Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
FIDEPOC: Consensus on Inspiratory Flow and Lung Deposition as Key Decision Factors in COPD Inhaled Therapy
Authors González-Torralba F, Baloira A ![]() , Abad A, Fuster A
, Abad A, Fuster A ![]() , García-Rivero JL, García-Sidro P, Márquez-Martín E, Palop M, Soler N, Velasco JL
, García-Rivero JL, García-Sidro P, Márquez-Martín E, Palop M, Soler N, Velasco JL
Received 15 February 2022
Accepted for publication 27 April 2022
Published 4 May 2022 Volume 2022:17 Pages 1005—1015
DOI https://doi.org/10.2147/COPD.S360938
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Fernando González-Torralba,1 Adolfo Baloira,2 Araceli Abad,3 Antonia Fuster,4 Juan Luis García-Rivero,5 Patricia García-Sidro,6 Eduardo Márquez-Martín,7 Marta Palop,8 Néstor Soler,9 José Luis Velasco10
1Respiratory Department, University Hospital of Aranjuez, Madrid, Spain; 2Respiratory Department, University Hospital of Pontevedra, Pontevedra, Spain; 3Respiratory Department, University Hospital of Getafe, Madrid, Spain; 4Respiratory Department, University Hospital Son Llatzer, Palma de Mallorca, Spain; 5Respiratory Department, University Hospital Marqués de Valdecilla, Santander, Spain; 6Respiratory Department, University Hospital of La Plana, Castellón, Spain; 7Respiratory Department, University Hospital Virgen del Rocío, Sevilla, Spain; 8Respiratory Department, Hospital of Sagunto, Valencia, Spain; 9Respiratory Department, Hospital Clinic, Barcelona, Spain; 10Respiratory Department, University Hospital Virgen de la Victoria, Málaga, Spain
Correspondence: Adolfo Baloira, Email [email protected]
Purpose: The pharmacological treatment of chronic obstructive pulmonary disease (COPD) is largely based on inhaled bronchodilators. Inspiratory flow and lung deposition are key parameters to be considered in inhaled therapy; however, the relationship between these two parameters, the patient specificities, and the suitability of the inhaler type for COPD management has not been fully addressed. The present study follows a Delphi Panel methodology to find expert consensus on the role of inspiratory flow and lung deposition as key decision factors in COPD inhaled therapy.
Methods: A two-round Delphi Panel, consisting of 38 statements (items) and completed by 57 Spanish pulmonologists, was carried out to measure the experts’ consensus degree with each item.
Results: A high degree of consensus was reached on most of the items consulted, among these inspiratory flow or inspiratory capacity should be periodically considered when choosing an inhalation device and to ensure the suitability of the inhaler used; the outflow velocity and particle size of the different devices should be considered to ensure adequate lung deposition; an active device (pressurized metered-dose inhalers (pMDI) or soft mist inhalers (SMI)) should be used in patients with low inspiratory flow to achieve adequate lung deposition; and, the use of dry powder inhalers (DPI) should be re-evaluated in patients with severe obstruction and severe exacerbations.
Conclusion: This study shows the relevance of inspiratory flow and the degree of particle deposition in the lung in the choice of an inhalation device for COPD management, as well as the convenience of an SMI type device in cases of low inspiratory flow. Moreover, it highlights the scarcity of information on the specific features of inhalation devices in COPD guidelines.
Keywords: dry powder inhalers, pressurized metered-dose inhalers, soft mist inhaler, inhaled therapy device, exacerbations
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive, life-threatening lung disease that predisposes to exacerbations and other serious diseases1 More than 3 million people die each year from COPD worldwide, accounting for 6% of all deaths globally.2 In recent years, the prevalence of COPD has enlarged dramatically, with an increase of 44.2% between 1990 and 20153- In fact, COPD was the third leading cause of death worldwide in 2019.4
Long-acting bronchodilators are a key component of COPD pharmacological management, either in monotherapy or in combination depending on the patient’s risk level.5 Therefore, the selection of an inhalation device is a crucial step in the therapeutic management of COPD, as it influences drug efficacy and patient adherence to treatment, and consequently long-term outcomes.6 There are different types of inhalation devices, the most frequently used being: pressurized metered-dose inhalers (pMDI), dry powder inhalers (DPI) and soft mist inhalers (SMI).7–11 Two key characteristics of an inhaler device are: a high lung deposition, defined as the average probability of an inhaled particle being deposited in the lung, and the correct delivery of the drug despite the presence of a low inspiratory flow.12 A low inspiratory flow is associated with the presence of pulmonary hyperinflation, which is defined by an increase in functional residual capacity and is the main mechanism explaining dyspnea in COPD patients. Furthermore, COPD exacerbations are associated with a decrease in peak inspiratory flow,13 that can influence inspiratory flow rate.2 In fact, COPD exacerbations are also associated with a decrease in peak inspiratory flow14 Given the relevance of the inspiratory flow and lung deposition in the therapeutic management of COPD, and the scarcity of information on the relation between these two parameters and the features of each inhaler type on Spanish and international COPD guidelines, it is key to develop a consensus document to help clinicians in the choice of the appropriate type of device.
The present study, named FIDEPOC for its acronym in Spanish, follows a Delphi Panel methodology to find consensus on the role of inspiratory flow and lung deposition as key decision factors in COPD inhaled therapy. The Delphi method consists of a structured process to reach consensus on issues of interest among a group of experts when there is a lack of robust evidence on the topic15–17 This study analyses through the opinion of a Spanish COPD expert pulmonologists panel, the factors that affect inspiratory flow and lung deposition in COPD patients and the features of different inhalation device types (pMDI, DPI and SMI) in relation with these parameters. The FIDEPOC study is the first expert consensus study published to date focusing on inspiratory flow and lung deposition as key decision factors in COPD inhaled therapy.
