Back to Journals » Journal of Inflammation Research » Volume 17
Adolescent Non-Puerperal Mastitis: Risk Factors, Clinical Characteristics, and Prognosis Analysis
Authors Tang H ![]() , Wu X, Feng J, Gao Q, Shao S, Qu W
, Wu X, Feng J, Gao Q, Shao S, Qu W ![]() , Xie L
, Xie L ![]() , Sun J
, Sun J
Received 15 November 2023
Accepted for publication 16 January 2024
Published 24 January 2024 Volume 2024:17 Pages 487—495
DOI https://doi.org/10.2147/JIR.S447181
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Huili Tang, Xueqing Wu, Jiamei Feng, Qingqian Gao, Shijun Shao, Wenchao Qu, Lu Xie, Jiaye Sun
Department of Breast, Shuguang Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, 201203, People’s Republic of China
Correspondence: Xueqing Wu, Department of Breast, Shuguang Hospital, Shanghai University of Traditional Chinese Medicine, 185 Pu ‘an Road, Huangpu District, Shanghai, People’s Republic of China, Tel + 86-13817792022, Fax + 86-200021, Email [email protected]
Purpose: To determine the risk factors, clinical characteristics, and prognosis of adolescent non-puerperal mastitis patients.
Patients and methods: A retrospective analysis was conducted on 10 cases of NPM in adolescents who underwent surgical treatment at Shuguang Hospital affiliated to Shanghai University of Traditional Chinese Medicine from August 2021 to August 2023. We analyze the patient’s general information, clinical characteristics, related medical history, laboratory indicators, breast magnetic resonance imaging examination, postoperative pathology, prognosis, etc.
Results: The clinical manifestations of NPM in adolescents mainly included redness, swelling and pain in the breasts, congenital nipple retraction, and extensive lesion range. Inflammatory markers and prolactin were elevated. Magnetic resonance imaging showed circular enhancement with abscess formation as the main type. All patients underwent surgical treatment with a fast recovery time after surgery. No recurrence was observed during follow-up and the postoperative breast appearance was satisfactory. Multivariate Logistic regression analysis indicated that congenital nipple retraction, elevated prolactin levels and trauma were independent risk factors for adolescents non-puerperal mastitis.
Conclusion: Adolescent non-puerperal mastitis is a rare and unique type. Summarizing its main risk factors, clinical characteristics, and prognosis provides a basis for further research.
Keywords: adolescents, non-puerperal mastitis, risk factors, clinical characteristics, prognosis
Introduction
Non-puerperal mastitis is a chronic inflammatory disease that occurs in the breast during the non-lactation period. It is characterized by a high recurrence rate and long duration. The incidence of NPM is increasing annually. The prevalence of NPM is progressively increasing over the years, constituting 0.3–1.9% of all breast disorders globally, while in China it accounts for 2–5% of all breast lesions.1 A retrospective analysis of 926 patients with NPM who underwent surgical treatment between April 2004 and May 2019 at the Breast Department of Shuguang Hospital revealed that the age range at onset was 13–70 years, with a median age of 31 years. The highest incidence occurred in women aged 21–40, and approximately 65.5% of cases were observed within the first five years after childbirth.2 A foreign study found that non-puerperal mastitis is more prevalent in women aged 26 to 45, with an average age of 35.5 years.3 The disease mainly affects young and middle-aged women, with fewer cases in adolescents.
The current literature on NPM in adolescents is scarce. The records of adolescent breast disease visits at a tertiary referral hospital between January 2009 and December 2011 were reviewed in a study, revealing that out of the 81 patients, 20 (24.7%) were diagnosed with NPM.4 The occurrence of NPM in adolescent breast disease warrants our attention. To date, there is only one retrospective study encompassing 22 adolescent non-puerperal mastitis patients,5 which lacks comprehensive evidence regarding the underlying pathogenesis, treatment approaches, and long-term follow-up.
This study aims to retrospectively analyze various aspects related to NPM in adolescent patients under 20 years old, including general information, clinical characteristics, medical history, laboratory indicators, breast MRI results, pathology findings, prognosis and other relevant factors. By summarizing the disease characteristics specific to adolescent NPM, this study aims to determine the understanding of this particular population affected by the condition.
