Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Psychological-Symptom Mismatch Phenotypes and Their Clinical Implications in Patients with Chronic Obstructive Pulmonary Disease
Authors Cai Y, Ren X, Wang K, Cheng H
Received 5 January 2026
Accepted for publication 1 June 2026
Published 11 June 2026 Volume 2026:21 593901
DOI https://doi.org/10.2147/COPD.S593901
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Yingying Cai,1 Xiaohe Ren,2 Kefang Wang,3 He Cheng4
1Gynecology, Qilu Hospital of Shandong University (Qingdao), Qingdao, Shandong, People’s Republic of China; 2Outpatient Department, Qilu Hospital of Shandong University (Qingdao), Qingdao, Shandong, People’s Republic of China; 3School of Nursing and Rehabilitation, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, People’s Republic of China; 4Otolaryngology Head and Neck Surgery Center, Qingdao Otolaryngology Head and Neck Surgery Clinical Research Center, Qilu Hospital of Shandong University (Qingdao), Qingdao, Shandong, People’s Republic of China
Correspondence: He Cheng, Otolaryngology Head and Neck Surgery Center, Qingdao Otolaryngology Head and Neck Surgery Clinical Research Center, Qilu Hospital of Shandong University (Qingdao), Qingdao, Shandong, People’s Republic of China, Email [email protected]
Purpose: Psychological distress in Chronic obstructive pulmonary disease (COPD) patients often does not correspond to symptom severity. The clinical significance of psychological–symptom mismatch phenotypes is unclear. To identify psychological–symptom mismatch phenotypes in COPD and examine their associations with clinical outcomes.
Patients and Methods: A cross-sectional study was conducted in 306 COPD patients from a tertiary hospital in Shandong, China. Latent profile analysis was applied to standardized measures of anxiety, depression, lung function, symptom severity, and dyspnea to identify phenotypes. Multivariable linear and negative binomial regressions assessed associations with clinical outcomes.
Results: Four phenotypes were identified: psychological-dominant mismatch (22%), low (47%), moderate (26%), and high psychological–symptom burden (5%). The mismatch phenotype was characterized by disproportionately elevated psychological burden relative to symptom burden and was associated with the poorest quality of life. In adjusted analyses, patients in the low, moderate, and high burden phenotypes had better quality of life than those in the mismatch phenotype (all P < 0.001). Patients in the low and moderate burden phenotypes had fewer hospitalizations in the preceding year (incidence rate ratios, 0.592 [95% CI, 0.355– 0.989] and 0.233 [95% CI, 0.141– 0.386], respectively), whereas no significant difference was observed for the high burden phenotype. Differences in self-management and coping were limited, while patterns of health locus of control varied across phenotypes.
Conclusion: Psychological–symptom mismatch appears to be a common and clinically relevant pattern in COPD. Patients with a psychological-dominant mismatch phenotype exhibited poorer quality of life and a higher likelihood of hospitalization. These findings highlight the potential importance of incorporating psychological assessment into routine COPD care and suggest that phenotype-informed approaches may help identify patients with differing clinical needs.
Keywords: psychological distress, symptom burden, latent profile analysis, hospitalization, quality of life
Introduction
Chronic obstructive pulmonary disease (COPD) is a common chronic condition characterized by persistent airflow limitation and chronic respiratory symptoms and has become a major global public health challenge.1 According to the Global Burden of Disease study, COPD has consistently ranked among the leading causes of death worldwide and is associated with a substantial burden of disability, profoundly impairing patients’ quality of life, functional status, and social participation.2,3 With accelerating population aging and the continued prevalence of risk factors such as tobacco smoking, the prevalence and disease burden of COPD are expected to rise further, posing sustained challenges to health care systems and societal resources.
Traditionally, the assessment and management of COPD have focused primarily on pulmonary function impairment and respiratory symptoms, including the degree of airflow limitation, dyspnea, and the frequency of acute exacerbations. However, accumulating evidence suggests that reliance on lung function measures alone is insufficient to capture patients’ lived disease experience and health outcomes.4 Even among patients with comparable levels of pulmonary impairment, substantial heterogeneity exists in symptom perception, psychological status, self-management capacity, and quality of life.5 This pronounced heterogeneity underscores that COPD is not merely a “pulmonary disease,” but rather a complex chronic condition involving dynamic interactions among physiological, psychological, and behavioral dimensions. Within this context, increasing attention has been directed toward the role of psychological factors in the development, progression, and prognosis of COPD. Anxiety and depression are among the most prevalent psychological comorbidities in patients with COPD, with rates substantially exceeding those observed in the general population.6 These conditions are not only closely associated with greater symptom burden, poorer quality of life, and functional limitation, but may also indirectly increase the risk of acute exacerbations and hospitalizations by influencing illness perceptions, coping strategies, and treatment adherence.7 Nevertheless, most existing studies have examined psychological status and symptom burden as independent or linearly related variables, implicitly assuming a concordant relationship in which greater symptom severity corresponds to higher psychological distress.8 Such an approach overlooks the possibility of mismatch between psychological responses and symptom experiences. In clinical practice, some patients with COPD exhibit marked anxiety or depression despite relatively mild symptoms or limited pulmonary impairment, whereas others report substantial symptom burden while experiencing comparatively low levels of psychological distress. This inconsistency, or “mismatch,” between psychological burden and symptom burden may reflect individual differences in illness perception, coping resources, psychological resilience, and social support.9 Failure to recognize such mismatch patterns may result in underestimation or misclassification of patient risk and intervention needs, thereby undermining the development of precise, individualized management strategies.
In recent years, latent profile analysis (LPA), a person-centered statistical approach, has been increasingly applied to identify latent subgroups of patients with chronic diseases based on multidimensional characteristics.10 Compared with traditional variable-centered methods, LPA allows for the integration of multiple continuous or ordinal indicators without prespecified classification thresholds, enabling the identification of patient groups with similar patterns of characteristics and offering a novel methodological perspective for elucidating disease heterogeneity.11 However, in the field of COPD, studies that simultaneously integrate psychological burden and symptom burden to systematically examine psychological–symptom mismatch phenotypes remain scarce, and their clinical relevance has not been adequately established. More importantly, it remains unclear whether distinct psychological–symptom mismatch phenotypes differ meaningfully in key clinical outcomes. For example, it is unknown whether these phenotypes are differentially associated with hospitalization risk, quality of life, self-management capacity, health locus of control, or medical coping styles, and thus whether they possess identifiable and actionable clinical value. Addressing this gap may deepen understanding of the psychological–symptom interaction mechanisms in COPD and facilitate earlier identification of high-risk patients, thereby informing stratified management and precision intervention strategies in clinical practice.