Materials and Methods
The Delphi Panel
The Delphi Panel employed in this study is characterized by three aspects: anonymity of the answers given by the participants throughout the process, to avoid influences of opinion within the expert group; allowing panel participants to change their opinion from one round of questionnaires or surveys to another (iteration); and controlled feedback, implying that the panelists receive the results of the previous rounds.18
According to the selection criteria, the 57 participating experts that constituted the Delphi panel were Spanish practicing pulmonologists with more than 10 years of experience in the management of COPD, 53% of them with a specialized practice on COPD. The experts were contacted by email and were selected based on their experience and with a representation from all over the country (the hospitals are detailed in the acknowledgments). Of the 65 pulmonologists contacted, 8 declined to participate. The 57 experts completed the second round of the survey.
Study Questionnaire and Objectives
Based on the evidence generated in the recent systematic literature review (SLR) on inspiratory flow and lung deposition in COPD patients using different inhaler devices,2 a questionnaire with a total of 38 items was designed by a panel of 8 COPD experts overseen by a coordinating committee of 2 pulmonologists, and provided to the participating panelists whom, in turn, indicated their degree of agreement or disagreement on the items of the questionnaire in a first consultation round according to a Likert scale (1, fully disagree; 2) partially disagree; 3) doubtful; 4) partially agree; 5, fully agree). Subsequently, a controlled evaluation of the questionnaire results was carried out, the experts’ responses were then analyzed quantitatively and qualitatively, and a second consultation round was performed. In this second round, only the items for which there was weak consensus or disagreement in the first round were subjected to a second consultation. The statements that did not reach this predefined level of agreement were reassessed by the scientific committee, to discern if the lack of consensus was due to the ambiguity of the statement itself, in which case it was reformulated, or due to the asseveration being controversial in the field, in which case the statement remained unchanged in the second.
Delphi Round
The questionnaire was parameterized in a proprietary web tool (Ampersand Consulting) built in PHP (personal home page) and MySQL (My Structured Query Language) database. This Access database allowed results collection and data export to Microsoft Excel. To avoid the possibility of abstention, the design of the web platform made it mandatory for the experts to indicate a degree of agreement with the items.
The questionnaire was divided into 4 categories according to the study objectives: category 1 - to identify the patient factors, related to inspiratory flow and lung deposition, to be considered in inhaled therapy; category 2 – to identify the characteristics of the devices to be taken into account, related to inspiratory flow and lung deposition in inhaled therapy; category 3 – to establish the relationship between the characteristics of the different types of inhalation devices; and category 4 – to recommend action guidelines in clinical practice for the selection of inhalation devices.
Data Analysis
