Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
Clinical and Economic Burden Following Percutaneous Coronary Intervention for STEMI: A US Real-World Evidence Study
Authors Krishnaswami S ![]() , Clark B
, Clark B ![]() , Tyagi M, Sinha M, Donato BMK
, Tyagi M, Sinha M, Donato BMK ![]() , Wittrup-Jensen V, Cao Z
, Wittrup-Jensen V, Cao Z ![]()
Received 28 February 2026
Accepted for publication 11 June 2026
Published 25 June 2026 Volume 2026:18 605902
DOI https://doi.org/10.2147/CEOR.S605902
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Shanthi Krishnaswami,1 Brendan Clark,2 Manu Tyagi,1 Meenal Sinha,1 Bonnie MK Donato,2 Villum Wittrup-Jensen,3 Zhun Cao1
1Premier Applied Sciences, Premier Inc, Charlotte, NC, USA; 2Boehringer Ingelheim Pharmaceuticals, Inc., Ridgefield, CT, USA; 3Boehringer Ingelheim Intl. GmbH, Ingelheim Am Rhein, Germany
Correspondence: Shanthi Krishnaswami, Premier Applied Sciences, Premier Inc, Charlotte, NC, USA, Email [email protected]
Introduction: ST-segment-elevation myocardial infarction (STEMI) affects approximately 250,000 people in the U.S. annually, causing substantial morbidity and mortality. One-year outcomes following percutaneous coronary intervention (PCI) for STEMI vary across studies.
Aim: To assess clinical and economic outcomes following PCI among patients with STEMI.
Methods: This study analyzed adult patients with STEMI undergoing PCI between 2016 and 2021, using Premier Healthcare Database and additional mortality and claims data. Clinical outcomes, healthcare resource use, and costs following first PCI discharge (index visit) were assessed for at least 1 year, with outcomes at 3-year follow-up assessed among a subset of patients. Multivariable regression (Cox, logistic or generalized linear) was used to identify risk factors for key outcomes.
Results: A total of 180,691 patients underwent PCI for STEMI in 633 US hospitals during the study period. The median age was 62 years, most were male (71%), non-Hispanic White (62.7%), and had Medicare as the primary payor (42.9%). At index visit, 13.8% had ventricular tachycardia, 8.8% had ventricular fibrillation, with a median cost of $17,582, and a mortality rate of 5.5%. Within 1 year, there were 1,966 (1.1%) additional deaths, 17.4% were readmitted, 13.4% developed heart failure (HF), 2.5% were hospitalized primarily for HF (HHF), 3.9% had atrial fibrillation, and 1% experienced recurrent STEMI. The median total study cost by 1 year was $21,010. A Charlson Comorbidity Index (CCI) score of ≥ 4 (vs < 4) at index visit was most strongly associated with higher risk of death at 1 year: hazard ratio: 4.1, (95% CI: 3.66 to 4.49), higher odds of readmissions (OR: 2.6, 95% CI: 2.50 to 2.70), HHF (OR: 4.1 (95% CI: 3.83 to 4.42)), and 74% higher costs (p< 0.05). Similar associations were observed at 3-year follow-up (n=59,714).
Conclusion: This study identified risk factors associated with one-year negative clinical outcomes and increased cost following PCI for the treatment of STEMI.
Keywords: heart attack, reperfusion procedure, risk factors, mortality, cost
Introduction
Coronary heart disease (CHD) is the leading cause of death in the United States (US), with 382,820 deaths in 2020.1 From 2005 to 2014, the estimated annual incidence of myocardial infarction in the US was 605,000 new events and 200,000 recurrent events. The estimated direct and indirect cost of heart disease in 2018 to 2019 (average annual) was $239.9 billion in the US.2 ST-segment-elevation myocardial infarction (STEMI), a presentation of acute coronary artery disease, is estimated to affect about 250,000 Americans each year, leading to a significant burden of mortality and morbidity.2
Rapid diagnosis and treatment are critical for patients with STEMI to reduce the risk of mortality and morbidity. Timely reperfusion with thrombolytics and/or percutaneous coronary intervention (PCI) are recommended for these patients to minimize myocardial damage.3 More than 600,000 PCIs are performed in the US each year, and the cost associated with these procedures alone is estimated at around $10 billion.4 Treating STEMI with PCI aims to reduce the risk of cardiovascular death and hospitalization for heart failure (HF), but post-STEMI care optimization remains crucial. Assessing clinical and economic outcomes and identifying risk factors associated with negative outcomes is the first step in developing care pathways for patients with STEMI following PCI procedures. Also, PCI success depends on patient-specific factors, lesion complexity, and repeat interventions. Existing studies on PCI outcomes mainly focus on outcomes within PCI hospitalizations, or within the 30-day or 90-day follow-up periods,5–9 while contemporary, real-world data on 1-year effects of PCI in large hospital-based STEMI patient groups is still limited. It is important to understand the full impact of PCI on economic and clinical burdens for both patients and healthcare systems. The aim of this study is to update the current STEMI-PCI-related literature by evaluating detailed clinical outcomes, costs, and healthcare resource utilization (HCRU) in patients undergoing PCI for STEMI and to explore the risk factors for 1-year outcomes using hospital-based real-world data in the US.
Materials and Methods
Study Design
A retrospective observational study was conducted using the Premier Healthcare Database (PHD), a large, geographically diverse, US hospital database that includes 25% of inpatient discharges. Hospitals in the database represent the 4 geographic US regions and more than 1.3 billion patient encounters. Patient-related data are collected from all payers and therapeutic areas.10 Data were supplemented with closed claims and general mortality data from proprietary third-party vendors linked with tokens (Supplementary Exhibit 1). The General Mortality database (GMDB) was used to follow patients’ death events after the PCI procedure through 3 years after index discharge. Data from GMDB provided mortality information from external sources covering newspapers, government mortality data, private media, private claims, and funeral homes. The closed claims database was used to identify additional visits in all treatment settings for those who could be linked to the PHD database, and outcomes were assessed at follow-up timepoints.
This study included adult patients (aged ≥18 years) who underwent PCI for a primary diagnosis (the chief reason for hospital encounter) of STEMI (ICD-10-CM diagnosis codes: I21.01, I21.02, I21.09, I21.11, I21.19, I21.21, I21.29, I21.3), and were discharged from US hospitals between 1 October 2016 and 31 December 2021. Patients who had elective admission type were excluded from the study. The evidence of treatment with PCI during the same visit was identified using ICD-10 procedure codes, CPT codes, or HCPCS codes (Supplementary Table S1).
The entire study period was 1 October 2015 to 31 December 2022, ensuring a 12-month baseline period and a minimum of 12 months for follow-up for each patient. Outcomes at 3-year follow-up were assessed among a subset of patients who had their first PCI for STEMI on or before December 31, 2019.
Study Variables
The primary outcomes were mortality and incidence of clinical events (including HF or cardiac arrythmias) following PCI for STEMI, identified by ICD-10 diagnosis codes. Secondary outcomes included recurrent STEMI events, repeat PCIs, HCRU (eg., readmissions, outpatient visits, length of hospital and intensive care unit [ICU] stays for inpatient encounters only), and all-cause total costs. The outcomes among patients alive at index discharge were assessed at various time points including during index visit, and within 30 days, 90 days, and 1 year following index discharge. Outcomes at 3-year follow-up were assessed among a subset of patients (n=59,714 alive patients at index discharge) who had their first PCI for STEMI on or before December 31, 2019. Diagnosis and procedure codes to identify patients with outcomes are provided in Supplementary Table S1.
