Back to Journals » Open Access Emergency Medicine » Volume 14
Characteristics and Outcomes of Mechanically Ventilated Patients at Adult ICU of Selected Public Hospitals in Addis Ababa, Ethiopia
Authors Alemayehu M ![]() , Azazh A, Hussien H, Baru A
, Azazh A, Hussien H, Baru A ![]()
Received 14 April 2022
Accepted for publication 27 July 2022
Published 2 August 2022 Volume 2022:14 Pages 395—404
DOI https://doi.org/10.2147/OAEM.S369752
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Micheal Alemayehu,1,2 Aklilu Azazh,2 Heyria Hussien,2 Ararso Baru3
1Department of Emergency and Critical Care, Tiruneshi Beijing General Hospital, Addis Ababa, Ethiopia; 2Department of Emergency Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Nursing, College of Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Micheal Alemayehu, Email [email protected]
Introduction: Mechanical ventilation is the primary method of supporting organ function for patients admitted to intensive care units (ICU). The information on the characteristics and outcomes of patients requiring mechanical ventilation is essential to understanding the causes of mortality among mechanically ventilated patients. However, the available literature in developing countries, including Ethiopia, is limited.
Objective: The objective of this study was to assess the characteristics and outcomes of mechanically ventilated patients in adult intensive care units in selected public hospitals, in Addis Ababa, Ethiopia, from 2019 to 2020.
Methods: An institutional-based cross-sectional study design was employed. All adult patients who were mechanically ventilated and admitted to ICU for at least 24 hours between July 2019 and July 2020 were included in the study. The collected data were evaluated with SPSS version 26 software. Multiple logistic regression models were used to indicate the association between dependent and independent variables. The variables, which have an independent association with poor outcomes, were identified with a p-value less than 0.05.
Results: Of 180 mechanically ventilated patients, 98(54.4%) were male. The main reason for ventilation was respiratory failure. The mean duration of stay on the ventilator was 7.09± 6.06, and the mortality rate in mechanically ventilated patients was 41.7%. The mortality rate was higher in patients with cardiac diseases 43(57.70%). Inotropic use, not taking sedation, and length of stay on a mechanical ventilator were independently associated with mortality.
Conclusion: The mortality rate of mechanically ventilated patients in the selected public hospitals was high. The clinicians must strive to balance the necessity and benefit of sedation use with the potential to negatively affect the patient outcome. In addition, the risk:benefit assessment of ventilation must be done for all patients requiring ventilator support.
Keywords: mechanical ventilation, intensive care unit, characteristics, outcome, Ethiopia
Background
The number of patients requiring intensive care is increasing worldwide. Many of these patients need mechanical ventilation.1 Mechanical ventilation is the essential strategy of supporting organ function in patients treated in intensive care units (ICUs) and has become emblematic of the ICU since its use has resulted in the development of intensive care units and the establishment of intensive therapy as a separate medical area.2
The fundamental objectives of mechanical ventilation are to improve pulmonary gas exchange and relieve respiratory distress, thus facilitating lung and airway healing while at the same time lessening the risk for iatrogenic complications.3
Despite its importance, patients who are put on ventilators are prone to preventable complications like ventilator-associated pneumonia, pneumothorax, pulmonary embolism, and atelectasis.4 A chart review study done in southern India and Egypt, Cairo, also found that a higher mortality rate among ventilated patients, which were 67.21% and 64%, respectively. Patient management and pre‑mechanical ventilation factors were found to be independently associated with increased mortality.5,6
Understanding the characteristics of the mechanically ventilated patients such as the indication for mechanical ventilation, the ventilator management strategy, techniques used to identify patients capable of ventilator discontinuation, management of the interaction between weaning and sedation, and the outcome of the patient may help minimize both complications and resource consumption during mechanical ventilation.7,8
Most studies on the characteristics and outcome of ventilator support were usually carried out in high-income countries, and very little contemporary data from low-income countries are available.9,10 Therefore, this study aimed at assessing the characteristics and outcomes of mechanically ventilated patients at adult ICUs of selected public hospitals in Addis Ababa.
Methods
Study Design and Study Period
An institutional-based cross-sectional study was employed through a review of patients’ medical cards, which were admitted from July 2019 to July 2020.
Study Setting
The study was conducted in Addis Ababa, which is the capital city of Ethiopia, and the seat of the African Union. The city encompasses 40 private hospitals and 14 public hospitals. Of the 14 public hospitals, 4 were excluded from the study. Due to Ethiopia’s Tigray war, two of them were providing services for combat injuries and were closed for research (national security issue), and the other hospitals were excluded due to lack of ICU service. The study was conducted in three randomly selected public hospitals in the city. These are Menelik II Hospital, Yekatit 12 Hospital, and St. Paul Hospital, where they provide ICU services for critically ill patients.
