Back to Journals » Journal of Inflammation Research » Volume 19
Body Weight-Related Differences in Adipokines and Inflammatory Markers Among Women with Systemic Lupus Erythematosus
Authors Carvalho LM, Da Mota JC, Ribeiro AA, Souza LL, Sales RCDS, Gualano B, Martínez-Urbistondo M, Martínez JA, Borba EF, Nicoletti CF
Received 18 November 2025
Accepted for publication 22 February 2026
Published 28 February 2026 Volume 2026:19 579501
DOI https://doi.org/10.2147/JIR.S579501
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chaim Putterman
Lucas M Carvalho,1,2 Jhulia CNL Da Mota,1,2 Amanda A Ribeiro,1,2 Leticia L Souza,1,2 Ruan Célio dos Santos Sales,1,2 Bruno Gualano,1– 4 María Martínez-Urbistondo,5 J Alfredo Martínez,6,7 Eduardo F Borba,3 Carolina F Nicoletti1– 3
1Applied Physiology and Nutrition Research Group – School of Physical Education and Sport and Faculdade de Medicina FMUSP, Universidade de Sao Paulo, Sao Paulo, SP, Brazil; 2Center of Lifestyle Medicine, Faculdade de Medicina FMUSP, Universidade de São Paulo, Sao Paulo, SP, Brazil; 3Rheumatology Division, Hospital das Clínicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Sao Paulo, SP, Brazil; 4Laboratory of Assessment and Conditioning in Rheumatology; Hospital Das Clínicas HCFMUSP, Faculdade de Medicina FMUSP, Universidade de São Paulo, Sao Paulo, SP, Brazil; 5Internal Medicine Service, Puerta de Hierro University Hospital of Majadahonda, Majadahonda, Spain; 6Precision Nutrition and Cardiometabolic Health, IMDEA Food, Madrid, Spain; 7Biomedical Research Centre for Obesity Physiopathology and Nutrition Network (CIBEROBN), Instituto de Salud Carlos III (ISCIII), CIBERON, Madrid, Spain
Correspondence: Carolina F Nicoletti, Rheumatology Division, Faculty of Medicine, University of São Paulo, Av. Dr Arnaldo, 455 – 3rd Floor Room 3148, São Paulo, SP, 01246-903, Brazil, Tel +55 11 30618789, Email [email protected]
Background: Systemic lupus erythematosus (SLE) is an autoimmune disease marked by chronic inflammation and frequent metabolic disturbances. Understanding the influence of body weight and hydroxychloroquine on adipokines and inflammatory markers may clarify their role in SLE progression.
Purpose: This study examined metabolic health, adipose tissue gene expression, and serum adipokine and inflammatory profiles in normal-weight (NW) and excess body weight (EBW) female patients with SLE and explored associations with disease activity and hydroxychloroquine (HCQ) use.
Patients and methods: Fifty women with SLE were classified as NW or EBW. Laboratory analyses included antibodies against double-stranded DNA, complement components (C3, C4), fasting glucose, triglycerides, total and fractionated cholesterol, and C-reactive protein (CRP). Subcutaneous adipose tissue gene expression was assessed by real-time PCR.
Results: Mean age, disease duration, and SLEDAI-2K scores were similar between groups (p > 0.05). HCQ dose adjusted by body weight was lower in EBW patients (p < 0.05). EBW patients had higher total cholesterol, LDL-c, CRP, and leptin, with lower adiponectin and reduced adiponectin/leptin ratio (p < 0.05). Adipose tissue expression of TNF-α, LEP, IL-6, and ADIPOQ was elevated in EBW (p < 0.05). Stratifying by adipo/lep ratio (≤ 5 vs > 5) showed similar disease activity (p > 0.05), though patients with preserved adipose function (ratio > 5) had higher serum C4 (p = 0.004) and a trend for increased C3 (p = 0.055). Multiple regression indicated HCQ dose (mg/kg/day) was inversely associated with abdominal circumference (β = − 0.43; p = 0.003) and fat mass(β = − 0.38; p = 0.009) and positively associated with adiponectin (β = 0.45; p = 0.002) and adipo/lep ratio (β = 0.39; p = 0.009). Higher HCQ doses tended to increase HDL-C (p = 0.059) and reduce leptin (p = 0.058).
Conclusion: Excess body weight in SLE is linked to an adverse adipokine profile and increased inflammation, raising metabolic and cardiovascular risk. Weight-adjusted HCQ shows protective effects on adipose metabolism, HDL-c, and adiponectin. These findings emphasize individualized, weight-based HCQ therapy and early adipose biomarker assessment to guide precision medicine in SLE management.
Keywords: systemic lupus erythematosus, adipose tissue, obesity, gene expression, adipo/lep ratio, cardiometabolic
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune inflammatory disease that affects millions of individuals worldwide,1 with a predominance in female gender.2 The pathophysiology of SLE involves a complex interplay of environmental, hormonal, and genetic/epigenetic factors3,4 that lead to the production of autoantibodies against cellular antigens, promoting excessive immune activation and resulting in progressive inflammation and tissue damage.5 The immune dysregulation in SLE is largely driven by the inflammatory response of autoreactive CD4+ T lymphocytes. These cells initiate a cascade of events that lead to the overproduction of pro-inflammatory cytokines, including interleukin (IL)-6, IL-2, IL-17, IL-22, and tumor necrosis factor (TNF)-α.6,7 Clinical manifestations are notably complex and diverse, reflecting the multifaceted nature of this autoimmune disease.8 Common manifestations include skin lesions (the most frequent one), joint involvement, nephritis, neuropsychiatric symptoms, and hematological abnormalities.5,9
The treatment of SLE focuses on symptom control, complication prevention, and reducing organ damage. This therapeutic approach typically includes medications such as glucocorticoids, immunosuppressants, and antimalarial drugs, complemented by lifestyle modifications like physical exercise and dietary adjustments.10 Antimalarial drugs, particularly hydroxychloroquine (HCQ), play a crucial role in SLE management by controlling inflammation, reducing disease activity, and preventing organ damage.10–12 Beyond these immunomodulatory effects, HCQ has demonstrated significant metabolic benefits. Studies indicate that HCQ use is associated with a 71% reduction in the prevalence of metabolic syndrome among patients, highlighting its potential to mitigate metabolic risks commonly seen in SLE.13–17 Additionally, HCQ appears to exert a protective effect against the adverse metabolic consequences of corticosteroid therapy, improving lipid profiles and enhancing insulin sensitivity in patients with SLE.18
The presence of metabolic disorders in SLE adds complexity to disease management, potentially impacting symptom severity, disease progression, and treatment efficacy.19–21 Obesity potentially accelerates the progression of SLE,22,23 likely due to adipose tissue (AT) accumulation, which plays significant immunometabolic effects.24–26 Several studies have shown a link between chronic low-grade inflammation due to excess AT and poor outcomes in SLE,27–30 such as an increase exacerbation of disease activity,23 impairment of renal function,31 and worsening of cognitive and functional capacity,32 as well as overall quality of life.33 Additionally, excess AT is known to contribute to endothelial dysfunction, thereby increasing the risk of cardiovascular disease in patients with SLE.34,35 Morphological changes in AT associated with obesity are driven by the activation of immune cells and the secretion of key adipokines such as leptin, adiponectin, and inflammatory cytokines.36 Moreover, hypertrophy and hyperplasia of the AT lead to tissue expansion, resulting in hypoxia and increased lipolysis rates. This, in turn, promotes elevated fatty acid circulation, insulin resistance, and increased oxidative stress.20,37
As for AT, body mass index (BMI) also positively associates with serum leptin38,39 and negatively with serum adiponectin.40 However, there are conflicting results regarding adipokine levels in SLE.41–43 Some studies have reported elevated serum levels of leptin44,45 and adiponectin43,46 in patients with SLE compared to controls, but the precise mechanisms remain unclear. A recent meta-analysis that included 34 studies (1,844 SLE patients and 1,511 healthy controls) revealed elevated plasma leptin levels in SLE.47 In contrast, other recent studies have demonstrated either unchanged or decreased levels in SLE patients.48,49 Given the role of body fatness in these parameters, it is possible to speculate that nutritional status could partially explain this discrepancy.
This study aimed to investigate the influence of body weight on serum adipokine profiles and adipose tissue gene expression in women with SLE. Specifically, it evaluated leptin, adiponectin, the adiponectin-to-leptin ratio, IL-6, and TNF-α according to nutritional status, and explored their associations with metabolic, anthropometric, and immunological parameters. In addition, the study examined the relationship between HCQ dosage and metabolic–inflammatory markers to elucidate potential protective metabolic effects of HCQ in SLE.
Patients and Methods
Study Design and Patients Selection
We performed a cross-sectional study nested within a randomized controlled trial (clinicaltrials.org: NCT05097365).50 Consecutive recruitment was conducted at the Lupus Outpatient Clinic of the Rheumatology Division, HCFMUSP, and all patients fulfilled the 2019 European League Against Rheumatism and American College of Rheumatology (EULAR/ACR) classification criteria for SLE.51 Inclusion criteria were as follows: 1. female gender; 2. pre-menopausal status, 3. aged between 18 and 45 years; 4. inactive disease (SLEDAI-2K score ≤ 4);52 5. prednisone uses ≤ 10 mg/day, 6. hydroxychloroquine use at a stable dose at least 3 months, 7. BMI greater than 18.5 kg/m2. Additionally, exclusion criteria included 1. current chronic disease (diabetes mellitus, arterial hypertension, or cancer), 2. current smokers, 3. use of anticoagulants, 4. current methotrexate use, 5. current infection, 6. pregnancy, 7. current use of any supplementation with methyl donor micronutrients (eg vitamin B12, folic acid), 8. cognitive dysfunctions that impede adequate comprehension of the intervention recommendations.