Materials and Methods
Patients
Ten cases of non-puerperal mastitis in adolescent females admitted to our hospital from August 2021 to August 2023 were included. Inclusion criteria: 1) meeting the NPM diagnostic criteria in the Expert Consensus on Non-Puerperal Mastitis;6 2) females under the age of 20; 3) undergoing surgical treatment without contraindications and signing an informed consent form. Exclusion criteria: 1) patients with primary diseases affecting cardiovascular, liver, kidney, hematopoietic system or other life-threatening conditions; 2) patients with other breast diseases; 3) patients with psychological or mental disorders such as anxiety disorder or depression; and 4) participants with incomplete or lost follow-up data.
Method
General information about the patients (including age, height, weight, duration of illness, etc.) was collected; clinical characteristics of the patients (including etiological factors, lesion location and extent, symptom manifestation, etc.) and relevant medical history (personal diet and lifestyle conditions, past medical history, medication history, family history, trauma history) were recorded. All patients underwent surgical treatment. The adolescents in this study were treated by small incision staging surgery. The initial small incision and drainage procedure was performed to minimize glandular tissue damage and reduce postoperative scarring. Traditional Chinese medicine was also utilized during this period to control inflammation. Subsequently, a second suture plastic surgery was conducted to decrease the risk of recurrence while maintaining optimal breast appearance.
Laboratory indicators of the patients (including white blood cell count, C-reactive protein level, bacterial culture results), breast magnetic resonance imaging examination and postoperative pathology were organized. Prognostic outcomes were statistically analyzed including postoperative recovery time, recurrence rate, and satisfaction with postoperative appearance.
Statistical Analysis
Statistical analyses were performed using SPSS 26. Numerical variables conforming to the normal distribution are described as mean and standard deviation, otherwise as the median and interquartile range. Categorical data were analyzed by using Chi-squared test or Fisher’s exact test, while numerical data using independent t-test or Mann–Whitney test. In addition, multivariable logistic regression analysis was performed with the pathogenesis of adolescent non-puerperal mastitis. P values <0.5 were considered significant.
Results
Analysis of Clinical Characteristics
The clinical characteristics of NPM in adolescents are shown in Table 1. There were a total of 10 adolescent patients, ranging in age from 13 to 19 years, with a mean age of 16.40 ± 2.06. Among them, there were 4 (40.0%) patients aged 15 years and younger, while the remaining 6 (60.0%) patients were over the age of 15. The average duration of the disease course for these adolescents was (1.75 ± 1.27) months. Nipple involvement was observed in 90% of adolescents, while skin redness was present in 80% of them. All ten cases (100%) reported breast swelling and pain as their primary symptoms, while seven cases (70%) displayed multifocal breast lesions spanning across two quadrants. The average size of breast masses measured approximately (104.50 ±52 0.21) cm², with five cases exhibiting sizes around or equal to 100cm² and four cases showing sizes smaller than 100cm².
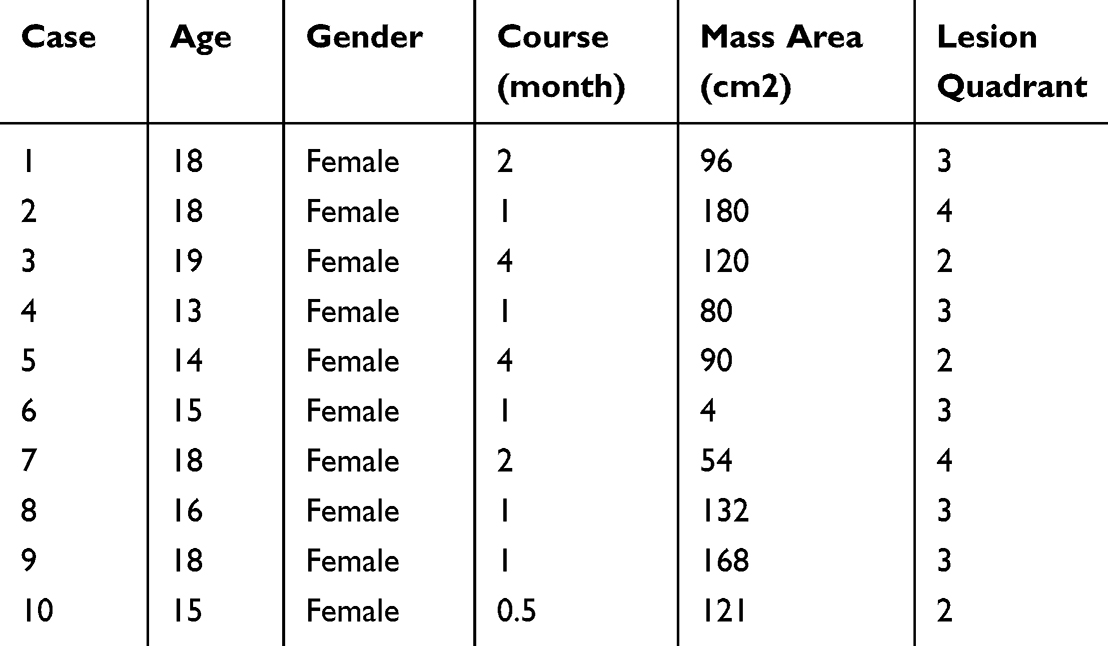 |
Table 1 Clinical Characteristics Analysis of 10 Cases of Adolescent NPM |
The Etiology Analysis
The etiology analysis specifically focused on NPM in adolescents is available in Table 2. Four cases (40%) of patients had a recent history of breast trauma. Nine cases (90.0%) exhibited congenital nipple depression, while 2 cases (22.2%) presented with three-degree nipple depression. Papillary discharge was observed in 2 patients (20%), while preoperative serum prolactin levels were elevated in 8 patients (80%), with one patient having a level exceeding 1000 mlU/L. Only one patient (10.0%) had a documented history of pituitary tumor prior to the study.