Study Participants
The source population was all patients who were admitted to adult ICU in selected public hospitals during the stated period. Eligibility criteria included being the age greater than 18 and being mechanically ventilated for at least 24 hours. Incomplete recording and lost charts were excluded from the study.
Sample Size Determination
A single population proportion formula was used to calculate the sample size (n) by considering the following statistical assumptions; the prevalence of mortality among mechanically ventilated patients was 28.6 which was taken from a study conducted at Ayder comprehensive specialized hospital, Ethiopia.11 The level of confidence (α) was set at 0.05 (Z (1-α) = 1.96) and the margin of error was taken as 0.05. Consequently, the calculated sample size adjusted with 10% consideration for the non-response rate was 202.
where n = Minimum sample size for a statistically significant survey
Z = Standard normal deviate at 95% confidence interval two-tailed test is; = 1.96
P = proportion of ICU mortality rate for patients under mechanical ventilation taken as 28.6%,
q = 1-p, d = margin of error taken as 5% = 0.05
Sampling Procedures
The three public hospitals were selected by simple random sampling. Then, to select the study participants from each hospital, the proportional allocation formula was used based on caseloads. There were 450 mechanically ventilated patients admitted to the selected hospitals (154 from Yekatiti 12 hospital, 120 from Menelik II hospital, and 176 from Saint Paul Hospital) from July 8, 2019 to July 7, 2020. After that, medical records of mechanically ventilated adult patients were taken from the identified cards in each hospital; a simple random sampling technique was applied to select the study participants.
Data Collection Techniques and Instrument
Data was collected from the study population using a structured data abstraction tool adapted from different works of literature5,11,12 based on the elements intended to study.
The charts were reviewed based on the questions created to measure the characteristics of mechanically ventilated patients. These variables are defined as what was male-to-female ratio, the age of mechanically ventilated patients, how (in what mode), what was their initial diagnosis while admission to ICU, what was their main indication, what access to the airway was employed, type of sedation used and for how long adult patients used the mechanical ventilator and what was the main complications they developed and also the method of weaning from a mechanical ventilator. And also, did the patient develop acute respiratory distress syndrome (ARDS), sepsis, and multiple organ dysfunction syndromes (MODS) during the mechanical ventilation period. In this study, the outcome is interpreted as a patient after mechanical ventilation whether survived or not survived. This dichotomous measure was coded 1= for not survived, 0 if otherwise.
Data Quality Assurance
A properly designed and structured data extraction tool was used. Data collectors were given 2 days of training and closely supervised during data collection and entry. The data collectors were health professionals, who hold a master of science in Emergency Medicine and Critical care nursing, for better understanding and interpretation of the patients’ medical charts. The pre-test was carried out in Tirunesh Beijing Hospital to check the completeness and clarity of the tool. And some parts of the collection tool were revised and adjusted.
Data Entry, Processing, and Analysis
Clean-up and cross-checking of data were done before analysis. Data were checked for completeness and coded manually and entered into EpiData version 4.6 for validation. Then, exported to SPSS version 26 for analysis. Descriptive statistics such as frequency and percentage were used to summarize the data while tables and graphs were used for the presentation of the data. Purposive selections of the variable with a p-value of <0.25 on bivariate analysis were considered to identify factors associated with outcomes of the ventilated patient. A multivariable logistic regression model was fitted to control the possible effect of confounders. Finally, the variables which have an independent association with poor outcomes were identified and reported with OR, with 95% CI and a p-value less than 0.05.
Ethical Consideration
The ethical clearance was obtained from Addis Ababa University College of Health Sciences Department of Emergency Medicine and Addis Ababa Regional Health Bureau. Informed consent was obtained from all hospitals before proceeding with data collection from charts. This was done after a clear description of the objectives of the study and its procedures. Additionally, the confidentiality of all the data to be gained was respected. This study also complies with the Declaration of Helsinki. Confidentiality was ensured by not mentioning patients’ names in the questionnaire, and unauthorized individuals were not allowed to access the data that were collected by using a password-protected computer.
Results
Socio-Demographic Characteristics of Ventilated Adult Patients
From 202 randomly selected mechanically ventilated patients, admitted from July 2019 to July 2020, 22 patients were excluded from the analysis because their charts were incomplete or could not be located. So, 180 (89.1%) patients were included in this study. The majority 107(59.4%) of the participants were between 18 and 40 years. The mean and standard deviation age of respondents was 42.2±18.1 years with a minimum of 18 years and a maximum of 92 years. More than half of the patients were male 98(54.4%) (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Mechanically Ventilated Adult Patients in Selected Public Hospital ICU (n=180) 2021 |
Characteristics of Mechanically Ventilated Patients
Categories and Source of Admission to ICU
Of the total of 180 ventilated patients, the majority [123(68.3%)] of them had medical illnesses, while 42(23.3%) had a surgical illnesses. Regarding the source of ICU admission, the majority were from Emergency [94(52.2%)], followed by inpatient wards [57(37.1%)], operation room [23(12.1%)], and 6(3.3%) were from other hospitals. Regarding the reason for admission, 56(31.1%) had respiratory problems, followed by neurologic (18.4%), and cardiac (11%). The readmission rate was 8.3% (Table 2).
