Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Characterization of Patients with COPD and GOLD E Classification in the United States
Authors Bhatt SP ![]() , Zhang Y, White J, Stanford RH
, Zhang Y, White J, Stanford RH ![]() , Mayen Herrera E, Cunoosamy D, Djandji M, Soliman M, Qureshi T, Subramaniam A
, Mayen Herrera E, Cunoosamy D, Djandji M, Soliman M, Qureshi T, Subramaniam A
Received 26 January 2026
Accepted for publication 11 March 2026
Published 19 March 2026 Volume 2026:21 598962
DOI https://doi.org/10.2147/COPD.S598962
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Vanesa Bellou
Surya P Bhatt,1 Yiran Zhang,2 John White,2 Richard H Stanford,3 Ernesto Mayen Herrera,4 Danen Cunoosamy,4 Michel Djandji,4 Mena Soliman,5 Tabarak Qureshi,4 Arun Subramaniam4
1Department of Pulmonary, Allergy, & Critical Care Medicine, University of Alabama at Birmingham, Birmingham, AL, USA; 2Optum, Inc., Eden Prairie, MN, USA; 3AESARA, Inc., Chapel Hill, NC, USA; 4Sanofi, Cambridge, MA, USA; 5Regeneron Pharmaceuticals, Inc., Tarrytown, NY, USA
Correspondence: Arun Subramaniam, Email [email protected]
Background: The 2023 Global Initiative for Chronic Obstructive Lung Disease (GOLD) update reclassified patients with chronic obstructive pulmonary disease (COPD) into group E based solely on exacerbation history, regardless of symptom burden. However, there are limited real-world descriptions of these patients at high risk of future exacerbation. This study therefore characterized patients in GOLD E, including subgroups based on blood eosinophil count (BEC), triple inhaler therapy use, and smoking status.
Methods: Retrospective analysis of administrative claims and electronic health records obtained from Optum’s Market Clarity Dataset between 2016 and 2021. Adults aged 40– 80 years with COPD and continuous enrollment were observed for three years. Year 1 (baseline) included the earliest evidence of COPD. GOLD E status was defined as ≥ 2 moderate or ≥ 1 severe exacerbation during baseline.
Results: Of 145,341 patients with COPD, 38,648 (26.6%) met GOLD E criteria. Patients in GOLD E had a higher prevalence of comorbidities (including cardiovascular-related conditions), elevated BEC (≥ 300 cells/μL), triple inhaler use, and former smoking status, compared with non-GOLD E. Approximately 58.2% of patients in GOLD E had evidence of a BEC test. Despite treatment recommendations, only 14.2% of patients in GOLD E with elevated BEC used triple inhalers. Notably, 34.8% of GOLD E had no evidence of any maintenance medication use. Of those with known smoking status (65.6%), current smokers had fewer severe exacerbations than never or former smokers. However, current smokers were 4.5– 5.5 years younger, had lower prevalences of obesity and cardiovascular comorbidities, and the highest use of rescue medications—factors that help explain this unexpected result.
Conclusion: Many patients in the United States with COPD in GOLD E were not treated according to recommendations, and BEC testing remains underutilized. Exacerbation rates were high, even among never or former smokers with COPD.
Plain Language Summary: Among all patients with COPD, those in Group E of the Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification system experience the most frequent exacerbations. Patients in GOLD E also face the highest risk of future exacerbations. These events are associated with increased mortality, patient burden, and health care costs. However, there remains a lack of research on the demographic, clinical, and treatment characteristics of this high-risk group. Accordingly, this retrospective study used 12 months of insurance claims data to help payers and clinicians better understand these patients and their unmet needs.
Results showed that 38,648 patients in GOLD E had a higher prevalence of comorbidities (eg, asthma, cardiovascular disease, hypertension), and elevated blood eosinophil count (BEC ≥ 300 cells/μL), compared to 106,693 patients with COPD but not in GOLD E. The proportion of current smokers was similar between GOLD E and non-GOLD E.
Importantly, many patients in GOLD E were not treated according to recommendations. For example, 34.8% of GOLD E had no evidence of any maintenance medication, and only 14.2% with BEC ≥ 300 cells/μL used the recommended triple inhaler therapy.
Because both moderate and severe exacerbations are associated with increased risk of disease progression, economic burden, and mortality, they should be addressed early—even among never or former smokers.
Keywords: COPD, disease burden, eosinophilic COPD, exacerbations, tobacco smoking, type 2 inflammation
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the world’s most common chronic respiratory diseases, affecting approximately 10.3% of adults worldwide.1 Prevalent in approximately 6.0% of adult Americans, COPD is the fifth leading cause of death in the US.2–5 Exacerbations of COPD—characterized by acute worsening of symptoms that require specific treatments—are central to adverse health outcomes and result in lung function decline.6–11 Over 40% of American adults with COPD experience an exacerbation in a given year,12 despite the documented benefits of inhaler therapy.13 Exacerbations have important consequences: patients with at least one exacerbation are at significantly greater risk of death compared with no exacerbation, while the risk of cardiovascular events increased fourfold after any exacerbation that required hospitalization.9,10 Importantly, exacerbation history predicts the risk of future exacerbations.9
Exacerbations of COPD also impose a substantial health care burden, accounting for as much as 70% of COPD-related costs.14 For example, Mayen Herrera et al reported that annual direct costs in the US rose from $1425 among patients with no exacerbations to $12,765 among patients with at least two exacerbations15 Exacerbation costs vary widely depending on the severity of the event: Bogart et al reported that the mean (SD) cost of a severe exacerbation (involving hospitalization or death) was $22,729 ($26,663; 2017 USD), while moderate exacerbations (treated with medication only) averaged $2107 ($4865).16 In addition, Nordon et al determined that patients with at least one severe exacerbation incurred an average of 460% higher COPD-related costs than those with moderate exacerbations only17 Although moderate exacerbations may be less burdensome, they are nevertheless associated with increased risk of future hospitalization and mortality, especially when treated with higher oral corticosteroid (CS) doses.18
Given the impact of exacerbations, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) updated its 2023 patient classification schema from ABCD to ABE.19 The update created a high-risk group (Group E) based exclusively on exacerbation history, where even frequent moderate exacerbations are predictive of both future exacerbations and mortality.18,20,21 Specifically, GOLD E includes patients with at least two moderate or one severe exacerbation in the preceding year.19 Up to 47.0% of patients with COPD are in GOLD E,22 and US patients who progressed from GOLD A/B to GOLD E incurred more than double the mean COPD-related annual health care costs (from $4350 to $9880).23 Although the rate of exacerbations has declined among participants in clinical trials with strict eligibility criteria,24 there is a dearth of real-world data on the characteristics of patients classified as GOLD E.
