Back to Journals » International Journal of Women's Health » Volume 15
Clinical Analysis and Prognostic Prediction Model for Patients with Uterine Leiomyosarcoma at FIGO Stage I
Authors Chen S ![]() , Deng Y, Zhai Y, Zhan Y, Li X, Wang J, Bai H
, Deng Y, Zhai Y, Zhan Y, Li X, Wang J, Bai H
Received 30 January 2023
Accepted for publication 6 April 2023
Published 11 April 2023 Volume 2023:15 Pages 545—557
DOI https://doi.org/10.2147/IJWH.S406381
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Shuya Chen,1 Yunhan Deng,2 Yan Zhai,2 Yang Zhan,3 Xue Li,4 Jiandong Wang,1 Huimin Bai2
1Department of Gynecological Oncology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Beijing, People’s Republic of China; 2Department of Obstetrics and Gynecology, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Department of Pathology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Beijing, People’s Republic of China; 4Department of Pathology, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Jiandong Wang, Department of Gynecological Oncology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Qihelou Street, Dongcheng District, Beijing, 100006, People’s Republic of China, Tel +0086-13910566755, Email [email protected] Huimin Bai, Department of Obstetrics and Gynecology, Beijing Chao-Yang Hospital, Capital Medical University, No. 8, North Road of Workers Stadium, Chaoyang District, Beijing, 100020, People’s Republic of China, Tel +0086-01085231765, Email [email protected]
Purpose: To reveal the clinical status and construct a predictive prognostic model for patients with uterine leiomyosarcoma (uLMS) at International Federation of Gynecology and Obstetrics (FIGO) stage I.
Patients and Methods: The medical records of patients with stage I uLMS during the study period were retrospectively reviewed. Multiple imputation, Martingale residuals and restricted cubic spline were used for data processing. Univariate and multivariate analyses were used to determine independent prognostic factors. The Schoenfeld individual test was used to verify the proportional hazards (PH) assumption. The predictive ability of the nomogram was validated internally.
Results: Ultimately, 102 patients were included. The median age at diagnosis was 51 years old. During the medium follow-up time of 68 months, 55 (53.9%) patients developed recurrence. The median recurrence interval was 32 months. The most common metastatic site was the lung (27 cases). Eventually, 38 (37.3%) patients died of uLMS. The 3-year and 5-year overall survival rates were 66.0% and 52.0%, respectively. Age at diagnosis > 49 years, larger tumor size, MI> 10/10HPF, presence of LVSI and Ki-67 labeling index (LI) > 25% (P=0.0467, 0.0077, 0.0475, 0.0294, and 0.0427, respectively) were independent prognostic factors. The PH assumption remained inviolate. The concordance index was 0.847, the area under the time-dependent receiver operating characteristic curve surpassed 0.7, and the calibration curve showed gratifying consistency.
Conclusion: Age at diagnosis, tumor size, MI, LVSI, and Ki-67 LI were identified as independent prognostic factors for stage I uLMS. This prognostic nomogram would provide personalized assessment with superior predictive performance.
Keywords: uterine leiomyosarcoma, prognosis, nomogram, risk stratification
Introduction
Uterine leiomyosarcoma (uLMS) is a rare and heterogeneous entity with unknown aetiology, accounting for approximately 60–70% of uterine sarcomas.1 ULMS occurs most frequently in perimenopausal women and shows indistinct manifestations, such as vaginal bleeding and increasing abdominal girth.2 Approximately 60% of uLMS cases are diagnosed at International Federation of Gynecology and Obstetrics (FIGO) stage I, and stage is recognized as the most important prognostic factor of uLMS.1–7 However, patients with uterine-confined disease unexceptionally exhibited unfavourable prognoses. The reported 5-year overall survival (OS) rate was as low as 50.4–61.0% for stage I uLMS, while decreased to 22.3–47.7%, 16.0%-37.7% and 9.8%-17.4% for stage II, III and IV disease, respectively.4 Several other prognostic factors of uLMS have been discussed previously, but consensus was not reached.2–7 Despite, in terms of surgical management, whether oophorectomy and lymphadenectomy could be safely omitted in premenopausal women remains controversial.3,4,6 Reasons for these conflicting conclusions were partly owing to the small sample size and the unadjusted confounding bias in patients with all-stage diseases.
A medical nomogram is a pictorial representation of complex mathematical formulas. Compared with FIGO staging systems, nomograms are more comprehensive and conform to the trend of personalized medicine.8 Due to its rapid computation using user-friendly digital interfaces, increased accuracy and straightforward prognostic instructions, nomograms are widely adopted in prognostic prediction for many human diseases, especially malignancies.8 However, this evaluation mode is rarely used in uLMS.
Herein, focusing on stage I uLMS, this study aims to evaluate the current status, identify independent prognostic factors, construct the nomogram and build risk stratifications, thus to provide useful information for clinical managements and facilitate future clinical trials.
