Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Breathlessness Matters – Australian Cohort Study Evaluating the Impact of a Multidisciplinary, Home-Based Breathlessness Intervention Service Targeting Patients with Chronic Obstructive Pulmonary Disease (COPD)
Authors Cochrane B ![]() , Akhunji MZ, Xuan W, Lee JSY, Smith TA
, Akhunji MZ, Xuan W, Lee JSY, Smith TA ![]() , Smith SM, Foo SW, Garcia L
, Smith SM, Foo SW, Garcia L ![]() , Kemp TA
, Kemp TA ![]()
Received 30 November 2025
Accepted for publication 23 May 2026
Published 22 June 2026 Volume 2026:21 570099
DOI https://doi.org/10.2147/COPD.S570099
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Belinda Cochrane,1,2 Mohmedsaqib Zakirhusen Akhunji,1,3 Wei Xuan,3,4 Jonathan Shung-Yi Lee,1 Tracy A Smith,5,6 Sheree M Smith,7,8 Soo Wei Foo,1,2 Luisa Garcia,9 Teresa Anne Kemp1
1Department of Respiratory and Sleep Medicine, Campbelltown Hospital, Campbelltown, NSW, Australia; 2School of Medicine, Western Sydney University, Sydney, NSW, Australia; 3South Western Sydney Clinical School, University of New South Wales, Sydney, NSW, Australia; 4Ingham Institute for Applied Medical Research, Liverpool, NSW, Australia; 5Department of Respiratory and Sleep Medicine, Westmead Hospital, Westmead, NSW, Australia; 6Faculty of Medicine and Health, The University of Sydney at Westmead Hospital, Westmead, NSW, Australia; 7Faculty of Health and Medical Science, University of Adelaide, Adelaide, SA, Australia; 8Faculty of Medicine, University of Queensland, Brisbane, QLD, Australia; 9School of Nursing and Midwifery, Western Sydney University, Sydney, NSW, Australia
Correspondence: Belinda Cochrane, Department of Respiratory and Sleep Medicine, Campbelltown Hospital, PO Box 149, Campbelltown, NSW, 2560, Australia, Email [email protected]
Background and Objectives: Chronic breathlessness causes reduced quality of life (QoL) and high healthcare costs. Accumulating evidence shows that multidisciplinary breathlessness services can ameliorate breathlessness which persists despite guideline-directed treatments. Current literature largely reflects trials of interventions in European settings applied to cancer-predominant populations, raising doubt about broad applicability. The research objective was to evaluate whether Macarthur Breathless Clinic (MBC), a bespoke health service intervention, could reduce the impact of chronic breathlessness for a cohort of Australians with COPD.
Methods: The MBC intervention was tested in a prospective, single-arm cohort study, targeting recruitment of 92 patients. Eligible patients had chronic breathlessness impacting QoL and at least moderately severe COPD, defined by spirometry. Following detailed case review to ensure optimal medical therapy, an individualized program was developed and implemented by MBC’s multidisciplinary team during a nine-week program. Questionnaires assessing breathlessness burden, mental health and QoL were administered at baseline, repeated on program completion and again at 12 months.
Results: Eighty-nine eligible subjects were mean age 71 years, 65% female and 10% Aboriginal Australian with 18% reporting breathlessness at rest. Mean FEV1 was 37% predicted. Compared with baseline, the primary outcome, Chronic Respiratory Questionnaire – Mastery Subscale improved after program completion (0.5 at nine and 0.8 at 52 weeks, p< 0.0001). Measures of confidence, COPD symptom burden and breathlessness also yielded durable positive results at 12 months.
Conclusion: Clinically relevant gains seen after MBC were retained or even increased at 12 months and more reflected enhanced coping skills and confidence than reduced breathlessness intensity.
Plain Language Summary: Breathlessness is a distressing, disabling symptom, contributing to high healthcare costs. Hence, addressing breathlessness represents an unmet need for patients and a health system priority. Breathlessness intervention services, largely comprising non-pharmacological strategies have proven beneficial for patients in the short term; largely for those patients with life-limiting disease such as cancer. Chronic obstructive pulmonary disease (COPD) and emphysema are common conditions, increasing in prevalence worldwide. Even with best available treatments, such patients have persistent and pervasive symptom burden, particularly from breathlessness. This research explores the utility of a breathlessness intervention service for durable impact when applied to patients with COPD. We report sustained improvements in breathlessness mastery and related symptom burden at 12 months following a multidisciplinary, home-based breathlessness intervention program in a cohort of Australians with COPD.
Keywords: dyspnea, quality of life, symptom burden, non-pharmacological strategies
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive, multisystem disease primarily affecting the lungs, characterized by persistent, incompletely reversible airflow obstruction.1 COPD is common, affecting an estimated 10% of adults globally2 and 14% of Australians aged above 40 years.3 COPD, ranked third worldwide after cardiovascular diseases and Coronavirus of 2019 (COVID-19) as cause for mortality,4 is not only deadly but imparts substantial morbidity to individuals and thereby demands on health systems. COPD in Australia is ranked seventh for personal disease burden,5 was a leading cause of preventable hospitalizations in 2017−86 (prior to the COVID-19 pandemic) and cost the Australian healthcare system an estimated $994.8 million in 2019–20.7 Despite best treatment, residual symptoms are burdensome; the foremost being breathlessness, which contributes to physical and psychological distress, reducing functional status and community participation.8 Thus, addressing refractory breathlessness in COPD represents an unmet need for patients and a priority for healthcare systems.