Among those in GOLD E, three additional factors may further distinguish patient treatment strategies and outcomes. First, elevated blood eosinophil count (BEC [≥ 300 cells/μL]) is associated with higher exacerbation risk.25 Characteristic of type 2 inflammation, elevated BEC shows better responsiveness to anti-inflammatory therapy, including inhaled corticosteroid (ICS) treatment and biologics.25–27 Second, triple inhaler use (combination of ICS, long-acting beta-2 agonists [LABA], and long-acting muscarinic antagonists [LAMA]) may be used differentially based on BEC.8 Finally, smoking status is a modifiable risk factor that is associated with exacerbation risk, disease progression, and COPD-related costs.28–31
The primary objective of this study was to comprehensively describe the demographic and clinical characteristics, medication use, BEC levels, smoking status, and disease burden among patients in the United States (US) who meet GOLD E criteria. Among those in GOLD E, we further aimed to describe subgroups based on BEC levels, triple inhaler use, and smoking status. Although prior analyses examined COPD populations using real-world data,32 our study extends this work by specifically characterizing patients in the recently defined GOLD E category. Exploring the heterogeneity of these patients and the intersection of exacerbation history, BEC testing patterns, and treatment utilization may support individualized clinical approaches to disease management.
Materials and Methods
Data Source and Study Time Periods
This retrospective study used Optum’s Market Clarity Dataset to identify patients with COPD between January 1, 2016, and December 31, 2021. The Market Clarity Dataset is a de-identified resource that deterministically links administrative claims with electronic health record (EHR) information. The dataset is compliant with the Health Insurance Portability and Accountability Act and includes patients who received medical and pharmacy benefits under commercial, Medicaid, Medicare/Medicare Advantage, and other programs.
Medical claims information includes diagnosis and procedure codes from the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM); Current Procedural Terminology (CPT) or Healthcare Common Procedure Coding System (HCPCS) codes; laboratory test codes; service site code; and other information. Pharmacy claims information includes drug name, National Drug Code (NDC), dosage, dosage form, and fill date. A patient’s EHR information includes both structured and unstructured fields like smoking status, laboratory test results, and provider notes.
Each patient was assessed during a period of three consecutive calendar years beginning on January 1st of a given year (eg, January 1, 2017) Baseline was the first year of the observation period (eg, 2017), while follow-up included years two and three (eg, 2018–2019) Among patients eligible for more than one three-year observation period, the baseline year was randomly selected to reduce the potential bias of assessing patients during a particular time period of disease or the COVID-19 pandemic. Study time periods are depicted in Supplemental file 1.
Study Population
The study population comprised adults with at least two medical claims with ICD-10-CM codes for COPD, in any position, at least 30 days apart during the three-year observation period. Claims for COPD were required to be non-diagnostic, which are claims that are not affiliated with corresponding testing or procedures that establish a diagnosis (eg, imaging or laboratory tests). Patients aged 40–80 years were included, as COPD is uncommon below age 40 and is frequently accompanied by frailty and severe comorbidities over age 80.33,34 Additional eligibility criteria included survival during baseline; at least three years of continuous enrollment with medical and pharmacy benefits (unless death occurred during follow-up, in which case only baseline continuous enrollment was required); evidence of clinical activity in the EHR during both baseline and follow-up (unless death occurred, in which case no clinical activity was required in the year of death); and at least two non-diagnostic medical claims of COPD during baseline and one during follow-up (unless death occurred, in which case no COPD claim was required in the year of death).
Patients were excluded if they died during the 12-month baseline period. Additional exclusion criteria were missing demographic information or at least one non-diagnostic claim with an ICD-10-CM diagnosis code for cystic fibrosis, alpha-1 antitrypsin deficiency, sarcoidosis, or eosinophilic granulomatosis with polyangiitis during the three-year observation period.
Variable Definitions and Outcome Measurements
Baseline demographic characteristics included baseline year; age; sex; race/ethnicity; insurance type; and geographic region. Baseline clinical characteristics included the Charlson Comorbidity Index (CCI) score35 and the presence of COPD-related comorbidities (defined by at least one non-diagnostic medical claim for anemia, asthma, bronchiectasis, coronary artery disease, diabetes mellitus [all types], gastroesophageal reflux disease, heart failure, hypertension, interstitial lung disease, lung cancer, metabolic syndrome [apart from diabetes], myocardial infarction, obesity [body mass index ≥ 30 kg/m2], osteoporosis, psychological disturbances [depression/anxiety], pulmonary hypertension, skeletal muscle dysfunction, and sleep disorders).
According to recommendations, a patient was classified as GOLD E if there was evidence of at least two moderate or one severe exacerbation during the baseline year.19 Patients not meeting the exacerbation criteria were classified as non-GOLD E. Similar to Nordon et al,36 a severe COPD exacerbation was defined by overnight hospitalization with an ICD-10-CM diagnosis code for COPD in the primary position.
A moderate COPD exacerbation was also defined similar to prior literature36 as
- an emergency room visit with an ICD-10-CM diagnosis code for COPD in the primary position, or
- an ambulatory visit with an ICD-10-CM diagnosis code for COPD in the primary position, plus any of
- a pharmacy claim for three to 14 days of supply of a systemic corticosteroid (SCS) and/or antibiotic within ± five days of the visit;
- a CPT/HCPCS code for SCS and/or antibiotic administered on the same claim as the visit; or
- a medical claim with CPT/HCPCS code for SCS and/or antibiotic administered, plus an ICD-10-CM diagnosis code of J44 (plus all codes under the parent code of J44) in any position within ± five days of the visit.
Baseline BEC was defined as the highest available value among all valid results contained in claims or EHR data during the observation year. Smoking status was ascertained from EHRs during baseline; the most recent entry was categorized as current/former/never.
Maintenance and rescue medication use during baseline was assessed at the class level using NDCs from pharmacy claims. Maintenance medications included ICS, LABA, combination ICS/LABA (fixed dose), LAMA, combination LAMA/LABA (fixed dose), combination ICS/LABA/LAMA (fixed dose), methylxanthines, methylxanthine combinations (guaifenesin/dyphylline, guaifenesin/theophylline), mast cell stabilizers, anti-immunoglobulin E agents, leukotriene-receptor antagonists, phosphodiesterase-4 enzyme inhibitors, dual interleukin-4/interleukin-13 receptor antagonists, and interleukin-5 inhibitors. Rescue medications included short-acting beta-agonists (SABA), short-acting antimuscarinic agents (SAMA), and SABA/SAMA fixed-dose combinations. Oral CS and antibiotic use were captured from pharmacy claims, while injected CS and antibiotic use were assessed using NDCs from pharmacy claims or any combination of NDC/CPT/HCPCS codes from medical claims.
Data Analysis
All analyses were descriptive in nature; formal hypotheses were neither proposed nor tested. Descriptive statistics of the baseline period included mean (SD) or median (IQR) for continuous variables and count (proportion) for categorical variables. All variables and outcomes were analyzed using SAS 9.4 (Cary, NC).
Ethics Approval
Institutional review board approval or waiver of approval was not required for this study because the study data were secondary and de-identified in accordance with the United States Department of Health and Human Services Privacy Rule’s requirements for de-identification codified at 45 C.F.R. § 164.514(b).
Results
In a total of 145,341 patients, 38,648 (26.6%) were classified as GOLD E (Figure 1). Table 1 includes the baseline demographic and clinical characteristics of the study population, stratified by GOLD E status.
