L, p < 0.001). No significant differences were observed between the groups in WBC, NEU, MON, EC, PLT, or FIB levels (Table 3).
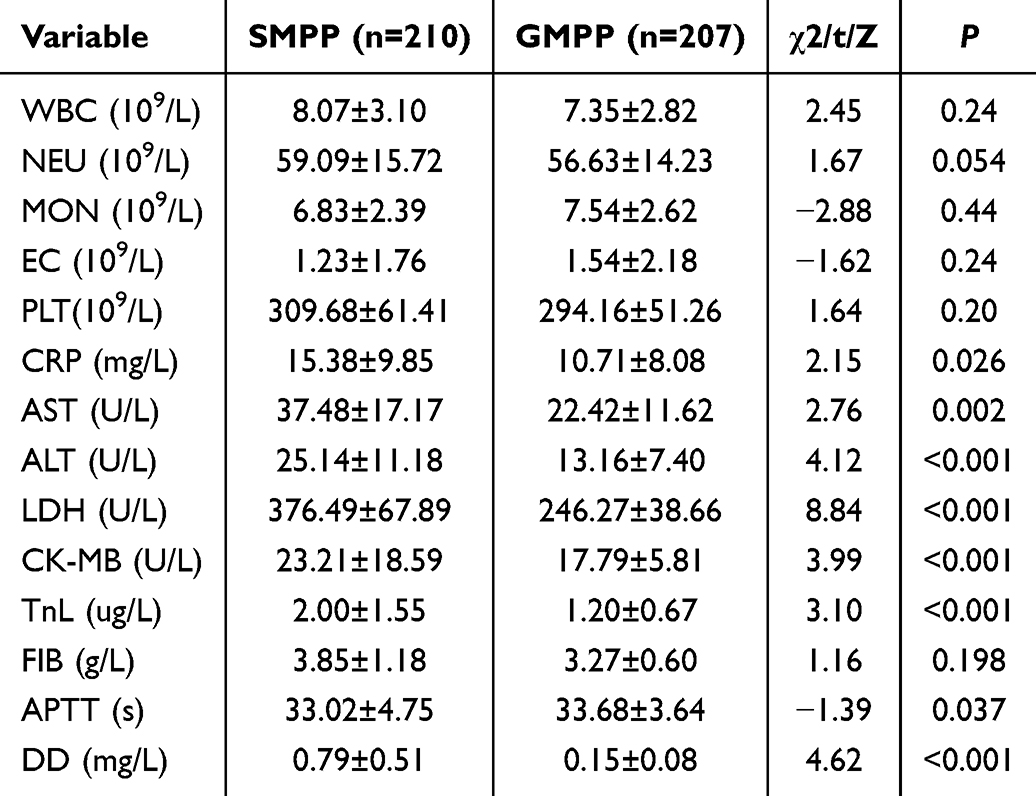 |
Table 3 Laboratory Test Results in Children with SMPP and GMPP |
Comparison of Imaging Analysis Results Between SMPP and GMPP Groups
Abnormal imaging findings were more pronounced in the SMPP group. The incidence of infectious lesions (p = 0.025), lobar pneumonia (p = 0.01), atelectasis (7.1% vs 1.4%, p = 0.004), pleural effusion (23.3% vs 4.8%, p < 0.001), and pericardial effusion (2.4% vs 0%, p = 0.025) was significantly higher in the SMPP group compared with the GMPP group (Table 4).
