Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Factors Associated with the Outcome of a Pediatric Patients Admitted to Intensive Care Unit in Resource-Limited Setup: Cross-Sectional Study
Authors Dendir G ![]() , Awoke N
, Awoke N ![]() , Alemu A, Sintayhu A
, Alemu A, Sintayhu A ![]() , Eanga S, Teshome M, Zerfu M, Tila M, Dessu BK, Efa AG
, Eanga S, Teshome M, Zerfu M, Tila M, Dessu BK, Efa AG ![]() , Gashaw A
, Gashaw A ![]()
Received 22 September 2022
Accepted for publication 24 February 2023
Published 2 March 2023 Volume 2023:14 Pages 71—79
DOI https://doi.org/10.2147/PHMT.S389404
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Getahun Dendir,1 Nefsu Awoke,2 Afework Alemu,3 Ashagrie Sintayhu,1 Shamill Eanga,4 Mistire Teshome,2 Mahlet Zerfu,5 Mebratu Tila,1 Blen Kassahun Dessu,1 Amelework Gonfa Efa,3 Amanu Gashaw6
1School of Anesthesia, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 2School of Nursing, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 3School of Medicine, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 4College of Health Science and Medicine, Wolkite University, Wolkite, Ethiopia; 5School of Medicine, College of Health Science and Medicine, Yekatit 12 Medical College, Addis Ababa, Ethiopia; 6Department of Anesthesia, College of Health Science and Medicine, Hawassa University, Hawassa, Ethiopia
Correspondence: Afework Alemu, Tel +251 984570056, Email [email protected]
Background: Critical care is a multidisciplinary and interprofessional specialty devoted to treating patients who already have or are at danger of developing acute, life-threatening organ dysfunction. Due to the higher disease load and mortality from preventable illness, patient outcomes in intensive care units are challenging in settings with inadequate resources. This study aimed to determine factors associated with outcomes of pediatric patients admitted to intensive care units.
Methods: A cross-sectional study was conducted at Wolaita Sodo and Hawassa University teaching hospitals in southern Ethiopia. Data were entered and analyzed using SPSS version 25. Normality tests using the Shapiro–Wilk and Kolmogorov–Smirnov data were normally distributed. The frequency, percentage, and cross-tabulation of the different variables were then determined. Finally, the magnitude and associated factors were first analyzed using binary logistic regression and then multivariate logistic regression. Statistical significance was set at P < 0.05.
Results: A total of 396 Pediatric ICU patients were included in this study, and 165 (41.7%) deaths were recorded. The odds of patients from urban areas (AOR = 45%, CI 95%: 8%, 67% p-value = 0.025) were less likely to die than those in rural areas. Patients with co morbidities (AOR = 9.4, CI 95%: 4.5, 19.7, p = 0.000) were more likely to die than pediatric patients with no co-morbidities. Patients admitted with Acute respiratory distress syndrome (AOR = 12.86, CI 95%: 4.3, 39.2, p = 0.000) were more likely to die than those with not. Pediatric patients on mechanical ventilation (AOR = 3, CI 95%: 1.7, 5.9, p = 0.000) more likely to die than not mechanically ventilated.
Conclusion: Mortality of paediatric ICU patients was high (40.7%) in this study. Co-morbid disease, residency, the use of inotropes, and the length of ICU stay were all statistically significant predictors of death.
Keywords: outcome, paediatrics, intensive care unit, Wolaita, Ethiopia
Background
An intensive care unit (ICU) may be a hospital location where a higher concentration of staff with specialized training, drugs on hand, and monitoring tools enables more thorough and frequent interventions in critically ill patients. It is a multidisciplinary and inter-professional specialty devoted to providing excellent care for patients who have acute, life-threatening organ dysfunction or who are at risk of acquiring it.1–4
The concept of critical care was developed during the poliomyelitis epidemic in the 1920–1950s. Critical care services, with focused attention and expertise provided by medical and nursing staff for patients with multiorgan failure and life-threatening illness, have quickly spread worldwide.3 First, pediatric critical care units (PICU) were established in 1955 in Sweden. This unit treated children with pneumonia and sepsis by extending the knowledge added from the adult ICUs.2
The patient may need to be admitted to the intensive care unit (ICU) if their hemodynamic instability necessitates continuous vital sign monitoring, invasive hemodynamic monitoring, and rapid titration of intravenous medicine while being monitored, and respiratory assistance in the ICU. Critically ill and injured patients, especially in high-resource settings, may benefit greatly from this, both in terms of care quality and results.5,6
However, patient outcomes in an intensive care unit are challenging in resource-limited settings, where the burden of disease and mortality from treatable illnesses is at the top of resource-rich areas. Currently, critical care in low middle-income countries (LMICs) remains in its infancy in most hospitals. The majority of hospitals lack designated intensive care units, healthcare staff trained to worry about critically ill children, adequate number of staff, rapid guidelines and protocols, access to necessary medications, supplies, equipment, and institutional obstacles during the implementation of life-saving interventions.1,7
The primary factors that cause death in children under the age of five in poor nations, according to the World Health Organization, are both preventable and treatable. Since these factors have been shown to significantly reduce mortality and morbidity, improving outcomes are attainable with well-equipped and staffed critical care units. Numerous studies have shown the undeniable value of intensive care, which could lower death rates by 15% to 60%.8–11
Malnutrition (35.9%), tuberculosis (28.1%), malaria (10.2%), and human immunodeficiency virus (10.2%) were the leading causes of pediatric ICU admissions in low-resource countries. Respiratory and congenital heart diseases are the most common admissions in both resource-limited and resource-rich countries. The highest mortalities in both resource-limited and resource-rich countries were for respiratory, multi-organ failure, and cardiac reasons.7
In Forty-two of the world’s poorest nations, about 90% of the young children under the age of five who die each year worldwide dwell. These nations have a high prevalence of preventable and treatable diseases that result in numerous illnesses and injuries.12 According to a research done in Jimma and Mekele, Ethiopia, the mortality rates were 40% and 27%, respectively.13,14 A similar study carried out at Tanzania’s critical care units on patients of all ages found a death rate of 41.4%.5 The death rate in a study of patients with severe head injuries in the ICU of the National Hospital Abuja in Nigeria was 68.4%.15 The mortality rate was highest among patients with sepsis, according to studies done in Uganda and Mozambique’s intensive care units,16,17 while a study done in Nepal found that post-discharge mortality among children with infections was higher.18 Vasoactive medication use was found to be a predictor of mortality in a research from Rwanda.19
Death before discharge is a rare event in modern nations. It is challenging to provide aid and improve outcomes because there are limited data on children’s critical care in least developed nations. Additionally, there are issues with medications, oxygen, blood products, and monitoring equipment in Africa’s critical care for children. Because of this, critical care in low-income countries is of very poor quality.20–22
In a low-resource setup (including Ethiopia, particularly the southern part of the country), there are limited studies on the outcomes of pediatric patients admitted to an intensive care unit. Therefore, this study aimed to identify the contributing factors that affect the outcomes of pediatric patients admitted to the Wolaita Sodo University Teaching and Referral hospital (WSUTRH) intensive care unit.