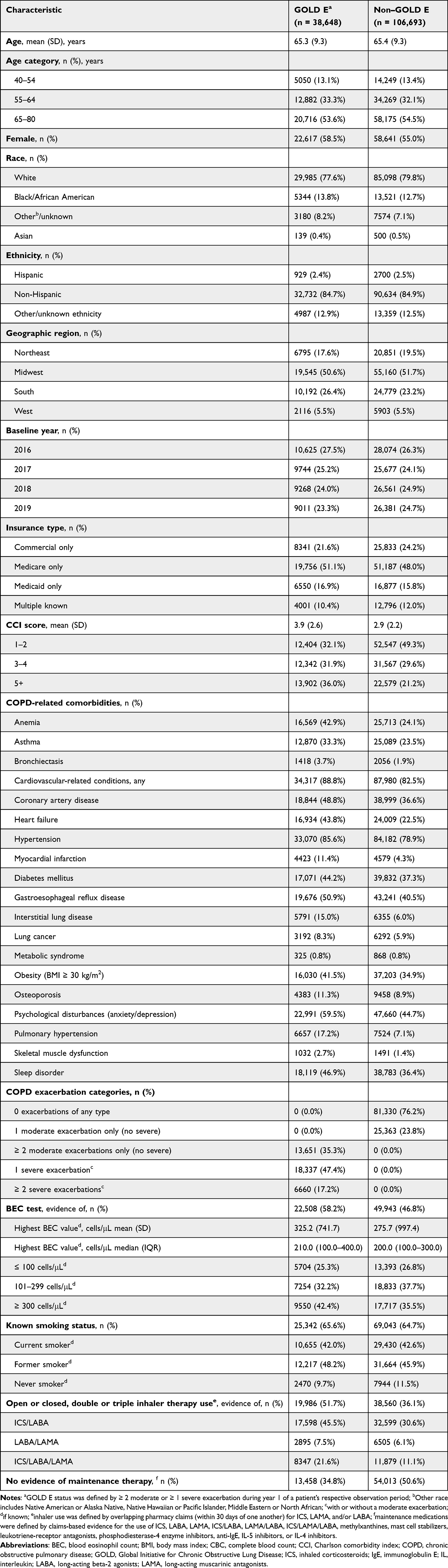 |
Table 1 Baseline Demographic and Clinical Characteristics, by GOLD E Status |
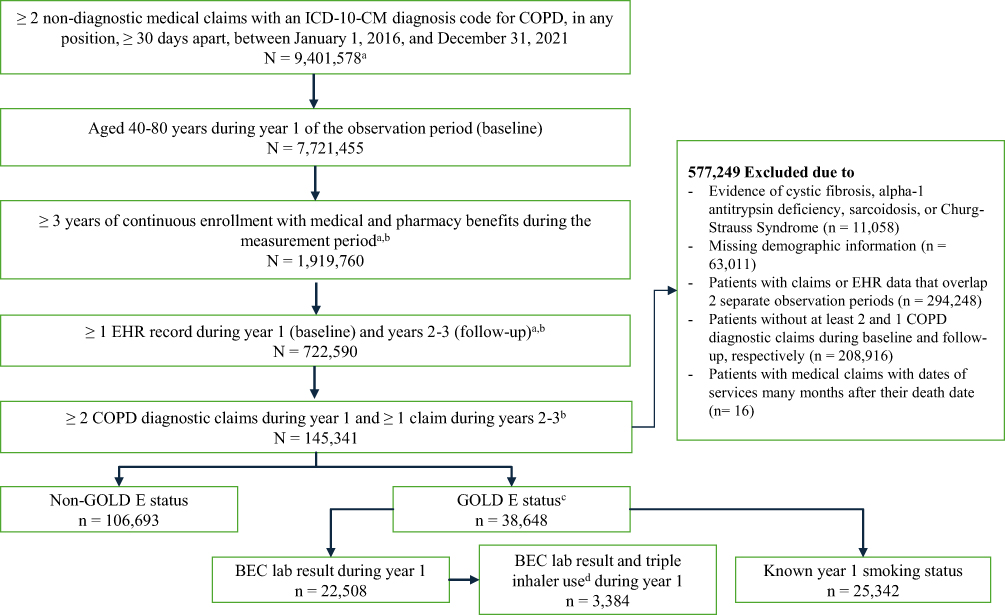 |
Figure 1 Patient identification and attrition. aNumber of observations; patients could be included in more than one three-year observation period; bPatients were retained if they died during years 2–3 of their respective measurement period; cGOLD E status was defined by ≥ 2 moderate or ≥ 1 severe exacerbation during year 1 of a patient’s respective measurement period; dtriple inhaler use was defined by overlapping pharmacy claims (within 30 days of one another) for inhaled corticosteroids, long-acting beta-2 agonists, and long-acting muscarinic antagonists. Abbreviations: BEC, blood eosinophil count; COPD, chronic obstructive pulmonary disease; EHR, electronic health record; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICD-10-CM, International Classification of Disease, Clinical Modification, 10th revision. |
The baseline exacerbation history of patients in GOLD E included 35.3% with two or more moderate exacerbations only (no severe), 47.4% with one severe exacerbation (with or without moderate), and 17.2% with two or more severe exacerbations (with or without moderate, Table 1). Meanwhile, 23.8% of patients in non–GOLD E had one moderate exacerbation during baseline.
A BEC lab test result was also more common among patients in GOLD E (58.2%) than non–GOLD E (46.8%). Where available, mean (SD) BEC value was higher among those in GOLD E (325.2 [741.7] vs 275.7 [997.4] cells/μL), as was median (IQR) BEC (210.0 [100.0–400.0] vs 200.0 [100.0–300.0] cells/μL) and the proportion of patients with elevated BEC (≥ 300 cells/μL): 42.4% vs 35.5%.
Baseline smoking status was known for 65.6% and 64.7% of patients in GOLD E and non–GOLD E, respectively (Table 1). Where known, the proportion of current smokers was approximately equal between groups (42.0% vs 42.6%), while the proportion of former smokers was higher among GOLD E (48.2% vs 45.9%). Any dual or triple inhaler use was more common among those in GOLD E (51.7% vs 36.1%), and this trend was observed for all inhaler types.
Mean CCI score was higher in GOLD E (3.9 [2.6] vs 2.9 [2.2]) in non–GOLD E; COPD-related comorbidities were more prevalent in GOLD E (Table 1). Cardiovascular-related conditions were the most common comorbidities and were more prevalent among patients in GOLD E, despite being of similar age as non–GOLD E. Specifically, the prevalence of heart failure was nearly double among patients in GOLD E (43.8% vs 22.5%), myocardial infarction was nearly triple (11.4% vs 4.3%), while hypertension (85.6% vs 78.9%) and coronary artery disease (48.8% vs 36.6%) were also more common. Obesity was more prevalent in GOLD E: 41.5% vs 34.9% than non–GOLD E. Additional comorbidities of interest were again more prevalent among GOLD E than non–GOLD E, including lung cancer (8.3% vs 5.9%), psychological disturbances (59.5% vs 44.7%), asthma (33.3% vs 23.5%), and diabetes of all types (44.2% vs 37.3%).
Patients in GOLD E with a BEC Lab Test Result During Baseline
Among the 22,508 patients in GOLD E with a BEC lab test result during baseline, 5704 (25.3%) had BEC ≤ 100 cells/μL, 7254 (32.2%) had BEC between 101–299 cells/μL, and 9550 (42.4%) had elevated BEC (≥ 300 cells/μL, Tables 1 and 2). Among patients with two or more severe exacerbations, a higher proportion had elevated BEC, compared with BEC ≤ 100 cells/μL (Table 2).
