Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Blood-Based Inflammatory and Metabolic Biomarkers for Assessing Symptom Burden and Quality of Life in Older Adults with Cancer: A Narrative Review
Received 24 March 2026
Accepted for publication 7 June 2026
Published 18 June 2026 Volume 2026:22 611486
DOI https://doi.org/10.2147/TCRM.S611486
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Lu Lu,1 Yu Zhang2
1The Second Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Oncology, Zhejiang Hospital, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Yu Zhang, Department of Oncology, Zhejiang Hospital, No. 1229 Gudun Road, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Background: To evaluate the clinical utility of blood-based inflammatory and metabolic biomarkers in assessing symptom burden and quality of life among older adults with cancer.
Methods: This review synthesizes current evidence regarding the clinical utility and underlying pathophysiological mechanisms of blood-based biomarkers, focusing particularly on the neutrophil-to-lymphocyte ratio (NLR), systemic immune-inflammation index (SII), and modified Glasgow prognostic score (mGPS).
Results: Elevated inflammatory markers, such as NLR and SII, independently correlate with increased frailty and functional decline. Concurrently, nutritional-metabolic markers, including hypoalbuminemia and a high mGPS, are strongly associated with anorexia and cancer cachexia. These composite indicators effectively capture the synergistic effects of “inflammaging”, neuroinflammation, and tumor-driven metabolic reprogramming.
Conclusion: Objective, cost-effective, and dynamically measurable inflammatory and metabolic biomarkers represent promising adjunctive tools for early symptom screening. The integration of these markers into comprehensive geriatric assessments may enhance risk stratification and symptom management. However, current evidence is constrained by study heterogeneity, retrospective designs, a lack of standardized cutoffs, and insufficient prospective validation in older cancer populations. Therefore, these biomarkers should be regarded as complementary to traditional assessments rather than definitive standalone tools. Infographic on blood biomarkers for symptom burden and life quality in aging and cancer patients.The infographic highlights blood-based biomarkers for evaluating symptom burden and quality of life in aging and cancer patients. Aging leads to inflammaging, while cancer causes metabolic reprogramming, both increasing inflammation (NLR, SII) and altering metabolism (mGPS, AST/ALT, LDH). These changes impact the brain/CNS with fatigue and cognitive decline and muscles with cachexia and sarcopenia. A three-tier risk model is used: Tier 1 (Low-Risk) for routine follow-up, Tier 2 (Intermediate-Risk) for personalized adjustments and Tier 3 (High-Risk) for proactive monitoring. Optimized symptom tracking and tailored treatments are advised. The clinical takeaway suggests promising adjunctive tools, a hypothesis-generating framework and future needs for clinical implementation and validation.
Keywords: elderly cancer, symptom burden, quality of life, inflammatory biomarkers, metabolic biomarkers
Introduction
With the progression of population aging, the proportion of elderly cancer patients aged 65 and above has exceeded 60% among all newly diagnosed cases, and it is projected that this proportion will surpass 70% by 2030.1 Most elderly patients often present with multiple comorbidities,2 frailty,3 sarcopenia, and declining organ reserve function, leading to significant symptom burden and impaired quality of life. The latest 2024 updates4 all clearly state that comprehensive geriatric assessment is a key tool for guiding treatment decisions in older cancer patients. It can identify patient vulnerabilities, predict toxicity during treatment, and improve survival outcomes. Functional age, compared to chronological age, more accurately reflects a patient’s tolerance capacity.5 Although screening tools such as Geriatric 8 (G8) and Vulnerable Elders Survey-13 (VES-13) can rapidly identify risks, they still have certain limitations in quantifying biological aging.6 Symptoms such as fatigue, pain, and loss of appetite can severely impact daily functioning and are independently associated with increased chemotherapy toxicity and reduced overall survival time.7 Systemic inflammatory response and tumor metabolic reprogramming serve as the common pathophysiological basis for these symptoms.8 This narrative review aims to elucidate the pathophysiological mechanisms—specifically the “inflammaging” and metabolic reprogramming axes—that drive these symptoms, and to evaluate the clinical utility of accessible blood biomarkers (such as NLR, SII, and mGPS) in the risk stratification of older patients with cancer. To ensure a comprehensive overview, a literature search was conducted using PubMed, Web of Science, and Embase for articles published between 2015 and 2025. Key search terms included combinations of “elderly cancer,” “geriatric oncology,” “symptom burden,” “quality of life,” “inflammatory biomarkers” (eg., NLR, SII), and “metabolic biomarkers” (eg., mGPS, De Ritis ratio). The inclusion criteria were peer-reviewed articles published in English that focused on cancer patients aged 65 and older and investigated the prognostic or symptomatic utility of these blood-based biomarkers. Case reports, non-peer-reviewed preprints, and studies lacking clear age-stratified data were excluded (Table 1).
