")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Burden of Disease in Patients with Mild or Mild-to-Moderate Chronic Obstructive Pulmonary Disease (Global Initiative for Chronic Obstructive Lung Disease Group A or B): A Systematic Literature Review
Authors Czira A , Purushotham S, Iheanacho I, Rothnie KJ , Compton C , Ismaila AS
Received 27 October 2022
Accepted for publication 6 April 2023
Published 29 April 2023 Volume 2023:18 Pages 719—731
DOI https://doi.org/10.2147/COPD.S394325
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Russell
Alexandrosz Czira,1 Sneha Purushotham,2 Ike Iheanacho,2 Kieran J Rothnie,1 Chris Compton,3 Afisi S Ismaila4,5
1Value Evidence and Outcomes, R&D Global Medical, GSK, Brentford, UK; 2Evidera, London, UK; 3Global Medical, GSK, London, UK; 4Value Evidence and Outcomes, GSK, Collegeville, PA, USA; 5Department of Health Research Methods, Evidence, and Impact, McMaster University, Hamilton, ON, Canada
Correspondence: Alexandrosz Czira, Value Evidence and Outcomes, R&D Global Medical, GSK, 980 Great West Road, Brentford, Middlesex, TW8 9GS, UK, Tel +44 7788 351610, Email [email protected]
Background: Patients with mild or mild-to-moderate chronic obstructive pulmonary disease (COPD), defined as Global Initiative for Chronic Obstructive Lung Disease (GOLD) group A/B, are regarded as having a lower risk of experiencing multiple or severe exacerbations compared with patients classified as GOLD group C/D. Current guidelines suggest that patients in GOLD A/B should commence treatment with a bronchodilator; however, some patients within this population who have a higher disease burden may benefit from earlier introduction of dual bronchodilator or inhaled corticosteroid-containing therapies. This study aimed to provide research-based insights into the burden of disease experienced by patients classified as GOLD A/B, and to identify characteristics associated with poorer outcomes.
Methods: A systematic literature review (SLR) was conducted to identify evidence (burden of disease and prevalence data) relating to the population of interest (patients with COPD classified as GOLD A/B).
Results: A total of 79 full-text publications and four conference abstracts were included. In general, the rates of moderate and severe exacerbations were higher among patients in GOLD group B than among those in group A. Among patients classified as GOLD A/B, the risk of exacerbation was higher in those with more symptoms (modified Medical Research Council or COPD Assessment Test scales) and more severe airflow limitation (forced expiratory volume in 1 second % predicted).
Conclusion: Data from this SLR provide clear evidence of a heavier burden of disease for patients in GOLD B, compared with those in GOLD A, and highlight factors associated with worse outcomes for patients in GOLD A/B.
Keywords: COPD Assessment Test, COPD, disease burden, GOLD A/B, modified Medical Research Council, systematic review
Introduction
Chronic obstructive pulmonary disease (COPD) is a common and progressive respiratory disorder that represents a major cause of global morbidity and mortality.1,2 In 2019, the prevalence of COPD was 174 million and the disease accounted for 3.23 million deaths worldwide, of which more than 80% occurred in low- and middle-income countries.1,2 COPD has been projected to be one of the four leading causes of death by 2030,3 with a substantial associated economic burden.4
Within the disease spectrum, patients classified as having mild or mild-to-moderate COPD (defined as Global Initiative for Chronic Obstructive Lung Disease [GOLD] group A or B) are regarded as having a comparatively lower risk of experiencing multiple or severe exacerbations, a key cause of morbidity and mortality. The GOLD “ABCD” categorization for COPD was introduced in 2011 and initially used a combination of symptom severity, history of exacerbations, and/or spirometry grading to classify individual patients into one of the four groups for the purpose of selecting an initial maintenance therapy.5 A refinement in 2013 recommended that comorbidities should be considered in addition to the “ABCD” classification as part of a combined COPD assessment.6 In 2017, the “ABCD” classification was updated to categorize patients into one of the four groups based on exacerbation history and symptoms alone, without the use of spirometry.7 Although spirometry was noted as being important at a population level, at an individual patient level, it was considered less valuable in making individualized treatment decisions.7 Patients with a modified Medical Research Council (mMRC) score 0–1 or a COPD Assessment Test (CAT) score <10 and a history of zero or one moderate, and no severe, exacerbations in the previous year, would be classified as GOLD group A. Patients with mMRC ≥2 or CAT ≥10, and a history of zero or one moderate, and no severe, exacerbations in the previous year would be classified as GOLD group B. Using this categorization, the GOLD treatment strategy indicates that patients classified as GOLD group A should commence short- or long-acting bronchodilator therapy. The strategy recommends that patients classified as GOLD group B should commence long-acting bronchodilator therapy, but if they present with severe breathlessness, two long-acting bronchodilators may be offered.7 A further update was made to this classification tool in the GOLD 2023 strategy document; however, while this was published after the current study, there were no changes to the criteria for classification of GOLD group A and GOLD group B used in this research.8
Given the removal of spirometry assessment for classification of GOLD group, it is possible that a significant proportion of patients at higher risk of poorer outcomes who would previously have been labeled as GOLD group C/D (due to severe airflow obstruction) are now classified as GOLD group A/B (due to less frequent exacerbations). Therefore, GOLD group A/B may contain a subgroup of patients with a higher disease burden than would be expected, and such patients may benefit from earlier optimization of treatment, potentially with earlier initiation of dual or triple therapy, particularly since poorer lung function is a strong predictor of severe exacerbation and death.9
This study aimed to provide a comprehensive assessment of research-based insights from published evidence on the baseline characteristics of, and burden of disease experienced by, patients categorized as GOLD group A and GOLD group B. The analyses also investigated whether or how the burden of disease in GOLD A and GOLD B groups changed with clinical characteristics that may indicate greater disease severity or poorer prognosis, in order to inform the treatable-traits approach.
Methods
This systematic literature review (SLR; GSK study number 214854) was conducted according to the principles outlined in the Cochrane Handbook for Systematic Reviews of Interventions,10 and is reported per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.11 The risk of bias of each included study was assessed using the Mixed Methods Appraisal Tool (MMAT; see the study selection section for further details).12
Identification of Studies
Searches for English-language studies published between January 2013 and January 2021 were conducted in electronic database (Embase, MEDLINE and MEDLINE In-Process, PsycINFO, and EconLit [accessed via Ovid SP]) and gray literature data sources, to identify peer-reviewed studies on topics of interest relating to the target population (patients with COPD in GOLD groups A or B). These topics were clinical burden, economic burden, humanistic burden, and prevalence data. A date limit of 2013–2021 was applied to ensure that the most recent peer-reviewed evidence was identified (specifically any studies that used the 2013, 2017, or 2020 classification for GOLD A/B groups). Searches were also carried out to identify any relevant conference abstracts indexed in Embase in the previous 2 years (2019–2020). The database searches were conducted using a combination of free-text search terms and controlled vocabulary terms specific to each database, as recommended by the Cochrane Collaboration.10 Search strings were developed using guideline-recommended filters specific for each platform to identify real-world evidence studies.13 The search strategies for each SLR topic and database are detailed in Supplementary Tables 1–11.
