")
Back to Journals » International Journal of General Medicine » Volume 15
Low Circulating Free Triiodothyronine Levels are Associated with the Progression of Diabetic Nephropathy in Patients with Type 2 Diabetes
Authors Siddiqui K , Nawaz SS , Alfadda AA , Mujammami M
Received 20 September 2022
Accepted for publication 14 November 2022
Published 19 December 2022 Volume 2022:15 Pages 8659—8668
DOI https://doi.org/10.2147/IJGM.S389071
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Khalid Siddiqui,1 Shaik Sarfaraz Nawaz,1 Assim A Alfadda,1– 3 Muhammad Mujammami1,2,4
1Strategic Center for Diabetes Research, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2Department of Medicine, College of Medicine, and King Saud University Medical City, King Saud University, Riyadh, Saudi Arabia; 3Obesity Research Center, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 4University Diabetes Center, King Saud University Medical City, King Saud University, Riyadh, Saudi Arabia
Correspondence: Khalid Siddiqui, Strategic Center for Diabetes Research, College of Medicine, King Saud University, P.O. Box 245, Riyadh, 11411, Saudi Arabia, Tel +966 114724179 Ext.3106, Fax +966 114725682, Email [email protected]
Background: Diabetic Nephropathy (DN) is one of the most typical causes of end-stage renal disease and thyroid hormone exerts effects on the kidney. There are few reports on the role of thyroid hormone in the progression of DN. We aimed to assess the relationship between thyroid hormone and DN.
Methods: In this cross-sectional study, 400 patients with type 2 diabetes (T2D) (aged between 35 and 70 years) were divided into two groups T2D control and DN group according to albumin creatinine ratio (ACR). Clinical biochemistry parameters were measured using the Rx Daytona chemistry analyzer and thyroid hormone levels (TT4, TT3, TSH, FT4, and FT3) using the Evidence Biochip analyzer. To assess the relationship between thyroid hormone and DN, multiple logistic regression models were developed.
Results: Serum FT4 and FT3 levels were significantly lower in DN compared to T2D controls (p< 0.05). Thyroid hormone levels tend to decrease with the progression of DN. In unadjusted and adjusted logistic regression models, FT3 levels were negatively associated with odds of having DN (OR=0.28, CI=0.128– 0.616, p=0.002).
Conclusion: The free triiodothyronine level was negatively associated with the progression of DN. Further longitudinal studies are required to assess the cause of thyroid hormone differences.
Keywords: diabetic nephropathy, type 2 diabetes, thyroid hormone
Introduction
Diabetic nephropathy (DN) is one of the most typical causes of end-stage renal disease in people with type 2 diabetes worldwide.1 However, it is known that DN development is closely associated with levels of hyperglycemia. Moreover, improving glycemic control will decrease the rate of progression of DN and loss of renal function.2 Many studies have found evidence that hyperglycemia and persistent diabetes duration lead to chronic metabolic and hemodynamic changes that modulate various intracellular signaling pathways, transcription factors, cytokines, and chemokines.3,4 The growing consequences of these changes promote abnormal features such as glomerular basement membrane thickening, mesangial matrix expansion, podocyte injury, glomerular sclerosis, and tubulointerstitial fibrosis.4–6
Thyroid hormone has been reported to exert both pre-renal and direct renal effects causing renal blood flow, glomerular filtration rate, and renal tubular functions.7 Clinical effects of hypothyroidism are associated with increased serum creatinine, decreased serum cystatin C, and an increase in 24-h urine protein.7 While hyperthyroidism was associated with decreased serum creatinine, increase serum cystatin C and increased 24-h urine protein.7 Several recent studies demonstrate the interaction of thyroid hormones and renal function, and free triiodothyronine (FT3) was also associated with DN.8–10 Moreover, the metabolism of thyroid hormone is abnormal in patients with T2D and DN.8,11 Several studies have shown that thyroid hormone is associated with the risk factors of DN.12–14 According to studies, adult women have a higher prevalence of diabetic kidney disease (DKD) compared to men; sex-related disparities were prominent in women with similar DKD risk factors.15 Proteinuria was a risk factor for males, hyperglycemia was a risk factor for females, and blood pressure was a shared risk factor for both males and females.16 According to recent research, FT3 is an independent risk factor for DKD, and a low FT3 level increases the risk of DKD progression.17,18 The levels of thyroid hormones in individuals with T2D and DN are compared in the current study, and the association between thyroid hormones and DN in an adult population is examined.
Materials and Methods
Design and Subjects
This cross-sectional study is part of the Saudi Diabetes Kidney Disease (SAUDI-DKD) cohort was conducted at University Diabetes Center, King Saud University Medical City, King Saud University, and Strategic Center for Diabetes Research, College of Medicine, King Saud University, Riyadh.19 A total of 400 T2D subjects were selected from Saudi Diabetes Kidney Disease (SAUDI-DKD) cohort between April 2014 to June 2015.19 T2D Mellitus was diagnosed using the American Diabetes Association (ADA) 2013 criteria.20 All of the T2D patients had been living with the disease for more than 10 years and were older than 35. All the T2D patients were on oral hypoglycemic agents and or insulin treatment. An exclusion criterion includes current smokers, pregnant women, or the use of any thyroid medications (levothyroxine anti-thyroid drugs, glucocorticoids), type 1 diabetes, and gestational diabetes. Flow diagram showing the selection of the study participants in Figure 1. This study was approved by the Institution Review Board of the College of Medicine, King Saud University, Riyadh. The ethical guidelines for using human subjects in medical research were followed during the conduct of this investigation. All the T2D patients involved in the study signed informed consent.