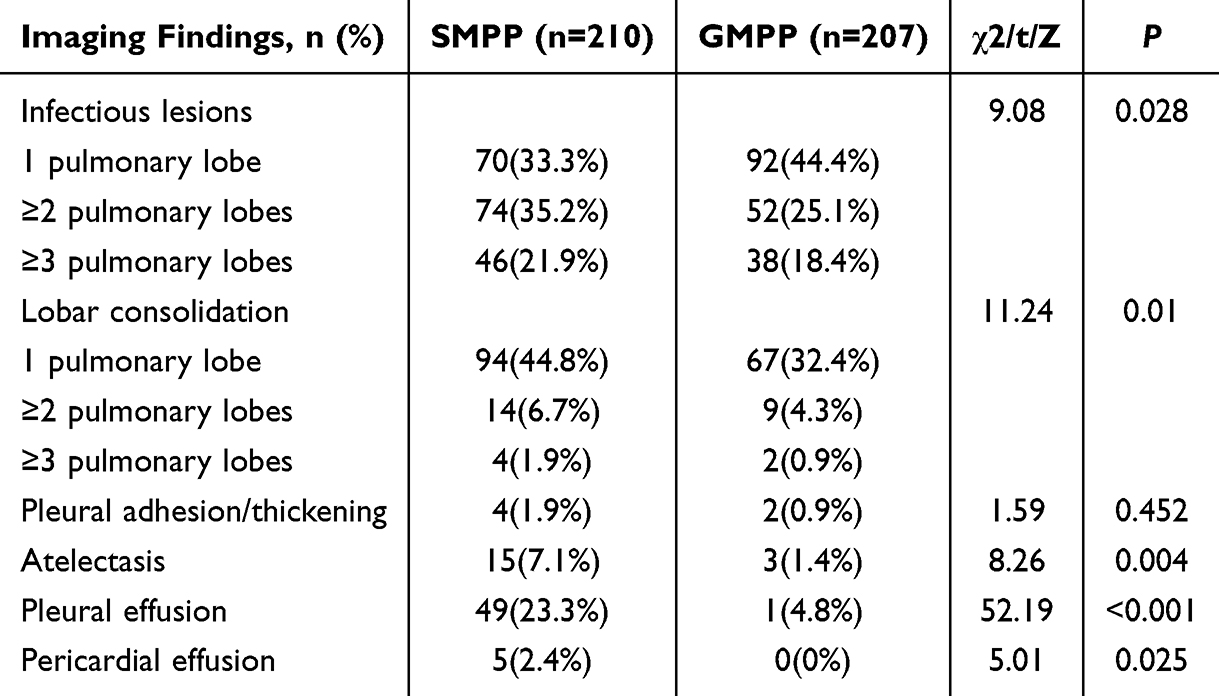 |
Table 4 Chest Imaging Findings in Children with SMPP and GMPP |
Correlation Analysis Between Different Clinical Indicators and SMPP Occurrence
Univariate analysis of clinical data from all children with MPP indicated that length of hospital stay, TNF-α, IFN-γ, IL-4, IL-5, IL-6, IgM, IgE, CRP, AST, ALT, LDH, CK-MB, TnI, APTT, and DD were significantly associated with SMPP (p < 0.05). Multivariate binary logistic regression analysis including these statistically significant variables identified length of hospital stay (p < 0.001), CRP (p = 0.026), AST (p = 0.011), ALT (p = 0.004), LDH (p < 0.001), and DD (p = 0.002) as independent risk factors for SMPP (Table 5).