Study Selection
Following the searches, all identified articles were screened for inclusion by two independent reviewers, based on the pre-defined population, exposures, characteristics, outcomes, and study design (PECOS) criteria outlined in Supplementary Table 12. Any disagreements were resolved by a third, senior reviewer. Studies that fulfilled all of the inclusion criteria and none of the exclusion criteria were eligible for inclusion in the review.
Quality assessment via the MMAT was conducted by one reviewer and validated by a second reviewer (Supplementary Materials–Data File 1). The MMAT included two initial screening questions: “Are there clear research questions?” and “Do the collected data allow the research questions to be addressed?”; A “No” or a “Can’t tell” response to either or both queries would indicate further assessment of the study in question might not be appropriate. Studies that passed the initial screening questions were then assessed by the following five questions designed for evaluating “quantitative descriptive studies”: “Is the sampling strategy relevant to address the research question?”; “Is the sample representative of the target population?”; “Are the measurements appropriate?”; “Is the risk of nonresponse bias low?”; and “Is the statistical analysis appropriate to answer the research question?”; A “Yes” response indicated that bias was unlikely to affect the findings. One point was assigned for each “Yes” response (ie a maximum of five points per study); no points were awarded for a “No” or a “Can’t tell” response. Studies with higher MMAT scores were considered of higher quality. The consideration of how each study rated according to each of these criteria was used to inform an overall judgement of whether that study was of “low”, “moderate”, or “high” quality with respect to the objectives of the current SLR.
Data Extraction
Data from the included studies were extracted into a pre-specified Microsoft Excel® template by one investigator and independently validated by a second, more senior researcher. For studies with more than one publication, the most recent results, records with the longest follow-up period, or results reported in the primary full-text publication were extracted and summarized as appropriate. Indirect mapping to GOLD classification was applied to studies that did not categorize patients based on GOLD “ABCD” classification but reported history of exacerbation and, where applicable, symptoms (mMRC/CAT score), which allowed participants to be mapped indirectly, but definitively, to GOLD A/B groups. To indirectly categorize patients in this study as being in GOLD group A, they were required to have a history of zero or one exacerbations in the previous year that did not lead to hospitalization, with either an mMRC score 0–1 or a CAT score <10. Similarly, to categorize patients as being in GOLD group B, they would have had to have a history of zero or one exacerbations in the previous year that did not lead to hospitalization, with either an mMRC score ≥2 or CAT score ≥10. If it was not possible to definitively categorize patients to GOLD group A or B specifically, they were alternatively classified as being in a combined A/B group, if this could be done reliably on the basis of baseline exacerbation history. It can be assumed that these methods of categorization were used to derive all results presented below for indirectly mapped A/B groups.
Results
Literature Search Results
The electronic database searches yielded a total of 1808 records. After removal of 487 duplicates, 1321 unique records were screened via title and abstract. Of these, 575 publications met the eligibility criteria for full-text screening (Figure 1).
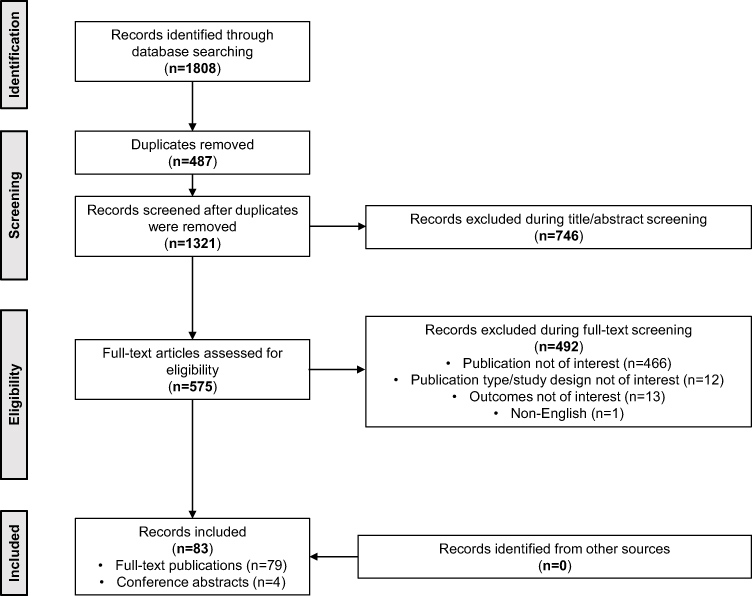 |
Figure 1 PRISMA Flow Chart. Abbreviation: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses. |
Following full-text review, 83 unique records met the PECOS selection criteria and were included in the review (Supplementary Table 13). Of these, 79 were full-text publications and four were conference abstracts. Of the 79 full-text publications, 75 reported clinical outcomes, 52 reported economic outcomes, 26 reported humanistic burden of disease, and three reported prevalence outcomes. Twelve publications reported clinical, humanistic, and economic outcomes in the same paper; 46 publications reported both clinical and economic outcomes; and 25 reported both clinical and humanistic outcomes. Many studies were from Europe (n=53) and the majority (n=76) were single-centre-based. Around half of the included publications (n=42) were of prospective design, followed by a considerable number of cross-sectional studies (n=28) and a small number of retrospective studies (n=13). Most of the publications reported data collected in an outpatient setting (n=51), while fewer studies reported a mix of inpatient and outpatient settings (n=9) or exclusively inpatient settings (n=2). For some studies, the settings were unavailable or unclear (n=21). In total, 73 publications categorized patients into separate GOLD groups (A and B). Two publications reported GOLD group A only and one publication reported GOLD group B only. One publication reported outcomes for GOLD groups A and B combined. Six publications did not report patients’ GOLD group and patients were indirectly mapped to GOLD A/B groups based on exacerbation history. Assessment of GOLD classification was most commonly based on the 2017 GOLD classification update (n=38), followed by 2013 GOLD update (n=17).
Patient Characteristics
The baseline characteristics of the patients described in the included publications are presented in Supplementary Table 14. Across the various GOLD group categorizations, the mean patient age at baseline ranged from 57.614 to 74.715 years (GOLD A), 59.114 to 77.915 years (GOLD B), 64.316 to 67.817 years (combined GOLD A/B), and 60.518 to 74.119 years (indirectly mapped combined GOLD A/B). The proportion of males ranged from 10.0%20 to 98.3%21 (GOLD A), 15.8%22 to 96.5%23 (GOLD B), 51.1%16 to 61.1%17 (combined GOLD A/B), and 52.1%24 to 94.4%25 (indirectly mapped combined GOLD A/B). The proportion of patients who were current smokers ranged from 15.2%26 to 62.4%27 (GOLD A) and 17.5%28 to 68.7%15 (GOLD B).