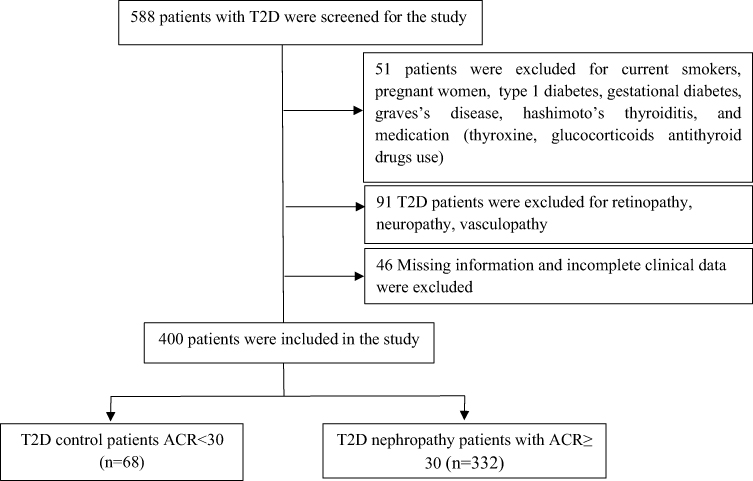 |
Figure 1 Flow diagram showing the selection of the study participants. |
DN was defined as albumin creatinine ratio (ACR) (≥30 mg/g Cr; n=332), while T2D patients with ACR (<30 mg/g Cr; n=68) are defined as control subjects without any complications such as retinopathy, neuropathy, and vasculopathy as showing in Figure 1. Furthermore, DN patients were sub-groups based on ACR (mg/g Cr). Microalbuminuria (30–300 mg/g Cr; n=142), macroalbuminuria (>300 mg/g Cr; n=70), and end-stage renal disease (n=116). eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.21
Data Collection
We collected patient data, including demographic information, previous medical history, medication of diabetes, duration of diabetes, and thyroid disease from medical records. Body mass index (BMI) was calculated as (weight in kg/height in m2), and the waist-hip ratio was calculated as (waist circumference in cm/hip circumference in cm) during the clinical visit. The blood pressure was measured in the sitting position after resting the patient for 10 min.
Biochemical Assessment
Blood samples were collected after an overnight fast of 10–12 hours. The serum was separated and stored at −20° C for analysis. The clinical biochemistry test for each patient, including alanine transaminase (ALT), aspartate transaminase (AST), total cholesterol (TC), triglyceride (TG), direct-high-density lipoprotein (HDL), Direct-low-density lipoprotein (LDL), fasting blood sugar (FBS), HbA1c, urea, and serum creatinine was performed using Randox Daytona chemistry analyzer (Randox Laboratories, United Kingdom). Urinary albumin excretion was estimated by calculating the albumin-to-creatinine ratio (ACR) in mg/g units.
Measurement of Thyroid Hormone
Thyroid hormone was measured using an Evidence Biochip analyzer (Randox Laboratories Limited, United Kingdom). Thyroid total array (TT4, TT3, and TSH) Catalog number EV3545 and Thyroid free array (FT3, FT4, and TSH) catalog number EV3546 were used for quantitative detection of multiple analytes from a single patient sample. The expected normal reference range for TSH, TT3, and TT4 assay was 0.4–4.0 uIU/mL, 0.8–1.9 ng/mL, and 5–11.5 ug/dl. Furthermore, the expected normal reference range for FT3 and FT4 assay was 2.23–5.35 pmol/l; 10.3–25.7 pmol/l from the kit. The sensitivity of TSH was determined to be 0.016 μIU/mL, 0.3 ng/mL for TT3, and 0.891 μg/dl for TT4. While the sensitivity of FT3 was determined to be 1.29 pmol/l and 1.64 pmol/l for FT4 respectively.
Statistical Analysis
All the statistical analyses were performed using SPSS version 21. For normally distributed variables, the data are expressed as mean standard deviation, and for skewed variables, as median (interquartile range). The Student’s t-test was used to compare variables between the two groups. One-way ANOVA for multiple group comparison was performed. To examine the relationship between thyroid hormone indices (TT3, TT4, TSH, FT3, and FT4) and DN we calculated the unadjusted and adjusted odds ratio (OR) and their corresponding 95% confidence interval (CI) with unadjusted and adjusted logistic regression models were developed to report the odds ration after controlling for confounders such as age, gender, and duration of diabetes. Statistical significance was set at p ≤ 0.05.
Results
The general characteristics of the study subjects are shown in Table 1. A total of 400 T2D subjects were included in this study. Among 400 T2D patients, 332 (83.0%) were diagnosed with DN. No significant difference was observed between the T2D control and DN group for gender, BMI, Hip, Waist, Waist/Hip ratio, Diastolic blood pressure, AST, total cholesterol, Direct HDL, Direct LDL, TT4, and TSH. Furthermore, DN patients were significantly older with prolonged duration of diabetes compared to T2D control patients (p≤0.05) respectively. DN patients demonstrate higher systolic blood pressure, triglycerides, urea, creatinine, fasting blood glucose, HbA1c%, and ACR compared to T2D control patients (all p≤0.05). In addition, DN patients have low eGFR, FT4, and FT3 levels (p≤0.05). Moreover, the TT4, TT3, and TSH levels remained unaltered between the T2D control and DN groups.