Breathlessness, a common, distressing and disabling symptom, has inspired the development of breathlessness intervention services (BIS)9 offering support and training in breathlessness self-management using predominantly non-pharmacological strategies. BIS have their origins within palliative care settings, designed to reduce suffering due to breathlessness in the context of advanced malignant disease. In this patient population, the primary focus has been to provide relief over the short term, given limited life expectancy, with the goal of maximizing comfort and dignity for the remainder of life. Cumulative randomized controlled trial evidence suggests clinically relevant benefit, although BIS have varied widely in terms of target population, duration, setting and clinical disciplines involved.10 These services are considered resource-intensive, making it essential to identify patients who are most likely to benefit – especially those who may achieve lasting improvement to ensure cost-effective care. Importantly, some services have reported reduction in urgent healthcare utilization11,12 and reasonable cost-effectiveness.12–14 However, the evidence for benefit in mixed populations, particularly in cohorts with non-malignant disease has been less clear.9,14–16
COPD may lend itself particularly well to non-pharmacologic interventions. Despite multiple potential contributing factors, the main pathophysiology underlying breathlessness in COPD is dynamic hyperinflation, which worsens during exertion.17,18 Moreover, COPD patients have high prevalence of targetable comorbid conditions adversely impacting breathlessness, such as anxiety, depression, sarcopenia, suboptimal nutrition and frailty, which may respond over the longer term. These characteristics make it likely that patients with COPD and disabling breathlessness will achieve short-term gains addressing dynamic hyperinflation by practising breathing techniques, applying self-pacing, “best breathing posture”, energy conservation advice, correcting inhaler device technique and optimizing bronchodilator medications. Over the longer term, they may also benefit from cognitive approaches, nutritional supplements, exercise and respiratory muscle training.
Already, pulmonary rehabilitation (PR) is recognized as an effective modality of treatment in COPD, associated with benefits to quality of life, endurance and healthcare utilization (HCU).19 However, the majority of patients with COPD do not attend (or complete) PR for a variety of reasons, including access issues.20 Whilst BIS and PR emerged from separate specialist disciplines, these approaches are complementary and are best viewed as a spectrum, with components which can be escalated or attenuated according to individual patient needs and characteristics. PR’s emphasis is moderate intensity exercise training, with improvements in breathlessness attributed to enhanced conditioning and self-management capability. In BIS, exercise is encouraged as part of a multidisciplinary service prioritising non-pharmacological coping strategies,9 unlike PR where formal exercise is the core modality of therapy. Hence, BIS physical interventions may be more suited to frailer patients or those less capable of formal exercise.
Macarthur Breathless Clinic (MBC), the clinical intervention evaluated in this research, was developed as part of clinical service expansion at Macarthur Health in response to the refractory symptom burden and disability associated with COPD. Of particular concern were the frequent emergency department visits and hospital admissions, most of which were driven by breathlessness. Initially MBC was envisaged as a second site for Westmead Hospital’s BIS21 to demonstrate transferability of the service. Hence, its design and format were largely informed by collaboration with clinical colleagues from this group and then adapted to accommodate Macarthur’s distinctly different resources, infrastructure and catchment.
This research tests the hypothesis that patients with COPD and chronic breathlessness will realise measurable improvements compared to baseline in terms of coping ability, symptom burden, quality of life (QoL), and psychological distress after completion of the MBC program. A secondary hypothesis is that these improvements will be sustained over 12 months.
Methods
Study Design
This was a prospective single-arm cohort study, comparing outcomes assessed at baseline with those assessed subsequently (participants acting as their own controls).
Setting
Recruitment was sourced from Macarthur’s inpatient wards, outpatient clinics, pulmonary rehabilitation program and local specialist rooms via clinician referrals. Consecutive referrals were screened for eligibility by clinical team-members prior to undertaking informed consent and study enrolment. Study enrolments occurred between March 2022 and February 2023, with patients participating in study activities and follow-up for a duration of 52 weeks.
The MBC intervention was delivered via a combination of two encounters held in an outpatient clinic setting and seven encounters held within patients’ homes, undertaken by nursing, physiotherapy and occupational therapy clinicians. Patient data were collected during initial, 9-week and 12-month home visit assessments.
Eligibility and Exclusion Criteria
Potential participants were screened based on the inclusion and exclusion criteria outlined in Box 1. Eligible participants had at least moderate COPD, confirmed by current or previously documented spirometry, and experienced chronic breathlessness, defined as modified Medical Research Council (mMRC) score of ≥2. An mMRC score of 2 equates to “walks slower than people of the same age because of dyspnea or has to stop for breath when walking at own pace”. Exclusion criteria for study participation mainly reflected factors that would adversely influence capability to engage and participate in MBC’s education strategies.
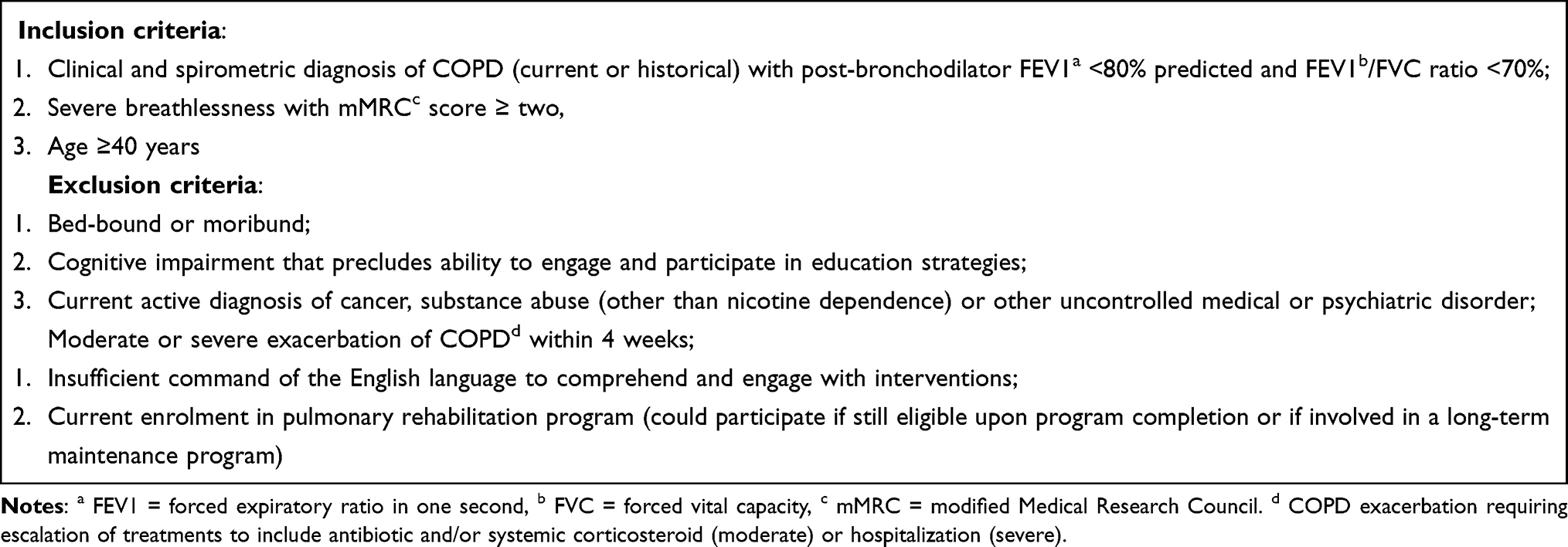 |
Box 1 Study Inclusion and Exclusion Criteria |
Intervention
The MBC was a multidisciplinary, predominantly home-based, health service intervention. Figure 1 represents the MBC structure and processes, showing the timeline and location for clinical interactions and component activities relating to each clinical discipline. MBC comprised nine “visits” at approximately weekly intervals. The multidisciplinary team (MDT) included a respiratory physician, occupational therapist, specialist respiratory nurse and physiotherapist. Between them, the non-medical clinicians undertook six home-based clinical visits, in addition to an initial home-based assessment. Two MDT appointments occurred in weeks two and nine, usually within the outpatient clinic setting and involved representatives from at least two clinical disciplines, one being the respiratory physician.