Method
Study Design, Area and Period
This cross-sectional study was conducted at two teaching and referral hospitals in southern Ethiopia, namely, Hawassa University Specialized and Comprehensive Teaching Hospital (HUSCTH) and Wolaita Sodo University Comprehensive Teaching Hospital (WSUCTH), selected from teaching and referral hospitals in southern Ethiopia by lottery method.
HUSCH is located in southern Ethiopia, in the Sidama region and Hawassa town, 273 kilometers from Addis Ababa, the capital city. Currently, Hawassa town has one comprehensive specialized hospital, one regional hospital, and eight government health centers. HUSCH is a teaching hospital that provides services to more than five million people, including the Sidama region, southern nationalities, and the people of the neighboring zones and regions, including Oromia. The hospital has about 500 beds and 11 operating rooms. WSUCTH is situated in Sodo town, east of the town. It is 165km from Hawassa, SNNPR, and 396km from Addis Ababa, Ethiopia. It serves people in a catchment area of about 3.5–5 million, including the neighboring Dawuro Zone, Gamo Zone, Gofa Zone, and Kambata Tambaro Zone. The hospital has 350 functional beds with an average admission rate of 800 per month. The study was conducted from June 01, 2018 to May 31, 2020.
Population
We reviewed the registries and clinical charts of pediatric patients (≤18 years) admitted to intensive care unit. The source populations were charts of patients who were admitted to intensive care unit at HUSCTH and WSUTRH from June 01, 2018 to May 31, 2020. We consecutively reviewed all 396 pediatric patient charts admitted to ICU over two-year period.
Inclusion Criteria
- We included all paediatric patients who were admitted to ICU during the study period.
Exclusion Criteria
- We excluded patients with incomplete charts.
Data Collection Tools and Techniques
Data was collected by using a structured questionnaire regarding socio-demographic, clinical characteristics of the patients and treatment given during their stay at pediatric intensive care unit. Data was collected using a pretested checklist developed after reviewing various literature. Four trained anesthetists and 10 intensive care unit nurses collected the data for one-month duration. Using a patient’s card number, data collectors used a checklist to trace and collect data from all consecutive charts that met the inclusion criteria. Two supervisors were in charge of daily supervision.
Data Quality Control
The authenticity of the checklist was tested beforehand. Following the pretest, ambiguous words and order of questions were amended accordingly. Content validity was assured through proofreading and expert evaluation of the questionnaire. Data collectors and supervisors received intensive two-day training (one day theoretical and one day practical) on each item included in the study tools, as well as the study’s aims, relevance, and confidentiality of the information acquired. Throughout the data collection process, there was constant oversight and follow-up. To ensure its completeness and consistency, each datum was checked by the supervisors and members on a daily basis to maintain the quality of the data.
Data Processing and Analysis
The collected data were cleaned, coded, and entered into Epi-Data version 4.6 then exported and analyzed using SPSS version 25. Normality tests checked by using Shapiro–Wilk and Kolmogorov–Smirnov test, data were normally distributed. Then, the frequency, percentage, and cross-tabulation with different variables were determined. Finally, the magnitude and associated factors were analyzed using binary logistic regression and multivariate logistic regression. Variables with a P-value <0.25, binary logistic regression were included in a multivariate logistic regression, and variables with a p-value less than 0.05 were taken as statistically significant association.
Ethical Considerations
Ethical approval was first obtained from Wolaita Sodo University’s Ethical Review Board, with the ethical clearance approval letter reference number CRCSD 87/02/13. Then, a letter of cooperation was written to the administrations of Wolaita Sodo University Teaching and Referral Hospital (WSUTRH) and Hawassa University Specialized and Comprehensive Hospital (HUSCH). The Ethical Clearance Committee waived the requirement for informed consent in order to obtain data from patient medical records. By excluding names and identifiers from the checklist, participants’ confidentiality of information is ensured and we confirm that this manuscript complies with the Declaration of Helsinki.