Patients with SLE were categorized into two groups based on nutritional status according to BMI: Normal Weight (NW) group (BMI between 18.5 and 24.9 kg/m2) and Excess Body Weight (EBW) group (BMI ≥ 25 kg/m2).
Ethical Considerations
Ethical approval was obtained by the Ethics Committee of the Clinical Hospital of the Faculty of Medicine of the University of São Paulo (CAAE.: 47,317,521.8.0000.0068). All participants signed the Informed Consent Form. All procedures were carried out following ethical standards and recommendations of the Declaration of Helsinki.
Patients Protocol
Patients with SLE attended our laboratory and completed phenotypic assessments (clinical, anthropometric, and biochemical). Personal characteristics (ie age, self-declared race, previous smoking history) and disease parameters [ie disease duration and disease activity (according SLEDAI-2K)],53 and current drug therapy were obtained during personal interview and medical records. Patients were evaluated during periods of clinical remission, defined by low disease activity (SLEDAI-2K), to minimize the influence of active clinical manifestations on metabolic and inflammatory outcomes.
Blood samples were collected for biochemical analysis. In addition, patients had adipose tissue collected via percutaneous biopsies for gene expression analysis. Immediately after the biopsy procedure, the adipose tissue sample was placed in a cryogenic tube and immersed in liquid nitrogen solution for instant freezing.
Anthropometric Analysis
For weight and height measurements, a Filizola scale (Campo Grande, MS, Brazil), 1–200 kg, with an error margin of 50 g and a stadiometer coupled to the same Filizola scale were used, respectively. The formula BMI = weight (kg)/height (m2) was applied to BMI calculation. For abdominal circumference measurements, a plastic tape measure was placed midway between the lowest rib and the iliac crest. Abdominal obesity was considered if the abdominal circumference was ≥80 cm.54
Serum Biochemical Analysis
Laboratory measures included serum levels of serum antibodies against double-stranded DNA (anti-dsDNA) detected by enzyme-linked immunosorbent assay (ELISA) (INOVA Diagnostics Inc., San Diego, CA) and confirmed by indirect immunofluorescence within Crithidia luciliae; serum complement levels (C3 and C4) [measured by immunoturbidimetric assay], fasting blood glucose, triglycerides, total cholesterol and its fractions [measured by the enzymatic colorimetric technique], and C-reactive protein (CRP) [measured by the immunoturbidimetric technique].
The analysis of serum leptin and adiponectin was performed using the commercial kit MILLIPLEX MAP Human Adipocyte Magnetic Bead Panel – Endocrine Multiplex Assay and TNF-α and IL-6 were assessed by MILLIPLEX® Human Cytokine/Chemokine/Growth Factor Panel A – Immunology Multiplex Assay (Millipore, Missouri, USA) on a Luminex® analyzer (Luminex®, MiraiBio, USA) according to the manufacturer’s instructions. Finally, the data obtained were normalized and expressed using Milliplex Analyst 5.1 software (EMD Millipore). The adiponectin:leptin (adipo/lep) ratio was determined using the equation: (adiponectin (μg/mL)/leptin (ng/mL).55 Adipo/lep ratio of <0.5 indicates a severe increase in cardiometabolic risk.56
TNF-α, IL6, LEP, and ADIPOQ Gene Expression Analysis
RNA was extracted using the RNeasy Mini Kit (Qiagen) according to the manufacturer’s instructions and cDNA synthesis was carried out with the High-Capacity cDNA Reverse Transcription Kit (Applied Biosystems), following the manufacturer’s guidelines on a thermocycler (MJ Research PTC-100®). Expression of TNF-α, IL6, LEP, and ADIPOQ genes were analyzed in duplicate using quantitative real-time polymerase chain reaction (PCR) on a Step One Plus Real-Time PCR System (Applied Biosystems). The reaction included 10 ng of cDNA, TaqMan MGB 6-FAM fluorogenic probes (Applied Biosystems), and TaqMan™ Gene Expression Master Mix (Applied Biosystems). The thermal cycling conditions were 50°C for 2 minutes, 95°C for 10 minutes, followed by 40 cycles of denaturation at 95°C for 15 seconds, and annealing/extension at 60°C for 60 seconds. Relative expression levels were calculated using the 2-ΔΔCt method57 with glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and beta-actin (ACTB) as endogenous controls.58,59 Relative gene expression was calculated using the comparative Ct (2−ΔΔCt) method, with the normal-weight group used as the calibrator (expression = 1).
Statistical Analysis
All analyses were conducted using the Statistical Package for the Social Sciences (SPSS version 22.0 [IBM Corp., Chicago, IL]). Variables were reported as mean and standard deviation. The normality of data distribution was assessed using the Shapiro–Wilk test. Independent samples t-tests and Mann–Whitney tests were employed to compare numeric variables between groups. Multiple linear regression was used to determine the contribution of HCQ use (per kg) to lipid profile, leptin, adiponectin serum levels and adipo/lep ratio, as well as, the contribution of leptin, adiponectin serum levels to metabolic parameters. Separate linear regression models were constructed for each outcome variable. Statistical significance was set at 5% (p < 0.05).
Results
Participant Characteristics
Fifty patients with SLE were enrolled in this study; classified according to BMI as normal weight (NW; n= 23) and excess body weight (EBW; n = 27). As expected, BMI, abdominal circumference, and body fat percentage were significantly higher in the EBW group compared with normal-weight women (p < 0.001). Additionally, the EBW group had elevated serum levels of total cholesterol, LDL-c, and CRP compared to the NW group (p < 0.05) (Table 1). The groups were comparable in age, disease duration, SLEDAI scores, anti-dsDNA, and complement C3 and C4 levels (all p > 0.05), confirming that disease activity was similarly low across participants. HCQ use by body weight (mg/kg/day) was higher in NW group (p < 0.05) (Table 1). Glucocorticoid use was similar between groups, with 5 patients in the NW group and 5 in the EBW group receiving treatment (p > 0.05).
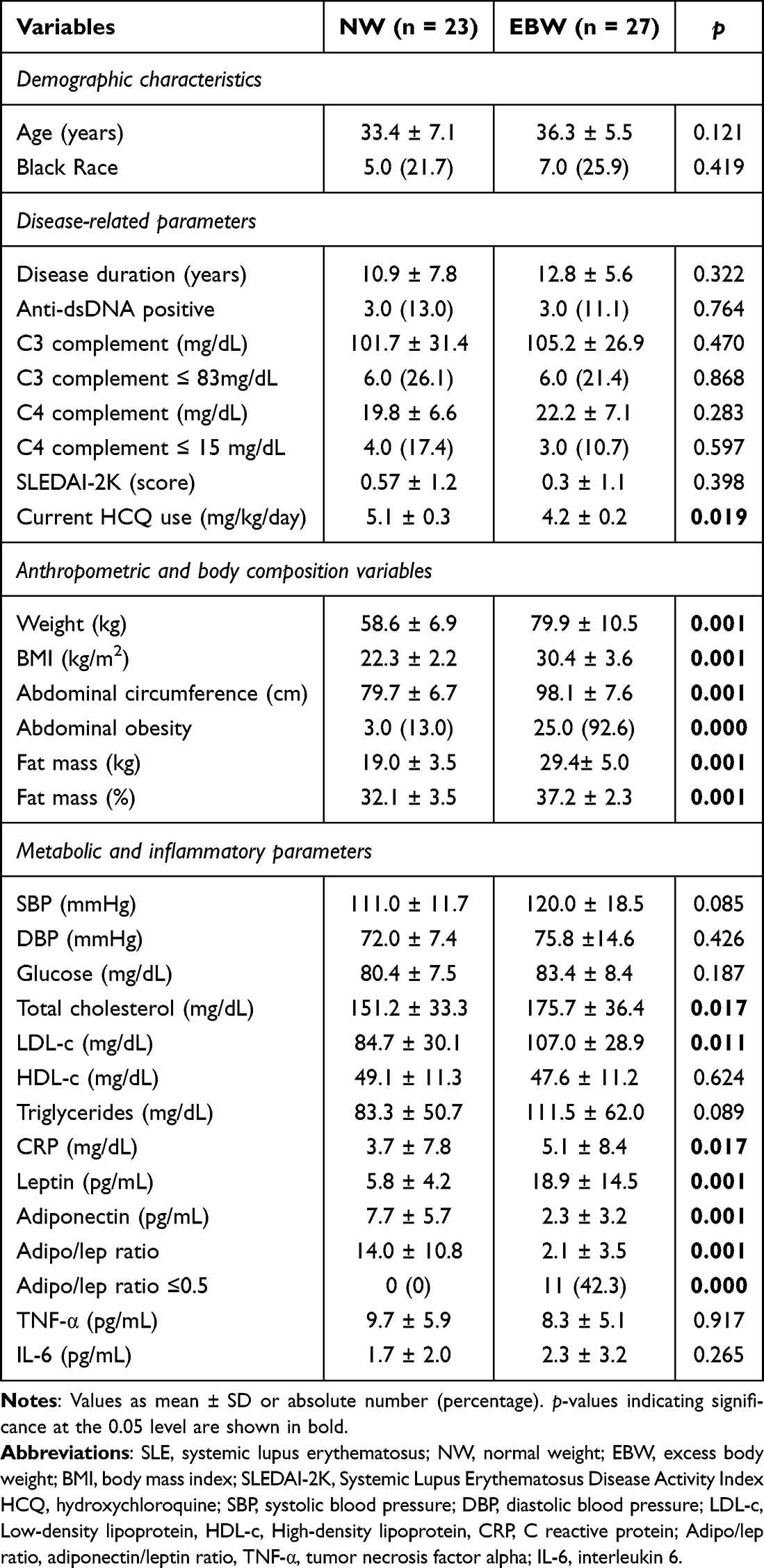 |
Table 1 General Characteristics of Patients with Systemic Lupus Erythematosus by Body Weight Category |
Adipokine and Inflammatory Profiles
Serum leptin levels were higher, while adiponectin levels were lower in the EBW group compared to those of NW group. The leptin/adiponectin ratio was markedly elevated in the EBW group (p < 0.001), indicating an adipose tissue dysfunction pattern. In contrast, TNF-α and IL-6 levels were similar in both groups (p > 0.05) (Table 1).