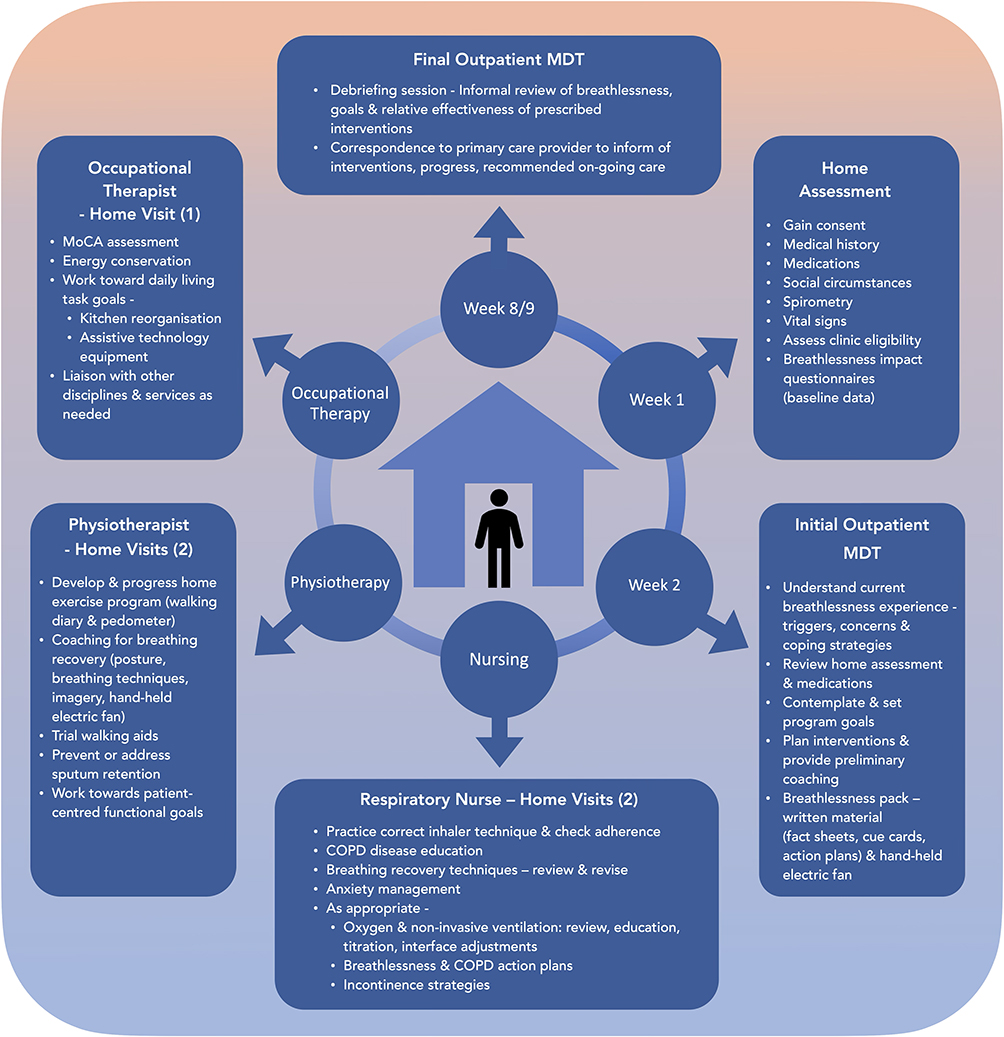 |
Figure 1 Macarthur Breathless Clinic (MBC) - Structure and Composition. The MBC comprised eight “visits”, intended to be at approximately weekly intervals. The multidisciplinary team (MDT) included a respiratory physician, occupational therapist, specialist respiratory nurse and physiotherapist. Two MDT appointments occurred in weeks two and nine, usually located in the outpatient clinic setting. |
Patients provided demographic data and underwent an extensive COPD-focussed health assessment at the outset. Nutritional status and swallowing were also screened, using the Mini Nutritional Assessment – Short Form (MNA-SF)22,23 and Eating Assessment Tool (EAT-10),24 respectively. Formal cognitive function screening via Montreal Cognitive Assessment (MoCA)25 was undertaken during the subsequent occupational therapy sessions. For each patient, detailed case review was undertaken using the clinic’s assessment template (Supplement Figure 1: Breathless Clinic Initial Assessment Template). An individualized program was developed, which included optimization of guideline-based medical treatments, prior to implementation by the MDT. Referrals to additional clinical disciplines, if needed, were negotiated via patients’ general practitioners. Applying Cambridge Breathlessness Intervention Service’s “Breathing, Thinking, Functioning” model,26 the MDT targeted treatable physical, emotional, intellectual and functional traits utilizing strategies such as respiratory muscle training and exercise, sputum clearance and breathing techniques, use of a hand-held electric fan, affirmatory self-talk, visualization and motivation, disease education, troubleshooting barriers to treatment adherence, energy conservation and nutritional supplement advice, all via clinical interactions with patients in their own homes.