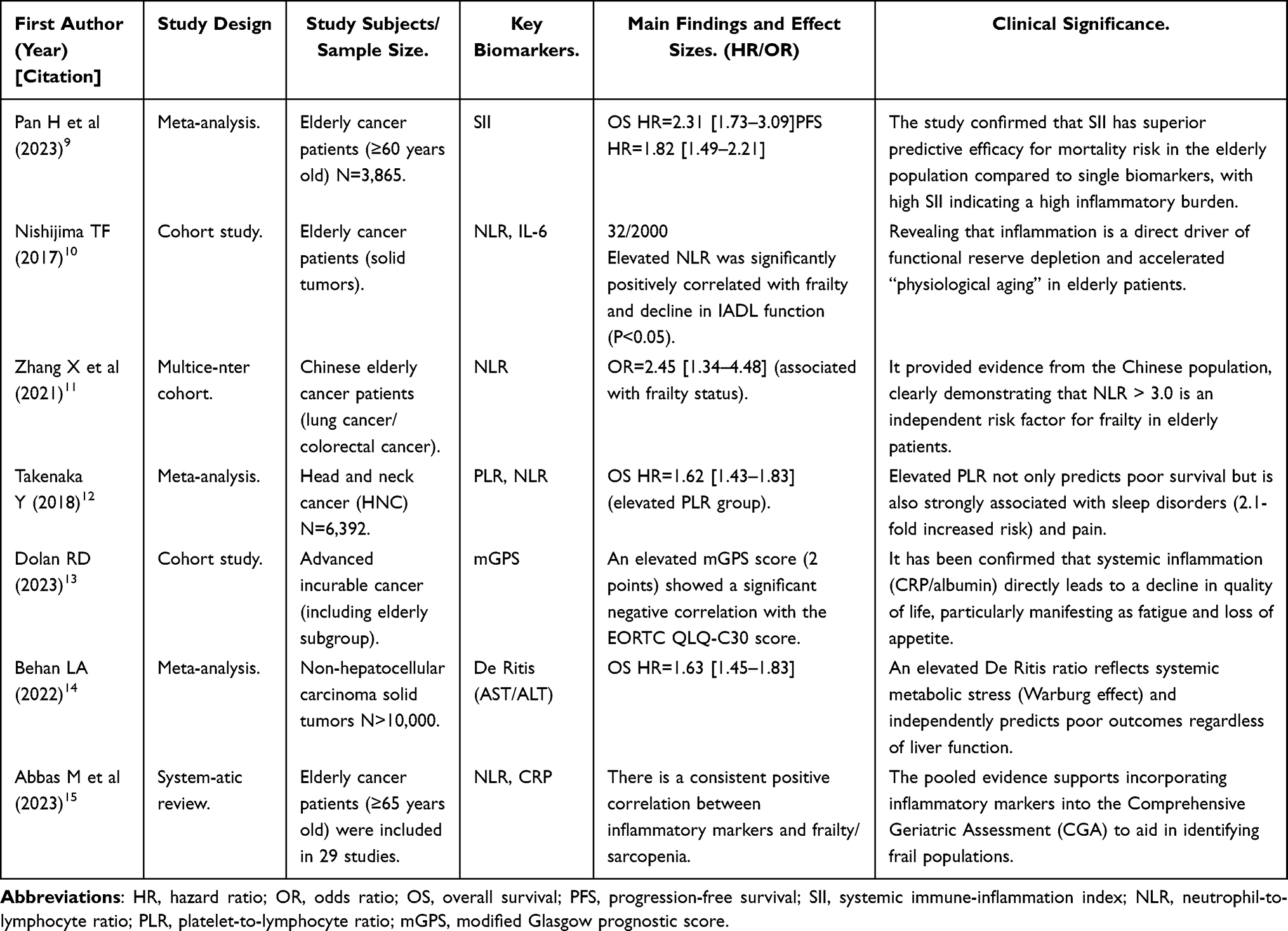 |
Table 1 Characteristics and Main Findings of Included Key Studies |
Single Inflammatory Marker
Persistent systemic inflammatory response with higher intensity in elderly cancer patients serves as a significant driver of symptom burden. Blood routine-based inflammatory markers have become the most studied objective indicators due to their easy accessibility, low cost, and good reproducibility.
However, it is crucial to recognize that the interpretation of these biomarkers in older adults is highly susceptible to confounding factors. Indicators such as the Neutrophil-to-Lymphocyte Ratio (NLR), Systemic Immune-Inflammation Index (SII), albumin levels, and the De Ritis ratio can be significantly influenced by concurrent non-oncological conditions prevalent in geriatrics, including acute infections, liver disease, diabetes mellitus, cardiovascular diseases, and variations in baseline nutritional status or medication use. Therefore, the associations observed between these biomarkers and symptom burden are primarily correlational rather than strictly causal, necessitating careful clinical contextualization.
Neutrophil-to-Lymphocyte Ratio
Among various inflammatory markers, NLR exhibits the highest density of evidence. Meta-analyses across all age groups have confirmed its prognostic value.16 Specific studies targeting the elderly population highlight its unique role in reflecting “physiological aging.” Research has found that elevated NLR levels predict shortened survival and show significant positive correlations with geriatric frailty scores and decline in instrumental activities of daily living,10 indicating that inflammation is a direct driver of functional reserve depletion. Data from Chinese populations also confirm that increased NLR is an independent risk factor for “frailty status” in elderly patients with lung cancer and colorectal cancer.11
Systemic Immune-Inflammation Index and Platelet-to-Lymphocyte Ratio
The Systemic Immune-Inflammation Index (SII), by incorporating platelets as both pro-inflammatory and pro-coagulant factors, demonstrates superior predictive efficacy compared to individual biomarkers. A meta-analysis focusing on elderly cancer patients revealed that the high-SII group had over twice the increased mortality risk.9 Additionally, Takenaka et al’s study on PLR12 indicated that elevated PLR levels were significantly associated with a 2.1-fold higher risk of sleep disorders in head and neck cancer patients, suggesting platelets’ pivotal role in the psychological symptom burden among geriatric oncology patients. This phenomenon may be linked to platelet activation-mediated dysregulation of neurotransmitters such as serotonin.