Results
Socio-Demographic and Clinical Characteristics of Pediatric Patients
The death rate in this study, which included 396 pediatric ICU patients, was 41.7%. They had a 1.7:1 male-to-female ratio, with 250 (63.1%) males and 146 (36.7%) females. The majority 211 (53.3%) of the pediatric patients lived in urban areas. The majority 341 (86.1%) of the pediatric patients were of age older than two years. Most 293 (74%) of pediatric patients had an average stay of less than seven days. The mortality rate among 172 pediatric patients on mechanical ventilation was 61%, compared to a mortality rate of 26.8% for pediatric patients not on mechanical ventilation. The mortality rate was 71.8% among 78 pediatric patients who also had concomitant conditions. The majority of children admitted to the intensive care unit, 221 (55.7%), had an infection. The majority of pediatric patients were unconscious at the time of admission, 223 (56.3%) (Table 1).
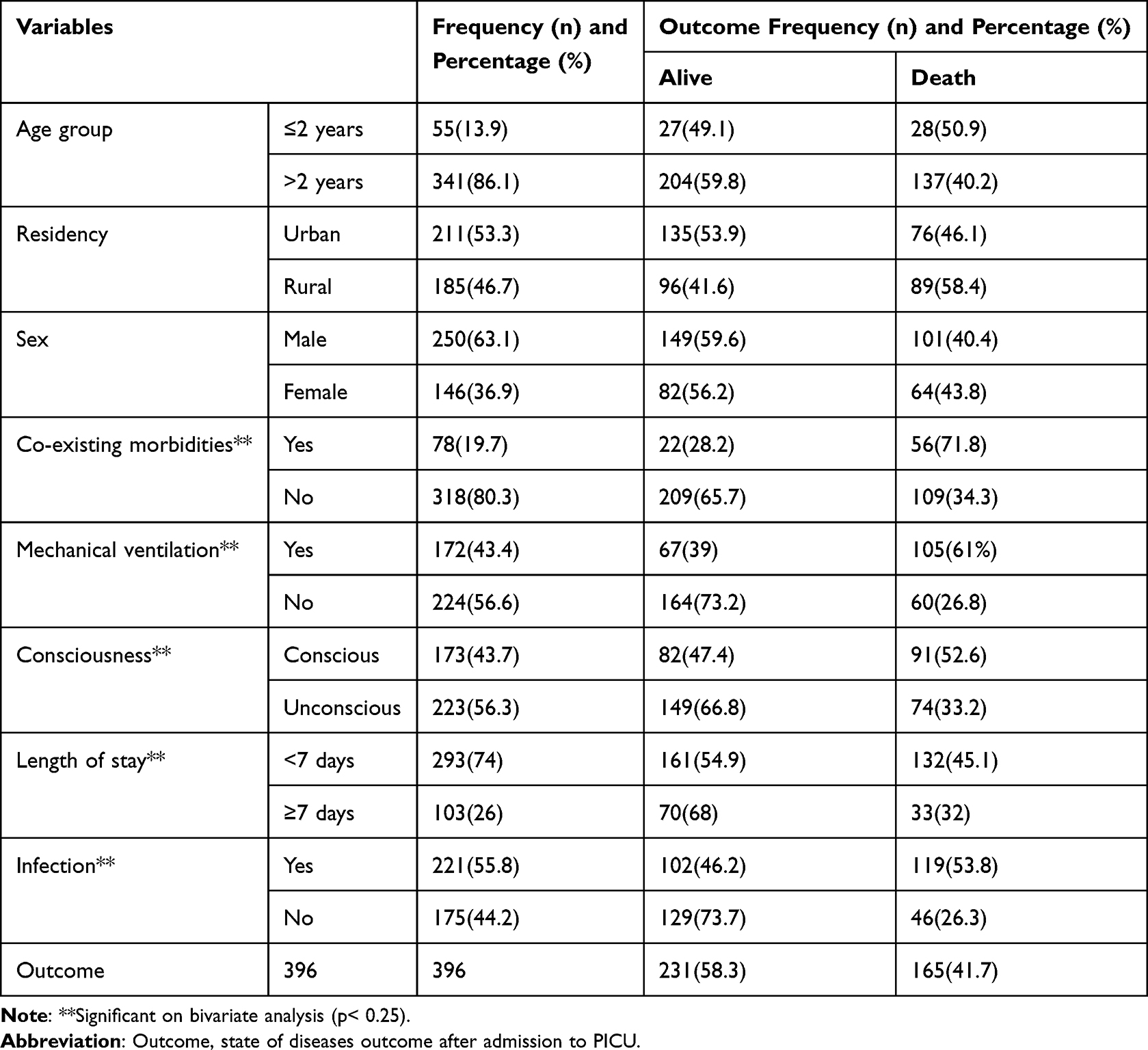 |
Table 1 Socio-Demographic and Clinical Characteristics of Pediatric Patients Admitted to the Intensive Care Unit of Wolaita Sodo and Hawassa University Teaching and Referral Hospital, 2020 |
Diagnosis of a Pediatric Patient Admitted to the Intensive Care Unit
The majority of pediatric patients admitted to the intensive care unit (ICU) were admitted due to various types of surgery 84 (21.2%), with meningitis 63 (15.9%) and Guillain-Barre syndrome 57 (14.4%). The mortality rate for patients with ARDS was 17 (77.3%), sepsis was 12 (66.7%), and meningitis was 35 (55.6%), respectively (Table 2).