Against this background, the present study enrolled patients with COPD and constructed a symptom burden index based on pulmonary function grading, symptom severity, and dyspnea level, alongside a psychological burden index derived from anxiety and depression measures. Latent profile analysis was applied to identify psychological–symptom mismatch phenotypes. Subsequently, demographic and clinical characteristics were compared across phenotypes, and associations between phenotype membership and multidimensional clinical outcomes—including annual hospitalizations, quality of life, self-management, health locus of control, and medical coping styles—were systematically examined. This study aimed to elucidate the existence and clinical significance of psychological–symptom mismatch phenotypes in patients with COPD, providing novel theoretical insights and empirical evidence to support patient-centered, precision assessment and integrated management.
Material and Methods
Study Design, Participants, and Ethical Considerations
This study used a cross-sectional design and was conducted between May 2021 and June 2022 at the pulmonary rehabilitation outpatient clinic of the Department of Respiratory and Critical Care Medicine in a tertiary general hospital in Shandong Province, China. Convenience sampling was applied to recruit eligible patients with COPD. Inclusion criteria were as follows: (1) a confirmed diagnosis of COPD according to the Guidelines for the Diagnosis and Treatment of Chronic Obstructive Pulmonary Disease (2021 edition), established by a respiratory physician; (2) age 18 years or older, with basic reading and comprehension ability, and the capacity to complete the questionnaire independently or with assistance from a trained investigator; and (3) voluntary participation with provision of written informed consent. Exclusion criteria included: (1) critical illness or acute exacerbation at the time of survey, precluding participation; and (2) a prior diagnosis of a psychiatric disorder or the presence of significant cognitive impairment that could interfere with questionnaire comprehension or completion.
Sample size estimation was based on methodological recommendations for latent profile analysis and regression modeling. In the present study, LPA was conducted using two composite indicators representing psychological and symptom burden, derived from multiple validated instruments, thereby reducing model dimensionality. Prior methodological research suggests that sample sizes of approximately 200–500 are generally sufficient to yield stable and reliable latent profile solutions when the number of indicators is limited and classification quality is adequate.12 A total of 310 questionnaires were distributed, of which 308 were returned (response rate: 99.35%). After exclusion of two questionnaires with substantial missing data, 306 valid questionnaires were included in the final analysis, yielding an effective response rate of 98.71%. The final sample size of 306 participants, together with satisfactory classification accuracy (entropy = 0.853) and adequate class proportions, was therefore considered appropriate for the present analysis.
This study was approved by the Ethics Committee of Qilu Hospital of Shandong University (Qingdao) (approval No. KYLL-QDQI2020084). All procedures involving human participants were conducted in accordance with the ethical standards of the institutional research committee and with the Declaration of Helsinki and its later amendments. Written informed consent was obtained from all participants prior to enrollment.
Measures
Sociodemographic and Clinical Characteristics
Sociodemographic and clinical characteristics were collected using a self-designed questionnaire, including age (years), sex (male/female), BMI, place of residence (rural area/county-level town or urban area), living arrangement (living alone/living with spouse and/or children), monthly per capita household income (<3000 yuan, 3000–5000 yuan, >5000 yuan), educational attainment (primary school or less, junior high school, senior high school, junior college or above), smoking status (current smoker, former smoker, never smoker), alcohol consumption status (current drinker, former drinker, never drinker), disease duration (years), and comorbidities (yes/no). Information on comorbidities was obtained through a combination of medical record review and patient self-report.
Psychological Burden
Psychological burden was assessed using the Hospital Anxiety and Depression Scale (HADS), which comprises two subscales: anxiety (HADS-A) and depression (HADS-D), each consisting of 7 items.12 Each item is rated on a 4-point Likert scale (0–3), yielding subscale scores ranging from 0 to 21, with higher scores indicating greater levels of anxiety or depression. The HADS is a widely validated instrument for assessing psychological distress in patients with chronic diseases, including COPD, and has demonstrated robust reliability and validity across diverse clinical populations. In the present study, HADS-A and HADS-D were treated as core dimensions of psychological burden and were used as primary indicators for psychological stratification in the latent profile analysis, allowing differentiation of distinct psychological symptom patterns. HADS-A and HADS-D scores were calculated separately and subsequently standardized prior to inclusion in the analytic models.13
Symptom Burden
Symptom burden was comprehensively assessed using multidimensional indicators, including pulmonary function grade, symptom severity, and degree of dyspnea. Pulmonary function grade was classified based on clinical spirometry results into grades I through IV. Symptom severity was measured using the CAT, which consists of 8 items scored from 0 (no impact) to 5 (very severe impact), with total scores ranging from 0 to 40; higher scores indicate a greater impact of COPD on daily life.14 Dyspnea severity was assessed using the mMRC scale, which classifies breathlessness from grade 0 to 4 according to the level of activity that provokes dyspnea; higher grades indicate more severe dyspnea.15
Quality of Life
Health-related quality of life was assessed using the Airways Questionnaire 20 (AQ20), a disease-specific instrument designed for patients with chronic respiratory diseases, particularly COPD. The AQ20 consists of 20 dichotomous items (yes/no), scored as 1 or 0, respectively, yielding a total score ranging from 0 to 20, with higher scores indicating poorer quality of life. The AQ20 has been validated in COPD populations and is widely used to evaluate disease-related functional impairment and health status.16
COPD Self-Management Ability
COPD self-management ability was evaluated using the CSMS. This scale comprises 51 items across five dimensions: symptom management, daily life management, emotional management, information management, and self-efficacy. Items are rated on a 5-point Likert scale, with total scores ranging from 51 to 255; higher scores indicate better self-management ability.17
Health Locus of Control
Health locus of control was assessed using the MHLC scale, which includes three dimensions: IHLC, CHLC, and PHLC. Each dimension contains 6 items, with scores ranging from 6 to 36. Higher scores indicate a stronger tendency toward the corresponding locus of control orientation.18
Medical Coping Styles
Medical coping styles were assessed using the MCMQ, which evaluates three coping dimensions: confrontation, avoidance, and resignation. Given the differing number of items across dimensions, mean scores for each dimension were calculated to enhance comparability, with higher scores indicating a greater tendency to adopt the corresponding coping style.19
Annual Number of Hospitalizations
The annual number of hospitalizations due to COPD-related causes during the preceding year was recorded as a count outcome, based on patient self-report and verified using medical records.