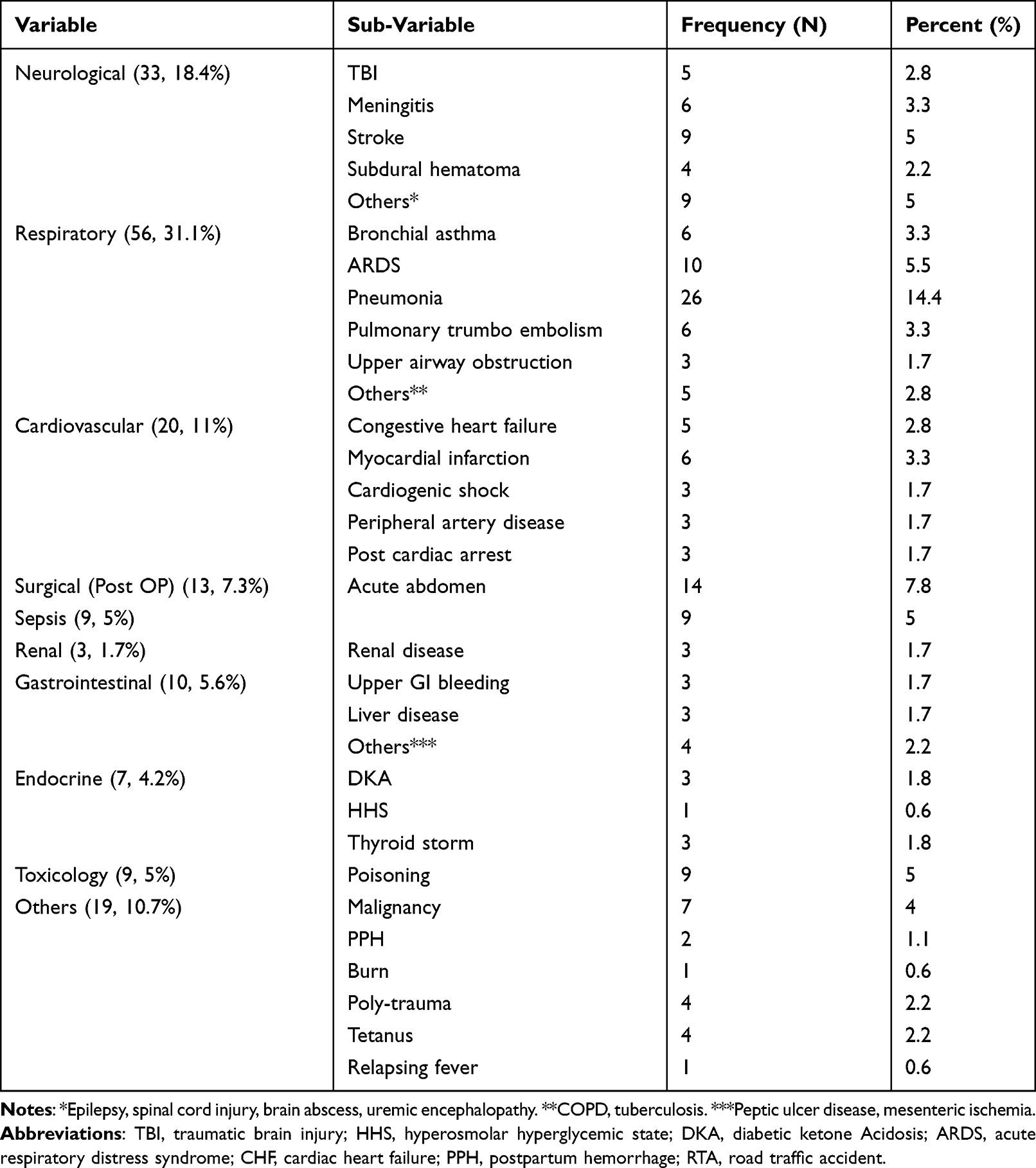 |
Table 2 Clinical Diagnosis of Patients in MV, of Selected Public Hospitals, 2021 |
Indication and Initial Mode of Mechanical Ventilation
Respiratory failure and Airway protection were the major indications for mechanical ventilation in this study representing 86(47.8%) and 75(41.7%), respectively. Other indications included cardiovascular failure (shock) [17(9.4%)] and neuromuscular disease [2(1.1%)]. Access to the airway used were ETT [179(98.9%)] and tracheostomy [2(1.1%)]. Various modes of ventilation strategy used in ICU and the frequency of each mode are as follows: The most commonly utilized initial ventilator modes were A/C VCV [92(51.1%)], followed by (A/C PCV [42(23.3%)], SIMV [35(19.4%)], and CPAP [9(5%)].
