Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Clinical and Pathological Features of Chinese Patients with Type 2 Diabetes, Biopsy-Proven Diabetic Kidney Disease, and Rapid eGFR Decline
Authors Qin C, Wang Y ![]() , Zhao L, Zhang J, Ren H, Zou Y, Wu Y, Wang T, Zhao Y, Zhang R, Xu H, Zhang J, Cooper ME, Liu F
, Zhao L, Zhang J, Ren H, Zou Y, Wu Y, Wang T, Zhao Y, Zhang R, Xu H, Zhang J, Cooper ME, Liu F ![]()
Received 4 July 2022
Accepted for publication 2 September 2022
Published 16 September 2022 Volume 2022:15 Pages 2847—2856
DOI https://doi.org/10.2147/DMSO.S381052
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Chunmei Qin,1– 3 Yiting Wang,1,2 Lijun Zhao,1,2 Junlin Zhang,1,2 Honghong Ren,1,2 Yutong Zou,1,2 Yucheng Wu,1,2 Tingli Wang,1,2 Yuancheng Zhao,1,2 Rui Zhang,1,2 Huan Xu,4 Jie Zhang,5 Mark E Cooper,6 Fang Liu1,2
1Division of Nephrology, West China Hospital of Sichuan University, Chengdu, People’s Republic of China; 2Laboratory of Diabetic Kidney Disease, Centre of Diabetes and Metabolism Research, West China Hospital of Sichuan University, Chengdu, People’s Republic of China; 3Department of Nephrology, Luzhou People’s Hospital, Luzhou, People’s Republic of China; 4Division of Pathology, West China Hospital of Sichuan University, Chengdu, People’s Republic of China; 5Key Laboratory of Transplant Engineering and Immunology, Chengdu, People’s Republic of China; 6Department of Diabetes, Central Clinical School, Monash University, Melbourne, Australia
Correspondence: Fang Liu, Division of Nephrology, West China Hospital of Sichuan University, No. 37, Guoxue Alley, Chengdu, Sichuan, 610041, People’s Republic of China, Tel +86-28-18980601214, Fax +86-28-85422335, Email [email protected]
Objective: The rate of kidney function decline in patients with diabetic kidney disease (DKD) is known to differ. This study analyzed the clinicopathologic features and related risk factors affecting long-term renal survival in Chinese type 2 diabetic patients with rapid estimated glomerular filtration rate (eGFR) decline.
Methods: In this retrospective descriptive study, 191 DKD patients were first classified as rapid eGFR decliners and slow eGFR decliners on the basis of the median eGFR slope value (− 8.0 mL/min/1.73 m2/year). In total, 96 patients with rapid eGFR decline were included in the analyses and subsequently allocated to end-stage renal disease (ESRD) and non-ESRD groups. Baseline clinicopathological data of rapid eGFR decliners were collected. Cox proportional hazard analysis was performed to calculate the hazard ratios (HRs) for progression to ESRD.
Results: During a median follow-up of 25 months, 52 (54.2%) rapid eGFR decliners progressed to ESRD. These 52 rapid eGFR decliners had poorer renal function, lower hemoglobin and albumin concentrations, higher total cholesterol and baseline proteinuria levels, and more severe interstitial inflammation than those who did not progress to ESRD. After adjustment for age, gender, baseline eGFR, proteinuria, hemoglobin level, serum albumin concentration, and histopathologic parameters, multivariate Cox proportional hazard analysis revealed that eGFR (HR 0.973, 95% CI 0.956– 0.989) and proteinuria (HR 1.125, 95% CI 1.030– 1.228) were associated with the increased risk of progression to ESRD.
Conclusion: Higher proteinuria and lower eGFR were independent risk factors for renal progression in Chinese patients with type 2 diabetes and rapid eGFR decline.
Keywords: diabetic kidney disease, rapid eGFR decline, clinical, pathological, type 2 diabetes
Introduction
Diabetic kidney disease (DKD) is the main cause of end-stage renal disease (ESRD) and a global socioeconomic burden.1 DKD can coexist with other renal pathologies, such as IgA nephropathy and membranous nephropathy. At present, the gold standard for DKD diagnosis is the pathological examination of renal biopsies.
The characteristic histopathologic changes in DKD include glomerular basement membrane thickening, podocyte foot-process effacement, mesangial matrix expansion, and formation of Kimmelstiel–Wilson nodules, ultimately leading to interstitial fibrosis and tubular atrophy (IFTA), and diffuse glomerulosclerosis.2 The clinical onset of DKD typically involves diagnosis of microalbuminuria or a reduction in the glomerular filtration rate (GFR). However, DKD is a complex disease with a high degree of heterogeneity, and various clinical manifestations may be observed. For example, a recent analysis of autopsies revealed that some patients with DKD never develop microalbuminuria.3 Conversely, a progressive decline in GFR precedes ESRD, which has recently been established as the predominant clinical feature of DKD.4–6 In general, renal function in DKD patients declines gradually, although some DKD patients can experience a sudden decline and quickly reach ESRD. DKD patients who experience a rapid decline in renal function frequently demonstrate an increased risk of cardiovascular disease and higher all-cause mortality.7,8 Notably, in a cohort of French patients with type 2 diabetes, the annual GFR decline was more pronounced in individuals with major cardiovascular events than in those without (−3.0 vs −1.7 mL/min/1.73 m2/year).7 These results suggest that physicians should pay more attention to the rate of GFR decline, and the risk factors affecting renal disease progression and prognosis in DKD patients.
