Back to Journals » International Journal of Women's Health » Volume 17
Causal Association of Primary Biliary Cholangitis with Adverse Pregnancy and Neonatal Outcomes: A Two-Sample Mendelian Randomization Study
Authors Li R ![]() , Tan J
, Tan J ![]() , Yang X, Ning Z
, Yang X, Ning Z
Received 4 September 2024
Accepted for publication 24 January 2025
Published 17 February 2025 Volume 2025:17 Pages 407—415
DOI https://doi.org/10.2147/IJWH.S494570
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Ruifang Li, Jieying Tan, Xia Yang, Zong Ning
Department of General Practice, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi Zhuang Autonomous Region, 530021, People’s Republic of China
Correspondence: Zong Ning, Department of General Practice, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi Zhuang Autonomous Region, 530021, People’s Republic of China, Email [email protected]
Background: Primary biliary cholangitis (PBC) is associated with multiple adverse pregnancy events and neonatal outcomes. However, the available observational study evidence results are inconsistent, and causality is unclear.
Methods: We used a two-sample Mendelian randomization (MR) analysis to assess the association between PBC and multiple adverse pregnancy events and neonatal outcomes in a European population. Independent SNPs associated with PBC from genome-wide association studies (GWAS) were selected as instrumental variables. The inverse variance weighting (IVW) method was used as the primary analysis method, supplemented by the remaining four MR analysis methods. Heterogeneity and sensitivity analyses of instrumental variables were examined using Cochrane’s Q, MR-PRESSO, MR-Egger, and leave-one-out methods.
Results: IVW estimates indicated that genetically predicted increased PBC was associated with lower birth weight (OR 0.991, 95% CI 0.983 ~ 0.998, P=0.018), decreased gestational age (OR 0.992, 95% CI 0.987 ~ 0.998, P=0.007), and increased risk of preterm birth (OR 1.043, 95% CI 1.007 ~ 1.081, P=0.019) were associated. For birth weight, the OR estimates obtained by weighted median (OR 0.988, 95% CI 0.980 ~ 0.996, P= 0.006) were consistent with IVW. In addition, no significant causal associations were found between genetically predicted PBC and preeclampsia or eclampsia, miscarriage, placental abruption, gestational diabetes mellitus, and postpartum hemorrhage.
Conclusion: Our study reveals that genetically predicted PBC is associated with low birth weight, decreased gestational age, and increased risk of preterm labor in a European population. However, current research does not establish a causal relationship between PBC and adverse pregnancy outcomes.
Keywords: primary biliary cholangitis, pregnancy, preterm delivery, Mendelian randomization, gestational age, birth weight
Introduction
Primary biliary cholangitis (PBC) is an immune-mediated, chronic cholestatic liver disease marked by tiny to medium-sized bile duct lesions, which are often accompanied by severe cholestasis.1 The pathogenesis of PBC is complex and results from a combination of environmental triggers, epigenetic alterations, and autogenetic susceptibility. However, an inherited genetic predisposition is a major factor in the development of PBC. It was found that five out of eight identical twins had PBC at the same time, with a 63% pairwise concordance rate. Conversely, researchers found no pairwise concurrent PBC in dizygotic twins.2 The clinical features of PBC include dysregulation of the body’s immune balance, bile metabolism disorders, and progressive fibrosis, which will eventually progress to cirrhosis and liver failure if not treated in time.3–5 Currently, the treatment of PBC mainly focuses on relieving cholestasis, and ursodeoxycholic acid is still the first-line therapeutic drug for PBC.6–8
Epidemiologic investigations have shown that PBC is more common, mainly in postmenopausal middle-aged women, with about one-quarter of PBC patients being of childbearing age. However, only a few studies have reported on pregnancy in PBC, primarily case reports and small cohort studies.9 Pregnancy in women with PBC typically results in pruritic symptoms. However, we have not observed any adverse maternal events or adverse neonatal outcomes during the perinatal period.10,11 Another study noted a significantly increased risk of preterm labor during pregnancy in patients with PBC.9 Additionally, chronic cholestasis and bile acid disorders often accompany PBC progression, affecting approximately 4% of pregnancies.12 Cholestasis usually occurs late in pregnancy; in a few cases, it begins as early as seven weeks of gestation.13 Studies have shown that elevated serum bile acid levels during pregnancy are an essential risk factor for adverse pregnancy and fetal abnormalities.14,15 However, the impact of the progression of PBC during pregnancy concerning adverse pregnancy events and fetal outcomes remains understudied, with most studies focusing on only a few specific outcomes and lacking a comprehensive assessment of the overall impact. In addition, traditional observational studies may produce controversial results due to confounding factors and reverse causality. Therefore, reassessment of the effects of PBC on a wide range of adverse pregnancy and neonatal outcomes is essential to protect maternal and fetal health.