Comorbidity and GCS at Admission
Of the total study population, 78(43.3%) patients had comorbidity. Hypertension [26(14.4%)] and diabetes mellitus [18(10%)] were the most common comorbidities followed by HIV/AIDS [14(7.8%)], tuberculosis [6(3.3%)], CHF [9(5%)], stroke [5(2.8%)] and others [7(5.6%)]. From the physical examination, the GCS of patients at admission was ≤8 in 68(37.8%), 9–12 in 48(26.7%) and for the remaining 64(35.6%) patients GCS was from 13 to 15.
Length of Stay
The mean and standard deviation length of stay of respondents in the hospital was 16.85± 19.737, in ICU was 10.04 ±10.242, and on a mechanical ventilator was 7.09±6.06. The majority of the patients stay in hospital (75%) and ICU (50%) for more than 7 days. On the other hand, the majority of the patients stay on a mechanical ventilator for 4–7 days (Figure 1). In our study, those with Neuromuscular cases as a reason for ventilation had a longer duration on the ventilator (13.50 ± 2.121) followed by toxicology cases (11.13 ± 10.934), sepsis (8.56 ± 5.175), GI diseases (8.44 ± 7.418), and neurologic disease (7.87 ± 6.224).
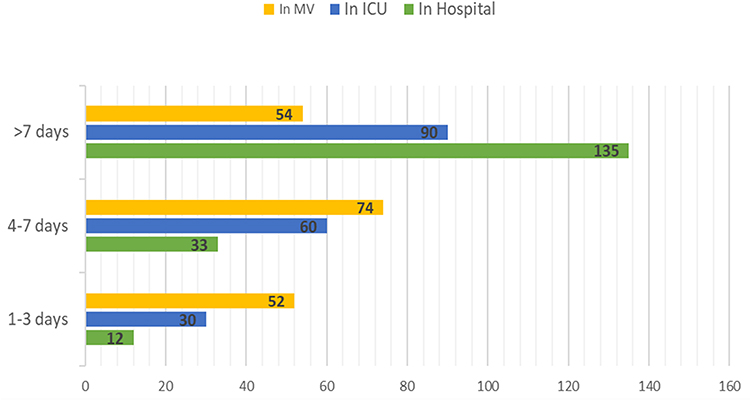 |
Figure 1 Length of stay in the hospital, ICU, and on mechanical ventilator of ventilated adult patients in selected public hospitals, ICU, Addis Ababa Ethiopia, 2021. |
The Sedation Used and Weaning Methods
Of 180 patients who were on MV 150 (83.3%) used sedative drugs. Among them, more than half (53.8%) were sedated using Diazepam followed by ketamine (25.3%), Propofol (9.1%), and thiopental 4(1.6%). The weaning methods used for the improved patients were CPAP [54 (53.5%)], T-tube trial [23(22.7%)], and PS with CPAP [24(23.8%)]. In this study, 4(4%) of the survived patients accidentally extubated themselves.
Complications
Of the total study participants, 40(22.2%) had developed mechanical ventilation-related complications. Of which, ventilator-associated pneumonia was developed in 27(15%) patients; pneumothorax in 6(3%) patients, emphysema and post-extubation stridor each account for 3(1.7%) patients, and other complications account for 7(3.8%)
Organ Failure and Other Characteristics
From the total of 180 ventilated patients, more than half 122(67.8%) developed at least one organ failure. Forty-nine (27.2%) developed multi-organ dysfunction syndrome. Of these, 59(32.8%) developed cardiac, 48(26.7%) renal, 51(28.3%) neurological, 15(8.3%) hematologic and 13(7.2%) hepatic failure. Acute respiratory distress syndrome was seen in 24(13.3%) of the patients. Regarding inotropic drug use, 74(41.1%) patients were on ionotropic support, ulcer and DVT prophylaxis were used by 118(65.6%), and 136(75.6%) of them, respectively. For 13(7.2%) patients, cardiopulmonary resuscitation procedures were performed before they were admitted to the intensive care unit.
Outcome
Among the total study participants, 105(58.3%) survived and 75(41.7%) dead. Sepsis was the leading cause of death 35(46.67%). The mortality rate was higher in patients with cardiac diseases [43(59%)], followed by respiratory disease (48%). The mortality rate was 57.7% in patients ventilated for 1–3 days, 44% in patients who stayed for more than 7 days on mechanical ventilation, and 28.37% for patients ventilated for 4–7days.
Factors Associated with the Outcome of Mechanically Ventilated Patients Admitted at ICU
In bivariate logistic regression analysis GCS level, readmission status, sepsis, cardiovascular failure, length of stay in ICU, length of stay on MV, CPR before admission, inotropic use, multi-organ dysfunction syndrome (MODS), and sedation used were eligible for multivariable regression.