Associations Between Adipokines and Metabolic–Inflammatory Parameters
Serum leptin levels correlated positively with BMI (r = 0.66; p < 0.001), abdominal circumference (r = 0.61; p < 0.001), and CRP (r = 0.36; p = 0.01). In contrast, serum adiponectin levels showed inverse correlations with BMI (r = - 0.58; p < 0.001), abdominal circumference (r = - 0.66; p < 0.001), total cholesterol (r = - 0.30; p = 0.034) and LDL-c (r = - 0.32; p = 0.026). The leptin/adiponectin ratio correlated negatively with BMI (r = - 0.69; p < 0.001), abdominal circumference (r = - 0.72; p < 0.001), total cholesterol (r = - 0.30; p = 0.040) and LDL-c (r = - 0.31; p = 0.030). No significant correlations were observed between adipokines levels and C3, C4, or anti-dsDNA levels, however, the adipo/lep ratio showed inverse correlations with C4 complement levels (r = - 0.31; p = 0.030).
Gene Expression in Adipose Tissue
Expression of TNF-α, IL6, LEP, and ADIPOQ genes were significantly upregulated in EBW groups compared with normal-weight women (p < 0.05) (Figure 1). No significant correlations were observed between adipose tissue gene expression levels serum levels (all p > 0.05).
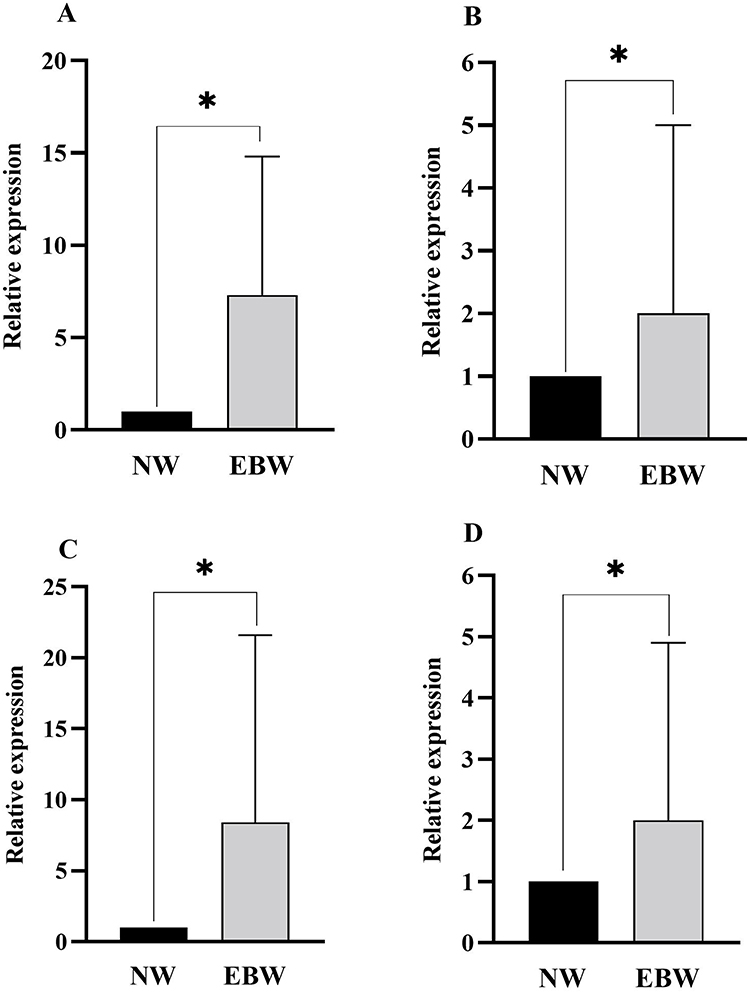 |
Figure 1 Relative TNF-α ((A), n = 36), IL-6 ((B), n = 39), LEP ((C), n = 44) and ADIPOQ ((D), n = 45) expressions in patients with systemic lupus erythematosus according to nutritional status. Expression of TNF-α, IL-6, LEP and ADIPOQ were higher in patients with systemic lupus erythematosus and excess body weight than normal weight. NW values were used as the calibrator (expression = 1) in the 2−ΔΔCt analysis. The indicated sample size (n) corresponds to samples with valid amplification included in each gene expression analysis. *: p <0.05. Abbreviations: NW, Normal Weight; EBW, excess body weight. |
Stratification by Adipo/Lep Ratio
To further explore the relationship between adipose dysfunction and immunological parameters, patients were divided into two groups according to the adipo/lep ratio: ≤ 5 (adipose dysfunction) and > 5 (normal adipose function). Both groups were comparable in age, disease duration, SLEDAI scores and anti-dsDNA levels (all p > 0.05), indicating similar levels of clinical disease activity. Notably, serum C4 levels were significantly higher in patients with an elevated adipo/lep ratio (p = 0.004), whereas C3 levels showed a similar upward trend that did not reach statistical significance (p = 0.055) (Table 2).
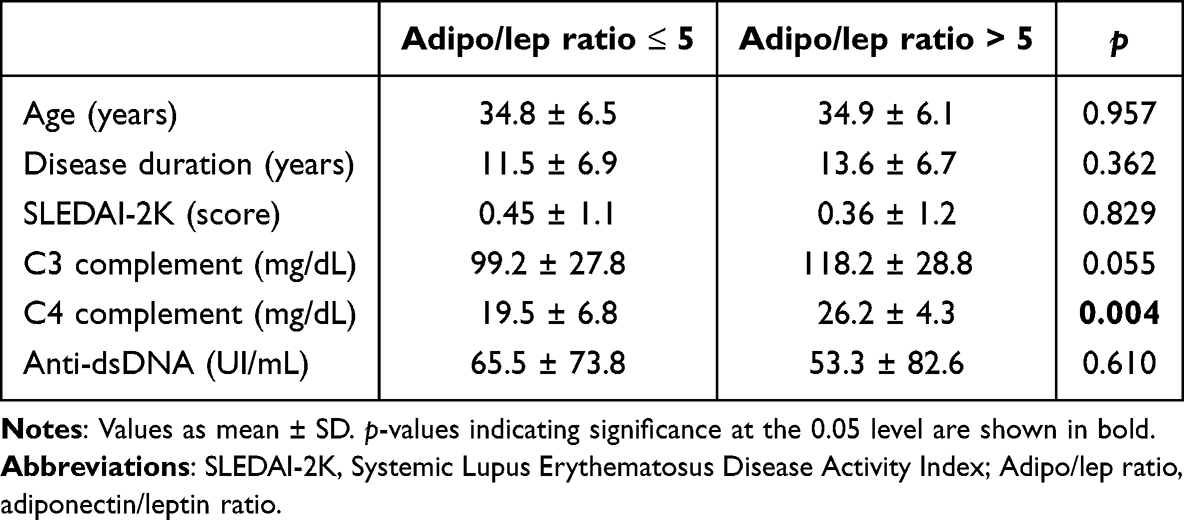 |
Table 2 Clinical and Complement Profile in Patients Stratified by Adiponectin/Leptin Ratio |
Impact of Hydroxychloroquine
Multiple linear regression analyses were performed to examine the associations between HCQ use and anthropometric or metabolic parameters (Table 3). HCQ daily dose normalized by body weight (mg/kg/day) showed negative associations with abdominal circumference (β = −0.43; 95% CI: −5.91 to −1.34; p = 0.003) and fat mass percentage (β = −0.38; 95% CI: −1.83 to −0.27; p = 0.009). Conversely, HCQ use was positively associated with adiponectin levels (β = 0.45; 95% CI: 6.85 to 28.8; p = 0.002) and the adipo/lep ratio (β = 0.39; 95% CI: 2.98 to 19.5; p = 0.009), suggesting a protective metabolic profile. There was also a trend for higher HCQ doses to be associated with increased HDL-c (p = 0.059) and reduced leptin levels (p = 0.058).