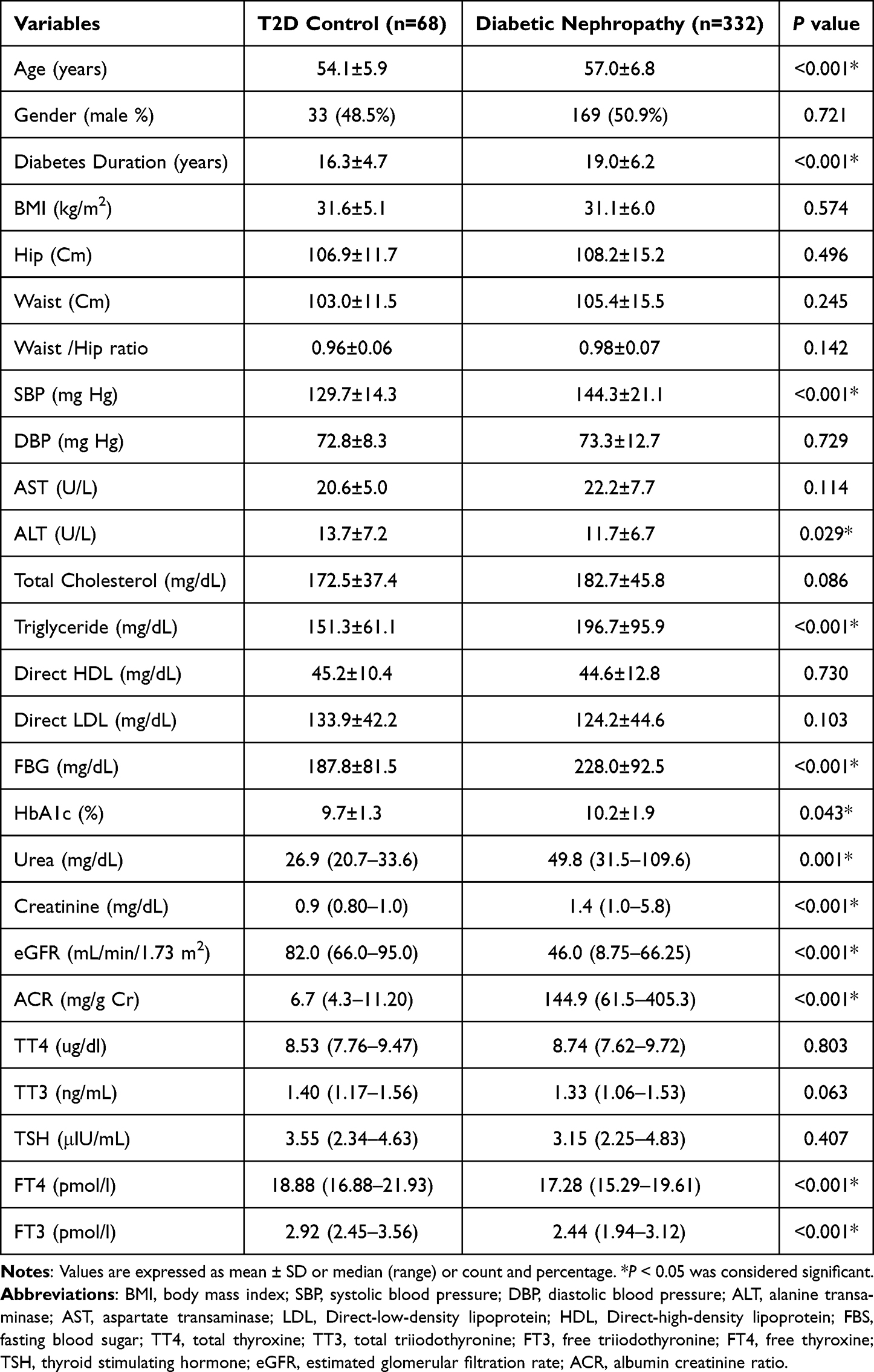 |
Table 1 Clinical Characteristics and Biochemical Assessment of Study Participants |
The clinical characteristics of male and female subjects are shown in Table 2. Among 202 male T2D patients, 169 (83.6%) were DN. No significant difference was observed between male T2D control and male DN group for BMI, Hip, Waist, Waist/Hip ratio, Diastolic blood pressure, AST, Total cholesterol, Triglyceride, Direct HDL, Direct LDL, FBS, HbA1c% TT4, TT3, and TSH. Male DN patients were older with prolonged duration of diabetes compared to the male T2D control patients (all p≤0.05) respectively. In addition, male patients with DN had significantly higher systolic blood pressure, urea creatinine, and ACR (all p≤0.05). Moreover, male patients with DN exhibit lower eGFR, FT4, and FT3 levels (p≤0.05). Among 198 female T2D patients, 169 (82.3%) were DN. No significant difference was observed between female T2D control and female DN group for BMI, Hip, Waist, Waist/Hip ratio, AST, Total cholesterol, Direct HDL, Direct LDL, HbA1c%, TT4, TT3, FT4, and TSH respectively. Furthermore, female patients with DN had significantly higher systolic blood pressure, diastolic blood pressure, triglycerides, fasting blood glucose, urea creatinine, and ACR (all p≤0.05). In addition, female patients with DN had low eGFR, and FT3 levels (p≤ 0.05) respectively.