In multivariable regression analysis, length of stay on MV, inotropic use, GI prophylaxis use, and not taking sedation were statistically positively associated with mortality at a p-value of less than 0.05 but the other variables were not found statistically significant. The probability of mortality for those who stay in a mechanical ventilator for more than 7 days is greater than by 19.2%(OR, 0.192; 95% CI, 0.040–0.926) as compared to those who stay for 4–7 days. The odds of mortality for those who hadreceived sedation is higher by 3.951 times (OR, 3.951; 95% CI, 1.035–15.089) as compared to those who have taken sedatives. The odds of those who took inotropes mortality were 17.5 times more likely (OR, 17.5; 95% CI, 4.652–65.959) than those who have not taken inotropes (Table 3).
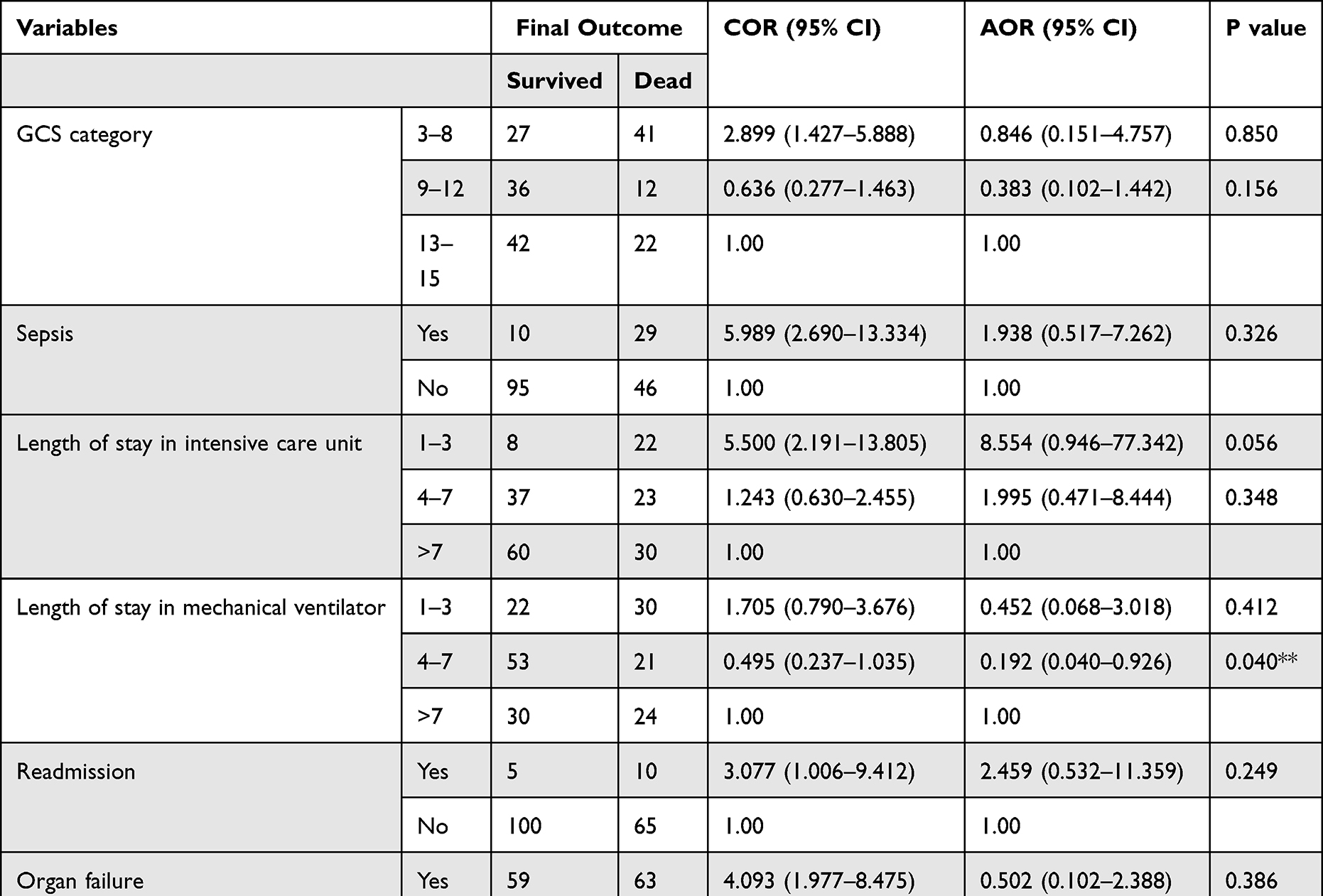 |
Table 3 Logistic Regression Analysis of Associated Factors with the Outcome of Mechanically Ventilated Patients Among Adult ICU of Selected Hospitals, Addis Ababa, Ethiopia, 2021 |
Discussion
The use of a mechanical ventilator in patients admitted to ICU has been increasing. The data regarding the characteristics and outcome of the ventilated patient are vital since it allows better conveying the outcome to the patient’s family.13 This study assessed the characteristics and outcomes of mechanically ventilated adult patients admitted to the ICU of selected public hospitals in Addis Ababa.