Materials and Methods
All consecutive patients with uLMS who were diagnosed and treated at Beijing Obstetrics and Gynecology Hospital and Beijing Chaoyang Hospital from January 2011 to December 2021 were registered within a computerized cancer database. The patients’ clinical information was retrospectively reviewed, and all cases were restaged according to the 2009 FIGO staging system for uLMS. Hallmark histologic features of uLMS included spindle cells with blunt-ended nuclei, brisk mitotic activity (>10/10HPF) with atypical forms, nuclear pleomorphism, hypercellularity with a fascicular growth pattern, coagulative necrosis, and infiltration of the surrounding myometrium.2 The inclusion criteria were: (1) tumors were pathologically confirmed as stage I uLMS without any evidence of extrauterine metastasis; and (2) the initial treatment was surgery. Patients who received preoperative adjuvant radiotherapy and/or chemotherapy, had other types of malignant tumors, or were lost to follow-up immediately after surgery were excluded. Two experienced pathologists, specialized in gynecologic pathology, were blinded to patient outcomes and independently reviewed all the pathological sections for the purposes of this study. In case of discrepancy, a third pathologist reviewed the slides. Consensus was ultimately reached through discussion. Patient consent was waived due to the retrospective nature of this study. We confirmed that the privacy of participants would be kept in strict confidence. The study was carried out in accordance with the ethical standards laid down in the Declaration of Helsinki, and was approved by the ethics committees of Beijing Obstetrics and Gynecology Hospital, Affiliated China Capital Medical University, and Beijing Chao-Yang Hospital, Affiliated China Capital Medical University.
All patients received total hysterectomy with or without oophorectomy as the initial treatment. Suspected lymph nodes (LNs) or the discretion of the senior surgeon for complete disease staging influenced the decision of applying systematic pelvic with or without para-aortic lymphadenectomy. Omentectomy was selectively performed for surgical staging. Tumor size was defined as the maximum dimension of a single tumor.3 Lymph-vascular space invasion (LVSI) was defined by the presence of tumor cells in or attached to blood vessels or lymphatic spaces. Mitotic index (MI) was defined as the highest count in any one set of 10 HPFs (HPF = 0.196 mm2) in the most cellular areas.9 The expression level of the Ki-67 labeling index (LI) was detected using immunohistochemical staining. The Ki-67 LI proliferation level was measured and presented as the coverage percentage of positive tumor cells.10
Postoperative adjuvant treatment was chemotherapy alone or combined with radiotherapy. The main adjuvant intravenous chemotherapy regimens consisted of GD (gemcitabine, 900 mg/m2, Day 1 and Day 8, and docetaxel, 75 mg/m2, Day 1, iv, q21 days) and PEI (cisplatin, 70 mg/m2, d1, epirubicin, 60 mg/m2, d1, ifosfamide, 1.5 g/m2, d1–3, mesna, 0.2 g, 0, 4, or 8 h postifosfamide application, d1–3, iv, q28 days). In total, 4–6 cycles of chemotherapy were administered. Pelvic irradiation with a total dose of 40–50 Gy delivered over 5–6 weeks was the main scheme.
Regular surveillance was arranged every 3 months for 3 years and then every 6 months thereafter when treatment accomplished. Patients for whom regular information was not available were contacted through telephone or mail to acquire more data. Complete response was defined by the disappearance of all known lesions. Recurrence was defined by clinical or imaging evidence and confirmed by pathology. Debulking surgery, salvage chemotherapy, and/or radiation therapy was administered based on the doctor’s advice, patients’ physical condition and/or their fully informed consent. Progression-free survival (PFS) was defined as the period between initial surgery and recurrence. OS was calculated in months from the date of initial surgery to the date of death. Patients who died from other conditions and survivors at the last follow-up were censored.
Statistical Analysis
The missing data were imputed by multiple imputation using the Markov chain Monte Carlo method.11 Martingale residual was adopted to assess the functional forms of continuous variables and survival analysis.12 Restricted cubic spline (RCS) was used for nonlinear fitting. The cut-off value was excavated to transform continuous variables into categorical variables. To balance the best fit and overfitting in the main splines for variables and survival outcomes, 5 knots was chosen as the lowest value for the Akaike information criterion (AIC).8 The Kaplan–Meier method and Log rank test were used to analyse the survival curves. A Cox proportional hazards (PH) model was used to assess all significant parameters in the univariate analysis. The PH assumption was assessed using the Schoenfeld individual test, and visually inspected for potential time-variant biases. All P values were two-tailed. P < 0.05 was considered as statistically significant.
A nomogram was constructed to estimate the 3-/5-year death probabilities of FIGO stage I uLMS. Each variable corresponded to a certain value. The total points (TPs) was determined based on the individual scores. The concordance index (C-index) and area under the time-dependent receiver operating characteristic curve (time-dependent AUC) calculated by 1000 bootstrapped samples were adopted to assess discriminative ability. Calibration plots were used to evaluate calibration ability. The C-index and AUC values vary from 0.5 to 1.0, where 0.5 represents random chance and 1.0 indicates a perfect fit. Typically, a reasonable estimation was defined as both C-index and AUC values greater than 0.7. X-tile 3.6.1 software was used to excavate the cut-off point for risk stratification.13
All statistical analyses were conducted using the R 4.1.1 programming language and environment (http://www.r-project.org/).
Results
A total of 112 cases of stage I uLMS were diagnosed and treated during the study period. Patients with other concurrent types of carcinomas (n=4) or lacking follow-up information (n=6) were excluded. Ultimately, 102 patients were included.