Patient Demographics, Hospital, Visit, and Clinical Characteristics
We examined patients’ demographics (age, sex, self-reported race, ethnicity), primary insurance payor, hospital characteristics (populations served [rural or urban], teaching status, US census geographical regions, and number of beds), and visit characteristics (admission type and discharge disposition) for the index visit. Charlson-Deyo Comorbidity Index (CCI)11 was used to assess comorbidities for the index and within 365 days prior to index visit, and the most frequent comorbidities at index visit were also assessed. CCI is a validated tool that quantifies a patient’s overall disease burden by assigning weighted scores to specific comorbid conditions, with higher scores indicating greater mortality risk. The CCI score is calculated by assigning predefined weights to each of 17 comorbid conditions based on their associated mortality risk, then summing these weights to produce a total score. Higher total scores indicate greater comorbidity burden and a worse prognosis. The CCI score was categorized as 0, 1–3, 4 + conditions to indicate the comorbidity status of the patient. We also evaluated all patient-refined diagnoses related groups (APR-DRG) severity of illness,12,13 COVID-19 diagnosis, infarct location, and number of diseased vessels involved. APR-DRG severity of illness measure categorizes inpatients into four levels reflecting clinical complexity and physiological compromise, informing outcomes assessment, and resource use. This measure evaluates the burden of illness and the difficulty of treatment. To determine multivessel involvement, we utilized CPT modifiers to identify each specific vessel involved and then aggregated these data to obtain the total number of vessels affected. Medications at index visit were identified via generic and/or brand name, indicating any use of the medication of interest, namely beta blockers, calcium channel blockers, angiotensin-converting enzyme inhibitors, antiplatelets, anticoagulants, statins, or sodium glucose co-transporter-2 inhibitors. We used Social Vulnerability Index (SVI)14 to assess the social vulnerability status of patients undergoing PCI. The SVI was calculated using county-level data, including 15 US census variables and the county of the patient’s residence. The SVI indicates the relative vulnerability of every US county, and 15 social factors are grouped into 4 major themes and an overall rank/score. Higher overall scores indicate higher vulnerability. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.15
Statistical Analysis
Descriptive analyses for continuous variables and categorical variables were performed and expressed as mean (standard deviation, SD) or median (interquartile range, IQR) for continuous data and counts and percentages for categorical data. For continuous outcomes such as length of stay (LOS) and costs, outliers that were higher than the value of the 99th percentile were replaced by the value of the 99th percentile and outliers lower than 1st percentile were replaced by the value of the 1st percentile to improve the stability and robustness of statistical estimates and reflect the typical utilization of healthcare resources. For the mortality related analysis, patients with a recorded death date in GMDB were considered deceased; those without such a record were censored. Time to death was measured from index discharge to the recorded death date. For censored cases, fixed duration of 365.25 days (1-year analysis) and 1,096 days (3-year analysis) were assigned. Kaplan-Meier curves were generated to visualize survival probabilities (unadjusted) over time across risk groups and survival distributions statistically compared by Log rank test (Figure S1 and Figure S2).
Multivariable regression analyses were performed to assess risk factors for mortality, incidence of HF, readmissions, and study cost within 1 year and 3 years following index discharge using PHD data. We used Cox proportional hazard regression method to identify risk factors associated with time to death, generalized linear regression models with gamma distribution, log link function for cost outcomes, and logistic regression analysis to identify factors associated with dichotomous outcomes (HF, readmissions). Covariates in the regressions were selected based on descriptive results and clinical experts’ opinion and included age, sex, race-ethnicity, insurance, hospital characteristics (size, region, type, and setting [rural/urban]), comorbidity, SVI, and multivessel involvement at index visit. Multicollinearity between covariates were tested using variance inflation factors. The adjusted mean cost was computed based on the model predictors. For multivariable analysis, odds/ hazard ratios or percent difference in outcomes (cost outcomes) were estimated along with 95% confidence interval (CI), and p values. A 2-sided p<0.05 was considered statistically significant. Patients with missing values for covariates were removed from risk factor analysis, and we did not conduct additional analysis on missing values, as the proportion of patients with missing values was ≤1.7%. Using PHD linked claims data, outcomes were assessed at different follow-up timepoints descriptively.
Results
A total of 295,848 patients aged 18 years or older with a primary diagnosis of STEMI between 1 October 2016 and 31 December 2021 were identified (Figure 1). About 2.5% of patients with elective admissions were excluded. A total of 180,691 patients (inpatient: 179,086, outpatient: 1,605) underwent PCI for STEMI at 633 hospitals and met study selection criteria. Overall, 93,083 patients (51.5%) presented with anterior wall STEMI, 87,608 patients (48.5%) presented with non-anterior wall STEMI, and 25,987 patients (14.4%) had multi-vessel (coronary artery) disease (MVD). There were 63,469 (35.1%) patients who had their first PCI between October 2016 and December 2019 and were analyzed for 3-year follow-up assessment. Overall, 11.3% of patients (n=20,391) were linked with closed claims data.
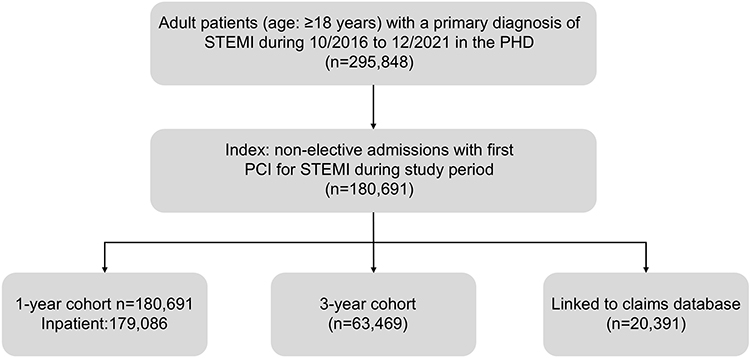 |
Figure 1 Study Analytical Sample Derivation (flow diagram). |
Patient and Hospital Characteristics
The mean (SD) age of eligible patients was 62.1 (±11.7) years. Patients aged 50–64 years accounted for 42.3% of the total sample. Among all patients, 71% were male, 62.7% were non-Hispanic White, 6.9% were non-Hispanic Black, 42.9% had Medicare, and 34.2% had commercial insurance. More than one-third of patient index visits (36.8%) were at hospitals with 500 or more beds, almost half were hospitals in the South region, 52.4% were teaching hospitals, and 89% were urban hospitals. Overall, 29,560 patients (16.4%) resided in the highest vulnerable counties (SVI quintile 5) needing some type of social assistance (Table 1).