In this study, the mean age was 42.2±18.1 years and 54.4% of them were males. This finding was similar to a study conducted in Maharashtra, India (43.22 years) and lower than studies done in western India (58.80 years) and chili (54.6 years).5,9,14 This may be due to the lower mean age of the Ethiopian population. The preponderance of male sex was similar to a study done in Brazil (52%).15
Respiratory failure was the main indication for mechanical ventilation in this study representing 47.8%. This finding was in line with other published studies in India, Chile, Nigeria, and Ethiopia, which ranged from 38.6% to 86.07%.5,9,11,16 Nevertheless, the study conducted in Cairo prevails cardiac disease as the predominant indication of mechanical ventilation. This discrepancy in indication might be due to the type of intensive care unit and the difference in the category of diseases in the setting.
More than half (51.1%) of the study participants were on (Assist control volume-controlled ventilation) A/C VCV as initial ventilator modes. Similarly, Tobi et al found volume-controlled ventilation (VCV) as the main (61.8%) initial ventilation strategy.6 On the other hand, the study conducted in India and Brazil indicates the predominant mode of initial ventilation (66% and 73%) was the PCV, and in Benin teaching hospital, Nigeria the preferred mode of ventilation was SIMV (52.3%) which is different from our study.5,15,17 The selection of initial ventilation strategy can be varying based on individual preferences and needs.
In this study, the mean duration of patients’ stay on mechanical ventilators and ICU was 7.09± 6.06 and 10.04 ± 10.242 days, respectively. Likewise, a multicenter study conducted in 19 Chilean ICUs showed that the Mean duration of MV and length of stay in ICU were 7.8±8.7 and 11.1± 14 days, respectively.19 The report from Nassar et al also showed that the duration of mechanical ventilation was 6±10 days, which is slightly similar to our study.6 However, the study from southern Brazil and Nigeria showed a higher mean duration of stay on mechanical ventilation which is 9.3 days and 12.3 days, respectively.15,17 The discrepancy in ventilator stay might be attributed to the late admission of patients.
Multi-organ dysfunction syndrome was found in 27.2% of the study participants. The organ failed were cardiac 59 (32.8%), neurological 51 (28.3%), renal 48 (26.7%), hematologic [15(8.3%)] and hepatic failure [13(7.2%)]. On contrary, the study conducted in southern Brazil shows higher multi-organ dysfunction (45%) and the organ failing were renal (26%), cardiovascular (20.4%), coagulopathy (18%), neurological (10%), and hepatic (7.7%). This might be due to the diagnostic capability and specialization of the ICU.
In this study, 22.2% of the study participants developed mechanical ventilation-related complications. Ventilator-associated pneumonia (15%) was the main complication. This finding is in line with the finding by Nassar et al in which 14.8% of the patients developed VAP as a major complication.6 However, the report from Berhe et al shows a higher VAP (27.6%) rate than our study.11 This might be due to better care in our study setting.
Weaning from the ventilator is the main issue in ICUs. The main weaning technique employed for the survived patients in this study was CPAP (51%) followed by a T-tube trial (22%). Our finding is different from the studies conducted in Chile and Egypt. In those studies, the preferred method of weaning were T-tube and PS-CPAP, respectively.6,9 The variation in the findings could be attributed to the preference of the physicians and the patient’s tolerance for both methods.
In the present study, the mortality among mechanically ventilated patients was 41.7%. The report from different published study shows 34% in Brazil, 42.1% in central India, 67.21% in western India, 31.8% in Nigeria, 64% in Egypt, 73.5% in Uganda and 28.6% in Ayder Hospital, Ethiopia.5,6,11,15,16,18,19 Our findings were almost the same as the study conducted by Chiwhane and Diwan, which reported 42.1%. On other hand, our finding was higher than the studies conducted in Brazil (34%), Nigeria (31.8%), and Ayder Hospital, Ethiopia (28.6%). The highest mortality in our study might be due to delayed admission to intensive care (due to delayed professional decision, lack of beds, and an inadequate number of a ventilator), late referral, and admission problems (admitting unsalvageable patients, lack of standardized illness severity scoring strategies). In this study, mortality rate was higher in patients with cardiac diseases (59%). Similarly, Nassar et al reported that the mortality rate was higher in patients with cardiac diseases.