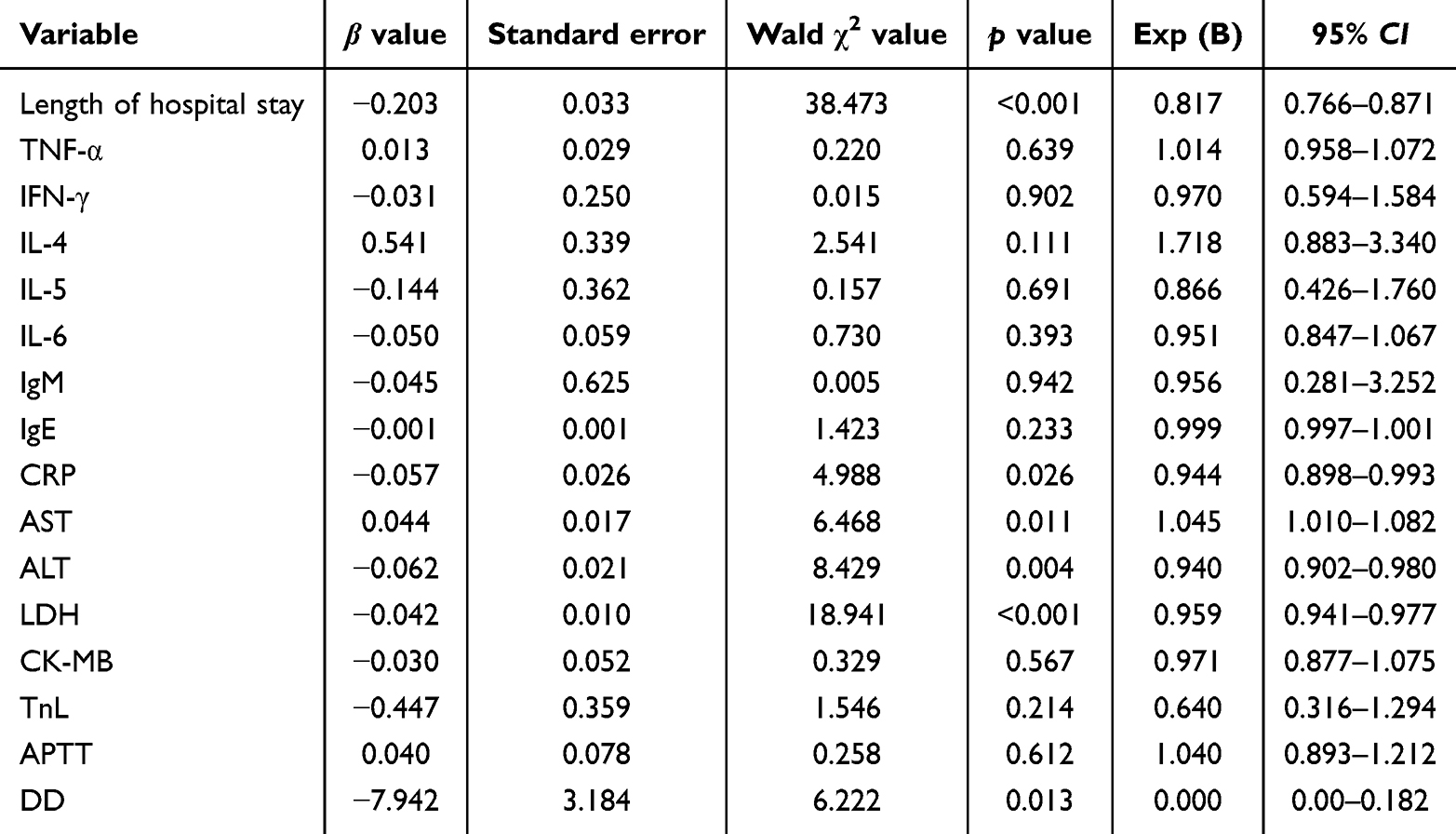 |
Table 5 Multivariate Logistic Regression Analysis of Independent Risk Factors for SMPP |
Predictive Value Analysis of Independent Correlative Factors for SMPP
ROC curve analysis evaluated the predictive performance of each independent risk factor for SMPP. LDH demonstrated the strongest predictive capability (AUC = 0.860, sensitivity = 77.4%, specificity = 90.1%), with levels exceeding 286.5 U/L effectively predicting SMPP. DD also demonstrated strong predictive value (AUC = 0.815, sensitivity = 73.8%, specificity = 77.6%), with levels above 0.1965 mg/L demonstrating high diagnostic utility. AST provided moderate predictive value (AUC = 0.675, sensitivity = 56.0%, specificity = 74.3%). CRP (AUC = 0.596, sensitivity = 53.0%) and ALT (AUC = 0.611, sensitivity = 57.1%) demonstrated weaker predictive performance (Table 6, Figure 2).