The intervention was designed to be flexible and adaptable according to changing circumstances and patient needs, which meant that visit format could be telehealth at patient request when clinically appropriate. Clinicians involved in home visits could extensively cross-cover MBC component strategies and so the clinician visit schedule could be weighted according to individual patient priorities or adjusted in the setting of staff leave or furlough requirements, patients or their household members being unwell or to comply with infection control measures in the wake of the COVID-19 pandemic.
To ensure program fidelity, participants were offered a consistent menu of interventions with the most important elements being disease education aspects, the information package about breathlessness, physical therapies and the exercise program, breathing techniques, advice on use of the hand-held electric fan, the COPD action plan and energy conservation. To facilitate consistent messaging, the clinician team were kept as constant as possible for the duration of the study, with only one clinician from each discipline involved in the clinic for the majority of the study. The use of a purpose-designed clinic documentation template, specifying domains of assessment for the initial outpatient visit (Supplement Figure 1: Breathless Clinic Initial Assessment Template) also helped to ensure a consistent approach for all participants. Lastly, fortnightly multidisciplinary team meetings were held to update the clinicians, to discuss patients’ progress within the program and to formulate therapy plans for future home visits.
Breathlessness Impact Outcomes
Breathlessness impact was objectively assessed at baseline using interviewer-administered questionnaires related to breathlessness severity and intensity, overall respiratory symptom burden, QoL and psychological distress (Table 1). Mastery, a subscale of the Chronic Respiratory Questionnaire27 (CRQ-M) was chosen to be the study’s primary outcome as this assessment tool avoids the issue of breathlessness interactions with exertion and is therefore more suitable than breathlessness intensity measures, instead providing insights into control and coping, which are more pertinent to the chronic disease setting. In addition, CRQ-M has been used in several other studies of BIS, so enabling comparison across trials. The interviewer, usually MBC’s respiratory nurse, administered the questionnaires using pen-and-paper format during a home visit. Questionnaire responses were provided without prompting (uninformed), except when patients were unable to respond. Questionnaires were readministered on completion of the nine-week program and at 12 months.
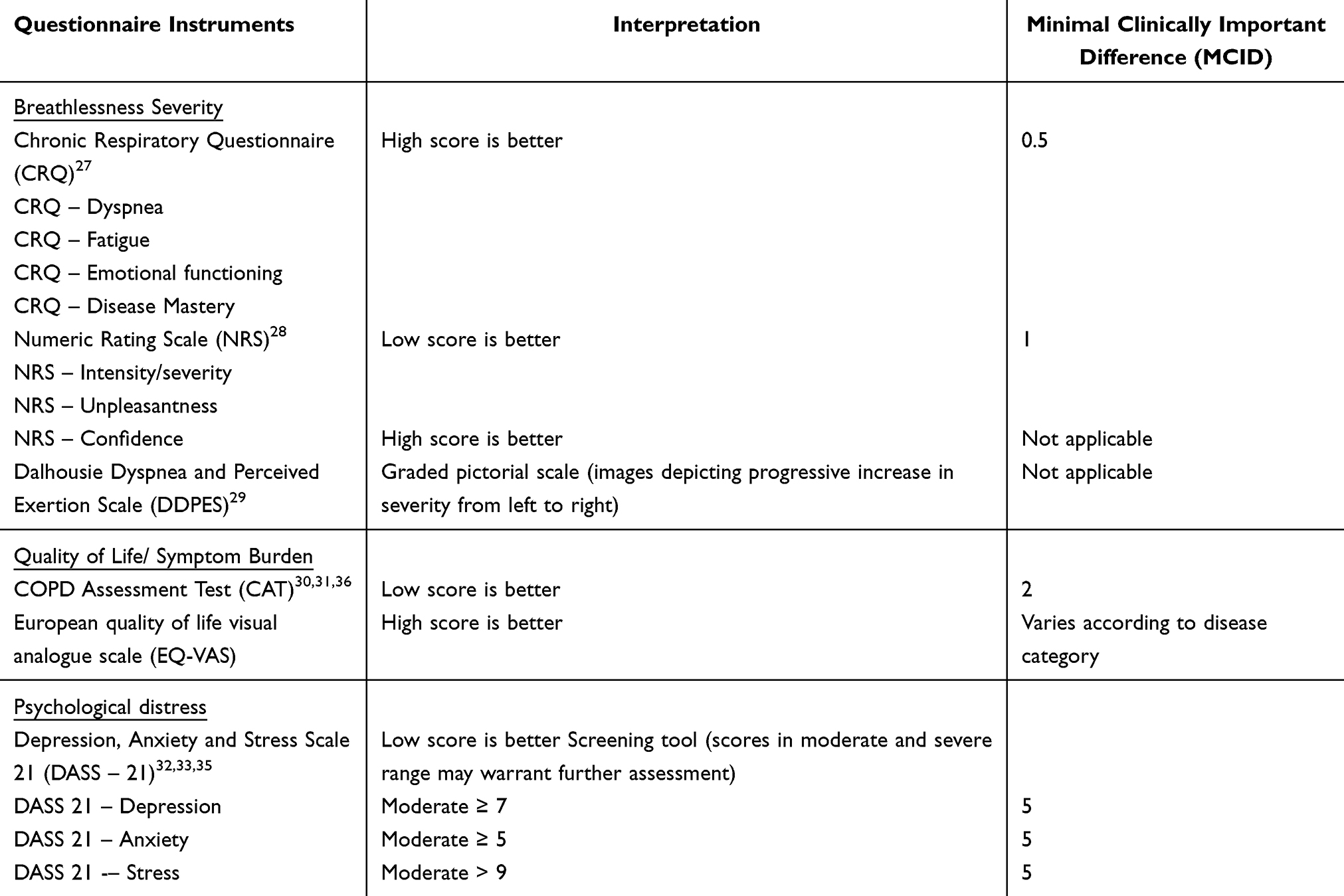 |
Table 1: Breathlessness Impact Questionnaire Tools - Outcome Variables |
Statistical Analysis
A recruitment target of 92 participants was set, informed by pilot data from Westmead Hospital’s BIS.34 The target incorporated an estimated 30% discontinuation due to the clinical frailty of these patients. Descriptive statistics were undertaken for baseline variables to characterize the study population. Continuous variables were expressed in terms of mean, standard deviation, median and range. Categorical variables were expressed as percentages. To account for nonparametric distribution of some variables, Friedman’s nonparametric rank test was applied to compare primary and secondary outcome measures at three timepoints (baseline, nine and 52 weeks). Missing values were not imputed. P-values were two-sided and a value of less than 0.05 was considered statistically significant.