Data Collection and Quality Control
Prior to the formal survey, a pilot study involving 35 patients with COPD was conducted at the same study site. Based on participant feedback, the wording and logical structure of the sociodemographic questionnaire were revised and refined. During the formal data collection phase, trained investigators conducted face-to-face questionnaire surveys in the pulmonary rehabilitation outpatient clinic. Standardized instructions were used to explain the study purpose and questionnaire requirements to participants. All questionnaires were completed anonymously. For participants with reading or writing difficulties, investigators provided assistance as needed. Completed questionnaires were collected on site and reviewed individually for completeness. Any missing or logically inconsistent responses were verified and supplemented immediately; when necessary, information was cross-checked with medical records or confirmed with family members to ensure data accuracy and consistency.
Statistical Analysis
All statistical analyses were performed using R software (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables are presented as mean ± standard deviation or median (interquartile range), as appropriate, and categorical variables are presented as frequencies and percentages.
To identify psychological–symptom mismatch phenotypes in patients with COPD, pulmonary function grade, CAT score, and mMRC score were first standardized using Z-score transformation to construct a composite symptom burden indicator. Similarly, HADS-A and HADS-D scores were standardized to construct a composite psychological burden indicator. Latent profile analysis was then conducted based on these two continuous indicators. This approach was theory-driven, as the primary aim was to characterize the relative alignment or discordance between psychological and symptom burden, rather than to model each observed indicator independently. The use of composite indicators to represent higher-order latent constructs is consistent with established practices in person-centered analyses, particularly when multiple correlated measures reflect a common underlying domain and when the research focus is on the interplay between domains rather than within-domain heterogeneity. This strategy also reduces dimensional redundancy and improves model stability, especially in moderate sample sizes. Model selection was guided by a combination of statistical fit indices and clinical interpretability, including the AIC, BIC, aBIC, BLRT, and entropy. Lower AIC, BIC, and aBIC values indicate better model fit; a statistically significant BLRT (p < 0.05) suggests that a model with k classes fits better than a model with k − 1 classes; and entropy values greater than 0.80 indicate high classification accuracy. The final model was determined based on an integrated consideration of statistical indices, class size, and clinical plausibility.
Participants were subsequently assigned to phenotype groups based on the LPA results. One-way analysis of variance or the Kruskal–Wallis test was used to compare continuous variables across phenotypes, and the χ2-test or Fisher exact test was used for categorical variables. To evaluate the clinical significance of psychological–symptom mismatch phenotypes, multivariable linear regression analyses were performed with phenotype membership as the independent variable and quality of life, dimensions of self-management ability, dimensions of health locus of control, and dimensions of medical coping styles as dependent variables. Two models were constructed for each outcome: Model 1 adjusted for age, sex, and educational attainment; Model 2 further adjusted for BMI, place of residence, living arrangement, monthly per capita household income, smoking status, alcohol consumption status, disease duration, and comorbidities. Because the annual number of hospitalizations is a count variable with overdispersion, negative binomial regression models were used to estimate IRRs and their 95% CIs. All statistical tests were two-sided, and a p value < 0.05 was considered statistically significant.
Results
Baseline Characteristics of the Study Population
A total of 306 patients with COPD were included in this study, of whom 258 were men (84.3%). The mean age of the participants was 70.3 ± 5.9 years. Overall, 152 patients (49.7%) resided in urban areas, and 54 (17.6%) lived alone. Most participants reported a per capita monthly household income of 3000–5000 CNY (n = 160, 52.3%). The predominant educational level was primary school or below (n = 132, 43.1%). Current or former smokers accounted for 114 patients (37.3%), and 31 patients (10.1%) reported alcohol consumption. Detailed demographic and clinical characteristics of the study population are presented in Table 1.
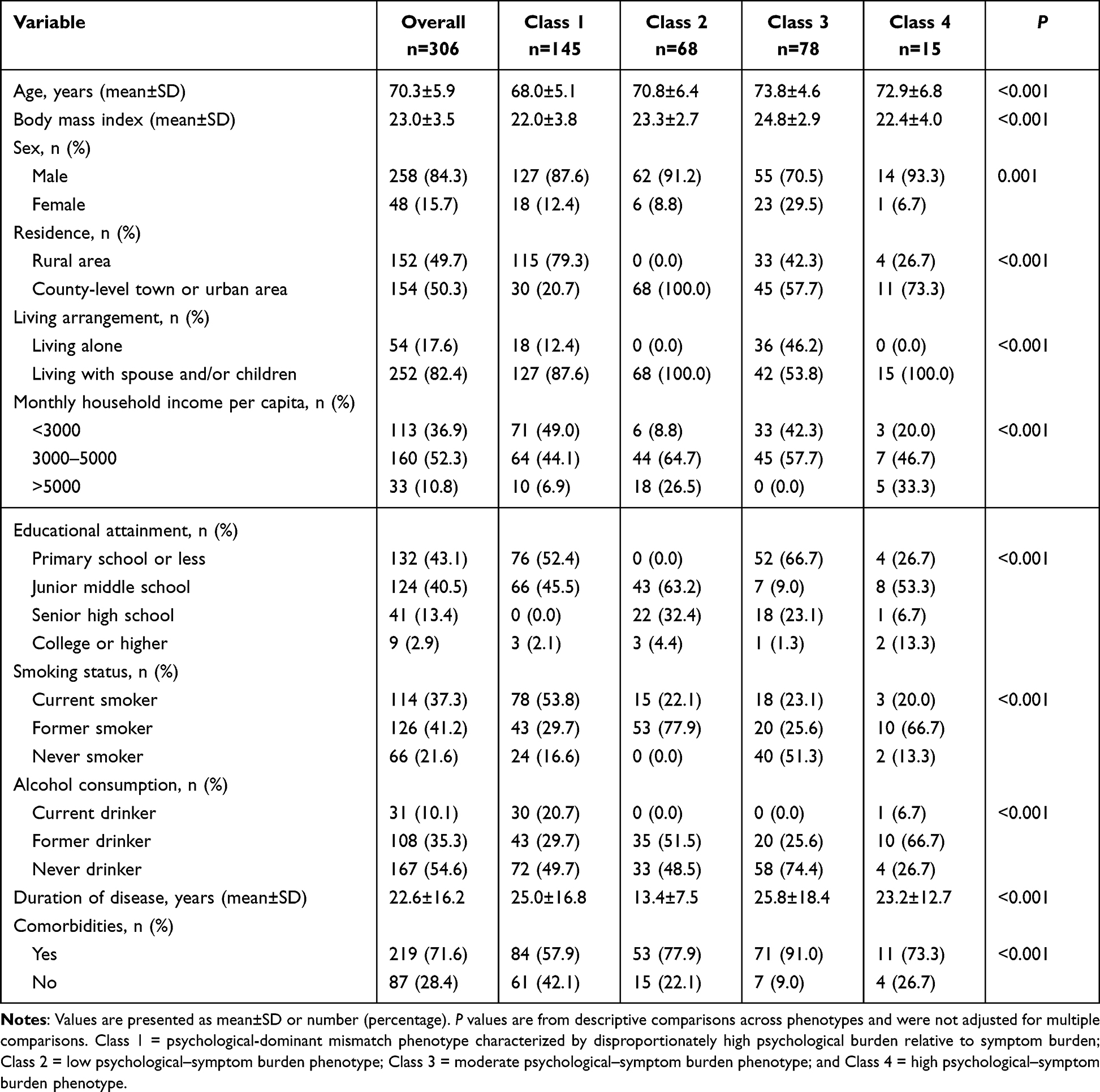 |
Table 1 Characteristics of Patients with COPD by Psychological–Symptom Mismatch Phenotype |
Identification of Psychological–Symptom Mismatch Phenotypes
Latent profile analysis was conducted to identify psychological–symptom mismatch phenotypes among patients with COPD, based on standardized psychological burden indicators (anxiety and depression) and symptom burden indicators (lung function grade, symptom severity, and dyspnea level). Model fit indices are summarized in Table 2.