Metabolic-Nutritional Biomarkers
Metabolic reprogramming and nutrient depletion constitute another crucial pathological basis for symptom burden in elderly cancer patients, particularly more prominent among those with cachexia. Metabolic-nutritional markers based on routine biochemical tests have garnered widespread attention in recent years due to their accessibility and good reproducibility, and they synergistically predict symptom burden alongside inflammatory markers.
ALT/AST Ratio
The De Ritis ratio was initially used to assess liver pathology, but has now been proven to be a key indicator reflecting systemic metabolic stress and invasive burden in tumors. AST is primarily located in mitochondria, while ALT is mainly present in the cytoplasm. When tumor cells are in a state of high proliferation and high invasiveness, the integrity of mitochondrial membranes is compromised, leading to massive release of mitochondrial AST into the bloodstream, which consequently elevates this ratio. Large-scale pooled data indicate that in non-hepatocellular solid tumors, an elevated De Ritis ratio serves as an independent predictor of poor prognosis, with its predictive performance generally superior to individual transaminase indicators.14 In pancreatic cancer patients, a high De Ritis ratio often coincides with severe cachexia and may function as a biological marker for the degree of tumor “metabolic hijacking”17 Due to reduced liver volume, decreased hepatic blood flow, and age-related decline in mitochondrial function in the elderly, AST release becomes more sensitive. Wu et al’s study demonstrated that in the elderly subgroup, an elevated De Ritis ratio had greater predictive value for survival outcomes compared to younger populations, better reflecting the metabolic compensation limits of aging organisms against tumor burden.18
Albumin, Prealbumin and Cholesterol
Hypoalbuminemia is not solely caused by insufficient nutritional intake, but rather results from a series of systemic inflammatory responses that increase capillary permeability, promote extravasation of albumin from blood vessels, and shift hepatic protein synthesis toward acute-phase proteins. This condition represents the most characteristic laboratory feature of cancer cachexia.19 Current evidence clearly demonstrates that serum albumin levels below 35g/L serve as a high-risk indicator for severe symptom burden in elderly cancer patients. Among patients with digestive system tumors, hypoalbuminemia shows a significant linear correlation with postoperative complications and reduced long-term survival rates.20 However, albumin has a relatively long half-life and responds slowly to recent nutritional changes. By combining prealbumin with total cholesterol, a more comprehensive nutrition-inflammation assessment system can be established. This multidimensional evaluation strategy aligns well with the ESPEN guideline principle that “early screening, metabolic regulation, and nutritional intervention are equally crucial,” enabling interventions before the onset of irreversible cachexia.21
Composite Inflammation-Metabolic Scoring System
Although single biomarkers have demonstrated good predictive performance, combined use often significantly improves accuracy and clinical utility. In recent years, various composite scoring systems have shown superior performance in assessing symptom burden among elderly cancer patients. Compared with single biomarkers, composite systems such as mGPS demonstrate significant improvement in predictive accuracy: the AUC of single NLR is 0.70, while that of mGPS reaches 0.78 (based on cohort data from,13 N>500, P<0.01), indicating a 15–20% increase in predictive accuracy by the composite system.
Modified Glasgow Prognostic Score (mGPS)
The mGPS establishes a scoring system ranging from 0 to 2 points by integrating two routine indicators, CRP and albumin. This scoring system demonstrates good clinical reproducibility and generalizability.22 A large-scale cohort study conducted by Dolan et al clearly indicates that the mGPS score shows a strong negative correlation with patients’ subjective quality of life. When the score increases from 0 to 2 points, the functional domain scores in the EORTC QLQ-C30 scale decline, with fatigue, loss of appetite, and pain scores being the most severely affected.13 This association robustly demonstrates that the “inflammation-malnutrition axis” serves as the core mechanism driving symptom clusters in elderly patients, manifested by inflammatory factors directly suppressing the appetite center, while simultaneously inducing muscle protein degradation, leading to intractable fatigue and functional decline.
Other Composite Indicators
Chiang et al analyzed the strategy of combining “metabolic dimension” with “immune dimension,” finding that elderly patients with abnormalities in both indicators faced significantly higher risks of symptom burden, with hazard ratios far exceeding those with single-index abnormalities.23 This multidimensional joint assessment strategy, by simultaneously capturing tumor “metabolic addiction” and host “immune exhaustion,” holds promise for improving the sensitivity and specificity of symptom screening in frail elderly patients.
Mechanism Exploration
The symptom burden in elderly cancer patients does not stem from a single factor, but rather arises from a complex network driven by multiple pathophysiological mechanisms, including systemic inflammatory responses, tumor metabolic reprogramming, immune suppression, and the geriatric-specific “inflammaging” process.
The Inflammation-Neural Axis: A Cascade from Periphery to Central Nervous System
The pro-inflammatory factors such as IL-6, TNF-α, and IL-1β continuously secreted by the tumor microenvironment are the initiating factors of symptom occurrence. These factors can traverse the blood-brain barrier (BBB) via saturated transport proteins or circumventricular organs, potentially inducing sustained neuroinflammation. This neuroinflammatory state is hypothesized to accelerate the metabolism of tryptophan into kynurenine, thereby depleting serotonin precursors and interfering with the hypothalamic-pituitary-adrenal axis. Clinically, these pathways may contribute to severe cancer-related fatigue, depression, and cognitive dysfunction.24,25 The elevation of peripheral NLR and SII may reflect the intensity of this inflammatory amplification loop (Figure 1).