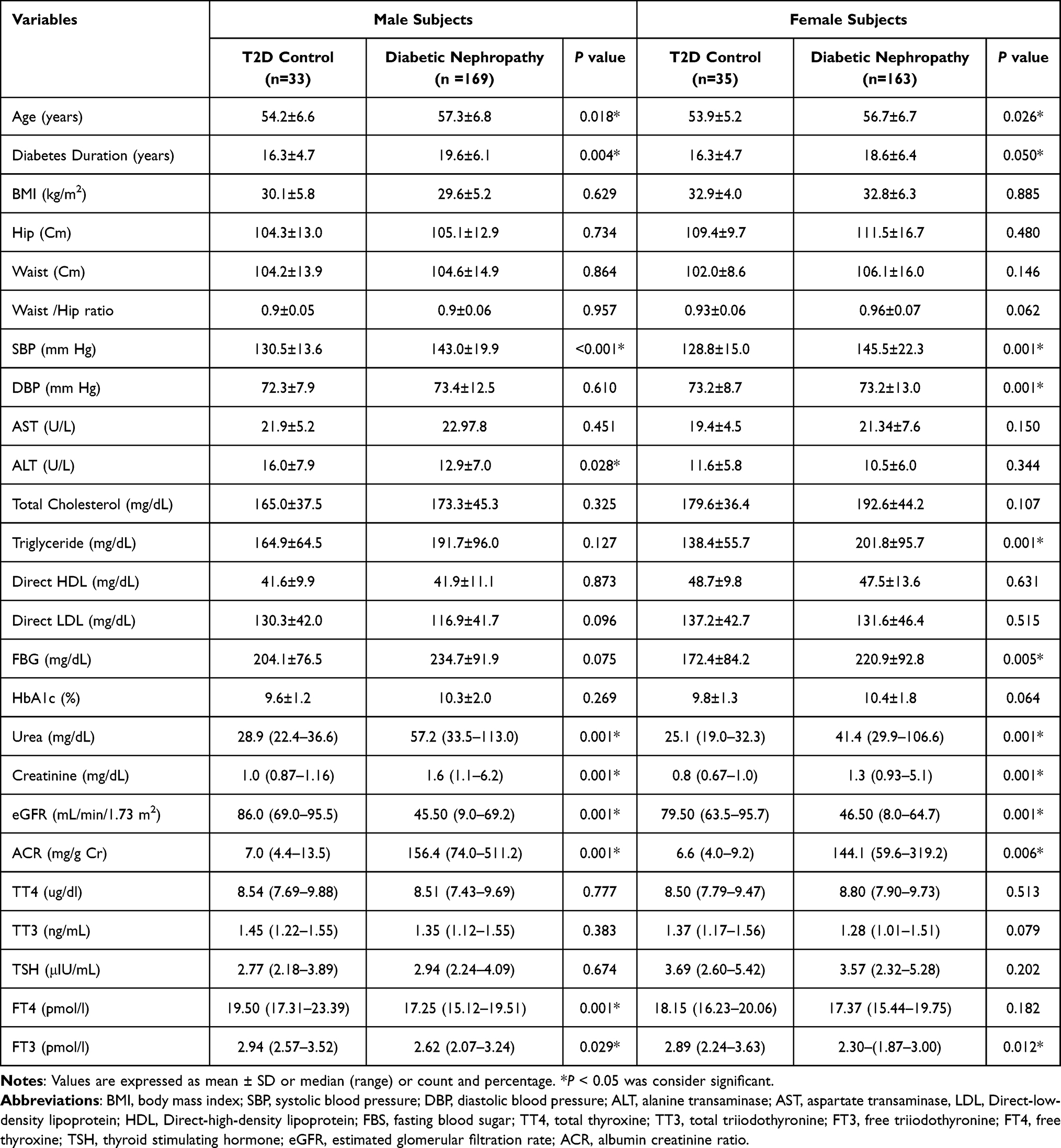 |
Table 2 Clinical Characteristics of the Study Subjects According to Gender |
Table 3 shows thyroid hormone levels TT3, TT4, TSH, FT3, and FT4 in T2D control and sub-groups of DN. No significant difference was observed in the level of TT4 among the normoalbuminuria, microalbuminuria, microalbuminuria, and end-stage renal disease group (p>0.05). Furthermore, a significant difference was observed in the level of TT3, TSH, FT3, and FT4, in normoalbuminuric, microalbuminuria, macroalbuminuria, and end-stage renal disease groups (all p≤0.05) respectively.
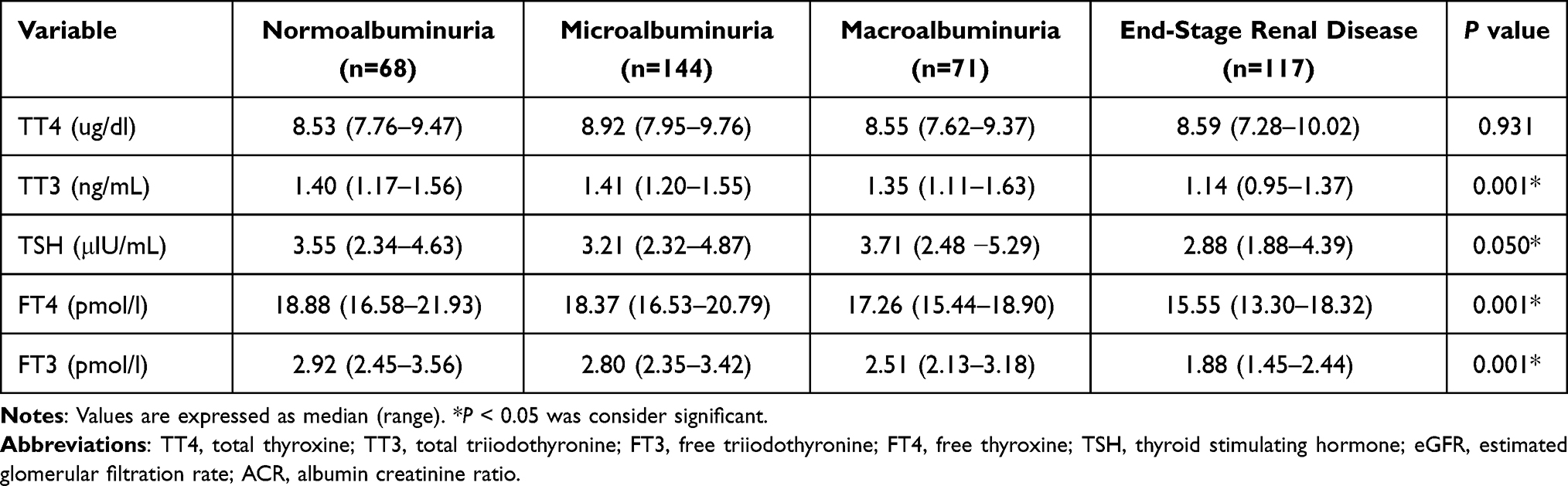 |
Table 3 Thyroid Hormone Levels in Different Groups of Diabetic Nephropathy |
Table 4 shows the relationship between thyroid hormone levels and DN in the total subject. In unadjusted and adjusted logistic regression models, elevated TT3 levels were significantly associated with higher odds of having DN. In the unadjusted model, the OR (95% CI) for DN in relation to quartiles Q2, Q3, and Q4 of TT3 hormones levels were 0.54 (0.341–0.846; p=0.007), 0.55 (0.352, 0.872; p=0.011), and 0.58 (0.368–0.922; p=0.021) respectively. After adjusting for factors such as age, gender, and diabetes duration, the OR (95% CI) for DN in relation to quartiles Q2, Q3, and Q4 of TT3 hormones levels were 0.47 (0.274–0.809; p=0.006), 0.52 (0.307–0.899; p=0.019), an 0.54 (0.316–0.925; p=0.025) respectively.