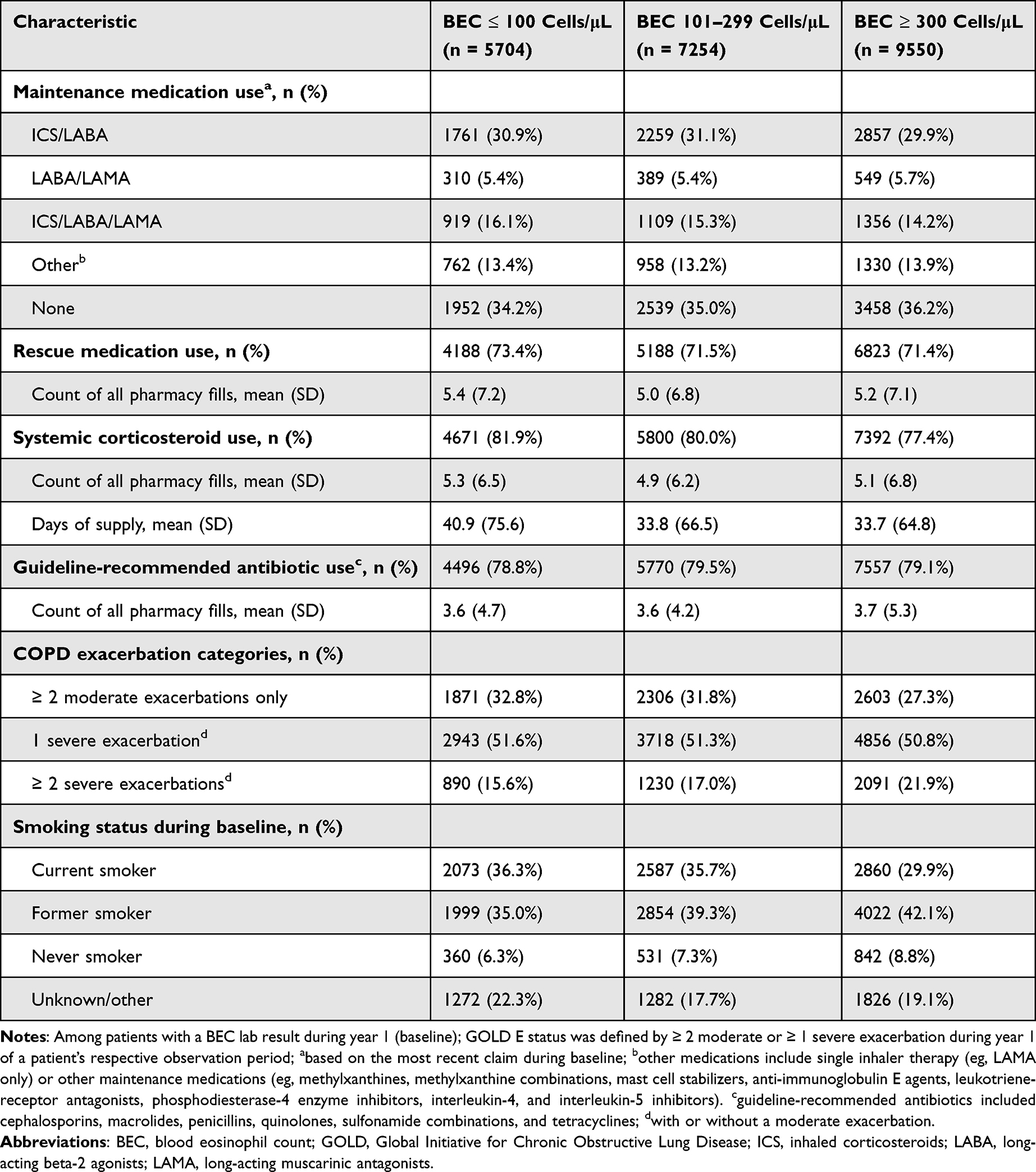 |
Table 2 Baseline Medication Use, Exacerbation History, and Smoking Status by BEC Among Patients in GOLD E with at Least One BEC Lab Test Result |
Table 2 also includes baseline utilization of COPD-related medications, exacerbation history, and smoking status, distinguished by BEC category. Patients with BEC ≤ 100 cells/μL were most likely to be prescribed SCS (81.9%) and had greater mean days of supply (40.9 [75.6]). These patients also had the highest prevalence of current smoking status (36.3%) and evidence of triple inhaler use (16.1%). Characteristics of this subcohort are further described in Supplemental file 2.
Patients in GOLD E with a BEC Lab Test Result and Evidence of Open or Closed Triple Inhaler Use During Baseline
A total of 3384 patients were included in this subcohort: 919 (27.2%) had BEC ≤ 100 cells/μL, 1109 (32.8%) had BEC between 101–299 cells/μL, and 1356 (40.1%) had BEC ≥ 300 cells/μL (Table 3). Compared with elevated BEC, those with BEC ≤ 100 cells/μL had a higher prevalence of only moderate exacerbations, while two or more severe exacerbations were less prevalent. Characteristics of this subcohort are further described in Supplemental file 3.