 |
Table 2 Etiological Analysis of 10 Cases of Adolescent NPM |
Results Analysis of the Laboratory Indicators
The white blood cell (WBC) counts were elevated in 10 adolescent NPM, with one patient (10%) exhibiting a count exceeding 20×109/L and four patients (40%) having counts ranging from 10×109/L to 20×109/L. The levels of C-reactive protein were observed to be increased in all ten individuals (100%). Only one patient (10.0%) tested positive for S. aureus, while the remaining cases showed no bacterial infection.
Analysis of Magnetic Resonance Imaging Features of the Breast
All ten adolescent NPM patients included in this study underwent preoperative breast MRI imaging. The observed MRI signs indicated non-mass enhancement, characterized by prominent ring enhancement and vindication of the inner wall, indicative of pus formation in Figure 1. Epidermal thickening and edema were present in five patients (50%) as depicted in Figure 2.
 |
Figure 1 The ring exhibits enhanced and uniformly smooth inner wall morphology. |
 |
Figure 2 Epidermal hypertrophy and tissue swelling. |
Postoperative Pathology
One case (10%) exhibited typical cystic neutrophilic granulomatous mastitis (CNGM),7 characterized by the presence of non-caseous granuloma formation with a central granuloma surrounded by neutrophils and an inflammatory granuloma structure in the outer circle, as depicted in Figure 3. Conversely, the remaining nine patients (90%) displayed dilated tal expansion along with acute and chronic inflammatory cell infiltration, as illustrated in Figure 4.
 |
Figure 3 Typical pathological characteristics observed in cystic neutrophilic granulomatous lobular mastitis. (H&E staining, 100x). |
 |
Figure 4 Catheter dilation accompanied by infiltration of acute and chronic inflammatory cells. (H&E staining, 100x). |
Prognostic Situation
Nine patients (90%) of the adolescents achieved complete healing within one month, with a mean postoperative healing time of 21.60 ± 6.13 days. Notably, no cases exhibited any signs of recurrence. Furthermore, the patients were assessed for their level of satisfaction with the postoperative breast appearance using a scoring system ranging from 1 (very unsatisfactory) to 5 (very satisfactory), and the average score for breast appearance satisfaction was found to be 4.30 ± 0.67, indicating a generally high level of satisfaction among the participants in this study.
Multivariate Analysis of Factors Influencing the Incidence of Adolescent NPM
Multivariate logistic regression analysis was conducted to examine the association between adolescent NPM and various factors including general data, clinical characteristics, laboratory indicators, and prognosis. The findings revealed that nipple invagination, elevated prolactin levels, and trauma were identified as independent risk factors for NPM in adolescents (P <0.05), as presented in Table 3.
 |
Table 3 Multivariate Analysis of Factors Influencing the Incidence of Adolescent NPM |
Discussion
In this study, a cohort of 10 adolescent patients was included to analyze the risk factors, clinical characteristics, and prognosis in order to comprehensively summarize the disease characteristics of NPM in adolescents. This research endeavor aims to enhance clinicians’ understanding, diagnosis, and treatment proficiency specifically tailored for this unique age group, thereby contributing towards improving patient care outcomes.