The main factors independently associated with mortality in this study were the length of stay on the mechanical ventilator, inotropic use, and sedation use. Our findings are different from a study conducted in southern Brazil; Maharashtra, India; and Ayder, which reported that age, organ failures, ARDS, comorbidity, sepsis, length of stay on mechanical ventilation, and ICU stay were significantly associated with mortality.11,15,18 This difference might be due to the study design, sample size, and setup of the hospital.
Limitation of the Study
The findings in this study are subjected to some limitations. Since the nature of the study was retrospective, no direct intervention or direct observation of patients was done. The limited number of patients is also another limitation. Despite the limitations, this study has strengths. It is the first multicenter study on the characteristics and outcomes of mechanically ventilated patients in the adult ICU of Addis Ababa, possibly in Ethiopia. It also tried to incorporate most of the pertinent characteristics of mechanically ventilated patients.
Generalizability
The potential generalizability of the evidence generated by this study to other settings should be considered in view of the study setting, context, methods, and limitations described in this study.
Conclusion
The mortality rate of mechanically ventilated patients in the selected public hospitals was substantially high. Patients with cardiac diseases were found to have higher mortality rates. The main reason for admission was respiratory causes. Respiratory failure was the main indication for the initiation of mechanical ventilation. The main factors independently associated with mortality in this study were the length of stay on the mechanical ventilator, inotropic use, and not taking sedation. This suggests that clinicians must strive to balance the necessity and benefit of sedation use with the potential to negatively affect the patient outcome. In addition, the risk:benefit assessment of ventilation must be done for all patients requiring ventilator support.
Abbreviations
A/C, assist control; ARDS, acute respiratory distress syndrome; CPAP, continuous positive airway pressure; DVT, deep vein thrombosis; ETT, endotracheal tube; FIO2, fraction of inspired oxygen; GCS, Glasgow Coma Score; ICU, intensive care unit; MODS, multiple organ dysfunction syndromes; MV, mechanical ventilation; PEEP, peak end-expiratory pressure; PCV, pressure-controlled ventilation; PSV, pressure support ventilation; SIMV, synchronized intermittent mandatory ventilation; SPSS, Statistical Package for Social Sciences; VAP, ventilator-associated pneumonia; VCV, volume-controlled ventilation.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available without restriction.
Acknowledgments
My special thanks go to Addis Ababa University College of Health Science, Emergency Medicine, and Critical Care Department. I also place on record, my sense of gratitude to the data collectors, and all who directly and indirectly contributed their help to this research. This paper was uploaded to the Addis Ababa University repository as a thesis.20
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors would like to declare that funding was not received for this study. However, logistic expenses that covered duplication of the study tools, data collections, and transportation were covered by Addis Ababa University.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work
References
1. Carson SS, Cox CE, Holmes GM, Howard A, Carey TS. The changing epidemiology of mechanical ventilation: a population-based study. J Intensive Care Med. 2006;21(3):173–182. doi:10.1177/0885066605282784
2. Kacmarek RM. The mechanical ventilator: past, present, and future. Respir Care. 2011;56(8):1170–1180. doi:10.4187/respcare.01420
3. Pettenuzzo T, Fan E. 2016 Year in review: mechanical ventilation. Respir Care. 2017;62(5):629–635. doi:10.4187/respcare.05545
4. Lee HW, Cho Y-J. The impact of mechanical ventilation duration on the readmission to intensive care unit: a population-based observational study. Tuberc Respir Dis. 2020;83(4):303–311. doi:10.4046/trd.2020.0024
5. Khatib KI, Dixit SB, Joshi MM. Factors determining outcomes in adult patient undergoing mechanical ventilation: a “real-world” retrospective study in an Indian Intensive Care Unit. Int J Crit Illn Inj Sci. 2018;8(1):9–16. doi:10.4103/IJCIIS.IJCIIS_41_17
6. Nassar Y, Magdy M, Hamed L, Algohary T. A 5-year registry of mechanically ventilated patients comprising epidemiology, initial settings, and clinical outcome. Egypt J Chest Dis Tuberc. 2018;67:250. doi:10.4103/ejcdt.ejcdt_34_18
7. Tomicic V, Espinoza M, Andresen M, et al. Characteristics and factors associated with mortality in patients receiving mechanical ventilation: first Chilean multicenter study. Rev Med Chil. 2008;136(8):959–967.
8. Esteban A, Anzueto A, Alía I, et al. How is mechanical ventilation employed in the intensive care unit? An international utilization review. Am J Respir Crit Care Med. 2000;161(5):1450–1458. doi:10.1164/ajrccm.161.5.9902018
9. Peñuelas O, Frutos-Vivar F, Fernández C, et al. Characteristics and outcomes of ventilated patients according to time to liberation from mechanical ventilation. Am J Respir Crit Care Med. 2011;184(4):430–437. doi:10.1164/rccm.201011-1887OC
10. Needham DM, Bronskill SE, Sibbald WJ, Pronovost PJ, Laupacis A. Mechanical ventilation in Ontario, 1992–2000: incidence, survival, and hospital bed utilization of noncardiac surgery adult patients. Crit Care Med. 2004;32(7):1504–1509. doi:10.1097/01.CCM.0000129972.31533.37
11. Berhe E, Slassie K, Zeabher T. Clinical characteristics and outcomes of patients under invasive mechanical ventilation at Ayder comprehensive specialized hospital adult intensive care unit, Mekelle, Ethiopia. Eur Respir J. 2018;1:153.