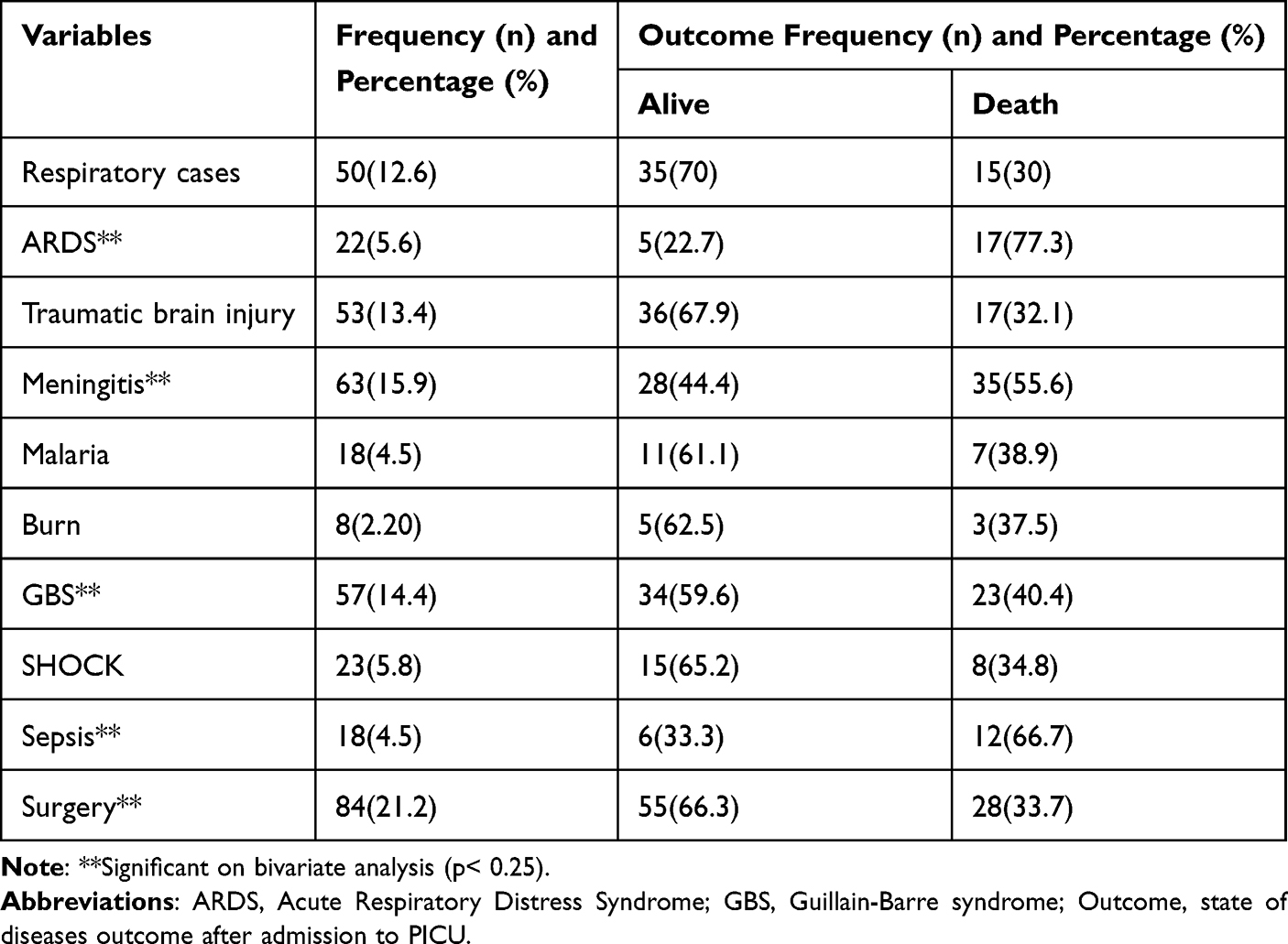 |
Table 2 Diagnosis of Pediatric Patients Admitted to the Intensive Care Unit of Wolaita Sodo and Hawassa University Teaching and Referral Hospital, 2020 |
Treatment Given Intensive Care Unit
All pediatric patients admitted to an intensive care unit were given antibiotics, and the majority of patients were given respiratory support 377 (95.2%) and blood transfusion 78 (19.7%) (Table 3).