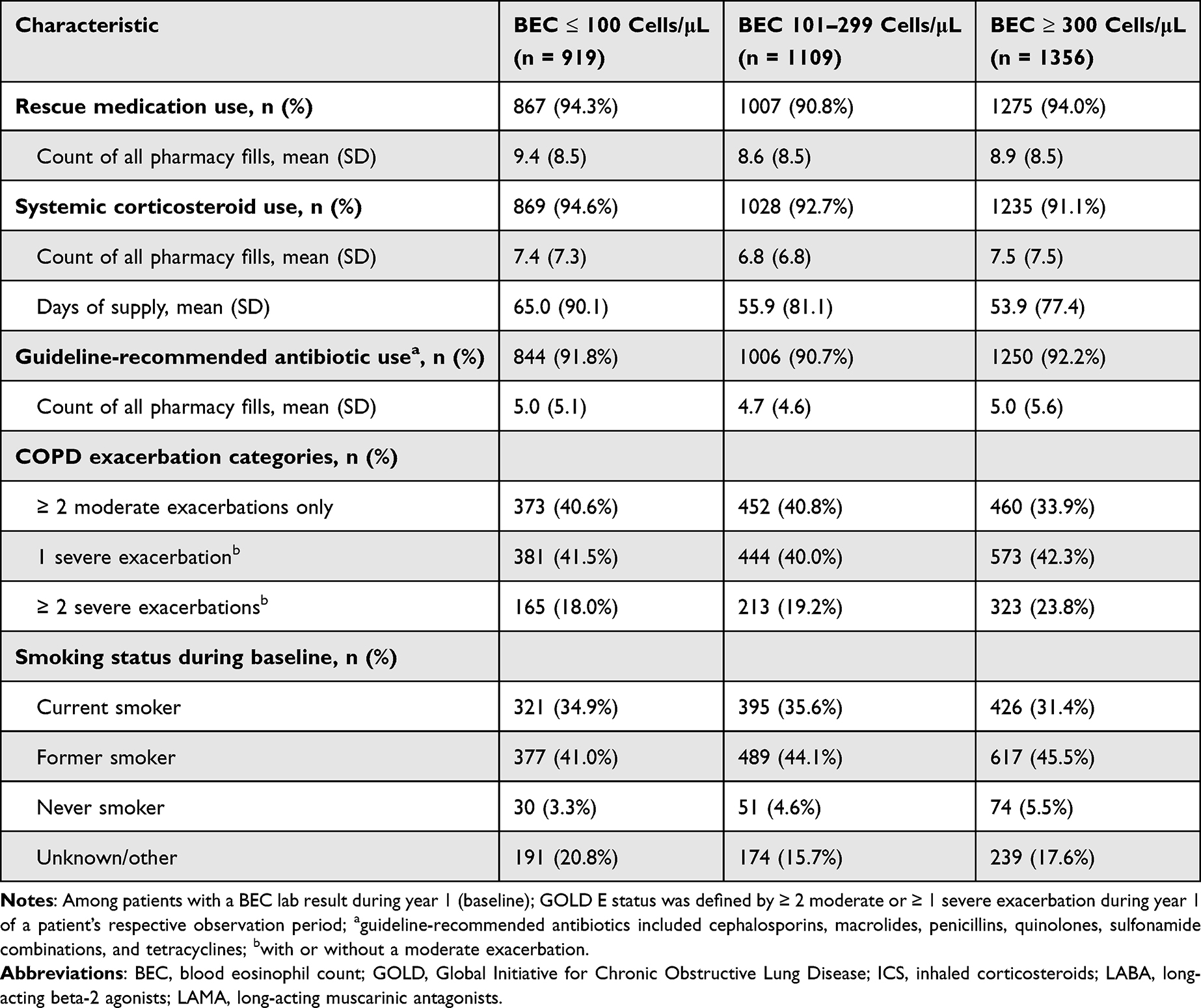 |
Table 3 Baseline Medication Use, Exacerbation History, and Smoking Status, by BEC Among Patients in GOLD E with at Least One BEC Lab Test Result and Evidence of Open or Closed Triple Inhaler Use |
Patients in GOLD E with Known Smoking Status During Baseline
Among the 25,342 patients with known smoking status, 10,655 (42.0%) were current smokers, 12,217 (48.2%) were former smokers, and 2470 (9.7%) never smoked (Table 4). Notably, current smokers were younger (62.2 years) than former or never smokers (67.7 and 66.7 years, respectively). Among current smokers, 40.1% had moderate exacerbations only, compared with former smokers (31.2%) and never smokers (29.6%). Rescue medication use, SCS use, and BEC ≤ 300 cells/μL were more common among current smokers. Although current smokers were less likely to have a severe exacerbation, they also had a lower prevalence of most comorbidities, including cardiovascular-related conditions, diabetes mellitus, pulmonary hypertension, anemia, and asthma (Supplemental file 4).
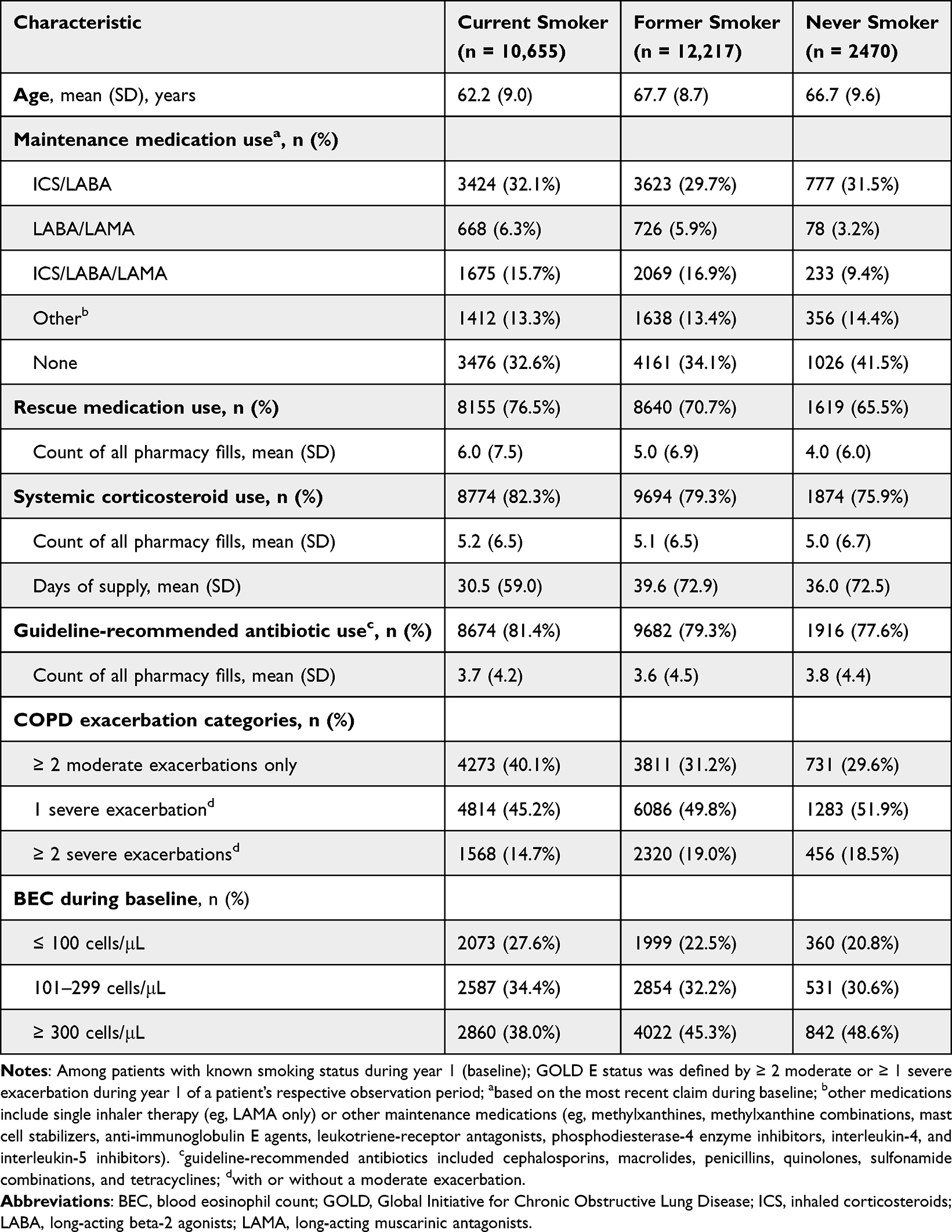 |
Table 4 Baseline Medication Use, Exacerbation History, and BEC Category Among Patients with COPD and GOLD E Classification, by Smoking Status |
Discussion
This retrospective analysis used administrative claims and EHR data to comprehensively characterize 38,648 patients with COPD in GOLD E (26.6% of the COPD study population). Within the GOLD E group’s baseline year, 34.8% of patients did not use any maintenance medication, while 58.2% had evidence of a BEC test result. Mean BEC and the proportion with elevated BEC were higher in GOLD E. These patients also had higher prevalences of COPD-related comorbidities, including obesity and cardiovascular conditions such as coronary artery disease, heart failure, and myocardial infarction. Given the limited real-world characterization of patients in GOLD E, our results may inform providers, payers, and researchers about the characteristics and treatment needs of this high-risk population.