The proportion of overall patients in individual GOLD classification groups ranged from 4.7%29 to 77.4%30 (GOLD A), 10.7%27 to 63.2%31 (GOLD B), 60.0%24 to 68.7%16 (GOLD A/B), and 28.6%19 to 81.7%25 (indirectly mapped combined GOLD A/B) (Figure 2).
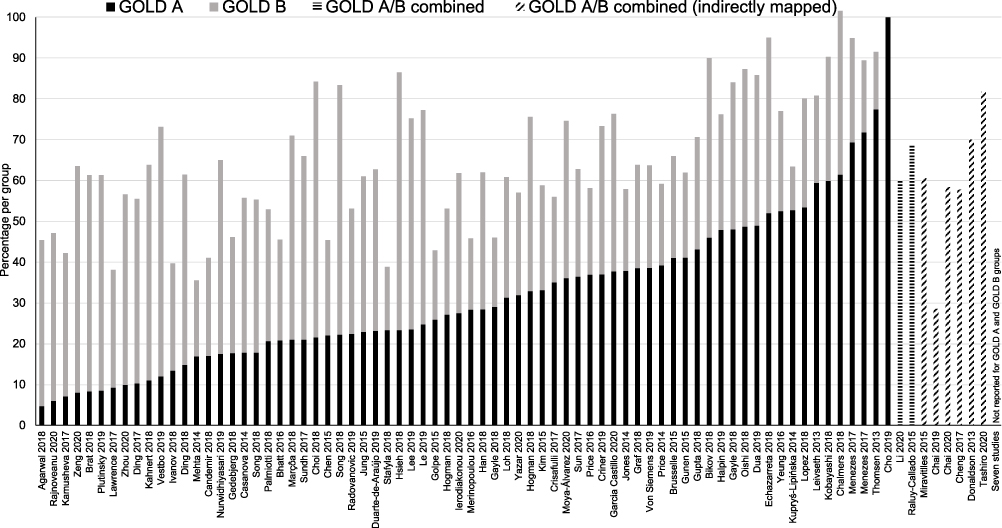 |
Figure 2 Percentage of Patients in GOLD A and GOLD B Groups Across Publications. Abbreviation: GOLD, Global Initiative for Chronic Obstructive Lung Disease. |
Forced expiratory volume in 1 second (FEV1) % predicted ranged from 54.3%32 to 83%30 (GOLD A), 40%33 to 72.8%15 (GOLD B), and 43.6%18 to 75.4%25 (indirectly mapped combined GOLD A/B). One publication reported an FEV1% predicted of 57% among GOLD A/B patients17 (Figure 3).
 |
Figure 3 FEV1% Predicted Among Patients in GOLD A and GOLD B Groups Across Publications. Abbreviations: FEV1, forced expiratory volume in 1 second; GOLD, Global Initiative for Chronic Obstructive Lung Disease. Notes: Scores are mean values unless otherwise stated; †Median scores. |
The proportion of patients with zero moderate/severe exacerbations in the previous year ranged from 62%34 to 100%15,35,36 (GOLD A), 38%34 to 100%15,35,36 (GOLD B), and 26%29 to 59%17 (combined GOLD A/B). The proportion of patients with one moderate exacerbation in the previous year (outpatient-treated, not leading to hospitalization) ranged from 0%15,36 to 47%34 (GOLD A), 0%15,36 to 53%34 (GOLD B), and 19%29 to 41%17 (combined GOLD A/B).
The mean mMRC baseline score ranged from 0.537 to 1.023,38–40 (GOLD A), 0.841 to 2.940 (GOLD B), and 1.4825 to 2.1342 (combined GOLD A/B). The mean CAT scores at baseline ranged from 3.737 to 13.943 (GOLD A [patients had been categorized as GOLD A based on mMRC score]), 11.537 to 21.844 (GOLD B), and 5.518 to 23.842 (combined indirectly mapped GOLD A/B groups) (Figure 4).
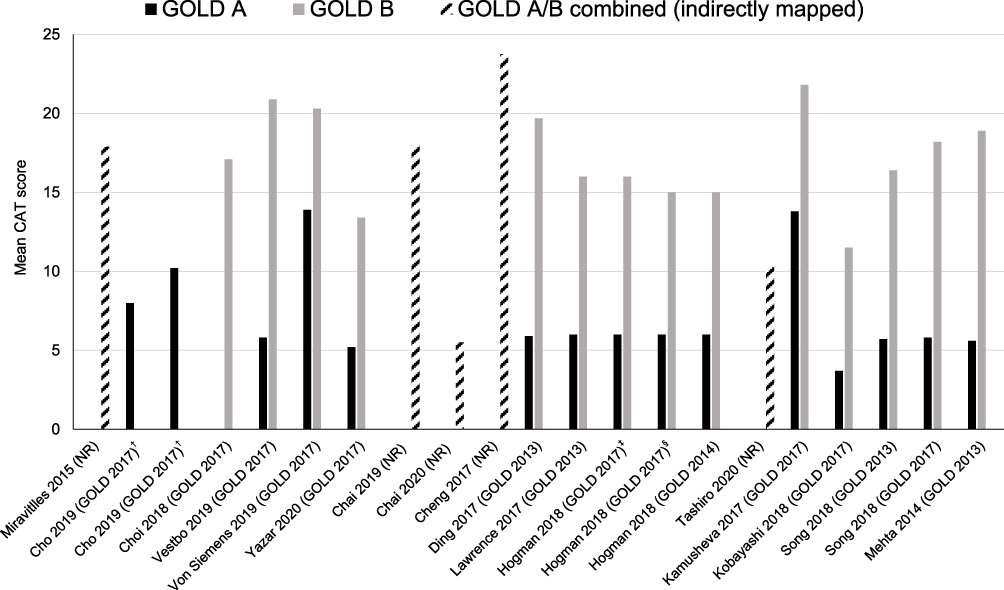 |
Figure 4 Distribution of Baseline CAT Score Among Patients in GOLD A and GOLD B Groups Across Publications. Abbreviations: CAT, COPD Assessment Test; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; NR, not reported; SD, standard deviation. Notes: †Cho 2019 reports CAT score for subgroups with and without regular treatment; ‡Hogman 2018 group C changing to group A with GOLD 2017: mean 6.0; group D changing to group B with GOLD 2017: mean 16.0; §Hogman 2018 group A remaining in group A GOLD 2017: mean 6.0; group B remaining in group B with GOLD 2017: mean 15.0. GOLD classification followed per study is shown in brackets (where reported). |
St George’s Respiratory Questionnaire (SGRQ) scores were not widely reported at baseline. Among the 11 studies reporting mean score, this ranged from 14.745 to 4133 (GOLD A), 32.623 to 64.033 (GOLD B), and 16.418 to 43.046 (combined GOLD A/B).