In a recent study involving Japanese DKD patients, the clinicopathological features of fast estimated glomerular filtration rate (eGFR) decliners were evaluated.9 However, the risk factors for progression to ESRD in rapid eGFR decliners were not analyzed. Moreover, no comparable studies have been conducted in China. Therefore, to better understand the course of DKD in Chinese patients, we conducted a retrospective study of type 2 diabetes patients with biopsy-proven DKD and rapid eGFR decline. A major aim was to identify independent risk factors affecting renal prognosis.
Materials and Methods
Patient Selection
A total of 523 patients with type 2 diabetes mellitus (T2DM) who underwent renal biopsies at West China Hospital, Sichuan University, between January 2010 and January 2019 were analyzed. The indications for renal biopsy in this study were T2DM patients with renal damage who lacked absolute contraindications, especially patients without diabetic retinopathy (DR) or with obvious glomerular hematuria and/or short diabetic duration, and patients with sudden onset overt proteinuria. The diagnostic criteria for T2DM were based on the recommendations of the American Diabetes Association.10 DKD was diagnosed by at least two renal pathologists and/ or nephrologists based on the Renal Pathology Society (RPS) classification.11 The trajectories of eGFR decline were evaluated using a simple linear model. Using the median eGFR slope value (−8.0 mL/min/1.73 m2/year) from the present study, patients with T2DM and DKD with an eGFR of ≤−8.0 mL/min/1.73 m2/year were defined as rapid eGFR decliners. The exclusion criteria were as follows: (1) coexisting nondiabetic renal disease; (2) serum creatinine levels measured less than three times during follow-up; (3) eGFR < 15 mL/min/1.73 m2; (4) follow-up time < 1 year; (5) eGFR slope > −8.0 mL/min/1.73 m2/year. Overall, 191 DKD patients were classified into rapid eGFR decliners and slow eGFR decliners using the median eGFR slope value (−8.0 mL/min/1.73 m2/year). A total of 96 patients with rapid eGFR decline were included in the analyses and subsequently allocated to ESRD and non-ESRD groups (Figure 1).
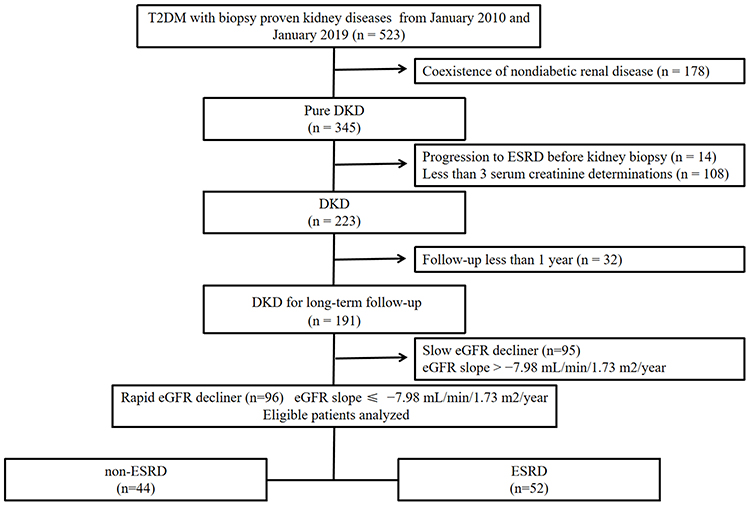 |
Figure 1 Flowchart of study participants. |
Written informed consent was obtained from all patients before kidney biopsy for study participation. The study protocol was reviewed and approved by the Ethics Committee of West China Hospital. The study protocol conformed to the principles of the Declaration of Helsinki.
Clinical and Renal Pathologic Data
Clinical data were collected from the electronic records system of our hospital. Data on demographic parameters and clinical variables were collected at or close to the time of renal biopsy. These included age, gender, body mass index, systolic/diastolic blood pressure, duration of diabetes, presence of DR, presence of hypertension, fasting blood glucose, glycosylated hemoglobin, serum albumin, 24-h urinary protein, blood urea nitrogen, serum creatinine, hemoglobin, uric acid, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, total cholesterol, and eGFR, which was calculated using the Chronic Kidney Disease (CKD) Epidemiology Collaboration creatinine equation.12 DR was diagnosed through optical coherence tomography and fundus color photography and was defined as present if any of the following lesions were detected: microaneurysms, retinal hemorrhages, soft exudates, hard exudates, or vitreous hemorrhage.13 The renal biopsy specimens were processed for light microscopy, immunofluorescence, and electron microscopy. For the light microscopy studies, hematoxylin and eosin, periodic acid Schiff’s, periodic Schiff-methenamine, and Masson’s trichrome stainings were performed. Immunofluorescence staining was performed to detect IgA, IgG, IgM, C3, C4, C1q, Fib, and κ/λ light chains. At least two pathologists independently graded the lesions based on the criteria of the Renal Pathology Society for glomerular alterations, interstitial inflammation, IFTA, and arteriolar hyalinosis.11
Renal Outcome
Renal outcome was defined as progression to ESRD with eGFR < 15 mL/min/1.73 m2 or the commencement of renal replacement therapy. All patients enrolled between 2010 and 2019 were followed until December 2019.
Statistical Analysis
Statistical analysis was performed using SPSS software, version 22.0 (IBM Inc., Armonk, NY, USA). Quantitative variables with a normal distribution are expressed as the mean ± standard deviation (SD). Data with a skewed distribution are expressed as the median (range), and categorical data are presented as frequencies (n) and percentages (%). Differences between continuous variables were assessed using the t-test or the Wilcoxon test, whereas categorical variables were analyzed using the chi-square test or Fisher’s exact test. Kaplan–Meier analysis was used for renal survival analysis, and survival rates were compared with the Log rank test. Univariable and multivariable logistic regressions were performed to assess the association between risk factors and a rapid decline in eGFR. Univariate and multivariable Cox proportional hazard models were used to evaluate hazard ratios (HRs) and 95% confidence intervals (CI) for ESRD.