The clinicopathological features and treatment profiles of 102 stage I uLMS patients are shown in Table 1. The median age at diagnosis was 51 (range: 35–79) years, and 57.8% of patients were over 49 years. Premenopausal women accounted for 65 (63.7%) cases, and 8 (7.8%) women were nonnulliparous. Metrorrhagia was the most common presentation (50 cases), followed by pelvic pain (38 cases). Twenty (19.6%) patients were asymptomatic. The median serum CA125 level was 12.7 (range: 1.4–122.0) U/mL, and 10 (9.8%) patients exhibited an elevation over 35 U/mL. Preoperative diagnostic curettage was performed in 19 patients, yet only 14 were accurately diagnosed with uLMS. Fifty-one (50%) were diagnosed through postoperative paraffin pathology.
 |
Table 1 Clinico-Pathological Characteristics of 102 Patients with Stage I uLMS |
All patients underwent hysterectomy by means of laparotomy (58 cases) or laparoscopy (44 cases) (Table 1). Bilateral oophorectomy was performed in 79 cases (77.5%). Initial lymphadenectomy was performed in 31 (30.4%) cases. Two (2.0%) received omentectomy. Tumor size ranged from 0.7 to 22 cm, with an average of 8.2±4.0 cm. Spindle cell tumors remained the most common type (102 cases, 91.2%). The medium MI was 10/10HPF, ranging from 2 to 28/10HPF, and 44 (43.1%) showed MI surpassing 10/10HPF. Coagulative necrosis was observed in 69 (67.6%) cases. LVSI was present in 25 (24.5%) cases. The mean number of removed LNs was 15 per patient, yet none were positive. Ki-67 LI varied widely from 3% to 85%, with a medium value of 35%, and 58 (56.9%) cases exhibited a Ki-67 LI over 25%. No extrauterine diseases were identified through pre/postoperative imaging examinations, such as abdominal/pelvic ultrasound, computed tomography and/or magnetic resonance imaging.
Adjuvant chemotherapy and chemoradiotherapy were performed in 70 (68.6%) and 10 (9.8%) patients, respectively. The remaining 22 (21.6%) patients received simple observation. The main side effects were digestive tract reactions (57 cases) and myelosuppression (45 cases). No G3/G4 side effects and no treatment-related deaths were identified in this series.
When treatment was completed, all patients attained complete response and were followed up accordingly. During the medium follow-up time of 68 (range: 12–144) months, 56 (53.9%) patients developed recurrence. The median recurrence interval was 32 (range: 5–144) months. Lung (27 cases) was the most common metastatic site, followed by the pelvis (17 cases), peritoneum (14 cases), liver (4 cases), bone (2 cases) and ureter (1 case) (Table 1). The 3- and 5-year PFS rates were 48.0% and 38.0%, respectively. Salvage surgery or combined with chemotherapy were performed in 17 and 6 patients, respectively. Palliative chemotherapy was administered to 11 patients. Tumor control was achieved again in 17 (50%) patients. The remaining 22 patients, among whom 15 aged over 49 years, could not afford any further aggression treatment due to their poor physical condition. At the last contact, 39 (38.2%) patients died of uLMS. Thirteen (12.7%) patients lived with the disease and 50 (49.0%) patients had no evidence of disease. The 3- and 5-year OS rates were 66.0% and 52.0%, respectively.