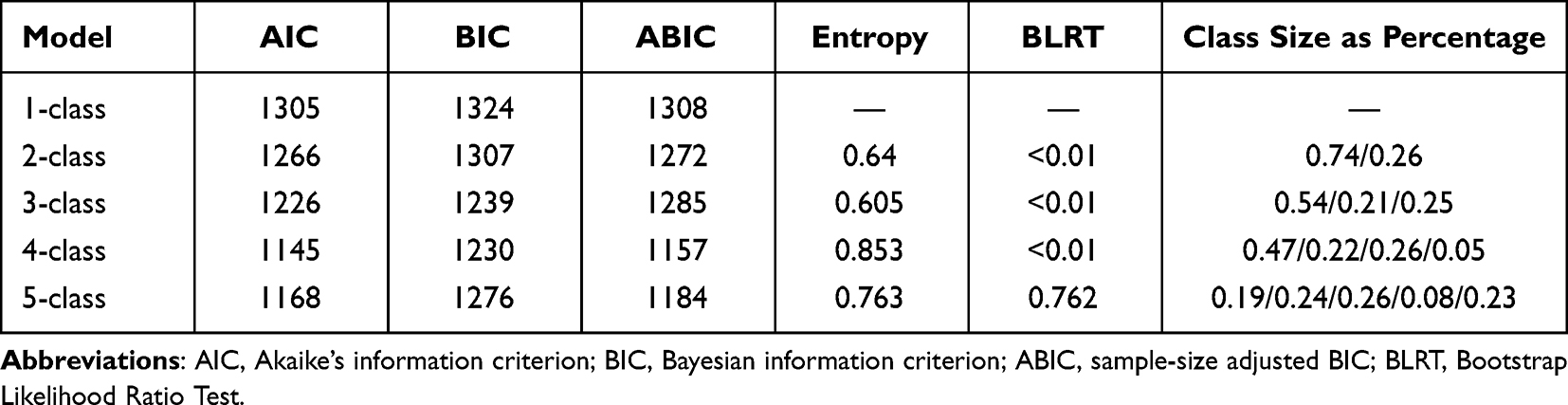 |
Table 2 Summary of Model Selection Indices of Latent Profile Analysis |
With increasing numbers of latent classes, the AIC, BIC, and sample-size–adjusted BIC (ABIC) showed a consistent downward trend. The 4-class model yielded relatively lowest AIC, BIC, and ABIC values, with an entropy of 0.853, indicating good classification accuracy. The bootstrap likelihood ratio test demonstrated that the 4-class model provided a significantly better fit than the 3-class model (P < 0.01), whereas the 5-class model did not further improve model fit (BLRT, P = 0.762) and showed reduced classification accuracy. Considering statistical fit, classification precision, clinical interpretability, and class size distribution, the 4-class solution was selected as the optimal model.
The four psychological–symptom phenotypes accounted for 47%, 22%, 26%, and 5% of the sample, respectively, all meeting recommended minimum class size criteria for latent profile analysis. Figure 1 illustrates the scatter distribution of standardized psychological and symptom burden indicators across phenotypes, and Figure 2 presents the corresponding mean profiles. Phenotype labels were assigned based on the overall level and cross-domain pattern of psychological and symptom burden, with particular attention to the degree of concordance or mismatch between domains. Specifically, (1) the psychological-dominant mismatch phenotype was characterized by disproportionately elevated psychological burden relative to symptom burden; (2) the low psychological–symptom burden phenotype exhibited consistently low levels across both domains; (3) the moderate psychological–symptom burden phenotype showed intermediate and relatively balanced levels; and (4) the high psychological–symptom burden phenotype demonstrated concurrently elevated levels in both domains without marked discordance. Notably, although the psychological-dominant mismatch phenotype exhibited higher psychological burden than other groups, it was distinguished by imbalance rather than overall burden, which informed the current labeling strategy.