 |
Table 6 Predictive Value of Independent Risk Factors for SMPP Based on ROC Curve Analysis |
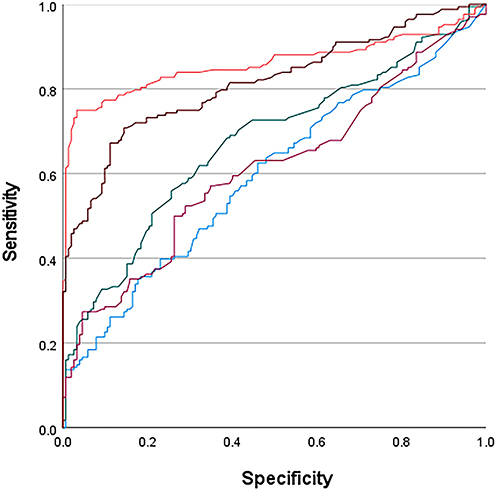 |
Figure 2 ROC curve analysis of each independent risk factors for SMPP. Blue: CRP; Green: AST; Purple: ALT; Red: LDH; Brown: DD. |
Discussion
MPP is one of the most common forms of community-acquired pneumonia in children and demonstrates clear seasonality and clustering patterns. Due to the immature immune function in children, particularly in the preschool age group, susceptibility to infection is increased. Recent research has indicated that the age of onset of MPP has gradually shifted toward younger children. Clinically, fever and cough represent the predominant manifestations, and early targeted antibiotic administration typically results in substantial symptom improvement. However, some children experience slow recovery or prolonged illness, which may lead to varying levels of intrapulmonary lesions and extrapulmonary involvement. Reports have indicated that approximately 6% to 23% of affected children may develop pulmonary sequelae. As the inflammatory response intensifies, some patients progress to SMPP, which is characterized by persistent high fever, dyspnea, and multi-organ functional impairment. Early recognition of disease severity and accurate prognostic assessment remain essential for optimizing therapeutic strategies and improving clinical outcomes.
The findings of this analysis indicated notable differences between SMPP and GMPP in clinical manifestations and laboratory characteristics. The longer hospitalization duration observed in children with SMPP may reflect increased disease complexity and challenges in clinical management. Fever, cough, and extrapulmonary complications occurred more frequently in the SMPP group, indicating that severe disease may be associated with heightened immune responses or more extensive infection. Extrapulmonary involvement may be related to systemic inflammatory responses triggered when Mycoplasma enters the bloodstream, although the underlying mechanisms require further clarification.15
Interleukins (ILs) are cytokines secreted by immune cells that regulate immune responses and are closely associated with the development and progression of MPP.16–18 IL-4 promotes B-cell proliferation, differentiation, and activation, stimulates airway epithelial cells to secrete mucus, and contributes to airway smooth muscle activation, all of which may provoke airway hyperresponsiveness. IL-4 is frequently used as an indicator of the risk of refractory MPP in children.19 IL-5 plays a crucial role in the differentiation, recruitment, and activation of eosinophils, contributing to airway inflammation and remodeling and promoting Mycoplasma-associated or Mycoplasma-aggravated asthma.20 IL-6 is involved in anti-infection responses through activation of immune cells, but persistently elevated IL-6 levels may result in tissue damage and immunopathological responses.21 TNF-α facilitates the release of chemokines by macrophages and neutrophils, and the combined effect of these pathways results in rapid neutrophil migration and accumulation at inflammatory sites, leading to aggravated local inflammation and tissue injury.22 Consistent with domestic and international research findings, the present results demonstrated that levels of IL-4, IL-5, IL-6, and IFN-γ were significantly higher in children with SMPP compared with those with GMPP.23–25
A recent retrospective, cross-sectional study involving CAP children in the pediatric intensive care unit has found that mortality was significantly associated with infectious agent type, respiratory support type, length of stay, lactate, and lactate/albumin ratio.26 Their results suggest that CRP/mean platelet volume may be useful in assessing mortality, clinical severity, and respiratory support type, and the lactate/albumin ratio may be a more valuable predictor of mortality than lactate alone. Our study also incorporated laboratory indicators reflecting infection and inflammation (WBC, NEU, MON, EC, CRP, serum amyloid A [SAA], erythrocyte sedimentation rate [ESR], LDH), liver function (ALT, AST), myocardial involvement (CK-MB, TnI), coagulation function (FIB, APTT, DD), and PLT to provide a comprehensive assessment of inflammatory status, organ injury, and multi-system functional changes. Compared with the GMPP group, the SMPP group demonstrated significantly higher levels or activities of CRP, LDH, AST, ALT, CK-MB, TnI, APTT, and DD. CRP and LDH represent important inflammatory biomarkers, and their levels are closely related to the severity of inflammation.