The results of univariate and multivariate analysis were shown in Table 2. The scatter gram demonstrated that among continuous variables, only “tumor size” linearly correlated with patient survival (Figure 1A). The cut-off values were 49 years for age, 10/10HPF for MI and 25% for Ki-67 LI calculated by RCS (Figure 1B). In univariate analyses, age at diagnosis >49 years, larger tumor size, MI>10/10 HPF, LVSI and Ki-67 LI>25% were significantly associated with decreased OS (P=0.00035, <0.0001, <0.0001, <0.0001 and <0.0001, respectively). In multivariate analyses, age at diagnosis >49 years, tumor size, MI>10/10 HPF, LVSI and Ki-67 LI>25% were independent factors for unfavourable prognosis (P =0.0467, =0.0077, 0.0475, 0.0294 and 0.0427, respectively) (Figure 2A). The Schoenfeld individual test showed no variable was significant when the P value threshold was set to 0.05 (Figure 2B), suggesting the PH assumption of the model remained inviolate.
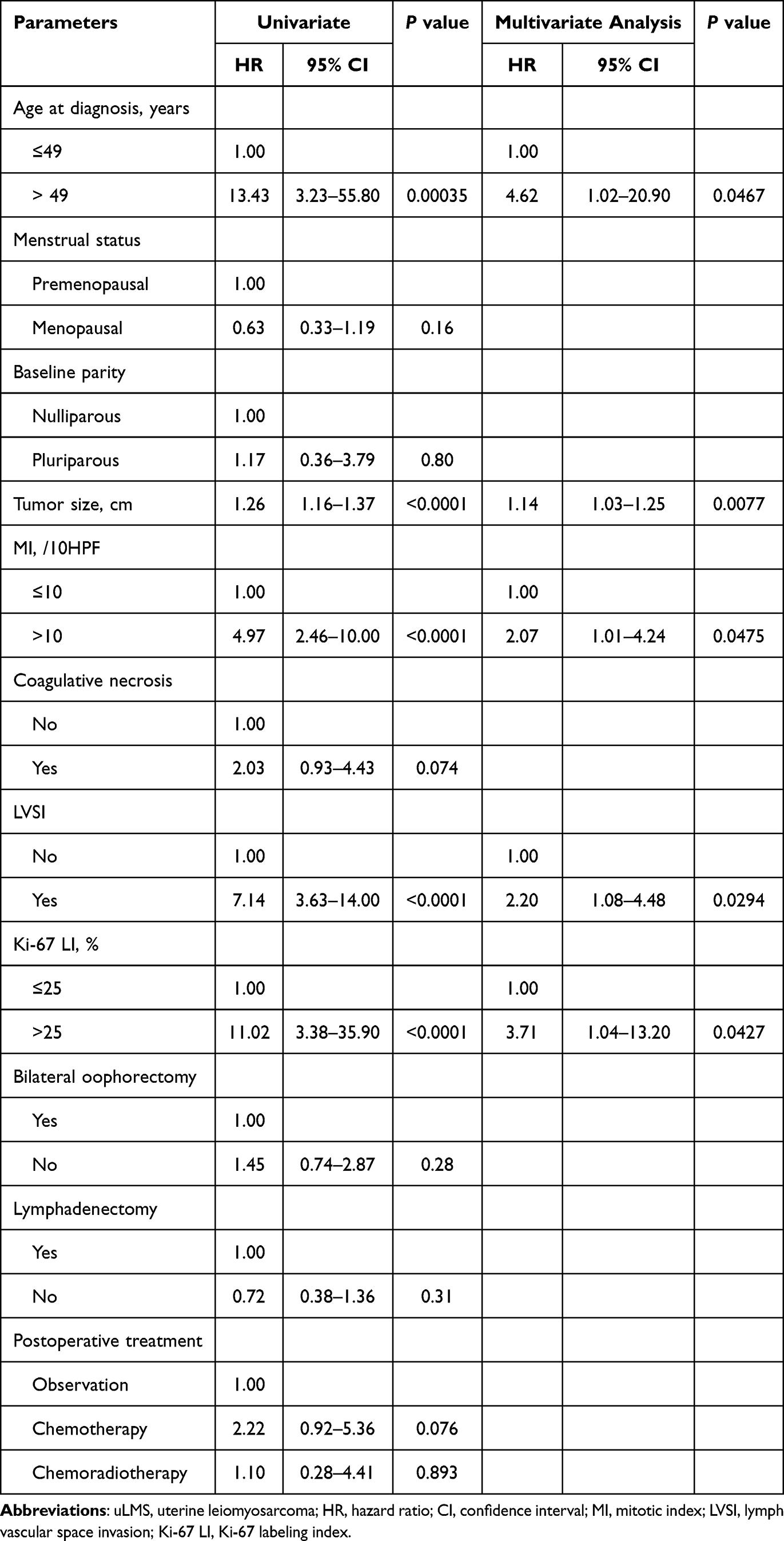 |
Table 2 Prognostic Factors of OS in Patients with Stage I uLMS |
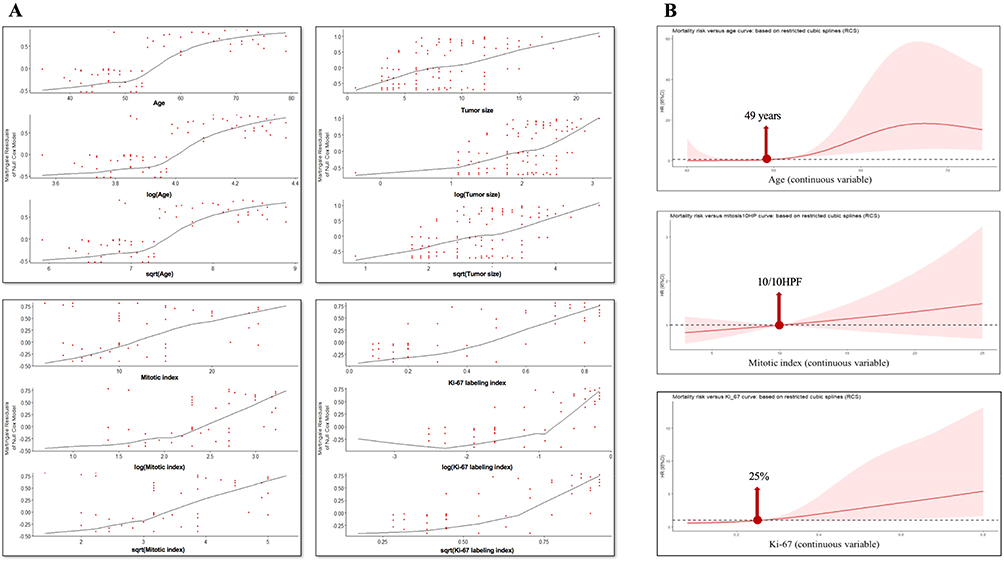 |
Figure 1 Data processing. (A) Martingale residual was adopted to assess the functional forms of continuous variables and survival analysis. The scatter gram showed that only “tumor size” conformed to the linear trend. (B) Restricted cubic spline with 5 knots was used for non-linear fit. The shaded area represented the 95% confidence index of hazard ratio. |
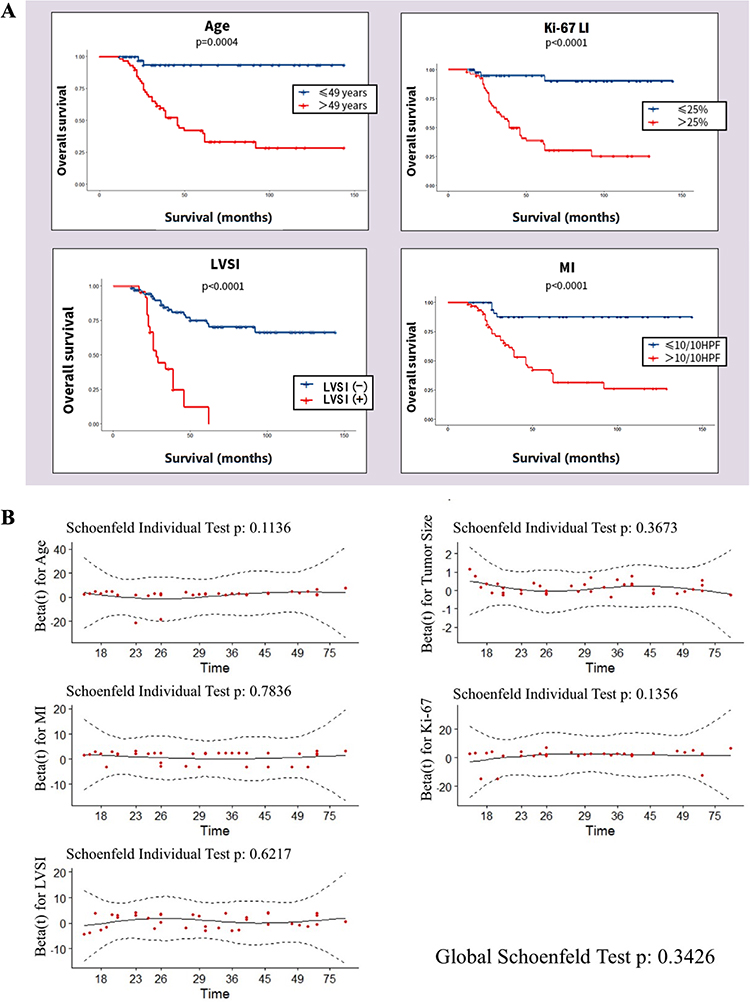 |
Figure 2 The prognostic factors and PH assumption validation of the Cox model. (A) Kaplan–Meier survival curves of prognostic factors for overall survival. The curve of tumor size was not shown owing to its continuous nature. (B) The Schoenfeld individual test showed all P values surpassed 0.05. |
A nomogram of stage I uLMS was showed in Figure 3. Patients had TPs ranging from 152 to 371. The C-index was 0.847. The time-dependent AUCs were both > 0.7 for the prediction of death within 3 and 5 years (Figure 4A), indicating its favourable discrimination. In the calibration curves of the nomogram, the red line was close to the blue dotted line, indicating the accuracy of the model for prediction of death probability (Figure 4B). Based on the nomogram’s TPs of 285 and 329, patients were stratified into low-, middle- and high-risk groups, with a 3-year death risk of <21.8%, 21.8–66.7% and >66.7% and a 5-year death risk of <38.3%, 38.3–88.5% and >88.5%, respectively. For patients with TPs lower than 258 and 233, their predictive 3-year and 5-year OS rates would surpass 90%. When TPs increased to 367 and 343, these two rates decreased to lower than 10%.
 |
Figure 3 The nomogram of stage I uLMS for overall survival prediction. Distributions of tumor size and total points were showed by density plot, while distributions of category variables were showed by sizes of boxes. The importance of each variable was ranked according to the standard deviation along nomogram scales. Abbreviations: MI, mitotic index; LVSI, lymph vascular space invasion; Ki-67 LI, Ki-67 labeling index. |