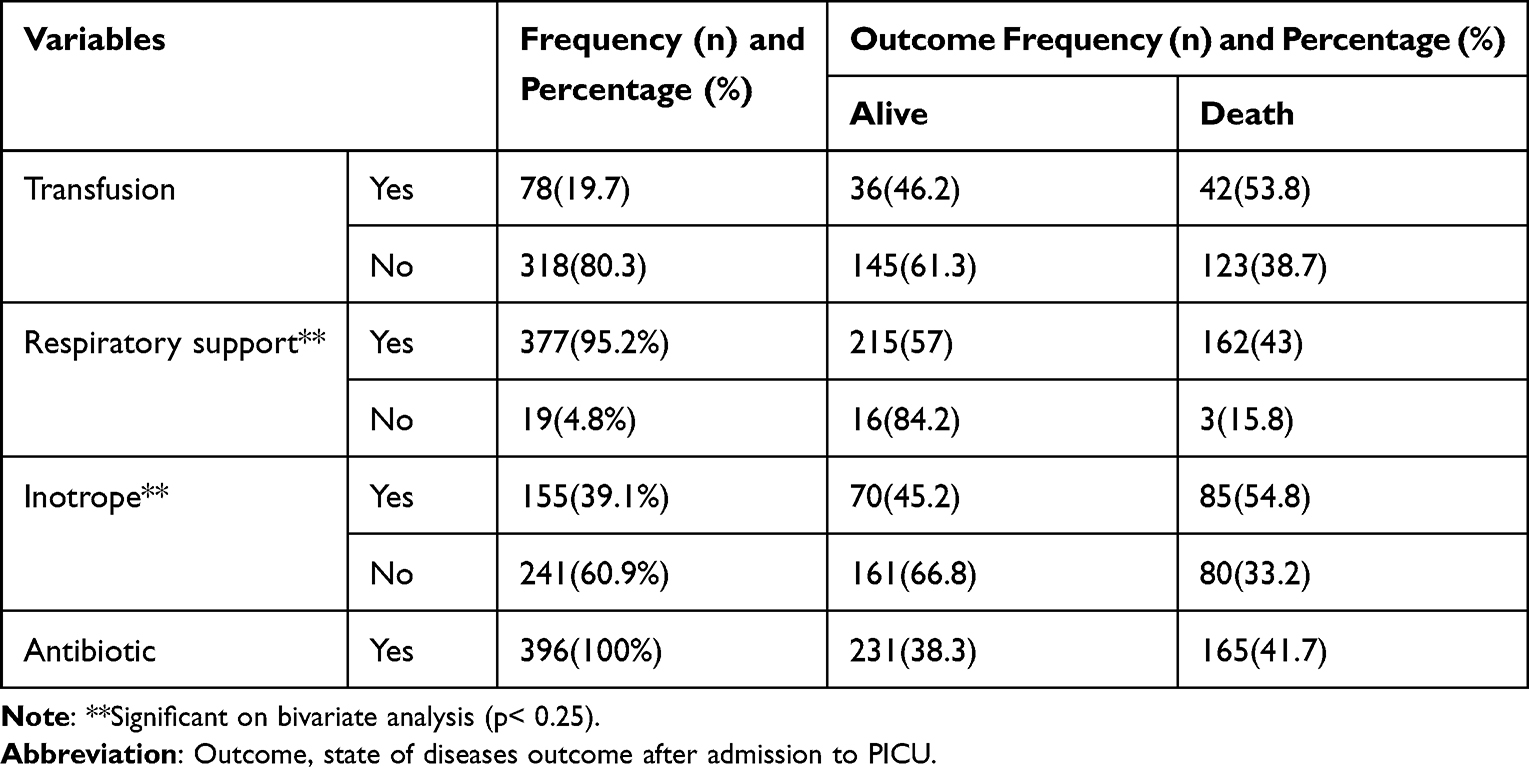 |
Table 3 Treatment Given Intensive Care Unit Wolaita Sodo and Hawassa University Teaching and Referral Hospital, 2020 |
Factors Associated with Outcome of a Pediatric Patients Admitted to an Intensive Care Unit
The results of multivariable logistic regression showed that different factors are associated with mortality of pediatric patients in intensive care unit. The odds of pediatric patients admitted to urban area (AOR = 45%, CI 95%: 8%, 67% p-value = 0.025) less likely died than rural. Odds of pediatric patients with comorbidity were more likely died (AOR = 9.4, CI 95%: 4.5, 19.7 p-value = 0.000) than patients with no co-morbidities. Pediatric patients admitted with Acute respiratory distress syndrome (AOR = 12.86 CI 95%: 4.3, 39.2 p-value = 0.000) more likely died than non-acute respiratory distress syndrome patients. Pediatric patients on mechanical ventilation (AOR = 3, CI 95%: 1.7, 5.9 p-value = 0.00) more likely died than not mechanically ventilated.
Meningitis patients were 3.5 times (AOR = 3.56, CI 95%: 1.5, 8.7) more likely to die than non-meningitis patients (p-value = 0.005). Pediatric patients who stayed for more than seven days were 2.8 times (AOR = 2.8, CI 95%: 1.5, 5.11 p-value = 0.00) more likely to die than those who stayed for less than seven days. Pediatric patients with infection were 1.9 times more likely to die (AOR = 1.94, CI 95%: 1.096, 3.44 p-value = 0.00) than non-infectious patients. Pediatric patients who received inotropes were 2.5 times more likely to die (AOR = 2.5, CI 95%: 1.4, 4.4 p-value = 0.00) than those who did not receive inotropes (Table 4).