These markers are considered sensitive for the early detection of MP infection in children.27 Children with SMPP were also more likely to develop pulmonary and extrapulmonary complications. Although the mechanisms underlying MP-related extrapulmonary complications are not fully understood, existing evidence indicates that both direct pathogen-induced injury and excessive immune activation contribute to their development.
Elevated ALT and AST levels indicated that infection may affect hepatic function, while increased CK-MB and TnI levels implied possible myocardial or skeletal muscle involvement.28,29 DD levels were also significantly higher in severe cases, consistent with prior evidence linking MPP to increased risks of thrombosis or embolism.30 The markedly elevated DD levels observed in SMPP align with previous research reporting enhanced thrombosis risk in children with MPP.31 However, no clinically confirmed thrombotic events, such as deep vein thrombosis or pulmonary embolism, were documented in this cohort, and none of the children had known predispositions to thrombophilia. The elevated DD levels may therefore reflect a localized pulmonary hypercoagulable state induced by Mycoplasma infection rather than secondary consequences of extrapulmonary thrombosis.
MP can involve the entire respiratory tract, including the bronchial, interstitial, and alveolar regions. Accordingly, MPP may present with diverse imaging manifestations. Although the distribution of lesions did not differ significantly between SMPP and GMPP, the infection in children with SMPP was more extensive, with significantly higher rates of lobar pneumonia, atelectasis, and pleural effusion. A prior analysis of 393 hospitalized children with MPP reported that pulmonary lobe or segmental consolidation was the most common imaging finding (37%).32 These observations indicate that MP infection can lead to substantial pulmonary tissue injury, underscoring the importance of early assessment to prevent adverse outcomes.
Early prediction of SMPP in the initial stages of MP infection has substantial clinical relevance. Multiple serological indicators were evaluated to determine their predictive utility. Logistic regression analysis identified length of hospital stay, CRP, AST, ALT, LDH, and DD as independent risk factors for SMPP. ROC curve analysis further demonstrated that LDH levels of 286.5 U/L or greater and DD levels of 0.1965 mg/L or greater served as reliable predictors of SMPP. Another study reported that LDH levels of 360 U/L or greater and DD levels of 0.6 mg/L or greater were meaningful predictors of SMPP. Collectively, these findings indicate that LDH and DD hold promise as key serological markers for evaluating disease severity and predicting progression to severe disease. Larger multicenter studies will be essential for validating their clinical reliability and establishing optimal cutoff values.
Conclusions
In conclusion, children with SMPP exhibited higher frequencies of persistent high fever, extrapulmonary manifestations, notable pulmonary imaging abnormalities, coagulation dysfunction, and marked elevations in inflammation and tissue-injury markers including CRP, LDH, AST, ALT, CK-MB, TnI, APTT, and DD compared with children with non-severe MPP. CRP, AST, ALT, LDH, and DD demonstrated meaningful value in predicting SMPP. When chest imaging at admission reveals substantial pulmonary consolidation and laboratory findings display markedly elevated levels of these biomarkers, clinicians should recognize the heightened risk of progression to SMPP. In such circumstances, prompt anti-Mycoplasma management alongside early use of glucocorticoids or immunomodulators may help reduce inflammation and prevent further disease progression. The indicators used in this analysis are easily obtainable in routine clinical practice, supporting their integration into early diagnostic and management strategies.