The proportion of patients receiving inhaled corticosteroids ranged from 4.8%28 to 77.6%21 (GOLD A) and 7.6%47 to 95.6%21 (GOLD B). The proportion of patients receiving triple therapy ranged from 0%28 to 55.2%21 (GOLD A) and 7.3%48 to 82.2%21 (GOLD B). One study (using the GOLD 2013 classification) found that among patients in the combined GOLD A/B group category, the proportion on triple therapy ranged from 5.9% in recently diagnosed patients to 21.1% in those with longer-established disease.16
Prevalence of GOLD A/B COPD
Three studies reported prevalence outcomes defined by the study criteria.16,49,50 Two of the studies used 2013 GOLD classification and one study used 2017 GOLD classification. One study reported the prevalence of GOLD A/B COPD among the general population and two studies report the prevalence of GOLD A/B COPD among those with COPD.
A retrospective study in the UK quantifying point prevalence of COPD in the general population during 2009–2013 reported a prevalence estimate (standardized for age and sex) for patients in a combined GOLD A/B group of 21.9 per 1000 persons (95% confidence interval [CI] 21.7 to 22.1) at the end of 2013.16 A higher prevalence was observed in males compared with females and in patients aged ≥75 years.
A population-based prevalence study in Argentina used cluster sampling and data collection from >4000 households to report the proportion of patients in GOLD A and GOLD B groups among all those with COPD, as opposed to an estimate of prevalence in the general population.49 A prevalence of 52% (95% CI 47 to 56) for GOLD A and 43% (95% CI 39 to 48) for GOLD B was estimated. Similarly, a cross-sectional study in Hong Kong estimating GOLD group prevalence among all patients with COPD in an outpatient setting reported that, overall, 77% of COPD patients were in GOLD A and GOLD B groups based on CAT score, with 52.5% and 24.5% being in GOLD A and GOLD B, respectively.50
Clinical Outcomes
In total, 75 of the included studies reported clinical outcomes of interest. Of these, 74 were full-text publications and one was a conference abstract. Of the 75 publications, 69 reported outcomes directly for GOLD A/B groups and six were indirectly mapped as reporting data for a combined A/B group. Thirty-two publications used the GOLD 2017 classification, 16 used GOLD 2013, four used 2014, two used 2015, three used 2016, and two used 2019. Ten publications used multiple GOLD classifications.
Exacerbations
Overall, 26 publications reported exacerbation outcomes. These data are presented in Supplementary Table 15. Two studies were indirectly mapped as GOLD A/B combined group (Supplementary Table 16).
In general, the rate of moderate exacerbations was higher among patients in GOLD group B compared with patients in GOLD group A (1.17 [95% CI 1.14 to 1.19] exacerbations per person-year in GOLD B vs 0.83 [95% CI 0.81 to 0.85] in GOLD A).51 Similarly, studies suggested that patients classified as GOLD B had at least a trend toward a higher relative risk of total exacerbations compared with patients classified as GOLD A (odds ratio [OR] 1.7 [95% CI 0.6 to 4.3]15 vs OR 2.95 [95% CI 1.60 to 5.45]37) and at least a trend towards significantly increased risk of severe exacerbations (OR 3.5 [95% CI 0.9 to 13.5]15 vs OR 8.19 [95% CI 2.82 to 23.8]37).
A higher proportion of patients were categorized as GOLD B (rather than GOLD D) when using 2017 GOLD classification, compared with previous classifications (2011–2016) based on exacerbation history/symptoms; GOLD B was reported to have the largest proportion of patients based on the 2017 classification (compared to pre-2017 classifications).52 Patients classified as GOLD B had a higher risk of exacerbation compared with patients classified as GOLD A as per pre-2017 classifications (GOLD B: 57.3% vs GOLD A: 25.8%) and 2017 to present classification (GOLD B: 55.3% vs GOLD A: 29.5%).52 According to data collected from the ECLIPSE study, at 3-year follow-up, exacerbations in the previous year were numerically higher based on the 2017 classification than the 2011 classification for GOLD A and GOLD B:32 GOLD A (2011 mean [standard deviation (SD)]: 0.2 [0.4]; 2017 mean [SD]: 0.3 [0.4]); GOLD B (2011 mean [SD]: 0.3 [0.4]; 2017 mean [SD]: 0.4 [0.5]).
Based on the 2017 classification, patients who shifted from GOLD A when defined by mMRC grade to GOLD B when defined by CAT score were less likely to be exacerbation-free at 36 months (55.7% vs 69.2%, p<0.0001), or severe exacerbation-free at 36 months (87.7% vs 95.5%, p=0.0002), and had more frequent exacerbations at 12 months (0.3±0.7 vs 0.1±0.4, p<0.0001) than those who remained in GOLD A.53 Among patients classified as GOLD A and GOLD B, risk of exacerbation was higher in those with lower body mass index (p=0.0168); more symptoms on either the mMRC (p<0.001) or CAT scales (p=0.0496); and more severe airflow limitation as defined by FEV1% predicted (p<0.001).37
Mortality
Sixteen publications reported mortality outcomes categorized by GOLD A and GOLD B groups. Mortality outcome data from all included studies are presented in Supplementary Table 17.
Higher mortality rates were consistently reported among patients classified as GOLD B compared with patients classified as GOLD A and GOLD C at various timepoints.15,32,37,40,48,54–57 A study with a follow-up of 4 years showed significantly higher mortality rates among patients in GOLD group B compared with those in GOLD group A (pre-2017 classification: 18.7% vs 14.3%, p=0.009; 2017 classification: 25.5% vs 14.8%, p=0.050).52 The use of spirometry findings in addition to the GOLD 2017 “ABCD” classification (to generate eight A/B subgroups) allowed more accurate prediction of mortality in the GOLD A and B groups.48 Age (p=0.001), mMRC score ≥2 (p<0.001), Charlson Comorbidity Index score (p<0.001), and history of exacerbation (p=0.006) were significant predictors of mortality (across GOLD A–D groups).48
Symptoms
Twenty-six publications reported symptom-related outcomes. Of these, 19 reported symptom-based outcomes for GOLD A and GOLD B groups. Symptom-related outcomes across all included studies are shown in Supplementary Table 18. Four publications were indirectly mapped as GOLD A/B combined group (Supplementary Table 19).
Patients with mMRC grade 1 showed a trend towards a higher risk of exacerbation in GOLD A groups (p=0.054) and a significantly increased risk of exacerbation in GOLD B (p<0.0001) compared with patients with mMRC grade 0.58 In GOLD A/B groups with a high prevalence of mMRC grade 1, patients had significantly lower pulmonary function (p<0.0001).58 Symptom burden as defined by mMRC score (OR 1.617; 95% CI 1.159 to 2.259, p=0.005), SGRQ score (OR 1.024; 95% CI 1.010 to 1.039, p=0.001), or FEV1% predicted (OR 0.979; 95% CI 0.962 to 0.995, p=0.013), and age (OR 1.049; 95% CI 1.010 to 1.089, p=1.049) were significantly associated with progression of patients in GOLD B (to GOLD D) at 1 year post-diagnosis, based on 2017 classification.41 Based on the 2017 classification, patients who shifted from GOLD A when defined by mMRC to GOLD B when defined by CAT were younger (65.4 [7.5] vs 67.5 [7.2] years, p<0.0001) and more likely to be current smokers (32.6% vs 18.2%, p<0.0001) compared with patients who remained in GOLD A.53
Economic Outcomes
Fifty-two publications reported economic burden outcomes for patients in GOLD A and/or GOLD B. Of these, 41 publications reported only data on proportion of patients on COPD medications, 13 publications reported healthcare resource utilization (HCRU) data for all GOLD groups. Eight publications reported HCRU data separately for GOLD A and GOLD B groups, and three publications reported data for overall GOLD cohort. Five publications reported data on total costs, including direct and indirect costs, separately for GOLD A and GOLD B groups. The studies that report the outcomes only for overall GOLD ABCD population are not discussed further in the report.