Results
Baseline Clinical and Laboratory Characteristics
The baseline characteristics of 191 DKD patients and slow eGFR decliners are shown in Supplemental Tables 1 and 2, respectively. The baseline clinical characteristics of the 96 rapid eGFR decliners are shown in Table 1. Briefly, 68.8% (66/96) of the patients were men, and the mean age was 48.6 ± 10.6 years. At the time of biopsy, median eGFR and proteinuria were 58 (43, 90) mL/min/1.73 m2 and 4.8 (2.6, 8.4) g/24 h, respectively. Compared with patients who did not progress to ESRD, patients who progressed to ESRD had lower baseline eGFR (49 [35, 65] vs 79 [57, 99] mL/min/1.73 m2, P < 0.001), lower serum albumin (31.1 ± 7.0 vs 35.4 ± 6.9 g/L, P = 0.003), and lower hemoglobin levels (106 ± 20 vs 125 ± 27 g/L, P < 0.001), but higher proteinuria (6.1 [3.6, 9.6] vs 2.9 [1.8, 6.8] g/24 h, P = 0.002) and total cholesterol levels (5.63 ± 1.82 vs 5 ± 1.20 mmol/L, P = 0.046). The proportion of patients in early stages (stage 1 and 2) of CKD who did not progress to ESRD was higher than the proportion who did (68.2 vs 26.9%). No differences were observed in terms of gender, age distribution, body mass index, systolic/diastolic blood pressure, duration of diabetes, or baseline fasting blood glucose levels between the two groups. Moreover, no significant differences were observed in the use of medications between the two groups. Notably, the proportion of patients treated with RAAS inhibitors who did not progress to ESRD was higher than the proportion who did (88.6 vs 73.1%, P = 0.057, although with borderline significance).
 |
Table 1 Baseline Clinical Features of Rapid eGFR Decliners Overall and Divided into Non-ESRD and ESRD Groups |
Histopathological Features
All patients included in this study underwent renal biopsy. The baseline histopathological characteristics of DKD patients and slow eGFR decliners are shown in Supplemental Tables 3 and 4, respectively. Based on the 2010 pathological classification of DKD, the rapid eGFR decliners included here were distributed as follows: class I with glomerular basement membrane thickening alone, 3 (3.1%); class II with mesangial expansion, 28 (29.2%); class III with nodular sclerosis, 45 (46.9%); and class IV with advanced diabetic glomerulosclerosis, 20 (20.8%). Hence, the glomerular histopathologic class III was the most common type. Additional factors, including IFTA and interstitial inflammation and arteriolar hyalinosis scores, are also reported in Table 2. Overall, patients with ESRD exhibited more severe interstitial inflammation (P = 0.023) than those without ESRD. However, no significant differences in IFTA or arteriolar hyalinosis scores were observed between the two groups. Moreover, immunofluorescence analysis revealed no significant difference between the ESRD and non-ESRD groups.