For data analysis and generation of results, the Likert scale values obtained during the consultation rounds were transformed into 3 categories of agreement (in disagreement -scores 1–2; indifferent - score 3 or in agreement - score 4−5)18 To measure the experts’ degree of agreement, the number of panelists who agreed, were indifferent, or disagreed with each item was transformed into agreement percentages. Consensus for each statement was defined as an agreement percentage of at least 70% of respondents, and consensus was not reached if the sum of responses for negative consensus or positive consensus was <70%.19 Subsequently, the degree of consensus for each item was defined as follows -Unanimity, 100% of the expert panelists agree on the same item; -Strong consensus, 80% or more of the experts agree on the same item; -Weak consensus, at least 70% of the experts on the panel agree on the same item without reaching unanimity or strong consensus; -Discrepancy, when 70% agreement among the panelists is not reached.
Results
The 57 participating pulmonologists completed the two rounds of the Delphi panel from December 2020 to March 2021, indicating their degree of agreement with the items proposed, and none of them abstained. The consensus degree reached by the panel in the first and second rounds in relation to the items consulted is shown in Figures 1–5, respectively. The results are shown by questionnaire categories according to the 4 objectives of the study.
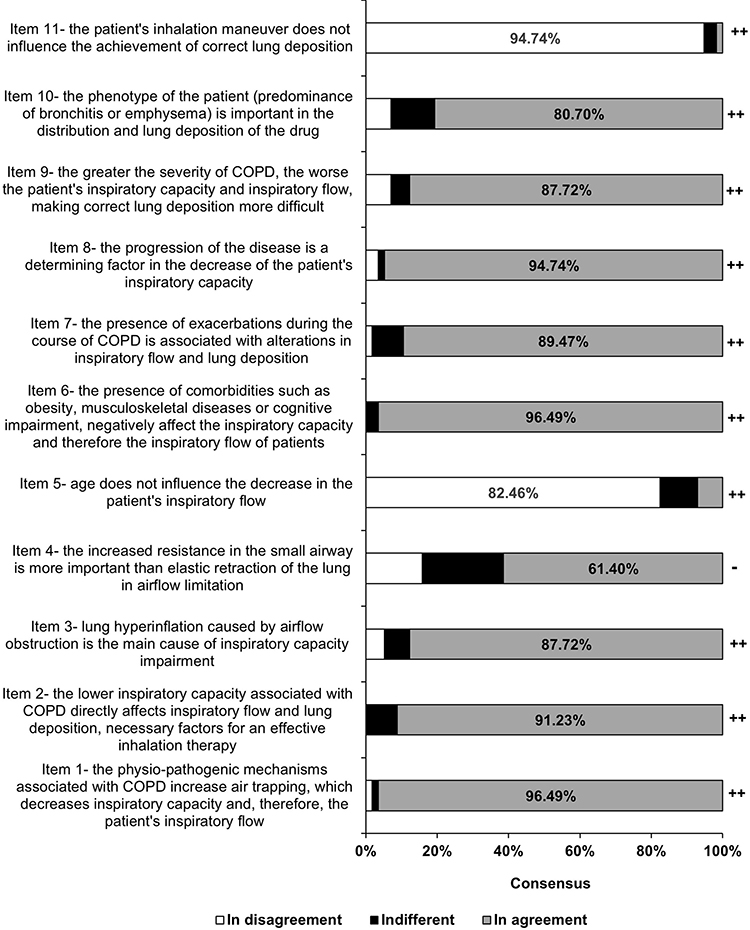 |
Figure 1 Expert consensus on the identification of patient factors, related to inspiratory flow and lung deposition, to be considered in inhaled therapy. A high level of consensus was reached in all items but in item 4, perhaps because it is an issue with complex pathophysiological implications. Consensus degree is shown as: ++(strong consensus, >80% of the experts agreed) and - (discrepancy, <70% agreed). |
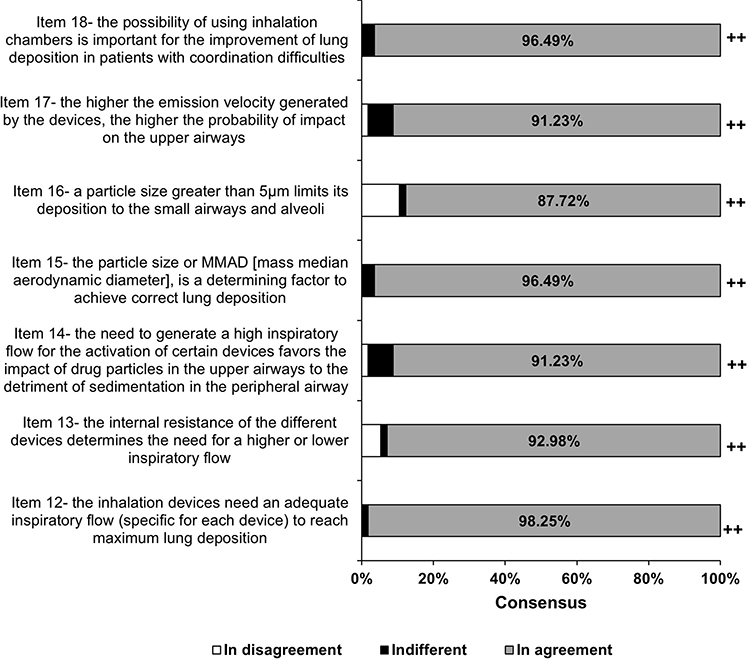 |
Figure 2 Expert consensus on the identification of the characteristics of the different inhalation devices related to inspiratory flow and lung deposition in inhaled therapy. The percentage of agreement among the experts is indicated. The panel reached strong consensus in all of these items. Consensus degree is shown as: ++(strong consensus, >80% of the expert panelists agreed). |
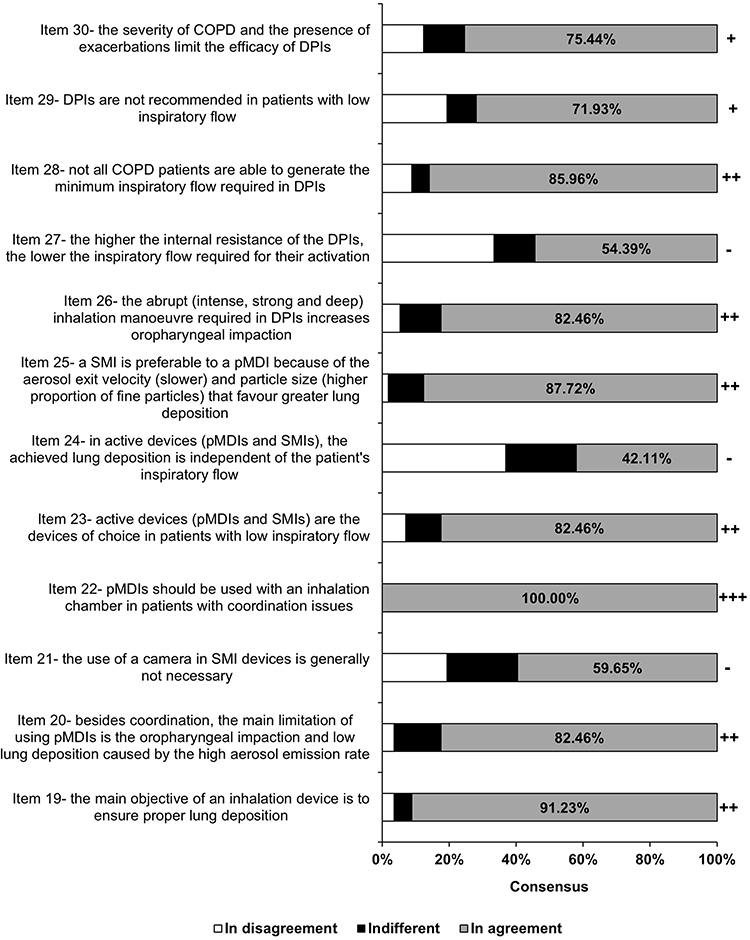 |
Figure 3 Expert consensus on the relationship between the characteristics of the different inhalation devices (DPI, pMDI and SMI). The percentage of agreement among the experts is indicated. Aspects related to the characteristics of the devices produced the greatest disagreement. The concepts of intrinsic resistance and inspiratory flow are likely to lead to some confusion even among expert pulmonologists. Consensus degree is shown as: +++(unanimity, 100% of the experts agreed); ++(strong consensus, >80% of the panelists agreed); +(weak consensus, <80% and >70% agreed); and - (discrepancy, <70% agreed). |
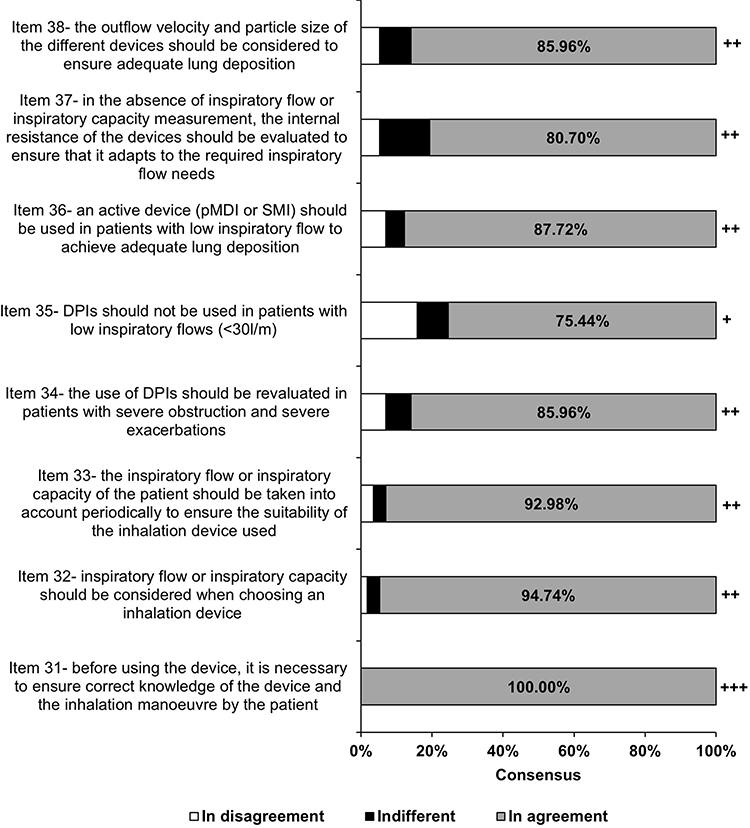 |
Figure 4 Expert consensus on recommended guidelines for the choice and use of inhaler devices in clinical practice with respect to inspiratory flow and lung deposition in inhaled therapy. The percentage of agreement among the experts is indicated. The most clinical-related issues reached strong agreement. Consensus degree is shown as: +++(unanimity, 100% of the experts agreed); ++(strong consensus, >80% agreed); and +(weak consensus, <80% and >70% agreed). |