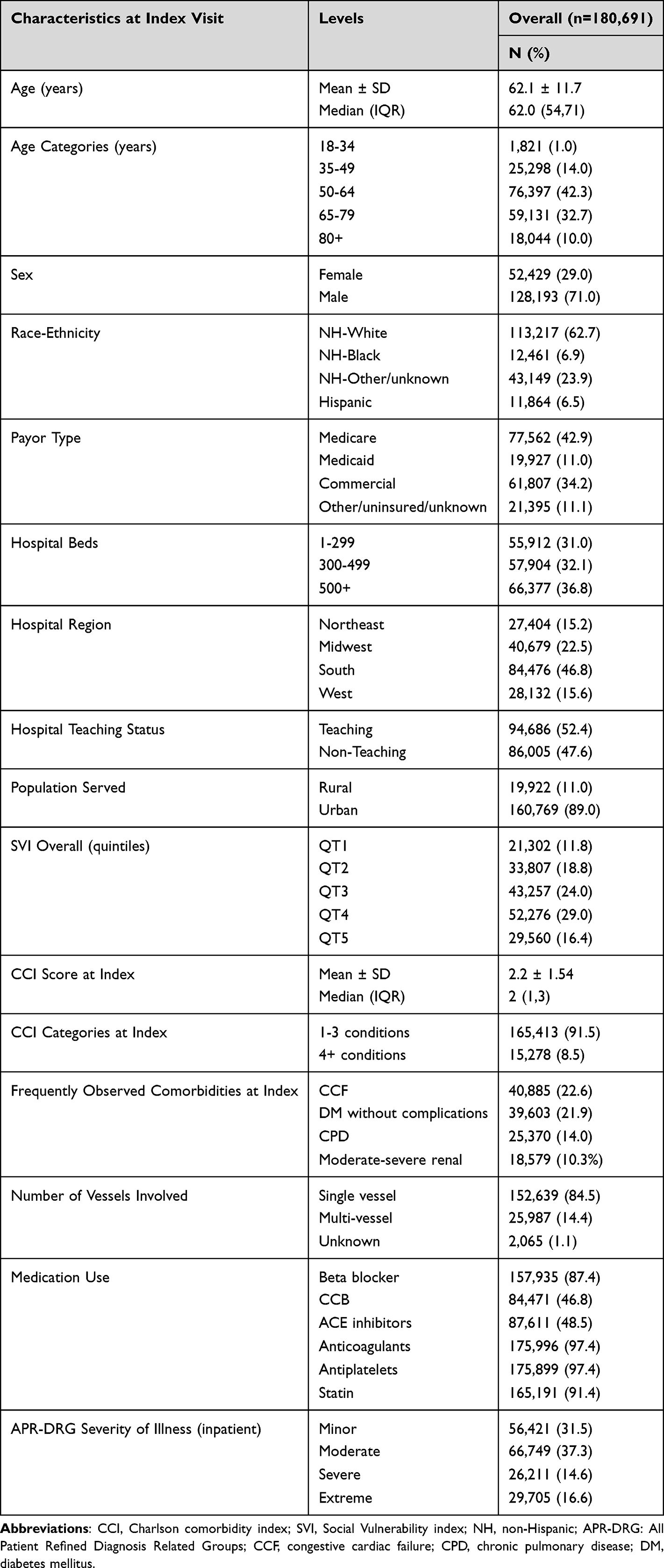 |
Table 1 Baseline Characteristics of the Study Population That Underwent PCI for STEMI |
Clinical Characteristics
Overall, the mean (SD) CCI score at index visit was 2.2 ± 1.54. Most patients (91.5%) had CCI scores between 1 and 3, and 8.5% had scores ≥4 during index visit. The most frequent comorbidities at index visit, other than myocardial infarction, included HF (22.6%), diabetes without chronic complications (21.9%), chronic pulmonary disease (14.0%), and moderate-severe renal disease (10.3%). Among inpatients, the APR-DRG measure was frequently rated as moderate for the severity of illness (37.3%). More than 85% of patients were prescribed anticoagulants, antiplatelets, statins, and beta blockers at index (Table 1).
Primary Outcomes
Death: The cumulative all-cause mortality rate was 5.5% at index visit, 5.9% at 30 days, 6.1% at 90 days, and 6.6% at 1 year following PCI (Table 2). Cardiac Arrythmias: At index visit, the most common arrythmias observed were ventricular tachycardia (13.8%), ventricular fibrillation (8.8%), atrial fibrillation (6.7%), and supraventricular tachycardia (2.1%). In the year following index discharge, a higher proportion of patients had atrial fibrillation (3.9%) vs other arrhythmias at <2%. Heart Failure: Fewer patients (2.5%) had a primary diagnosis of HF during hospitalization (HHF) at 1-year follow-up, while the cumulative incidence of new HF diagnosis (primary or secondary) at 1 year following index discharge was 13.4%.
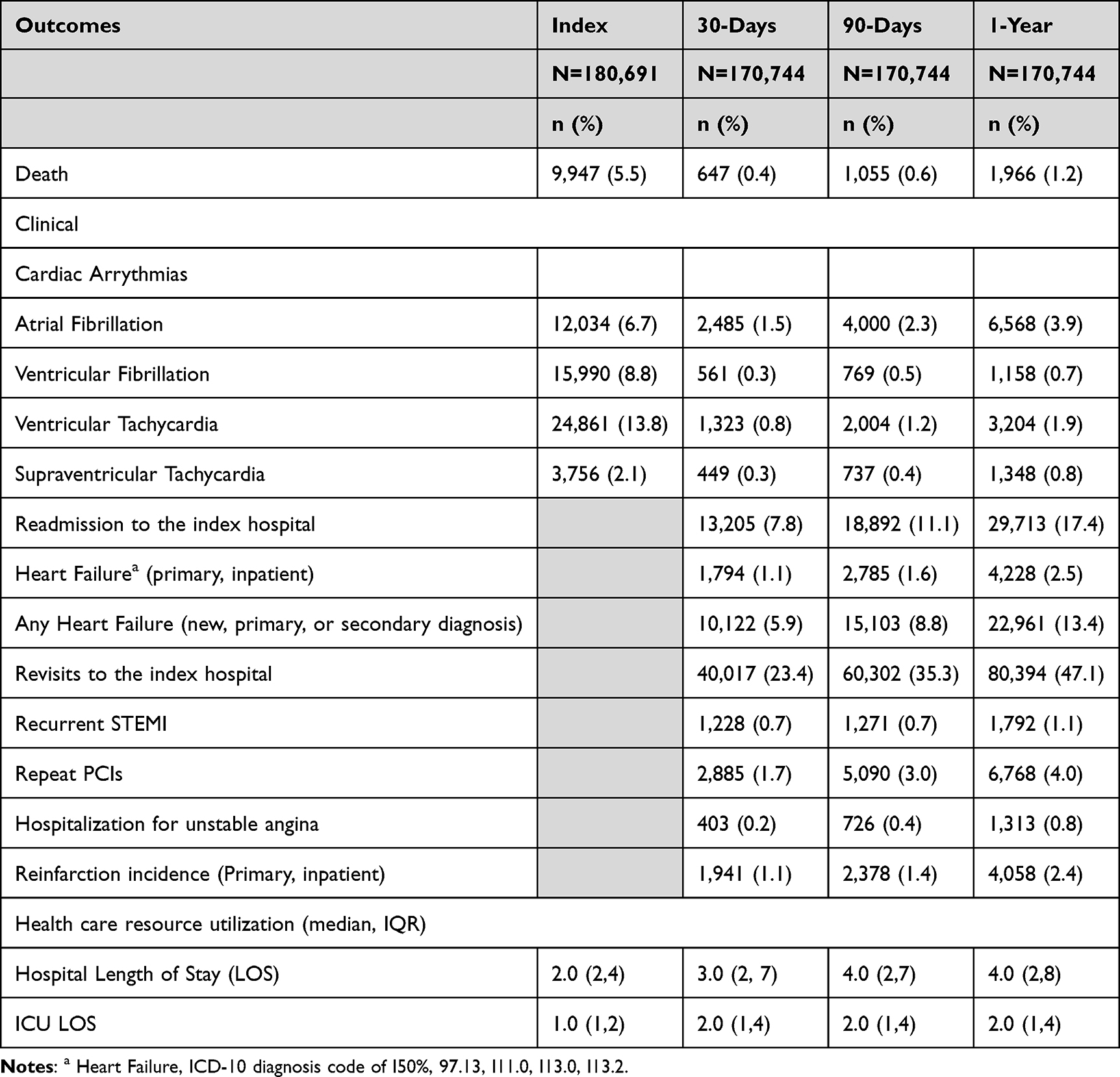 |
Table 2 Outcomes Following PCI for STEMI at Index and Within 1 Year Following Index Discharge |
Secondary Outcomes
Among all patients alive at index discharge, the cumulative all-cause readmission rate was 7.8% at 30 days, 11.1% at 90 days, and 17.4% at 1 year, while the cumulative hospital-based outpatient all-cause revisit rate was 23.4% at 30 days, 35.3% at 90 days, and 47.1% at 1 year. The reinfarction rate (non-STEMI or STEMI) ranged from 1.1% at 30 days to 2.4% at 1 year following index discharge, while the rate of recurrent STEMI events or hospitalization for unstable angina were ≤1% across the follow-up period. There were 6,768 repeat PCIs (4.0%) in the year following index discharge. The top 20 primary reasons for readmissions within 1 year following index discharge appear in Supplementary Table S2, with cardiac conditions listed frequently as reasons for readmits.