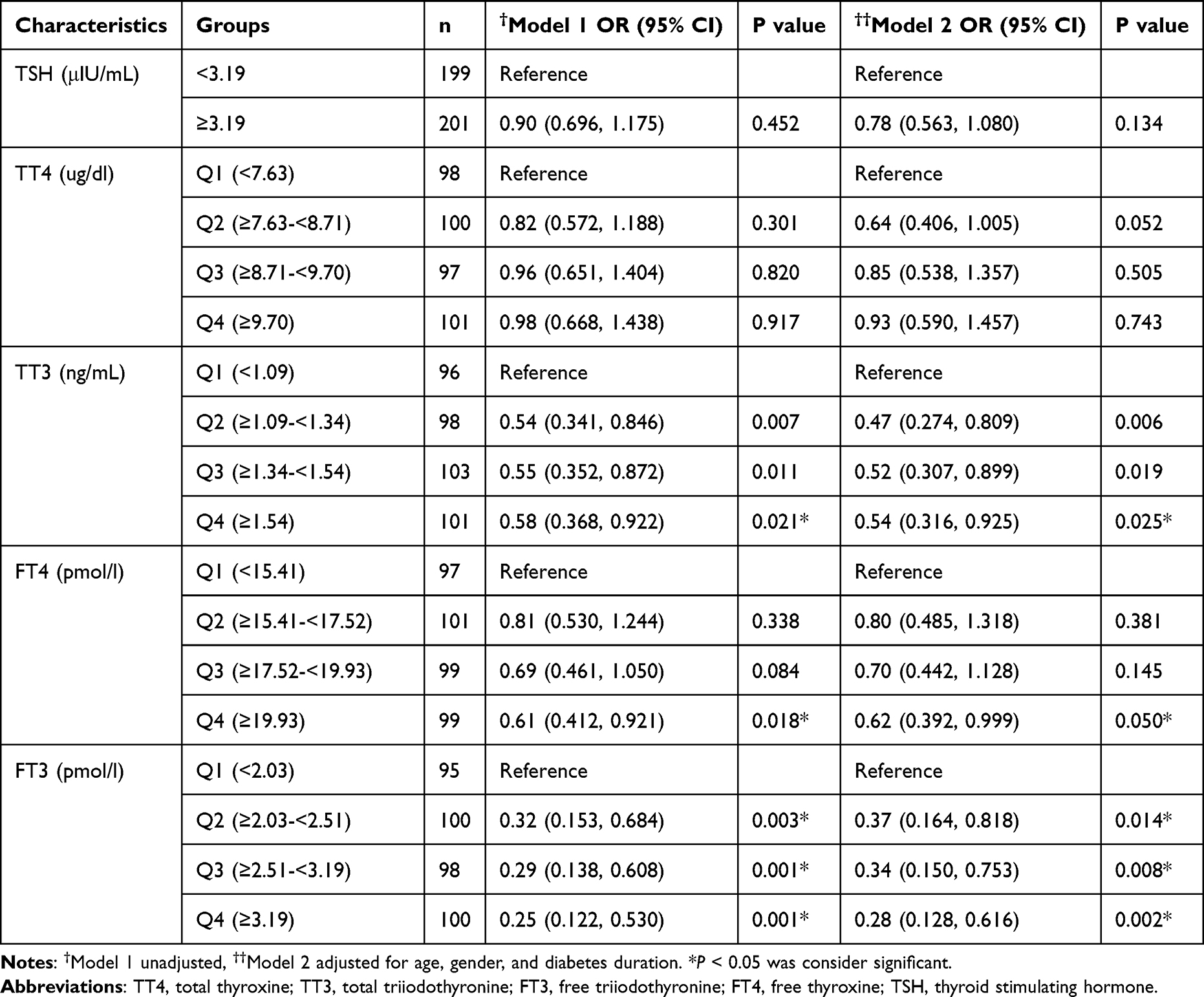 |
Table 4 Relationship Between Thyroid Hormones Levels and DN in Total Subjects |
On the other hand, FT3 levels were negatively associated with lower odds of having DN. In the unadjusted model, the OR (95% CI) for DN in relation to quartiles Q2, Q3, and Q4 of FT3 hormones levels were 0.32 (0.153–0.684; p=0.003), 0.29 (0.138–0.608; p=0.001), and 0.25 (0.122–0.530; p=0.001) respectively. After adjusting for factors such as age, gender, and diabetes duration, the OR (95% CI) for DN in relation to quartiles Q2, Q3, and Q4 of FT3 hormones levels were 0.37 (0.164–0.818; p=0.014), 0.34 (0.150–0.753; p=0.008), and 0.28 (0.128–0.616; p=0.002) respectively. However, no statistical significance was observed for TSH, TT4, and FT4 hormone levels.