The 2023 GOLD update simplified the prior ABCD classification schema by collapsing C and D into group E, reflecting the central role of exacerbations in disease management.19 Although this classification is relatively new, recent real-world evidence suggests that the majority of patients (58%) in GOLD A/B progress to GOLD E within five years.32 Patients with a history of one moderate exacerbation were nearly three times more likely (hazard ratio, 2.92) to progress to GOLD E, compared with those without a history of moderate exacerbation. Importantly, a majority of patients (53%) without any history of exacerbation still progressed to GOLD E within five years. As exacerbations are associated with increased mortality, cardiovascular risk, and economic burden,9,10,15,16,18,20 preventing these sentinel events should be a treatment goal for every patient, regardless of exacerbation history. Accordingly, current GOLD recommendations emphasize careful assessment of exacerbation risk and appropriate testing, including BEC, to guide treatment decisions.
To better describe the clinical and treatment heterogeneity within GOLD E, we assessed three subgroups defined by BEC, triple inhaler use, and smoking status. Patients with elevated BEC are of particular interest due to their high risk of future exacerbation and improved response to ICS and biologics.27,37,38 Elevated BEC was observed in 42.4% and 35.5% of GOLD E and non–GOLD E, respectively. Similar to the entire study population, 36.2% of GOLD E with elevated BEC did not use any maintenance medication. The 14.2% of patients with elevated BEC who used triple inhalers may be eligible for type 2 biologics, which show efficacy in both clinical trials and real-world analyses.39–41
The GOLD 2023 update also recommends using exacerbation history and biomarkers to inform treatment decisions.8,19 In practice, we found several examples of guideline-discordant care within the main and subgroup analyses. Despite GOLD’s recommendation for frequent eosinophil testing to guide treatment decisions,8 only 58.2% of patients in GOLD E had evidence of a test result during baseline (compared with 46.8% of non–GOLD E). In addition, 34.8% of patients in GOLD E had no evidence of any maintenance medication use. Instead of dual bronchodilators, triple inhaler therapy is recommended for patients in GOLD E with elevated BEC.19,42 However, only 14.2% used this treatment. These results suggest widespread underutilization of biomarker testing and treatment that may affect the risk of exacerbation. Identifying the root causes of such discordance warrants further investigation.
Because smoking has been associated with increased risk of exacerbation and COPD-related costs,28,29 we also assessed smoking status among patients in GOLD E. We found heterogeneous exacerbation history across all smoking types. However, these findings should not be interpreted as evidence that smoking lowers exacerbation risk. Instead, our results likely reflect underlying differences in age, comorbidity burden, and rescue medication use. For example, the current smokers in our cohort were younger, had lower prevalences of obesity and cardiovascular-related conditions, and used more rescue medications than never or former smokers. Former smokers were older and may have been encouraged to quit due to age-related comorbidities, symptom severity, and exacerbation history. In addition, the requirement of survival during the 12-month baseline period may have introduced survival bias by preferentially excluding never or former smokers with more advanced disease and/or comorbidity burden. Differences in underlying COPD phenotype (eg, emphysema-predominant disease) may also contribute to exacerbation variability across smoking categories; however, detailed phenotypic information was not available to evaluate this possibility. Collectively, these factors may help explain the observed heterogeneity and underscore the importance of early treatment regardless of smoking status.
Our study has several strengths. First, the combination of administrative claims and EHR data allowed us to present a breadth of patient characteristics, including demographics, comorbidities, medication use, BEC test results, and smoking status. These data may help inform providers, payers, and researchers about patients at the highest risk of exacerbation. Second, we were able to identify a large study population and create three subgroups among patients in GOLD E. These subgroups represented patients of considerable clinical interest and allowed us to explore guideline-discordant testing and treatment patterns.
Several limitations are common to retrospective analyses of EHRs and administrative claims. Primarily, we used real-world data that was not originally collected for the purpose of studying COPD or its treatment. For example, we cannot be certain if a BEC value was measured at a stable state or during an active period of acute exacerbation. Second, our data may not capture all patient care events, such as visits to free clinics or clinical trial participation. Third, we required continuous enrollment in medical and pharmacy benefit programs among those who did not die during baseline. Social determinants of health, especially financial strain that correlates with inconsistent insurance coverage, are associated with increased COPD prevalence and exacerbation.43 It is therefore unlikely that we reported an artificially high rate of treatments that differed from recommendations. Fourth, we identified patients at different places on the spectrum of disease progression. We could not establish a correlation between the proportion of patients with comorbidities and their years since COPD diagnosis. In addition, we did not assess lung function and excluded patients who died during baseline. Therefore, our results do not reflect a specific point in disease progression and may have excluded patients with the most severe conditions. Fifth, we restricted the study population to individuals aged 40–80 years. While this may limit the generalizability of our results, COPD at age < 40 is quite rare.33 Meanwhile, COPD in the population of patients with very advanced age (eg, > 80 years) is often accompanied by several unique comorbidities such as frailty, sarcopenia, and cognitive impairment.34 Finally, this was a descriptive study limited to the first year of a three-year observation period, selected to begin on January 1st of a given year. Although the study period spanned the COVID-19 pandemic, our analyses of baseline characteristics and treatment patterns were not time-dependent. Therefore, the COVID era is unlikely to bias results in one particular direction. This study did not include statistical control for known risk factors, such as age and obesity, which may confound the relationship between patient characteristics and exacerbation risk. Because causal inferences cannot be made here, future research may consider statistical adjustment to account for known risk factors.
Conclusions
Many patients with COPD in GOLD E were not treated according to recommendations. Despite recommendations, only 51.7% of these patients had any maintenance medication use, while 58.2% had a BEC test result. Also, only 14.2% of patients with elevated BEC received triple inhaler therapy, suggesting real-world underutilization of recommended treatments. These results indicate opportunities exist to improve recommendation-concordant testing and treatment in a population with substantial exacerbation history and risk of future exacerbations. Early identification and intervention—including treatments that address type 2 inflammation—is encouraged.
Abbreviations
BEC, Blood eosinophil count; COPD, Chronic obstructive pulmonary disease; CPT, Current Procedural Terminology (CPT); CS, Corticosteroids; EHR, electronic health record; GOLD E, Global Initiative for Chronic Obstructive Lung Disease Group E; HCPCS, Healthcare Common Procedure Coding System; ICS, inhaled corticosteroids; ICD-10-CM, International Classification of Diseases, 10th Revision, Clinical Modification; LABA, Long-acting beta-2 agonists; LAMA, Long-acting muscarinic antagonists; NDC, National Drug Code; SCS, systemic corticosteroid.
Data Sharing Statement
The data contained in our database contains proprietary elements owned by Optum and, therefore, cannot be broadly disclosed or made publicly available at this time. The disclosure of this data to third-party clients assumes certain data security and privacy protocols are in place and that the third-party client has executed our standard license agreement, which includes restrictive covenants governing the use of the data.