Healthcare Utilization
Overall, median hospital LOS was 2 days (Q1-Q3: 2–4) at index visit for all inpatients, 3 days (Q1-Q3: 2–7) at 30 days, 4 days (Q1-Q3: 2–8) at 90 days and 1 year following index discharge (Table 2). The median ICU LOS was 1 day (Q1-Q3: 1–2) at index visit and 2 days (Q1-Q3: 1–4) at 90 days and 1 year after index discharge.
Cost Outcomes
Adjusted to 2022 US dollars, the median index inpatient cost was $17,582 (Q1:Q3: $12,985- $26,288), the median index outpatient cost was $11,712 (Q1-Q3: $8,514- $16,861), with a total median index cost of $17,528 ($12,939-$26,203) (Figure 2). The median total all-cause study cost for all patients up to 1 year was $21,010 (Q1-Q3: $14,535- $34,604).
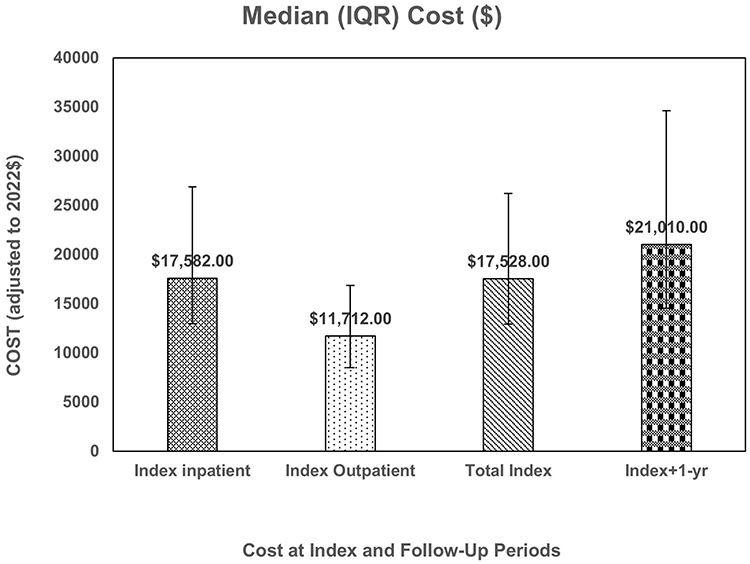 |
Figure 2 Distribution of Cost Among Patients with PCI for STEMI. |
Risk Factors Associated with All-Cause Mortality, Readmission, and Heart Failure
The Cox regression model results for assessing the risk of all-cause mortality censored at 1 year of index discharge indicate that NH-Black (HR: 1.3, 95% CI: 1.14–1.56), Medicare (HR: 2.5, 95% CI: 2.07–2.99), Medicaid (HR: 2.1, 95% CI: 1.74–2.53), those with the highest SVI (HR: 1.3, 95% CI: 1.04–1.52), CCI ≥4 (HR: 4.1, 95% CI: 3.66–4.49) and MVD (HR: 1.2, 95% CI: 1.06–1.35) compared to those who were NH-White, had commercial insurance, lowest SVI, CCI between 1–3, and single-vessel involvement respectively had significantly higher risk of mortality within 1 year of index PCI discharge, independent of other covariates in the model (Table 3).
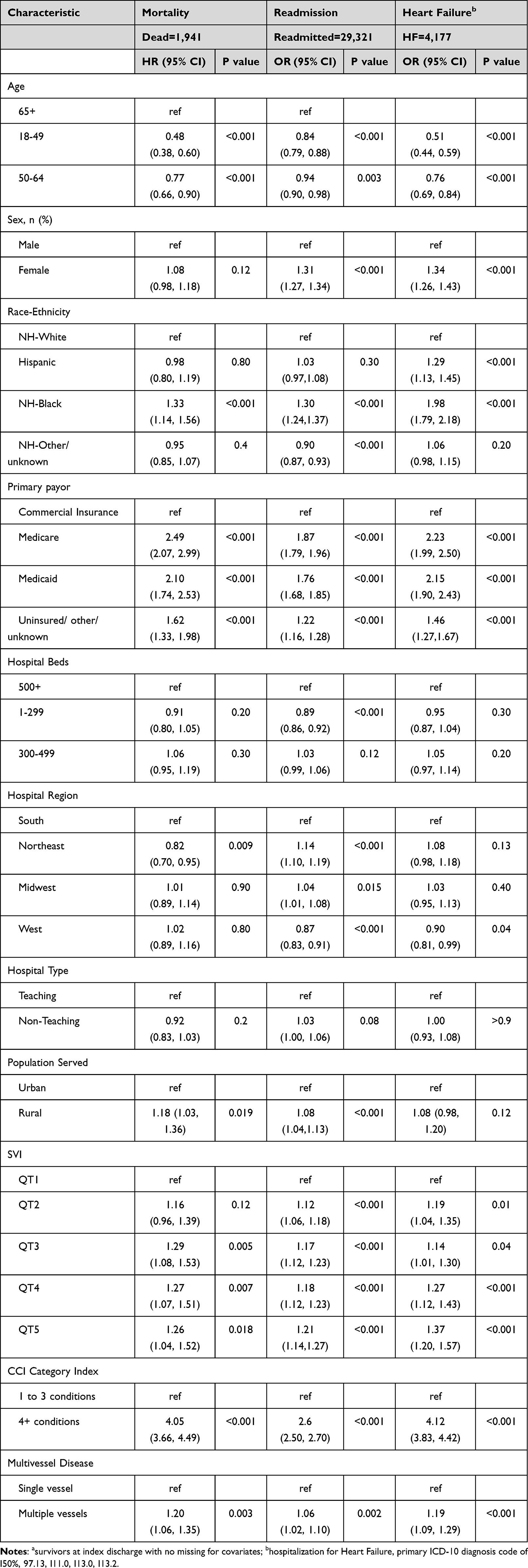 |
Table 3 Multivariable Regression Results for Assessing Factors Associated with 1-year Mortality, Readmission and Heart Failure Following Index Discharge in Patientsa with PCI for STEMI (n=168,043) |
Results of multivariable logistic regression analysis of risk factors for readmissions indicate that the odds of readmissions within 1 year of index PCI discharge were significantly higher for females, NH-Black, Medicare, Medicaid insurance, patients from rural hospitals, in the highest SVI group, CCI ≥4, and MVD. Odds of readmission within 1 year of index discharge was significantly lower for smaller size hospitals (vs. 500+ beds), those aged 18–64 years (vs. 65+), and hospitals in the West (p<0.05) compared to the respective reference groups. We observed a similar patient risk profile for HHF and increased total study cost at 1 year following index discharge (p<0.05). CCI ≥4 (vs. 1–3 conditions) and MVD contributed significantly more to higher all-cause total study cost adjusting for other factors (Table 4). The mean adjusted predicted total study cost up to 1 year since admission was $27,458.41 (95% CI: $26,938.94 -$27,987.89).