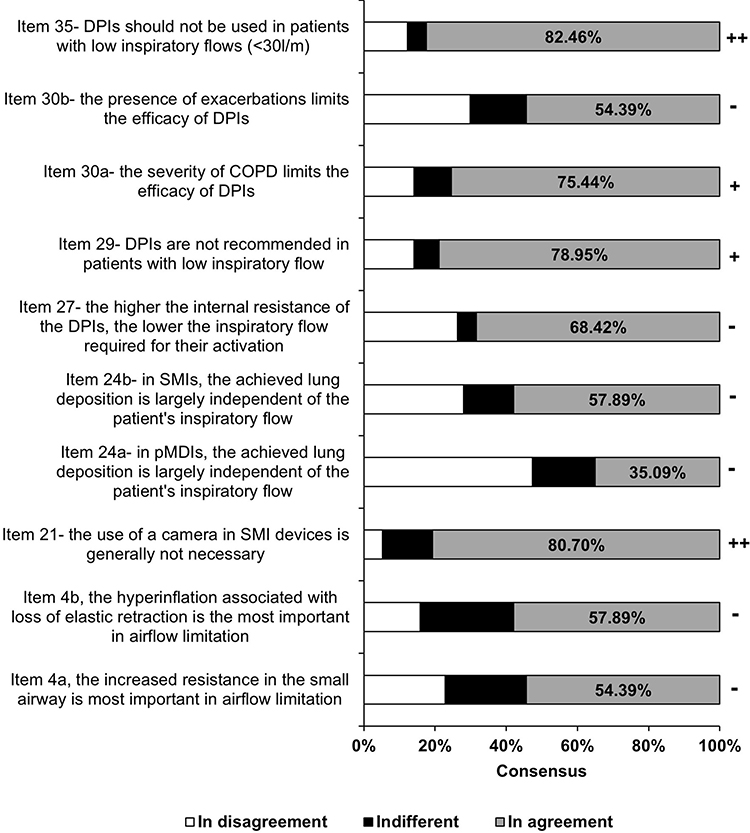 |
Figure 5 Expert consensus in the second round of the Delphi panel. In the second round, the issues related to the devices continued to maintain some discrepancies. Consensus degree is shown as: ++(strong consensus, >80% of the experts agreed); +(weak consensus, <80% and >70% agreed); and - (discrepancy, <70% agreed). |
The panel reached strong consensus (>80%) in all the items regarding the identification of patient factors, related to inspiratory flow and lung deposition, to be considered in inhaled therapy, except for item 4 (Figure 1). However, despite rephasing item 4 into items 4a and 4b, no consensus was reached on this topic during the second round (Figure 5). Of note, the strong consensus reached for items 5 and 11 indicates disagreement with these statements.
The consensus degree attained by the experts with respect to the identification of characteristics of the different inhalation devices (DPI, pMDI and SMI) related to inspiratory flow and lung deposition is shown in Figure 2. Strong first-round consensus was reached for all items in this category of the questionnaire.
The relationship between the characteristics of the different types of inhalation devices was analyzed in a category of items that deepened in the specific features of DPI, pMDI and SMI device types, that are relevant for their use in the clinical practice, comparing some of them. A strong consensus was reached in the first round for 7 out of 12 statements in this category of the questionnaire (Figure 3). Among these, experts unanimously agreed on item 22. For the remaining 6 items different outcomes were obtained after the second round of consultation (Figure 5). For items 21 and 29 specifically, consensus was attained (strong and weak consensus respectively), after the experts were confronted with these items maintaining the same wording. However, the discrepancies observed in the first round for items 24 and 27 were not solved, despite rephrasing item 24- in 24a and 24b, and presenting item 27 to the panelists during the second round. Finally, item 30- was split in: 30a and 30b, leading to a weak consensus for item 30a and to discrepancy for item 30b.
The degree of consensus on the recommendations for the choice and use of inhaler devices in clinical practice with respect to inspiratory flow and lung deposition in inhaled therapy is shown in Figure 4. The panelists unanimously agreed that it is essential to ensure correct knowledge of the device and the inhalation manoeuvre by the patient before using the device (item 31). The rest of the items in this category obtained a strong consensus, highlighting the need to consider the inspiratory flow or inspiratory capacity, both when the inhalation device is selected and periodically, to ensure its suitability for the patient. Additionally, since item 35 – (DPIs should not be used in patients with low inspiratory flows [< 30 L/m]), attained weak consensus in the first round of consultation, it was included in the second one (Figure 5).
Finally, the second round of the Delphi panel led to consensus in 4 items where an agreement below 70% was obtained during the first round (Figure 5). These included items: 21, strong consensus; 29 and 30a, weak consensus; and item 35, strong consensus.