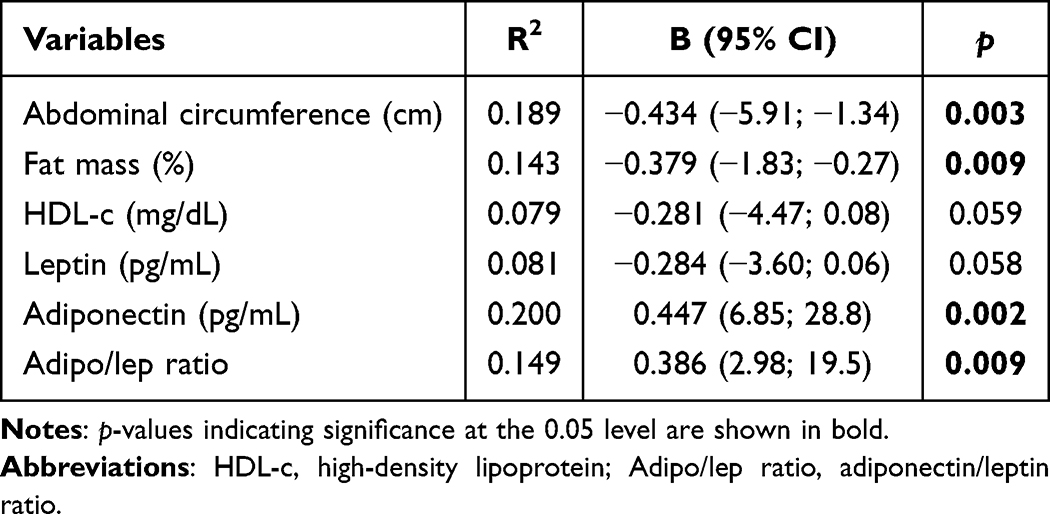 |
Table 3 Multiple Linear Regression Models Showing the Relationship Between Hydroxychloroquine Use (mg/kg/Day) and Metabolic and Body Composition Parameters in SLE |
Discussion
In this study involving women with SLE and low disease activity, excess body weight was associated with a pro-inflammatory and adverse metabolic profile, characterized by elevated TNF-α, IL-6, LEP expression in adipose tissue, higher serum leptin and lower adiponectin levels, and a decreased adiponectin/leptin ratio. Despite similar SLEDAI scores and immunological markers across BMI groups, patients with adipose tissue dysfunction, defined by a low adipo/lep ratio, showed higher C4 complement levels.60 Additionally, HCQ dosage adjusted by body weight correlated with more favorable metabolic parameters, including lower adiposity and higher adiponectin levels.
The great advantage of the present study was to include patients with definitive SLE diagnosis according to 2019 European League Against Rheumatism and American College of Rheumatology (EULAR/ACR) classification criteria.51 The main strength of this study was the robust control of confounders provided by a homogenous sample. First, only female patients were consecutively included due to avoid any specific sex-differences in metabolic patterns. Moreover, only patients with SLE and inactive disease were selected to avoid the influence of the exacerbated inflammation in the variables of interest.61 Also, only patients with SLE and current, stable use of HCQ, the cornerstone treatment of the disease61 to prevent heterogeneities in response to this drug.62,63 In this regard, all included patients should be at stable daily dose for at least 3 months since this period is required to promote significant metabolic changes.64 Importantly, any supplementation with vitamin B12 or folic acid was excluded, as it is part of the exclusion criteria of the clinical trial related to this study.50
Patients with SLE and excess weight demonstrated increased body fat and abdominal obesity which were indicative of significant adipose tissue accumulation, particularly in the abdominal region.65 This adipose tissue accumulation may exacerbate inflammatory status associated with SLE.66 The role of TNF-α and IL-6 in inflammatory processes, as well as their pleiotropic effects in autoimmune diseases67,68 and metabolic disorders,69 is well-established. Elevated IL-6 and TNF-α expression were observed in previous findings linking these cytokines to SLE serological activity70 and to metabolic–immune interactions.71 Therefore, it would be expected that both TNF-α and IL-6 levels would be increased in SLE68,72–74 and obesity.75–78 Despite these findings, the present study did not identify increased levels of TNF-α and IL-6 in patients with EBW. Importantly, transcriptional changes observed in adipose tissue should be interpreted cautiously, as mRNA levels do not necessarily correspond to protein expression or functional activity.
Corroborating our expectations, patients with excess body weight exhibited elevated gene expression levels and serum levels of leptin, along with a high incidence of hyperleptinemia. Elevated levels have been documented in patients with SLE,79,80 with prevalence rates reaching approximately 74%.81 Additionally, obesity has been extensively associated with increase serum leptin levels in different populations.82–84 The exact role of leptin in SLE disease is still unknown.85 Leptin, a pro-inflammatory adipokine produced by adipose tissue, contributes to SLE-related inflammation by promoting the proliferation of naïve T and B cells and enhancing the production of autoantibodies and pro-inflammatory cytokines.85,86 This increase in inflammatory biomarkers due to leptin could exacerbate symptoms, potentially accelerating the risk of metabolic syndrome and cardiovascular disease in patients with SLE, a hypothetical physio pathological mechanism illustrated in Figure 2.87,88
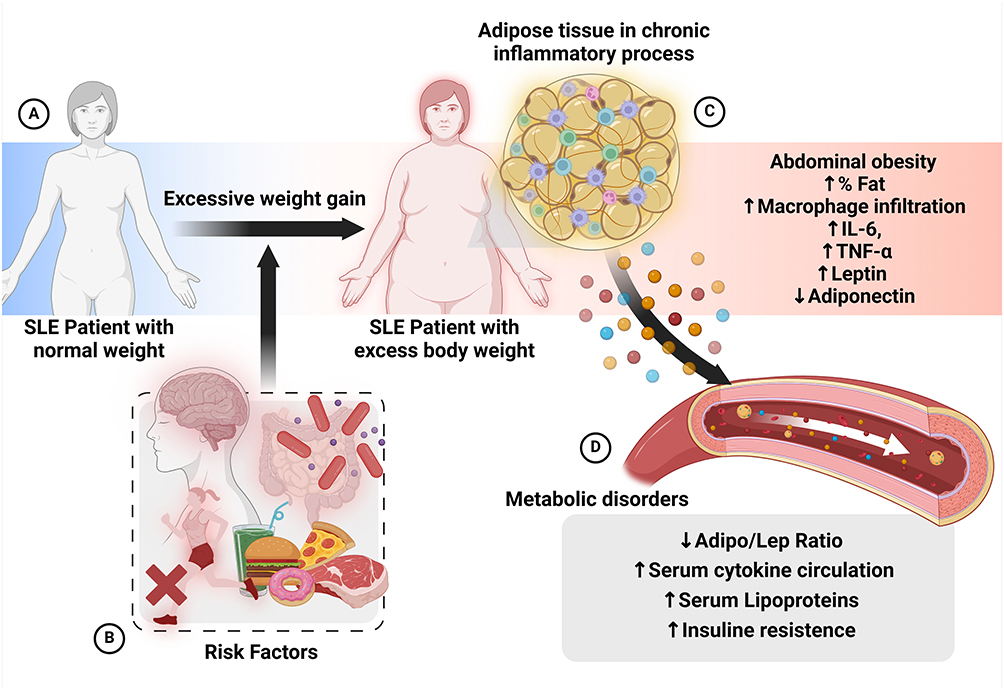 |
Figure 2 Possibles metabolic consequences of excess body weight in patients with systemic lupus erythematous. (A) Process of excess weight gain. (B) Possible risk factors that contribute to excessive weight gain or obesity: Stress, nutritional imbalance, microbiome, sedentary lifestyle. (C) Chronic inflammatory process mediated by adipose tissue, in which hypertrophy and hyperplasia of the cellular matrix and consequently increased hypoxia and inflammatory cytokines, leptin secretion. (D) Imbalance in the adiponectin/leptin ratio, higher serum inflammatory cytokines and lipoproteins levels and insulin resistance. |
Regarding adiponectin, a meta-analysis involving eight studies found that patients with SLE had higher serum adiponectin levels compared to controls.89 Moreover, our study aligns with previous research demonstrating lower serum adiponectin levels in individuals with excess body weight.90,91 Adiponectin is also secreted by adipose tissue and plays an anti-inflammatory role by modulating M2 macrophage functions, such as proliferation, plasticity, and polarization,92 and by inhibiting the production of pro-inflammatory cytokines.93 Low levels of adiponectin may exacerbate the inflammatory processes associated with obesity93 and contribute to insulin resistance in affected individuals.94 The relationship between obesity, adiponectin, and SLE activity suggests a complex interaction between nutritional status and immunological factors of the individual, highlighting how systemic inflammation and body composition can influence the progression of this autoimmune disease.41,46
Studies have been pointed out that adipo/lep ratio may serve as a marker of cardiometabolic protection and adipose tissue functionality.55,56 In fact, the relationship between the adipo/lep ratio and cardiometabolic markers has been demonstrated across various populations.95–98 A recent clinical trial involving 28 adults with obesity found that a lower adipo/lep ratio was correlated with higher BMI values.97 Additionally, some studies observed a negative correlation between the adipo/lep ratio and CRP levels.55 Elevated serum leptin levels, combined with a reduced response to leptin’s appetite-suppressing effects, suggest the presence of leptin resistance. Furthermore, individuals with low adiponectin levels may lose the hormone’s cardioprotective and anti-inflammatory benefits. Consequently, a low adipo/lep ratio indicates dysfunctional adipose tissue, which may be associated with metabolic disturbances linked to excess body weight.56 This finding, particularly among patients with SLE, is novel and suggests that the adipo/lep ratio could serve as a predictive marker for the development of cardiovascular complications in these patients. Moreover, in the present study, patients with a higher adipo/lep ratio (>5) exhibited higher complement C4 levels, suggesting that preserved adipose tissue function may be associated with reduced complement consumption and lower subclinical immune activation, even in clinically inactive disease.65 A higher adipo/lep ratio likely reflects a metabolically protective state characterized by anti-inflammatory adipokine balance. Collectively, these findings support the potential of the adipo/lep ratio as a sensitive marker of metabolic–immune interactions in SLE, warranting further investigation.