Abbreviations
MPP, Mycoplasma pneumoniae pneumonia; SMMP, severe Mycoplasma pneumoniae pneumonia; GMMP, gernal Mycoplasma pneumoniae pneumonia; CAP, community-acquired pneumonia; TNF-α, Tumor Necrosis Factor-α; IFN-γ, Interferon-γ; IL-2, Interleukin-2; IL-4, Interleukin-4; IL-5, Interleukin-5; IL-6, Interleukin-6; IL-17, Interleukin-17; IgG, Immunoglobulin G; IgM, Immunoglobulin M; IgA, Immunoglobulin A; IgE, Immunoglobulin E; WBC, White Blood Cell count; NEU, Neutrophil count; MON, Monocyte count; EC, Eosinophil count; PLT, Platelet count; CRP, C-reactive Protein; ALT, Alanine Aminotransferase; AST, Aspartate Aminotransferase; LDH, Lactate Dehydrogenase; CK-MB, Creatine Kinase-MB isoenzyme; TnI, Cardiac Troponin I; FIB, Fibrinogen; APTT, Activated Partial Thromboplastin Time; DD, D-dimer; ROC, Receiver Operating Characteristic curve; EOS, Eosinophil count.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author, Dr. Shunying Zhao, upon reasonable request.
Ethics Approval and Consent to Participate
The retrospective study was approved by ethics committee of The Seventh Medical Centre, Chinese PLA General Hospital (No. S2025-138-01). This study was conducted in accordance with the declaration of Helsinki. This was a retrospective study involving only the analysis of existing clinical data, with no direct patient contact or intervention; therefore, the ethics committee waived the requirement for informed consent.
Acknowledgments
We thank the staff for their dedicated work in implementing the study’s intervention and evaluation.
Disclosure
The authors declare that they have no competing interests.
References
1. Harris M, Clark J, Coote N, et al. British thoracic society guidelines for the management of community acquired pneumonia in children: update 2011. Thorax. 2011;66(Suppl 2):ii1–10. doi:10.1136/thoraxjnl-2011-200598
2. Brown RJ, Nguipdop-Djomo P, Zhao H, et al. Mycoplasma pneumoniae epidemiology in england and wales: a national perspective. Front Microbiol. 2016;7:157. doi:10.3389/fmicb.2016.00157
3. Gao LW, Yin J, Hu YH, et al. The epidemiology of paediatric Mycoplasma pneumoniae pneumonia in North China: 2006 to 2016. Epidemiol Infect. 2019;147:e192. doi:10.1017/S0950268819000839
4. Wang Z, Peng Y, Yang S, et al. Risk factors for complications of Mycoplasma pneumoniae pneumonia in hospitalized children in China: a systematic review and meta-analysis. BMC Pediatric. 2024;24(1):810. doi:10.1186/s12887-024-05279-9
5. Kim CK, Chung CY, Kim JS, et al. Late abnormal findings on high-resolution computed tomography after Mycoplasma pneumonia. Pediatrics. 2000;105(2):372–378. doi:10.1542/peds.105.2.372
6. Tang Y, Shi C, Sun L, et al. Herb pair of glycyrrhiza radix–platycodonis radix alleviates respiratory syncytial virus pneumonia in mice by modulating lipid metabolism and inhibiting inflammation. World J Tradit Chin Med. 2024;10(3):322–333. doi:10.4103/wjtcm.wjtcm_79_24
7. Li CM, Gu L, Yin SJ, et al. Age-specific Mycoplasma pneumoniae pneumonia-associated myocardial damage in children. The Journal of International Medical Research. 2013;41(5):1716–1723. doi:10.1177/0300060513497559
8. Song JX, Luo L, Tian CL, et al. Clinical characteristics and related factors of childhood Mycoplasma pneumoniae pneumonia with different early imaging findings. 2025;15.
9. Pediatric branch of Chinese medical association, respiratory group, national clinical research center for respiratory diseases, Evidence-Based Guidelines for Diagnosis and Treatment of Mycoplasma Pneumonia in Children (2023). Editorial Committee of Chinese Journal of Pediatrics. 2024;62(12):1137–1144.