Ethics Approval, Informed Consent, and Consent for Publication
Not applicable. Institutional review board approval or waiver of approval was not required for this study because the study data were secondary and de-identified in accordance with the United States Department of Health and Human Services Privacy Rule’s requirements for de-identification codified at 45 C.F.R. § 164.514(b). No patient interactions occurred during this study.
Acknowledgments
The authors would like to thank Soniya Biswas (Sanofi) for submission support; Max Prokopy (Optum, Inc.) for medical writing, editorial, and data visualization; and Kate Quicksell (Optum, Inc.) for project management support. These services were funded by Sanofi. Notation of prior abstract publication/presentation: ATS, San Diego, CA, USA, May 17-22, 2024. CHEST, Boston, MA, USA, Oct 6-9, 2024. ERS, Vienna, Austria, Sep. 7-11, 2024. ATS, San Francisco, CA, USA, May 16-21, 2025.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Financial support for this work and all supporting resources was provided by Sanofi.
Disclosure
Surya P. Bhatt reports fees for consulting or advisory boards from Apreo, AstraZeneca, Boehringer Ingelheim, Chiesi, Connect Biopharma, Genentech, GSK, Kymera, Merck, Polarean, Regeneron Pharmaceuticals Inc., Sanofi, Uniquity, Verona Pharma; honoraria for CME from Horizon CME, Illuminate Health, Integritas Communications, Integrity CE, Medscape; his institute has received funds for research from Genentech, COPD Foundation, Nuvaira, and Sanofi. Yiran Zhang is an employee of Optum/UnitedHealth Group, which was contracted to conduct this research. John White is an employee and shareholder of Optum/UnitedHealth Group, which was contracted to conduct this research. Richard H. Stanford is an employee and shareholder of AESARA, Inc. and consultant to Sanofi, Pfizer, Chiesi, Boehringer-Ingelheim. Ernesto Mayen Herrera is an employee and shareholder of Sanofi. Danen Cunoosamy is an employee and shareholder of Sanofi. Mena Soliman is an employee and shareholder of Regeneron Pharmaceuticals, Inc. Michel Djandji is an employee and shareholder of Sanofi. Tabarak Qureshi is an employee and shareholder of Sanofi. Arun Subramaniam is an employee and shareholder of Sanofi. The authors report no other conflicts of interest in this work.
References
1. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–15. doi:10.1016/s2213-2600(21)00511-7
2. Soriano JB, Kendrick PJ, Paulson KR. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/s2213-2600(20)30105-3
3. Bleecker ER, Al-Ahmad M, Bjermer L, et al. Systemic corticosteroids in asthma: a call to action from world allergy organization and respiratory effectiveness group. World Allergy Organ J. 2022;15(12):100726. doi:10.1016/j.waojou.2022.100726
4. Liu Y, Carlson SA, Watson KB, Xu F, Greenlund KJ. Trends in the prevalence of chronic obstructive pulmonary disease among adults aged≥ 18 years—United States, 2011–2021. MMWR Morb Mortal Wkly Rep. 2023;72(46):1250–1256. doi:10.15585/mmwr.mm7246a1
5. Ahmad FB, Cisewski JA, Anderson RN. Leading causes of death in the US, 2019-2023. JAMA. 2024;332(12):957–958. doi:10.1001/jama.2024.15563
6. Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957–963. doi:10.1136/thoraxjnl-2011-201518
7. Gutiérrez Villegas C, Paz-Zulueta M, Herrero-Montes M, Parás-Bravo P, Madrazo Pérez M. Cost analysis of chronic obstructive pulmonary disease (COPD): a systematic review. Health Econ Rev. 2021;11(1):1–12. doi:10.1186/s13561-021-00329-9
8. Venkatesan P. GOLD COPD report: 2025 update. Lancet Respir Med. 2025;13(1):e7–e8. doi:10.1016/s2213-2600(24)00413-2
9. Rothnie KJ, Müllerová H, Smeeth L, Quint JK. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464–471. doi:10.1164/rccm.201710-2029OC
10. Kunisaki KM, Dransfield MT, Anderson JA, et al. Exacerbations of chronic obstructive pulmonary disease and cardiac events. a post hoc cohort analysis from the SUMMIT randomized clinical trial. Am J Respir Crit Care Med. 2018;198(1):51–57. doi:10.1164/rccm.201711-2239OC
11. Kerkhof M, Voorham J, Dorinsky P, et al. Association between COPD exacerbations and lung function decline during maintenance therapy. Thorax. 2020;75(9):744–753. doi:10.1136/thoraxjnl-2019-214457
12. Wallace AE, Kaila S, Bayer V, et al. Health care resource utilization and exacerbation rates in patients with COPD stratified by disease severity in a commercially insured population. J Manag Care Spec Pharm. 2019;25(2):205–217. doi:10.18553/jmcp.2019.25.2.205
13. Adrish M, Hanania NA. POINT: should triple inhaled therapy be considered in all patients with group E COPD? Yes. Chest. 2024;166(1):12–17. doi:10.1016/j.chest.2024.03.029
14. Agarwal D. COPD generates substantial cost for health systems. Lancet Glob Health. 2023;11(8):e1138–e1139. doi:10.1016/s2214-109x(23)00304-2
15. Herrera EM, Stanford R, Njue A, et al. SA61 economic burden of patients in the United States with moderate-to-severe chronic obstructive pulmonary disease: a focused literature review. Value Health. 2023;26(12):S553. doi:10.1016/j.jval.2023.09.2970
16. Bogart MR, Hopson SD, Shih HC, Stanford RH, Coutinho AD. COPD exacerbation costs in the IMPACT study: a within-trial analysis. Am J Manag Care. 2020;26(5):e150–e154. doi:10.37765/ajmc.2020.43157
17. Nordon C, Carstens D, Fageras M, et al. RWD14 healthcare resource utilization and associated costs in COPD patients at high risk of exacerbation despite treatment with dual or triple inhaled therapy: results from the sirius observational study in the US. Value Health. 2024;27(6):S359. doi:10.1016/j.jval.2024.03.1668
18. Sivapalan P, Ingebrigtsen TS, Rasmussen DB, et al. COPD exacerbations: the impact of long versus short courses of oral corticosteroids on mortality and pneumonia: nationwide data on 67 000 patients with COPD followed for 12 months. BMJ Open Respir Res. 2019;6(1):e000407. doi:10.1136/bmjresp-2019-000407
19. Agustí A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Am J Respir Crit Care Med. 2023;207(7):819–837. doi:10.1164/rccm.202301-0106PP
20. Whittaker H, Rubino A, Müllerová H, et al. Frequency and severity of exacerbations of COPD associated with future risk of exacerbations and mortality: a UK routine health care data study. Int J Chron Obstruct Pulmon Dis. 2022;17:427–437. doi:10.2147/copd.S346591
21. Scioscia G, Blanco I, Arismendi E, et al. Different dyspnoea perception in COPD patients with frequent and infrequent exacerbations. Thorax. 2017;72(2):117–121. doi:10.1136/thoraxjnl-2016-208332