Clinical factors influencing lipid metabolism, such as disease activity, age, menopause, presence of serum autoantibodies and inflammatory cytokines, are similar between NW and EBW groups. Thus, we hypothesize that despite high body weight, HCQ use may have a significant impact on the metabolic profile of these patients, indicating potential predictors of lipid profile changes from drug therapy. According to EULAR recommendations, the target dose of HCQ should stay at 5 mg/kg/day; however, it should be individualized based on the risk of flare-ups and retinal toxicity, without exceeding 400 mg/day.61 In our sample, despite daily dose be, in most cases, 400 mg, the average daily use/kg was higher in patients with SLE, and normal weight compared to those patients with excess body weight. Interestingly, higher HCQ dose adjusted per weight was associated with lower abdominal circumference, fat mass, and with higher adiponectin level and adipo/lep ratio. Additionally, higher HCQ daily dose was associated with higher HDL-c serum levels. These findings suggest that individualized HCQ therapy may positively impact the lipid profile and metabolic homeostasis in patients with SLE.70,71,99 Furthermore, the increase in adiponectin, which has anti-inflammatory properties and enhances insulin sensitivity, indicates that HCQ may not only help control disease activity but also promote a healthier metabolic environment.
Several studies previously demonstrated the hypolipidemic property of antimalarials drugs in SLE.100–103 The potential influence of HCQ specifically in HDL function is not completely defined, however, recent studies evidenced that HCQ use may increase HDL levels in lupus patients, reducing atherosclerosis risk.63 Considering that patients with SLE have less efficient incorporating unesterified cholesterol (UC) for subsequent esterification, some in vitro results demonstrated higher transfer of UC in those patients under HCQ treatment.63 Curiously, an experimental study showed that HCQ improved body weight gain, hyperglycemia, and lipid profile, while also preserving heart and liver function in rats fed with a high-fat diet, ameliorating obesity negative effects.104
Previous studies have documented improvements in adiponectin levels in animal models of obesity treated with hydroxychloroquine. It has been proposed that HCQ might help to normalize leptin levels, alleviate leptin resistance, and restore the leptin-to-adiponectin balance in rats fed a high-fat diet and treated with hydroxychloroquine, suggesting an adiponectin-mediated mechanism for hydroxychloroquine’s effects on obesity.104 In a clinical study involving 41 patients with SLE (mean age 41.3 ± 13.2 years) treated with supplemental hydroxychloroquine, serum adiponectin levels significantly increased after three months. The authors proposed that this increase in adipokine levels might contribute to hydroxychloroquine’s beneficial effects on dyslipidemia in SLE patients.105
Considering that high abdominal obesity, fat mass and low adiponectin levels and adipo/lep ratio contribute to the development of metabolic disturbances, we suggest that patients with SLE associated with overweight or obesity would have an increased risk of metabolic syndrome and consequently, cardiovascular diseases.106 These findings underscore the importance of an integrated approach that addresses both metabolic and inflammatory aspects in managing patients with SLE, to better understand and treat the disease’s complications, including cardiovascular diseases. Additionally, early identification of individuals at high risk for metabolic complications, through the assessment of adipose tissue dysfunction and the staging of obesity and its early forms, can enhance therapeutic decision-making. An integrated approach to investigating gene expression and serum levels is crucial for understanding the underlying mechanisms of SLE heterogeneity and its correlation with other medical conditions and treatment responses. Precision medicine and nutrition emerge as promising paradigms, aiming to individualize therapeutic measures for more accurate prognoses,107 thereby improving functional and prognostic evaluations for patients with SLE.108
It is important to acknowledge that, while the present results presented are novel and bring promising perspectives, this study has several limitations. First, the relatively small sample size reflects the complexity of recruiting patients with SLE willing to undergo adipose tissue biopsy, which may limit statistical power and generalizability. Second, the cross-sectional design precludes causal inference. Third, gene expression analysis does not necessarily reflect protein abundance or biological activity in adipose tissue. Although protein-level measurements would strengthen the findings, the available adipose tissue samples were limited and prioritized for RNA extraction. Finally, the absence of a healthy control group should be considered when interpreting the results. The primary aim of this study was to investigate body weight–related differences within SLE patients, minimizing heterogeneity related to disease status, immune activation, and medication exposure. Future studies including healthy controls and longitudinal designs are warranted.
Conclusions
In conclusion, women with SLE and excess body weight exhibit a distinct inflammatory–metabolic profile characterized by higher leptin levels, lower adiponectin, and increased expression of pro-inflammatory and adipokine-related genes in adipose tissue. These findings support the concept that adipose tissue dysfunction may contribute to systemic inflammation and cardiometabolic risk in SLE. Additionally, hydroxychloroquine dosage adjusted by body weight was associated with lower adiposity and a more favorable adipokine profile, suggesting a potential metabolic benefit of weight-adjusted dosing. The association between the adiponectin-to-leptin ratio and complement C4 levels further highlights the interaction between metabolic regulation and immune activity in SLE. Together, these results reinforce the importance of considering metabolic status in the clinical management of SLE.
Data Sharing Statement
The datasets generated during and/or analyzed during this study are available from the corresponding author on reasonable request.
Acknowledgments
We thank Andreia Bispo and all Team of SLE Outpatient Clinic of the Rheumatology Division, Hospital das Clínicas da Faculdade de Medicina da Universidade de Sao Paulo for their contribution to the enrollment of subjects.
Author Contributions
LMC – Investigation, Data curation, Formal analysis, Writing – original draft, Writing – review and editing, Conceptualization, Methodology; J.C.N.L.M. Investigation, Writing – review and editing, Visualization; A.A.R. Investigation, Writing – review and editing, Resources, Visualization, Validation, Conceptualization; L.L.S. Writing – review and editing, Investigation, Data Curation; R.C.S.S. Resources, Writing – review and editing, Investigation; B.G. Formal analysis, Writing – review and editing; M.M.U. Formal analysis, Writing – review and editing, Supervision, Validation,; J.A.M. Formal analysis, Writing – review and editing; E.B. Formal analysis, Writing – review and editing, Funding acquisition; C.F.N. Conceptualization, Funding acquisition, Writing – original draft, Writing – review and editing; All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Sao Paulo Research Foundation – FAPESP grant number [#2020/01893-2, #2020/15126-3, #2021/09777-4 and #2021/09745-5]. Supported by research grants from Conselho Nacional de Desenvolvimento Científico e Tecnológico (#303378/2022-0 to E.F.B.).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Tian J, Zhang D, Yao X, Huang Y, Lu Q. Global epidemiology of systemic lupus erythematosus: a comprehensive systematic analysis and modelling study. Ann Rheum Dis. 2023;82(3):351–14. doi:10.1136/ard-2022-223035
2. Barber MRW, Falasinnu T, Ramsey-Goldman R, Clarke AE. The global epidemiology of SLE: narrowing the knowledge gaps. Rheumatology. 2023;62(Supplement_1):i4–9. doi:10.1093/rheumatology/keac610
3. Hedrich CM. Epigenetics in SLE. Curr Rheumatol Rep. 2017;19(9):1. doi:10.1007/s11926-017-0685-1
4. Selmi C, Lu Q, Humble MC. Heritability versus the role of the environment in autoimmunity. J Autoimmun. 2012;39:249–252. doi:10.1016/j.jaut.2012.07.011
5. Fortuna G, Brennan MT. Systemic Lupus Erythematosus. Dent Clin North Am. 2013;57(4):631–655. doi:10.1016/j.cden.2013.06.003
6. Krebs CF, Schmidt T, Riedel JH, Panzer U. T helper type 17 cells in immune-mediated glomerular disease. Nat Rev Nephrol. 2017;13(10):647–659. doi:10.1038/nrneph.2017.112
7. López P, De Paz B, Rodríguez-Carrio J, et al. Th17 responses and natural IgM antibodies are related to gut microbiota composition in systemic lupus erythematosus patients. Sci Rep. 2016;6(1). doi:10.1038/srep24072.