For CRQ-M, and those breathlessness impact outcomes showing significant improvement attaining minimal clinically important difference (MCID), predictors of response were sought in an exploratory analysis using linear regression models. Pre-specified variables under consideration included sex, body mass index (BMI), forced expiratory volume in one second (FEV1), ratio of FEV1 to forced vital capacity (FEV1/FVC), MoCA and baseline scores for Depression, Anxiety and Stress Scale 21, depression and anxiety components (DASS 21-D and DASS 21-A).32,35 Subsequently, COPD exacerbation status for the year prior and urgent healthcare visits during the nine-week clinic intervention were also investigated as predictors of response.
Finally, to investigate potential for selection bias from attrition, unpaired Student’s t-tests (assuming equal or unequal variances as appropriate) were undertaken to compare study completer and non-completer groups in terms of baseline parameters – gender, age, FEV1, pack years, BMI, CRQ-M, COPD Assessment Test (CAT)36 score and MoCA.
Results
Of 92 recruited patients, three were excluded due to ineligible spirometry, leaving 89 patients contributing to baseline data. Of these, 85 (96%) completed the MBC intervention, providing breathlessness impact questionnaire data at week nine. Seventy-four patients (83%) contributed to the final data collection at 52 weeks. Of non-completers, eight patients died, six partially withdrew, as described below, and one fully withdrew from the study. Of the four patients who left the study prior to MBC graduation, all “partially withdrew” from the MBC project, meaning that there was ongoing permission to use their existing data and to collect healthcare outcome data. Two were hospitalized, then discharged to a residential aged-care facility, one was accepted onto the lung transplant waiting list (therefore requiring formal enrolment to a pulmonary rehabilitation program) and one changed her mind about study participation. Reasons given for withdrawal after graduation from MBC related to the burden of repeated questionnaire completion, dwindling interest and lack of conviction about MBC benefit. Figure 2 details participant recruitment and retention through the study protocol.
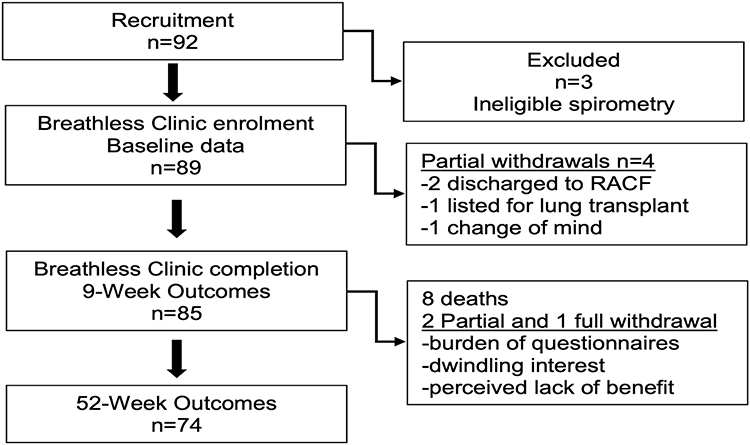 |
Figure 2 Subject Recruitment and Retention. Participants who “partially withdrew” discontinued the study protocol but gave ongoing permission to use their existing data and to collect healthcare outcome data. Abbreviation: RACF, residential aged care facility. |
Characteristics of the MBC study population are detailed in Table 2 and Figure 3. Participants had severe airflow obstruction, substantial smoking exposure and adverse body mass. Applying the MoCA indicated 59% prevalence of cognitive impairment, defined as score <26. Screening with MNA-SF identified malnourishment in 20% and risk of malnutrition in a further 38%. Baseline DASS-21 and CAT scores were elevated, respectively signifying abnormal levels of psychological distress and high COPD-related symptom burden. Within the year prior to participation in MBC, 61 patients (69%) reported at least one exacerbation and during the clinic intervention 21 (24%) had unplanned health care utilization (HCU), either an emergency department visit or hospitalization.