Healthcare Resource Utilization
Across the included studies, outcomes on hospitalization and physician visits were commonly reported. HCRU outcomes across included studies are detailed in Supplementary Table 20.
In the UK, the rate of hospitalizations was reported to increase with an increase in severity of GOLD group (GOLD group A to GOLD group B). The annual rate of COPD-related hospital admissions ranged from 0.22 (95% CI 0.20 to 0.25) to 0.35 (95% CI 0.31 to 0.40) in GOLD A and 0.48 (95% CI 0.46 to 0.51) to 0.57 (95% CI 0.54 to 0.61) in GOLD B.51 A Norwegian-based study indicated that GOLD B patients had a significantly increased risk of all-cause hospitalization (OR 3.1 [95% CI 2.1 to 4.4]) and respiratory hospitalization (OR 5.0 [95% CI 2.9 to 8.7]) compared with GOLD A patients.40 A UK study with a 3-year follow-up reported an increase in the annual rate of general practitioner visits per person per year based on severity of GOLD group. The rate of general practitioner visits ranged from 4.82 (95% CI 4.74 to 4.93) to 4.72 (95% CI 4.62 to 4.84) for GOLD A and 5.91 (95% CI 5.78 to 6.07) to 5.71 (95% CI 5.54 to 5.89) for GOLD B.51
Costs
Across studies, treatment costs, direct costs, and indirect costs were commonly reported. Cost outcomes across the studies are detailed in Supplementary Table 21.
A cross-sectional Vietnamese study reported a statistically significant difference in mean total cost per hospitalization for an exacerbation of COPD between GOLD groups (6.4 million Vietnamese dong [VND] vs 14.1 million VND [p<0.05], for GOLD A and GOLD B, respectively).59 A Danish registry study (2008–2017) reported total annual direct costs per patient to be higher in GOLD B versus GOLD A (€12,884 vs €8687, respectively) and lowest for GOLD A across all GOLD groups.60 A Bulgarian study reporting indirect costs across GOLD A and B groups estimated that the total mean indirect costs per patient per year were higher for GOLD B versus GOLD A (€692.51 vs €575.11, respectively [p<0.001]).44 A cross-sectional UK study using Clinical Practice Research Datalink data predicted lower treatment costs per patient per year based on GOLD 2017 treatment recommendations compared with 2013 recommendations (GOLD A: actual cost £465 vs predicted cost £275; GOLD B: actual cost £568 vs predicted cost £392), suggesting potential significant cost savings using the GOLD 2017 treatment strategy.34
Humanistic Burden
Twenty-six publications reported outcomes on humanistic burden. Of these, 12 publications reported health-related quality-of-life outcomes for GOLD A, GOLD B, or GOLD A/B combined based on GOLD 2013 and 2017 classifications (Supplementary Table 22). Four other studies reported outcomes that could be indirectly mapped to these groups based on patients’ exacerbation characteristics defined by the study criteria (Supplementary Table 23).
Across all studies there was a trend towards worse SGRQ scores (ie higher scores, indicating poorer health-related quality of life) in patients classified as GOLD B compared with patients classified as GOLD A and many were statistically significant (p<0.001).26,33,41,45,52 SGRQ total scores ranged from 22.052 to 5033 among patients classified as GOLD A and 26.326 to 5433 among patients classified as GOLD B. Patients classified as GOLD B experienced worse quality of life compared with patients classified as GOLD A in terms of total mean SGRQ score (44.5 [SD: 15.0] vs 22.8 [SD: 10.8] for patients classified as GOLD B and GOLD A, respectively).33 Significant predictors for worse total SGRQ score were more severe airflow limitation, frequent exacerbations, and pre-existing diabetes mellitus and cardiac disease (all p values <0.001).61 Higher SGRQ scores were significantly associated with patients progressing from GOLD B to GOLD D at 1 year of follow-up (OR 1.024 [95% CI 1.010 to 1.039], p=0.001), based on 2017 classification.41
Discussion
The broad characterization of GOLD A/B patients as having “mild-to-moderate” disease is long-established and reflected in initial treatment recommendations for such individuals. This SLR aimed to provide a systematic assessment of research-based insights into the burden of disease experienced by patients classified as GOLD group A or B, including those with characteristics of more severe disease, such as differences in symptoms, frequency of mild-to-moderate exacerbations, lung function, and health-related quality of life.
Evidence across the studies indicated a consistently higher disease burden among patients in GOLD group B compared with patients in GOLD group A with regard to various outcomes including clinical, humanistic, and economic measures. There was also evidence indicating predictors of worse outcomes among patients classified as GOLD group B and GOLD group A. These included older age, more severe airflow limitation (specifically FEV1% predicted), and heavier symptom burden (mMRC/CAT) at baseline. There was also some evidence to suggest that the subset of patients classified as GOLD A as defined by mMRC scale but GOLD B as defined by CAT scores are more prone to any, or severe, exacerbations than those who remain in GOLD A on both scales. This suggests that CAT is a more precise tool for assessing symptom burden than mMRC score. This is particularly important in GOLD A and GOLD B patients, who differ only in symptom severity. Although the disease burden was greater among GOLD B patients compared with GOLD A patients, there is still a significant range of disease burden among GOLD A patients, including significant risk of exacerbation and disease-related HCRU, suggesting that patients should be assessed individually when making treatment decisions rather than relying on GOLD category.
Previous reports have suggested that early intervention with maintenance therapy in COPD may be associated with improvements in lung function and symptoms, and a reduction in the risk of recurrent exacerbations.62 Understanding specific predictors of disease burden is important for helping physicians to categorize patients, allowing them to intervene earlier in the disease pathway and to tailor appropriate treatment to the individual patient where there is an unmet need (ie patients with a high disease burden). Consistent with the high disease burden observed among GOLD group B patients in the current study, such individuals have also been reported to have a higher risk of severe exacerbation during follow-up than GOLD group C patients per the 2017 classification criteria.63 This finding challenges the common assumption that GOLD C patients have more severe disease on account of their history of more frequent or severe exacerbations and suggests that symptoms provide prognostic information in the assessment of severe exacerbation risk. The mortality rate among patients classified as GOLD B has also been found to be higher compared with patients classified as GOLD C,48 suggesting the importance of symptoms as an indicator of future risk and need for assessment and appropriate management strategies. Overall, the evidence suggests the use of the “ABCD” classification tool does not perform well in stratifying risk of exacerbation and mortality for disease management decisions, given the variability in both the outcomes, and the potential drivers of these, seen among GOLD A and GOLD B patients. These findings highlight the need to assess and re-assess disease burden on an individual patient basis, particularly for those who have poorer lung function or are more symptomatic.
