Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Cholinesterase is a Potential Biomarker with High Accuracy for the Nephrotic Syndrome Diagnosis in Minors
Received 20 June 2022
Accepted for publication 3 October 2022
Published 17 October 2022 Volume 2022:15 Pages 2375—2383
DOI https://doi.org/10.2147/JMDH.S379249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiaoli Zhu,1 Jinxi Hu2
1Department of Laboratory Medicine, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Taizhou, People’s Republic of China; 2Department of Oncological Surgery, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Taizhou, People’s Republic of China
Correspondence: Jinxi Hu, Department of Oncological Surgery, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, No. 150 Ximen Road of Linhai, Taizhou, 317000, People’s Republic of China, Tel +86 18257689350, Email [email protected]
Background: Serum Cholinesterase (CHE) levels have been found to be elevated in individuals with nephrotic syndrome (NS); nevertheless, it is unknown whether CHE can serve as a biomarker for NS diagnosis and what its diagnostic relevance is for NS in minors.
Methods: In this study, 138 minors aged 1– 17 years with NS were enrolled, including 101 patients with the first episode of NS and 37 patients with relapsing NS. One hundred and four minors suffering from nephritis and 109 healthy minors were included as control groups. The clinical information and laboratory data of all NS patients and the control group were obtained. Logistic regression, correlation analyses and receiver operator characteristic curve were used to examine the value of CHE for NS patients.
Results: Compared to patients diagnosed with nephritis and healthy minors in the control group, the serum CHE levels of total/first episode/relapsing NS patients were substantially higher (P < 0.05). The CHE was an independent risk predictor of total (adjusted odds ratio [OR] = 2.23, 95% confidence interval [CI]: 1.57– 3.18)/first episode (adjusted OR = 4.02, 95% CI: 1.47– 11.08)/relapsing (adjusted OR = 2.04, 95% CI: 1.42– 2.93) NS, and was positively correlated with total cholesterol in total/first episode/relapsing NS patients, respectively. The optimal cutoff for total/first episode/relapsing NS all was 11 KU/L, but the diagnostic accuracy in first episode NS (area under the curve [AUC] = 0.96, 95% CI: 0.94– 0.98) was higher than the total NS (AUC = 0.93, 95% CI: 0.91– 0.96) and relapsing NS (AUC = 0.85, 95% CI: 0.78– 0.92).
Conclusion: CHE is a possible biomarker for NS and has good diagnostic accuracy for NS in minors, particularly for the first episode of NS in minors.
Keywords: cholinesterase, nephrotic syndrome, biomarker, diagnosis, minors
Introduction
Nephrotic syndrome (NS) is the most common kidney disorder predominant in children, with an incidence ranging from 2 to 7/100,000 children/year.1 NS is characterized by severe proteinuria, hypoalbuminemia, hypercholesterolemia, and peripheral edema. NS can run a frequently relapsing course and may be complicated with infection, venous thromboembolism, and acute kidney injury in children.2 Corticosteroid therapy is the main treatment approach for primary nephrotic syndrome (PNS), and approximately 80–90% of children with PNS achieve remission with initial corticosteroid therapy.3 There is a favorable prognosis for children with steroid-sensitive nephrotic syndrome (SSNS); however, around 80% of SSNS patients relapse after the first treatment regimen of corticosteroids.4 Therefore, approximately 10% of the cases of NS in children do not respond to corticosteroid therapy and are classified as steroid-resistant nephrotic syndrome (SRNS).5
Cholinesterase (CHE) is an enzyme capable of hydrolyzing various choline esters and is an alpha-glycoprotein synthesized in the liver.6 It plays a crucial part in the catabolism of various drugs.7 Increased CHE levels have been closely related to liver steatosis, obesity, lipid profile, insulin resistance, hypertension, and fatty liver infiltration degree.8 Way et al also reported that a significant increase in the activity of serum CHE was observed in 16 children with NS compared to 22 healthy children of comparable ages.9 However, with such a limited sample size, a clear conclusion for whether CHE level is associated with NS would be difficult to uphold. In addition, a few articles confirming this phenomenon have been published, and the relationship between CHE and NS is still not completely clear. Therefore, this study aimed to understand the relationship between serum CHE activity and NS in minors and further evaluate the accuracy of its diagnostic value by using CHE for NS.