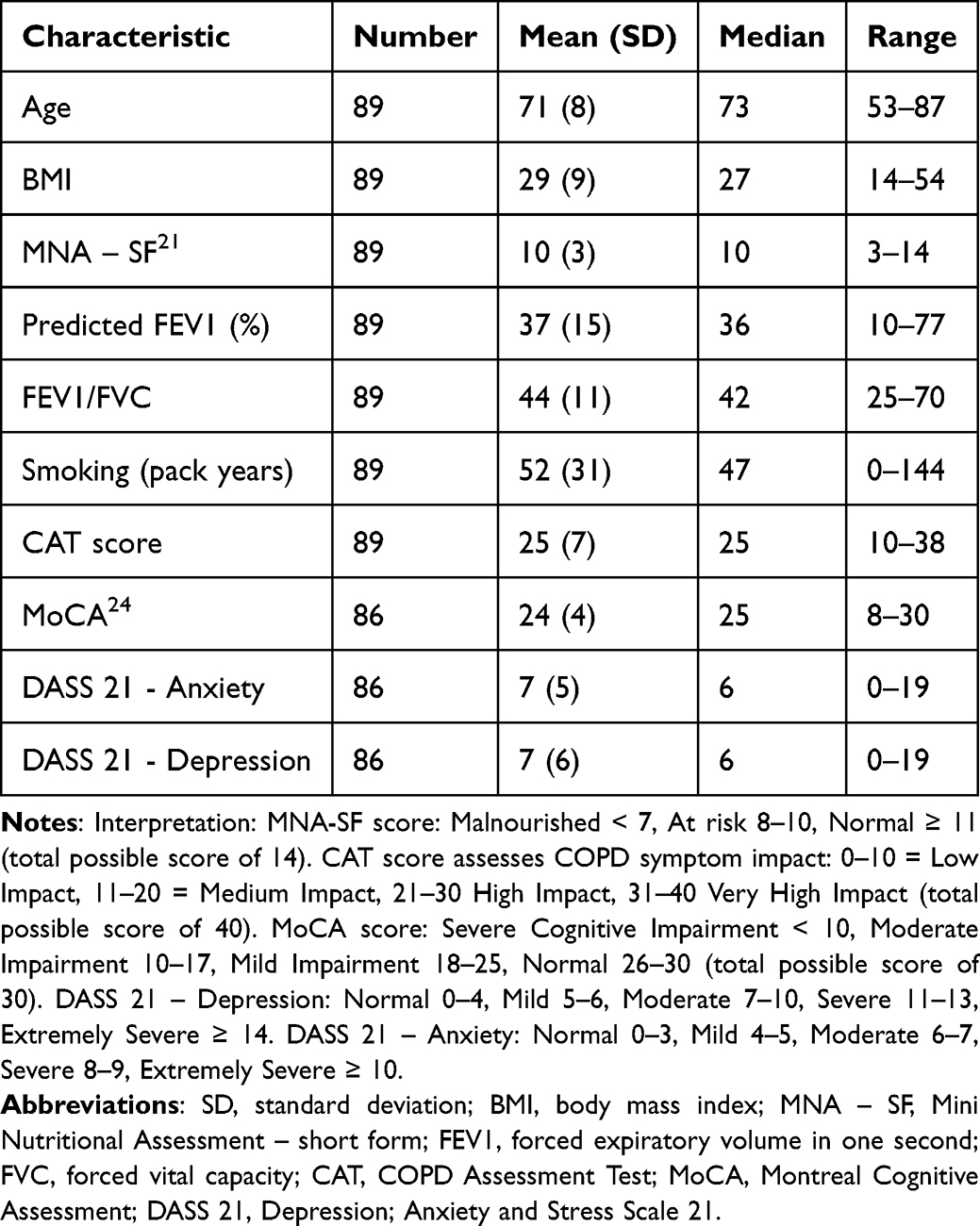 |
Table 2 Macarthur Breathless Clinic Population Characteristics at Baseline |
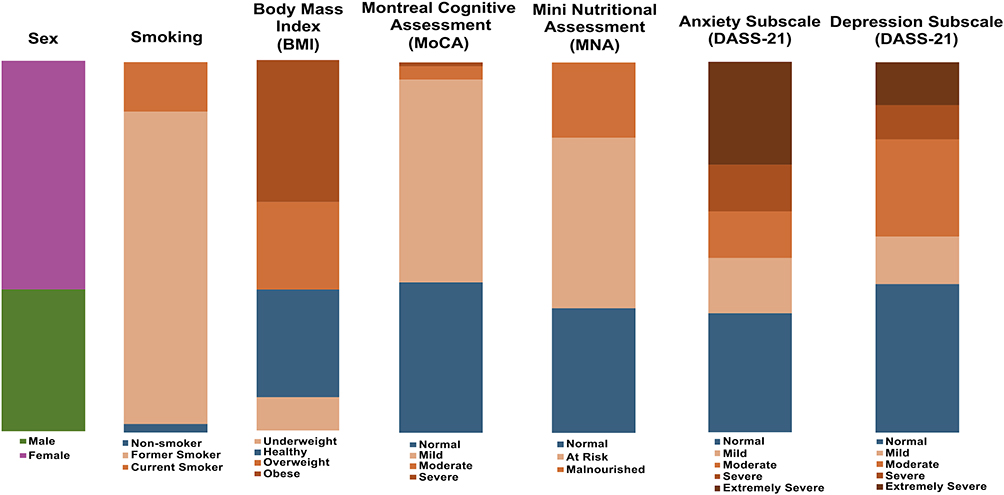 |
Figure 3 Macarthur Breathless Clinic Population Characteristics at Baseline – categorical data presented as percentage stacked bar charts. BMI (kg/m2) Categories – Underweight < 18.5, Normal 18.5–24.9, Overweight 25–29.9, Obese > 30 NMA-SF Categories – Malnourished < 7, At risk 8–10, Normal ≥ 11 (total possible score of 14) MoCA Categories – Severe Cognitive Impairment < 10, Moderate Impairment 10–17, Mild Impairment 18–25, Normal 26–30 (total possible score of 30) Depression Anxiety and Stress Scale (DASS-21) – Depression: Normal 0–4, Mild 5–6, Moderate 7–10, Severe 11–13, Extremely Severe ≥ 14 Anxiety: Normal 0–3, Mild 4–5, Moderate 6–7, Severe 8–9, Extremely Severe ≥ 10 Stress: Normal 0–7, Mild 8–9, Moderate 10–12, Severe 13–16, Extremely Severe ≥ 17. |
Breathlessness impact outcomes are presented in Table 3. After 12 months, breathlessness impact outcome data from baseline, nine and 52 weeks were subject to Friedman’s nonparametric rank test. All breathlessness impact outcome measures showed statistically significant improvement with the exception of European Quality of Life – Visual Analogue Scale (EQ-VAS), CRQ – fatigue and DASS 21 – anxiety subscales. Parameters which showed improvements considered clinically meaningful based on MCID include the study’s primary outcome, CRQ-M, with baseline mean value 3.9, increasing to 4.4 at week nine and further to 4.8 at week 52 (p < 0.0001). The Numeric Rating Scale (NRS) results for confidence in managing breathlessness were aligned with the mastery score (mean baseline score 5.8, week nine score 7.1 and week 52 score 7.6, p<0.0001). Scores representing symptom burden too showed sustained improvements, with CAT and CRQ-Dyspnea (CRQ-D) subscale scores respectively improving by 2 points (p=0.0002, MCID 2) and by 0.6 points (p=0.0003, MCID 0.5) at week 52. Analysis after transformation to numeric scale format 1 to 7, showed statistically significant symptom improvement for all Dalhousie pictorial scales.29 However, with the exception of CRQ-D, other questionnaire tools assessing breathlessness per se (NRS for breathlessness severity and unpleasantness) showed no clinically relevant change.