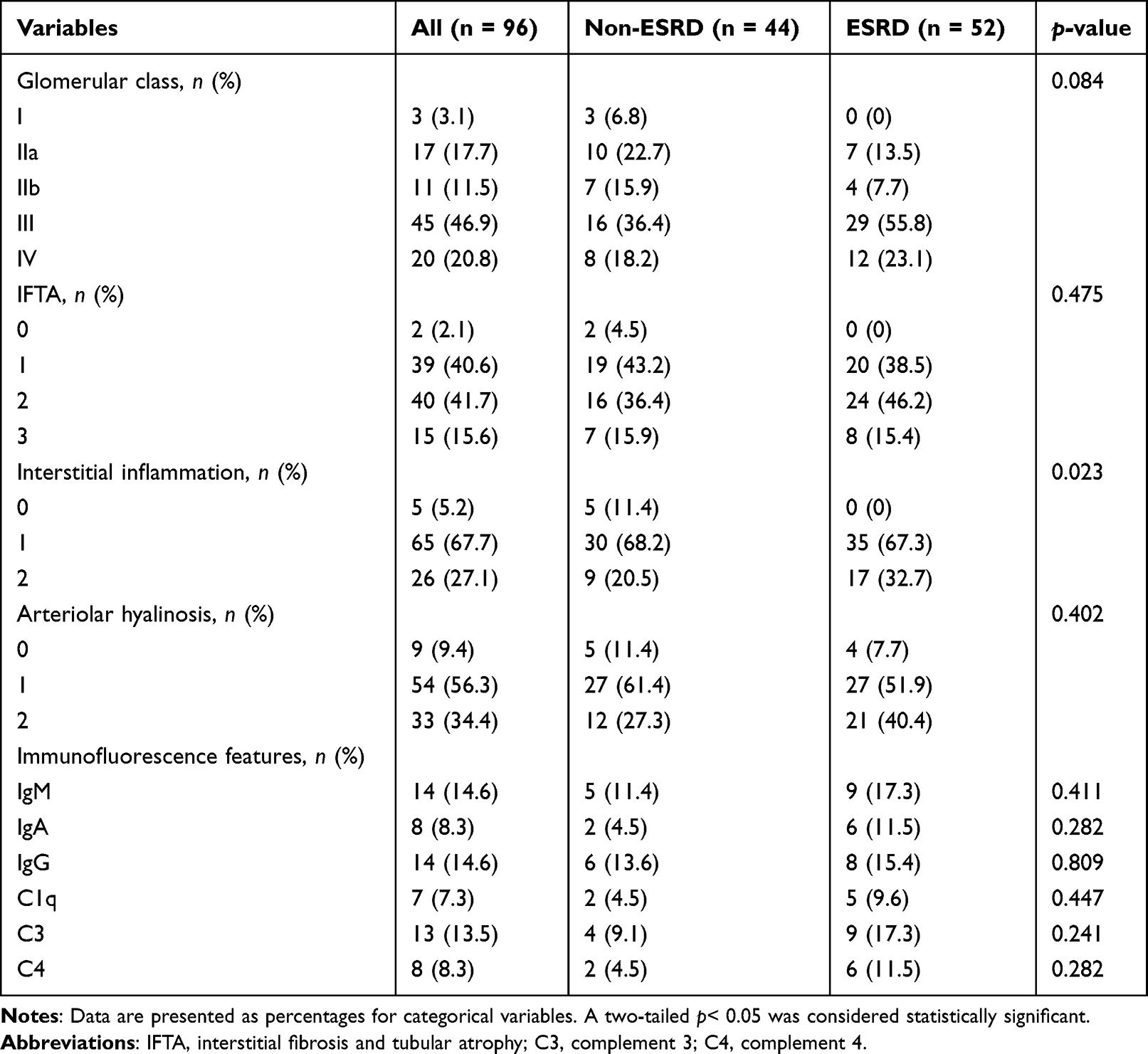 |
Table 2 Baseline Pathological Features of Rapid eGFR Decliners |
Risk Factors Associated with Rapid eGFR Decline
As shown in Table 3, the univariate logistic regression demonstrated that age [odds ratio (OR) 0.962, 95% CI 0.935–0.991, P = 0.01], proteinuria (OR 1.143, 95% CI 1.055–1.239, P = 0.001), and interstitial inflammation (OR 1.773, 95% CI 1.015–3.096, P = 0.044) were associated with a rapid decline in eGFR. Furthermore, the multivariable logistic regression indicated that higher degree of proteinuria (OR 1.151, 95% CI 1.054–1.256, P = 0.002) was independently associated with a rapid decline in eGFR.
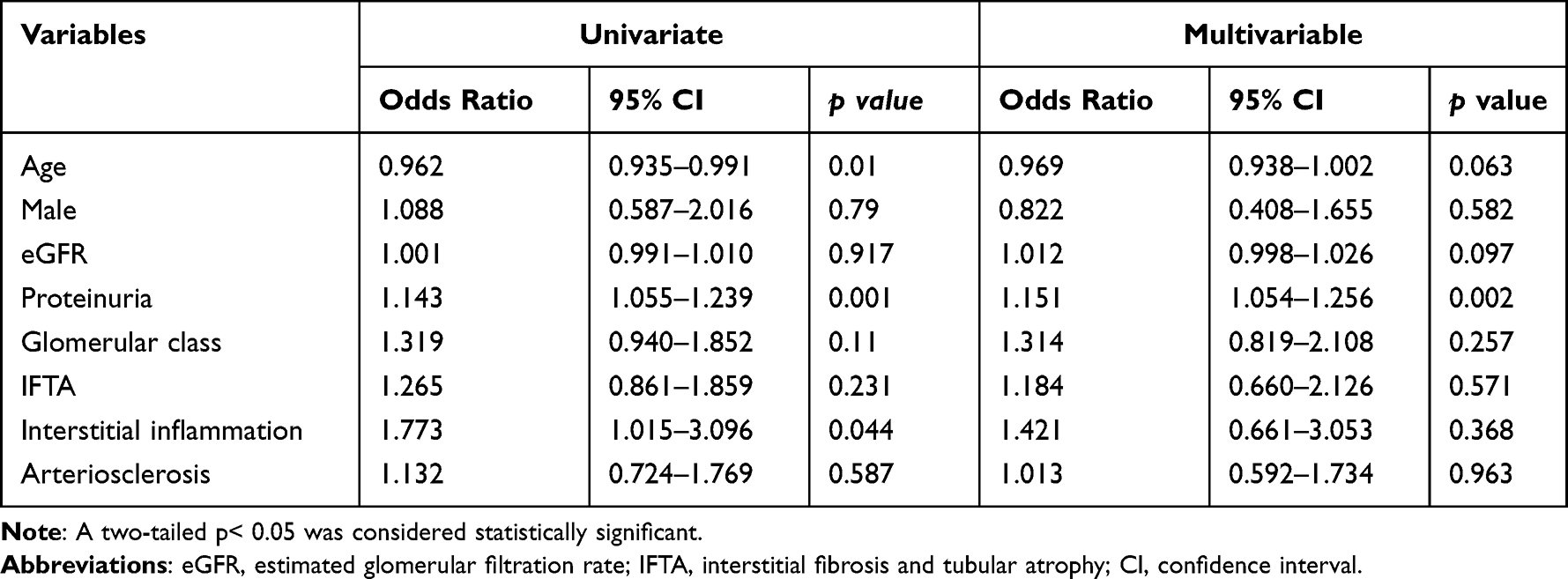 |
Table 3 Logistic Regression Analyses of Patients with Diabetic Kidney Disease |
Clinical and Pathological Risk Factors for ESRD
During a median follow-up period of 25 months, 52 patients (54.2%) with rapid eGFR decline progressed to ESRD. The overall 3-year and 5-year renal survival rates were estimated to be 44.4% and 10.8%, respectively. Kaplan–Meier curves demonstrated that baseline proteinuria was significant for ESRD in rapid eGFR decliners (Figure 2). Univariable Cox proportional hazard analysis revealed that baseline eGFR (HR 0.960, 95% CI 0.946–0.974, P < 0.001), proteinuria (HR 1.140, 95% CI 1.078–1.204, P < 0.001), hemoglobin level (HR 0.974, 95% CI 0.963–0.984, P < 0.001), serum albumin concentration (HR 0.928, 95% CI 0.893–0.964, P < 0.001), glomerular lesion (HR 2.211, 95% CI 1.129–4.332, P = 0.021), and interstitial inflammation (HR 2.228, 95% CI 1.234–4.022, P = 0.008) were associated with ESRD in rapid eGFR decliners. After adjustment for age, gender, baseline eGFR, proteinuria, hemoglobin level, serum albumin concentration, and histopathological parameters, baseline eGFR (HR 0.973, 95% CI 0.956–0.989, P = 0.001) and proteinuria (HR 1.125, 95% CI 1.030–1.228, P = 0.009) were found to be independent risk factors for progression to ESRD in rapid eGFR decliners (Table 4). In addition, multivariate Cox proportional hazard analysis revealed that interstitial inflammation (HR 4.598, 95% CI 1.470–14.378, P = 0.009) was an independent risk factor for progression to ESRD in slow eGFR decliners (Supplemental Table 5).