8. Narváez J. Systemic lupus erythematosus 2020. Med Clin. 2020;155(11):494–501. doi:10.1016/j.medcli.2020.05.009
9. Mok CC. Metabolic syndrome and systemic lupus erythematosus: the connection. Expert Rev Clin Immunol. 2019;15(7):765–775. doi:10.1080/1744666X.2019.1620601
10. Federica FB, Konstantinos F, Schwarting TA, et al. Systemic Lupus Erythematosus (SLE) Therapy: the Old and the New. Rheumatol Ther. 2020;7:433–446. doi:10.6084/m9.figshare.12288038
11. Ruiz-Irastorza G, Ramos-Casals M, Brito-Zeron P, Khamashta MA. Clinical efficacy and side effects of antimalarials in systemic lupus erythematosus: a systematic review. Ann Rheumatic Dis. 2010;69(1):20–28. doi:10.1136/ard.2008.101766
12. Alarcón GS, McGwin G, Bertoli AM, et al. Effect of hydroxychloroquine on the survival of patients with systemic lupus erythematosus: data from LUMINA, a multiethnic US cohort (LUMINA L). Ann Rheum Dis. 2007;66(9):1168–1172. doi:10.1136/ard.2006.068676
13. Muniz LF, Pereira RMR, Silva TF, Bonfá E, Borba EF. Impact of Therapy on Metabolic Syndrome in Young Adult Premenopausal Female Lupus Patients: beneficial Effect of Antimalarials. Arthritis Care Res. 2015;67(9):1255–1262. doi:10.1002/acr.22593
14. Penn SK, Kao AH, Schott LL, Elliott JR, Toledo FGS, Kuller L. Hydroxychloroquine and Glycemia in Women with Rheumatoid Arthritis and Systemic Lupus Erythematosus. J Rheumatol. 2010;37(6):1136–1142. doi:10.3899/jrheum.090994
15. Yang DH, Leong PY, Sia SK, Wang YH, Wei JCC. Long-Term Hydroxychloroquine Therapy and Risk of Coronary Artery Disease in Patients with Systemic Lupus Erythematosus. J Clin Med. 2019;8(6):796. doi:10.3390/jcm8060796
16. Levinson D, Abugroun A, Osinski K. Hydroxychloroquine lowers the risk for Diabetes Mellitus in patients with Systemic Lupus Erythematosus. Diabetes Epidemiol Management. 2022;8:100089. doi:10.1016/j.deman.2022.100089
17. Qiao X, Zhou ZC, Niu R, et al. Hydroxychloroquine Improves Obesity-Associated Insulin Resistance and Hepatic Steatosis by Regulating Lipid Metabolism. Front Pharmacol. 2019;10. doi:10.3389/fphar.2019.00855
18. Ponticelli C, Moroni G. Hydroxychloroquine in systemic lupus erythematosus (SLE). Expert Opin Drug Saf. 2017;16(3):411–419. doi:10.1080/14740338.2017.1269168
19. Hannan MT. Introduction to special theme section: obesity and the rheumatic diseases. Arthritis Care and Research. 2013;65(1):4. doi:10.1002/acr.21904
20. Choe SS, Huh JY, Hwang IJ, Kim JI, Kim JB. Adipose Tissue Remodeling: its Role in Energy Metabolism and Metabolic Disorders. Front Endocrinol. 2016;7. doi:10.3389/fendo.2016.00030
21. Versini M, Jeandel PY, Rosenthal E, Shoenfeld Y. Obesity in autoimmune diseases: not a passive bystander. Autoimmunity Rev. 2014;13(9):981–1000. doi:10.1016/j.autrev.2014.07.001
22. Gomez A, Hani Butrus F, Johansson P, et al. Impact of overweight and obesity on patient-reported health-related quality of life in systemic lupus erythematosus. Rheumatology. 2021;60(3):1260–1272. doi:10.1093/rheumatology/keaa453
23. Kono M, Nagafuchi Y, Shoda H, Fujio K. The impact of obesity and a high-fat diet on clinical and immunological features in systemic lupus erythematosus. Nutrients. 2021;13(2):1–12. doi:10.3390/nu13020504
24. Stojan G, Li J, Wittmaack A, Petri M. Cachexia in Systemic Lupus Erythematosus: risk Factors and Relation to Disease Activity and Damage. Arthritis Care Res. 2021;73(11):1577–1582. doi:10.1002/acr.24395
25. Cao H. Adipocytokines in obesity and metabolic disease. J Endocrinol. 2014;220(2):T47–59. doi:10.1530/JOE-13-0339
26. George MD, Baker JF. The Obesity Epidemic and Consequences for Rheumatoid Arthritis Care. Curr Rheumatol Rep. 2016;18(1):6. doi:10.1007/s11926-015-0550-z
27. Zhang X, Meng J, Shi X, et al. Lupus pathogenesis and autoimmunity are exacerbated by high fat diet-induced obesity in MRL/lpr mice. Lupus Sci Med. 2023;10(1):e000898. doi:10.1136/lupus-2023-000898
28. Huang A, Zhou L, Xu W. The causal associations of inflammatory cytokines with obesity and systemic lupus erythematosus: a Mendelian randomization study. Int J Rheum Dis. 2024;27(6). doi:10.1111/1756-185X.15214
29. Nikiphorou E, Fragoulis GE. Inflammation, obesity and rheumatic disease: common mechanistic links. A narrative review. Ther Adv Musculoskelet Dis. 2018;10(8):157–167. doi:10.1177/1759720X18783894
30. Sinicato NA, Postal M, Peres FA, et al. Obesity and Cytokines in Childhood-Onset Systemic Lupus Erythematosus. J Immunol Res. 2014;2014:1–6. doi:10.1155/2014/162047
31. Kotsis V, Martinez F, Trakatelli C, Redon J. Impact of Obesity in Kidney Diseases. Nutrients. 2021;13(12):4482. doi:10.3390/nu13124482
32. Leigh SJ, Morris MJ. Diet, inflammation and the gut microbiome: mechanisms for obesity-associated cognitive impairment. Biochim Biophys Acta Mol Basis Dis. 2020;1866(6):165767. doi:10.1016/j.bbadis.2020.165767
33. Abiri B, Hosseinpanah F, Banihashem S, Madinehzad SA, Valizadeh M. Mental health and quality of life in different obesity phenotypes: a systematic review. Health Qual Life Outcomes. 2022;20(1):63. doi:10.1186/s12955-022-01974-2
34. Conrad N, Verbeke G, Molenberghs G, et al. Autoimmune diseases and cardiovascular risk: a population-based study on 19 autoimmune diseases and 12 cardiovascular diseases in 22 million individuals in the UK. Lancet. 2022;400(10354):733–743. doi:10.1016/S0140-6736(22)01349-6
35. Restivo V, Candiloro S, Daidone M, et al. Systematic review and meta-analysis of cardiovascular risk in rheumatological disease: symptomatic and non-symptomatic events in rheumatoid arthritis and systemic lupus erythematosus. Autoimmunity Rev. 2022;21(1):102925. doi:10.1016/j.autrev.2021.102925
36. Gómez R, Conde J, Scotece M, Gómez-Reino JJ, Lago F, Gualillo O. What’s new in our understanding of the role of adipokines in rheumatic diseases? Nat Rev Rheumatol. 2011;7(9):528–536. doi:10.1038/nrrheum.2011.107
37. Hanna Kazazian N, Wang Y, Roussel-Queval A, et al. Lupus Autoimmunity and Metabolic Parameters Are Exacerbated Upon High Fat Diet-Induced Obesity Due to TLR7 Signaling. Front Immunol. 2019;10. doi:10.3389/fimmu.2019.02015
38. Martin MC, Lima Faleiro L, Fonseca A. Relationship between leptin and body mass and metabolic syndrome in an adult population. Revista Portuguesa de Cardiologia. 2012;31(11):711–719. doi:10.1016/j.repc.2012.08.002
39. Mohammed SF, Abdalla MA, Ismaeil WM, Sheta MM. Serum leptin in systemic lupus erythematosus patients: its correlation with disease activity and some disease parameters. Egypt Rheumatologist. 2018;40(1):23–27. doi:10.1016/j.ejr.2017.06.005
40. Gradidge PJL, Jaff NG, Norris SA, Toman M, Crowther NJ. The negative association of lower body fat mass with cardiometabolic disease risk factors is partially mediated by adiponectin. Endocr Connect. 2022;11(12). doi:10.1530/EC-22-0156
41. Carbone F, Montecucco F, Poggi A, et al. Serum adiponectin levels are associated with presence of carotid plaque in women with systemic lupus erythematosus. Nutr Metab Cardiovasc Dis. 2020;30(7):1147–1151. doi:10.1016/j.numecd.2020.03.020
42. Hassan Ali M, Emad Shaker G, Elsayed Amr G, Albendary Altanahy M. Conditions of the Creative Commons Attribution (CC BY-SA) license Serum Adiponectin Level in Patients with Systemic Lupus Erythematosus and its Correlation with Disease Activity [Internet]. Egypt J Hosp Med. 2020;80(1):647–653.
