Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Predictive Value of Postnatal Weight Gain Rate for Severe Retinopathy of Prematurity in Preterm Infants: A Retrospective Analysis
Received 13 March 2025
Accepted for publication 15 August 2025
Published 30 August 2025 Volume 2025:18 Pages 5381—5391
DOI https://doi.org/10.2147/JMDH.S528155
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jiangya Wang,1 Qingmin Ma,2 Fangfang Du1
1Department of Pediatrics, Hebei General Hospital, Shijiazhuang, 050000, People’s Republic of China; 2Department of Ophthalmology, Hebei General Hospital, Shijiazhuang, 050000, People’s Republic of China
Correspondence: Jiangya Wang, Department of Pediatrics, Hebei General Hospital, No. 348 Heping West Road, Xinhua District, Shijiazhuang, 050000, People’s Republic of China, Tel +86 18330181686, Email [email protected]
Background: Retinopathy of prematurity (ROP) is rising in China alongside improved neonatal intensive care. Current screening, reliant on gestational age (GA) and birth weight (BW), faces challenges of resource constraints and infant burden. Postnatal weight gain rate (WGR) is a potential predictive marker, but robust data on its value, particularly for severe ROP, and validated thresholds within the Chinese population are lacking. The study aimed to examine the risk factors linked with the incidence of retinopathy of ROP.
Methods: A retrospective cohort analysis was conducted on 230 preterm infants (GA ≤ 32 weeks, BW ≤ 2000g) admitted to a neonatal intensive care unit (2016– 2020). Infants were categorized into non-ROP (n=189) and ROP (n=41) groups; the ROP group was further stratified into mild (n=32) and severe (n=9) subgroups. Clinical data, including GA, BW, comorbidities and WGR, were analyzed. Univariate analysis, multivariate logistic regression, and receiver operating characteristic (ROC) curve analysis were employed.
Results: In the univariate analysis, the non-ROP group manifested superior values in GA, BW, and rates of weight gain in comparison to the ROP group (all P < 0.05). Multivariate analysis identified lower GA (OR=0.91, 95% CI=0.83– 0.99, P=0.03), lower BW (OR=0.99, 95% CI=0.99– 1.00, P=0.04), and lower WGR (OR=0.73, 95% CI=0.63– 0.83, P< 0.01) as independent risk factors for ROP. GA, BW, and WGR were significantly higher in the mild vs severe ROP group (all P< 0.05). ROC analysis demonstrated that WGR < 24.5 g/day predicted any ROP (AUC=0.939, 95% CI=0.905– 0.973, sensitivity 90.2%, specificity 86.8%, P< 0.05). Crucially, WGR < 18 g/day predicted severe ROP (AUC=0.865, 95% CI=0.70– 1.00, sensitivity 100%, specificity 66,7%, P< 0.05).
Conclusion: Diminished GA, reduced BW, and sluggish weight gain rates have been correlated with an elevated susceptibility to ROP. Notably, a diminished rate of weight gain can serve as an anticipatory marker for severe ROP, given its heightened propensity to precipitate the onset of severe ROP.
Trial Registration: Full name of the registry: Chinese Clinical Trial Registry, http://www.chictr.org.cn. Trial registration number: chiCTR2400087938. Date of registration: 2024-08-07.
Keywords: birth weight, gestational age, retinopathy of prematurity, risk factors, weight gain rate
Background
Retinopathy of prematurity (ROP) manifests as aberrant proliferation of retinal vasculature and stands as a significant etiology of childhood blindness.1 The proliferation of neonatal intensive care units (NICUs) and advancements in medical technology have concomitantly elevated the survival rates of preterm and low/very-low-birth-weight infants, yet this positive trend is paralleled by a commensurate increase in the incidence of ROP. Although most infants afflicted with ROP exhibit a gradual recuperation with subsequent attainment of normal vision, the trajectory of the condition may, in some instances, exhibit exacerbation. Left untreated, ROP has the potential to precipitate retinal detachment, culminating in irreversible blindness.2 The imperative of early screening and intervention cannot be overstated, serving as pivotal measures to impede disease progression and enhance prognostic outcomes in neonates afflicted with ROP.3 Nevertheless, high expenditure and pain during examination associated with frequent fundus examinations underscore the urgent need for a more convenient and economical screening strategy for ROP. In accordance with existing studies, the etiology of ROP is contingent upon a confluence of determinants, encompassing gestational age (GA), birth weight (BW), and oxygen exposure in premature neonates.4–7 Notably, recent studies founded that the incidence of ROP was associated with suboptimal postnatal weight accrual, suggesting its potential utility in refining screening criteria.8,9 A 2025 Korean national cohort study of 13,778 very low birth weight infants (<1500 g) revealed a severe ROP (stage ≥3 or requiring treatment) incidence of 14.8%, with histological chorioamnionitis paradoxically reducing risk in infants 26–31 weeks’ gestation.10 Conversely, in low- and middle-income countries, ROP incidence has surged to 20%–47.4%, attributed to expanded neonatal intensive care unit coverage without commensurate screening infrastructure.11 China exemplifies this trend: with approximately 7–10% of 20 million annual births being preterm, ROP affects 30–40,000 infants yearly, of whom 20,000–30,000 face blindness risk.12 Despite this growing international evidence, data specifically evaluating the predictive value of WGR for ROP, and particularly for severe ROP, within the Chinese preterm population remain limited. Existing Chinese studies have primarily focused on associations or smaller cohorts, and the critical question of defining clinically applicable WGR thresholds to predict severe ROP risk in this population has not been adequately addressed. Therefore, this retrospective cohort study aimed to identify risk factors associated with ROP development in Chinese preterm infants, specifically evaluate the predictive value of postnatal weight gain rate (WGR) for both any ROP and, crucially, severe ROP, and determine optimal WGR cut-off values using ROC curve analysis to stratify the risk of severe ROP.
Our study addresses a significant gap by providing robust data on WGR as a predictive marker for ROP, with a specific focus on severe disease, within a well-characterized cohort of Chinese preterm infants. Crucially, we establish and validate a clinically relevant WGR threshold predictive of severe ROP risk. This novel finding has direct implications for refining ROP screening protocols in China, potentially reducing unnecessary examinations while ensuring timely intervention for the highest-risk infants.