Table 5 shows the relationship between thyroid hormone level and DN in gender (male) in the total subject. In unadjusted and adjusted logistic regression models, higher TSH levels were significantly associated with higher odds of having DN in males. In the unadjusted model, the OR (95% CI) for DN in males in relation to quartiles Q2 of TSH levels was 1.72 (1.159–2.558; p=0.007). After adjusting for factors such as age, gender, and diabetes duration, the OR (95% CI) was 2.09 (1.304–3.361; p=0.002) respectively.
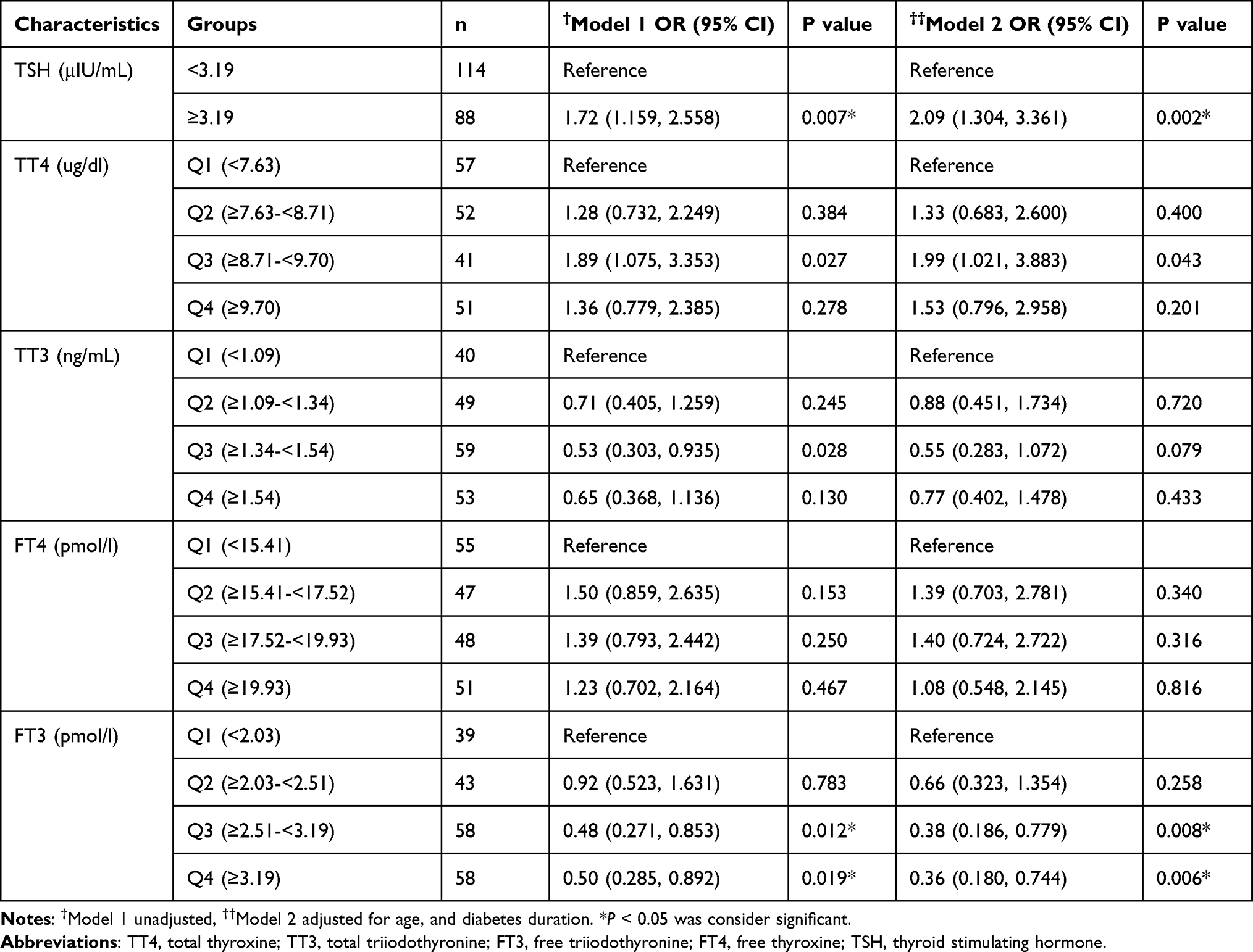 |
Table 5 Relationship Between Thyroid Hormones Levels and Gender (Male) in Total Subjects |
On the other hand, FT3 levels were negatively associated with lower odds of having DN in males. In the unadjusted model, the OR (95% CI) for DN in relation to quartiles Q2, Q3, and Q4 of FT3 hormones levels were 0.92 (0.532–1.631; p=0.789), 0.29 (0.138–0.608; p=0.001), and 0.25 (0.122–0.530; p=0.001) respectively. After adjusting for factors such as age, gender, and diabetes duration, the OR (95% CI) for DN in relation to quartiles Q2, Q3, and Q4 of FT3 hormones levels were 0.66 (0.323–1.354; p=0.258), 0.38 (0.186–0.779; p=0.008), and 0.36 (0.180–0.744; p=0.006) respectively. However, no statistical significance was observed for T4, TT3, and FT4 hormone levels.
Discussion
DN is a chronic kidney disease characterized by an increase in albumin creatinine ratio (ACR) and decreased glomerular filtration rate leading to ESKD.5,22 However, its early diagnosis, treatment, and improving glycemic control will delay the progression of the disease and loss of renal function. In the current study, we evaluated the thyroid hormone levels in patients with T2D and DN in an adult population. Our results showed that patients with DN had low FT3 and FT4 levels than T2D control patients without DN. Our results indicated that FT4 and FT3 levels significantly decreased in male DN compared to male T2D control patients. Our results also indicated that FT3 levels significantly decreased in female DN compared to female T2D control patients. This finding indicates that low levels of FT3 and FT4 thyroid hormone levels may be a potential risk factor for DN development.