Mendelian randomization (MR) is a genetic variation-based research strategy that identifies causal links between exposure and disease. Mendelian randomization (MR) uses genetic variants to minimize confounders and reverse causation, offering clearer evidence of causation compared to observational studies. This study used two-sample MR analysis to find for the first time a causal relationship between PBC and adverse pregnancy and neonatal outcomes. This approach emphasizes PBC’s distinct significance in maternal and fetal outcomes from a genetic perspective and helps doctors gain a better understanding of the effects of PBC throughout pregnancy.
Materials and Methods
Study Design
As shown in Figure 1, in order to reduce unnecessary bias caused by external environmental factors in the study of causality between exposure and outcome, we utilized multiple single nucleotide polymorphisms (SNPs) as instrumental variables (IVs) for subsequent MR analyses. According to the guiding specifications of the STROBE - MR statement, we performed the MR analysis process subject to 3 core assumptions: 1) there is a strong correlation between the IVs and PBC; 2) the IVs are independent of any confounding factors that may influence the relationship between PBC and the eight adverse pregnancy and neonatal outcomes; and 3) the IVs can influence the eight adverse pregnancy and neonatal outcomes only through PBC.16
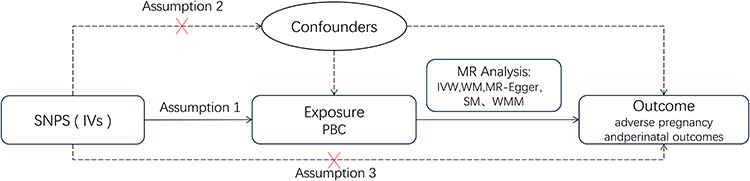 |
Figure 1 Two-sample Mendelian randomization between PBC and eight adverse pregnancy and neonatal outcomes. IVs: instrumental variables; SNP: single nucleotide polymorphism. |
Data Sources
GWAS (Genome-Wide Association Study) identifies genetic variants associated with specific traits or diseases by comparing genomic differences across individuals. This research leverages whole-genome sequencing to detect statistical associations between single nucleotide polymorphisms (SNPs) and PBC.17 Details of the GWAS data between PBC and the eight adverse pregnancy and neonatal outcomes are shown in Table 1. We retrieved the maximum GWAS pooled dataset for PBC from the IEU OpenGWAS Database Project (https://gwas.mrcieu.ac.uk/) and the FinnGen GWAS database (version R9, https://r9.finngen.fi/) retrieved for the largest GWAS pooled datasets for PBC, gestational diabetes mellitus, miscarriage, placental abruption, preeclampsia or eclampsia, and postpartum hemorrhage. The PBC GWAS pooled dataset was obtained from 13,239 participants (2,764 patients and 10,475 controls) of European descent. Miscarriage GWAS pooled dataset from 49,996 patients and 174,109 controls from the European population. GWAS summary statistics for preeclampsia and eclampsia from a European sample comprising 114,735 controls and 3,903 cases. Data from 5,687 cases and 117,892 controls in a European population were utilized in the gestational diabetes mellitus GWAS. The placental abruption GWAS included data from a European sample of 294 cases and 104,247 controls. Postpartum hemorrhage GWAS pooled data from a European population of 44,559 patients and 202,621 controls. GWAS data for gestational age, birth weight, and preterm labor were obtained from the Early Growth Genetics Consortium (http://egg-consortium.org/).18,19 The birth weight GWAS data included 210,267 European populations. GWAS data for gestational age included 84,689 European populations. Preterm labor GWAS data contained 4,775 patients and 60,148 controls. The GWAS data utilized in this investigation were published openly by the host research institution; therefore, no further ethical approval was required.