Methods
Participants
This retrospective cohort study was conducted on premature infants exhibiting GA < 32 weeks and/or BW ≤ 2000 g. The infants under study were those admitted to our neonatal intensive care unit from September 1, 2016, to December 31, 2020, and were selected in strict adherence to the screening criteria outlined in the Guidelines for International Classification of Retinopathy Prematurity, Third Edition.13
Inclusion criteria were as follows: (1) infants with complete medical records; (2) infants who underwent screening tests for ROP, with detailed records of examination and treatment for fundus lesions; (3) infants without congenital developmental malformations or metabolic diseases. We initially enrolled 243 premature infants and three subjects were excluded for being concomitant with Down’s syndrome, congenital heart disease, and phenylketonuria, respectively. In addition, four cases died and six infants did not receive fundus screening in our hospital, for which the infants were also excluded. A total of 230 premature infants met the inclusion criteria.
Data of all enrolled infants were collected, encompassing GA, BW, ROP staging, weight gain rate, in vitro fertilization (IVF), occurrences of multiple births (including twins), instances of invasive ventilator-assisted ventilation before the initial fundus screening, and associated comorbidities like neonatal respiratory distress syndrome (NRDS), intracranial hemorrhage, asphyxia, bronchopulmonary dysplasia (BPD), patent ductus arteriosus (PDA), history of blood transfusion, as well as maternal comorbidities including gestational diabetes mellitus (GDM) and gestational hypertension (GH).
The BW of each infant was meticulously measured by a designated individual at 7, 14, 21, and 28 days postnatally up to the first fundus screening. Low-birth-weight infants undergo generalized weight loss at the first postnatal week, for which the weight gain rate (g/d) was computed from the second postnatal week to the initial postnatal fundus screening. The average daily weight gain rate was determined using the formula: average daily weight gain rate = (weight at initial postnatal fundus screening - weight at the second postnatal week)/number of days between measurements.
All weights were measured with an ACS-20-YE electronic infant scale with a precision of 1 g, and the measuring instruments underwent regular calibration by a designated individual. The study received approval from the Ethics Committee of Hebei Provincial People’s Hospital (Research Review No. 138).
Study Methods
Screening Method for ROP
ROP was assessed by two qualified ophthalmologists respectively. When there were discrepant results, the more serious result should be taken as the standard, which would be verified by an experienced ophthalmologist. Only those premature infants exhibiting GA < 32 weeks, BW ≤ 2000 g, and/or being with oxygen therapy history underwent fundus examinations according to the screening criteria outlined in the International Classification of Retinopathy Prematurity, Third Edition. The kind of infants have high risk of developing ROP and finally irreversible blindness if left untreated. Employing a wide-angle digital pediatric retinal imaging system, specifically the Ret Cam 3, fundus examinations were conducted within the temporal window of 4 to 6 weeks postpartum or at a corrected GA of 32 weeks, contingent upon the stability of vital signs in the neonates. Subsequent to a meticulous evaluation of the overall health status of the infants, informed consent for the examination was obtained from their respective families.
For the attainment of comprehensive mydriasis, infants received 1% compound tropicamide eye drops one hour before the examination, followed by the administration of oxybuprocaine hydrochloride eye drops for corneal anesthesia. The infants were securely immobilized in the supine position by nursing personnel. The ophthalmologist, utilizing an eye speculum, meticulously exposed the eyelids, applied gel to the corneal surface, and systematically examined each quadrant of the retina in both eyes employing the Ret Cam 3.
Diagnostic Criteria for ROP
ROP was identified using the criteria outlined in the International Classification of Retinopathy Prematurity, Third Edition. Lesion locations were divided into zones I, II, and III, and severity was graded across five stages. The extent of involvement was denoted by clock numbers, with additional lesions marked by “+”. Screening was conducted at 1 to 2-week intervals based on the disease stage and severity, continuing until the corrected GA reached 44 weeks or complete vascularization of the peripheral retina.
Study Indicators
Infants were categorized into ROP and non-ROP groups based on screening results and diagnostic criteria. Information on premature infants in both groups was collected, encompassing factors such as GA, BW, ROP staging, rate of weight gain, delivery method, use of invasive ventilation (including tracheal cannula and machine-assisted ventilation), IVF, multiple births (including twins), and presence of comorbidities like NRDS, intracranial hemorrhage, asphyxia, BPD, and PDA. Additionally, data included a history of blood transfusions (such as plasma, red blood cells, and platelets during hospitalization) and maternal comorbidities such as GDM and GH, with GDM diagnosed based on the American Diabetes Association’s Standards of Medical Care in Diabetes-2021,14 and GH diagnosed following the 2020 edition of the Guidelines.15
Stratification into Severe and Mild ROP Groups
Infants with ROP were further allocated into severe and mild ROP groups according to the degree of lesions. The severe ROP group comprised infants who were receiving treatment. Treatment was administered to infants falling within this category with an indication for surgical intervention. Conversely, the mild ROP subgroup included instances of stage 1 and 2 ROP, wherein spontaneous progression to retinal degeneration or complete retinal vascularization occurred by 45 weeks post-gestation. Criteria of treatment were delineated as follows: Infants diagnosed with threshold ROP, pre-threshold type 1 ROP, or AROP received treatment with the anti-vascular endothelial growth factor (VEGF) drug Lucentis. In instances of lesion recurrence or exacerbation post-treatment, a subsequent administration of anti-VEGF or laser treatment ensued. Persistent retinal neovascularization post-anti-VEGF treatment prompted a repetition of laser treatment in the avascular region of the peripheral retina for the management of non-regressed retinal conditions.16,17
Statistical Analysis
Statistical analyses were conducted using SPSS 25.0 software. The measurement data of normal distribution was expressed as mean ± standard deviation and non-normally distributed measurement data was expressed as median with quartiles [M (P25, P75)]. Comparisons of GA, BW, and weight gain rate between mild ROP group and severe group were performed using Wilcoxon rank-sum test. Other measurement data were compared using t test between groups. In addition, comparisons of count data between groups were conducted using chi-squared test. Initially, univariate analyses were conducted to identify pertinent factors associated with ROP. These identified factors were subsequently subjected to rigorous multivariate logistic regression analysis, employing the forward stepwise method to derive their respective odds ratios (OR) and 95% confidence intervals (95% CI). In multivariate logistic regression analysis, count data was transformed. Further, a receiver-operating characteristic (ROC) curve was meticulously constructed for the weight gain rate to prognosticate ROP, and the ensuing area under the curve (AUC) was meticulously calculated to assess the discerning efficacy of the model. Statistical significance was considered at P< 0.05.
Results
General Data
This study encompassed the screening of 230 prematurely born infants, with a distribution of 114 males and 116 females. GA spanned from 25 to 32 weeks, demonstrating an average GA of 30.75 ± 1.25 weeks. BW ranged between 650 and 2000 g, with a mean BW of 1546.52 ± 285.68 g. Notably, 41 infants were identified with ROP, constituting 17.8% of the group (41/230), while 82.2% remained unaffected (189/230).