NPM presents a range of symptoms, including breast mass, breast pain, nipple discharge, breast sinus tract, erythema of lower extremity nodules, and fever as its clinical manifestations. Moreover, it exhibits a high tendency for relapse and poses challenges in terms of delayed healing. In this study encompassing 10 adolescent NPM patients, the primary and predominant symptom observed was breast redness accompanied by heat and pain. Notably, 7 cases (70%) exhibited lesions extending beyond 2 quadrants with a considerable average mass size. Additionally, there was a notable incidence of nipple discharge alongside a relatively short disease duration. These findings underscore the urgent onset and brief course of the disease among teenagers while highlighting their main clinical manifestations characterized by redness, heat, and pain.
NPM is a multifactorial disease with a complex etiology. Risk factors for morbidity may include autoimmune dysfunction, bacterial infection, mammary ductal occlusion, hormone secretion disorders, smoking, and medication use.8,9 Our study identified nipple invagination, elevated prolactin levels, and trauma as independent risk factors for NPM in adolescents. These findings contribute to the understanding of the pathogenesis of this condition and may inspire future prevention strategies.
It has been reported that nipple invagination is a common complication in NPM patients, with a prevalence ranging from 46% to 87.5%.10 These findings align with the results of our study, where nipple depression also emerges as a prominent factor among adolescents. The underlying mechanism may involve inward traction and subsidence of the nipple due to abnormal breast development, shortened breast ducts, or fibrosis contracture in adolescent females. Papillary invagination can lead to the accumulation of breast duct contents and subsequent inflammation.
Several other studies have reported an association between NPM and elevated prolactin levels.11 In a literature review conducted by Anatoly Nikolaev et al12 out of 260 patients with granulomatous lobular mastitis, four exhibited hyperprolactinemia along with pituitary microadenomas, as pituitary disorders are known to contribute to hyperprolactinemia. In our study, nine patients (90%) displayed abnormal elevation in prolactin levels, one of whom had a history of a pituitary tumor. These findings suggest that prolactin plays a role in the development of NPM among adolescents. It could be attributed to the ability of hyperprolactinemia to modulate signaling pathways in immune cells and mammary epithelial cells, leading to the production of pro-inflammatory cytokines and promoting inflammatory responses associated with NPM.13 Female puberty is a crucial phase characterized by the vigorous development of endocrine functions. Any aberrations in hormone secretion levels can trigger an upsurge in prolactin release, thereby leading to excessive mammary duct secretion. Consequently, this results in ductal expansion and secretion’s overflow into the lobular connective tissue, causing localized inflammatory reactions and ultimately inducing non-puerperal mastitis.
In this study, 40% of adolescent female patients had a recent history of breast trauma, which was identified as an independent risk factor for NPM. Notably, local bumping of the breast was found to be the second most significant risk factor after hyperprolactinemia.14 Due to their lack of awareness and rapid breast development, young women are particularly susceptible to traumatic injury that can lead to bacterial infection and subsequent mastitis. In cases where trauma is the cause, inflammation-induced symptoms such as redness, heat and pain will be more severe in adolescent NPM patients.
The latest study revealed a disparity in the composition of breast tissue flora between healthy individuals and NPM patients. Tsai et al15 identified coagulase-negative staphylococci as the most prevalent pathogen, followed by Corynebacterium. However, our investigation primarily observed aseptic inflammation among adolescent NPM patients, with one case exhibiting Staphylococcus aureus infection. This finding aligns with Stricker et al’s summary of 22 adolescent patients, where three cases detected S. aureus.5 Additionally, Hao Xiaoying’s domestic study also suggests that Staphylococcus aureus may be the predominant pathogenic bacterium responsible for non-puerperal mastitis in adolescents.16 Therefore, we hypothesize that most cases of adolescent non-puerperal mastitis are characterized by aseptic inflammation; however, bacterial infections such as Staphylococcus aureus can also occur concurrently.
MRI plays a crucial role in the diagnosis and treatment of NPM. Aslan et al’s study demonstrated that MRI had a significantly higher detection rate for NPM than color Doppler ultrasound and breast X-ray photography.17 In another investigation by Zhang et al, the accuracy of MRI assessment in determining the extent of NPM lesions was reported as 88.9%, surpassing ultrasound and X-ray breast photography assessments.18 More than 90% of these patients exhibited MRI signs indicating non-mass enhancement. Interestingly, adolescent women with NPM displayed ring enhancement on MRI imaging, suggesting the presence of purulent cavities, predominantly large ones. This finding provides evidence that abscess formation is prevalent in adolescent cases of NPM. Furthermore, additional investigations have revealed a positive correlation between elevated prolactin levels and abscess formation.19 The majority of adolescents diagnosed with NPM exhibit increased prolactin levels and primarily present with an abscess type manifestation, thereby further supporting the association between prolactin level and abscess development.