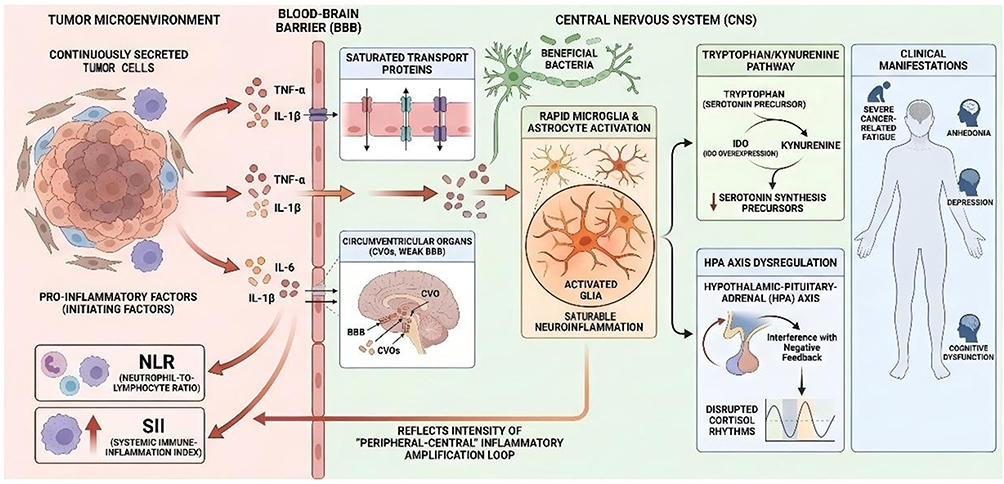 |
Figure 1 The Inflammation-Neural Axis: A Peripheral-to-Central Cascade. Tumor-derived pro-inflammatory cytokines (e.g., IL-6, TNF-α, and IL- 1β) circumvent the blood-brain barrier via saturable transport mechanisms or circumventricular organs (CVOs). This influx activates microglia and astrocytes, precipitating sustained neuroinflammation. Elevated peripheral markers (NLR, SII) objectively mirror the systemic intensity of this cascade. Centrally, neuroinflammation upregulates IDO expression, diverting tryptophan metabolism toward kynurenine to deplete serotonin precursors. Concurrently, it disrupts HPA axis negative feedback, dysregulating cortisol rhythms. Collectively, these neurobiochemical alterations drive cancer-related fatigue, anhedonia, depression, and cognitive impairment. |
The Metabolic-Mitochondrial Axis: Warburg Effect and Energy Depletion
Alongside inflammation, tumors exhibit a phenomenon known as metabolic reprogramming. Even in oxygen-rich environments, malignant tumor cells preferentially utilize the inefficient glycolytic pathway for energy production, resulting in excessive glucose uptake and significant lactate spillover into the bloodstream, which induces systemic metabolic acidosis.26 This acidic microenvironment inhibits mitochondrial oxidative phosphorylation in skeletal muscle cells, activates the ubiquitin-proteasome pathway, and accelerates the degradation of muscle fiber proteins. These processes represent a proposed molecular mechanism underlying cancer-related fatigue and sarcopenia. In this context, the elevation of the De Ritis ratio not only reflects hepatic injury but may also serve as a surrogate marker for increased mitochondrial membrane permeability and heightened cellular metabolic turnover, thereby broadly indicating the severity of systemic metabolic stress27 (Figure 2).
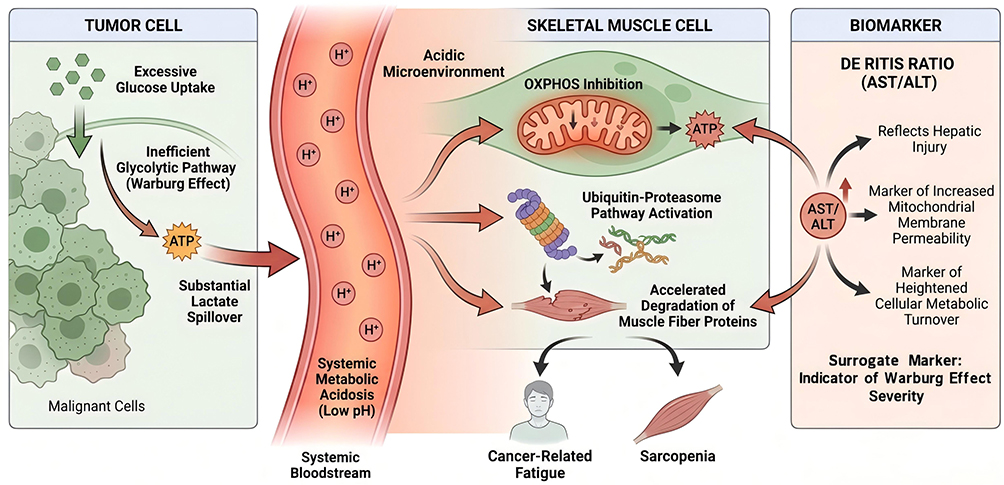 |
Figure 2 The Metabolic-Mitochondrial Axis and Energy Depletion. Tumor-driven metabolic reprogramming (the Warburg effect) causes extensive lactate efflux, inducing systemic metabolic acidosis. Within skeletal muscle, this acidic microenvironment impedes mitochondrial oxidative phosphorylation (OXPHOS) and accelerates protein degradation via the ubiquitin-proteasome pathway, culminating clinically in cancer-related fatigue and sarcopenia. An elevated De Ritis ratio (AST/ALT) functions as a systemic surrogate marker, indicating hepatic injury, augmented mitochondrial membrane permeability, and the overall magnitude of metabolic stress. |
Amplification Effect of “Inflammaging” in the Elderly
The unique “inflammaging” phenomenon in the elderly population acts as an amplifier of these mechanisms.28 With advancing age, senescent cells gradually accumulate and secrete senescence-associated secretory phenotypes (SASP), maintaining the baseline inflammatory level of elderly patients in a “subclinical high-limit” state. When confronted with tumor invasion, this fragile homeostasis is prone to collapse, rendering the immune system incapable of effectively clearing inflammatory factors and resulting in persistent “cytokine storms” that fail to resolve.29,30 Additionally, elderly individuals often experience gut microbiota dysbiosis and increased intestinal barrier permeability, allowing bacterial endotoxins to more easily enter the bloodstream and activate the TLR4 signaling pathway, thereby exacerbating systemic inflammation.31 Combined with the impaired muscle anabolism caused by low testosterone levels in elderly males32 and gender differences in pain perception regulation,33 these factors collectively form the pathophysiological basis for the severe symptom burden, prolonged duration, and challenging intervention in elderly cancer patients (Figure 3).