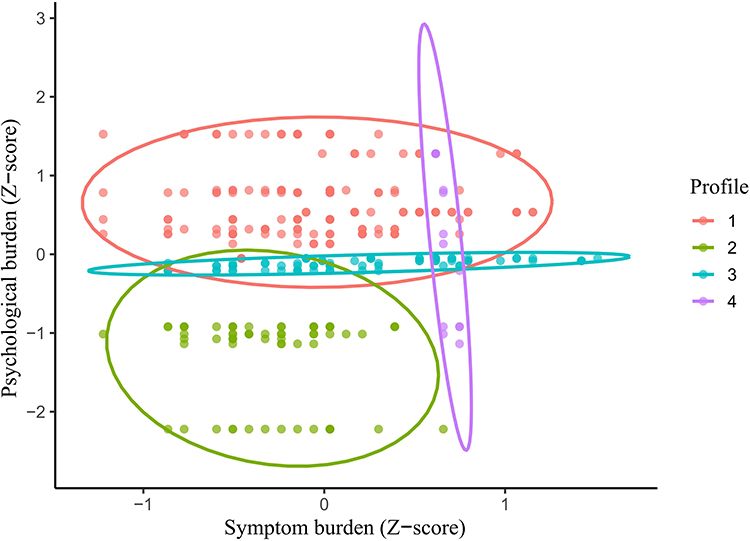 |
Figure 1 Distribution of Psychological–Symptom Burden Profiles Among COPD Patients Identified by Latent Profile Analysis. Notes: Profile 1: psychological-dominant mismatch phenotype characterized by disproportionately high psychological burden relative to symptom burden; Profile 2: low psychological–symptom burden phenotype; Profile 3: moderate psychological–symptom burden phenotype; Profile 4: high psychological–symptom burden phenotype. |
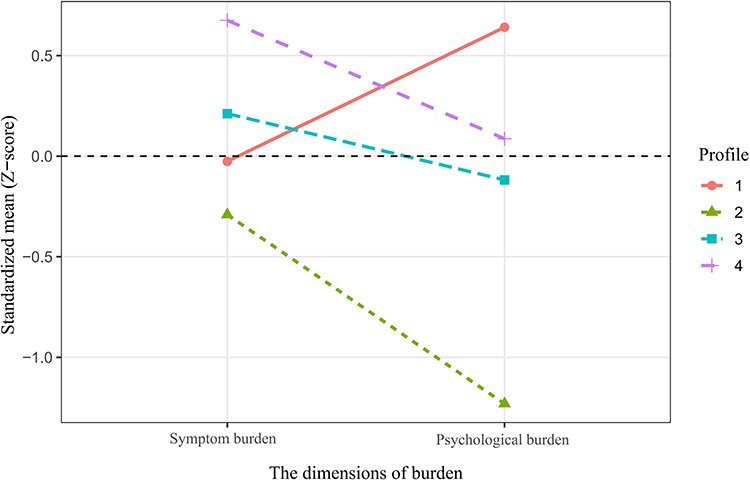 |
Figure 2 Standardized Symptom and Psychological Burden Scores Across Latent Profiles. Notes: Profile 1: psychological-dominant mismatch phenotype characterized by disproportionately high psychological burden relative to symptom burden; Profile 2: low psychological–symptom burden phenotype; Profile 3: moderate psychological–symptom burden phenotype; Profile 4: high psychological–symptom burden phenotype. |
Demographic, Clinical Characteristics, and Clinical Outcomes by Phenotype
Comparisons of demographic and clinical characteristics across psychological–symptom mismatch phenotypes are shown in Table 1. Significant differences were observed among phenotypes in age, body mass index, residence, living arrangement, household income level, educational attainment, smoking and alcohol use status, disease duration, and comorbidity distribution (all P < 0.001).
Differences in psychological and symptom burden indicators across phenotypes are presented in Supplementary Table S1. Differences in clinical outcomes, including quality of life, annual number of hospitalizations, self-management ability, health locus of control, and medical coping modes, are summarized in Supplementary Table S2.
Associations of Psychological–Symptom Mismatch Phenotype with Clinical Outcomes
Results of the multivariable linear regression analyses are presented in Table 3. Using the psychological-dominant mismatch phenotype as the reference group, patients in the low, moderate, and high psychological–symptom burden phenotypes had significantly lower AQ20 scores in the fully adjusted model (Model 2) (all P < 0.001), indicating relatively better quality of life.
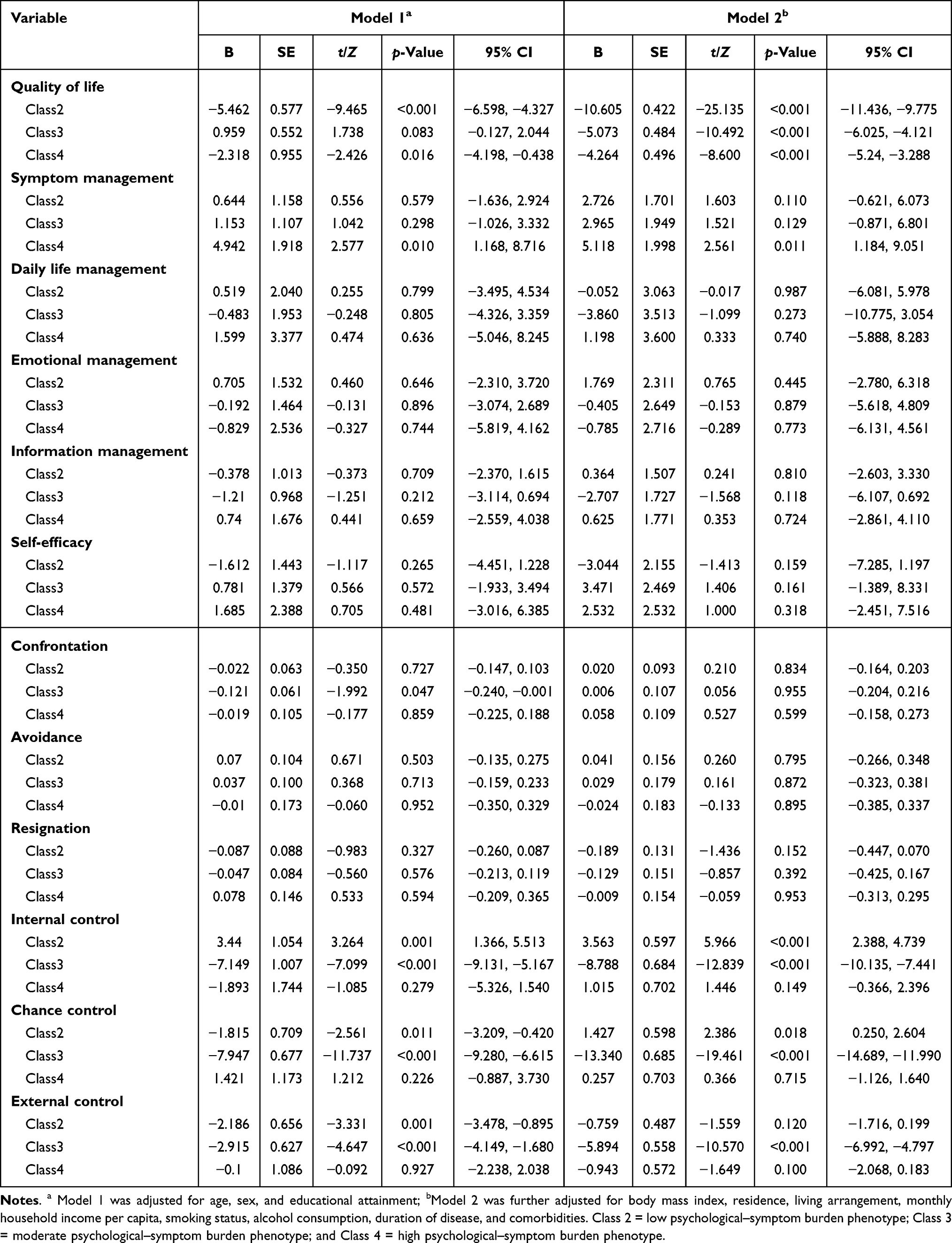 |
Table 3 Associations of Psychological–Symptom Mismatch Phenotypes with Hospitalizations, Quality of Life, Coping Styles, and Health Locus of Control in Patients with COPD |
Regarding self-management ability, only the high psychological–symptom burden phenotype was significantly associated with higher scores in the symptom management dimension (B = 5.118, P = 0.011). No statistically significant differences were observed across phenotypes for the remaining self-management dimensions.