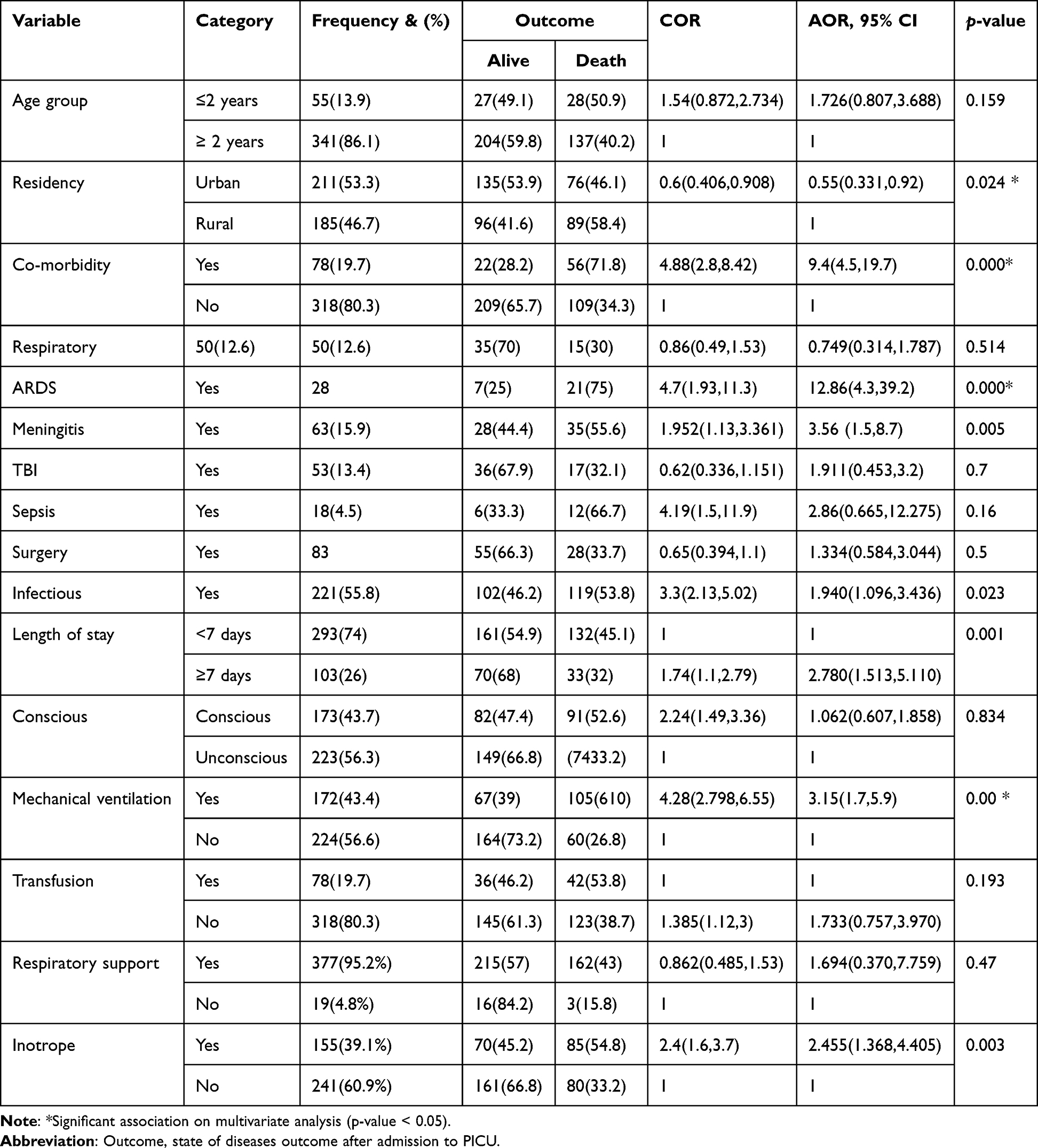 |
Table 4 Factors Associated with Outcome of Pediatric Patients Admitted to the Intensive Care Unit of Wolaita Sodo and Hawassa University Teaching and Referral Hospital, 2020 |
Discussion
This study looked at treatment outcomes and associated factors in pediatric patients admitted to the PICU. The PICU is a special unit that focuses on the care of critically ill patients. In order to achieve a positive outcome, all aspects of patient management must be thoroughly understood.23 A pediatric intensive care unit’s goal is to prevent death by closely monitoring and treating critically ill children who are considered to be at higher risk of death.
According to the findings of this study, the most common reasons for admission to the tertiary care center’s PICU were cardiovascular, neurological, and respiratory illnesses. Patients who require technical assistance, such as mechanical ventilation or intrusive monitoring, are eligible for admission to the facility.24 Along with post-surgical patients needing critical care, patients who are critically ill but treatable and need care outside of the general wards are covered.
The majority of the children admitted to this study (86.1%) were over the age of two. This finding is consistent with previous research in Ethiopia25,26 and Mozambique.16 A similar study in India found a different result than ours, in which more than 50.7% of the participants were infants.27
Furthermore, a majority of 84 (21.2%) of the pediatric patients in our study were admitted to the intensive care unit for post-operative treatment, which is the second most prevalent reason for admission in Singaporean studies after pulmonary reasons (21.7%).28 On top of that septic shock (27.14%) and respiratory disorders (20.9%) were the most prevalent causes, according to this study’s findings, which differ from those of similar studies conducted in Ethiopia at various points in time.26,29 According to a research done in India, cardiovascular illness accounted for 41.1% of admissions.27 Due to poor health seeking habits and the nation’s low socioeconomic status, the bulk of admissions for post-operative care may be explained by patients seeking care later in the course of their illness when complications require surgical interventions.
For 396 pediatric intensive care patients, the mortality rate was 165 (41.7%). Seventeen ARDS patients (or 77.3% of them) had the highest case fatality rate. This result is in line with other PICU studies that have been conducted in Ethiopia and have found mortality rates between 40% and 44%.13,26 The death rate was 2%, 2.1%, and 4.5%, respectively, in similar studies conducted in India, Singapore, and Switzerland, but the findings were different.27,28,30 Given that most families live in rural areas of the country with inadequate infrastructure and that most arrive at hospitals with advanced stages of illness after consulting traditional healers before going there, the disparity in mortality rates may be the result of a delay in seeking medical attention by the families of the children. Additionally, there are other potential factors, including a subpar referral system, a shortage of skilled medical professionals, and subpar infection prevention and control procedures in the PICU.