43. Dan YL, Wang P, Cheng Z, et al. Circulating adiponectin levels and systemic lupus erythematosus: a two-sample Mendelian randomization study. Rheumatology. 2021;60(2):940–946. doi:10.1093/rheumatology/keaa506
44. Balaji C, Saranya C, Bhuvanesh M, Ramesh R, Sriram S, Rajeswari S. Serum Adipokine leptin levels in systemic lupus erythematosus patients and its correlation with clinical manifestations and disease activity – a cross-sectional study from a tertiary care center. Indian J Rheumatol. 2021;16(1):3. doi:10.4103/injr.injr_6_20
45. Garcia-Gonzalez A, Gonzalez-Lopez L, Valera-Gonzalez IC, et al. Serum leptin levels in women with systemic lupus erythematosus. Rheumatol Int. 2002;22(4):138–141. doi:10.1007/s00296-002-0216-9
46. Ali MH, Shaker GE, Amr GE, Altanahy MA. Serum Adiponectin Level in Patients with Systemic Lupus Erythematosus and its Correlation with Disease Activity. Egypt J Hosp Med. 2020;80(1):647–653. doi:10.21608/ejhm.2020.93889
47. Yuan Q, Zhang L, Tian Y, Li W, Li X, Lu Z. Circulating leptin level, soluble leptin receptor level and their gene polymorphism in patients with systemic lupus erythematosus: a systematic review and meta-analysis. Clin Exp Rheumatol. 2020;38(6):1238–1246.
48. Wisłowska M, Rok M, Stępień K, Kuklo-Kowalska A. Serum leptin in systemic lupus erythematosus. Rheumatol Int. 2008;28(5):467–473. doi:10.1007/s00296-008-0526-7
49. Chougule D, Nadkar M, Venkataraman K, et al. Adipokine interactions promote the pathogenesis of systemic lupus erythematosus. Cytokine. 2018;111:20–27. doi:10.1016/j.cyto.2018.08.002
50. da Mota JCNL, Carvalho LM, Ribeiro AA, et al. Methyl-donor supplementation in women with systemic lupus erythematosus with different nutritional status: the protocol for a randomised, double-blind, placebo-controlled trial. Lupus Sci Med. 2024;11(2):e001279. doi:10.1136/lupus-2024-001279
51. Aringer M, Costenbader K, Daikh D, et al. European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019;71(9):1400–1412. doi:10.1002/art.40930
52. Gladman D, Ginzler E, Goldsmith C, et al. The development and initial validation of the systemic lupus international collaborating clinics/American college of rheumatology damage index for systemic lupus erythematosus. Arthritis Rheum. 1996;39(3):363–369. doi:10.1002/art.1780390303
53. Gladman DD, Ibañez D, Urowitz MB. Systemic lupus erythematosus disease activity index 2000. J Rheumatol. 2002;29(2):288–291.
54. Ma S, Xi B, Yang L, Sun J, Zhao M, Bovet P. Trends in the prevalence of overweight, obesity, and abdominal obesity among Chinese adults between 1993 and 2015. Int J Obes. 2021;45(2):427–437. doi:10.1038/s41366-020-00698-x
55. Frühbeck G, Catalán V, Rodríguez A, Gómez-Ambrosi J. Adiponectin-leptin ratio: a promising index to estimate adipose tissue dysfunction. Relation with obesity-associated cardiometabolic risk. Adipocyte. 2018;7(1):57–62. doi:10.1080/21623945.2017.1402151
56. Frühbeck G, Catalán V, Rodríguez A, et al. Adiponectin-leptin Ratio is a Functional Biomarker of Adipose Tissue Inflammation. Nutrients. 2019;11(2):454. doi:10.3390/nu11020454
57. Heid CA, Stevens J, Livak KJ, Williams PM. Real time quantitative PCR. Genome Res. 1996;6(10):986–994. doi:10.1101/gr.6.10.986
58. Hieronymus K, Dorschner B, Schulze F, et al. Validation of reference genes for whole blood gene expression analysis in cord blood of preterm and full-term neonates and peripheral blood of healthy adults. BMC Genomics. 2021;22(1):489. doi:10.1186/s12864-021-07801-0
59. Barber RD, Harmer DW, Coleman RA, Clark BJ. GAPDH as a housekeeping gene: analysis of GAPDH mRNA expression in a panel of 72 human tissues. Physiol Genomics. 2005;21(3):389–395. doi:10.1152/physiolgenomics.00025.2005
60. Martínez-Urbistondo M, Higuera-Gómez A, De Cuevillas B, et al. Visceral fat, cardiovascular risk factors and quality of life in lupus activity categorised via complement C3. Lupus Sci Med. 2025;12(1):e001423. doi:10.1136/lupus-2024-001423
61. Fanouriakis A, Kostopoulou M, Andersen J, et al. EULAR recommendations for the management of systemic lupus erythematosus: 2023 update. Ann Rheum Dis. 2024;83(1):15–29. doi:10.1136/ard-2023-224762
62. de Carvalho JF, Bonfá E, Borba EF. Systemic lupus erythematosus and “lupus dyslipoproteinemia”. Autoimmun Rev. 2008;7(3):246–250. doi:10.1016/j.autrev.2007.11.016
63. Lang MG, Vinagre CG, Bonfa E, et al. Hydroxychloroquine increased cholesterol transfer to high-density lipoprotein in systemic lupus erythematosus: a possible mechanism for the reversal of atherosclerosis in the disease. Lupus. 2022;31(6):659–665. doi:10.1177/09612033221090127
64. Cairoli E, Rebella M, Danese N, Garra V, Borba EF. Hydroxychloroquine reduces low-density lipoprotein cholesterol levels in systemic lupus erythematosus: a longitudinal evaluation of the lipid-lowering effect. Lupus. 2012;21(11):1178–1182. doi:10.1177/0961203312450084
65. Chero-Sandoval L, Martínez-Urbistondo M, Cuevas-Sierra A, et al. Comparison of Metabolic Syndrome, Autoimmune and Viral Distinctive Inflammatory Related Conditions as Affected by Body Mass Index. J Clin Med. 2024;13(21):6298. doi:10.3390/jcm13216298
66. Carvalho LM, Carvalho BG, Souza LL, da Mota JC, Ribeiro AA, Nicoletti CF. Obesity as an aggravating factor of systemic lupus erythematosus disease: what we already know and what we must explore? - A Rapid Scoping Review. Nutrition. 2024;128:112559. doi:10.1016/j.nut.2024.112559
67. de Oliveira PSS, da Paixão ABF, da Rocha Junior LF, et al. Atorvastatin inhibits IL-17A, TNF, IL-6, and IL-10 in PBMC cultures from patients with severe rheumatoid arthritis. Immunobiology. 2020;225(3):151908. doi:10.1016/j.imbio.2020.151908
68. Jin S, Yu C, Yu B. Changes of serum IL-6, IL-10 and TNF-α levels in patients with systemic lupus erythematosus and their clinical value. Am J Transl Res. 2021;13(4):2867–2874.
69. Shi C, Zhu L, Chen X, et al. IL-6 and TNF-α Induced Obesity-Related Inflammatory Response Through Transcriptional Regulation of miR-146b. J Interferon Cytokine Res. 2014;34(5):342–348. doi:10.1089/jir.2013.0078
70. Moreno-Torres V, Castejón R, Mellor-Pita S, et al. Usefulness of the hemogram as a measure of clinical and serological activity in systemic lupus erythematosus. J Transl Autoimmun. 2022;5:100157. doi:10.1016/j.jtauto.2022.100157
71. Moreno‐Torres V, Castejón R, Martínez‐Urbistondo M, et al. Serum cytokines to predict systemic lupus erythematosus clinical and serological activity. Clin Transl Sci. 2022;15(7):1676–1686. doi:10.1111/cts.13283
72. Coppack SW. Pro-inflammatory cytokines and adipose tissue. Proc Nutr Soc. 2001;60(3):349–356. doi:10.1079/PNS2001110
73. Fan JL, Wu D, Zhu TT, Tian XL, Liu SJ, Zhang SL. The exploration of shared genes and molecular mechanisms of systemic lupus erythematosus and atherosclerosis. Lupus. 2023;32(2):239–251. doi:10.1177/09612033221144596
74. Ding J, Su S, You T, et al. Serum interleukin-6 level is correlated with the disease activity of systemic lupus erythematosus: a meta-analysis. Clinics. 2020;75:e1801.