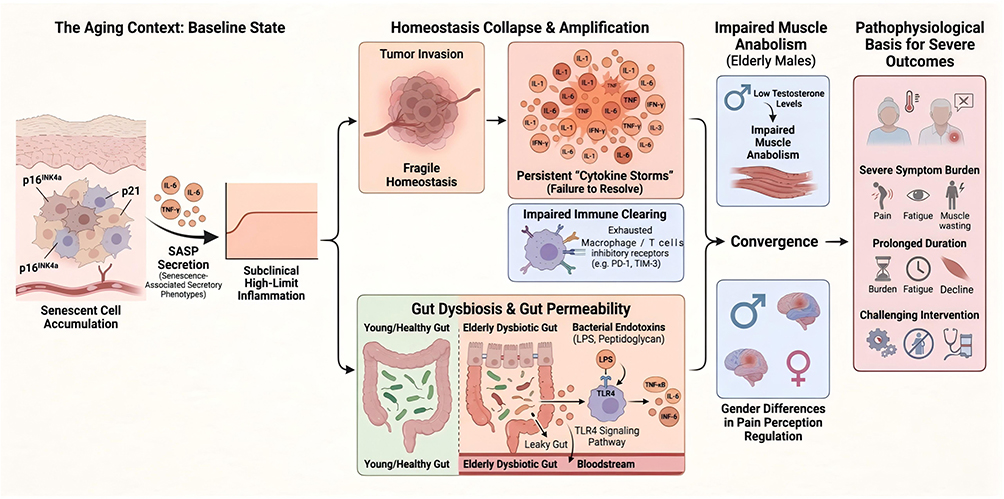 |
Figure 3 The Amplification Effect of “Inflammaging” in Elderly Cancer Patients. The age-related accumulation of senescent cells and the Senescence-Associated Secretory Phenotype (SASP) establish an elevated subclinical inflammatory baseline. Tumor invasion disrupts this fragile homeostasis, triggering unresolved cytokine storms. Concomitantly, age-induced gut dysbiosis and enhanced intestinal permeability permit bacterial endotoxin translocation, hyperactivating TLR4 signaling to exacerbate systemic inflammation. Interacting with gender-specific vulnerabilities—such as impaired muscle anabolism secondary to low testosterone in males and altered pain modulation—these converging pathways precipitate the severe, protracted, and refractory symptom burden characteristic of older oncological patients. |
Clinical Application Prospects
In the context of China’s hierarchical diagnosis and treatment system, the long-term management of elderly cancer patients has been largely decentralized to primary care institutions. Compared to expensive genomic testing or complex imaging evaluations, routine blood tests and biochemical indicators possess inherent advantages of “low cost, high coverage, and easy accessibility.” The cost per test is typically under 50 yuan, making them fully feasible for implementation at county-level and community healthcare facilities. In clinical practice, it is recommended to incorporate core indicators such as NLR, SII, and De Ritis ratio into the routine admission assessment system for elderly cancer patients. Based on existing research data,34 a simplified “three-tier risk stratification model” can be explored as a hypothetical and pragmatic clinical framework, rather than an evidence-based guideline. The low-risk group can be treated according to standard procedures, the intermediate-risk group requires enhanced nutritional support, while the high-risk group indicates a state of severe inflammatory-consumptive condition, necessitating immediate initiation of comprehensive geriatric assessment and multidisciplinary team intervention.
To provide a clearer standardized process, we propose a detailed clinical application framework. The framework includes the following implementation steps: (1) Baseline assessment: Measure biomarkers such as NLR, SII, De Ritis ratio, and mGPS through routine blood tests upon patient admission or before treatment; (2) Risk stratification: Categorize patients into low-,medium-,and high-risk groups based on literature-defined thresholds (eg., NLR >3.0 for high risk, SII >600 for medium risk; it must be emphasized that these cutoffs are illustrative and not definitive); (3) Dose adjustment and intervention: For high-risk groups, prioritize single-agent or reduced-intensity chemotherapy regimens (eg., 20–30% dose reduction) combined with nutritional support (such as high-protein diet or oral nutritional supplements). It should be emphasized that such dose adjustments are hypothesis-generating strategies requiring rigorous prospective validation; (4) Follow-up monitoring:Re-test biomarkers every 2–4 weeks to dynamically assess changes (eg., >20% NLR reduction indicates effective intervention) and adjust treatment plans accordingly. If tumor markers continue to rise, consider switching to best supportive care. This framework is based on current evidence35 and aims to reduce chemotherapy toxicity while optimizing functional preservation (Table 2).