Additionally, our results show that children with comorbidity had a 9.4 times higher mortality risk than children without comorbidity. The chance of mortality among patients with co-morbidities ranges between 8.38 and 10%, according to studies done in Ethiopia.25,26 This conclusion is consistent to other studies’ findings. This result contrasts with that of a Dutch study, which indicated that individuals with co-morbid illnesses had a 3.3-fold higher mortality risk than those without co-morbidities.31 When compared to middle- and high-income countries, pediatric patients in developing nations had a comparatively poor nutritional status and eating habits, which put them at risk for illnesses linked to inadequate nutrition. Another contributing cause is the inadequate standard of care in the pediatric ICU.
In this study, patients who were receiving mechanical ventilation had a threefold higher risk of passing away than those who were not. According to a research conducted in Gondar, Ethiopia, patients who require MV have a death rate that is 2.36 times greater than those who do not,32 and this result is in line with that finding. In a similar vein, an Italian study indicated that patients who did not require MV had a better likelihood of surviving after being admitted to the PICU (100% vs 26.1%, P 0.001).33
In our study, pediatric patients who stayed for more than or equal to seven days were three times more likely to pass away than those who stayed for fewer than seven days. This result is analogous to research from Jimma, Ethiopia, which reported a high mortality rate in patients who stayed for more than 28 days13 and Iran, which discovered a 2.49 times higher mortality rate in patients who stayed for longer than a week.34 Our findings may be explained by the fact that patients who stay in the hospital for a long time are more likely to develop hospital-acquired infections.
According to our study, children who used inotropes had a 2.5-fold higher risk of passing away than children who did not. Other research done in Rwanda and India revealed that patients who needed inotrope support died at rates that were 12 and 8 times greater than those who did not.19,35 It is probable that this is the case because inotropes are frequently utilized for critically ill individuals with hemodynamic instability.
Limitation
While this study has many strengths, it also has some limitations. The charts provide an incomplete history, including neonatal history of co-morbidities. In this study, the cross-sectional study design does not reveal a cause–effect relationship.
Conclusion and Recommendation
ARDS is the most common cause of death for pediatric patients referred to the intensive care units of Wolaita Sodo and Hawassa University Teaching and Referral Hospital, with a mortality rate of 40.7%. In this study, the likelihood of concurrent disease, residency, the need for mechanical ventilation, the use of inotropes, and the length of ICU stay were all statistically significant predictors of death. As shown in this study, the mortality rate in the pediatric intensive care unit was very high, necessitating additional research, benchmarking, and intervention. We would like to suggest that all governmental and nonprofit partners cooperate to raise community awareness of the benefits of early medical attention and to improve the caliber of PICU services. To reduce potential biases, we like to advise the researchers to take into account a multi-centered prospective study.
Ethics Approval
Ethical approval was first got from the Ethical Clearance Committee of Wolaita Sodo University Teaching and Referral Hospital. Then, a letter of cooperation was written to both hospital administrations. Participants’ confidentiality of information was assured by excluding names and identifiers in the checklist.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors declare that they have no competing interests.
References
1. Diaz JV, Riviello ED, Papali A, Adhikari NKJ, Ferreira JC. Global critical care: moving forward in resource-limited settings. Ann Glob Health. 2019;85(1):1. doi:10.5334/aogh.2413
2. Epstein D, Brill JE. A history of pediatric critical care medicine. Pediatr Res. 2005;58(5):987–996. doi:10.1203/01.PDR.0000182822.16263.3D
3. Marshall JC, Bosco L, Adhikari NK, et al. What is an intensive care unit? A report of the task force of the world federation of societies of intensive and critical care medicine. J Crit Care. 2017;37:270–276.
4. Schell CO, Wärnberg MG, Hvarfner A, et al. The global need for essential emergency and critical care. Crit Care. 2018;22(1):284.
5. Sawe HR, Mfinanga JA, Lidenge SJ, et al. Disease patterns and clinical outcomes of patients admitted in intensive care units of tertiary referral hospitals of Tanzania. BMC Int Health Hum Rights. 2014;14(1):1–8.
6. Randolph AG, Gonzales CA, Cortellini L, Yeh TS. Growth of pediatric intensive care units in the United States from 1995 to 2001. J Pediatr. 2004;144(6):792–798.
7. Tripathi S, Kaur H, Kashyap R, Dong Y, Gajic O, Murthy S. A survey on the resources and practices in pediatric critical care of resource-rich and resource-limited countries. J Intensive Care. 2015;3(1):40.
8. Earle M, Natera OM, Zaslavsky A, et al. Outcome of pediatric intensive care at six centers in Mexico and Ecuador. Crit Care Med. 1997;25(9):1462–1467.
9. Gemke R, Bonsel GJ, van Vught AJ. Long-term survival and state of health after paediatric intensive care. Arch Dis Child. 1995;73(3):196–201.
10. Butt W, Shann F, Tibballs J, et al. Long-term outcome of children after intensive care. Crit Care Med. 1990;18(9):961–965. doi:10.1097/00003246-199009000-00011
11. Young M, Birkmeyer J. Potential reduction in mortality rates using an intensivist model to manage intensive care units. Effect Clin Pract. 2000;3:6.