Since completion of this study, the GOLD 2023 strategy document has been published, in which the “ABCD” assessment tool is updated to an “ABE” assessment tool.8 Using this updated tool, patients with ≥2 moderate exacerbations or ≥1 severe exacerbation in the previous year are classified as GOLD group E and initial pharmacological treatment is recommended independent of the patients mMRC and/or CAT score.8 Criteria for GOLD A and GOLD B classification remain unchanged;8 however, initial maintenance therapy with dual long-acting β2-agonist + long-acting muscarinic antagonist therapy is now recommended for GOLD B patients, if appropriate.8 This updated recommendation is consistent with the higher disease burden seen among GOLD B patients versus GOLD A patients in the current analysis. This study has several key strengths including the rigorous and pragmatic approach to search for and select studies, with the aim of targeting representative cohorts. Evidence was therefore restricted to studies that reported on specific GOLD classifications (namely GOLD 2013 onwards, to help ensure comparability across studies), observational evidence, and articles published in the previous 10 years (to focus on evidence more likely to reflect current management and outcomes in routine practice). All studies included in the review were formally assessed for risk of bias and more than two-thirds of the studies included were rated as being moderate or high quality. Other strengths include the methodological rigor and comprehensive approach to collating data, which allowed identification of key trends in the evidence base. Further to this, no previous SLRs have been conducted that focus on both burden of illness and potential drivers in this population.
This study also has a number of limitations that should be taken into consideration. First, there was considerable heterogeneity across studies with regard to study location, data source, study period, and sample size, as well as a wide variation in duration of study follow-up; since most studies reported only short-term follow-ups, caution should be taken when extrapolating the findings to the longer term. Many of the studies were conducted in Europe or North America; this should be taken into account if considering the data from a global perspective. The implications of these findings may vary for different healthcare systems worldwide. Also, several studies did not report on GOLD A and GOLD B separately; findings from indirectly mapped studies should be considered alongside possible biases associated with the indirect mapping itself. In addition, some key data gaps in the literature were identified. These included a lack of studies providing true population prevalence estimates for patients in GOLD A and GOLD B groups, limited information on economic burden (particularly cost burden reported separately for GOLD A and GOLD B groups), and few studies assessing humanistic burden separately for GOLD A and GOLD B. The wide variation of instruments used across studies also limits their comparability. Addressing these gaps in future research will be important for further defining the disease burden and potential unmet need among such patients.
Conclusions
Data from this current SLR provide clear evidence of a generally heavier clinical, humanistic, and economic burden of disease for patients in GOLD B compared with patients in GOLD A, and highlight factors, such as FEV1% predicted and symptoms, that are associated with, and in some cases independently predict, worse outcomes for patients in GOLD A and B groups. Further research is warranted to explore the issues raised by the findings of this SLR, including key gaps in the published literature for the targeted population.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Institutional review board/ethics approval was not required for this study. No personal subject contact or primary collection of individual human data occurred.
Acknowledgments
Editorial support (in the form of writing assistance, including preparation of the draft manuscript under the direction and guidance of the authors, collating and incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing, and referencing) was provided by Rebecca Cunningham of Aura, a division of Spirit Medical Communications Group Limited (Manchester, UK), and was funded by GSK.
Author Contributions
All authors have made significant contributions to the work of the report, whether in terms of concept, research design, implementation, data acquisition, analysis and interpretation, or in all these areas; participate in the drafting, modification, or critical review of the clause; final approval of the forthcoming edition; an agreement has been reached on the journal to submit the article; and agree to be responsible for all aspects of the work.
Funding
This study was funded by GSK (study number 214854). The sponsor was involved in the study design, data analysis and interpretation, the writing of the report, and the decision to submit the article for publication. The sponsor was also given the opportunity to review the manuscript for medical and scientific accuracy, as well as intellectual property considerations.
Disclosure
Alexandrosz Czira, Kieran J. Rothnie, Chris Compton, and Afisi S Ismaila are employees of, and/or hold stocks/shares in, GSK. Afisi S Ismaila is also an unpaid part-time member of the McMaster University faculty in Canada. Sneha Purushotham and Ike Iheanacho are employees of Evidera. Evidera received funding from GSK to conduct the study. The authors report no other conflicts of interest in this work.
References
1. National Institute for Health and Care Excellence. Chronic obstructive pulmonary disease: how common is it? 2021; Available from: https://cks.nice.org.uk/topics/chronic-obstructive-pulmonary-disease/background-information/prevalence-incidence/.
2. World Health Organization. Chronic obstructive pulmonary disease (COPD); 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
3. Mathers CD, Loncar D, Samet J. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
4. Sullivan SD, Ramsey SD, Lee TA. The economic burden of COPD. Chest. 2000;117(Suppl 2):5S–9S. doi:10.1378/chest.117.2_suppl.5S
5. Vestbo J, Hurd SS, Rodriguez-Roisin R. The 2011 revision of the global strategy for the diagnosis, management and prevention of COPD (GOLD)--why and what? Clin Respir J. 2012;6(4):208–214. doi:10.1111/crj.12002
6. Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
7. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2017 report; 2017. Available from: https://goldcopd.org/wp-content/uploads/2017/02/wms-GOLD-2017-FINAL.pdf.
8. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2023 report; 2022. Available from: https://goldcopd.org/2023-gold-report-2/.
9. Müllerová H, Shukla A, Hawkins A, Quint J. Risk factors for acute exacerbations of COPD in a primary care population: a retrospective observational cohort study. BMJ Open. 2014;4(12):e006171. doi:10.1136/bmjopen-2014-006171
10. Higgins JPT, Thomas J, Chandler J et al, editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022); 2022. Available from: https://training.cochrane.org/handbook/current.
11. PRISMA Transparent Reporting of Systematic Reviews and Meta-Analyses. PRISMA statement; 2021. Available from: http://prisma-statement.org/PRISMAStatement/PRISMAStatement.aspx.
12. Hong QN, Pluye P, Fàbregues S, et al. Mixed Methods Appraisal Tool (MMAT) version 2018; 2018. Available from: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf.
13. Canadian Agency for Drugs and Technologies in Health. CADTH search filters database; 2019. Available from: https://searchfilters.cadth.ca/.