In terms of health locus of control, the moderate psychological–symptom burden phenotype was significantly associated with stronger internal control beliefs and greater chance control orientation, whereas the high psychological–symptom burden phenotype was associated with significantly lower levels of internal control beliefs, chance control, and external control orientation (all P < 0.001).
With respect to medical coping modes, no stable statistically significant differences among phenotypes were observed for the confrontation, avoidance, or resignation dimensions in the fully adjusted models.
Associations with Annual Number of Hospitalizations
Because the annual number of hospitalizations was an overdispersed count variable, negative binomial regression models were applied (Table 4). In the fully adjusted model (Model 2), compared with the psychological-dominant mismatch phenotype, patients in the low psychological–symptom burden phenotype (IRR = 0.592, 95% CI, 0.355–0.989) and the moderate psychological–symptom burden phenotype (IRR = 0.233, 95% CI, 0.141–0.386) had significantly fewer hospitalizations over the past year. No significant association was observed between the high psychological–symptom burden phenotype and annual number of hospitalizations.
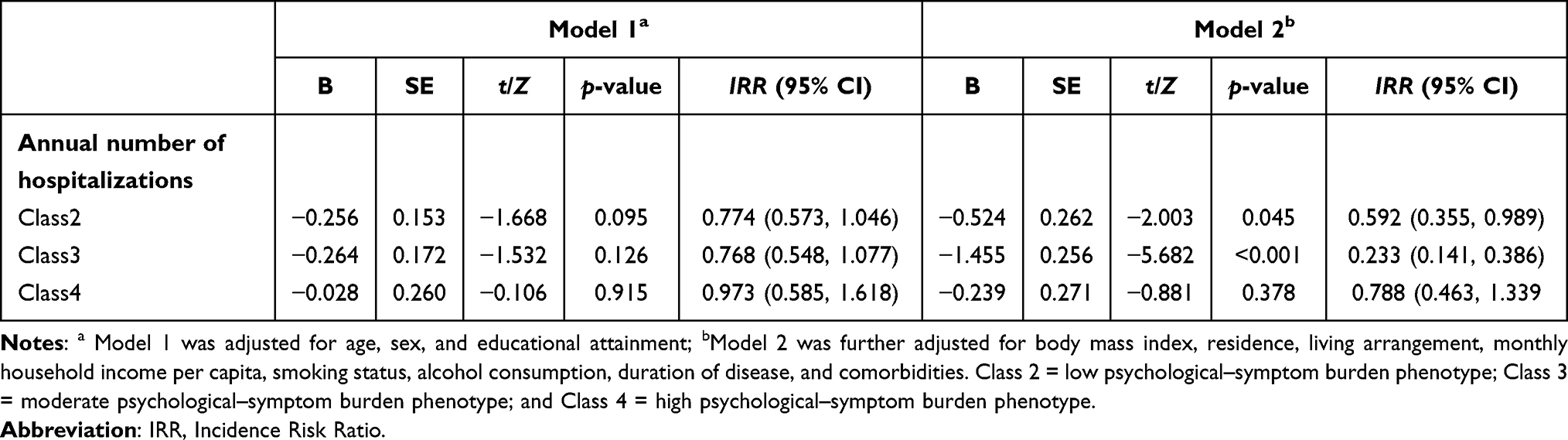 |
Table 4 Associations of Psychological–Symptom Mismatch Phenotypes with Annual Number of Hospitalizations in Patients with COPD Using Negative Binomial Regression |
Discussion
Key Findings
This study identified four distinct psychological–symptom mismatch phenotypes in patients with COPD using latent profile analysis. Approximately 22% of patients belonged to a psychological-dominant mismatch phenotype characterized by disproportionately high psychological distress relative to physiological symptom burden. This phenotype was associated with a higher likelihood of hospitalization in the previous year and worse health-related quality of life. Sociodemographic disadvantages, including lower income, lower educational attainment, and unhealthy behaviors, were more prevalent in this group. These findings suggest that psychological–symptom discordance represents a clinically meaningful dimension of COPD heterogeneity that is not captured by traditional symptom-based stratification.
Psychological–Symptom Mismatch as a Novel Stratification Dimension
Traditionally, COPD severity stratification has relied on physiological impairment, symptom scales, and exacerbation history. Although contemporary guidelines emphasize symptom burden and quality of life, psychological factors remain underrepresented in routine clinical stratification. Our findings extend current frameworks by demonstrating that psychological distress and symptom severity may follow dissociated patterns, forming distinct phenotypes with different clinical implications. Recent studies have similarly suggested that anxiety and depression in COPD are not fully explained by lung function impairment, supporting the concept of psychological–physiological dissociation.8 However, our study advances this literature by empirically identifying latent phenotypes integrating both domains and demonstrating their differential associations with hospitalization risk.