The treatment approaches for NPM in adolescent resemble those used for non-lactating individuals, encompassing antibiotics, hormonal therapy, surgical intervention, and traditional Chinese medicine. Currently, there is no literature documenting specific treatments tailored to adolescent NPM; however, due to the distinctive clinical manifestations observed in this age group, abscess formation is frequently encountered necessitating surgical management as the optimal choice.
In this study, the postoperative pathology revealed one case suggesting cystic neutrophil granulomatous mastitis(CNGM) with distinctive pathological characteristics, while the remaining cases exhibited ductal dilatation and acute and chronic inflammation. CNGM is a recently discovered form of non-puerperal mastitis characterized by unique pathological features. CNGM predominantly affects women in their childbearing years and presents with pronounced inflammatory response. The international recognition of this condition as CNGM occurred after 2011. Currently, there are limited reported cases both domestically and internationally. The finding of this study complements the research conducted by Shao et al7 and demonstrates that CNGM can also occur in adolescents, not just women of childbearing age. However, further data are required to summarize the pathological features of NPM in adolescents comprehensively.
The findings of this study demonstrate that adolescent patients exhibit a swift postoperative recovery period, absence of recurrence in the current follow-up cohort, and substantial contentment with their postoperative breast aesthetics. Additionally, during the follow-up phase, we observed one individual experiencing normal breast lactation. These results underscore the favorable prognosis associated with surgical intervention for NPM in adolescents, characterized by expedited healing, minimal recurrence rates, and heightened satisfaction regarding postoperative breast appearance.
Conclusion
In conclusion, our findings suggest that during adolescence, the occurrence of NPM may be associated with elevated levels of prolactin, nipple invagination, trauma, and bacterial infection. Notably, nipple invagination, increased prolactin levels, and trauma emerge as significant risk factors for adolescent onset. The unique clinical characteristics of adolescent NPM primarily manifest in abscess formation accompanied by evident local inflammatory response, a high inflammatory index, rapid healing process, favorable prognosis and low recurrence rate.
The present study provides a comprehensive overview of the risk factors, clinical manifestations, and prognosis associated with adolescent non-puerperal mastitis through retrospective case analysis. It is evident that adolescent non-puerperal mastitis possesses distinct characteristics, thereby enhancing clinicians’ comprehension of this condition. Consequently, it becomes imperative to recognize adolescent non-puerperal mastitis as an independent disease in order to facilitate early diagnosis, prompt intervention, rigorous follow-up. It will enable us to establish guidelines for the diagnosis and treatment of adolescent non-puerperal mastitis.
Furthermore, it is important to acknowledge that this retrospective study possesses certain limitations; therefore, subsequent studies are warranted to validate our findings and further elucidate the underlying causes.
Abbreviations
NPM, non-puerperal mastitis; MRI, Magnetic resonance imaging; CNGM, cystic neutrophilic granulomatous mastitis.
Ethics Approval
This study was approved by the ethics committee of Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine (approval no.2021-956-31-02). Written informed consent was obtained from all the participants for the publication of this study. We certify that the study was performed in accordance with the 1964 declaration of HELSINKI and later amendments. The written informed consent was obtained from the parents/legal guardians of patients under the age of 18. All patients/parents/legal guardians gave their informed consent for case details and any accompanying images published.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yang XQ, Zheng LF, Chen FX, et al. Efficacy analysis of the triple therapy with isoniazid + rifampicin + pyrazinamide in treating non-lactational mastitis. J Mathem Med. 2021;34(05):733–735.
2. Wan H, Lu DM. Non-lactational mastitis. Shanghai: Shanghai Scientific and Technical Publishers; 2022:28.
3. Verghese BG, Ravikanth R. Breast abscess, an early indicator for diabetes mellitus in non-lactating women: a retrospective study from rural India. World J Surg. 2012;5:1195–1198.