Within the ROP group, 85.4% of infants (35/41) manifested ROP at stages 1 and 2, 14.6% (6/41) exhibited ROP at stage 3, and none displayed ROP beyond stage 3 (refer to Table 1). Of particular significance, 22.0% of infants in the ROP group (9/41) were diagnosed with severe ROP. These cases were characterized by a GA of 27.17 ± 1.30 weeks and a BW of 886.11 ± 208.13 g. The subgroup of 9 infants comprised 5 males and 4 females. Treatment modalities included laser therapy for 2 infants and intravitreal injection of the anti-VEGF drug (Lucentis) for 7 infants.
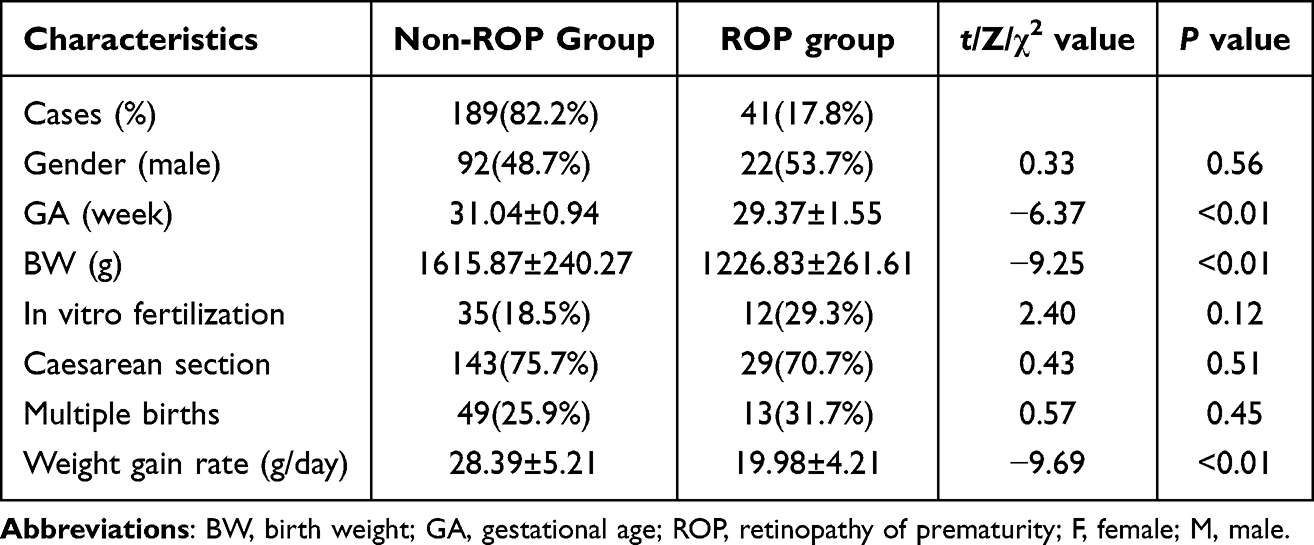 |
Table 1 Baseline Characteristics of Premature Infants |
Univariate Analysis Results
The two groups exhibited significant statistical differences in terms of GA (t = −6.37, P < 0.05), BW (t = −9.25, P < 0.05), weight gain rates (t = −9.69, P < 0.05), the proportion of infants with invasive ventilator-assisted ventilation (χ2 = 25.74, P < 0.05), the proportion of infants combined with NRDS (χ2 = 15.69, P < 0.05), BPD (χ2 = 19.56, P < 0.05), or PDA (χ2 = 5.67, P < 0.05), and the proportion of infants with a history of blood transfusion (χ2 = 18.34, P < 0.05) (Table 2).
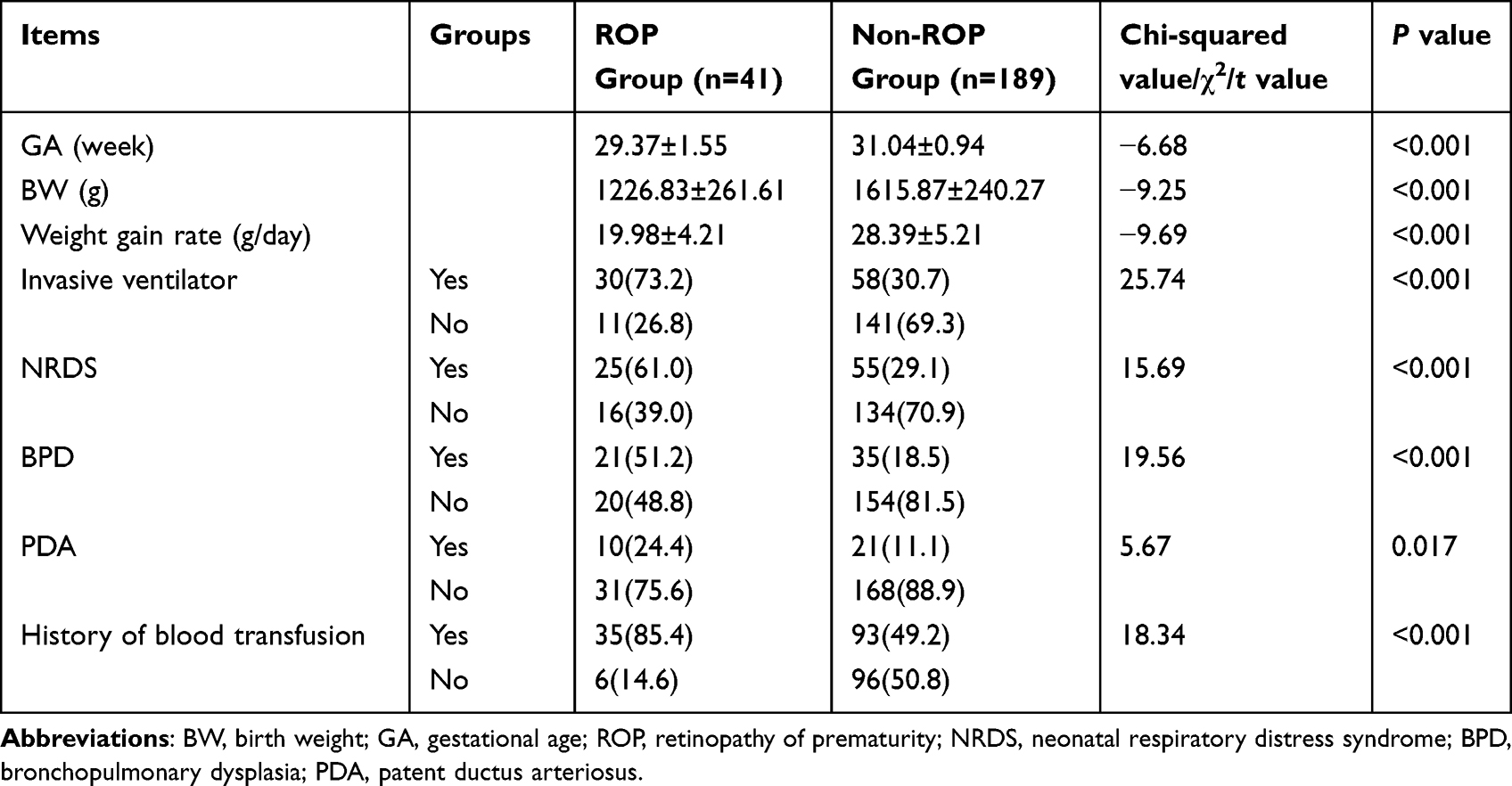 |
Table 2 Univariate Analysis of Factors Influencing ROP |
Conversely, no statistically significant differences was found between the two groups with respect to the proportion of mothers combined with GH (χ2 = 2.76, P = 0.10) or GDM (χ2 = 1.23, P = 0.27), the proportion of infants combined with asphyxia (χ2 = 1.47, P = 0.23), intracranial hemorrhage (χ2 = 1.70, P = 0.192), sepsis (χ2 = 3.41, P = 0.06), or intrauterine infectious pneumonia (χ2 = 4.00, P = 0.05).