10. Shi Y, Liu X, Du J, et al. Circulating cytokines associated with clinical outcomes in advanced non-small cell lung cancer patients who received chemoimmunotherapy. Thorac Cancer. 2022;13(2):219–227. doi:10.1111/1759-7714.14248
11. Ding HR, Tang ZT, Tang N, et al. Protective properties of FOXO1 inhibition in a murine model of non-alcoholic fatty liver disease are associated with attenuation of ER stress and necroptosis. Front Physiol. 2020;11:177. doi:10.3389/fphys.2020.00177
12. Zhang ZL, Ding XF, Tong J, Li BY. Enhanced radiosensitivity in 1,25-dihydroxyvitamin D3 deficient mice. J Radiat Res. 2011;52(2):215–219. doi:10.1269/jrr.10156
13. Martin-Toutain I, Jobic L, Mancic T, Ankri A. Évaluation de l’automate d’hémostase Sysmex(®) CS-2100i (Siemens) pour les tests TCA, TP, fibrinogène, facteurs V et VIII, antithrombine et D-dimères [Evaluation of the automated coagulation analyzer Sysmex(®) CS-2100i (Siemens)]. Ann Biol Clin (Paris). 2011;69(6):699–704. doi:10.1684/abc.2011.0624
14. Bozkaya G, Sisman AR. The comparison of analytical performances of mindray CL-1000i and Beckman coulter access II troponin I methods in the light of recent guidelines and the quality requirements. Ann Transl Med. 2020;8(19):1237. doi:10.21037/atm-20-6104
15. Luo XQ, Luo J, Wang CJ, et al. Clinical features of severe Mycoplasma pneumoniae pneumonia with pulmonary complications in childhood: a retrospective study. Pediatric Pulmonology. 2023;58(10):2815–2822. doi:10.1002/ppul.26593
16. Hardy RD, Jafri HS, Olsen K, et al. Elevated cytokine and chemokine levels and prolonged pulmonary airflow resistance in a murine Mycoplasma pneumoniae pneumonia model: a microbiologic, histologic, immunologic, and respiratory plethysmographic profile. Infect Immun. 2001;69(6):3869–3876. doi:10.1128/IAI.69.6.3869-3876.2001
17. Lieberman D, Livnat S, Schlaeffer F, et al. IL-1beta and IL-6 in community-acquired pneumonia: bacteremic pneumococcal pneumonia versus Mycoplasma pneumoniae pneumonia. Infection. 1997;25(2):90–94. doi:10.1007/BF02113582
18. Zhang Z, Dou H, Tu P, et al. Serum cytokine profiling reveals different immune response patterns during general and severe Mycoplasma pneumoniae pneumonia. Front Immunol. 2022;13:1088725. doi:10.3389/fimmu.2022.1088725
19. Shehata L, Thouvenel CD, Hondowicz BD, et al. Interleukin-4 downregulates transcription factor BCL6 to promote memory B cell selection in germinal centers. Immunity. 2024;57(4):843–58.e5. doi:10.1016/j.immuni.2024.02.018
20. Bajbouj K, Abujabal R, Sahnoon L, et al. IL −5 receptor expression in lung fibroblasts: potential role in airway remodeling in asthma. Allergy. 2023;78(3):882–885. doi:10.1111/all.15627
21. Wang H, Zhang Y, Zhao C, et al. Serum IL-17A and IL-6 in paediatric Mycoplasma pneumoniae pneumonia: implications for different endotypes. Emerging Microbes Infect. 2024;13(1):2324078. doi:10.1080/22221751.2024.2324078
22. Malaviya R, Laskin JD, Laskin DL. Anti-TNFα therapy in inflammatory lung diseases. Pharmacol Ther. 2017;180:90–98. doi:10.1016/j.pharmthera.2017.06.008
23. Ruan JP, Fu Z, Yan P, et al. Comparative analysis of clinical characteristics between severe pneumonia caused by mycoplasma and severe pneumonia caused by streptococcus in children. Front Pediatrics. 2024;42(6):497–502.