In general, the findings of the current study are consistent with an earlier report from China that found that patients with DN exhibit higher TSH and low serum FT3, and FT4 levels than those without DN.11,14,23 Similar, to the above findings, other studies from China report that patients with DN demonstrate low levels of FT3 and are inversely associated with DN, while TSH and FT4 levels did not differ between DN and T2D control patients.10 The discrepancies remain unclear, the difference in the research study setting and confounding factors are the cause of conflicting results. In the current study, we evaluated the relationship of thyroid hormone to DN and provided a more detailed analysis including regression models adjusted for various potential confounders such as age, gender, and diabetes duration. We also found the consistency of the results remained unaltered with cofounders.
Furthermore, we extend these results to the male gender in more detail. Since most of the previously reported studies showed thyroid hormones level in relation to DN, none of the studies have reported gender differences in thyroid hormone levels in both T2D and DN patients.10,11,14,23 On the other hand, only one research study illustrated the relationship between thyroid hormone and T2D. Further, demonstrates that T2DM is negatively related to FT3 and positively related to FT4 in both male and female patients.24 Furthermore, after categorizing for gender serum FT3, FT4 levels are significantly lower and had a more obvious correlation with male DN patients, while FT3 levels are significantly lower in female DN patients. These findings of the current study are consistent with earlier reports, where they have shown that FT3 levels have a significant correlation with both males and females in T2D.24
Thyroid hormone action on the target cells is mediated by ligand inducible nuclear receptors/transcription factors, thyroid hormone receptor (TR) α and β, of which TRβ (TRβ1 and TRβ2) seems to be predominantly expressed in the kidney and critically important in regulating kidney function.25,26 Sex hormones (such as estrogen and testosterone) can also regulate thyroid function.27,28 Mechanistic links between thyroid and renal disease have been demonstrated in experimental animals, hypothyroidism adversely affects renal growth, and decreases structure (proximal tubule, distal tubule), and glomerular filtration, during development and adulthood.29,30 In this study, DN patients with low FT3 had higher ACR. FT3 levels linearly decreased from normoalbuminuria to ESRD the findings of the current study are consistent with previous reports in which biopsy-proven DN patients had low FT3 levels as well as severe proteinuria, renal insufficiency, and glomerular lesions.8 According to a recent study, FT3 levels decreased with the worsening of kidney disease progression. Furthermore, the levels of FT3 and FT4 were negatively correlated with serum creatinine and ACR and positively correlated with eGFR. A low FT3 level is a risk factor for DKD and its progression FT3≤4.30 pmol/L in men and ≤3.99 pmol/L in women increases the risk of DKD.17 Although, FT3 levels were inversely associated with endothelial dysfunction in hemodialysis patients.31 In our study, a strong negative association was observed between FT3 levels and DN, and these results were consistent with the previous study.18,28
The present study has several limitations. Firstly, the cross-sectional nature of the study, this is impossible to infer causality. Further cohort studies and intervention trials with gender need to be undertaken to establish a causal relationship between thyroid hormone and DN. Secondly, serum thyroid level was measured at a one-time point in this study. Thirdly, we did not include T2D patients having risk factors such as smoking, alcohol, dietary factors, and medications that might affect thyroid hormone levels. Therefore, further research is necessary to confirm the role of these risk factors.
Conclusion
The present study showed that FT3 and FT4 levels were significantly decreased in DN patients. Further, FT3 levels were negatively associated with DN. Therefore, measurement of free thyroid hormone is necessary for the early diagnosis and better management of DN in the clinical setting. Further longitudinal studies are required to assess the causes of TH differences.
Data Sharing Statement
The study data are available from the corresponding author upon reasonable request.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the College of Medicine, King Saud University.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The author would like to acknowledge the Strategic Center for Diabetes Research, which is funded by the National Plan for Science, Technology and Innovation (MAARIFAH), King Abdul-Aziz City for Science and Technology, Kingdom of Saudi Arabia. We also like to thank the University Diabetes Center, King Saud University Medical City, King Saud University for patient recruitment.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Yu SMW, Bonventre JV. Acute kidney injury and progression of diabetic kidney disease. Adv Chronic Kidney Dis. 2018;25(2):166–180. doi:10.1053/j.ackd.2017.12.005
2. Soldatos G, Cooper M. Diabetic nephropathy: important pathophysiologic mechanisms. Diabetes Res Clin Pract. 2008;82:S75–S79. doi:10.1016/j.diabres.2008.09.042
3. Nawaz SS, Joy SS, Al Farsi Y, George TP, Siddiqui K. Potential role of serum fetuin-a in relation with pro-inflammatory, chemokine and adhesion molecules in diabetic kidney disease: a case–control study. Mol Biol Rep. 2019;46(1):1239–1246. doi:10.1007/s11033-019-04592-2