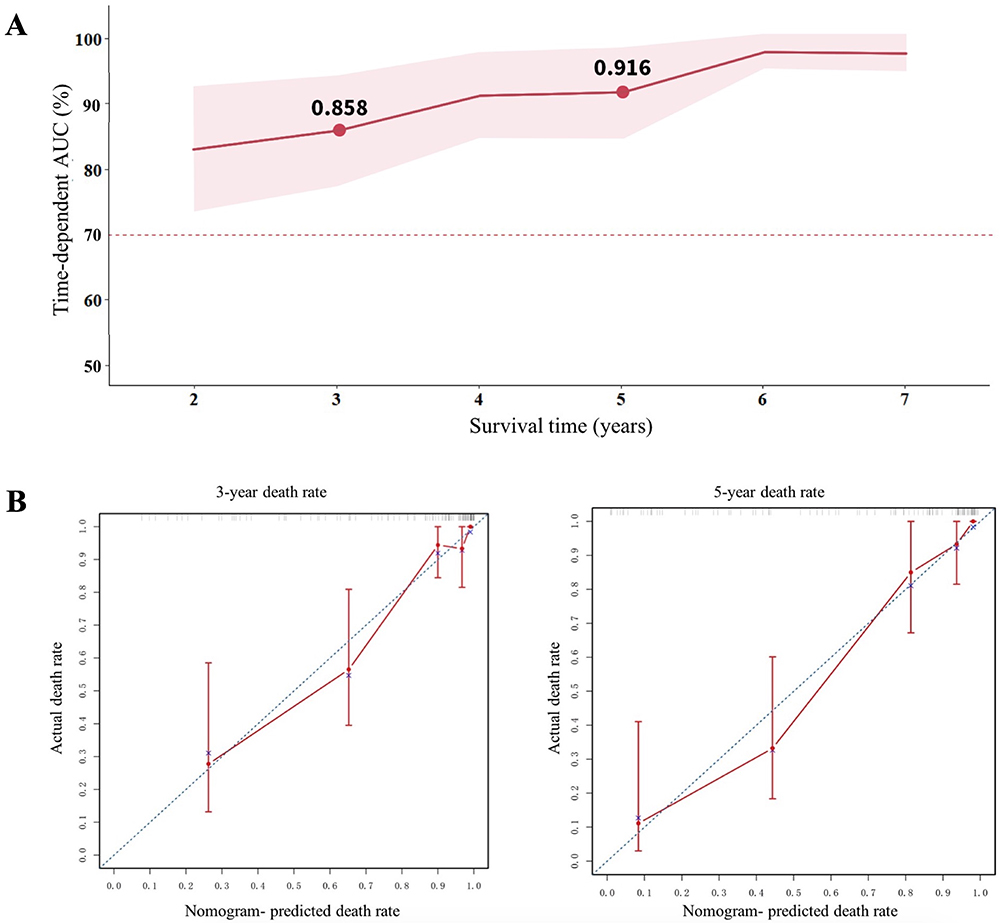 |
Figure 4 Time-dependent AUC and calibration curves of the nomogram. (A) The red line represented time-dependent AUC = 0.7. The shaded area represented 95% confidence interval, calculated by using the bootstrapping cross-validation method. (B) The blue dotted line represented the ideal reference line where predicted probabilities matched actual rates. The red dots represented the performance of the nomogram. Abbreviations: AUC, area under curve; uLMS, uterine leiomyosarcoma. |
Discussion
Studies regarding the clinical management and prognosis of stage I uLMS are rare. The majority of them were single case or very small series reports. Since data collection was challenging for uLMS, public databases have become a more common resource. Seagle et al4 compiled 1019 cases of stage I uLMS registered in the National Cancer Database (NCDB). Lu et al14 collected 1898 uLMS from the Surveillance, Epidemiology and End Results (SEER) database, depicted as localized, regional and distant disease (SEER stages). These two studies both claimed that a high grade of tumors significantly correlated with decreased survival. However, a universally accepted grading system for uLMS has not been established. The “grade criteria” used in these two studies were totally different. Tasci et al15 retrospectively analysed 95 uLMS patients, including 51 cases at stage I and revealed that grade was not necessarily associated with OS. In Pautier et al study,16 patients were graded according to the French Federation of Anticancer Centers grading score system. The authors also demonstrated that grade has no prognostic impact in uLMS. Apparently, the vast majority of accurately diagnosed uLMSs are high-grade tumors, with a reported proportion of 79.9% to 94.4%.4–6,15,17,18 Herein, in clinical practice, it was no longer mandatory for tumour grade to be described for uLMS in pathology reports.9 Additionally, several key parameters with potential prognostic impact on uLMS, such as LVSI and Ki-67 LI, were absent in the NCDB and SEER databases. These design flaws might bias their conclusions to some extent.
Nomograms have emerged as a simpler and more sophisticated tool to predict patient prognosis than conventional staging systems. The first uLMS-specific nomogram was constructed in 2012.19 The nomogram outperformed the traditional American Joint Committee on Cancer and FIGO staging systems. The C-index was 0.67. However, the predictive ability decreased discriminatively when the 5-year OS predicted probability surpassed 0.68.20 This study contained 185 uLMS at stages I to IV, which would introduce significant heterogeneity and lead to degradation in the reliability of the nomogram.