Multivariate Logistic Regression Analysis of ROP-Related Factors
The study entailed a multivariate logistic regression analysis utilizing the forward stepwise method. The independent variables comprised factors identified as statistically significant in the univariate analysis. The dependent variable was the presence or absence of ROP. The findings indicated that the occurrence of ROP was associated with GA (OR = 0.91; 95% CI = 0.83−0.99; P = 0.03), BW (OR = 0.99; 95% CI = 0.99−1.00; P = 0.04), and weight gain rates (OR = 0.73; 95% CI = 0.63−0.83; P = 0.00), all identified as risk factors (P < 0.05, Table 3).
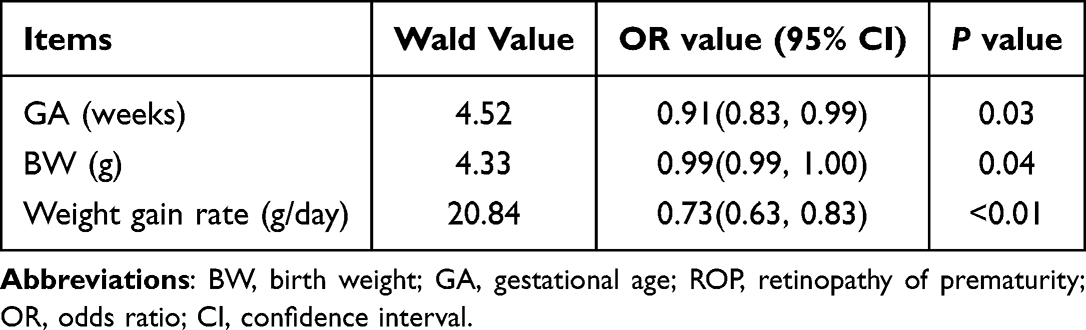 |
Table 3 Multivariate Logistic Regression Analysis of Factors Influencing ROP |
Analysis of Differences Between the Mild and Severe ROP Groups
GA, BW, and weight gain rates were subjected to comparative analysis between the mild and severe ROP groups, employing the Wilcoxon rank-sum test. The t-test outcomes demonstrated statistically significant disparities in GA, BW, and weight gain rates between the two groups (P < 0.05, Table 4).
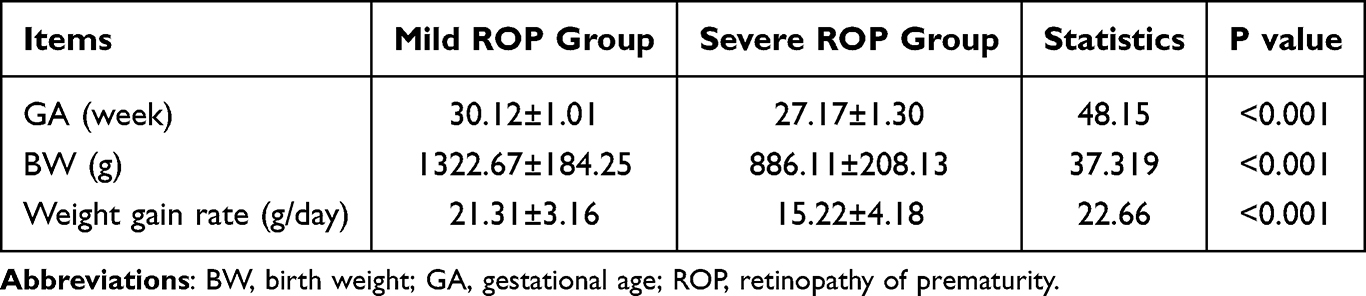 |
Table 4 Comparisons of GA, BW, and Rate of Weight Gain Between the Severe and Mild ROP Groups |
Differences in Weight Gain Rates Between the Mild and Severe ROP Groups
Infants were stratified according to their daily weight gain, utilizing intervals of 10 g/day. Subsequent to this categorization, data analysis ensued employing the chi-squared (χ2) test or, in instances where the expected frequency fell below 5, the exact test. Following these analytical procedures, an ROC curve was constructed, and the standard values and sensitivity were ascertained vis-à-vis specificity. The AUC was subsequently computed as a measure of performance.
The comparative analysis of frequency was conducted between the mild and severe ROP groups. The results delineated a prevailing pattern in the severe ROP group, where the majority of infants (7 out of 9, or 77.78%) exhibited a weight gain rate below 20 g/day. In contrast, the predominant trend in the mild ROP group was characterized by a weight gain rate surpassing 20 g/day for a significant proportion of infants (22 out of 32, or 68.8%). This discernible distinction suggests a lower weight gain rate in the severe ROP cohort relative to its mild counterpart. Furthermore, a notable inverse relationship was observed, indicating a diminishing proportion of infants with severe ROP as the weight gain rate increased, as visually depicted in Figure 1.