22. Radovanovic D, Contoli M, Marco FD, et al. Clinical and functional characteristics of COPD patients across GOLD classifications: results of a multicenter observational study. Copd. 2019;16(3–4):215–226. doi:10.1080/15412555.2019.1659760
23. Sethi S, Siddharthan T, Tejwani V, Lamprey C, Dixon A, Wan E. Progression to GOLD E in patients with COPD results in substantial health care resource utilization and costs. Chest. 2024;166(4):A4855–A4856. doi:10.1016/j.chest.2024.06.2877
24. Andreas S, Röver C, Heinz J, Straube S, Watz H, Friede T. Decline of COPD exacerbations in clinical trials over two decades - a systematic review and meta-regression. Respir Res. 2019;20(1):186. doi:10.1186/s12931-019-1163-2
25. Juthong S, Kaenmuang P. Association between blood eosinophils with exacerbation and patient-reported outcomes in chronic obstructive pulmonary disease patients in an endemic area for parasitic infections: a prospective study. J Thorac Dis. 2020;12(9):4868–4876. doi:10.21037/jtd-19-4101
26. Mathioudakis AG, Bate S, Sivapalan P, Jensen J-US, Singh D, Vestbo J. Rethinking blood eosinophils for assessing inhaled corticosteroids response in COPD: a post hoc analysis from the FLAME trial. Chest. 2024;166(5):987–997. doi:10.1016/j.chest.2024.06.3790
27. Singh D, Higham A, Mathioudakis AG, Beech A. Chronic obstructive pulmonary disease (COPD): developments in pharmacological treatments. Drugs. 2025;85(7):911–930. doi:10.1007/s40265-025-02188-8
28. Atsou K, Chouaid C, Hejblum G. Simulation-based estimates of effectiveness and cost-effectiveness of smoking cessation in patients with chronic obstructive pulmonary disease. PLoS One. 2011;6(9):e24870. doi:10.1371/journal.pone.0024870
29. Au DH, Bryson CL, Chien JW, et al. The effects of smoking cessation on the risk of chronic obstructive pulmonary disease exacerbations. J Gen Intern Med. 2009;24(4):457–463. doi:10.1007/s11606-009-0907-y
30. Nielsen AO, Lange P, Hilberg O, Farver-Vestergaard I, Ibsen R, Løkke A. COPD and smoking status–it does matter: characteristics and prognosis of COPD according to smoking status. Chronic Obstr Pulm Dis. 2023;11(1):56. doi:10.15326/jcopdf.2023.0433
31. Larsen DL. The quality of care and economic burden of COPD in the United States: considerations for managing patients and improving outcomes. 2022.
32. Siddharthan T, Sethi S, Wan E, et al. Progression from GOLD A/B to GOLD E: a claims analysis of patients with COPD newly initiating inhaled therapy. BMC Pulm Med. 2025;25(1):412. doi:10.1186/s12890-025-03898-1
33. Wang Z, Li Y, Lin J, et al. Prevalence, risk factors, and mortality of COPD in young people in the USA: results from a population-based retrospective cohort. BMJ Open Respir Res. 2023;10(1):e001550. doi:10.1136/bmjresp-2022-001550
34. Incalzi RA, Scarlata S, Pennazza G, Santonico M, Pedone C. Chronic obstructive pulmonary disease in the elderly. Eur J Intern Med. 2014;25(4):320–328. doi:10.1016/j.ejim.2013.10.001
35. Quan H, Li B, Couris CM, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(6):676–682. doi:10.1093/aje/kwq433
36. Nordon C, Carstens D, Fagerås M, et al. Characteristics and outcomes of people with COPD who experience exacerbations while on inhaled triple therapy: results of the SIRIUS I cohort study in the US (2015-2019). Int J Chron Obstruct Pulmon Dis. 2025;20:1851–1864. doi:10.2147/copd.S513573
37. Singh D, Agusti A, Martinez FJ, et al. Blood eosinophils and chronic obstructive pulmonary disease: a global initiative for chronic obstructive lung disease science committee 2022 Review. Am J Respir Crit Care Med. 2022;206(1):17–24. doi:10.1164/rccm.202201-0209PP
38. Singh D, Bafadhel M, Brightling CE, et al. Blood eosinophil counts in clinical trials for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2020;202(5):660–671. doi:10.1164/rccm.201912-2384PP
39. Bhatt SP, Rabe KF, Hanania NA, et al. Dupilumab for COPD with blood eosinophil evidence of type 2 inflammation. N Engl J Med. 2024;390(24):2274–2283. doi:10.1056/NEJMoa2401304
40. Bhatt SP, Rabe KF, Hanania NA, et al. Dupilumab for COPD with type 2 inflammation indicated by eosinophil counts. N Engl J Med. 2023;389(3):205–214. doi:10.1056/NEJMoa2303951
41. Shi X, Tan C, Chen X, et al. Efficacy of dupilumab in the treatment of COPD with type 2 inflammation: a real-world study. Allergy Med. 2024;2:100015. doi:10.1016/j.allmed.2024.100015
42. Suissa S. Single-inhaler triple versus dual bronchodilator therapy for GOLD group E and other exacerbating patients with COPD: real-world comparative effectiveness and safety. Eur Respir J. 2023;62(3):2300883. doi:10.1183/13993003.00883-2023
43. Stellefson M, Wang MQ, Yao Y, Campbell O, Sivalingam R. Exploring the link between social and economic instability and COPD: a cross-sectional analysis of the 2022 BRFSS. Int J Environ Res Public Health. 2025;22(8):1207. doi:10.3390/ijerph22081207
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
FIDEPOC: Consensus on Inspiratory Flow and Lung Deposition as Key Decision Factors in COPD Inhaled Therapy
González-Torralba F, Baloira A, Abad A, Fuster A, García-Rivero JL, García-Sidro P, Márquez-Martín E, Palop M, Soler N, Velasco JL
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1005-1015
Published Date: 4 May 2022
Patients with Chronic Obstructive Pulmonary Disease and Evidence of Eosinophilic Inflammation Experience Exacerbations Despite Receiving Maximal Inhaled Maintenance Therapy
Chen S, Miravitlles M, Rhee CK, Pavord ID, Jones R, Carter V, Emmanuel B, Alacqua M, Price DB
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2187-2200
Published Date: 9 September 2022
Use of Remote Cardiorespiratory Monitoring is Associated with a Reduction in Hospitalizations for Subjects with COPD
Polsky M, Moraveji N, Hendricks A, Teresi RK, Murray R, Maselli DJ
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:219-229
Published Date: 3 March 2023
Burden of Disease in Patients with Mild or Mild-to-Moderate Chronic Obstructive Pulmonary Disease (Global Initiative for Chronic Obstructive Lung Disease Group A or B): A Systematic Literature Review
Czira A, Purushotham S, Iheanacho I, Rothnie KJ, Compton C, Ismaila AS
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:719-731
Published Date: 29 April 2023
Exacerbations and Real-World Outcomes After Single-Inhaler Triple Therapy of Budesonide/Glycopyrrolate/Formoterol Fumarate, Among Patients with COPD: Results from the EROS (US) Study
Strange C, Tkacz J, Schinkel J, Lewing B, Agatep B, Swisher S, Patel S, Edwards D, Touchette DR, Portillo E, Feigler N, Pollack M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2245-2256
Published Date: 12 October 2023