The clinicopathological parameters in the present analysis were relatively thorough and complete. Potential prognostic factors were comprehensively assessed in the stepwise regression. The 5-year OS rate for stage I uLMS in this study was 52.0%, falling between the reported rates of 50.4%-61.0%.4 The C-index was as high as 0.847. The time-dependent AUC surpassed 0.7, and calibration curves showed high consistencies. All these suggested the universal applicability and satisfactory predictive ability of our nomogram. Furthermore, the risk stratification, based on TPs of the nomogram, was able to identify patient groups effectively. The low-risk group with TPs <285 achieved 3-year and 5-year survival rates over 78.2% and 61.7%, respectively, while the rates plunged to 33.3% and 11.5% for the high-risk group. For patients with TPs lower than 258 and 233, their predictive 3-year and 5-year OS rates, respectively, surpassed 90%.
Similar to several previous studies, we identified older age, larger tumor size and higher MI are associated with adverse prognosis of stage I uLMS.3,6,14,21–24 Whereas, different from those literatures, the cut-off values of age and MI were determined using RCS, which was rigorous and accurate. In the current study, over half of patients surpassed 49 years. In comparison with patients ≤ 49 years old, the elderly patient group had a 4.62 times higher death risk. Hence, more detailed preoperative assessments for this counterpart would help with better prognostic evaluation and treatment customization. Age-adjusted Charlson comorbidity index, calculated by summing the weighted comorbidities and age of each patient,25 and frailty measurement, with the modified frailty index the most commonly used tool to define this syndrome,26 have been demonstrated to be fundamental to predict survival outcomes in gynaecological cancers. With larger sample size, integrating these factors appropriately in analysis would make the prediction model more multidimensional and practical.
Despite, the assortment of tumor size also merited discussion. Two studies concordantly demonstrated that patients with tumor size >5 cm have a significantly shortened OS.3,5 However, when the threshold was set to 7 cm22 or 11 cm,15 tumor size had no impact on survival. These conflicting results suggested that describing tumor size in a qualitatively dichotomized manner was not always effective for prognosis prediction. In this study, the smooth curve and uniformly distributed scatter in the plot resulting from Martingale residuals revealed that tumor size was linearly correlated with patient survival. Survival decreases drastically with increasing tumor size of stage I uLMS, thus it is necessary to completely resect uLMS as early as possible.
LVSI is considered to be the manifestation of lymphogenous and haematogenous dissemination.27 The reported incidence of LVSI present in uLMS was 22.2%-37.8%.28 In this study, the rate was 24.5%. Based on our data, the presence of LVSI was associated with 2.2-fold decreased survival. Mayerhofer et al.24 Pellanda et al21 and Vaz et al29 also confirmed that the presence of LVSI was a negative prognostic factor for uLMS. Haematogenous spread is the major metastatic route of uLMS.2 In endometrial cancer, even in patients with negative LNs, the presence of LVSI was associated with decreased survival, suggesting its role in haematogenous dissemination.27 This correlation in uterine sarcoma has not been reported, and need to be further explored in future studies.