Clinical and Sociodemographic Characteristics of Phenotypes
Patients with the psychological-dominant mismatch phenotype were more likely to have socioeconomic disadvantage, lower educational attainment, and unhealthy lifestyle behaviors, including smoking and alcohol use. These findings are consistent with prior evidence showing that socioeconomic deprivation is strongly associated with increased psychological distress in COPD populations.20 Lower socioeconomic status may contribute to heightened psychological burden through reduced access to health care resources, increased disease uncertainty, and diminished self-efficacy. These factors may amplify anxiety and depressive symptoms independent of objective disease severity.21
Psychological Mechanisms Underlying Mismatch Phenotypes
Several potential mechanisms may explain the observed psychological–symptom mismatch. First, catastrophic illness perceptions and heightened symptom vigilance may lead patients to overinterpret mild respiratory symptoms as severe threats, amplifying anxiety and depressive responses.22 Prior research has demonstrated that illness perception is a strong determinant of psychological distress in COPD, independent of lung function.23,24 Second, intrinsic psychological vulnerability, such as neurotic personality traits or prior traumatic experiences, may predispose individuals to higher psychological burden. In addition, limited coping resources, including poor social support and financial strain, may further exacerbate emotional distress.25–27 Third, this phenotype may reflect underrecognized and undertreated psychological comorbidities that are relatively independent of pulmonary disease severity but substantially contribute to functional impairment and health care utilization. These findings are consistent with the stress–vulnerability model and highlight the multidimensional nature of psychological burden in COPD.28
Associations with Clinical Outcomes and Regression Findings
Importantly, regression analyses demonstrated that the psychological-dominant mismatch phenotype was independently associated with a higher risk of hospitalization compared with the moderate symptom-dominant phenotype. This association remained significant after adjustment for demographic and clinical covariates, suggesting that psychological–symptom discordance may confer incremental prognostic value beyond traditional indicators of disease severity. In addition, this phenotype was associated with the poorest health-related quality of life. These findings are consistent with previous studies reporting that anxiety and depression exert independent adverse effects on quality of life in COPD, beyond the contributions of lung function impairment and symptom burden.29
Health Locus of Control, Coping Patterns, and Behavioral Implications
Differences in health locus of control and coping strategies were observed across phenotypes, although patterns were modest. Patients with higher overall burden demonstrated more external or helplessness-oriented control beliefs, which may reflect maladaptive coping and reduced perceived control over disease progression.30 However, self-management behaviors did not differ substantially across phenotypes. This finding suggests that current COPD self-management programs, which primarily emphasize symptom monitoring and medication adherence, may not adequately address psychological distress. Recent systematic reviews similarly indicate that most COPD interventions insufficiently target anxiety and depression, limiting their impact on psychological outcomes.31,32
Clinical Implications
From a clinical perspective, these phenotypes may inform several aspects of patient management. First, they support the routine integration of standardized psychological screening into COPD assessment, including for patients with mild or moderate symptoms who might otherwise be overlooked. Second, they offer a basis for risk stratification that complements traditional physiological measures, enabling clinicians to identify high-risk patients earlier. Third, they suggest that targeted, phenotype-informed interventions may be warranted. For example, patients with psychological-dominant mismatch may particularly benefit from early implementation of psychological interventions (eg, cognitive behavioral therapy or mindfulness-based approaches), alongside self-management support and education, even in the absence of severe respiratory symptoms At the health system level, these findings also underscore the need for integrated, multidisciplinary care models that incorporate psychological assessment and intervention into routine COPD management. Future studies should evaluate whether phenotype-guided care pathways—including embedding psychological interventions within pulmonary rehabilitation or leveraging digital tools for continuous psychological monitoring—can improve patient-centered outcomes and reduce avoidable health care utilization.
Limitations
Several limitations should be considered when interpreting these findings. First, the cross-sectional design precludes causal inference regarding the associations between psychological–symptom mismatch phenotypes and clinical outcomes; longitudinal studies are needed to establish their predictive value. Second, participants were recruited from a single pulmonary rehabilitation outpatient clinic and were predominantly male, which may limit generalizability. Patients referred to pulmonary rehabilitation may differ from the broader COPD population in disease severity and health care access, potentially introducing selection bias. Third, although validated instruments were used, assessment of psychological and symptom burden relied partly on self-report and may be subject to recall bias. Fourth, the latent profile analysis was conducted using two composite indicators representing psychological and symptom burden. Although this approach was theory-driven and enabled direct characterization of cross-domain alignment or mismatch, it may have limited the ability to identify more granular subgroups driven by specific components. Future studies with larger samples may benefit from applying latent profile analysis using the original indicators or more flexible approaches, such as factor mixture modeling, to further evaluate the robustness of these phenotypes. Finally, the relatively small size of certain subgroups, particularly the high psychological–symptom burden phenotype, may reduce estimate stability, and these findings should be interpreted with caution.
Conclusion
In conclusion, psychological–symptom mismatch represents an important but underrecognized dimension of chronic obstructive pulmonary disease heterogeneity. Patients with disproportionate psychological distress may experience poorer clinical outcomes despite relatively lower symptom burden, including reduced quality of life and increased hospitalization risk. Incorporating psychological assessment into routine clinical care may support improved risk stratification and more individualized, patient-centered management strategies.
Acknowledgments
The authors thank all participants and staff involved in this study.
Author Contributions
Y. C.: Conceptualization, methodology, investigation, data curation, formal analysis, writing – original draft, and revision of the manuscript. X. R.: Conceptualization, methodology, writing – review & editing. K. W.: Interpretation of study findings, critical revision and restructuring of the Discussion section, and refinement of academic language and intellectual content. H. C.: Supervision, writing – review & editing. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Venkatesan P. GOLD COPD report: 2023 update. Lancet Respir Med. 2023;11(1):18. doi:10.1016/S2213-2600(22)00494-5
2. Bartziokas K, Papaporfyriou A, Hillas G, Papaioannou A, Loukides S. Global initiative for chronic obstructive lung disease (GOLD) recommendations: strengths and concerns for future needs. Postgrad Med. 2023;135(4):327–13. doi:10.1080/00325481.2022.2135893
3. Fazekas-Pongor V, Fekete M, Balazs P, et al. Health-related quality of life of COPD patients aged over 40 years. Physiol Int. 2021;108(2):261–273. doi:10.1556/2060.2021.00017
4. Coakley M, Drohan M, Bruce E, Hughes S, Jackson N, Holmes S. COPD Self-Management: a Patient-Physician Perspective. Pulm Ther. 2024;10(2):145–154. doi:10.1007/s41030-024-00258-y
5. Han M, Wu H, Xu H, Zhao J, Chang Z, Zhao Q. The relationship between social isolation and cognitive function in older patients with chronic obstructive pulmonary disease: a latent profile analysis. BMC Geriatr. 2025;25(1):561. doi:10.1186/s12877-025-06211-1
6. Chen M, Gong Z, Wang J, et al. High Anxiety in COPD: a Barrier to Effective Inhaler Medication Adherence and Disease Management. J Clin Nurs. 2026;35(1):208–218. doi:10.1111/jocn.17819
7. Hong YJ, Kim Y, Moon JY, et al. Associations between depression and anxiety index and frequency of acute exacerbation in chronic obstructive pulmonary disease. Ther Adv Respir Dis. 2023;17:17534666231216591. doi:10.1177/17534666231216591
8. Karlsen JH, Jorgensen KH, Weinreich UM. Association between impairment of lung function and risk of anxiety and depression in patients with chronic obstructive pulmonary disease-a systematic review. Syst Rev. 2024;13(1):300. doi:10.1186/s13643-024-02720-z
9. Gu J, Yang C, Zhang K, Zhang Q. Mediating role of psychological capital in the relationship between social support and treatment burden among older patients with chronic obstructive pulmonary disease. Geriatr Nur. 2021;42(5):1172–1177. doi:10.1016/j.gerinurse.2021.07.006
10. Cheng Y, Luo Y, Ju X, Yang J, Liu X. Exploring the eHealth literacy and related influencing factors in patients after lung cancer surgery: a latent profile analysis. Asia-Pac J Oncol Nurs. 2025;12:100818. doi:10.1016/j.apjon.2025.100818
11. Spurk D, Hirschi A, Wang M, Valero D, Kauffeld S. Latent profile analysis: a review and “how to” guide of its application within vocational behavior research. J Vocat Behav. 2020;120:103445. doi:10.1016/j.jvb.2020.103445
12. Nylund KL, Asparouhov T, Muthén BO. Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo simulation study. Struct Equation Model. 2007;14(4):535–569. doi:10.1080/10705510701575396
13. Zigmond A, Snaith R. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
14. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Leidy NK. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
15. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
16. Hajiro T, Nishimura K, Jones PW, et al. A novel, short, and simple questionnaire to measure health-related quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;159(6):1874–1878. doi:10.1164/ajrccm.159.6.9807097
17. Zhang C, He G, Li J, et al. Development and Evaluation of Self-Management Scale for Chinese Patients with Chronic Obstructive Pulmonary Disease. Chin General Pract Med. 2011;14(28):3219–3223.