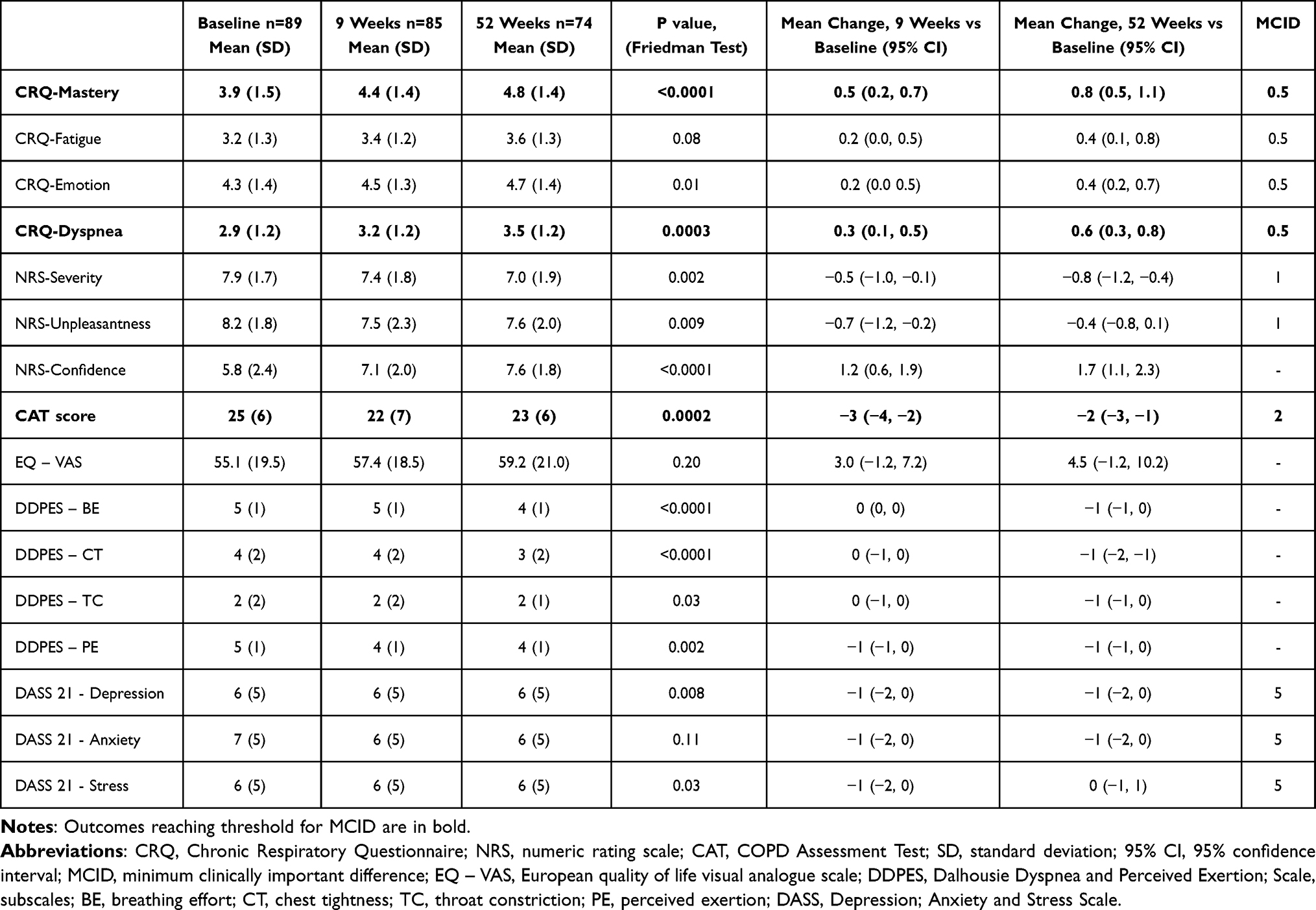 |
Table 3 Breathlessness Impact Questionnaires – Outcomes Over 12 Months |
Exploratory analyses were conducted, applying linear regression models to investigate predictors of response, with response defined as statistically significant improvement post MBC completion meeting MCID. For CRQ-M, increased baseline anxiety (DASS-A) predicted a positive response (p=0.04) and increased baseline depression (DASS-D) also approached significance as a predictor (p=0.06). However, the strongest predictors were for improvement in CAT score, with higher cognitive function (MoCA) score proving most potent (p=0.006). Decreased FEV1 (p=0.03) and increased baseline depression (DASS-D) (p=0.04) also predicted improvement. For confidence managing breathlessness, higher BMI and FEV1 both predicted lack of response (p=0.05). Whilst having at least one exacerbation in the 12 months prior to participating in MBC did not predict responses, an unplanned healthcare visit during the nine-week clinic intervention predicted achieving MCID for CRQ-M and CAT score at twelve months. No predictors were found for response in CRQ-D. Although sex was not discriminatory for any outcome, the mean improvement in females for CAT score was 2.9 points as opposed to 0.5 points in males (p=0.06). Whilst clearly these hypothesis-generating results should be interpreted with discretion, they may provide useful direction for future research particularly in terms of COPD patient selection.
Lastly, analysis was conducted to compare participants who completed the study protocol and those who left the study, to explore the potential impact of selection bias due to attrition. The patients who failed to complete the study protocol were similar to those who did in terms of age, sex distribution, BMI, FEV1 and baseline scores for CAT and CRQ-M (Table 4). Neither did they differ from the perspective of having exacerbations within the year prior to MBC participation. However, the non-completers had a lower mean MoCA (21 versus 25, p = 0.001) and greater mean pack years (68 versus 49, p = 0.03).