14. Gupta KK, Roy B, Chaudhary SC, et al. Prevalence of pulmonary artery hypertension in patients of chronic obstructive pulmonary disease and its correlation with stages of chronic obstructive pulmonary disease, exercising capacity, and quality of life. J Family Med Prim Care. 2018;7(1):53–57. doi:10.4103/jfmpc.jfmpc_18_17
15. Chen CZ, Ou CY, Yu CH, Yang SC, Chang HY, Hsiue TR. Comparison of global initiative for chronic obstructive pulmonary disease 2013 classification and body mass index, airflow obstruction, dyspnea, and exacerbations index in predicting mortality and exacerbations in elderly adults with chronic obstructive pulmonary disease. J Am Geriatr Soc. 2015;63(2):244–250. doi:10.1111/jgs.13258
16. Raluy-Callado M, Lambrelli D, MacLachlan S, Khalid JM. Epidemiology, severity, and treatment of chronic obstructive pulmonary disease in the United Kingdom by GOLD 2013. Int J Chron Obstruct Pulmon Dis. 2015;10:925–937. doi:10.2147/COPD.S82064
17. Chalmers JD, Poole C, Webster S, Tebboth A, Dickinson S, Gayle A. Assessing the healthcare resource use associated with inappropriate prescribing of inhaled corticosteroids for people with chronic obstructive pulmonary disease (COPD) in GOLD groups A or B: an observational study using the Clinical Practice Research Datalink (CPRD). Respir Res. 2018;19(1):63. doi:10.1186/s12931-018-0767-2
18. Chai CS, Mos SB, Ng DL, et al. Clinical phenotypes and health-related quality of life of COPD patients in a rural setting in Malaysia - a cross-sectional study. BMC Pulm Med. 2020;20(1):254. doi:10.1186/s12890-020-01295-4
19. Chai CS, Liam CK, Pang YK, et al. Clinical phenotypes of COPD and health-related quality of life: a cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2019;14:565–573. doi:10.2147/COPD.S196109
20. Nurwidhiyasari D, Rachmi SF, Indracahyani A, Nuraini T. Relationship between severity and quality of life in chronic obstructive pulmonary disease patients at hospitals’ outpatient units in Jakarta. Enfermería Clínica. 2019;29(Suppl 2):159–165. doi:10.1016/j.enfcli.2019.04.024
21. Kim J, Yoon HI, Oh YM, et al. Lung function decline rates according to GOLD group in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2015;10:1819–1827. doi:10.2147/COPD.S87766
22. Leivseth L, Brumpton BM, Nilsen TI, Mai XM, Johnsen R, Langhammer A. GOLD classifications and mortality in chronic obstructive pulmonary disease: the HUNT Study, Norway. Thorax. 2013;68(10):914–921. doi:10.1136/thoraxjnl-2013-203270
23. Song JH, Lee CH, Um SJ, et al. Clinical impacts of the classification by 2017 GOLD guideline comparing previous ones on outcomes of COPD in real-world cohorts. Int J Chron Obstruct Pulmon Dis. 2018;13:3473–3484. doi:10.2147/COPD.S177238
24. Li Y, Lim J, Stemkowski S, Kaila S, Renda A, Shaikh A. Initiation of triple therapy maintenance treatment among patients with COPD. Am J Manag Care. 2020;26(4):e106–e112 doi:10.37765/ajmc.2020.42837.
25. Tashiro H, Kurihara Y, Takahashi K, et al. Clinical features of Japanese patients with exacerbations of chronic obstructive pulmonary disease. BMC Pulm Med. 2020;20(1):318. doi:10.1186/s12890-020-01362-w
26. Lawrence PJ, Kolsum U, Gupta V, et al. Characteristics and longitudinal progression of chronic obstructive pulmonary disease in GOLD B patients. BMC Pulm Med. 2017;17(1):42. doi:10.1186/s12890-017-0384-8
27. Kupryś-Lipińska I, Kuna P. Impact of chronic obstructive pulmonary disease (COPD) on patient’s life and his family. Pneumonol Alergol Pol. 2014;82(2):82–95. doi:10.5603/PiAP.2014.0014
28. Rajnoveanu RM, Rajnoveanu AG, Ardelean AB, et al. Pulmonologists adherence to the chronic obstructive pulmonary disease GOLD guidelines: a goal to improve. Medicina (Kaunas). 2020;56(9):422. doi:10.3390/medicina56090422
29. Agarwal A, Batra S, Prasad R, Verma A, Jilani AQ, Kant S. A study on the prevalence of depression and the severity of depression in patients of chronic obstructive pulmonary disease in a semi-urban Indian population. Monaldi Arch Chest Dis. 2018;88(1):902. doi:10.4081/monaldi.2018.902
30. Thomsen M, Ingebrigtsen TS, Marott JL, et al. Inflammatory biomarkers and exacerbations in chronic obstructive pulmonary disease. JAMA. 2013;309(22):2353–2361. doi:10.1001/jama.2013.5732
31. Hsieh MJ, Huang SY, Yang TM, et al. The impact of 2011 and 2017 Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) guidelines on allocation and pharmacological management of patients with COPD in Taiwan: Taiwan Obstructive Lung Disease (TOLD) study. Int J Chron Obstruct Pulmon Dis. 2018;13:2949–2959. doi:10.2147/COPD.S176065
32. Faner R, Noell G, Badia JR, et al. Distribution, temporal stability and association with all-cause mortality of the 2017 GOLD groups in the ECLIPSE cohort. Respir Med. 2018;141:14–19. doi:10.1016/j.rmed.2018.06.015
33. Candemir I, Ergun P, Kaymaz D, Tasdemir F, Egesel N. The comparison of clinical variables in two classifications: GOLD 2017 combined assessment and spirometric stage of chronic obstructive pulmonary disease. Tuberc Respir Dis (Seoul). 2018;81(4):281–288. doi:10.4046/trd.2017.0114
34. Gayle A, Dickinson S, Morris K, Poole C, Mathioudakis AG, Vestbo J. What is the impact of GOLD 2017 recommendations in primary care? - a descriptive study of patient classifications, treatment burden and costs. Int J Chron Obstruct Pulmon Dis. 2018;13:3485–3492. doi:10.2147/COPD.S173664
35. Bikov A, Horváth A, Tomisa G, Bártfai L, Bártfai Z. Changes in the burden of comorbidities in patients with COPD and asthma-COPD overlap according to the GOLD 2017 recommendations. Lung. 2018;196(5):591–599. doi:10.1007/s00408-018-0141-7
36. Gedebjerg A, Szépligeti SK, Wackerhausen LH, et al. Prediction of mortality in patients with chronic obstructive pulmonary disease with the new Global Initiative for Chronic Obstructive Lung Disease 2017 classification: a cohort study. Lancet Respir Med. 2018;6(3):204–212. doi:10.1016/S2213-2600(18)30002-X
37. Kobayashi S, Hanagama M, Ishida M, et al. Clinical characteristics and outcomes in Japanese patients with COPD according to the 2017 GOLD classification: the Ishinomaki COPD Network Registry. Int J Chron Obstruct Pulmon Dis. 2018;13:3947–3955. doi:10.2147/COPD.S182905
38. Högman M, Sulku J, Ställberg B, et al. 2017 Global Initiative for Chronic Obstructive Lung Disease reclassifies half of COPD subjects to lower risk group. Int J Chron Obstruct Pulmon Dis. 2017;2018(13):165–173 doi:10.2147/COPD.S151016.