18. Wallston K, Wallston B, Devellis R. Development of Multidimensional Health Locus of Control (mhlc) Scales. Health Educ Monogr. 1978;6(2):160–170. doi:10.1177/109019817800600107
19. Feifel H, Strack S, Nagy V. Coping Strategies and Associated Features of Medically Ill Patients. Psychosom Med. 1987;49(6):616–625. doi:10.1097/00006842-198711000-00007
20. Lee H, Jung J, Yoon HY. Impact of socioeconomic status on chronic obstructive pulmonary disease prognosis: a national cohort study. Front Med. 2025;12. doi:10.3389/fmed.2025.1584945.
21. Rahi MS, Thilagar B, Balaji S, et al. The Impact of Anxiety and Depression in Chronic Obstructive Pulmonary Disease. Adv Respir Med. 2023;91(2):123–134. doi:10.3390/arm91020011
22. Huang LM, Tan CY, Chen X, Jiang YJ, Zhou YR, Zhao H. A Qualitative Study on Illness Perception and Coping Behaviors Among Patients with Chronic Obstructive Pulmonary Disease: implications for Intervention. Int J Chron Obstruct Pulmon Dis. 2024;19:2467–2479. doi:10.2147/COPD.S473790
23. Poletti V, Pagnini F, Banfi P, Volpato E. Illness Perceptions, Cognitions, and Beliefs on COPD Patients’ Adherence to Treatment-A Systematic Review. Patient Prefer Adherence. 2023;17:1845–1866. doi:10.2147/PPA.S412136
24. Christiansen CF, Lokke A, Bregnballe V, Prior TS, Farver-Vestergaard I. COPD-Related Anxiety: a Systematic Review of Patient Perspectives. Int J Chron Obstruct Pulmon Dis. 2023;18:1031–1046. doi:10.2147/COPD.S404701
25. Topp M, Vestbo J, Mortensen EL. Personality Traits and Mental Symptoms are Associated with Impact of Chronic Obstructive Pulmonary Disease on Patients’ Daily Life. Copd-J Chronic Obstr Pulm Dis. 2016;13(6):773–778. doi:10.3109/15412555.2016.1168793
26. Lee H, Yoon JY, Kim I, Jeong YH. The effects of personal resources and coping strategies on depression and anxiety in patients with chronic obstructive pulmonary disease. Heart Lung. 2013;42(6):473–479. doi:10.1016/j.hrtlng.2013.07.009
27. Tian X, Yi L, Liu X, et al. Relationship Between Social Support, Symptom Burden, Dyspnea, Perceived Stress, Perceived Stigma, Coping Styles, and Psychological Distress in Patients with Stable COPD: a Structural Equation Model. Int J Chron Obstruct Pulmon Dis. 2025;20:2183–2198. doi:10.2147/COPD.S521786
28. Wang JG, Bose S, Holbrook JT, et al. Clinical Characteristics of Patients With COPD and Comorbid Depression and Anxiety: data From a National Multicenter Cohort Study. Chronic Obstr Pulm Dis-J Copd Found. 2025;12(1):33–42. doi:10.15326/jcopdf.2024.0534
29. Hart JL, Summer AE, Ogunduyile L, et al. Accuracy of Expected Symptoms and Subsequent Quality of Life Measures Among Adults With COPD. JAMA Network Open. 2023;6(11):e2344030. doi:10.1001/jamanetworkopen.2023.44030
30. Mozafari S, Yang A, Talaei-Khoei J. Health Locus of Control and Medical Behavioral Interventions: systematic Review and Recommendations. Interact J Med Res. 2024;13:e52287. doi:10.2196/52287
31. Yadav UN, Lloyd J, Hosseinzadeh H, Baral KP, Harris MF. Do Chronic Obstructive Pulmonary Diseases (COPD) Self-Management Interventions Consider Health Literacy and Patient Activation? A Systematic Review. J Clin Med. 2020;9(3):646. doi:10.3390/jcm9030646
32. Sohanpal R, Pinnock H, Steed L, et al. A tailored psychological intervention for anxiety and depression management in people with chronic obstructive pulmonary disease: TANDEM RCT and process evaluation. Health Technol Assess. 2024;28(1):1–160. doi:10.3310/PAWA7221
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Models of Psychological Distress, Quality of Life, and Adherence to Medication in Breast Cancer Patients: A Scoping Review
Pezzolato M, Spada GE, Fragale E, Cutica I, Masiero M, Marzorati C, Pravettoni G
Patient Preference and Adherence 2023, 17:3461-3473
Published Date: 19 December 2023
Coping Profiles and Differences in Psychological Distress and Quality of Life in Clients Undergoing Assisted Reproductive Techniques: A Latent Profile Analysis
Bai J, Zheng J, Guo N, Dong Y, Wang K, Cheng C, Jiang H, Qian L
Journal of Multidisciplinary Healthcare 2024, 17:533-540
Published Date: 5 February 2024
Problematic Use of Internet Associates with Poor Quality of Life via Psychological Distress in Individuals with ADHD
Chen CY, Lee KY, Fung XCC, Chen JK, Lai YC, Potenza MN, Chang KC, Fang CY, Pakpour AH, Lin CY
Psychology Research and Behavior Management 2024, 17:443-455
Published Date: 9 February 2024
The Sequelae and Moderators of Influence of Dandruff on Mental Health Among Mainland Chinese Adults
Chan CS, Smith T, He Z, Garter C
Clinical, Cosmetic and Investigational Dermatology 2024, 17:1333-1346
Published Date: 11 June 2024
Factor Impacting Quality of Life Among Sepsis Survivors During and After Hospitalization: A Systematic Review of Current Empirical Evidence
Pongsuwun K, Puwarawuttipanit W, Nguantad S, Samart B, Saikaew K, Ruksakulpiwat S
Journal of Multidisciplinary Healthcare 2024, 17:3791-3802
Published Date: 6 August 2024