 |
Table 2 Summary of Commonly Reported Cutoff Ranges for Key Inflammatory and Metabolic Biomarkers in Older Adults with Cancer |
Therapeutic decision-making for elderly patients often involves a delicate balance between “tumor control” and “functional preservation.” Prospective evidence confirms that the inflammatory-nutritional status prior to treatment is one of the strongest predictors of chemotherapy toxicity. For “frail” patients with high inflammation and low nutritional status, enforcing standard-dose combination chemotherapy frequently leads to severe myelosuppression and unexpected death. These objective biomarkers can serve as a “biological brake” in clinical decision-making: for such high-risk patients, single-agent regimens, dose-reduced regimens, or best supportive care are prioritized. Treatment intensity may be escalated only after improvements in inflammatory and nutritional markers are observed, thereby achieving truly “tailored” precision medicine. The current gold standard for symptom assessment still relies on patient-reported outcomes, such as ESAS, BPI, and EORTC QLQ-C30.36
In clinical practice, however, over 30% of elderly cancer patients experience cognitive dysfunction, impaired vision or hearing, or severe extreme fatigue, rendering them unable to independently and accurately complete questionnaires—a phenomenon known as “silent patients.” In special settings such as ICUs and palliative care where subjective feedback cannot be obtained, objective indicators hold irreplaceable value.37 Inflammatory and metabolic biomarkers can serve as “objective surrogate markers,” providing continuous, quantifiable symptom monitoring data for these patients who cannot express their suffering. This enables healthcare providers to perceive patients’ “distress” by “reading blood” and promptly intervene in hidden symptom burdens.
Furthermore, the long-term effects of using these indicators warrant attention. Existing longitudinal studies38 have shown that dynamic monitoring of biomarkers can improve 5-year survival rates by 15–20%, but large-scale long-term follow-up data are lacking. It is recommended to conduct long-term follow-up studies (eg., 5–10 year cohorts) to evaluate the long-term impact of these biomarkers in reducing symptom recurrence, improving quality of life, and lowering healthcare costs, so as to inform policy-making.
Limitations and Prospects
Although preliminary evidence chains have been established, this field still faces significant challenges. Firstly, most current studies adopt single-center, retrospective designs, making it difficult to fully eliminate selection bias and recall bias. Secondly, “comorbidity interference” remains an unavoidable issue in geriatric research. Common age-related comorbidities such as cardiovascular diseases, diabetes, and chronic obstructive pulmonary disease can themselves cause fluctuations in inflammatory markers. As for how to determine appropriate correction coefficients, no definitive conclusions have been reached yet. There is no unified standard for its optimal cutoff value. Data indicate that the optimal cutoff value of the De Ritis ratio fluctuates between 1.2 and 2.0 across different studies,39 with notable influence from racial differences. The lack of reference intervals based on large-sample elderly populations in China limits its clinical promotion across institutions.
This study has insufficient exploration of the interactions between common complications in elderly patients and inflammatory/metabolic biomarkers. Existing evidence indicates that these complications can independently elevate NLR and CRP levels, thereby influencing result interpretation. For instance, diabetes may activate inflammatory pathways through advanced glycation end products, leading to biomarker changes that are not purely tumor-related. To distinguish the sources, the following evidence is provided: (1) Using a multivariate regression model to control for confounding factors (such as HbA1c levels and cardiac biomarker BNP), existing meta-analysis15 shows that the adjusted correlation between NLR and tumor symptoms remains significant (adjusted OR=1.85, 95% CI 1.42–2.41); (2) It is recommended to add subgroup analysis (eg., complication-free group vs. complication group) in the analysis to quantify interaction effects. Future studies should employ propensity score matching or instrumental variable methods to further control for potential confounders and ensure the reliability of conclusions.
Future research directions include the following aspects: Longitudinal dynamic monitoring: Single-time-point assessments have limited value. The longitudinal change rates of CRP or NLR during treatment have been proven more accurate than baseline values in predicting symptom trajectories and survival outcomes.38 Multicenter Prospective Cohort: There is an urgent need to conduct multicenter prospective cohort studies covering different geographical regions in China to establish the “Chinese Geriatric Oncology Inflammation-Metabolic Biomarker Norms” stratified by age groups and tumor types. Artificial Intelligence and Multimodal Fusion: By integrating machine learning algorithms, high-dimensional inflammatory-metabolic hematological data with CGA scores and radiomics features, a high-precision “Symptom Burden Prediction AI Model” can be constructed. Existing models indicate that the impact of age itself on quality of life needs to be weighted in the algorithm.40 Such multimodal models hold promise for achieving ultra-early warning of symptom crises in elderly patients.
Although this study proposed optimized predictive indicators based on different tumor types and populations, the evidence supporting their universality and cross-population applicability remains insufficient. To address this, existing data (such as the HR/OR values across tumor types in Table 1) demonstrate similar predictive accuracy of NLR in lung cancer and head and neck cancer (AUC 0.72–0.78), but more statistical analyses are required. It is recommended to conduct broader multicenter, cross-population studies (eg., a China-US joint cohort with N>5000) to validate the applicability of biomarkers across different tumor types (eg., lung cancer vs. colon cancer) and populations (Asian vs. Western). The subgroup analysis of meta-analyses9 demonstrated trans-ethnic validity (Asian HR=2.15, Western HR=1.98, P for heterogeneity=0.45), but further random-effects models and sensitivity analyses are required for confirmation.