4. Michala L, Tsigginou A, Zacharakis D, et al. Breast disorders in girls and adolescents. Is there a need for a specialized service? J Pediatr Adolesc Gynecol. 2015;2(2):91–94. doi:10.1016/j.jpag.2014.05.011
5. Stricker T, Navratil F, Forster I, et al. Nonpuerperal mastitis in adolescents. J Pediatr. 2006;2:278–281.
6. Zhou F, Liu L, Yu ZG. Expert consensus on the diagnosis and treatment of non-lactational mastitis. Chinese J Pract Sur. 2016;36(07):755–758.
7. Shao S, Wu L, Wu X, et al. Clinical and prognostic characteristics analysis of cystic neutrophilic granulomatous mastitis. J Capit Univ Med Sci. 2023;44(04):676–683.
8. Wei LG, Han M. Advances in the diagnosis and treatment of non-lactational mastitis. J Pra Med. 2022;38(09):1161–1165.
9. Barreto DS, Sedgwick EL, Nagi CS, et al. Granulomatous mastitis: etiology, imaging, pathology, treatment, and clinical findings. Breast Cancer Res Treat. 2018;3(3):527–534. doi:10.1007/s10549-018-4870-3
10. Song XY, Zhou XQ, Wang Y, et al. Clinical study on risk factors for the onset of granulomatous mastitis and plasma cell mastitis. J Liaoning Univ Traditional Chin Med. 2021;23(11):138–142.
11. Zhao M, Wang C, Zhu Q, et al. Risk factor analysis and prediction model establishment of non-puerperal mastitis. Chin J Med. 2021;56(05):497–500.
12. Nikolaev A, Blake CN, Carlson DL. Association between Hyperprolactinemia and Granulomatous Mastitis. Breast J. 2016;22(2):224–231. doi:10.1111/tbj.12552
13. Salgado-Lora MG, Medina-Estrada I, López-Meza JE, et al. Prolactin and estradiol are epigenetic modulators in bovine mammary epithelial cells during Staphylococcus aureusInfection. Pathogens. 2020;9(7):520–530. doi:10.3390/pathogens9070520
14. Xiao Q, Zhang CJ. Modern research advances in non-lactating mastitis. Med Philos. 2013;34(3):8–13.
15. Tsai MJ, Huang WC, Wang JT, et al. Factors associated with treatment duration and recurrence rate of complicated mastitis. J Microbiol Immunol Infect. 2020;53(6):875–881. doi:10.1016/j.jmii.2020.03.028
16. Hao XY, Liang TT, Hao M. Breast gland problems in pediatric and adolescent women. Chin J Fam Plan Gynecotokol. 2019;11(12):13–14.
17. Aslan S, Pourbagher A, Colakoglu T. Idiopathic granulomatous mastitis: magnetic resonance imaging findings with diffusion MRI. Acta Radiol. 2016;57(7):796–801. doi:10.1177/0284185115609804
18. Zhang CJ, Fan PZ, Liu P, et al. The application value of dynamic magnetic resonance imaging in the surgical evaluation of granulomatous mastitis. Chin J Mod Med. 2012;22(21):86–89.
19. Du NN, Feng JM, Wu XQ. Correlation analysis between MRI manifestations and pathology of granulomatous lobular mastitis. J Med Imaging. 2023;33(06):1003–1007.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Characteristics and Prognostic Risks of Philadelphia-Negative Myeloproliferative Neoplasms at Cipto Mangunkusumo General Hospital
Sukrisman L
Journal of Blood Medicine 2022, 13:495-503
Published Date: 12 September 2022
Association Between Breakfast Consumption and Suicidal Attempts in Adolescents
Park H, Lee K
Psychology Research and Behavior Management 2022, 15:2529-2541
Published Date: 13 September 2022
Clinical Features of Human Brucellosis and Risk Factors for Focal Complications: A Retrospective Analysis in a Tertiary-Care Hospital in Beijing, China
Zhang Z, Zhang X, Chen X, Cui X, Cai M, Yang L, Zhang Y
International Journal of General Medicine 2022, 15:7373-7382
Published Date: 19 September 2022
Maternal and Fetal Risk Factors for Neonatal Hypoxic-Ischemic Encephalopathy: A Retrospective Study
Chen X, Chen H, Jiang D
International Journal of General Medicine 2023, 16:537-545
Published Date: 13 February 2023
Clinical Implications and Novel Insights into Adolescent Primary Liver Cancer: A Nightmare for Adolescents?
Guo H, Chen X, Li R, Shen J, Gan D, Yin Y, Zhang H, Xie J, Xie L, Liu Y
Journal of Hepatocellular Carcinoma 2025, 12:2513-2540
Published Date: 7 November 2025