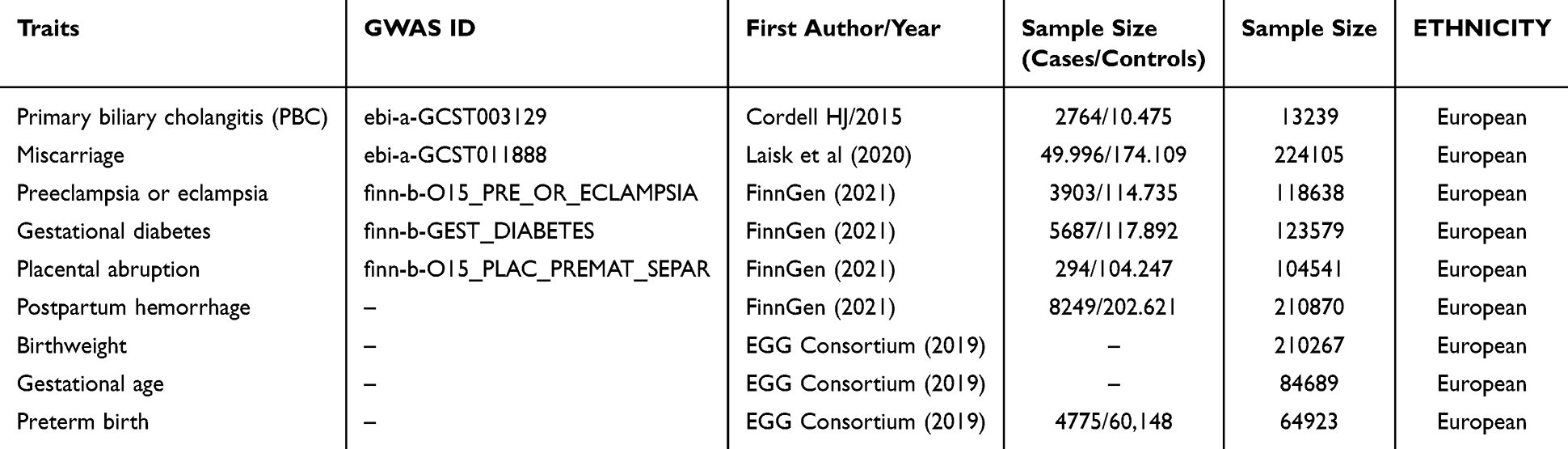 |
Table 1 Information on Data Included in the Study |
Selection of Genetic Instrument Variables
To ensure the statistical validity of the IVs, we used the following screening criteria: 1) We selected SNPs associated with PBC as potential candidate IVs (p < 5e-8); 2) to ensure genetic independence between the selected variables, we chose r2 < 0.001 and a window size of 10,000 kb; 3) SNPs with an F-statistic of < 10 were excluded to ensure that the IVs obtained muscular association strength with PBC,20 F = R2(N - K - 1) / [K (1-R2)], where K is the number of SNPs contained in IVs, R2 is the exposure variance explained by each SNP, and N is the total number of valid samples included in the GWAS; and 4) exclude SNPs that were allele incompatible in the palindromic sequences and had a minimum allele frequency < 1%.
Statistical Analysis
To assess the causal effects between PBC and eight adverse pregnancy and neonatal outcomes, five MR analysis methods were used in a two-sample MR study, including inverse variance weighting (IVW), weighted mode, simple mode, MR-Egger, and weighted median (WM) methods. IVW, as the primary assessment method for MR analysis, was used to assess the causal effect of PBC by averaging the causal effect values, and then the inverse of their variance was taken as a weight.21 The slope of the MR-Egger regression reflects the average causal effect of all genetic variants. The WM method ensured that >50% of the IVs were valid. MR estimates were expressed as the odds ratio (OR) and its 95% confidence interval (CI). Sensitivity analyses were performed using MR-Egger regression, MR-PPRESSO, and leave-one-out methods. We assessed the horizontal pleiotropy of causal effects using MR-Egger regression’s intercept and zero difference.22 MR PRESSO identifies outliers in IVs and reduces potential horizontal pleiotropy in the MR process by excluding outliers.23 The heterogeneity of MR analyses was evaluated using the Cochrane’s Q test; if P < 0.05, the IVW random effects model was applied. Otherwise, the IVW random effects model and fixed effects model were both applied.16 Furthermore, a leave-one-out analysis was implemented to evaluate the stability of the MR estimates following the individual exclusion of each selected SNP. We conducted all tests using the R software (version 4.3.3), Two Sample MR (version 0.6.4), and MR PRESSO (version 1.0). We deemed P-values statistically significant if they were less than 0.05.
Results
Selection of IVs
We screened 25 PBC-associated SNPs following the screening criteria for PBC-associated IVs. Each SNP met the F-statistic > 10 and the F-value in the range of 202.230–2004.173. Supplementary Table S1 displays the specific information about the SNP loci.
Causal Estimates of the Association Between Genetic Susceptibility to PBC and Adverse Pregnancy and Neonatal Outcomes
The IVW model showed that genetically predicted increased PBC was associated with lower birth weight (OR 0.991, 95% CI 0.983 ~ 0.998, P=0.018), decreased gestational age (OR 0.992, 95% CI 0.987 ~ 0.998, P=0.007), and increased risk of preterm labor (OR 1.043, 95% CI 1.007 ~ 1.081, P=0.019). For birth weight, the weighted median OR estimates (OR 0.988, 95% CI 0.980 ~ 0.996, P = 0.006) were consistent with IVW. The remaining causal association estimates from the four MR analysis methods, including MR-Egger regression and weighted median, were generally consistent with the IVW direction. In addition, there was no evidence of a significant causal association between genetically predicted PBC and miscarriage, preeclampsia or eclampsia, gestational diabetes mellitus, placenta previa, or postpartum hemorrhage in the IVW prediction results. The results of the MR analyses are shown in Figures 2 and 3 and Supplementary Table S2.