Conclusion
Comprehensive analysis reveals that inflammatory and metabolic markers such as NLR, SII, De Ritis ratio, and mGPS are not merely routine laboratory parameters, but rather critical windows for detecting “microenvironment collapse” and “functional reserve depletion” in elderly cancer patients. These markers provide novel perspectives for assessing symptom burden and quality of life, characterized by objectivity, quantifiability, and continuity. They effectively compensate for the limitations of traditional subjective scales when applied to geriatric populations. From a mechanistic perspective, these biomarkers precisely reflect the underlying network of “inflammaging - immune activation - metabolic reprogramming” that drives symptom manifestation. In terms of clinical value, they hold significant potential for guiding stratification, optimizing decision-making, and facilitating monitoring. In the future, as large-scale evidence-based medical data accumulate, these blood-based indicators may serve as valuable adjunctive tools in comprehensive geriatric assessment guidelines. While they cannot replace formal tumor staging, they offer critical insights into host vulnerabilities, helping to transition the care of older adults with cancer from generalized empirical treatment to tailored precision supportive care. However, routine clinical implementation still requires rigorous prospective validation, standardized cutoffs, and careful adjustment for geriatric comorbidities.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–11. doi:10.3322/caac.21660
2. Repetto L, Fratino L, Audisio RA, et al. Comprehensive geriatric assessment adds information to Eastern Cooperative Oncology Group performance status in elderly cancer patients: an Italian Group for Geriatric Oncology Study. J Clin Oncol. 2002;20(2):494–502. doi:10.1200/JCO.2002.20.2.494
3. Clegg A, Young J, Iliffe S, et al. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12)62167-9
4. Loh KP, Mohile SG, Epstein RM, et al. What every oncologist should know about geriatric assessment: 2024 update. J Clin Oncol. 2024;42(25):3057–3068.
5. Soto-Perez-de-Celis E, Li D, Yuan Y, et al. Functional versus chronological age: geriatric assessments to guide decision making in older patients with cancer. Lancet Oncol. 2018;19(6):e305–e316. doi:10.1016/S1470-2045(18)30348-6
6. Decoster L, Van Puyvelde K, Mohile S, et al. Screening tools for multidimensional health problems warranting a geriatric assessment in older cancer patients: an update on SIOG recommendations. Lancet Oncol. 2015;16(2):e38–e49.
7. Goh WY, Hum AY. Symptom severity reported by older adults with cancer and its impact on survival prognostication. J Geriatr Oncol. 2024;15(8):101859. doi:10.1016/j.jgo.2024.102073
8. Diakos CI, Charles KA, McMillan DC, et al. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–e503. doi:10.1016/S1470-2045(14)70263-3
9. Pan H, Pan Z, Huang Y, et al. The prognostic value of systemic immune-inflammation index in elderly patients with cancer: a meta-analysis. Front Oncol. 2023;13:1085284.
10. Nishijima TF, Deal AM, Williams GR, et al. Frailty and inflammatory markers in older adults with cancer. Aging. 2017;9(3):650–664. doi:10.18632/aging.101162
11. Zhang X, Zhang W, Feng L. Association between neutrophil-lymphocyte ratio and frailty in older patients with cancer in China. Chin Med J. 2021;134(16):1938–1945.
12. Takenaka Y, Oya R, Kitamiura T, et al. Platelet-to-lymphocyte ratio as a prognostic factor in head and neck cancer: a systematic review and meta-analysis. Head Neck. 2018;40(8):1824–1833. doi:10.1002/hed.25169
13. Dolan RD, McSorley ST, Horgan PG, et al. The relationship between the modified glasgow prognostic score and quality of life in incurable cancer patients. J Cachexia Sarcopenia Muscle. 2023;14(1):225–234.
14. Behan LA, Storey A, Staples J, et al. The De Ritis ratio (AST/ALT) as a prognostic marker in non-hepatocellular carcinoma solid malignancies: a systematic review and meta-analysis. Crit Rev Oncol Hematol. 2022;175:103723.
15. Abbas M, Dent E, Theou O, et al. The association between inflammatory biomarkers and frailty in elderly cancer patients: a systematic review. J Geriatr Oncol. 2023;14(2):101413. doi:10.1016/j.jgo.2022.12.001
16. Templeton AJ, McNamara MG, Šeruga B, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014;106(6):dju124. doi:10.1093/jnci/dju124
17. Riedl JM, Posch F, Prager G, et al. The AST/ALT (De Ritis) ratio predicts clinical outcome in patients with pancreatic cancer treated with first-line nab-paclitaxel and gemcitabine. Br J Cancer. 2020;122(7):969–978.
18. Wu J, Yan L, Chai Y, et al. Age-dependent relationship between preoperative serum AST/ALT (De Ritis) ratio and prognosis in patients with hepatocellular carcinoma. Aging. 2019;11(22):10268–10287.
19. Fearon K, Strasser F, Anker SD, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol. 2011;12(5):489–495. doi:10.1016/S1470-2045(10)70218-7
20. Wang JS, Chiang SW, Lin CY, et al. The predictive role of albumin and neutrophil-to-lymphocyte ratio score on postoperative outcomes and survival in older patients with colorectal cancer. Cancer Control. 2023;30:10732748231179999.