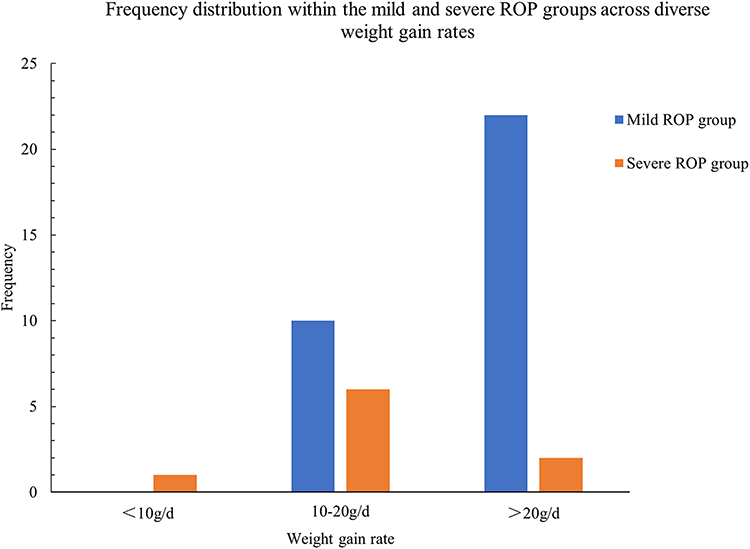 |
Figure 1 Frequency distribution within the mild and severe ROP groups across diverse weight gain rates. Mild ROP group; Severe ROP group; frequency; Weight gain rate. |
The predictive efficacy of the weight gain rate in anticipating the occurrence of ROP was assessed through the construction of an ROC curve. Sensitivity is represented on the y-axis, while (1-specificity) is plotted on the x-axis, with sensitivity and specificity values derived from various cutoff points. Examination of the ROC curve disclosed a notable association between premature infants with a weight gain rate below 24.5 g/day and an elevated susceptibility to ROP (AUC = 0.939; 95% CI = 0.905−0.973; P<0.05) (Figure 2a). The weight gain rate < 24.5 g/day exhibited a sensitivity of 90.2% and specificity of 86.8% in its predictive capacity for ROP.
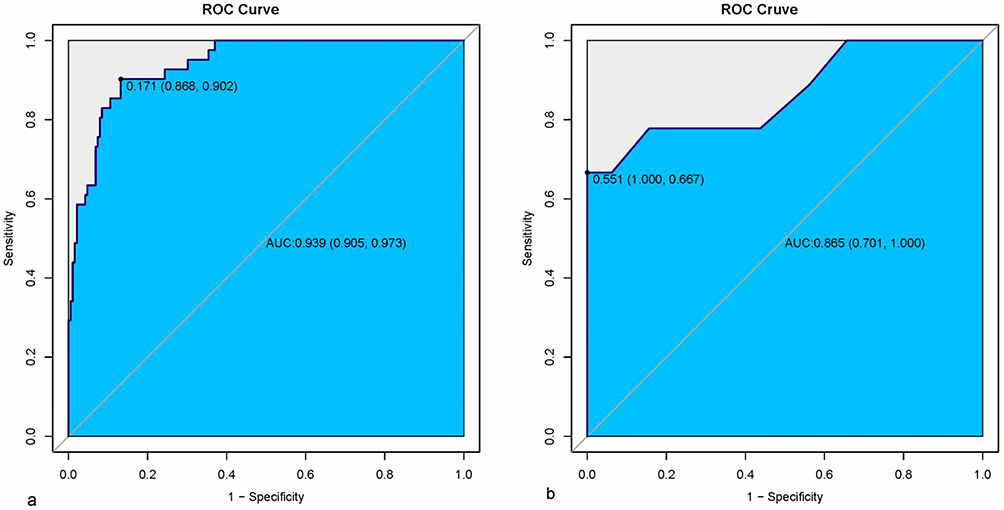 |
Figure 2 ROC curves for the prediction of ROP using the rate of weight gain. (a) The ROC curve for prediction of ROP using rate of weight gain rate (AUC = 0.939; 95% CI = 0.905−0.973; P < 0.05). (b) The ROC curve for prediction of severe ROP using rate of weight gain rate (AUC = 0.865; 95% CI = 0.70−1.00; P < 0.05). Abbreviations: CI, confidence interval; ROC, receiver-operating characteristic; ROP, retinopathy of prematurity. |
Similarly, an additional ROC curve was constructed to assess the accuracy of predicting severe ROP based on the rate of weight gain (see Figure 2b). According to the ROC curve analysis, premature infants manifesting a weight gain rate below 18 g/day were identified as being at a heightened risk of developing severe ROP (AUC = 0.865; 95% CI = 0.70−1.00; P < 0.05). The sensitivity and specificity at the designated threshold of a weight gain rate < 18 g/day for predicting severe ROP were determined to be 100% and 77.8%, respectively.
Discussion
While low GA, BW, and postnatal growth are established risk factors for ROP globally,4–7,18–23 significant knowledge gaps persist regarding their specific predictive utility, particularly for severe ROP, within the unique context of the Chinese preterm population. Existing Chinese studies have reported ROP incidence but often lacked granular analysis of severe ROP or robust evaluation of postnatal WGR as a predictive biomarker. Critically, clinically applicable WGR thresholds to stratify severe ROP risk, essential for optimizing resource-constrained screening programs in regions like China experiencing rapid NICU expansion without commensurate screening infrastructure,11,12 have not been well-defined or validated. This study aimed to specifically address this gap by rigorously evaluating WGR as a predictor for both any ROP and, more importantly, severe ROP in a well-characterized Chinese cohort, and establishing evidence-based WGR cut-offs for clinical risk stratification. Furthermore, we meticulously differentiated distinctions between mild and severe ROP groups, revealing statistically significant differences in BW and GA. This underscores the nuanced role of BW and GA, particularly in the context of severe ROP. Specifically, diminished GA and BW correlate with an augmented predisposition to severe ROP. Against the backdrop of an escalating survival rate among premature infants in China, the attendant risk of severe ROP is concomitantly surging. In light of these emergent trends, clinicians must intensify surveillance protocols and institute timely interventions for these vulnerable infants, thereby preempting the advent of deleterious complications.