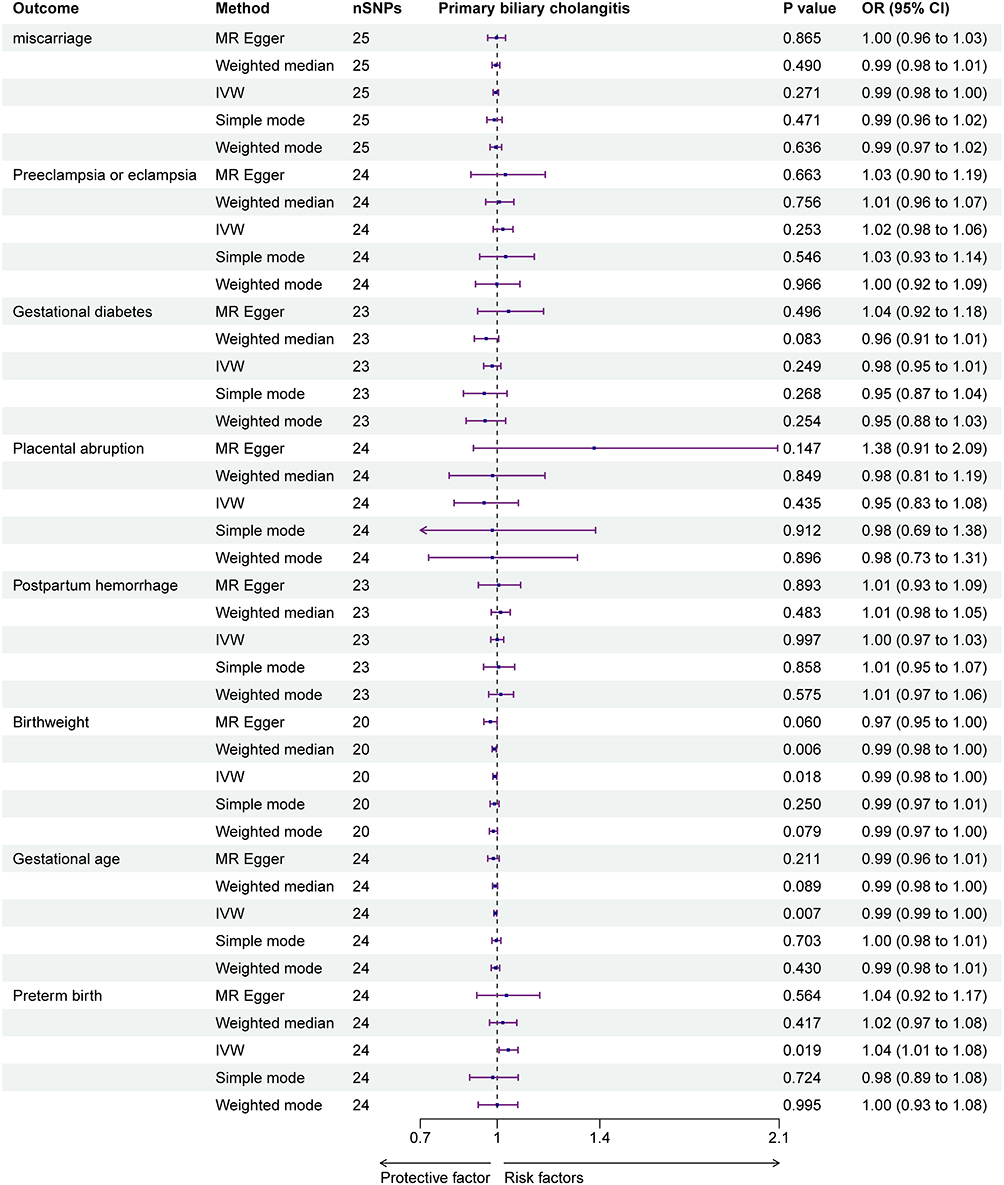 |
Figure 2 Forest plot visualization of MR estimates for genetic prediction of causal associations between PBC and adverse pregnancy and neonatal outcomes. |
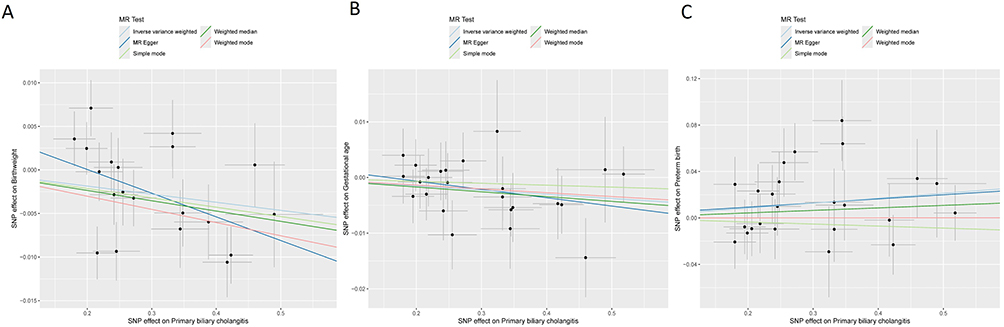 |
Figure 3 Scatter plots of causality between PBC and adverse pregnancy and neonatal outcomes. (A) Low birth weight. (B) Gestational age. (C) Preterm birth. Abbreviation: MR, Mendelian randomization. |
Sensitivity Analysis
A random effects model was employed for IVW in Cochran’s Q analysis, and the Q statistic for birth weight was P < 0.05, showing heterogeneity. A possible explanation is that the observed heterogeneity in birth weight may be attributable to genetic, environmental, and maternal health factors, which cannot be completely eliminated in Mendelian randomization studies. In addition, methodological errors (such as measurement inaccuracies and data entry problems) may also contribute to the heterogeneity of the observed results. We found no significant heterogeneity for the other outcomes (Supplementary Table S3). The MR-PRESSO results revealed outliers in birth weight (rs11065987, rs1800693, rs485499, rs2297067, rs7774434) and gestational diabetes mellitus (rs7774434). We eliminated these outliers and reanalyzed them using MR, presenting the MR results in Supplementary Figure S2. Leave-one-out plots (Supplementary Figure S1) display the effects and trends of SNPs on outcomes for each MR analysis method. All MR procedures showed no significant deviation of the MR-Egger regression intercept from zero, and the IVs for each outcome showed no evidence of horizontal pleiotropy in PBC (Supplementary Table S3). Furthermore, the results of the leave-one-out analysis indicate that the total risk estimate without any causal association is driven by a specific SNP (Supplementary Figure S1).
Discussion
Our MR results reveal for the first time a significant causal relationship between genetically predicted PBC and neonatal outcomes (birth weight, gestational age, and preterm birth) but not with adverse pregnancy outcomes (gestational diabetes mellitus, preeclampsia or eclampsia, placental abruption, miscarriage, and postpartum hemorrhage). The etiology is unknown.