24. Fan F, Lv J, Yang Q, et al. Clinical characteristics and serum inflammatory markers of community-acquired mycoplasma pneumonia in children. The Clinical Respiratory Journal. 2023;17(7):607–617. doi:10.1111/crj.13620
25. Wang LP, Hu ZH, Jiang JS, et al. Serum inflammatory markers in children with Mycoplasma pneumoniae pneumonia and their predictive value for mycoplasma severity. World Journal of Clinical Cases. 2024;12(22):4940–4946. doi:10.12998/wjcc.v12.i22.4940
26. Ari M, Ari HF, Cengiz H. Advanced biomarkers for prognostic evaluation of pneumonia severity in pediatric intensive care: focus on novel inflammatory and hematological ratios. Ital J Pediatr. 2025;51(1):168. doi:10.1186/s13052-025-01989-7
27. Jiang Y, Wang W, Zhang Z, et al. Serum amyloid a, C-reactive protein, and procalcitonin levels in children with Mycoplasma pneumoniae infection. J Clin Lab Analysis. 2022;36(3):e24265. doi:10.1002/jcla.24265
28. Lee KL, Lee CM, Yang TL, et al. Severe Mycoplasma pneumoniae pneumonia requiring intensive care in children, 2010-2019. Journal of the Formosan Medical Association. 2021;120(1 Pt 1):281–291. doi:10.1016/j.jfma.2020.08.018
29. Qi X, Sun X, Li X, et al. Significance changes in the levels of myocardial enzyme in the child patients with Mycoplasma Pneumoniae Pneumonia. Cell Mol Biol. 2020;66(6):41–45. doi:10.14715/cmb/2020.66.6.8
30. Jin P, Han C, Guo W, et al. Mycoplasma pneumoniae pneumonia-associated thromboembolism with plastic bronchitis: a series of five case reports and literature review. Italian Journal of pediatrics. 2024;50(1):117. doi:10.1186/s13052-024-01690-1
31. Zheng Y, Hua L, Zhao Q, et al. The level of D-dimer is positively correlated with the severity of Mycoplasma pneumoniae pneumonia in children. Front Cell Infect Microbiol. 2021;11:687391. doi:10.3389/fcimb.2021.687391
32. Cho YJ, Han MS, Kim WS, et al. Correlation between chest radiographic findings and clinical features in hospitalized children with Mycoplasma pneumoniae pneumonia. PLoS One. 2019;14(8):e0219463. doi:10.1371/journal.pone.0219463
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Characteristics and Risk Factors for in-Hospital Mortality in 240 Cases of Infective Endocarditis in a Tertiary Hospital in China: A Retrospective Study
Zhang X, Jin F, Lu Y, Ni F, Xu Y, Xia W
Infection and Drug Resistance 2022, 15:3179-3189
Published Date: 18 June 2022
Clinical Features of Human Brucellosis and Risk Factors for Focal Complications: A Retrospective Analysis in a Tertiary-Care Hospital in Beijing, China
Zhang Z, Zhang X, Chen X, Cui X, Cai M, Yang L, Zhang Y
International Journal of General Medicine 2022, 15:7373-7382
Published Date: 19 September 2022
A Lung Ultrasound-Based Nomogram for the Prediction of Refractory Mycoplasma pneumoniae Pneumonia in Hospitalized Children
Liu G, Wang G, Yang Z, Liu G, Ma H, Lv Y, Ma F, Zhu W
Infection and Drug Resistance 2022, 15:6343-6355
Published Date: 31 October 2022
Maternal and Fetal Risk Factors for Neonatal Hypoxic-Ischemic Encephalopathy: A Retrospective Study
Chen X, Chen H, Jiang D
International Journal of General Medicine 2023, 16:537-545
Published Date: 13 February 2023
Adolescent Non-Puerperal Mastitis: Risk Factors, Clinical Characteristics, and Prognosis Analysis
Tang H, Wu X, Feng J, Gao Q, Shao S, Qu W, Xie L, Sun J
Journal of Inflammation Research 2024, 17:487-495
Published Date: 24 January 2024