Ki-67 is a nuclear protein expressed in all active periods of the cell cycle but is absent in G0.10 In a quantitative systematic review, the authors compiled 84 cases of stage I–IV uLMS and demonstrated that a Ki-67 LI over 10% was significantly associated with shortened survival.10 Whereas, the small sample size from each study without unified diagnostic criteria would introduce heterogeneity. In this analysis, over half of the patients exhibited a Ki-67 LI surpassing 25%, suggesting uLMS proliferated actively and was aggressive in nature. Ki-67 LI over 25% was independently associated with shortened OS, with a 3.71-fold increased hazard of death in stage I uLMS.
Our study did not find any correlation between oophorectomy and prolonged survival in stage I uLMS, similar to previous studies.3–5,17,30 The risk of ovarian metastasis for stage I uLMS is quite low. In this study of 79 patients who underwent bilateral oophorectomy, the rate was zero, in line with the reported incidence that ranges from 0 to 4.0%.5,6 Herein, for young patients stratified in the low-risk group, ovaries could be safely preserved. Additionally, the reported lymph node metastasis incidence for stage I uLMS was merely 0–3.5%.1 No patient had a positive node in the current study. Haematogenous metastasis is the major route of uLMS.2 Thus, the significance of lymphadenectomy is mainly for tumor staging to guide postoperative treatment. This procedure can also be omitted in low-risk patient groups.
To our knowledge, this is the first nomogram focusing on stage I uLMS exclusively with a relatively large sample size. Inherent biases of retrospective nature represented the major limitations. In addition, the validation results calculated by bootstrapping and cross-validation methods indicated the reliability and practicality of the constructed nomogram. The accumulation of more uLMS cases is warranted for further external validation.
Conclusion
Consequently, the present study analysed the clinical status of early-stage uLMS, and identified age at diagnosis, tumor size, MI, LVSI, and Ki-67 LI as independent prognostic factors. Given its increased accuracy, good clinical utility, and superior predictive ability, our nomogram would promote personalized patient assessment and treatment.
Acknowledgments
This work was sustained by Science & Technology Plan for Social Development of Chaoyang District (contract No. CYSF2214).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Juhasz-Böss I, Gabriel L, Bohle RM, et al. Uterine leiomyosarcoma. Oncol Res Treat. 2018;41:680–686. doi:10.1159/000494299
2. Roberts ME, Aynardi JT, Chu CS. Uterine leiomyosarcoma: a review of the literature and update on management options. Gynecol Oncol. 2018;151:562–572. doi:10.1016/j.ygyno.2018.09.010
3. Takehara K, Yamashita N, Watanabe R, et al. Clinical status and prognostic factors in Japanese patients with uterine leiomyosarcoma. Gynecol Oncol. 2020;157:115–120. doi:10.1016/j.ygyno.2020.01.022
4. Seagle B-L-L, Sobecki-Rausch J, Strohl AE, et al. Prognosis and treatment of uterine leiomyosarcoma: a national cancer database study. Gynecol Oncol. 2017;145:61–70. doi:10.1016/j.ygyno.2017.02.012
5. Giuntoli RL 2nd, Metzinger DS, DiMarco CS, et al. Retrospective review of 208 patients with leiomyosarcoma of the uterus: prognostic indicators, surgical management, and adjuvant therapy. Gynecol Oncol. 2003;89:460–469. doi:10.1016/S0090-8258(03)00137-9
6. Kapp DS, Shin JY, Chan JK. Prognostic factors and survival in 1396 patients with uterine leiomyosarcomas: emphasis on impact of lymphadenectomy and oophorectomy. Cancer. 2008;112:820–830. doi:10.1002/cncr.23245
7. Abeler VM, Royne O, Thoresen S, et al. Uterine sarcomas in Norway. A histopathological and prognostic survey of a total population from 1970 to 2000 including 419 patients. Histopathology. 2009;54:355–364. doi:10.1111/j.1365-2559.2009.03231.x
8. Balachandran VP, Gonen M, Smith JJ, et al. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16:e173–e180. doi:10.1016/S1470-2045(14)71116-7
9. D’Angelo E, Espinosa I, Ali R, et al. Uterine leiomyosarcomas: tumor size, mitotic index, and biomarkers Ki67, and Bcl-2 identify two groups with different prognosis. Gynecol Oncol. 2011;121:328–333. doi:10.1016/j.ygyno.2011.01.022
10. Travaglino A, Raffone A, Catena U, et al. Ki67 as a prognostic marker in uterine leiomyosarcoma: a quantitative systematic review. Eur J Obstet Gynecol Reprod Biol. 2021;266:119–124. doi:10.1016/j.ejogrb.2021.09.026
11. Sterne JA, White IR, Carlin JB, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393. doi:10.1136/bmj.b2393
12. Burne RM, Abrahamowicz M. Martingale residual-based method to control for confounders measured only in a validation sample in time-to-event analysis. Stat Med. 2016;35:4588–4606. doi:10.1002/sim.7012
13. Robert LC, Dolled-Filhart M, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res. 2004;10:7252–7259. doi:10.1158/1078-0432.CCR-04-0713