Emerging evidence supports the role of PBC in neonatal outcomes. Research on PBC and neonatal outcomes is limited, and the precise mechanisms remain unclear. Genetic susceptibility, environmental factors, the accumulation of bile acids in the fetus during pregnancy, and the increased responsiveness of the myometrium to bile acids are considered potential factors. Researchers have reported an increased risk of adverse fetal outcomes, such as preterm labor and stillbirth, in pregnant women with elevated serum bile acids.24 A multicenter retrospective study revealed a higher rate of preterm delivery (up to 28%) in female patients with PBC during pregnancy and a negative correlation between the number of days of gestation and maternal serum bile acid levels during pregnancy.9 It was concluded that the rate of preterm labor increased significantly when the serum bile acid concentration in pregnant women was ≥40 μmol/L.25 A multicenter study in the Netherlands that included 215 pregnant women found that patients with severe cholestasis had a significantly lower gestational age at delivery, as well as a considerably higher risk of spontaneous preterm delivery compared to those with mild cholestasis.26 Chen et al27 conducted an observational study of pregnancy outcomes in patients with intrahepatic cholestasis in Hangzhou, China, during 2018–2020, which included 39,244 pregnant women, including 688 patients with intrahepatic cholestasis, and found that pregnant women with intrahepatic cholestasis were more likely to experience shorter gestational days and the resulting preterm delivery and weight loss of the fetus. Experiments on animals have also revealed that prolonged intravenous infusion of bile acids, which maintains higher levels of bile acids in the body, predisposes pregnant sheep to preterm labor and increases the risk of meconium contamination in their amniotic fluid.28 Additionally, studies have reported that administering exogenous bile acids to isolated uterine myocytes in vitro experiments led to elevated oxytocin receptor expression.29 Overall, clinicians should inform patients with PBC of the potential risk of preterm labor, weight loss, and decreased gestational age during pregnancy, particularly when serum bile acid levels are elevated, and enhance perinatal care and monitoring.