Discussion
Current Spanish and international guidelines on COPD (GesEPOC and GOLD; Global Initiative for COPD), devote little attention to the features of inhalation device types in relation with inspiratory flow and lung deposition. Given the absence of previous recommendations and the scarce scientific evidence available on the topic, FIDEPOC, the first study to follow a Delphi methodology with the participation of a broad panel of COPD expert pulmonologists to address this issue was carried out. The FIDEPOC study has identified eight consensus recommendations (items 31–38) for the selection and use of devices for inhalation therapy in COPD patients, considering inspiratory flow and lung deposition.
The experts unanimously recommended the need to ensure correct knowledge of the device and the inhalation manoeuvre by the patient before use (item 31). In this regard and in relation to the presence of comorbidities in COPD patients, specifically the presence of cognitive impairment, the panelists agreed that this difficulty is one of the main limitations of the use of pMDIs devices (item 20), and that the use of inhalation chambers is important to improve lung deposition in patients with coordination difficulties (item 18). Therefore, pMDIs should be used together with a chamber in patients with coordination problems (item 22). In line with the consensus, conventional pMDIs achieve a highly variable pulmonary deposition range from 8% to 53%,20–24 that can increase to 11–68% with the use of an inhalation chamber or a spacer.22,25–30
Regarding the identification of characteristics of the different inhalation device types related to inspiratory flow and lung deposition, the panelists agreed that the inhalation devices need an adequate inspiratory flow (specific for each device) to reach maximum lung deposition (item 12), and that the internal resistance of the different devices determines the need for a higher or lower inspiratory flow (item 13). In line with these consensus, inspiratory flow has been related to effective drug deposition in inhaled therapy in the management of other respiratory pathologies such as asthma31 It was thus agreed to recommend that inspiratory flow or inspiratory capacity should be considered in the choice of a particular inhaler device (item 32), and that the inspiratory flow or inspiratory capacity should be assessed periodically to ensure the suitability of the inhaler device used (item 33). In fact, the periodical assessment of these two functional parameters is further supported by the variable progression associated with COPD patients, as some patients follow a relatively stable course, while others experience severe disease progression.32
The experts also agreed to recommend that, in the absence of inspiratory flow or inspiratory capacity measurement, the internal resistance of the devices should be assessed to ensure that it matches the required inspiratory flow needs (item 37). Two factors that would determine the inspiratory flow needed in each inhaler are the internal resistance, which is specific to each device and will generate a specific turbulence, and the unbundling of the drug, in the case of DPIs33,34 Therefore, the patient must generate a certain inspiratory flow to overcome this resistance and achieve adequate inhalation.2,35 According to the expert’s consensus, not all COPD patients are able to generate the minimum inspiratory flow needed (item 28). Therefore, as a guideline for action on the use of DPIs, the expert panelists agreed to recommend the use of active devices (pMDI or SMI) in patients with low inspiratory flow (item 36) and not to use DPI-type devices in these same patients (item 35). Likewise, there was strong consensus with the recommendation, the use of DPIs should be re-evaluated in patients with severe obstruction and severe exacerbations (item 34). In this respect, the panelists also agreed that the need to generate a high inspiratory flow for the activation of certain devices favours the impact of drug particles in the upper airways to the detriment of sedimentation in the peripheral airway (item 14).
The last recommended guideline agreed-upon by the panelists regarding the characteristics of the devices is that the exit velocity and particle size of the different devices should be considered to ensure adequate lung deposition (item 38). As a matter of fact, there is evidence linking airway deposition of inhaled drugs to the patient’s inspiratory flow, aerosol velocity and the particle size of the inhaled drug.31,36,37 On one hand, experts agreed that the higher the emission velocity generated by the devices, the higher the probability of upper airway impact (item 17). In line with this assertion, compared to pMDIs and DPIs, the SMI device generates a fine, slow-moving mist that could reduce oropharyngeal deposition.38 Indeed, scintigraphic analyses with the SMI device indicated that, compared to a pMDI with a hydrofluoroalkane propellant, lung deposition is higher (up to 50%) and oropharyngeal deposition lower.39 Furthermore, this slower release rate of around 1.2 seconds in SMI compared to 0.1 seconds in traditional pMDIs could largely reduce the effect of poor coordination between device activation and inhalation.11 Moreover, the greater stability of cloud emission in SMIs is likely to contribute to easier and more comfortable use for patients.39 Accordingly, the panelists agreed that an SMI is preferable to a pMDI because of the aerosol exit velocity (slower) and particle size (higher proportion of fine particles) that favour greater lung deposition (item 25). On the other hand, the experts panel agreed that particle size, or MMAD (mass median aerodynamic diameter), is a determining factor in achieving proper lung deposition (item 15), and that particle size greater than 5 µm limits particle deposition to the small airways and alveoli (item 16). In line with the expert consensus, it has been observed that the distribution of deposition sites of inhaled particles is highly dependent on their aerodynamic diameters.40 According to a recent SLR, MMAD for conventional pMDIs range from 1.22 to 8 μm and from 1.19 to 3.57 μm when using a valved holding chamber or spacer, and from 0.72 to 2.0 μm with Modulite®. The DPIs produce medium particle sizes (1.8–4.8 μm), while with the SMI type 60% of the particles reach an MMAD <5 μm.2
Finally, although the FIDEPOC study has allowed the definition of eight consensus recommendations for the choice and use of inhaler devices in the management of COPD, it has limitations. First, the wording of some of the items proposed to the experts may have influenced the degree of discrepancy among them due to categorical statements or lack of specificity. Additionally, there are specific concepts related to the pathophysiology of COPD and its influence on inspiratory flow and lung deposition, and the physical characteristics of inhaler devices, that are complex and for which more medical literature and evidence dissemination are needed in national and international COPD management guidelines.
Conclusion
First, the high degree of consensus on most of the items included in the FIDEPOC study demonstrates the importance given by COPD pulmonologists to the inspiratory flow and lung deposition in inhaled therapy, and their relevance in the choice of inhalation device. Several factors influence inspiratory flow and lung deposition. Among them, the experts highlight COPD pathophysiology, disease course and inhaler device characteristics.
Second, SMI devices would be of choice in patients with lower inspiratory flow due to the combination of a low emission velocity and an adequate particle size which, in turn, would increase lung deposition. In this regard, it is recommended to re-evaluate the use of DPIs, as experts agreed that not all COPD patients are able to generate the minimum inspiratory flow required for the use of these devices. This is especially important in patients with severe exacerbations, as these may affect inspiratory flow and lung deposition.