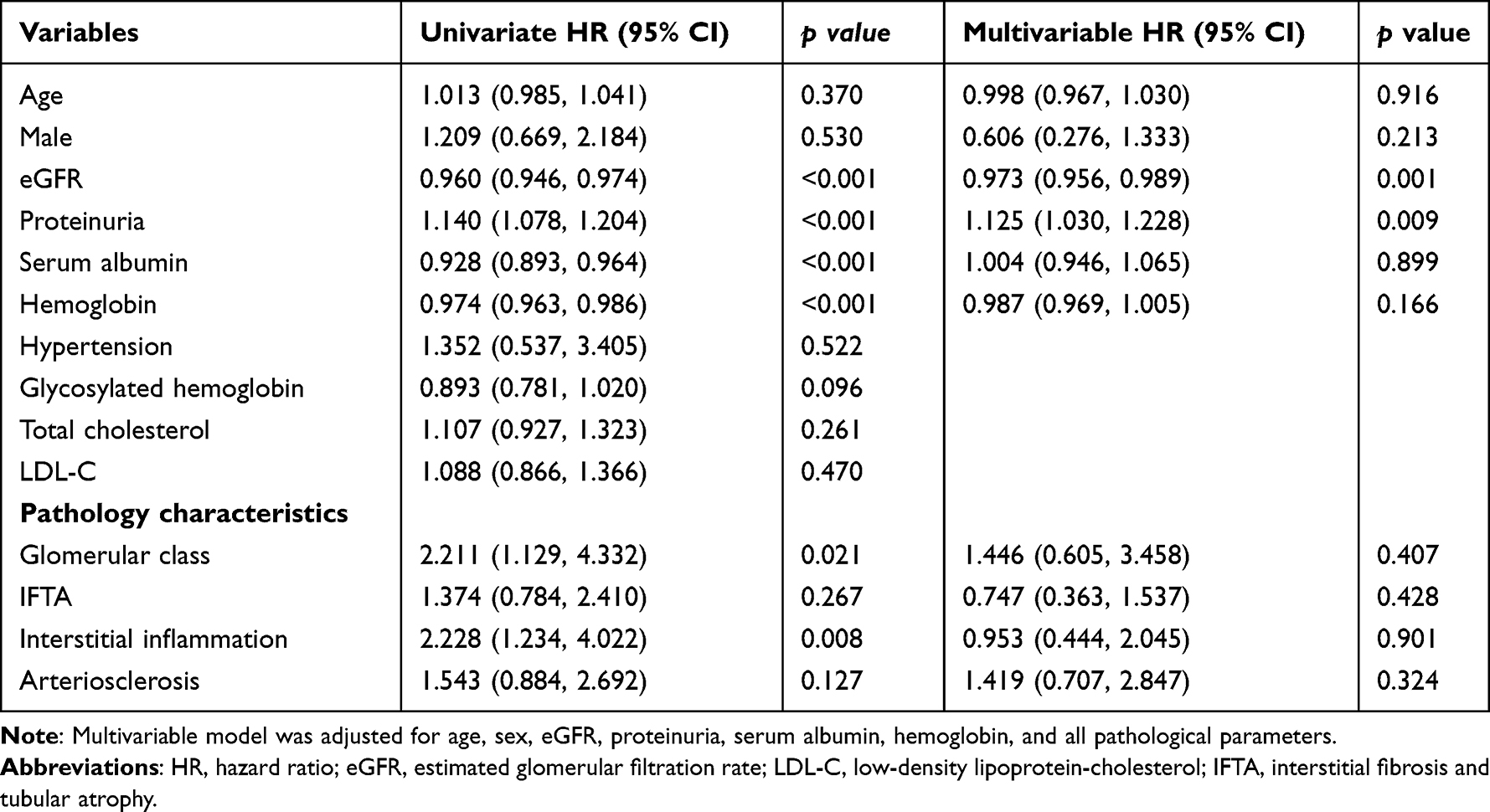 |
Table 4 Univariable and Multivariable Cox Proportional Hazard Analyses for the Prediction of ESRD in Rapid eGFR Decliners |
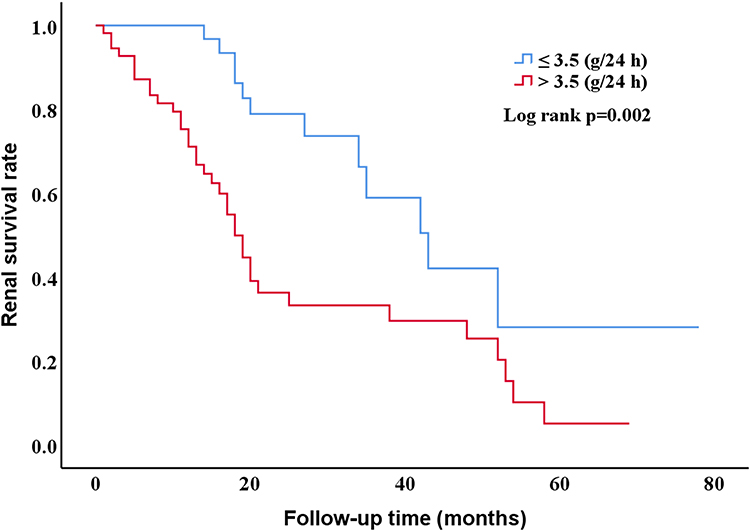 |
Figure 2 Renal survival curves for end-stage renal disease according to proteinuria subgroups. Proteinuria ≤ 3.5g/24 h (n = 35) and Proteinuria > 3.5 g/24 h (n = 61). |
Discussion
In the present study, we analyzed the clinicopathologic features and independent risk factors associated with poor renal prognosis in rapid eGFR decliners diagnosed with type 2 diabetes and biopsy-proven DKD. Rapid eGFR decliners who progressed to ESRD demonstrated poorer baseline renal function, higher proteinuria, and more severe interstitial inflammation than patients who did not progress. Baseline eGFR and proteinuria were independently associated with progression to ESRD in rapid eGFR decliners.