Patients’ Methods
Patient Populations
The retrospective study was conducted at the Taizhou Hospital of Zhejiang Province from January 2012 to March 2019. One hundred and thirty-eight minors with NS (including 101 cases of the first episode NS and 37 cases of relapsing NS) were enrolled in the study, and 104 minors with nephritis and 109 healthy minors were enrolled as control groups. All minors were aged between 1 and 17 years old. The diagnostic criteria were in accordance with the 2012 KDIGO Clinical Practice Guideline for Glomerulonephritis.10 Among the 104 instances of nephritis, there were 90 cases of glomerulonephritis, 11 cases of nephritis of Schonlein-Henoch purpura, 1 case of lupus nephritis, and 2 cases of chronic glomerulonephritis. The Health Management Centre at Taizhou Hospital in Zhejiang Province conducted routine physical examinations on 109 healthy minors. Patients with fever, viral infections, autoimmune disorders, viral hepatitis, and other liver conditions were excluded. The research obtained informed consent from the minor’s parents or legal guardians and was authorized by the Zhejiang Province Ethical Committee of The Taizhou Hospital (#K20220845).
Data Management
The clinical and laboratory data were collected from the date of initial hospital admission (prior to any treatment). The concentration of serum CHE, alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), γ-glutamyl transpeptidase (GGT), glucose (GLU), total protein (TP), albumin (ALB), prealbumin (PA), serum creatinine (Scr), blood urea nitrogen (BUN), uric acid (UA), total cholesterol (TC), triglycerides (TG), total bilirubin (TB) and direct bilirubin (DB) were measured by the autoanalyzer (Hitachi 7600; Hitachi, Tokyo, Japan).
Statistical Analysis
SPSS Statistics 20.0 was used to conduct the statistical analysis. The independent samples t-test and the Mann–Whitney U-test were utilized to assess the differences in laboratory parameters between NS patients and nephritis/healthy adolescents. The independent sample t-test was utilized when the data had a normal distribution and were reported as mean and standard deviation. Conversely, when the data were not normally distributed, the Mann–Whitney U-test was utilized, and the values were represented as p50% (p25%, p75%). Moreover, univariate and multivariate logistic regression analyses were conducted to investigate putative risk variables for NS. The correlation between CHE and other laboratory values in NS was determined using correlation analysis, and the diagnostic value of CHE for NS was evaluated using a Receiver Operator Characteristic (ROC) curve. The difference of AUC of each index was compared by MedCalc statistical software.
Results
Baseline Characteristics Analysis in NS Patients
The clinical features of the NS and control groups are analyzed and listed in Table 1. The study included 138 minors (mean age: 8.6 ± 6.0 years, 27 females and 111 males) with NS, 104 minors (mean age: 9.6 ± 3.9 years, 58 females and 46 males) with nephritis, and 109 healthy minors (mean age: 8.8 ± 3.8 years, 39 females and 70 males). The NS patients were divided into two groups: the first episode NS (N = 101, mean age: 7.4 ± 5.9 years, 20 females and 81 males) and relapsing NS (N = 37, mean age: 11.9 ± 5.4 years, 7 females and 30 males). Compared to the nephritis patients, the levels of CHE, ALT, AST, TC and TG were significantly higher in the serum of total NS patients (all P < 0.05), and the levels of TP, ALB, PA, Scr, TB and DB were significantly lower in the serum of total NS patients (all P < 0.01). There were no significant differences across age, ALP, GGT, GLU, BUN and UA between the two groups (all P > 0.05). Compared to the nephritis patients, the levels of CHE, AST, TC and TG were significantly higher in the serum of first NS patients (all P < 0.01), and the levels of age, TP, ALB, PA, Scr, TB and DB were significantly lower in the serum of first episode NS patients (all P < 0.05). There were no significant differences in ALT, ALP, GGT, GLU, BUN and UA between the two groups (all P > 0.05). Compared to the nephritis patients, the levels of age, CHE, ALT, GGT, UA, TC and TG were significantly higher in the serum of relapsing NS patients (all P < 0.05), and the levels of ALP, TP, ALB, PA, TB and DB were significantly lower in the serum of relapsing NS patients (all P < 0.05), and there was no significant differences in AST, GLU, Scr and BUN between the two groups (all P > 0.05). Compared to the healthy minors, the levels of CHE, AST, UA, TC and TG were significantly higher in the serum of total NS patients (all P < 0.01), and the levels of ALP, TP, ALB, PA, TB and DB were significantly lower in the serum of total NS patients (all P < 0.01). There were no significant differences in age, ALT, GGT, GLU, Scr and BUN between the two groups (all P > 0.05). Compared to the healthy minors, the levels of CHE, AST, UA, TC and TG were significantly higher in the serum of first NS patients (all P < 0.01), and the levels of age, ALP, TP, ALB, PA, Scr, TB and DB were significantly lower in the serum of first episode NS patients (all P < 0.05). There were no significant differences in ALT, GGT, GLU and BUN between the two groups (all P > 0.05). Compared to the healthy minors, the variables of age, CHE, ALT, GGT, Scr, UA, TC and TG were significantly higher in the serum of relapsing NS patients (all P < 0.05), and the levels of ALP, TP, ALB, PA, TB and DB were significantly lower in the serum of relapsing NS patients (all P < 0.05), and there were no significant differences in AST and GLU between the two groups (all P > 0.05).