Increasing attention is being directed toward the examination of postnatal factors in relation to ROP among premature infants. A focal point of research interest lies in exploring the correlation between weight gain and nutritional support and their impact on ROP. Scholars propose that postnatal weight gain assumes a pivotal role as a predictive factor for ROP occurrence in premature infants.21–23 Several studies have put forth the notion that the rate of weight gain may serve as a substitute for serum insulin-like growth factor (IGF-1) and VEGF as a critical predictor of ROP.24,25
In a retrospective analysis encompassing premature infants with a GA of ≤ 30 weeks and BW of ≤ 1500 g, McCauley et al observed a heightened risk of severe ROP among infants with a weight gain rate of less than 23 g/day. Employing the weight gain rate as a significant predictor of ROP, they proposed a substantial reduction in the number of ophthalmologic tests without a concurrent increase in missed diagnoses.26 Doshi et al conducted a screening study for ROP in western India, noting that infants with ROP exhibited a mean weight gain rate of 18.21 (±10.84) g/day, while those with severe ROP had a mean weight gain rate of 11.56 (±7.77) g/day. Their hypothesis centered on the relevance of a low weight gain rate to the occurrence of severe ROP.27 However, there was limited studies concerning weight gain rate and ROP in premature infants in our country. Similarly, the present study, involving a retrospective analysis of 230 premature infants with GA ≤ 32 weeks and BW ≤ 2000 g, identified the weight gain rate as a risk factor for ROP development. Notably, among the 41 infants with ROP, those with severe ROP (9 infants) had an average weight gain rate of 15.22 g/day, while the mild ROP group exhibited a rate of 21.31 g/day, and the non-ROP group showed a rate of 28.39 ± 5.21 g/day. These findings suggest that a lower weight gain rate is indicative of a higher risk of both ROP and severe ROP. Consistent with findings of Doshi et al, the results indicated association between weight gain rate and high incidence of ROP in our country. More attention should be paid to weight gain rate of premature infants, for that infants with low weight gain rate are more likely to develop ROP and even severe ROP.
Despite the normal weight gain rate being approximately 25−30 g/day in the first 3 months post-birth, premature infants, owing to the immaturity of their systems and organs, require a combination of enteral and parenteral nutrition to sustain growth and development.28 Insufficient caloric supply at an early stage can impede the division of retinal vascular epithelial cells, leading to impaired retinal maturation. Low levels of IGF-1 fail to adequately activate retinal VEGF, resulting in poor retinal vascular growth and the eventual development of ROP. Notably, IGF-1 levels correlate with postnatal weight gain rates. However, while IGF-1 requires a blood test, the weight gain rate can be easily measured. Consequently, the weight gain rate may serve as a viable substitute for IGF-1 as a marker for ROP, a hypothesis corroborated by our findings that infants with a lower weight gain rate manifested more severe ROP.
The core innovation and clinical significance of our findings lie in the establishment of validated WGR thresholds (<24.5 g/day for any ROP; <18 g/day for severe ROP) within a Chinese cohort. These thresholds provide quantifiable, easily measurable targets that significantly enhance risk prediction beyond GA and BW alone, particularly for identifying infants at highest risk of vision-threatening severe ROP. This is a crucial advancement for the Chinese setting, where optimizing screening efficiency is paramount. Our findings thus bridge the gap between a measurable clinical parameter (WGR) and the underlying pathophysiology, offering a practical tool for risk assessment. While McCauley et al26 and Doshi et al27 reported associations between low WGR and ROP/severity, our study is the first to define and validate specific WGR cut-offs predictive of severe ROP risk within the Chinese preterm population, directly addressing the critical need for locally applicable risk stratification tools. Our validated WGR thresholds have direct and significant implications for refining ROP screening protocols in China, directly addressing the challenge of balancing screening sensitivity with resource constraints and infant burden. Integrating WGR into risk stratification models offers a clear pathway to personalized screening: Infants with WGR ≥ 24.5 g/day, despite meeting traditional GA/BW criteria, may represent a lower-risk subgroup. For these infants, screening intensity or frequency could potentially be safely reduced after initial assessment, significantly alleviating the burden of frequent, costly, and distressing examinations without compromising detection of significant disease. Conversely, infants with WGR < 18 g/day demand the highest vigilance and constitute the highest-risk group for severe ROP. This threshold serves as a critical red flag, warranting more frequent or prioritized screening schedules regardless of GA/BW being borderline, ensuring that sight-threatening disease is detected at the earliest possible stage for timely intervention (eg, anti-VEGF therapy). Implementing this WGR-stratified approach holds substantial promise for transforming ROP management in China: it can dramatically reduce unnecessary examinations and associated costs/discomfort for lower-risk infants while concentrating limited resources on those infants at the quantifiable highest risk of severe, vision-threatening ROP. This represents a tangible step towards more efficient, targeted, and patient-centered screening. In subsequent clinical endeavors, vigilant scrutiny of weight gain and nutritional status of premature infants is recommended. This proactive stance holds promise in augmenting ROP prediction, enabling the timely identification of infants at elevated risk for both ROP and severe ROP, thereby facilitating early diagnostic and therapeutic interventions.
Our study also demonstrated that the utilization of invasive ventilator-assisted ventilation did not amplify the susceptibility to ROP. In contrast, certain studies have revealed an association between the use of invasive ventilators and an increased risk of ROP. These studies suggest factors such as hyperbaric oxygen exposure and fluctuating oxygen levels during mechanical ventilation may influence the development of retinal vasculature, or that invasive ventilator-assisted ventilation may directly contribute to lung injury.29
In China, oxygen therapy is indicated for premature infants experiencing respiratory distress, arterial partial pressure of oxygen below 50 mmHg, or transcutaneous oxygen saturation on inhaled air below 85%. Accordingly, we propose that maintaining strict adherence to the prescribed indications for oxygen therapy during the treatment and rescue of preterm infants is crucial. Furthermore, we assert that with a judicious understanding and application of the criteria for the use of invasive ventilators, their use does not heighten the risk of ROP.
In mainland China, a study conducted by Zhou et al in 2015 revealed a prevalence of 15.2% for ROP among premature infants with a GA of 34 weeks or less. This cohort exhibited a distribution of 92.3% for mild ROP (stages 1 and 2) and 7.7% for severe ROP (stages 3 and above).30 In our study, we identified a prevalence of 17.8% for ROP in premature infants with a GA ≤ 32 weeks. Within this group, 85.4% (35/41) presented with mild ROP (stages 1–2), while 14.6% exhibited severe ROP (stages 3 and above). The disparity in prevalence rates can be attributed to different participant selection criteria, wherein a diminutive GA is concomitant with an augmented susceptibility to ROP manifestation.