Studies on PBC and adverse pregnancy events are scarce and limited to a few case reports and case-control studies. The present study did not find genetic evidence of a causal association between PBC and pregnancy outcomes, which is consistent with the findings of several previous studies. Possible biological explanations include a weak effect of genetic polymorphisms on these specific results, or a dominant role of other environmental factors. In addition, methodological limitations, such as insufficient sample size, measurement error of exposure variables, etc., may also lead to non-significant results. Studies have demonstrated that patients with PBC experience no significant adverse pregnancy events during pregnancy, and 70% of these patients tend to enter clinical remission during pregnancy, maintaining most of their hepatic biochemical markers at normal levels.11 Similarly, Floreani et al10 included in their case-control study 233 female PBC patients (186 of whom had at least one conception) and 367 healthy women (who had at least one conception in their lifetime) seen from 1987 to 2012 and found that when compared to the healthy group, PBC patients had no significant differences. However, some studies have found an increased risk of miscarriage during pregnancy in patients with PBC. A meta-analysis that included a total of 2,179 female PBC patients in 11 observational studies showed that pregnant women with PBC had a significant 1.27-fold increased risk of miscarriage.30 In addition, patients with PBC are often clinically associated with intrahepatic cholestasis, which is considered a risk factor for adverse pregnancy events during pregnancy. A 12-year Swedish cohort study examined the association between intrahepatic cholestasis in pregnancy and the risk of adverse pregnancy and fetal outcomes and found that, compared with those without intrahepatic cholestasis, those with intrahepatic cholestasis had a significantly higher risk of preeclampsia (OR 2.62, 95% CI 2.32–2.78), and gestational diabetes (OR 2.81, 95% CI 2.32–3.41) had a significantly higher risk.31 A recent 4-year retrospective study similarly found that pregnant women with comorbid intrahepatic cholestasis had a higher risk of gestational diabetes mellitus and preeclampsia and were significantly associated with adverse perinatal outcomes.32 Elevated serum bile acids interfere with the normal rhythm of cardiomyocytes as well as the production of lung surface-active substances, which may lead to fetal distress and stillbirth.14,15 Moreover, studies suggest that pregnancy has an immune-tolerant effect on PBC development, and higher serum estrogen levels during pregnancy contribute to the conversion of cytokine type I cytotoxic profiles to type 2 anti-inflammatory profiles, thereby indirectly attenuating the impact of PBC on pregnancy outcomes.33,34 More extensive prospective multicenter studies are necessary for validation, as clinical studies remain controversial.
This is the first MR investigation that investigates the possible causative relationship between PBC and unfavorable pregnancy and newborn outcomes, as far as we are aware. As confounding bias is often present in observational studies, it prevents us from obtaining valid and reliable conclusions when determining causal effects between diseases. The foundation of Mendelian randomisation is the idea of genetic random assignment, which successfully eliminates reverse causality and confounding variables. The GWAS significance threshold for MR analysis was set at p < 5e-8 so that there was a significant correlation between the candidate SNPs and the exposure. SNPs with an F-statistic of F < 10 were also excluded. Finally, robust and strongly associated IVs were obtained, which ensured the reliability of the results of the MR analysis. In the MR analysis, in addition to IVW as the primary analysis method, we used four different MR analysis methods for iterative analysis to obtain robust results and eliminate anomalous outliers in the sensitivity analysis to minimize false-positive results due to horizontal pleiotropy and heterogeneity. The population source for the aggregated GWAS data we included was primarily European, reducing the confounding problem of population stratification. However, there are some limitations here. Because of differences in the prevalence and incidence of PBC, adverse pregnancy events, and neonatal outcomes among different ethnic populations, GWAS data for other ethnic populations was also lacking in our MR study. Therefore, one should exercise caution when extrapolating these findings to other non-European ethnic populations. Furthermore, we anticipate further refinement of the causal relationship between PBC and adverse pregnancy and neonatal events in different ethnic populations in the future as we update and pool relevant GWAS databases.
Conclusion
Our findings suggest that there is a link between genetically predicted PBC and an increased risk of newborn outcomes such as low birth weight, short gestational age, and premature birth. We recommend further in-depth studies to uncover the pathophysiologic mechanisms underlying this relationship and to offer clinicians new and compelling evidence to guide perinatal monitoring and postpartum neonatal care.
Abbreviations
CIs, confidence intervals; GWAS, genome-wide associated studies; IVs, instrumental variables; IVW, inverse-variance weighted; MR, Mendelian randomization; ORs, odds ratios; SNPs, single-nucleotide polymorphisms; WM, weighted median; PBC, primary biliary cholangitis.
Data Sharing Statement
All GWAS datasets used in this study were obtained from online publicly available summary statistics.
Ethics Statement
Since the GWAS data used in this study are entirely based on publicly available online GWAS summary-level statistics, no ethical approval is required. According to Article 32 of China’s “Measures for the Ethical Review of Biomedical Research Involving Humans,” which came into effect on February 18, 2023, the specific contents are as follows: Article 32: Biomedical research involving humans may be exempted from ethical review in the following circumstances: 1. Item 1: Research based on public databases that does not involve the identification or use of personal information. 2. Item 2: Analysis of collected data that does not involve the collection of new data or direct intervention in participants. These two provisions clarify that this article is exempt from ethical review when using public data and conducting data analysis.