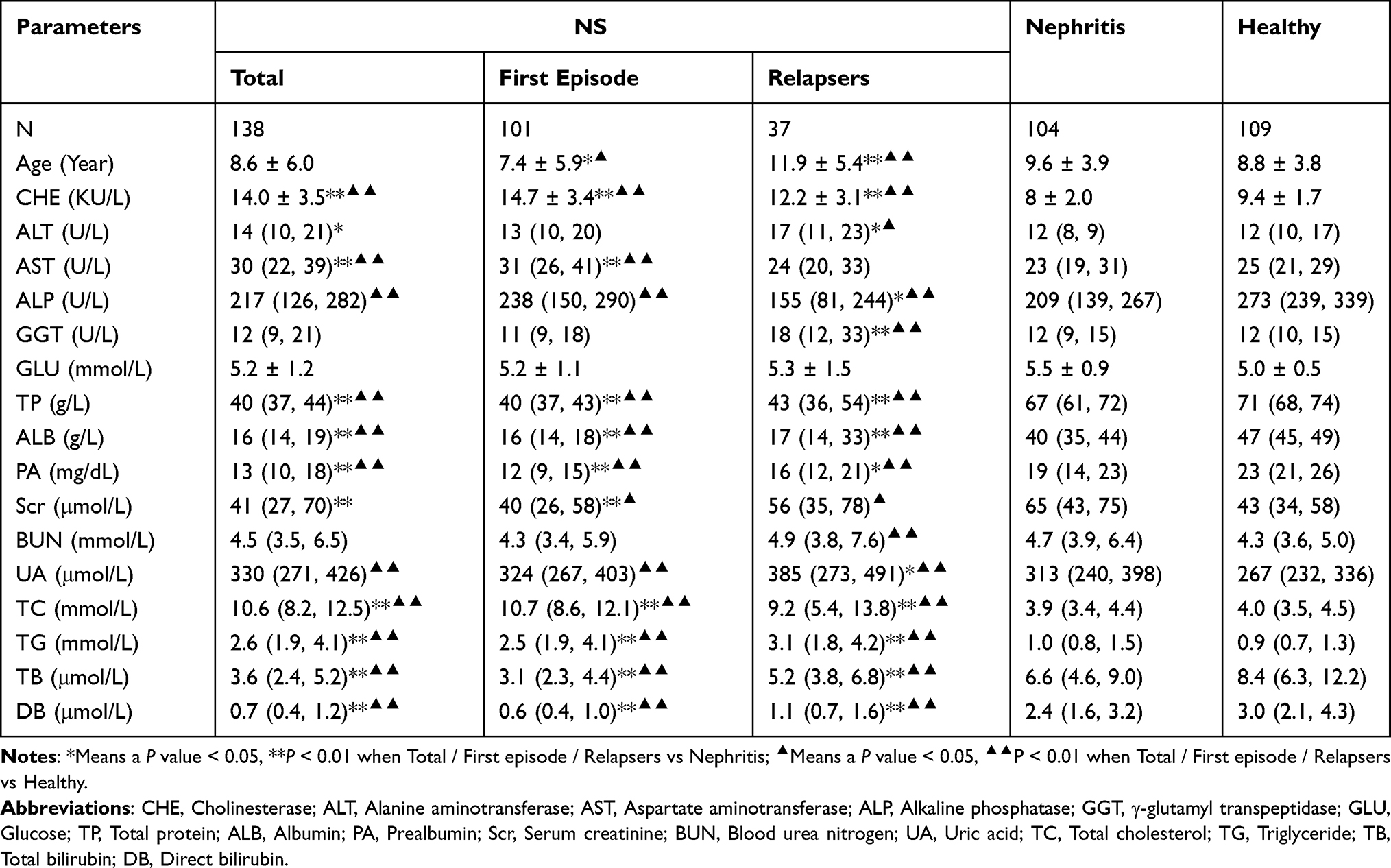 |
Table 1 Demographic Data and Laboratory Parameters of NS, Nephritis and Healthy Minors |
The Risk Factors for NS by Logistic Regression Analysis
Laboratory values were analyzed using logistic regression to determine risk factors for NS. According to Table 2, CHE, AST, TC, and TG are risk factors for NS, whereas TP, ALB, PA, TB, and DB are protective factors against total NS. The results indicate that CHE, AST, TC, and TG were risk factors for patients with their first episode of NS, whereas age, TP, ALB, PA, Scr, BUN, TB, and DB were protective variables. Age, CHE, GGT, TC, and TG were risk factors for recurrent NS, while TP, ALB, PA, TB, and DB acted as protective factors. As shown in Table 3, the CHE (adjusted odds ratio [OR] = 2.23, 95% confidence interval [CI]: 1.57–3.18) is shown to be the significant and independent risk predictor for total NS, while the TP (adjusted OR = 0.83, 95% CI: 0.77–0.89) and the DB (adjusted OR = 0.44, 95% CI: 0.22–0.88) were the significant and independent protective factors for total NS. The CHE (adjusted OR = 4.02, 95% CI: 1.47–11.08) was also the significant and independent risk predictors for the first episode NS, only the TP was a significant and independent protective factor of the first episode NS (adjusted OR = 0.75, 95% CI: 0.63–0.90). CHE (adjusted OR = 2.04, 95% CI: 1.42–2.93) was a substantial and independent risk predictor for relapsing NS, whereas TP (adjusted OR = 0.84, 95% CI: 0.78–0.91) and PA (adjusted OR = 0.86, 95% CI: 0.76–0.98) were both significant and independent protective variables for relapsing NS.