Although renal function deteriorates gradually in most patients with T2DM, certain patients exhibit a rapid decline in renal function. Importantly, a rapid decline in renal function is associated with a poor prognosis, and, in some cases, ESRD may be reached within months.14 Because early initiation of intensive therapy in patients at a risk of rapid renal deterioration is associated with a better outcome,15 prompt identification of rapid eGFR decliners is important. The presence and severity of proteinuria were shown to be associated with rapid renal function decline.16 A clinical model incorporating proteinuria was previously reported to exhibit the largest area under the curve, suggesting that proteinuria is the best clinical predictor of a rapid decrease in GFR.17 In our study, logistic regression analyses show that proteinuria as an independent risk factor was associated with rapid eGFR decline, which is consistent with the results of previous studies. Proteinuria is also a well-established risk factor for poor renal outcome in DKD.18 In the present study, proteinuria, especially nephrotic-range proteinuria, remains the main independent risk factor for rapid eGFR decliners reaching ESRD. According to previous studies, high proteinuria may accelerate the deterioration of renal function in patients, possibly by inducing tubular chemokine expression and complement activation.19 Hence, an effective reduction in proteinuria may help prevent progression to ESRD in Chinese patients with DKD.
GFR is a key marker for the early detection of DKD, and in a steady state, reflects the degree of established CKD. In our study, rapid eGFR decliners had a considerably higher baseline eGFR than those in Japan (58 vs 46.1 mL/min/1.73 m2).17 Approximately a quarter of rapid eGFR decliners, although still in the early stages (stages 1 and 2) of CKD, were at a high risk of rapid progression to ESRD, suggesting that timely detection and treatment are important. Notably, in our study, the mean rate of loss in rapid eGFR decliners at 17.1 mL/min/1.73 m2/year was considerably higher than the rate of loss reported in other studies.17 This was likely due to the heterogeneity of the populations studied. In addition, most patients in our hospital were referred from other hospitals or lower-level hospitals, and their condition might be much more serious.
DR has been viewed as a non-invasive predictor of DKD in patients with T2DM.13 DR was significantly associated with ESRD in patients with T2DM and biopsy-confirmed DKD.20 In our study, rapid eGFR decliners who progressed to ESRD had a higher prevalence of DR than those who did not progress (63.5% vs 45.5%). This difference, although it does not slightly reach statistical significance (P = 0.07) due to the low sample size, expresses the close correlation between the two forms of diabetic microangiopathy. Thus, screening for retinopathy may be helpful in identifying high-risk patients. The early diagnosis of DR is of great importance. The possibility of studying fondus oculi through telemedicine is certainly to be considered, especially as a screening method, and in particular, during the current COVID-19 pandemic.21,22
Notably, RAAS inhibitors reduce proteinuria and have a renal protective effect in DKD patients independent of their blood pressure-lowering effect.18,23 Although 80.2% of rapid eGFR decliners in our study received RAAS inhibitors, these medications did not seem to delay the onset of rapid GFR decline. However, the use of RAAS inhibitors in the ESRD group was slightly lower than the use of RAAS inhibitors in the non-ESRD group (73.1 vs 88.6%), which is consistent with the notion that RAAS inhibitors contribute to reducing proteinuria and improving renal outcome in rapid eGFR decliners. To the best of our knowledge, this is the first clinical study to emphasize and determine the risk factors associated with poor long-term renal prognosis in rapid eGFR decliners. Because the limited sample size may affect the final statistical analysis, we will continue to observe the characteristics of rapid eGFR decliners in future clinical work. Sodium-glucose cotransporter 2 inhibitors (SGLT2is) have recently been shown to exert a protective effect against DKD progression, reducing proteinuria24 and preventing GFR decline.25,26 A consensus report by the American Diabetes Association and the European Association for the Study of Diabetes recommended the use of SGLT2is in patients with type 2 diabetes and CKD.27 Indeed, SGLT2is are promising medications that may address many unmet needs, ultimately preventing DKD development and progression. However, because SGLT2is have only recently become widely available in China, their use was not observed in our cohort.