75. Su X, Cheng Y, Chang D. The Important Role of Leptin in Modulating the Risk of Dermatological Diseases. Front Immunol. 2021;11. doi:10.3389/fimmu.2020.593564
76. Larsson A, Carlsson L, Lind AL, et al. The body mass index (BMI) is significantly correlated with levels of cytokines and chemokines in cerebrospinal fluid. Cytokine. 2015;76(2):514–518. doi:10.1016/j.cyto.2015.07.010
77. Rość D, Adamczyk P, Boinska J, et al. CRP, but not TNF-α or IL-6, decreases after weight loss in patients with morbid obesity exposed to intensive weight reduction and balneological treatment. J Zhejiang Univ Sci B. 2015;16(5):404–411. doi:10.1631/jzus.B1400219
78. Sindhu S, Thomas R, Shihab P, Sriraman D, Behbehani K, Ahmad R. Obesity Is a Positive Modulator of IL-6R and IL-6 Expression in the Subcutaneous Adipose Tissue: significance for Metabolic Inflammation. PLoS One. 2015;10(7):e0133494. doi:10.1371/journal.pone.0133494
79. Reagan M, Aprilia Salim N, Junaidi H. Comparison of leptin serum levels between systemic lupus erythematosus (SLE) and non-SLE patients at Mohammad Hoesin Hospital Palembang. J Phys Conf Ser. 2019;1246(1):012046. doi:10.1088/1742-6596/1246/1/012046
80. Afifi AEMA, Shaat RM, Gharbia OM, Elhanafy M, Hasan ASG. Role of serum leptin levels and leptin receptor gene polymorphisms in systemic lupus erythematosus. Clin Rheumatol. 2020;39(11):3465–3472. doi:10.1007/s10067-020-05120-5
81. Kondratyeva LV, Gorbunova YN, Panafidina TA, Popkova TV. Hyperleptinemia as a Marker of Various Phenotypes of Obesity and Overweight in Women with Rheumatoid Arthritis and Systemic Lupus Erythematosus. Dokl Biochem Biophys. 2024;517(1):182–194. doi:10.1134/S1607672924700893
82. Ghadge AA, Khaire AA. Leptin as a predictive marker for metabolic syndrome. Cytokine. 2019;121:154735. doi:10.1016/j.cyto.2019.154735
83. Kumar R, Mal K, Razaq MK, et al. Association of Leptin With Obesity and Insulin Resistance. Cureus. 2020. doi:10.7759/cureus.12178
84. khan Z, Khan A, Ghaffar T, Kainat A, Arabdin M, Orakzai S. Correlation between serum leptin level and body mass index (BMI) in patients with type II diabetes mellitus. J Pak Med Assoc. 2019;1:1.
85. Villa N, Badla O, Goit R, et al. The Role of Leptin in Systemic Lupus Erythematosus: is It Still a Mystery? Cureus. 2022. doi:10.7759/cureus.26751
86. Yuan Q, Chen H, Li X, Wei J. Leptin: an unappreciated key player in SLE. Clin Rheumatol. 2020;39(2):305–317. doi:10.1007/s10067-019-04831-8
87. Gigante A, Iannazzo F, Navarini L, et al. Metabolic syndrome and adipokine levels in systemic lupus erythematosus and systemic sclerosis. Clin Rheumatol. 2021;40(10):4253–4258. doi:10.1007/s10067-021-05731-6
88. Corona-Meraz FI, Vázquez-Del Mercado M, Sandoval-García F, et al. Biomarkers in Systemic Lupus Erythematosus along with Metabolic Syndrome. J Clin Med. 2024;13(7):1988. doi:10.3390/jcm13071988
89. Dini AA, Wang P, Ye DQ. Serum Adiponectin Levels in Patients With Systemic Lupus Erythematosus. JCR: J Clinic Rheumatol. 2017;23(7):361–367.
90. Al-Tahami BA, Bee YTG, Ismail AAAS, Rasool AHG. Impaired microvascular endothelial function in relatively young obese humans is associated with altered metabolic and inflammatory markers. Clin Hemorheol Microcirc. 2011;47(2):87–97. doi:10.3233/CH-2010-1370
91. Sanip Z, Ariffin FD, Al-Tahami BAM, Sulaiman WAW, Rasool AHG. Obesity indices and metabolic markers are related to hs-CRP and adiponectin levels in overweight and obese females. Obes Res Clin Pract. 2013;7(4):e315–20. doi:10.1016/j.orcp.2012.05.002
92. Luo Y, Liu M. Adiponectin: a versatile player of innate immunity. J Mol Cell Biol. 2016;8(2):120–128. doi:10.1093/jmcb/mjw012
93. Febriza A, Ridwan R, As’ad S, Kasim VN, Idrus HH. Adiponectin and Its Role in Inflammatory Process of Obesity. Mol Cellular Biomed Sci. 2019;3(2):60. doi:10.21705/mcbs.v3i2.66
94. Choi K, Kim YB. Molecular Mechanism of Insulin Resistance in Obesity and Type 2 Diabetes. Korean J Intern Med. 2010;25(2):119. doi:10.3904/kjim.2010.25.2.119
95. Jung CH, Rhee EJ, Choi JH, et al. The Relationship of Adiponectin/Leptin Ratio with Homeostasis Model Assessment Insulin Resistance Index and Metabolic Syndrome in Apparently Healthy Korean Male Adults. Korean Diabetes J. 2010;34(4):237. doi:10.4093/kdj.2010.34.4.237
96. Oda N, Imamura S, Fujita T, et al. The ratio of leptin to adiponectin can be used as an index of insulin resistance. Metabolism. 2008;57(2):268–273. doi:10.1016/j.metabol.2007.09.011
97. Castela I, Morais J, Barreiros-Mota I, et al. Decreased adiponectin/leptin ratio relates to insulin resistance in adults with obesity. Am J Physiol Endocrinol Metab. 2023;324(2):E115–9. doi:10.1152/ajpendo.00273.2022
98. Tremblay EJ, Tchernof A, Pelletier M, Joanisse DR, Mauriège P. Plasma adiponectin/leptin ratio associates with subcutaneous abdominal and omental adipose tissue characteristics in women. BMC Endocr Disord. 2024;24(1):39. doi:10.1186/s12902-024-01567-8
99. Moreno-Torres V, Martínez-Urbistondo M, Gutiérrez-Rojas A, et al. Impact of severe infections in SLE: an observational study from the Spanish national registry. Lupus Sci Med. 2022;9(1):e000711. doi:10.1136/lupus-2022-000711
100. Wallace DJ, Metzger AL, Stecher VJ, Turnbull BA, Kern PA. Cholesterol-lowering effect of hydroxychloroquine in patients with rheumatic disease: reversal of deleterious effects of steroids on lipids. Am J Med. 1990;89(3):322–326. doi:10.1016/0002-9343(90)90345-E
101. Babary H, Liu X, Ayatollahi Y, et al. Favorable effects of hydroxychloroquine on serum low density lipid in patients with systemic lupus erythematosus: a systematic review and meta‐analysis. Int J Rheum Dis. 2018;21(1):84–92. doi:10.1111/1756-185X.13159
102. Borba EF, Bonfá E. Longterm beneficial effect of chloroquine diphosphate on lipoprotein profile in lupus patients with and without steroid therapy. J Rheumatol. 2001;28(4):780–785.
103. Petri M, Lakatta C, Magder L, Goldman D. Effect of prednisone and hydroxychloroquine on coronary artery disease risk factors in systemic lupus erythematosus: a longitudinal data analysis. Am J Med. 1994;96(3):254–259. doi:10.1016/0002-9343(94)90151-1
104. Hasan MA, Ammar OA, Amer MA, Othman AI, Zigheber F, El-Missiry MA. Hydroxychloroquine improves high-fat-diet-induced obesity and organ dysfunction via modulation of lipid level, oxidative stress, and inflammation. Egypt J Basic Appl Sci. 2023;10(1):368–379. doi:10.1080/2314808X.2023.2211832
105. Wakiya R, Ueeda K, Shimada H, et al. Supplemental hydroxychloroquine therapy regulates adipokines in patients with systemic lupus erythematosus with stable disease. Clin Rheumatol. 2022;41(11):3345–3353. doi:10.1007/s10067-022-06282-0
106. Moreno-Torres V, Tarín C, Ruiz-Irastorza G, et al. Trends in Hospital Admissions and Death Causes in Patients with Systemic Lupus Erythematosus: spanish National Registry. J Clin Med. 2021;10(24):5749. doi:10.3390/jcm10245749
107. Wampler Muskardin TL, Paredes JL, Appenzeller S, Niewold TB. Lessons from precision medicine in rheumatology. Mult Scler J. 2020;26(5):533–539. doi:10.1177/1352458519884249
108. Ribeiro AA, Carvalho LM, da Mota JCNL, et al. Diet, DNA methylation and systemic lupus erythematosus: evidence and perspectives focused on personalized nutrition. Lifestyle Genom. 2024. doi:10.1159/000537917
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Elevated CTSL Gene Expression Correlated with Proinflammatory Cytokines in Omental Adipose Tissue of Patients with Obesity
Zhou Q, Zhu Y, Li C, Li Z, Tang Z, Yuan B, Wang X, Zhang S, Wu X
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2277-2285
Published Date: 30 July 2022
Interactive Effect of Combined Intermittent and Sustained Hypoxia and High-Fat Diet on the Colonic Mucosal Microbiome and Host Gene Expression in Mice
Mashaqi S, Laubitz D, Morales EJD, De Armond R, Alameddin H, Ghishan FK, Kiela PR, Parthasarathy S
Nature and Science of Sleep 2022, 14:1623-1639
Published Date: 9 September 2022
Effects of NKT Cells on Metabolic Disorders Caused by High-Fat Diet Using CD1d-Knockout Mice

Ishikawa H, Nagashima R, Kuno Y, Sasaki H, Kohda C, Iyoda M
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2855-2864
Published Date: 19 September 2023
Bariatric Surgery and Gut-Brain-Axis Driven Alterations in Cognition and Inflammation
Custers E, Franco A, Kiliaan AJ
Journal of Inflammation Research 2023, 16:5495-5514
Published Date: 22 November 2023
Determinants of Metabolic Syndrome Among Patients Receiving Anti-Retro-Viral Treatment in A Tertiary Hospital, Central Ethiopia: Unmatched Case–Control Study
Jarso G, Aman H, Megerso A
Therapeutics and Clinical Risk Management 2024, 20:195-205
Published Date: 18 March 2024