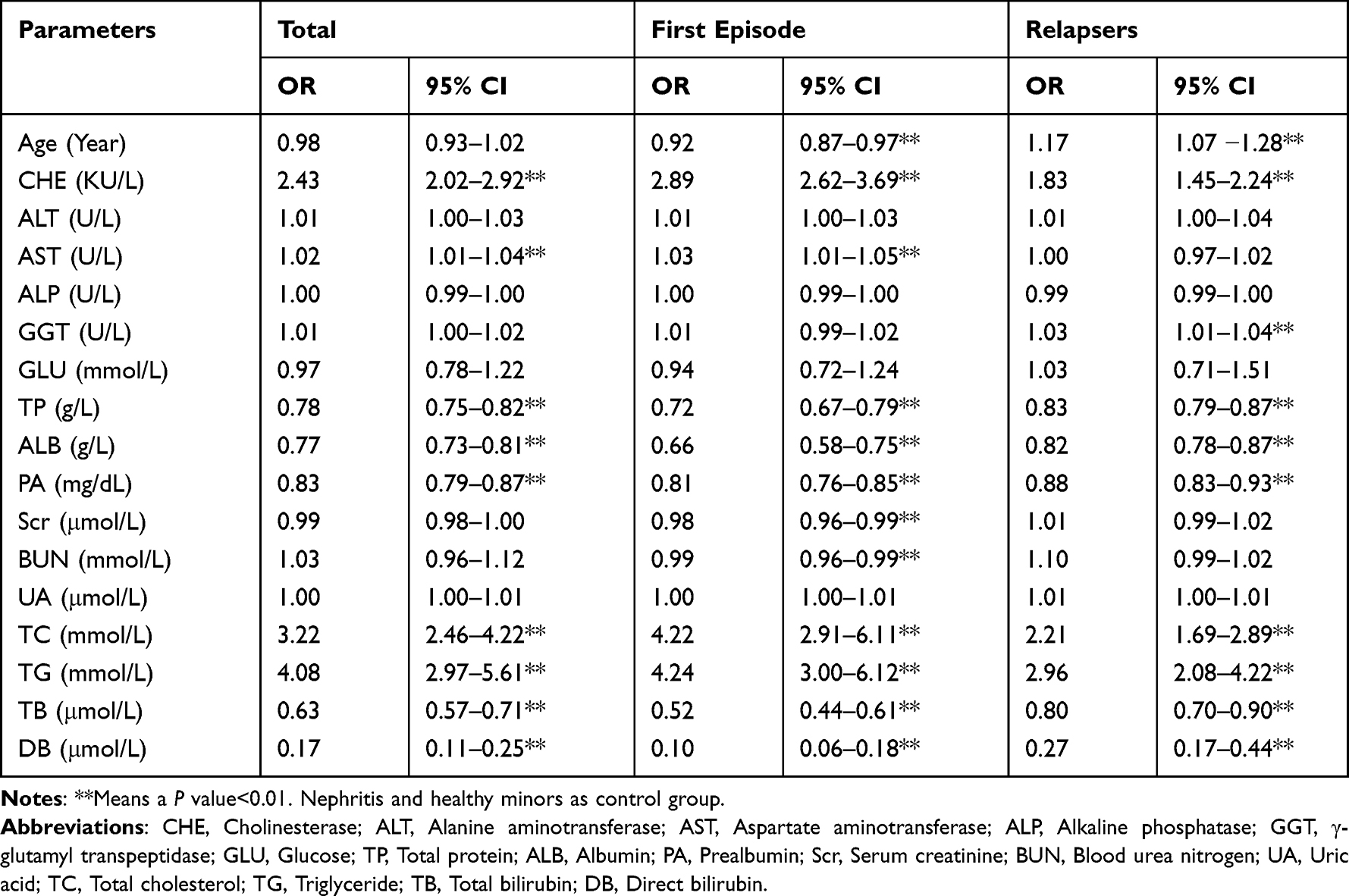 |
Table 2 Association of Laboratory Parameters with the Risk of NS (Univariable Logistic Regression Analysis) |
 |
Table 3 The Risk Factors for NS by Logistic Regression Analysis (Multivariate Logistic Regression Analysis) |
Correlations Between CHE Level and Laboratory Parameters in the Total/First Episode/Relapsing NS
As shown in Table 4, CHE level was positively correlated with TC (r = 0.429, P < 0.001), while negatively correlated with both ALB (r = −0.359, P < 0.001) and PA (r = −0.320, P < 0.001) in total NS patients. For first episode NS patients, CHE level was positively correlated with TC (r = 0.510, P < 0.001), while negatively correlated only with PA (r = −0.312, P = 0.002). Also, CHE level was positively correlated with TC (r = 0.385, P = 0.019), while negatively correlated only with ALB (r = −0.345, P = 0.037) in relapsing NS.
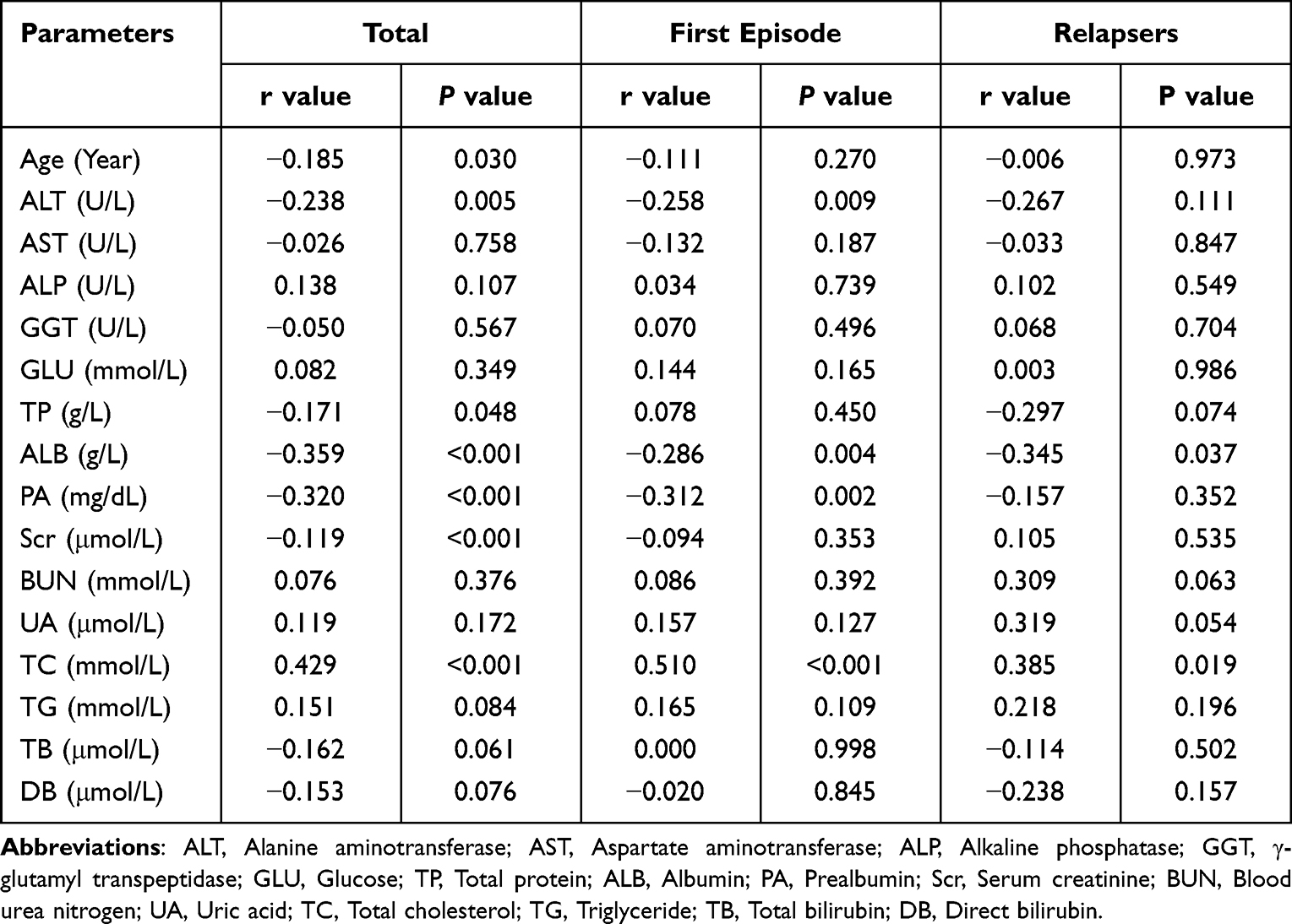 |
Table 4 Correlations Between CHE and Laboratory Parameters in Total/First Episode/Relapsing NS |
The Diagnostic Value of CHE for the Total/First Episode/Relapsing NS