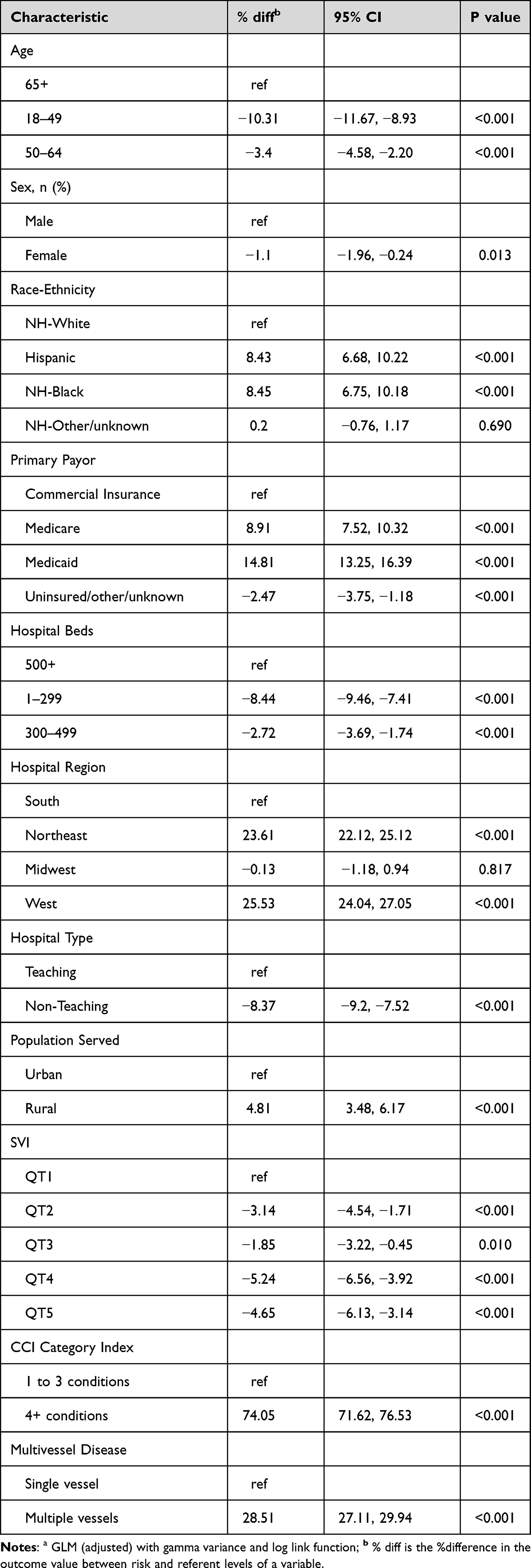 |
Table 4 Multivariable Regressiona Analysis for Total Study Costs Up to 1 Year, n=177,071 |
Results on 3-year Cohort
There were 63,469 patients who had their first PCI between October 2016 and December 2019 with a total of 59,714 patients alive at index discharge and were analyzed for 3-year follow-up outcome assessment. Patient, hospital, and clinical characteristics of this sample are provided in Supplementary Table S3. The cumulative all-cause death rate was 7.5% at 3 years following PCI. The proportion of cardiac arrythmias within 3 years following discharge ranged between 0.8% and 3.6%. We found rates of readmission and HHF rates were similar to rates observed for the full sample, and there were similar risk profiles associated with 3-year mortality, readmissions, HHF, and total study cost as those associated at 1 year (data not shown).
Sensitivity Analysis
We conducted descriptive analysis of clinical and economic outcomes on claims linked data (n= 20,391 patients) to evaluate the patient journey, including encounters in non-PHD hospitals (Supplementary Table S4). Diagnosis of atherosclerotic heart disease, hypertension, STEMI of unspecified site, non-STEMI, and sepsis were the top reasons for 1-year readmission. Among the clinical outcomes, the following were observed at 1 year after index discharge (n=19,890 alive patients): atrial fibrillation (9.8%), ventricular tachycardia (6.4%), ventricular fibrillation (4.1%), and HF (12.6%). About 20% were readmitted (19.1%), and 87% revisited a hospital-based outpatient clinic. Less than 5% had reinfarctions (4.1%) or recurrent STEMI events (2.9%). The repeat PCI rate was less than 10%, with fewer patients (n=177) hospitalized for unstable angina. The median length of hospital stay was 6 days (Q1-Q3: 3.0–12.0), and the median total follow-up cost at 1 year was $9,472 (Q1-Q3: $3,296- $24,538). Results on HF rates (primary or secondary diagnosis) were consistent with the main analysis.
Discussion
This large, contemporary, observational study documents several major findings in patients with STEMI following PCI over a 5-year study period. First, there was a high prevalence of comorbid conditions in these patients and those with MVD. Second, significant associations with outcomes were observed in the demographic, clinical, and risk profiles of patients undergoing PCI for STEMI, indicating inequities in health outcomes. Third, increased cost and high utilization of healthcare services continued among patients with STEMI after PCI. Finally, although we found a lower incidence of HHF in the year after index discharge, HF with other circulatory conditions and 1-year cumulative mortality rates were comparable to published results, indicating the presence of unmet healthcare needs of patients with STEMI following PCI.