12. Tsegaye N. Characteristics and outcome of mechanical ventilation in pediatric Addis Ababa University. J Health Sci. 2018;31:875.
13. Seneff MG, Wagner DP, Wagner RP, Zimmerman JE, Knaus WA. Hospital and 1-year survival of patients admitted to intensive care units with acute exacerbation of chronic obstructive pulmonary disease. JAMA. 1995;274(23):1852–1857. doi:10.1001/jama.1995.03530230038027
14. Yadav V, Jadhao GU, Salame RN. Aetiology and predictors of outcome of mechanically ventilated patients admitted in intensive care unit of a rural tertiary health care center. Int J Biomed Adv Res. 2018;9:265.
15. Fialkow L, Farenzena M, Wawrzeniak I, et al. Mechanical ventilation in patients in the intensive care unit of a general university hospital in southern Brazil: an epidemiological study. Clinics. 2016;71(3):145–151. doi:10.6061/clinics/2016(03)05
16. Ku T, It E, Mechanical CO. Ventilation in the intensive care unit: a prospective study of indications and factors that affect outcome in a tertiary hospital in Nigeria. Jo AnesClin Res. 2017;08(04). doi:10.4172/2155-6148.1000718
17. Tobi K, Ekwere I, Mechanical CO. Ventilation in the intensive care unit: a prospective study of indications and factors that affect outcome in a tertiary hospital in Nigeria. J Anaesth Clin Res. 2017;26(8):1–4.
18. Chiwhane A, Diwan S. Characteristics, outcome of patients on invasive mechanical ventilation: a single-center experience from central India. Egypt J Crit Care Med. 2016;4(3):113–118. doi:10.1016/j.ejccm.2016.10.003
19. Ttendo SS, Was A, Preston MA, Munyarugero E, Kerry VB, Firth PG. Retrospective Descriptive study of an intensive care unit at a Ugandan Regional Referral Hospital. World J Surg. 2016;40(12):2847–2856. doi:10.1007/s00268-016-3644-520
20. Alemayehu M. Characteristic and Outcomes of Mechanically Ventilated Patients at Adult ICU of Selected Public Hospitals in Addis Ababa, Ethiopia, 2021 [dissertation]. Addis Ababa: University of Addis Ababa; 2021. Available from: http://213.55.95.56/handle/123456789/28724. Accessed July 31, 2022.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Associated with the Outcome of a Pediatric Patients Admitted to Intensive Care Unit in Resource-Limited Setup: Cross-Sectional Study
Dendir G, Awoke N, Alemu A, Sintayhu A, Eanga S, Teshome M, Zerfu M, Tila M, Dessu BK, Efa AG, Gashaw A
Pediatric Health, Medicine and Therapeutics 2023, 14:71-79
Published Date: 2 March 2023
Determinants of Pneumothorax Among Mechanically Ventilated COVID-19 Intensive Care Unit Patients, a Single Centre Study
Hundie TG, Alemu ZA, Getachew LZ, Abera LA, Seyoum AB, Mogus LS, Admasu NM, Regassa GB, Tilahun YB, Bareamichael PI, Tessema AG, Derese TN
Journal of Multidisciplinary Healthcare 2023, 16:3977-3989
Published Date: 11 December 2023
Incidence and Predictors of Cardiac Arrest Among Patients Admitted to the Intensive Care Units of a Comprehensive Specialized Hospital in Central Ethiopia
Ashine TM, Heliso AZ, Babore GO, Ezo E, Saliya SA, Muluneh BB, Alaro MG, Adeba TS, Sebro SF, Hailu AG, Abdisa EN
Patient Related Outcome Measures 2024, 15:31-43
Published Date: 15 February 2024
Prevalence, Characteristics, and Treatment Pattern of Menstrual-Related Headache Among Undergraduate Health Sciences Students at Addis Ababa University, Ethiopia
Ali HE, Tadesse TA, Beyene DA, Gebremariam GT
International Journal of Women's Health 2024, 16:707-716
Published Date: 20 April 2024
Factors Influencing the Length of Emergency Intensive Care Unit Stay in Adult Tetanus Patients
Xu J, Wang Y, Huang G, Zhou L, Mo X, Yang N, Wu P, Hu S, She C
International Journal of General Medicine 2025, 18:1855-1864
Published Date: 31 March 2025