As shown in Table 5, Figures 1–3, the optimal cutoff value of the CHE for diagnosis of the total/first episode/relapsing NS is 11 KU/L. As shown in the data, for total NS, the area under the curve (AUC) was 0.93 (95% CI: 0.91–0.96), the sensitivity was 87.0%, the specificity was 88.7%, the positive predictive value was 83.3%, the negative predictive value was 91.3%, and the Youden index was 75.7%. For the first episode NS, the AUC was 0.96 (95% CI: 0.94–0.98), the sensitivity was 94.1%, the specificity was 88.7%, the positive predictive value was 79.8%, the negative predictive value was 96.9%, and the youden index was 82.8%. And for relapsing NS, the AUC was 0.85 (95% CI: 0.78–0.92), the sensitivity was 67.6%, the specificity was 88.7%, the positive predictive value was 51.0%, the negative predictive value was 94.0%, and the youden index was 56.3%.
 |
Table 5 The Diagnostic Value of CHE for Total/First Episode/Relapsing NS |
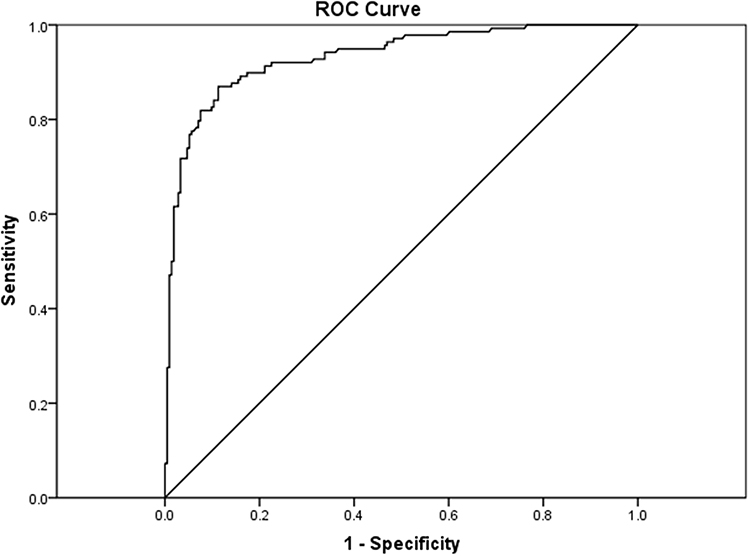 |
Figure 1 ROC curve demonstrating sensitivity and specificity of the CHE to detect total NS. |
 |
Figure 2 ROC curve demonstrating sensitivity and specificity of the CHE to detect the first episode of NS. |
 |
Figure 3 ROC curve demonstrating sensitivity and specificity of the CHE to detect relapsing NS. |
Discussion
NS is caused by various factors, including increased glomerular basement membrane permeability, presenting as a group of clinical syndromes of edema, proteinuria, hypoalbuminemia and hyperlipidemia. This study compared the laboratory experimental parameters between NS and nephritis/healthy minors. Our results showed that the protein content was significantly decreased and lipids were significantly increased in the serum samples, which were consistent with the characteristics of NS. The condition may be caused by the increased permeability of the glomerular capillary wall for proteins the loss of plasma protein in the urine,11 the decrease in the apolipoprotein content, and the increase in liver compensatory synthetic lipoprotein that leads to hyperlipidemia. According to research, hypercholesterolemia in NS patients is primarily associated with the up-regulation of 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase and hepatic cholesterol acyltransferase (ACAT) levels and down-regulations of the levels of low-density lipoprotein (LDL) and high-density lipoprotein (HDL) receptors.12
In addition, we found that the serum concentration of CHE in patients with NS was substantially higher than that of patients with nephritis and healthy minors. Similarly, Way et al observed that the CHE levels of NS patients were considerably greater than those of healthy minors.9 A recent adult observational study found that serum CHE is connected with the severity of proteinuria in individuals with NS, high serum CHE levels are associated with minimal change nephrotic syndrome (MCNS) severity.13 In our study, the multiple logistic regression analysis showed that CHE level was an independent risk factor for NS. Thus, CHE has the potential to function as a biomarker for NS in juvenile minors.