4. Siddiqui K, George TP, Nawaz SS, Yaslam M, Almogbel E, Al-Rubeaan K. Significance of glycated LDL in different stages of diabetic nephropathy. Diabetes Metab Syndr. 2019;13(1):548–552. doi:10.1016/j.dsx.2018.11.023
5. Navarro-González JF, Mora-Fernández C, De Fuentes MM, García-Pérez J. Inflammatory molecules and pathways in the pathogenesis of diabetic nephropathy. Nat Rev Nephrol. 2011;7(6):327–340. doi:10.1038/nrneph.2011.51
6. Wada J, Makino H. Inflammation and the pathogenesis of diabetic nephropathy. Clin Sci. 2013;124(3):139–152. doi:10.1042/CS20120198
7. Basu G, Mohapatra A. Interactions between thyroid disorders and kidney disease. Indian J Endocrinol Metab. 2012;16(2):204–213. doi:10.4103/2230-8210.93737
8. Han Q, Zhang J, Wang Y, et al. Thyroid hormones and diabetic nephropathy: an essential relationship to recognize. Nephrology. 2019;24(2):160–169. doi:10.1111/nep.13388
9. Schultheiss UT, Daya N, Grams ME, et al. Thyroid function, reduced kidney function and incident chronic kidney disease in a community-based population: the atherosclerosis risk in communities study. Nephrol Dial Transplant. 2017;32(11):1874–1881. doi:10.1093/ndt/gfw301
10. Wu J, Li X, Tao Y, Wang Y, Peng Y. Free triiodothyronine levels are associated with diabetic nephropathy in euthyroid patients with type 2 diabetes. Int J Endocrinol. 2015;204893. doi:10.1155/2015/204893
11. Wang J, Li H, Tan M, et al. Association between thyroid function and diabetic nephropathy in euthyroid subjects with type 2 diabetes mellitus: a cross-sectional study in China. Oncotarget. 2019;10(2):88–97. doi:10.18632/oncotarget.26265
12. Asvold BO, Bjøro T, Vatten LJ. Associations of TSH levels within the reference range with future blood pressure and lipid concentrations: 11-year follow-up of the HUNT study. Eur J Endocrinol. 2013;169(1):73–82. doi:10.1530/EJE-13-0087
13. Wang J, Zheng X, Sun M, et al. Low serum free thyroxine concentrations associate with increased arterial stiffness in euthyroid subjects: a population-based cross-sectional study. Endocrine. 2015;50(2):465–473. doi:10.1007/s12020-015-0602-1
14. Zhao W, Li X, Liu X, Lu L, Gao Z. Thyroid function in patients with type 2 diabetes mellitus and diabetic nephropathy: a single center study. J Thyroid Res. 2018;9507028. doi:10.1155/2018/9507028
15. Margaret KY, Lyles CR, Bent-Shaw LA, Young BA. Risk factor, age and sex differences in chronic kidney disease prevalence in a diabetic cohort: the pathways study. Am J Nephrol. 2012;36(3):245–251. doi:10.1159/000342210
16. Chang P-Y, Chien L-N, Lin Y-F, Wu M-S, Chiu W-T, Chiou H-Y. Risk factors of gender for renal progression in patients with early chronic kidney disease. Medicine. 2016;95(30):e4203. doi:10.1097/MD.0000000000004203
17. Yang Z, Duan P, Li W, et al. The correlation between thyroid hormone levels and the kidney disease progression risk in patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2022;15:59–67. doi:10.2147/DMSO.S347862
18. Li Y, Yi M, Deng X, Li W, Chen Y, Zhang X. Evaluation of the thyroid characteristics and correlated factors in hospitalized patients with newly diagnosed type 2 diabetes. Diabetes Metab Syndr Obes. 2022;15:873–884. doi:10.2147/DMSO.S355727
19. Al-Rubeaan K, Siddiqui K, Al-Ghonaim MA, Youssef AM, AlNaqeeb D. The Saudi Diabetic Kidney Disease study (Saudi-DKD): clinical characteristics and biochemical parameters. Ann Saudi Med. 2018;38(1):46–56. doi:10.5144/0256-4947.2018.03.01.1010
20. Association AD. Standards of medical care in diabetes—2013. Diabetes Care. 2013;36(Supplement1):S11–S66. doi:10.2337/dc13-S011
21. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
22. Al-Rubeaan K, Nawaz SS, Youssef AM, Al Ghonaim M, Siddiqui K. IL-18, VCAM-1 and P-selectin as early biomarkers in normoalbuminuric type 2 diabetes patients. Biomark Med. 2019;13(6):467–478. doi:10.2217/bmm-2018-0359
23. Fei X, Xing M, Wo M, Wang H, Yuan W, Huang Q. Thyroid stimulating hormone and free triiodothyronine are valuable predictors for diabetic nephropathy in patient with type 2 diabetes mellitus. Ann Transl Med. 2018;6(15):305. doi:10.21037/atm.2018.07.07
24. Gu Y, Li H, Bao X, et al. The relationship between thyroid function and the prevalence of type 2 diabetes mellitus in euthyroid subjects. J Clin Endocrinol Metab. 2017;102(2):434–442. doi:10.1210/jc.2016-2965
25. Cheng S-Y, Leonard JL, Davis PJ. Molecular aspects of thyroid hormone actions. Endocr Rev. 2010;31(2):139–170. doi:10.1210/er.2009-0007
26. Kim H-Y, Mohan S. Role and mechanisms of actions of thyroid hormone on the skeletal development. Bone Res. 2013;1(1):146–161. doi:10.4248/BR201302004
27. Boucai L, Hollowell JG, Surks MI. Thyroid dysfunction: hypothyroidism, thyrotoxicosis, and thyroid function tests: an approach for development of age-, gender-, and ethnicity-specific thyrotropin reference limits. Thyroid. 2011;21(1):5–11. doi:10.1089/thy.2010.0092
28. Zou J, Tian F, Zhang Y, et al. Association between thyroid hormone levels and diabetic kidney disease in euthyroid patients with type 2 diabetes. Sci Rep. 2018;8(1):4728. doi:10.1038/s41598-018-22904-7
29. Mariani LH, Berns JS. The renal manifestations of thyroid disease. J Am Soc Nephrol. 2012;23(1):22–26. doi:10.1681/ASN.2010070766
30. Natesan V, Kim SJ. Lipid metabolism, disorders and therapeutic drugs - review. Biomol Ther. 2021;29(6):596–604. doi:10.4062/biomolther.2021.122
31. Tatar E, Kircelli F, Asci G, et al. Associations of triiodothyronine levels with carotid atherosclerosis and arterial stiffness in hemodialysis patients. Clin J Am Soc Nephrol. 2011;6(9):2240–2246. doi:10.2215/CJN.02540311
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.