Despite these promising implications, several critical research gaps remain that warrant further investigation to fully realize the potential of WGR in clinical practice. Firstly, our study established WGR thresholds within a specific cohort (GA ≤ 32 weeks, BW ≤ 2000 g). The generalizability and optimal thresholds for subpopulations with even lower GA/BW (eg, < 28 weeks, BW < 1000 g) or in diverse geographic/ethnic settings within China need prospective validation in larger, multi-center cohorts. Such studies should specifically assess whether the identified thresholds (24.5 g/day and 18 g/day) require adjustment for these higher-risk subgroups or different healthcare environments. Secondly, while we identified WGR as a powerful predictor, the precise biological mechanisms linking suboptimal weight gain to severe ROP pathogenesis, particularly the dynamics of IGF-1 and VEGF signaling in relation to longitudinal WGR patterns in the Chinese population, require deeper mechanistic exploration. Future studies integrating serial measurements of IGF-1, VEGF, and other relevant biomarkers alongside meticulous WGR tracking could elucidate these pathways and potentially identify even earlier or more specific predictive signatures. Thirdly, translating these WGR thresholds into optimized, cost-effective screening algorithms demands implementation research. Future work should focus on developing and prospectively evaluating integrated risk prediction models that combine GA, BW, WGR, and potentially other readily available clinical factors (eg, oxygen duration, comorbidities like BPD). Crucially, the impact of incorporating WGR on real-world screening efficiency (reduction in examinations), cost savings, workload burden on NICUs and ophthalmology services, and crucially, the sensitivity and specificity for detecting all treatable ROP (ensuring no severe cases are missed) must be rigorously assessed in operational settings. Cost-effectiveness analyses comparing WGR-stratified screening versus standard GA/BW-based protocols are essential to guide policy decisions in resource-constrained settings. Fourthly, the interplay between nutritional strategies, WGR, and ROP risk needs clarification. Future research should investigate whether specific nutritional interventions aimed at optimizing postnatal growth trajectories can demonstrably reduce the incidence of severe ROP. Randomized controlled trials evaluating targeted nutritional support for infants identified as high-risk based on early WGR patterns would be highly valuable.
Despite its potential benefits, translating WGR-based stratification into routine practice faces practical hurdles. Key barriers include: (1) Ensuring consistent and accurate WGR measurement across diverse NICUs, requiring standardized protocols for weighing timing and technique; (2) Integrating WGR calculation and risk flagging into clinical workflows, necessitating health IT system adaptations; (3) Fostering effective interdisciplinary collaboration between neonatology, nursing, nutrition, and ophthalmology teams. Addressing these operational challenges is crucial for successful real-world adoption.
Conclusion
In this retrospective cohort study of 230 Chinese preterm infants (GA ≤ 32 weeks, BW ≤ 2000 g), we identified low GA, low BW and diminished postnatal WGR as significant independent risk factors for the development of ROP. Crucially, we established and validated clinically applicable WGR thresholds predictive of ROP risk within this population: a WGR < 24.5 g/day was significantly associated with any ROP, and a WGR < 18 g/day specifically predicted severe ROP. These findings underscore the critical role of postnatal growth velocity, measured simply by WGR, as a robust predictor, particularly for severe disease. Integrating WGR thresholds into existing GA/BW-based screening protocols offers a promising strategy for personalized risk stratification. This approach has the potential to significantly reduce the frequency of unnecessary, costly, and distressing fundus examinations for lower-risk infants while ensuring intensified surveillance and timely intervention for those infants at the highest quantifiable risk of vision-threatening severe ROP, thereby improving both clinical outcomes and resource allocation.
While this study provides valuable insights and practical thresholds, several limitations warrant consideration. Firstly, the retrospective design at a single center inherently limits causal inference and may introduce selection bias. Secondly, the sample size, particularly for the severe ROP subgroup, though sufficient for initial threshold derivation, necessitates validation in larger, prospective cohorts. Thirdly, our cohort focused on infants with GA ≤ 32 weeks and BW ≤ 2000 g; the generalizability of the specific WGR thresholds (24.5 g/day and 18 g/day) to extremely preterm infants (eg, GA < 28 weeks, BW < 1000 g) or diverse geographic/ethnic populations within China requires confirmation. Fourthly, we excluded infants with major congenital anomalies or metabolic diseases, potentially limiting applicability to these high-risk subgroups. Finally, longer-term follow-up data on visual outcomes beyond the screening period were not available. Future research should focus on validating these findings in larger, multi-center cohorts and exploring the biological mechanisms underpinning the link between weight gain and ROP. Additionally, further work is needed to integrate these findings into practical clinical tools and assess their impact on clinical outcomes.
Abbreviations
GA, Gestational Age; BW, Birth Weight; ROP, Retinopathy of Prematurity; NRDS, Neonatal respiratory distress syndrome; BPD, Bronchopulmonary Dysplasia; PDA, Patent ductus arteriosus; IGF-1, Insulin-like growth factor IL; VEGF, Vascular endothelial growth factor; AP-ROP, ROP Acute poirier retinopathy of prematurity.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Hebei General Hospital (No.2023184). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from the guardians of all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
Medical Science Research Topic in Hebei Province (20200719).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Higgins Rosemary D. Oxygen saturation and retinopathy of prematurity. Clin Perinatol. 2019;46(3):593–599. doi:10.1016/j.clp.2019.05.008
2. Kim SJ, Port AD, Swan R, et al. Retinopathy of prematurity: a review of risk factors and their clinical significance. Surv Ophthalmol. 2018;63(5):618–637. doi:10.1016/j.survophthal.2018.04.002
3. Nedime S-K, Imren A, Birgin T. Favorable outcomes in the treatment of aggressive posterior retinopathy of prematurity. Eur J Ophthalmol. 2021;31(1):179–183. doi:10.1177/1120672119886989
4. Rivera-Rueda MA, Fernandez-Carrocera LA, Bsalgado-Valladares M, et al. Retinopathy of prematurity, frequency and risk factors in very low birth weight infants. Boletin Medico del Hospital Infantil de Mexico. 2020;77(3):135–141. doi:10.24875/BMHIM.19000203
5. Fierson WM. American Academy of Pediatrics Section on Ophthalmology, American Academy of Ophthalmology, American Association for Pediatric Ophthalmology and Strabismus, American Association of Certified Orthoptists. Screening examination of premature infants for retinopathy of prematurity. Pediatrics. 2018;142(6):e20183061. doi:10.1542/peds.2018-3061
6. Chan H, Cougnard-Grégoire A, Korobelnik JF, et al. Screening for retinopathy of prematurity by telemedicine in a tertiary level neonatal intensive care unit in France: review of a six-year period. J Francais D Ophalmol. 2018;41:926–932.