Studies have shown that CHE activity may be associated with lipid and lipoprotein metabolism.14 Abbott et al reported that CHE activity was significantly elevated in both type 1 and type 2 diabetic patients compared to the healthy control group and serum CHE activity was positively correlated with TG in patients suffering from type 1 and type 2 diabetes.15 In an analysis of risk factors for atherosclerosis, it revealed that CHE activity was associated with lipoprotein synthesis, and the CHE activity was positively correlated with TG, TC, low-density lipoprotein cholesterol (LDL-C), and Apolipoprotein B (ApoB).16 Our results showed that there is a positive correlation between CHE and TC in NS, especially in first episode NS patients. Further research is required to clarify the processes of cholinesterase and lipid metabolism in NS minors, as this finding verifies the link between CHE and lipid metabolism.
In this study, we found that the optimal cutoff for total/first episode/relapsing NS all was 11 KU/L, and the serum CHE level had high accuracy and discriminatory power for diagnosing NS. However, the diagnostic accuracy in the first episode NS (AUC = 0.96, 95% CI: 0.94–0.98) was better than for total NS (AUC = 0.93, 95% CI: 0.91–0.96) and relapsing NS (AUC = 0.85, 95% CI: 0.78–0.92). Hypoproteinemia and hypercholesterolemia are the blood abnormalities observed in adults and children with NS, protein and lipid levels in the blood have been added as diagnostic criteria for NS.17 In diagnosing NS, we compared the AUC of serum CHE, TP, ALB, TG, and TC (see Supplementary Table 1). In total NS, there was no difference between the AUCs of CHE and TC, and there was no difference between the AUC of CHE, TC, and TG in relapsing NS. This study indicates that CHE level may be a good diagnostic indicator for NS.
The CHE level was an independent risk factor for NS in minors. In addition, the serum CHE level was extremely accurate for the diagnosis of NS, particularly in the first episode of NS in minors.
Ethical Approval and Informed Consent
This research did not affect the patients’ health and privacy. The study obtained informed consent from the minor’s parents or legal guardians and was approved by the Zhejiang Province Ethical Committee of The Taizhou Hospital (#K20220845). All procedures performed in the studies involving human participants accorded with the 1964 Helsinki Declaration and its later amendments, or other comparable ethical standards.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Eddy AA, Symons JM. Nephrotic syndrome in childhood. Lancet. 2003;362(9384):629–639. doi:10.1016/S0140-6736(03)14184-0
2. Zhao J, Liu Z. Treatment of nephrotic syndrome: going beyond immunosuppressive therapy. Pediatr Nephrol. 2020;35:569–579. doi:10.1007/s00467-019-04225-7
3. Thalgahagoda S, Abeyagunawardena S, Jayaweera H, et al. Pulsed vincristine therapy in steroid-resistant nephrotic syndrome. Biomed Res Int. 2017;2017:1757940. doi:10.1155/2017/1757940
4. Bakkum L, Willemen AM, Zoetebier L, et al. A longitudinal study on the effects of psychological stress on proteinuria in childhood steroid-sensitive nephrotic syndrome. J Psychosom Res. 2019;121:8–13. doi:10.1016/j.jpsychores.2019.01.011
5. Mishra OP, Jain P, Srivastava P, et al. Urinary N-acetyl-beta-D glucosaminidase (NAG) level in idiopathic nephrotic syndrome. Pediatr Nephrol. 2012;27(4):589–596. doi:10.1007/s00467-011-2041-4
6. Kimura S, Soria F, D’Andrea D, et al. Prognostic value of serum cholinesterase in non-muscle-invasive bladder cancer. Clin Genitourin Cancer. 2018;16:e1123–e1132. doi:10.1016/j.clgc.2018.07.002
7. Albertí J, Martinet A, Sentellas S, et al. Identification of the human enzymes responsible for the enzymatic hydrolysis of aclidinium bromide. Drug Metab Dispos. 2010;38(7):1202–1210. doi:10.1124/dmd.109.031724
8. Lampón N, Hermida-Cadahia EF, Riveiro A, et al. Association between butyrylcholinesterase activity and low-grade systemic inflammation. Ann Hepatol. 2012;11(3):356–363. doi:10.1016/S1665-2681(19)30932-9
9. Way RC, Hutton CJ, Kutty KM. Relationship between serum cholinesterase and low density lipoproteins in children with nephrotic syndrome. Clin Biochem. 1975;8(1–6):103–107. doi:10.1016/s0009-9120(75)91072-3
10. Cattran DC, Feehally J, Cook HT, et al.; Kidney Disease: Improving Global Outcomes (KDIGO) Glomerulonephritis Work Group. KDIGO clinical practice guideline for glomerulonephritis. Kidney Int Suppl. 2012;2:139–274.