In this study, although the number of PCIs performed from October 2016 to December 2021 remained stable (average: 8,604 procedures/per quarter), a higher number of older, women, racial/ethnic minority patients, and those residing in high-vulnerable counties were at higher risk of negative outcomes, which underscores the importance of including underserved populations for pre-revascularization risk assessment. The higher prevalence of clinical comorbid conditions with a CCI comorbidity index score of 4+ conditions, and the fact that more than 30% of patients in this study were at severe to extreme severity of illness stage at index visit, may reflect the actual US population health status, thus posing a challenge in managing these patients post-PCI. With the increasing prevalence of comorbid conditions, the 1-year risk-adjusted mortality also increased. In addition, MVD as an independent predictor of 1-year mortality and HF in this study is consistent with a published report in which findings were attributed to reduced left ventricular ejection fraction (LVEF) and a high prevalence of risk factors.16 Information on LVEF and infarct size were unavailable in our database.
Despite advances in PCI and management of STEMI, studies reported that survival after PCI varies depending on several factors. Globally, there is variability in mortality prevalence. A Danish matched study showed that STEMI was associated with a 5.9% excess mortality from 0 to 30 days, and this excess rate remained from 31 to 90 days. However, this study reported low excess mortality of 2% by 10 years among those who survived the first 90 days after PCI, probably due to high use of preventive medications and close monitoring of patients.17 The cumulative 1-year mortality rate of 6.6% found in our study is consistent with a previous report,18 but it is less than the pooled mortality rate of 10% (prevalence range: 2% to 59%) reported in a systematic review and meta-analysis of 91 cohort studies, in which 17 risk factors significantly associated with mortality were identified.19
Generally, the 30-day, 90-day, and 1-year mortality rates following PCI for STEMI are 2.7% to 8%,20 2.3% to 13.1% depending on age,21 and 2% to 59%,19 respectively. We did not assess door-to-balloon time, hospital volume, operator experience, or complexity of coronary lesions, which could have influenced our risk adjustment.
Readmission Rate
All-cause readmissions to the hospital after PCI discharge has a potential impact on patient outcomes and cost of care. Although similar to published literature (with 4.7 to 15.6% at 30 days7,22,23 and 18.6–50.4% at 1 year),24 the all-cause readmission rate following PCI we observed in our study (7.8% at 30 days, 11.1% at 90 days, and 17.4% at 1 year) demonstrates a need to improve care quality for these patients. The predictors of 1-year readmission such as being female, being of Black race, having MVD, and having more comorbid conditions may indicate women delay seeking medical care and present with more complications than men, and those with MVD resulting in recurrent ischemic events and those with comorbid conditions with poor compliance to medical therapy may contribute to the risk of readmission following PCI. We found a lower prevalence of use of antiplatelets, beta blockers, and other therapeutic medications following PCI discharge (data not shown), likely due to patients obtaining prescriptions over the counter, receiving medications during hospitalizations at a non-index hospital, or facing challenges in maintaining an antithrombotic or antiplatelet regimen due to cardiac arrythmias like atrial fibrillation.
Length of Stay
Our study participants tended to stay longer when readmitted within 1 year following index discharge, thus driving hospital follow-up cost, contrary to findings reported in another study,7,25 but within the range reported in a scoping review (LOS: up to 10.2 days).26 The average longer LOS post-PCI could be due to post-procedure complications, including those associated with HF, reinfarctions, and higher prevalence of comorbidities.
Heart Failure
Globally, HF is a significant clinical burden with high readmission and mortality rates,27,28 although HF rates vary across countries due to differences in healthcare access, treatment protocols, HF definitions used, and patient characteristics. One study on patients with primary PCI for STEMI reported HF rates of 7.9% at 1 year and 13.3% at 3 years with a HF related hospitalization rate of 6.1% at 1 year and 9.5% at 3 years.29 A European study reported HF incidence of 10% during a median follow-up of 3.7 years post-STEMI with intact or reduced LVEF.30 In the US, studies report 1-year and 2-year readmission rates for HF to be 10.6% and 19.3%, respectively. This is particularly observed in Medicare and older populations.31 Attempts to reduce HF incidence after PCI for STEMI need effective post-PCI management strategies, including treatment optimization.
At index, we found higher rates of HF and use of anticoagulants, antiplatelets, and beta blockers, comparable to those reported in the literature, but lower prevalence of primary diagnosis of HF within 1 year following index discharge (both hospitalizations and revisits) when we defined HF with and without other diseases of the circulatory system (eg., hypertensive heart and chronic kidney disease). Lower prevalence at follow-up could be due to more patients already having HF during the index visit, and the primary reason for readmission or revisit was something more serious than HF alone. Also, we did not assess how many patients underwent complete revascularization during index visit which limits our ability to attribute the observed reduction in hospitalization rate due to primary diagnosis of HF in the year following index discharge. When we considered primary or secondary diagnosis of HF with/without other circulatory disease conditions, the prevalence of HF in the year following index discharge was consistent with previous studies.29,32 This was also confirmed in our sensitivity analysis using PHD linked claims data, in which patients visiting non-index hospitals were also captured (1-year: HF: 12.9%, 3-year: 16.6%, Supplementary Table S4).
Among other cardiac clinical events, cardiac arrythmias, especially ventricular fibrillation (VF) and tachycardia (VT), are frequently reported (8.9%) complications following PCI for STEMI, with an overall risk of 2.4% for late VT or VF. These late events have shown significant associations with in-hospital mortality (OR: 6.4, 95% CI: 5.63–7.29).33 We found similar prevalence of VF (8.8%) and slightly higher rates of VT (13.8%) at index visit, but found higher rates of atrial fibrillation (3.9%) than VT or VF by 1 year following index discharge, indicating patients may be at higher risk for stroke and mortality, which warrants continued, effective therapeutic strategies to prevent adverse outcomes.
Cost: The burden of cost following PCI for STEMI is substantial, averaging $19,327, with 1-year readmission cost averaging $8,037.25 We observed a slightly higher average index cost of $23,927 with a total burden of $30,340 up to 1 year following index discharge, which may indicate a higher risk profile of patients with STEMI. Identifying high-impact users is important to reduce costs, as is finding ways to reduce the cost of care without compromising the quality of recommended care for these patients.
Limitations
The PHD database is an administrative database, and therefore it is subject to several limitations as with all databases of this type. For example, the cause of death was not captured directly, and thus, we were not able to ascertain deaths due to cardiac causes without medical records but relied on ICD diagnosis codes for the hospital visit. Misclassification was possible due to diagnostic or procedure coding errors, and we used the codes and descriptions provided by the hospitals. In addition, we may have missed some readmissions / revisits as patients could have gone to different hospitals, and our databases may not have captured all readmissions and revisits. There may also be a potential selection bias with the use of a non-random sample of patients as well as with the first PCI, as this may not actually be the first time this procedure was performed for STEMI and may be outside the study timeframe. Complete patient journey up to 3 years after index discharge was evaluated for about 15% of patients who had linked claims data.
Although multivariable regression modelling was performed to identify risk factors for outcomes, there may have been unobservable characteristics we did not consider. For example, the cost of care after PCI may have been underestimated, as patients could have visited non-member hospital systems during the follow-up time. In addition, pre-index comorbidities and conditions not captured in the data may have influenced our results. We also relied on multiple sources for mortality information without confirming the actual date of death, which could have influenced our results. The study was also not designed to detect causal relationships between factors and outcomes, due to the retrospective nature of the study design. Finally, as 10% of the patients had unknown race, misclassification of race could have resulted in underestimation of the association between Black race and outcomes because the race and ethnicity captured in the PHD were based on self-report. As race is correlated with SVI and mortality,36 we acknowledge that missing race data can bias estimates of SVI–mortality associations by introducing confounding, potentially over- or underestimating effects, obscuring disparities, and diminishing overall model precision. Despite the above limitations, this study presents contemporary evidence and highlights the risk factors associated with 1-year negative clinical outcomes and higher cost following PCI for the treatment of STEMI in US adult patients.