Regarding our histopathological findings, glomerular basement thickening, glomerular extracellular matrix accumulation, tubulointerstitial inflammation/fibrosis, and vascular lesions were the main histopathological changes in DKD. However, few studies have investigated the histopathological features of rapid eGFR decliners diagnosed with DKD. A multicenter retrospective study reported that nodular lesions and mesangiolysis were characteristic histopathological features of rapid eGFR decliners in Japan.9 Our previous biopsy-based study revealed that glomerular class was higher in rapid eGFR decliners.28 Mise et al17 also reported that rapid eGFR decliners had more severe histopathological lesions than slow eGFR decliners. In addition, significantly more rapid eGFR decliners had exudative lesions. Consistent with these previous studies, 46.9% of rapid eGFR decliners in our cohort were diagnosed with class III lesions, implying that class III may be a threshold for rapid GFR decline in DKD patients. Therefore, clinicians should pay more attention to DKD patients with severe histopathological lesions, including KW nodules, because a very rapid decline in their GFR may occur imminently.
The presence of glomerular lesions is considered to be the main factor associated with DKD progression.29,30 However, Okada et al31 provided evidence that interstitial lesions (not glomerular and vascular lesions) were significant predictors of renal prognosis in DKD patients. In our study, interstitial inflammation was an independent risk factor for progression to ESRD in slow eGFR decliners. In rapid eGFR decliners, both glomerular classification and interstitial inflammation were not associated with ESRD, although the glomerular class and interstitial inflammation score were higher in patients who progressed to ESRD than in those who did not progress. These results suggest that inflammatory mechanisms play a crucial role in the pathophysiology of Chinese patients with DKD, especially those with slow eGFR decline.
We acknowledge several limitations of our study. First, because we only analyzed DKD patients in a West China Hospital, sampling bias may be present. However, selection bias is inevitable in any biopsy-based study. This was an observational study and the sample size was relatively small. Therefore, the information on causality could not be obtained. Second, we used eGFR to assess renal function, and the conclusions might differ if measured GFR was used. Some other variables were not assessed in the present study, including history of acute kidney injury, diet, and genetic factors, which might affect DKD prognosis. Third, due to the long enrollment period, changes in treatment plan may have an impact on the prognosis of patients. Finally, the participants were followed only for a median of 2.1 years, potentially limiting the magnitude of the observed effect. Further studies with a larger sample size and longer follow-up time should be conducted to confirm our findings, and further multicenter validation in China is required.
In summary, proteinuria and eGFR were independent risk factors for renal progression in rapid eGFR decliners. Understanding the mechanisms by which proteinuria leads to renal deterioration in rapid eGFR decliners is necessary to prevent this undesirable outcome. Moreover, in order to have a positive impact on the quality of life in rapid eGFR decliners, DR should be detected as early as possible and treated together.
Data Sharing Statement
Datasets are available from the corresponding author on reasonable request.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the institutional review board at the West China Hospital of Sichuan University. The approval number was 2013R01.
Patient Consent Form
The patient has given informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Key Research and Development Project of Sichuan Science and Technology Department (19ZDYF1273), and the National Natural Science Foundation of China (81970626 and 81670662). The funding sources played no role in study design, data analysis, and manuscript writing or submission.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Martinez-Castelao A, Navarro-Gonzalez JF, Górriz J., et al. The concept and the epidemiology of diabetic nephropathy have changed in recent years. J Clin Med. 2015;4(6):1207–1216. doi:10.3390/jcm4061207
2. Alicic RZ, Rooney MT, Tuttle KR. Diabetic Kidney Disease: challenges, Progress, and Possibilities. Clin J Am SocNephrol. 2017;12:2032–2045. doi:10.2215/CJN.11491116
3. Klessens CQF, Woutman TD, Veraar KAM, et al. An autopsy study suggests that diabetic nephropathy is underdiagnosed. Kidney Int. 2016;90:1–8. doi:10.1016/j.kint.2016.01.023
4. Skupien J, Warram JH, Smiles AM, et al. The early decline in renal function in patients with type 1 diabetes and proteinuria predicts the risk of end-stage renal disease. Kidney Int. 2012;82:589–597. doi:10.1038/ki.2012.189
5. Krolewski AS. Progressive renal decline: the new paradigm of diabetic nephropathy in type 1 diabetes. Diabetes Care. 2015;38(6):954–962. doi:10.2337/dc15-0184
6. Weldegiorgis M, de Zeeuw D, Li L, et al. Longitudinal estimated GFR trajectories in patients with and without type 2 diabetes and nephropathy. Am J Kidney Dis. 2018;71:91–101. doi:10.1053/j.ajkd.2017.08.010
7. Ragot S, Saulnier PJ, Velho G, et al. Dynamic changes in renal function are associated with major cardiovascular events in patients with type 2 diabetes. Diabetes Care. 2016;39:1259–1266. doi:10.2337/dc15-2607
8. Naimark DM, Grams ME, Matsushita K, et al. Past decline versus current eGFR and subsequent mortality risk. J Am SocNephrol. 2015;27:2456–2466.
9. Furuichi K, Shimizu M, Yamanouchi M, et al. Clinicopathological features of fast eGFR decliners among patients with diabetic nephropathy. BMJ Open Diab Res Care. 2020;8:e001157. doi:10.1136/bmjdrc-2019-001157
10. Pinsker JE, Shank T, Dassau E, et al. Comment on American Diabetes Association. Approaches to glycemic treatment. Sec. 7. In Standards of Medical Care in Diabetes-2015. Diabetes Care. 2015;38(Suppl.1):e174. doi:10.2337/dc15-0839
11. Tervaert TW, Mooyaart AL, Amann K, et al. Pathologic classification of diabetic nephropathy. J AmSocNephrol. 2010;21:556–563.