Finally, the FIDEPOC study has highlighted the absence of recommendations on inhaler devices specificities in national or international COPD management guidelines. To endorse the choice of the best inhaler device in each clinical situation, it would be necessary to generate quality literature on the devices, given that there are notable differences between them which are relevant to COPD management. Therefore, it is highly pertinent to include in COPD guidelines, recommendations regarding: the pathophysiology of COPD and its influence on inspiratory flow and lung deposition, the physical characteristics of inhalation devices and action guidelines for the choice of device according to the severity and phenotype of the patient.
Ethical Considerations
Due to the nature of the study that does not include research with people or animals it was not necessary to review by an ethics committee.
Acknowledgments
The authors would like to thank María Fontanals and Marc Sendra (Ampersand Consulting) for their contribution in the Delphi consensus and for their help in the nominal group meeting. We also would like to thank the expert pulmonologists that constituted the Delphi panel for their key contribution to this study: Beatriz Abascal Bolado (Hospital Marqués de Valdecilla, Cantabria), Bernardino Alcázar Navarrete (Hospital de Loja, Granada), Tamara Alonso Pérez (Hospital Universitario de la Princesa, Madrid), María Soledad Alonso Viteri (Hospital de Torrejón de Ardoz, Madrid), Carlos Amado Diago (Hospital de Liencres, Cantabria), Rosanel Amaro Rodríguez (Hospital Clínic, Barcelona), Antonio Pablo Arenas Vacas (Hospital Reina Sofía, Córdoba), María Jesús Avilés Inglés (Hospital Reina Sofía, Murcia), Nuria Avisbal Portillo (Hospital Virgen De La Victoria de Málaga), Javier Berraondo Fraile (Hospital Joan March, Palma de Mallorca), Carlos Cabrera (Hospital Negrín, Las Palmas de Gran Canaria), Myriam Calle Rubio (Hospital Clínico San Carlos, Madrid), Francisco Javier Callejas González (Hospital Universitario de Albacete), Santiago Carrizo Sierra (Hospital Miguel Servet, Zaragoza), Javier Cruz Ruiz (Hospital Universitario de Albacete), Javier de Miguel Díez (Hospital Gregorio Marañón, Madrid), Luis Miguel Domínguez Juncal (Complejo Hospitalario Universitario, A Coruña), Cristóbal Esteban González (Hospital de Galdakao, Vizkaya), Sergio Fandos Lorente (Hospital de Alcañiz, Aragón), Juan Marco Figueira Gonçalves (Hospital Virgen de la Candelaria, Tenerife), Federico Fiorentino (Hospital Son Espases, Palma de Mallorca), Raúl Galera Martíne (Hospital La Paz, Madrid), César García de Llanos (Hospital Doctor Negrín, Las Palmas), José Manuel García Pazos (Hospital Clínico de Santiago de Compostela), Raúl Godoy Mayoral (Hospital Universitario de Albacete), Rafael Golpe Gómez (Hospital Lucus Augusti, Lugo), Hugo Gómez Márquez (Complejo Hospitalario Universitario de Ourense), Carolina María Gotera Rivera (Hospital Fundación Jiménez Díaz, Madrid), José Luis Izquierdo Alonso (Hospital de Guadalajara), José Luis López-Campos Bodineau (Hospital Virgen del Rocío, Sevilla), Abigail Macias Paredes (Hospital de Calella, Barcelona), Pedro Jorge Marcos Rodríguez (Complejo Hospitalario Universitario A Coruña), Francisco Marín Sánchez (Hospital Virgen de la Victoria, Málaga), Miguel Ángel Martín Pérez (Hospital Reina Sofía, Córdoba), Patricia Mata Calderón (Hospital de Ciudad Real), Luis Mateos Caballero (Hospital de Mérida, Badajoz), Francisco Javier Michel de la Rosa (Hospital de Donostia, Guipúzcoa), Concepción Montón Soler (Hospital Parc Taulí, Sabadell), Concepción Morales (García Hospital Virgen de las Nieves, Granada), Elsa Naval Sendra (Hospital de la Ribera, Valencia), Gerardo Pérez Chica (Hospital de Jaén), Alicia María Pérez Rodríguez (Hospital de Tenerife), Ana Pueyo Bastida (Hospital de Burgos), Jacinto Ramos González (Hospital de Salamanca), Cristina Represas Represas (Hospital Álvaro Cunqueiro, Vigo), Juan Antonio Riesco Miranda (Hospital San Pedro de Alcántara, Cáceres), Tomás Ruiz Albi (Hospital de Valladolid), Antonio José Ruiz Reina (Hospital Juan Ramón Jiménez, Huelva), Leonardo Ernesto Saldaña Pérez (Hospital Universitario de Getafe), Sergio Salgado Aranda (Hospital Universitario del Tajo, Aranjuez), Raúl Sandoval Contreras (Hospital San Juan (Alicante), Jaime Signes-Costa (Hospital Clínico, Valencia), Patricia Sobradillo Ecenarro (Hospital de Cruces, Bilbao), Antonia Dolores Soto Venegas (Hospital San Juan de la Cruz, Úbeda), Esther Verdejo Mengual (Hospital General Universitario de Valencia), Felipe Villar Álvarez (Hospital Fundación Jiménez Díaz, Madrid) and Joaquín Vizcaino Ricoma (Hospital Poniente, Almería).