14. Lu YJ, Wang H, Fang LY, et al. A nomogram for predicting overall survival in patients with uterine leiomyosarcoma: a SEER population-based study. Future Oncol. 2020;16:573–584. doi:10.2217/fon-2019-0674
15. Tasci T, Karalok A, Taskin S, et al. Does lymphadenectomy improve survival in uterine leiomyosarcoma? Int J Gynecol Cancer. 2015;25:1031–1036. doi:10.1097/IGC.0000000000000452
16. Pautier P, Genestie C, Rey A, et al. Analysis of clinicopathologic prognostic factors for 157 uterine sarcomas and evaluation of a grading score validated for soft tissue sarcoma. Cancer. 2000;88:1425–1431. doi:10.1002/(SICI)1097-0142(20000315)88:6<1425::AID-CNCR21>3.0.CO;2-3
17. Leitao M, Sonoda Y, Brennan M, et al. Incidence of lymph node and ovarian metastases in leiomyosarcoma of the uterus. Gynecol Oncol. 2003;91:209–212. doi:10.1016/S0090-8258(03)00478-5
18. Hinchcliff E, Rumpf J, Ratan R, et al. Hormone receptor status and the role of oophorectomy in uterine leiomyosarcoma. Gynecol Oncol. 2022;167:490–495. doi:10.1016/j.ygyno.2022.09.024
19. Zivanovic O, Jacks LM, Iasonos A, et al. A nomogram to predict postresection 5-year overall survival for patients with uterine leiomyosarcoma. Cancer. 2012;118:660–669. doi:10.1002/cncr.26333
20. Iasonos A, Keung EZ, Zivanovic O, et al. External validation of a prognostic nomogram for overall survival in women with uterine leiomyosarcoma. Cancer. 2013;119:1816–1822. doi:10.1002/cncr.27971
21. Pellanda AF, De bari B, Deniaud-Alexandre E, et al. Outcome and prognostic factors in 110 consecutive patients with primary uterine leiomyosarcoma: a rare cancer network study. Chin J Cancer Res. 2017;29:521–532. doi:10.21147/j.issn.1000-9604.2017.06.06
22. Manuela P, Penault-Llorca F, Guillou L. Prognostic factors in early-stage leiomyosarcoma of the uterus. Int J Gynecol Cancer. 2009;19:385–390. doi:10.1111/IGC.0b013e3181a1bfbc
23. Mancari R, Signorelli M, Gadducci A, et al. Adjuvant chemotherapy in stage I-II uterine leiomyosarcoma: a multicentric retrospective study of 140 patients. Gynecol Oncol. 2014;133:531–536. doi:10.1016/j.ygyno.2014.03.001
24. Mayerhofer K, Obermair A, Windbichler G, et al. Leiomyosarcoma of the uterus: a clinicopathologic multicenter study of 71 cases. Gynecol Oncol. 1999;74:196–201. doi:10.1006/gyno.1999.5436
25. Di Donato V, D’Oria O, Giannini A, et al. Age-adjusted Charlson comorbidity index predicts survival in endometrial cancer patients. Gynecol Obstet Invest. 2022;87:191–199. doi:10.1159/000525405
26. D’Oria O, Golia D’Augè T, Baiocco E, et al. The role of preoperative frailty assessment in patients affected by gynecological cancer: a narrative review. Ital J Gynaecol Obstet. 2022;34:76–83. doi:10.36129/jog.2022.34
27. Tortorella L, Restaino S, Zannoni GF, et al. Substantial lymph-vascular space invasion (LVSI) as predictor of distant relapse and poor prognosis in low-risk early-stage endometrial cancer. J Gynecol Oncol. 2021;32:e11. doi:10.3802/jgo.2021.32.e11
28. Matsuo K, Takazawa Y, Ross MS, et al. Significance of lymphovascular space invasion by the sarcomatous component in uterine carcinosarcoma. Ann Surg Oncol. 2018;25:2756–2766. doi:10.1245/s10434-018-6547-x
29. Vaz J, Tian C, Richardson MT, et al. Impact of adjuvant treatment and prognostic factors in stage I uterine leiomyosarcoma patients treated in Commission on Cancer®-accredited facilities. Gynecol Oncol. 2020;157:121–130. doi:10.1016/j.ygyno.2019.12.008
30. Nasioudis D, Chapman-Davis E, Frey M, et al. Safety of ovarian preservation in premenopausal women with stage I uterine sarcoma. J Gynecol Oncol. 2017;28:e46. doi:10.3802/jgo.2017.28.e46
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Histological Severity of Cirrhosis Influences Surgical Outcomes of Hepatocellular Carcinoma After Curative Hepatectomy
Liang BY, Gu J, Xiong M, Zhang EL, Zhang ZY, Lau WY, Wang SF, Guan Y, Chen XP, Huang ZY
Journal of Hepatocellular Carcinoma 2022, 9:633-647
Published Date: 23 July 2022
A Nomogram Based on SEER Database for Predicting Prognosis in Patients with Mucinous Ovarian Cancer: A Real-World Study
Zhang K, Feng S, Ge Y, Ding B, Shen Y
International Journal of Women's Health 2022, 14:931-943
Published Date: 26 July 2022
A Novel Biomarker Scoring System Alone or in Combination with the GRACE Score for the Prognostic Assessment in Non-ST-Elevation Myocardial Infarction
Yao Y, Shao C, Li X, Wang Z, Zuo C, Yan Y, Lv Q
Clinical Epidemiology 2022, 14:911-923
Published Date: 2 August 2022
Nomogram for the Preoperative Prediction of the Macrotrabecular-Massive Subtype of Hepatocellular Carcinoma
Shan Y, Yu X, Yang Y, Sun J, Wu S, Mao S, Lu C
Journal of Hepatocellular Carcinoma 2022, 9:717-728
Published Date: 10 August 2022
Development and Validation of a Novel Nomogram Integrated with Hypoxic and Lactate Metabolic Characteristics for Prognosis Prediction in Hepatocellular Carcinoma
Qiu X, Dong L, Wang K, Zhong X, Xu H, Xu S, Guo H, Wei X, Chen W, Xu X
Journal of Hepatocellular Carcinoma 2024, 11:241-255
Published Date: 2 February 2024