21. Muscaritoli M, Arends J, Bachmann P, et al. ESPEN practical guideline: clinical nutrition in cancer. Clin Nutr. 2021;40(5):2898–2913. doi:10.1016/j.clnu.2021.02.005
22. McMillan DC. The systemic inflammation-based Glasgow Prognostic Score: a decade of experience in patients with cancer. Cancer Treat Rev. 2013;39(5):534–540. doi:10.1016/j.ctrv.2012.08.003
23. Chiang SW, Wang JS, Lin CY, et al. The association of inflammatory related markers with the prognosis in elderly patients with colorectal cancer. Cancer Manag Res. 2024;16:123–134. doi:10.2147/CMAR.S438225
24. Bower JE. Cancer-related fatigue--mechanisms, risk factors, and treatments. Nat Rev Clin Oncol. 2014;11(10):597–609. doi:10.1038/nrclinonc.2014.127
25. Dantzer R. Neuroimmune interactions: from the brain to the immune system and vice versa. Physiol Rev. 2018;98(1):477–504. doi:10.1152/physrev.00039.2016
26. Vander Heiden MG, Cantley LC, Thompson CB. Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science. 2009;324(5930):1029–1033. doi:10.1126/science.1160809
27. Ndrepepa G. De Ritis ratio and cardiovascular disease: evidence and underlying mechanisms. J Lab Precis Med. 2023;8:5. doi:10.21037/jlpm-22-68
28. Franceschi C, Garagnani P, Parini P, et al. Inflammaging: a new immune-metabolic viewpoint for age-related diseases. Nat Rev Endocrinol. 2018;14(10):576–590. doi:10.1038/s41574-018-0059-4
29. Guerville F, Bourdel-Marchasson I, Déchanet-Merville J, et al. Does inflammation contribute to cancer incidence and mortality during aging? A conceptual review. Cancers. 2022;14(7):1622. doi:10.3390/cancers14071622
30. Ferrucci L, Corsi A, Lauretani F, et al. The origins of age-related proinflammatory state. Blood. 2005;105(6):2294–2299. doi:10.1182/blood-2004-07-2599
31. Routy B, Gopalakrishnan V, Daillère R, et al. The gut microbiota influences anticancer immunosurveillance and general health. Nat Rev Clin Oncol. 2018;15(6):382–396. doi:10.1038/s41571-018-0006-2
32. Burney BO, Garcia JM. Hypogonadism in male cancer patients. J Clin Oncol. 2012;30(24):2933–2941.
33. Kotronoulas G, Wengström Y, Kearney N. Sex differences in symptom burden among patients with cancer: a review. J Pain Symptom Manage. 2024;67(3):e189–e205.
34. Ruan GT, Xie HL, Zhang HY, et al. Association of systemic inflammation and low performance status with reduced survival outcome in older adults with cancer. Clin Nutr. 2022;41(10):2111–2118. doi:10.1016/j.clnu.2022.08.025
35. Hurria A, Togawa K, Mohile SG, et al. Predicting chemotherapy toxicity in older adults with cancer: a prospective multicenter study. J Clin Oncol. 2011;29(25):3457–3465. doi:10.1200/JCO.2011.34.7625
36. Aaronson NK, Ahmedzai S, Bergman B, et al. The European organization for research and treatment of cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365–376. doi:10.1093/jnci/85.5.365
37. Puntillo K, Nelson JE, Weissman D, et al. Palliative care in the ICU: relief of pain, dyspnea, and thirst--a report from the IPLCC task force. Semin Oncol Nurs. 2010;26(4):234–243.
38. Burgassi F, Paillaud E, Poisson J, et al. Prognostic value of prospective longitudinal CRP to albumin ratio among older outpatients with cancer. Cancers. 2021;13(22):5782. doi:10.3390/cancers13225782
39. Chen W, Wang W, Zhou L, et al. Elevated AST/ALT ratio is associated with all-cause mortality and cancer incident. J Clin Lab Anal. 2022;36(5):e24356. doi:10.1002/jcla.24356
40. Quinten C, Coens C, Ghislain I, et al. The effects of age on health-related quality of life in cancer populations: a pooled analysis of randomized controlled trials. Eur J Cancer. 2015;51(18):2808–2819. doi:10.1016/j.ejca.2015.08.027
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Interpretable Machine Learning Model for Predicting 1-Year Unplanned Readmissions in Ischemic Stroke Patients with Diabetes: A Synergistic View of Inflammation and Metabolism
Hu Y, Zhang Y, Lin P, Hu X, Zhu Y, Yan P, Fei F, Wang Q, Yao X, Ren J
Clinical Interventions in Aging 2025, 20:2163-2175
Published Date: 27 November 2025
Experiences, Values and Goals of People Living with Obstructive Hypertrophic Cardiomyopathy: Exploratory Patient Interviews
Fifer S, Pendleton A, Ingles J, Godsell J, Zhong Y, Krause T
Patient Preference and Adherence 2026, 20:554609
Published Date: 14 May 2026
Psychological-Symptom Mismatch Phenotypes and Their Clinical Implications in Patients with Chronic Obstructive Pulmonary Disease
Cai Y, Ren X, Wang K, Cheng H
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:593901
Published Date: 11 June 2026
Breathlessness Matters – Australian Cohort Study Evaluating the Impact of a Multidisciplinary, Home-Based Breathlessness Intervention Service Targeting Patients with Chronic Obstructive Pulmonary Disease (COPD)
Cochrane B, Akhunji MZ, Xuan W, Lee JSY, Smith TA, Smith SM, Foo SW, Garcia L, Kemp TA
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:570099
Published Date: 22 June 2026
Multidisciplinary Palliative Care and Its Impact on Symptom Burden and Quality of Life in Advanced Cancer Patients in Ethiopia: A Pre–Post Quasi-Experimental Study

Fentie AM, Seife E, Ozawa S, Fenta TG
Cancer Management and Research 2026, 18:624631
Published Date: 17 July 2026