Funding
The project was sponsored by Boehringer-Ingelheim Spain. Boehringer-Ingelheim had no role in the design of the study, the collection, analysis, and interpretation of the data, and the writing of the manuscript. The authors received no direct compensation related to the development of the manuscript. Boehringer Ingelheim was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Disclosure
Dr. Baloira has received speaker fees from: Boehringer Ingelheim, GSK, Novartis, AstraZeneca and Chiesi, and research grants from GSK, AstraZeneca and Novartis. Dr. González-Torralba has received speaker fees in several congresses and scientific sessions from: Boehringer Ingelheim, GSK, Novartis, AstraZeneca, Chiesi, Pfizer, Esteve and Rovi. Dr. J. L. García-Rivero has received speaker fees from: Novartis, GSK, Boehringer-Ingelheim, AstraZeneca, Chiesi, ALK, Teva, Menarini, Viso and Sanofi; and consulting fees from Novartis, GSK, AstraZeneca, Teva, Boehringer-Ingelheim, ALK, Viso, Gebro and Sanofi. Dr. Marta Palop has received fees from: Boehringer-Ingelheim, Novartis, AstraZeneca, GSK, Gebro, Sanofi and MSD. The other authors declare no conflicts of interest directly or indirectly related to the manuscript contents.
References
1. Lim KE, Kim SR, Kim HK, Kim SR. Symptom clusters and quality of life in subjects with COPD. Respir Care. 2017;62:1203–1211. doi:10.4187/respcare.05374
2. Baloira A, Fuster A, Luis J, et al. Lung deposition and inspiratory flow rate in patients with chronic obstructive pulmonary disease using different inhalation devices: a systematic literature review and expert opinion. Int J COPD. 2021;16:1021–1033. doi:10.2147/COPD.S297980
3. Soriano JB, Abajobir AA, Abate KH, et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet Respir Med. 2017;5:691–706. doi:10.1016/S2213-2600(17)30293-X
4. WHO. Mortality and global health estimates. Glob Heal Obs World Heal Organ; 2020. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates.
5. Miravitlles M, Calle M, Molina J, et al. Actualización 2021 de la Guía Española de la EPOC (GesEPOC). Tratamiento farmacológico de la EPOC estable. Arch Bronconeumol. 2021. doi:10.1016/j.arbres.2021.03.005
6. López-Campos JL, Gallego EQ, Hernández LC. Status of and strategies for improving adherence to COPD treatment. Int J COPD. 2019;14:1503–1515. doi:10.2147/COPD.S170848
7. García-río F, Soler-cataluña JJ, Alcazar B, Viejo JL, Miravitlles M. Requirements, strengths and weaknesses of inhaler devices for COPD patients from the expert prescribers’ point of view: results of the EPOCA delphi consensus. COPD. 2017;14:573–580. doi:10.1080/15412555.2017.1365120
8. Sorino C, Negri S, Spanevello A, Visca D, Scichilone N. Inhalation therapy devices for the treatment of obstructive lung diseases: the history of inhalers towards the ideal inhaler. Eur J Intern Med. 2020;75:15–18. doi:10.1016/j.ejim.2020.02.023
9. Lavorini F, Corrigan CJ, Barnes PJ, et al. Retail sales of inhalation devices in European countries: so much for a global policy. Respir Med. 2011;105:1099–1103. doi:10.1016/j.rmed.2011.03.012
10. Usmani OS. Choosing the right inhaler for your asthma or COPD patient. Ther Clin Risk Manag. 2019;15:461–472. doi:10.2147/tcrm.s160365
11. Lavorini F, Fontana GA, Usmani OS. New inhaler devices - The good, the bad and the ugly. Respiration. 2014;88:3–15. doi:10.1159/000363390
12. Heyder J. Deposition of inhaled particles in the human respiratory tract and consequences for regional targeting in respiratory drug delivery. Proc Am Thorac Soc. 2004;1:315–320. doi:10.1513/pats.200409-046TA
13. Rossi A, Aisanov Z, Avdeev S, et al. Mechanisms, assessment and therapeutic implications of lung hyperinflation in COPD. Respir Med. 2015;109:785–802. doi:10.1016/j.rmed.2004.04.010
14. Broeders MEAC, Molema J, Hop WCJ, Vermue NA, Folgering HTM. The course of inhalation profiles during an exacerbation of obstructive lung disease. Respir Med. 2004;98:1173–1179. doi:10.1016/j.rmed.2004.04.010
15. Hohmann E, Brand JC, Rossi MJ, Lubowitz JH. Expert opinion is necessary: Delphi panel methodology facilitates a scientific approach to consensus. Arthroscopy. 2018;34:349–351. doi:10.1016/j.arthro.2017.11.022
16. Linstone HA, Turoff M. The Delphi method: techniques and applications. Electronic version. Newark: Information Systems Department College of Computing Sciences New Jersey Institute of Technology; 2002. DOI:10.2307/3150755.
17. Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32:1008–1015. doi:10.1046/j.1365-2648.2000.t01-1-01567.x
18. de Meyrick J. The Delphi method and health research. Health Educ. 2003;103:7–16. doi:10.1108/09654280310459112
19. Soler-Cataluña JJ, Cosío B, Izquierdo JL, et al. Documento de consenso sobre el fenotipo mixto EPOC-asma en la EPOC. Arch Bronconeumol. 2012;48:331–337. doi:10.1016/j.arbres.2011.12.009
20. Newman SP, Morén F, Pavia D, Little F, Clarke SW. Deposition of pressurized suspension aerosols inhaled through extension devices. Am Rev Respir Dis. 1981;124:317–320. doi:10.1164/arrd.1981.124.3.317
21. Steed KP, Towse LJ, Freund B, Newman SP. Lung and oropharyngeal depositions of fenoterol hydrobromide delivered from the prototype III hand-held multidose respimat nebuliser.1 the respimat device was formerly known as the Bineb.1. Eur J Pharm Sci. 1997;5:55–61. doi:10.1016/S0928-0987(96)00016-4
22. Vidgren MT, Paronen TP, Kärkkäinen A, Karjalainen P. Effect of extension devices on the drug deposition from inhalation aerosols. Int J Pharm. 1987;39:107–112. doi:10.1016/0378-5173(87)90204-3
23. Leach CL, Davidson PJ, Hasselquist BE, Boudreau RJ. Lung deposition of hydrofluoroalkane-134a beclomethasone is greater than that of chlorofluorocarbon fluticasone and chlorofluorocarbon beclomethasone: a cross-over study in healthy volunteers. Chest. 2002;122:510–516. doi:10.1378/chest.122.2.510
24. De Backer W, Devolder A, Poli G, et al. Lung deposition of BDP/formoterol HFA pMDI in healthy volunteers, asthmatic, and COPD patients. J Aerosol Med Pulm Drug Deliv. 2010;23:137–148. doi:10.1089/jamp.2009.0772
25. Ashworth HL, Wilson CG, Sims EE, Wotton PK, Hardy JG. Delivery of propellant soluble drug from a metered dose inhaler. Thorax. 1991;46:245–247. doi:10.1136/thx.46.4.245
26. Gillen M, Forte P, Svensson JO, et al. Effect of a spacer on total systemic and lung bioavailability in healthy volunteers and in vitro performance of the Symbicort(®) (budesonide/formoterol) pressurized metered dose inhaler. Pulm Pharmacol Ther. 2018;52:7–17. doi:10.1016/j.pupt.2018.08.001
27. Rahmatalla MF, Zuberbuhler PC, Lange CF, Finlay WH. In vitro effect of a holding chamber on the mouth-throat deposition of QVAR (hydrofluoroalkane-beclomethasone dipropionate). J Aerosol Med. 2002;15:379–385. doi:10.1089/08942680260473452
28. Richards J, Hirst P, Pitcairn G, et al. Deposition and pharmacokinetics of flunisolide delivered from pressurized inhalers containing non-CFC and CFC propellants. J Aerosol Med. 2001;14:197–208. doi:10.1089/08942680152484126
29. Newman SP, Weisz AW, Talaee N, Clarke SW. Improvement of drug delivery with a breath actuated pressurised aerosol for patients with poor inhaler technique. Thorax. 1991;46:712–716. doi:10.1136/thx.46.10.712
30. Newman SP, Pitcairn GR, Adkin DA, Vidgren MT, Silvasti M. Comparison of beclomethasone dipropionate delivery by easyhaler dry powder inhaler and pMDI plus large volume spacer. J Aerosol Med. 2001;14:217–225. doi:10.1089/08942680152484144
31. Usmani OS, Biddiscombe MF, Barnes PJ. Regional lung deposition and bronchodilator response as a function of β2-agonist particle size. Am J Respir Crit Care Med. 2005;172:1497–1504. doi:10.1164/rccm.200410-1414OC
32. Shaw JG, Vaughan A, Dent AG, et al. Biomarkers of progression of chronic obstructive pulmonary disease (COPD). J Thorac Dis. 2014;6:1532–1547. doi:10.3978/j.issn.2072-1439.2014.11.33
33. Hira D, Koide H, Nakamura S, et al. Assessment of inhalation flow patterns of soft mist inhaler co-prescribed with dry powder inhaler using inspiratory flow meter for multi inhalation devices. PLoS One. 2018;13:e0193082. doi:10.1371/journal.pone.0193082
34. Azouz W, Chrystyn H. Clarifying the dilemmas about inhalation techniques for dry powder inhalers: integrating science with clinical practice. Prim Care Respir J. 2012;21:208–213. doi:10.4104/pcrj.2012.00010
35. Clark A. Peak inspiratory conditions in healthy volunteers implications for in vitro testing. J Aerosol Med Pulm Drug Deliv. 1993;6:99–110.
36. Al-Showair RAM, Tarsin WY, Assi KH, Pearson SB, Chrystyn H. Can all patients with COPD use the correct inhalation flow with all inhalers and does training help? Respir Med. 2007;101:2395–2401. doi:10.1016/j.rmed.2007.06.008
37. Verbanck S, Kalsi HS, Biddiscombe MF, et al. Inspiratory and expiratory aerosol deposition in the upper airway. Inhal Toxicol. 2011;23:104–111. doi:10.3109/08958378.2010.547535
38. Iwanaga T, Kozuka T, Nakanishi J, et al. Aerosol deposition of inhaled corticosteroids/long-acting β2-agonists in the peripheral airways of patients with asthma using functional respiratory imaging, a novel imaging technology. Pulm Ther. 2017;3:219–231. doi:10.1007/s41030-017-0036-4
39. Brand P, Hederer B, Austen G, Dewberry H, Meyer T. Higher lung deposition with respimat® soft mistTM inhaler than HFA-MDI in COPD patients with poor technique. Int J COPD. 2008;3:763–770. doi:10.2147/COPD.S3930
40. Fernández Tena A, Casan Clarà P. Depósito pulmonar de partículas inhaladas. Arch Bronconeumol. 2012;48:240–246. doi:10.1016/j.arbres.2012.02.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Recent Exacerbation History on the Efficacy of Once-Daily Single-Inhaler Fluticasone Furoate/Umeclidinium/Vilanterol Triple Therapy in Patients with Chronic Obstructive Pulmonary Disease in the FULFIL Trial
Panettieri Jr RA, Camargo CA Jr, Cheema T, El Bayadi SG, Fiel S, Vila TM, Jain RG, Midwinter D, Thomashow B, Ludwig-Sengpiel A, Lipson DA
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2043-2052
Published Date: 1 September 2022
Plasma Extracellular Vesicle miRNA Profiles Distinguish Chronic Obstructive Pulmonary Disease Exacerbations and Disease Severity
O'Farrell HE, Bowman RV, Fong KM, Yang IA
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2821-2833
Published Date: 4 November 2022
Use of Remote Cardiorespiratory Monitoring is Associated with a Reduction in Hospitalizations for Subjects with COPD
Polsky M, Moraveji N, Hendricks A, Teresi RK, Murray R, Maselli DJ
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:219-229
Published Date: 3 March 2023
Anti-IL5/IL5R Treatment in COPD: Should We Target Oral Corticosteroid-Dependent Patients?
Laroche J, Pelletier G, Boulay M, Côté A, Godbout K
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:755-763
Published Date: 5 May 2023
Exacerbations and Real-World Outcomes After Single-Inhaler Triple Therapy of Budesonide/Glycopyrrolate/Formoterol Fumarate, Among Patients with COPD: Results from the EROS (US) Study
Strange C, Tkacz J, Schinkel J, Lewing B, Agatep B, Swisher S, Patel S, Edwards D, Touchette DR, Portillo E, Feigler N, Pollack M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2245-2256
Published Date: 12 October 2023