7. Fierson WM, Saunders RA, Good W, American Academy of Pediatrics Section on Ophthalmology, American Academy of Ophthalmology. Screening examination of premature infants for retinopathy of prematurity. Pediatrics. 2013;131(1):189–195. doi:10.1542/peds.2012-2996
8. Ingolfsland EC, Haapala JL, Buckley LA, et al. Late growth and changes in body composition influence odds of developing retinopathy of prematurity among preterm infants. Nutrients. 2019;12(1):78. doi:10.3390/nu12010078
9. Lundgren P, Stoltz Sjöström E, Domellöf M, et al. WINROP identifies severe retinopathy of prematurity at an early stage in a nation-based cohort of extremely preterm infants. PLoS One. 2013;8(9):e73256. doi:10.1371/journal.pone.0073256
10. Yoon YM, Shin SH, Park CW, Kim EK, Kim HS. Correlation between histologic chorioamnionitis and severe retinopathy of prematurity. Pediatr Res. 2025. doi:10.1038/s41390-025-04093-y
11. Coyner AS, Oh MA, Shah PK, et al. External validation of a retinopathy of prematurity screening model using artificial intelligence in 3 low- and middle-income populations. JAMA Ophthalmol. 2022;140(8):791–798. doi:10.1001/jamaophthalmol.2022.2135
12. Du J, Chen X, Wang Y, et al. Regional variations in retinopathy of prematurity incidence for preterm infants <32 weeks’ gestation in China. Public Health. 2024;226:91–98. doi:10.1016/j.puhe.2023.10.033
13. Chiang MF, Quinn GE, Fielder AR, et al. International classification of retinopathy of prematurity, third edition. Ophthalmology. 2021;128(10):e51–e68. doi:10.1016/j.ophtha.2021.05.031
14. Pregnancy-induced Hypertension Group, Chinese Society of Obstetrics and Gynecology. Guidelines for Diagnosis and Treatment of pregnancy-induced Hypertension (2020). Chin J Obstetrics Gynecol. 2021;55(04):227–238. Chinese.
15. Dwivedi D, Dwivedi A, Lakhtakia S, et al. Prevalence, risk factors and pattern of severe retinopathy of prematurity in eastern Madhya Pradesh. Ind J Ophthalmol. 2019;67(6):819–823. doi:10.4103/ijo.IJO_1789_18
16. Group of Ophthalmology, Society of Pediatrics, Chinese Medical Association. Expert consensus on treatment norms for retinopathy of prematurity. Chin J Fundus Dis. 2022;38(1):10–13. Chinese.
17. Pediatric Retinology Group, Ophthalmology Professional Committee, Cross-Straits Medicine Exchange Association; Ophthalmology Group, Ophthalmology Society of Chinese Medical Association. Expert consensus on intravitreal injection of anti-vascular endothelial growth factor for treatment of retinopathy of prematurity. Chin J Fundus Dis. 2021;37(11):836–840. Chinese.
18. Hartnett ME, Penn JS. Mechanisms and management of retinopathy of prematurity. N Engl J Med. 2012;367(12):2515–2526. doi:10.1056/NEJMra1208129
19. Bas AY, Demirel N, Koc E, et al. Incidence, risk factors and severity of retinopathy of prematurity in Turkey (TR-ROP study): a prospective, multicentre study in 69 neonatal intensive care units. Br J Ophthalmol. 2018;102(12):1711–1716. doi:10.1136/bjophthalmol-2017-311789
20. Acevedo Castellon R, Ramirez-Neria P, Garcia-Franco R. Incidence of retinopathy of prematurity type 1 and type 2 in a regional Hospital of Social Security in the state of Queretaro, Mexico (2017-2018). BMC Ophthalmol. 2019;19(1):91. doi:10.1186/s12886-019-1095-0
21. Ying GS, Bell EF, Donohue P, et al. Perinatal risk factors for the retinopathy of prematurity in postnatal growth and ROP study. Ophthalmic Epidemiol. 2019;26(4):270–278. doi:10.1080/09286586.2019.1606259
22. Lv Z, Mao JB, Chen YQ, et al. Correlation analysis between the growth rate of body mass in very low birth weight preterm infants and severe retinopathy of prematurity. Chin J Fundus Dis. 2016;32(2):172–176. Chinese.
23. Wang ZH, Gao PF, Bai H, et al. Postnatal weight gain in very low birth weight infants in Beijing and the risk of retinopathy of prematurity. Int J Ophthalmol. 2015;8(6):1207–1210. doi:10.3980/j.issn.2222-3959.2015.06.23
24. Jensen AK, Ying GS, Huang J, et al. Postnatal serum insulin-like growth factor I and retinopathy of prematurity. Retina. 2017;37(5):867–872. doi:10.1097/IAE.0000000000001247
25. Lundgren P, Wilde Å, Löfqvist C, et al. Weight at first detection of retinopathy of prematurity predicts disease severity. Br JOphthalmol. 2014;98(11):1565–1569. doi:10.1136/bjophthalmol-2014-304905
26. Mcauley K, Chundu A, Song H, et al. Implementation of a clinical prediction model using daily postnatal weight gain, birth weight, and gestational age to risk stratify ROP. Pediatr Ophthalmol Strabismus. 2018;55(5):326–334. doi:10.3928/01913913-20180405-02
27. Doshi S, Desai S, Nanavati R, et al. Children’s hospital of philadelphia score to predict severe retinopathy in Indian preterm infants. EYE. 2019;33(9):1452–1458. doi:10.1038/s41433-019-0431-1
28. Patel JK, Rouster AS. Infant nutrition requirements and options. In: StatPearls. Treasure Island (FL): Stat Pearls Publishing; 2021.
29. Pastro J, Brgo T. Influence of oxygen in the development of retinopathy of prematurity. Rev Bras Enferm. 2019. 72(3):592–599. English, Portuguese. PMID: 31269121. doi: 10.1590/0034-7167-2018-0361.
30. Zhou YQ, Chen C, Chen L, et al. Multicenter survey on the clinical features and fundus lesions of retinopathy in premature infants in mainland China. Chin J Evidence-based Pediatrics. 2015;10(3):161–165. Chinese.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Incidence and Risk Factors for Retinopathy of Prematurity in a Tertiary Hospital in China
Hu X, Zhang J, Zhang M, Chen X, Han S, Zhu J
Clinical Ophthalmology 2023, 17:3189-3194
Published Date: 25 October 2023
Causal Association of Primary Biliary Cholangitis with Adverse Pregnancy and Neonatal Outcomes: A Two-Sample Mendelian Randomization Study
Li R, Tan J, Yang X, Ning Z
International Journal of Women's Health 2025, 17:407-415
Published Date: 17 February 2025