Generalizability
The PHD is an all-payer administrative hospital database representing approximately 25% of all US inpatient admissions. Our results on patients visiting 633 US hospitals (both university-affiliated and community hospitals) are distributed across all regions of the US, and patients could be tracked across inpatient and outpatient settings within a single hospital and across multiple visits. Using linked claims data, we found that, although patients were more likely to be treated in a different hospital in the longer term, most came back to the same hospital for inpatient care in the short term. Therefore, findings on inpatient care in the short-term follow-up periods are more generalizable when PHD is used as the sole data source.
Conclusions
This study identified risk factors associated with 1-year negative clinical outcomes and increased cost following PCI for the treatment of STEMI. Despite improvements in care for patients with STEMI, risk-adjusted mortality has not been reduced but has remained stable, and adherence to guideline-directed medical therapies following PCI for this population is mostly underestimated. The results from this study suggest that continued efforts are needed to understand and identify vulnerable adult populations at risk for negative outcomes beyond the initial 3 months following PCI to improve outcomes and reduce disease burden in the US. Future research should also explore outcomes stratified by the location of the lesion, which may have an impact on LOS, readmission rate, and mortality. Timely referral to dedicated HF clinics, cardiac rehabilitation programs, and promotion of guideline-recommended prophylactic medical treatment should also be included in the STEMI-PCI care pathway.
Code Availability
All statistical analyses were conducted using RStudio V4.1.3 (Posit, PBC, Boston, MA). The programs are proprietary materials of Premier Applied Sciences, Premier Inc.; therefore, restrictions apply to the access of these codes, which cannot be made available publicly. Reasonable requests or questions related to the analysis will be addressed by authors.
Data Sharing Statement
The data supporting study findings are available from Premier Applied Sciences, Premier Inc. Restrictions apply to data availability due to license for the current study. Researchers interested in obtaining data used in this study can access the database through Premier Applied Sciences, Premier Inc., under a license agreement and payment of appropriate license fees.
Ethical Approval
Based on US Title 45 Code of Federal Regulations, Part 46, this study was exempt from institutional review board approval. The study consisted of records-based research using secondary de-identified Health Insurance Portability and Accountability Act compliant data and as such was exempt from ethics committee review. Informed consent was not obtained from study participants due to the nature of the deidentified data.
Acknowledgments
The authors would like to thank Cate Polacek, MLIS, Senior Medical Writer (formerly at Premier Applied Sciences, Premier Inc.) for her editorial support and Rheana Lipscomb, MPH, Manager Research Operations, Premier Applied Sciences, Premier Inc. in preparing this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported and funded by Boehringer Ingelheim Pharmaceuticals, Inc. The authors did not receive payment related to the development of the manuscript. The authors meet criteria for authorship as recommended by the ICMJE. Boehringer Ingelheim Pharmaceuticals, Inc. was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Disclosure
SK, MT, MS, and ZC are employees of Premier Inc. BC and BMKD are employees of Boehringer Ingelheim Pharmaceuticals, Inc. (BIPI). VWJ is an employee of Boehringer Ingelheim International GmbH. The authors report no other conflicts of interest in this work.
Part of the material in this manuscript was presented at the American Heart Association Annual Meeting, 16–18 Nov 2024, Chicago, IL, USA.
References
1. Martin SS, Aday AW, Almarzooq ZI, et al. 2024 heart disease and stroke statistics: a report of US and global data from the American Heart Association. Circulation. 2024;149(8):e347–17. doi:10.1161/CIR.0000000000001209
2. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2023 update: a report from the American Heart Association. Circulation. 2023;147(8):e93–e621. doi:10.1161/CIR.0000000000001123
3. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics--2014 update: a report from the American Heart Association. Circulation. 2014;129(3):e28–e292. doi:10.1161/01.cir.0000441139.02102.80
4. Amin AP, Patterson M, House JA, et al. Costs associated with access site and same-day discharge among medicare beneficiaries undergoing percutaneous coronary intervention: An Evaluation of the Current Percutaneous Coronary Intervention Care Pathways in the United States. JACC Cardiovasc Interv. 2017;10(4):342–351. doi:10.1016/j.jcin.2016.11.049
5. Ahmad M, Asghar M, Joshi U, et al. Study of association between different coronary artery disease presentations and its effect on short-term mortality, readmission, and cost in patients undergoing percutaneous coronary interventions. Cureus. 2021;13(8):e16862. doi:10.7759/cureus.16862
6. Asad ZUA, Khan SU, Amritphale A, et al. Early vs late discharge in low-risk ST-elevation myocardial infarction patients treated with percutaneous coronary intervention: a systematic review and meta-analysis. Cardiovasc Revasc Med. 2020;21(11):1360–1368. doi:10.1016/j.carrev.2020.04.030
7. Jang S-J, Yeo I, Feldman DN, et al. Associations between hospital length of stay, 30-day readmission, and costs in ST-segment–elevation myocardial infarction after primary percutaneous coronary intervention: a nationwide readmissions database analysis. J Am Heart Assoc. 2020;9(11):e015503. doi:10.1161/JAHA.119.015503
8. Raja DC, Chopra A, Subban V, et al. Predictors of short-term outcomes in patients undergoing percutaneous coronary intervention in cardiogenic shock complicating STEMI—A tertiary care center experience. Indian Heart J. 2018;70(Suppl 3):S259–S264. doi:10.1016/j.ihj.2018.03.006
9. Swaminathan RV, Rao SV, McCoy LA, et al. Hospital length of stay and clinical outcomes in older STEMI patients after primary PCI: a report from the National Cardiovascular Data Registry. J Am Coll Cardiol. 2015;65(12):1161–1171. doi:10.1016/j.jacc.2015.01.028
10. Premier Applied Sciences, Premier Inc. Premier Healthcare Database: Data That Informs and Performs (White Paper). 2025. Available from: https://offers.premierinc.com/Premier-Healthcare-Database-Download.html.
11. Quan H, Li B, Couris CM, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(6):676–682. doi:10.1093/aje/kwq433
12. Baram D, Daroowalla F, Garcia R, et al. Use of the All Patient Refined-Diagnosis Related Group (APR-DRG) risk of mortality score as a severity adjustor in the medical ICU. Clin Med Circ Respirat Pulm Med. 2008;2:19–25. doi:10.4137/ccrpm.s544
13. Iezzoni LI, Ash AS, Shwartz M, Daley J, Hughes JS, Mackiernan YD. Predicting who dies depends on how severity is measured: implications for evaluating patient outcomes. Ann Intern Med. 1995;123(10):763–770. doi:10.7326/0003-4819-123-10-199511150-00004
14. Agency for Toxic Substances and Disease Registry. CDC/ATSDR social vulnerability index. Available from: https://www.atsdr.cdc.gov/place-health/php/svi/svi-data-documentation-download.html.
15. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
16. van der Schaaf RJ, Timmer JR, Ottervanger JP, et al. Long-term impact of multivessel disease on cause-specific mortality after ST elevation myocardial infarction treated with reperfusion therapy. Heart. 2006;92(12):1760–1763. doi:10.1136/hrt.2005.086058
17. Thrane PG, Olesen KKW, Thim T, et al. 10-year mortality after ST-segment elevation myocardial infarction compared to the general population. J Am Coll Cardiol. 2024;83(25):2615–2625. doi:10.1016/j.jacc.2024.04.025
18. Gao M, Zhao W, Zhang Z, Qin L, Zhang W, Zheng Y. Clinical characteristics and outcomes in young patients with st-segment elevation myocardial infarction after primary percutaneous coronary intervention. Am J Med Sci. 2018;355(6):544–552. doi:10.1016/j.amjms.2018.02.003
19. Yan F, Zhang Y, Pan Y, et al. Prevalence and associated factors of mortality after percutaneous coronary intervention for adult patients with ST-elevation myocardial infarction: a systematic review and meta-analysis. J Res Med Sci. 2023;28(1):17. doi:10.4103/jrms.jrms_781_21
20. Pedersen F, Butrymovich V, Kelbaek H, et al. Short- and long-term cause of death in patients treated with primary PCI for STEMI. J Am Coll Cardiol. 2014;64(20):2101–2108. doi:10.1016/j.jacc.2014.08.037
21. Gharacholou SM, Lopes RD, Alexander KP, et al. Age and outcomes in ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention: findings from the APEX-AMI trial. Arch Intern Med. 2011;171(6):559–567. doi:10.1001/archinternmed.2011.36
22. Kwok CS, Rao SV, Potts JE, et al. Burden of 30-day readmissions after percutaneous coronary intervention in 833,344 patients in the United States: predictors, causes, and cost: insights from the nationwide readmission database. JACC Cardiovasc Interv. 2018;11(7):665–674. doi:10.1016/j.jcin.2018.01.248
23. Tripathi A, Abbott JD, Fonarow GC, et al. Thirty-day readmission rate and costs after percutaneous coronary intervention in the United States: a national readmission database analysis. Circ Cardiovasc Interv. 2017;10(12). doi:10.1161/CIRCINTERVENTIONS.117.005925
24. Eccleston D, Duong M-N, Chowdhury E, et al. Early vs. Late readmission following percutaneous coronary intervention: predictors and impact on long-term outcomes. J Clin Med. 2023;12(4):1684. doi:10.3390/jcm12041684
25. Cowper PA, Knight JD, Davidson-Ray L, et al. Acute and 1-year hospitalization costs for acute myocardial infarction treated with percutaneous coronary intervention: results from the TRANSLATE-ACS registry. J Am Heart Assoc. 2019;8(8):e011322. doi:10.1161/JAHA.118.011322
26. Sugiharto F, Trisyani Y, Nuraeni A, Mirwanti R, Melati Putri A, Aghnia Armansyah N. Factors associated with increased length of stay in post primary percutaneous coronary intervention patients: a scoping review. Vasc Health Risk Manag. 2023;19:329–340. doi:10.2147/VHRM.S413899
27. Butler J, Hammonds K, Talha KM, et al. Incident heart failure and recurrent coronary events following acute myocardial infarction. Eur Heart J. 2025;46:1540–1550. doi:10.1093/eurheartj/ehae885
28. Foroutan F, Rayner DG, Ross HJ, et al. Global comparison of readmission rates for patients with heart failure. J Am Coll Cardiol. 2023;82(5):430–444. doi:10.1016/j.jacc.2023.05.040
29. Costa R, Trepa M, Oliveira M, et al. Heart failure incidence following st-elevation myocardial infarction. Am J Cardiol. 2022;164:14–20. doi:10.1016/j.amjcard.2021.10.035
30. Lenselink C, Ricken K, Groot HE, et al. Incidence and predictors of heart failure with reduced and preserved ejection fraction after ST-elevation myocardial infarction in the contemporary era of early percutaneous coronary intervention. Eur J Heart Fail. 2024;26(5):1142–1149. doi:10.1002/ejhf.3225
31. Martin J. Persistent mortality and heart failure burden of anterior ST-segment elevation myocardial infarction following primary percutaneous coronary intervention: real-world evidence from the US medicare data set. BMJ Open. 2023;13(6):e070210. doi:10.1136/bmjopen-2022-070210
32. Gho J, Postema PG, Conijn M, et al. Heart failure following STEMI: a contemporary cohort study of incidence and prognostic factors. Open Heart. 2017;4(2):e000551. doi:10.1136/openhrt-2016-000551
33. Rymer JA, Wegermann ZK, Wang TY, et al. Ventricular arrhythmias after primary percutaneous coronary intervention for STEMI. JAMA Network Open. 2024;7(5):e2410288. doi:10.1001/jamanetworkopen.2024.10288
34. Bergmark BA, Osborn EA, Ali ZA, et al. Association between intracoronary imaging during PCI and clinical outcomes in a real-world US medicare population. J Soci Cardiovascu Angiography Intervent. 2023;2(2):100556. doi:10.1016/j.jscai.2022.100556
35. Centers for Medicare & Medicaid Services. Billing and coding: percutaneous coronary interventions. Available from: https://www.cms.gov/medicare-coverage-database/view/article.aspx?articleId=57479.
36. Tong X, Carlson SA, Kuklina EV, et al. Social vulnerability index and all-cause mortality after acute ischemic stroke, medicare cohort 2020-2023. JACC Adv. 2024;3(10):101258. doi:10.1016/j.jacadv.2024.101258
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiology, Drug Resistance, and Risk Factors for Mortality Among Hematopoietic Stem Cell Transplantation Recipients with Hospital-Acquired Klebsiella pneumoniae Infections: A Single-Center Retrospective Study from China
Liu YF, Liu Y, Chen X, Jia Y
Infection and Drug Resistance 2022, 15:5011-5021
Published Date: 30 August 2022
Mortality-Related Risk Factors and Novel Antimicrobial Regimens for Carbapenem-Resistant Enterobacteriaceae Infections: A Systematic Review
Hu Q, Chen J, Sun S, Deng S
Infection and Drug Resistance 2022, 15:6907-6926
Published Date: 28 November 2022
Multidrug-Resistant Bacteria on Critically Ill Patients with Sepsis at Hospital Admission: Risk Factors and Effects on Hospital Mortality
Maia MDO, da Silveira CDG, Gomes M, Fernandes SES, Bezerra de Santana R, de Oliveira DQ, Amorim FFP, Neves FDAR, Amorim FF
Infection and Drug Resistance 2023, 16:1693-1704
Published Date: 23 March 2023
A Prospective Study of Stroke Characteristics, Risk Factors, and Mortality in a Tertiary Hospital of Northern Ethiopia
Gidey K, Hailu A
International Journal of General Medicine 2023, 16:5051-5061
Published Date: 3 November 2023
The Burden of COPD with Type 2 Inflammation in North-West Continental Europe

Sandelowsky H, Løkke A, Kocks JWH, Grøttum HS, Bakke PS, Vasankari T
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2767-2785
Published Date: 7 August 2025