11. Tesar V, Zima T. Recent progress in the pathogenesis of nephrotic proteinuria. Crit Rev Clin Lab Sci. 2008;45:139–220. doi:10.1080/10408360801934865
12. Vaziri ND. Molecular mechanisms of lipid disorders in nephrotic syndrome. Kidney Int. 2003;63(5):1964–1976. doi:10.1046/j.1523-1755.2003.00941.x
13. Goto K, Kono K, Fujii H, et al. Clinical value of serum cholinesterase levels in nephrotic syndrome: an observational study. BMC Nephrol. 2022;23(1):128. doi:10.1186/s12882-022-02764-0
14. Chu MI, Fontaine P, Kutty KM, et al. Cholinesterase in serum and low density lipoprotein of hyperlipidemic patients. Clin Chim Acta. 1978;85(1):55–59. doi:10.1016/0009-8981(78)90100-6
15. Abbott CA, Mackness MI, Kumar S, et al. Relationship between serum butyrylcholinesterase activity, hypertriglyceridaemia and insulin sensitivity in diabetes mellitus. Clin Sci. 1993;85(1):77–81. doi:10.1042/cs0850077
16. Alcântara VM, Chautard-Freire-Maia EA, Scartezini M, et al. Butyrylcholinesterase activity and risk factors for coronary artery disease. Scand J Clin Lab Invest. 2002;62(5):399–404. doi:10.1080/00365510260296564
17. Hull RP, Goldsmith DJ. Nephrotic syndrome in adults. BMJ. 2008;336:1185–1189. doi:10.1136/bmj.39576.709711.80
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pro-Neurotensin as a Potential Novel Diagnostic Biomarker for Detection of Nonalcoholic Fatty Liver Disease
Mohamed AA, Abo-Elmatty DM, Ezzat O, Mesbah NM, Ali NS, Abd El Fatah AS, Alsayed E, Hamada M, Hassnine AA, Abd-Elsalam S, Abdelghani A, Hassan MB, Fattah SA
Diabetes, Metabolic Syndrome and Obesity 2022, 15:1935-1943
Published Date: 22 June 2022
CENPO is Associated with Immune Cell Infiltration and is a Potential Diagnostic and Prognostic Marker for Hepatocellular Carcinoma
He K, Xie M, Li J, He Y, Yin Y
International Journal of General Medicine 2022, 15:7493-7510
Published Date: 25 September 2022
Comprehensive Diagnostics of Diabetic Nephropathy by Transcriptome RNA Sequencing
Lei L, Bai Y, Fan Y, Li Y, Jiang H, Wang J
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3069-3080
Published Date: 10 October 2022
Characterization of the Microbiome and Host’s Metabolites of the Lower Respiratory Tract During Acute Community-Acquired Pneumonia Identifies Potential Novel Markers
Xiao Q, Tan S, Liu C, Liu B, Li Y, Guo Y, Hu P, Su Z, Chen S, Lei W, Li X, Su M, Rong F
Infection and Drug Resistance 2023, 16:581-594
Published Date: 26 January 2023
Can Oral Zinc Supplementation Reduce Relapses in Childhood Steroid-Sensitive Nephrotic Syndrome? A Systematic Review
Mbanefo NR, Uwaezuoke SN, Eneh CI, Odimegwu CL, Chikani UN, Muoneke UV, Nwolisa CE, Odo KE, Ogbuka FN, Akwue AT
International Journal of Nephrology and Renovascular Disease 2023, 16:143-153
Published Date: 20 April 2023