39. Jung YH, Lee DY, Kim DW, et al. Clinical significance of laryngopharyngeal reflux in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2015;10:1343–1351. doi:10.2147/COPD.S84337
40. Le LAK, Johannessen A, Hardie JA, et al. Prevalence and prognostic ability of the GOLD 2017 classification compared to the GOLD 2011 classification in a Norwegian COPD cohort. Int J Chron Obstruct Pulmon Dis. 2019;14:1639–1655. doi:10.2147/COPD.S194019
41. Choi HS, Na JO, Lee JD, et al. Which GOLD B patients progress to GOLD D with the new classification? Int J Chron Obstruct Pulmon Dis. 2018;13:3233–3241. doi:10.2147/COPD.S177944
42. Cheng Y, Tu X, Pan L, et al. Clinical characteristics of chronic bronchitic, emphysematous and ACOS phenotypes in COPD patients with frequent exacerbations. Int J Chron Obstruct Pulmon Dis. 2017;12:2069–2074. doi:10.2147/COPD.S140231
43. von Siemens SM, Jörres RA, Behr J, et al. Effect of COPD severity and comorbidities on the result of the PHQ-9 tool for the diagnosis of depression: results from the COSYCONET cohort study. Respir Res. 2019;20(1):30. doi:10.1186/s12931-019-0997-y
44. Kamusheva M, Dimitrova M, van Boven JF, et al. Clinical characteristics, treatment patterns, and socio-economic burden of COPD in Bulgaria. J Med Econ. 2017;20(5):503–509. doi:10.1080/13696998.2017.1279620
45. Cho J, Lee CH, Hwang YI, et al. Outcome of regular inhaled treatment in GOLD A chronic obstructive pulmonary disease patients. Respiration. 2019;98(4):312–320. doi:10.1159/000495756
46. Donaldson GC, Müllerova H, Locantore N, et al. Factors associated with change in exacerbation frequency in COPD. Respir Res. 2013;14(1):79. doi:10.1186/1465-9921-14-79
47. Price D, West D, Brusselle G, et al. Management of COPD in the UK primary-care setting: an analysis of real-life prescribing patterns. Int J Chron Obstruct Pulmon Dis. 2014;9:889–904. doi:10.2147/COPD.S62750
48. Han MZ, Hsiue TR, Tsai SH, Huang TH, Liao XM, Chen CZ. Validation of the GOLD 2017 and new 16 subgroups (1A–4D) classifications in predicting exacerbation and mortality in COPD patients. Int J Chron Obstruct Pulmon Dis. 2018;13:3425–3433. doi:10.2147/COPD.S179048
49. Echazarreta AL, Arias SJ, Del Olmo R, et al. Prevalence of COPD in 6 urban clusters in Argentina: the EPOC.AR study. Arch Bronconeumol (Engl Ed). 2018;54(5):260–269. doi:10.1016/j.arbres.2017.09.018
50. Yeung S, Chan P, Lai L, Chow K, Luk M, Chao D. Prevalence of different severities of chronic obstructive pulmonary disease in an out-patient clinic in Hong Kong. HK Pract. 2016;38:3–12.
51. Merinopoulou E, Raluy-Callado M, Ramagopalan S, MacLachlan S, Khalid JM. COPD exacerbations by disease severity in England. Int J Chron Obstruct Pulmon Dis. 2016;11:697–709. doi:10.2147/COPD.S100250
52. Plutinsky M, Brat K, Svoboda M, Zatloukal J, Popelkova P, Koblizek V. Prognostic accuracy of three COPD classification systems in relation to long-term mortality of COPD patients: a prospective multicenter study. Lung. 2019;197(2):173–179. doi:10.1007/s00408-019-00196-6
53. Ocheltree S, Male E, Zhao H, et al. Differences in GOLD 2017 treatment group assignments between the COPD assessment test and modified Medical Research Council Dyspnea Scale and their association with exacerbations: an analysis of the SPIROMICS cohort. Am J Respir Crit Care Med. 2019;199:A1113. doi:10.1164/ajrccm-conference.2019.199.1_MeetingAbstracts.A1113
54. García Castillo E, Alonso Pérez T, Ancochea J, et al. Mortality prediction in chronic obstructive pulmonary disease comparing the GOLD 2015 and GOLD 2019 staging: a pooled analysis of individual patient data. ERJ Open Res. 2020;6(4):00253–02020. doi:10.1183/23120541.00253-2020
55. Cabrera López C, Casanova Macario C, Marín Trigo JM, et al. Comparison of the 2017 and 2015 Global Initiative for Chronic Obstructive Lung Disease reports. Impact on grouping and outcomes. Am J Respir Crit Care Med. 2018;197(4):463–469. doi:10.1164/rccm.201707-1363OC
56. Criner RN, Labaki WW, Regan EA, et al. Mortality and exacerbations by Global Initiative for Chronic Obstructive Lung Disease Groups ABCD: 2011 versus 2017 in the COPDGene® cohort. Chronic Obstr Pulm Dis. 2019;6(1):64–73. doi:10.15326/jcopdf.6.1.2018.0130
57. Golpe R, Mengual-Macenlle N, Sanjuán-López P, Cano-Jiménez E, Castro-Añón O, Pérez-de-Llano LA. Prognostic indices and mortality prediction in COPD caused by biomass smoke exposure. Lung. 2015;193(4):497–503. doi:10.1007/s00408-015-9731-9
58. Oishi K, Hirano T, Hamada K, et al. Characteristics of 2017 GOLD COPD group A: a multicenter cross-sectional CAP study in Japan. Int J Chron Obstruct Pulmon Dis. 2018;13:3901–3907. doi:10.2147/COPD.S181938
59. Ngo CQ, Thi Bui T, Vu GV, et al. Direct hospitalization cost of patients with acute exacerbation of chronic obstructive pulmonary disease in Vietnam. Int J Environ Res Public Health. 2018;16(1):88. doi:10.3390/ijerph16010088
60. Løkke A, Lange P, Lykkegaard J, et al. Economic burden of COPD by disease severity - a nationwide cohort study in Denmark. Value Health. 2020;23(Suppl 2):S720. doi:10.1016/j.jval.2020.08.1903
61. Horner A, Burghuber OC, Hartl S, et al. Quality of life and limitations in daily life of stable COPD outpatients in a real-world setting in Austria - results from the CLARA project. Int J Chron Obstruct Pulmon Dis. 2020;15:1655–1663. doi:10.2147/COPD.S252033
62. Hanania NA. Optimizing maintenance therapy for chronic obstructive pulmonary disease: strategies for improving patient-centered outcomes. Clin Ther. 2007;29(10):2121–2133. doi:10.1016/j.clinthera.2007.10.006
63. Sansbury LB, Rothnie KJ, Bains C, Compton C, Anley G, Ismaila AS. Healthcare, medication utilization and outcomes of patients with COPD by GOLD classification in England. Int J Chron Obstruct Pulmon Dis. 2021;16:2591–2604. doi:10.2147/COPD.S318969
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.