Acknowledgments
Genetic association estimates for primary biliary cholangitis, adverse pregnancy, and neonatal outcomes were obtained from the MRC-IEU study and the FinnGen Consortium’s GWAS pooled analysis. The authors thank all participants for contributing to and sharing this data with adverse pregnancy and neonatal outcomes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the 2022 Guangxi Zhuang Autonomous Region Health Care Commission Self-funded Research Project in Western Medicine (Z-A20220406) and the Innovation Project of Guangxi Graduate Education (JGY2023080).
Disclosure
The authors declared no competing interests in this work.
References
1. Lindor KD, Gershwin ME, Poupon R, Kaplan M, Bergasa NV, Heathcote EJ. Primary biliary cirrhosis. Hepatology. 2009;50(1):291–308. doi:10.1002/hep.22906
2. Selmi C, Mayo MJ, Bach N, et al. Primary biliary cirrhosis in monozygotic and dizygotic twins: genetics, epigenetics, and environment. Gastroenterology. 2004;127(2):485–492. doi:10.1053/j.gastro.2004.05.005
3. Zollner G, Trauner M. Mechanisms of cholestasis. Clin Liver Dis. 2008;12(1):1–26. doi:10.1016/j.cld.2007.11.010
4. Zhuang Y, Ortega-Ribera M, Thevkar Nagesh P, et al. Bile acid-induced IRF3 phosphorylation mediates cell death, inflammatory responses, and fibrosis in cholestasis-induced liver and kidney injury via regulation of ZBP1. Hepatology. 2024;79(4):752–767. doi:10.1097/HEP.0000000000000611
5. Molinaro A, Marschall H-U. Bile acid metabolism and FXR-mediated effects in human cholestatic liver disorders. Biochem Soc Trans. 2022;50(1):361–373. doi:10.1042/BST20210658
6. Hirschfield GM, Dyson JK, Alexander GJM, et al. The British Society of Gastroenterology/UK-PBC primary biliary cholangitis treatment and management guidelines. Gut. 2018;67(9):1568–1594. doi:10.1136/gutjnl-2017-315259
7. Oo YH, Neuberger J. Options for treatment of primary biliary cirrhosis. Drugs. 2004;64(20):2261–2271. doi:10.2165/00003495-200464200-00001
8. Levy C, Bowlus CL. Primary biliary cholangitis: personalizing second-line therapies. Hepatology. 2024. doi:10.1097/HEP.0000000000001166
9. Cauldwell M, Mackie FL, Steer PJ, et al. Pregnancy outcomes in women with primary biliary cholangitis and primary sclerosing cholangitis: a retrospective cohort study. BJOG. 2020;127(7):876–884. doi:10.1111/1471-0528.16119
10. Floreani A, Infantolino C, Franceschet I, et al. Pregnancy and primary biliary cirrhosis: a case-control study. Clin Rev Allergy Immunol. 2015;48(2–3):236–242. doi:10.1007/s12016-014-8433-z
11. Trivedi PJ, Kumagi T, Al-Harthy N, et al. Good maternal and fetal outcomes for pregnant women with primary biliary cirrhosis. Clin Gastroenterol Hepatol. 2014;12(7):1179–1185.e1. doi:10.1016/j.cgh.2013.11.030
12. Dixon PH, Williamson C. The pathophysiology of intrahepatic cholestasis of pregnancy. Clin Res Hepatol Gastroenterol. 2016;40(2):141–153. doi:10.1016/j.clinre.2015.12.008
13. Geenes V, Lövgren-Sandblom A, Benthin L, et al. The reversed feto-maternal bile acid gradient in intrahepatic cholestasis of pregnancy is corrected by ursodeoxycholic acid. PLoS One. 2014;9(1):e83828. doi:10.1371/journal.pone.0083828
14. Zhang Y, Li F, Wang Y, et al. Maternal bile acid transporter deficiency promotes neonatal demise. Nat Commun. 2015;6:8186. doi:10.1038/ncomms9186
15. Gorelik J, Shevchuk A, de Swiet M, Lab M, Korchev Y, Williamson C. Comparison of the arrhythmogenic effects of tauro- and glycoconjugates of cholic acid in an in vitro study of rat cardiomyocytes. BJOG. 2004;111(8):867–870. doi:10.1111/j.1471-0528.2004.00166.x
16. Bowden J, Spiller W, Del Greco MF, et al. Improving the visualization, interpretation and analysis of two-sample summary data Mendelian randomization via the radial plot and radial regression. Int J Epidemiol. 2018;47(6):2100. doi:10.1093/ije/dyy265
17. Bush WS, Moore JH. Chapter 11: genome-wide association studies. PLoS Comput Biol. 2012;8(12):e1002822. doi:10.1371/journal.pcbi.1002822
18. Liu X, Helenius D, Skotte L, et al. Variants in the fetal genome near pro-inflammatory cytokine genes on 2q13 associate with gestational duration. Nat Commun. 2019;10(1):3927. doi:10.1038/s41467-019-11881-8