12. Levey AS, Stevens LA, Schmid CH, et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–612. doi:10.7326/0003-4819-150-9-200905050-00006
13. Zhang J, Wang Y, Li L, et al. Diabetic retinopathy may predict the renal outcomes of patients with diabetic nephropathy. Ren Fail. 2018;40:243–251. doi:10.1080/0886022X.2018.1456453
14. Levey AS, Coresh J. Chronic kidney disease. Lancet. 2012;379:165–180. doi:10.1016/S0140-6736(11)60178-5
15. Krolewski AS, Skupien J, Rossing P, et al. Fast renal decline to end-stage renal disease: an unrecognized feature of nephropathy in diabetes. Kidney Int. 2017;91:1300–1311. doi:10.1016/j.kint.2016.10.046
16. Clark WF, Macnab JJ, Sontrop JM, et al. Dipstick proteinuria as a screening strategy to identify rapid renal decline. J Am SocNephrol. 2011;22:1729–1736.
17. Mise K, Hoshino J, Ueno T, et al. Clinical and pathological predictors of estimated GFR decline in patients with type 2 diabetes and overt proteinuric diabetic nephropathy. Diabetes Metab Res Rev. 2015;31:572–581. doi:10.1002/dmrr.2633
18. De Zeeuw D, Remuzzi G, Parving HH, et al. Proteinuria, a target for renoprotection in patients with type 2 diabetic nephropathy: lessons from RENAAL. Kidney Int. 2004;65(6):2309–2320. doi:10.1111/j.1523-1755.2004.00653.x
19. Abbate M, Zoja C, Remuzzi G. How Does Proteinuria Cause Progressive Renal Damage? J Am Soc Nephrol. 2006;17:2974–2984. doi:10.1681/ASN.2006040377
20. Zhao L, Ren H, Zhang J, et al. Diabetic retinopathy, classified using the lesion-aware deep learning system, predicts diabetic end-stage renal disease in Chinese patients. Endocrine Practice. 2020;26:429–443. doi:10.4158/EP-2019-0512
21. Galiero R, Pafundi PC, Nevola R, et al. The Importance of Telemedicine during COVID-19 Pandemic: a Focus on Diabetic Retinopathy. J Diabetes Res. 2020;14:9036847.
22. Sasso FC, Pafundi PC, Gelso A, et al. for screening diabetic retinopathy: the NO BLIND Italian multicenter study. Diabetes Metab Res Rev. 2019;35(3):e3113. doi:10.1002/dmrr.3113
23. Parving H, Lehnert H, Bröchner-Mortensen J, et al. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med. 2001;345(12):870–878. doi:10.1056/NEJMoa011489
24. Jardine MJ, Mahaffey KW, Perkovic V. Canagliflozin and renal outcomes in diabetic nephropathy. Reply N Engl J Med. 2019;381:1089–1090.
25. Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med. 2017;377:644–657. doi:10.1056/NEJMoa1611925
26. Heerspink HJL, Jongs N, Chertow GM, et al. Effect of dapagliflozin on the rate of decline in kidney function in patients with chronic kidney disease with and without type 2 diabetes: a prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021;9:743–754. doi:10.1016/S2213-8587(21)00242-4
27. Davies MJ, D’Alessio DA, Fradkin J, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;41:2669–2701. doi:10.2337/dci18-0033
28. Wang Y, Zhao L, Zhang J, et al. Implications of a Family History of Diabetes and Rapid eGFR Decline in Patients With Type 2 Diabetes and Biopsy-Proven Diabetic Kidney Disease. Front Endocrinol (Lausanne). 2019;10:e00855. doi:10.3389/fendo.2019.00855
29. Li L, Zhang X, Li Z, et al. Renal pathological implications in type 2 diabetes mellitus patients with renal involvement. J Diabetes Complications. 2017;31:114–121. doi:10.1016/j.jdiacomp.2016.10.024
30. Mottl AK, Gasim A, Schober FP, et al. Segmental Sclerosis and Extracapillary Hypercellularity Predict Diabetic ESRD. J Am SocNephrol. 2018;29:694–703.
31. Okada T, Nagao T, Matsumoto H, et al. Histological predictors for renal prognosis in diabetic nephropathy in diabetes mellitus type 2 patients with overt proteinuria. Nephrology. 2012;17:68–75. doi:10.1111/j.1440-1797.2011.01525.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Value of Plasma Atherogenic Index for Microalbuminuria in Newly Diagnosed Patients with Type 2 Diabetes Mellitus
Qi L, Kang N, Chen X, Li Z, Deng C, Chen S
Diabetes, Metabolic Syndrome and Obesity 2022, 15:1245-1252
Published Date: 21 April 2022
Low Circulating Free Triiodothyronine Levels are Associated with the Progression of Diabetic Nephropathy in Patients with Type 2 Diabetes
Siddiqui K, Nawaz SS, Alfadda AA, Mujammami M
International Journal of General Medicine 2022, 15:8659-8668
Published Date: 19 December 2022
Differences and Clinical Significance of Serum 25-Hydroxyvitamin D3 and Vasohibin-1 (VASH-1) Levels in Patients with Diabetic Nephropathy and Different Renal Injuries
Liu H, Wang D, Tang J, Yu L, Su S
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1085-1091
Published Date: 19 April 2023
Machine Learning-Based Predictive Modeling of Diabetic Nephropathy in Type 2 Diabetes Using Integrated Biomarkers: A Single-Center Retrospective Study
Zhu Y, Zhang Y, Yang M, Tang N, Liu L, Wu J, Yang Y
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1987-1997
Published Date: 10 May 2024