12. Kissoon N. Out of Africa—A motherʼs journey. Pediatr Crit Care Med. 2011;12(1):73–79. doi:10.1097/PCC.0b013e3181ce74ef
13. Abebe T, Girmay M, Michael G, Tesfaye M. The epidemiological profile of pediatric patients admitted to the general intensive care unit in an Ethiopian university hospital. Int J Gen Med. 2015;8:63. doi:10.2147/IJGM.S76378
14. Haftu H, Hailu T, Medhaniye A, G/tsadik T. Assessment of pattern and treatment outcome of patients admitted to pediatric intensive care unit, Ayder Referral Hospital, Tigray, Ethiopia, 2015. BMC Res Notes. 2018;11(1):339. doi:10.1186/s13104-018-3432-4
15. Adudu O, Ogunrin O, Adudu O. Morbidity and mortality patterns among neurological patients in the intensive care unit of a tertiary health facility. Ann Afr Med. 2007;6(4):4. doi:10.4103/1596-3519.55701
16. Punchak M, Hall K, Seni A, et al. Epidemiology of disease and mortality from a PICU in Mozambique. Pediatr Crit Care Med. 2018;19(11):e603. doi:10.1097/PCC.0000000000001705
17. Kwizera A, Dünser M, Nakibuuka J. National intensive care unit bed capacity and ICU patient characteristics in a low income country. BMC Res Notes. 2012;5(1):1–6. doi:10.1186/1756-0500-5-475
18. Giri S, Halvas-Svendsen T, Rogne T, et al. Pediatric patients in a local nepali emergency department: presenting complaints, Triage and post-discharge mortality. Glob Pediatr Health. 2020;7:2333794X20947926. doi:10.1177/2333794X20947926
19. Nyirasafari R, Corden MH, Karambizi AC, et al. Predictors of mortality in a paediatric intensive care unit in Kigali, Rwanda. Paediatr Int Child Health. 2017;37(2):109–115. doi:10.1080/20469047.2016.1250031
20. Jones S, Rantell K, Stevens K, et al. Outcome at 6 months after admission for pediatric intensive care: a report of a national study of pediatric intensive care units in the United Kingdom. Pediatrics. 2006;118(5):2101–2108. doi:10.1542/peds.2006-1455
21. Dünser MW, Baelani I, Ganbold L. A review and analysis of intensive care medicine in the least developed countries. Crit Care Med. 2006;34(4):1234–1242. doi:10.1097/01.CCM.0000208360.70835.87
22. Okafor U. Challenges in critical care services in Sub-Saharan Africa: perspectives from Nigeria. Indian J Crit Care Med. 2009;13(1):25.
23. Downes JJ. Development of pediatric critical care medicine—how did we get here and why? In: Science and Practice of Pediatric Critical Care Medicine. Springer; 2009:1–28.
24. Chaboyer W, James H, Kendall M. Transitional care after the intensive care unit: current trends and future directions. Crit Care Nurse. 2005;25(3):16–28.
25. Haftu H, Hailu T, Medhaniye A. Assessment of pattern and treatment outcome of patients admitted to pediatric intensive care unit, Ayder Referral Hospital, Tigray, Ethiopia, 2015. BMC Res Notes. 2018;11(1):1–6.
26. Seifu A, Eshetu O, Tafesse D, Hailu S. Admission pattern, treatment outcomes, and associated factors for children admitted to pediatric intensive care unit of Tikur Anbessa specialized hospital, 2021: a retrospective cross-sectional study. BMC Anesthesiol. 2022;22(1):1–8.
27. Abhulimhen-Iyoha BI, Pooboni SK, Vuppali NKK. Morbidity pattern and outcome of patients admitted into a pediatric intensive care unit in India. Indian J Clin Med. 2014;5(IJCM):S13902.
28. Tan G, Tan T, Goh D, Yap H. Risk factors for predicting mortality in a paediatric intensive care unit. Ann Acad Med Singap. 1998;27:813–818.
29. Bacha T, Tsegaye N, Tuli W. Characteristics and outcomes of mechanically ventilated pediatric patients in a tertiary referral hospital, Addis Ababa, Ethiopia: cross sectional study. Ethiop J Health Sci. 2021;31:5.
30. Polito A, Combescure C, Levy-Jamet Y, Rimensberger P. Long-stay patients in pediatric intensive care unit: diagnostic-specific definition and predictors. PLoS One. 2019;14(10):e0223369.
31. Verlaat CW, Visser IH, Wubben N, et al. Factors associated with mortality in low-risk pediatric critical care patients in the Netherlands. Pediatr Crit Care Med. 2017;18(4):e155–e61.
32. Teshager NW, Amare AT, Tamirat KS. Incidence and predictors of mortality among children admitted to the pediatric intensive care unit at the University of Gondar comprehensive specialised hospital, northwest Ethiopia: a prospective observational cohort study. BMJ open. 2020;10(10):e036746.
33. Faraci M, Bagnasco F, Giardino S, et al. Intensive care unit admission in children with malignant or nonmalignant disease: incidence, outcome, and prognostic factors A single-center experience. J Pediatr Hematol Oncol. 2014;36(7):e403–e9.
34. Valavi E, Aminzadeh M, Shirvani E, Jaafari L, Madhooshi S. The main causes of mortality in pediatric intensive care unit in south west of Iran. Sepsis. 2018;7(16):34.
35. Dey PK, Ghosh A, Hemram SK, Mukherjee M, Annigeri S, Nair A. Morbidity pattern with treatment outcome and predictors of mortality of children admitted to pediatric intensive care unit in a peripheral medical college in India. Acta Med Iran. 2021;59(8):491.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Incidence and Predictors of Cardiac Arrest Among Patients Admitted to the Intensive Care Units of a Comprehensive Specialized Hospital in Central Ethiopia
Ashine TM, Heliso AZ, Babore GO, Ezo E, Saliya SA, Muluneh BB, Alaro MG, Adeba TS, Sebro SF, Hailu AG, Abdisa EN
Patient Related Outcome Measures 2024, 15:31-43
Published Date: 15 February 2024