19. Warrington NM, Beaumont RN, Horikoshi M, et al. Maternal and fetal genetic effects on birth weight and their relevance to cardio-metabolic risk factors. Nat Genet. 2019;51(5):804–814. doi:10.1038/s41588-019-0403-1
20. Burgess S, Thompson SG. Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. 2011;40(3):755–764. doi:10.1093/ije/dyr036
21. Burgess S, Butterworth A, Thompson SG. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. 2013;37(7):658–665. doi:10.1002/gepi.21758
22. Bowden J, Del Greco MF, Minelli C, Davey Smith G, Sheehan N, Thompson J. A framework for the investigation of pleiotropy in two-sample summary data Mendelian randomization. Stat Med. 2017;36(11):1783–1802. doi:10.1002/sim.7221
23. Verbanck M, Chen C-Y, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
24. Šimják P, Pařízek A, Vítek L, et al. Fetal complications due to intrahepatic cholestasis of pregnancy. J Perinat Med. 2015;43(2):133–139. doi:10.1515/jpm-2014-0089
25. Ovadia C, Seed PT, Sklavounos A, et al. Association of adverse perinatal outcomes of intrahepatic cholestasis of pregnancy with biochemical markers: results of aggregate and individual patient data meta-analyses. Lancet. 2019;393(10174):899–909. doi:10.1016/S0140-6736(18)31877-4
26. Brouwers L, Koster MPH, Page-Christiaens GCML, et al. Intrahepatic cholestasis of pregnancy: maternal and fetal outcomes associated with elevated bile acid levels. Am J Obstet Gynecol. 2015;212(1):
27. Odabaş RK, Sökmen Y, Dünder E, Taşpınar A. The incidence of intrahepatic cholestasis of pregnancy and its maternal, fetal, and neonatal adverse outcomes: a systematic review and meta-analysis. J Midwifery Women's Health. 2024;69(3):370–382. doi:10.1111/jmwh.13640
28. Campos GA, Guerra FA, Israel EJ. Effects of cholic acid infusion in fetal lambs. Acta Obstet Gynecol Scand. 1986;65(1):23–26. doi:10.3109/00016348609158224
29. Germain AM, Kato S, Carvajal JA, Valenzuela GJ, Valdes GL, Glasinovic JC. Bile acids increase response and expression of human myometrial oxytocin receptor. Am J Obstet Gynecol. 2003;189(2):577–582. doi:10.1067/S0002-9378(03)00545-3
30. El Jamaly H, Eslick GD, Weltman M. Primary biliary cholangitis in pregnancy: a systematic review with meta-analysis. Hepatobiliary Pancreat Dis Int. 2022;21(3):218–225. doi:10.1016/j.hbpd.2022.03.005
31. Wikström Shemer E, Marschall HU, Ludvigsson JF, Stephansson O. Intrahepatic cholestasis of pregnancy and associated adverse pregnancy and fetal outcomes: a 12-year population-based cohort study. BJOG. 2013;120(6):717–723. doi:10.1111/1471-0528.12174
32. Avsar HA, Atlıhan U, Ata C, Erkılınc S. Intrahepatic cholestasis of pregnancy and its association with preeclampsia and gestational diabetes: a retrospective analysis. Arch Gynecol Obstet. 2024;310(1):221–227. doi:10.1007/s00404-024-07507-0
33. Cutolo M, Sulli A, Straub RH. Estrogen metabolism and autoimmunity. Autoimmun Rev. 2012;11(6–7):A460–A464. doi:10.1016/j.autrev.2011.11.014
34. Ostensen M, Brucato A, Carp H, et al. Pregnancy and reproduction in autoimmune rheumatic diseases. Rheumatology. 2011;50(4):657–664. doi:10.1093/rheumatology/keq350
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Causal Association Between Circulating Inflammatory Proteins and Autoimmune Liver Disease: a Bidirectional Two-Sample Mendelian Randomization Study
Leng L, Li Y, Xu T, Shen J, Li L, Li X
ImmunoTargets and Therapy 2025, 14:279-289
Published Date: 26 March 2025
Predictive Value of Postnatal Weight Gain Rate for Severe Retinopathy of Prematurity in Preterm Infants: A Retrospective Analysis
Wang J, Ma Q, Du F
Journal of Multidisciplinary Healthcare 2025, 18:5381-5391
Published Date: 30 August 2025
The Prevalence of Asymptomatic Bacteriuria Among Jordanian Pregnant Women
Qatawneh A, Shaqour RAE, Al-Amayreh I, Abuhussein H, Abd Alnabi A, Alaiwah M, Khatatneh AS, Alqatawneh A, Thekrallah F
International Journal of Women's Health 2025, 17:4923-4931
Published Date: 27 November 2025