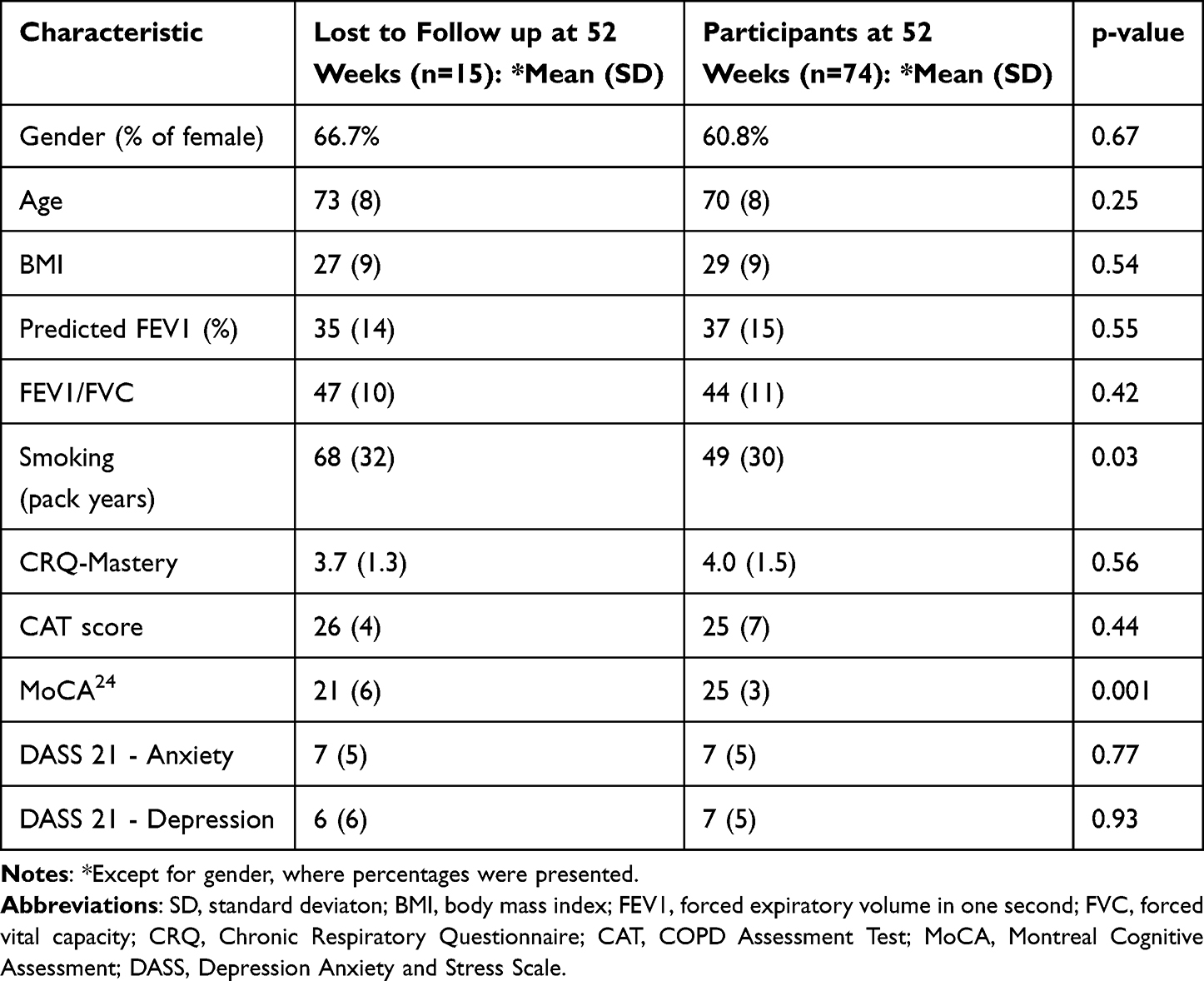 |
Table 4 Comparison Between Participants Lost to Follow up Versus Those Completing at 52 weeks |
Discussion
Following the Macarthur Breathless Clinic (MBC), we report statistically significant and clinically relevant within-subject improvement in the primary outcome of CRQ-Mastery, at nine weeks in an Australian cohort with COPD. Moreover, we are the first to report durable quantitative results after this type of intervention, with outcomes reported to 12 months.
Mean mastery of breathlessness increased by 0.5 (p=0.0001) at nine weeks and improved further, increasing by 0.9 at 12 months (p<0.0001). Given that the MCID for this measure is 0.5, such improvement should be readily appreciated by patients. Response durability is a particularly important finding for patients with COPD due to its chronic, progressive nature and hence an expectation of symptom deterioration rather than improvement over the long term.
We also report statistically significant within-subject improvements at nine weeks and 12 months in a variety of secondary outcomes measuring breathlessness impact, including measures of psychological distress and overall symptom burden from COPD. At 12 months following the intervention we report ongoing, clinically relevant within-subject improvements in CRQ-dyspnea (0.6, p<0.0003, MCID = 0.5), patient-reported confidence in managing breathlessness (1.8, p<0.0001) along with durable benefits in COPD symptom burden as measured by COPD Assessment Test (CAT) score (2, p=0.0002, MCID = 2).
Comparison to Other Literature
Our results are similar to the randomized controlled trials for BIS-targeting populations with non-malignant disease for the primary outcome of breathlessness mastery at nine weeks14,15 and seem superior to that reported in a systematic review10 of other published works, including populations with malignant disease, non-malignant disease or both combined. The reason for this difference remains unclear. Our intervention was longer (nine weeks versus two to six weeks), included a broader healthcare team and our target study population was more homogeneous, all subjects being diagnosed with COPD.
Longer term outcomes have been reported only rarely, although, in a qualitative paper, Luckett et al reported that patients seemed to have forgotten the intervention when interviewed at 6 months37 Our results suggest that even if so, patients continue to gain quantitative improvements across a range of breathlessness and illness domains.
Implications for Clinicians and Policy-Makers
Given the growing evidence base for BIS, clinicians should strive to incorporate non-pharmacological interventions aimed at alleviating breathlessness as part of standard care. Clinicians may be concerned that teaching these techniques will be time-consuming. However, it may be possible to introduce techniques sequentially, taking only a few minutes during a single encounter. Policy-makers need greater awareness and understanding of the potential for these interventions to significantly enhance patient well-being, with likely downstream benefits and even the possibility perhaps to impact urgent healthcare utilization. These findings have important implications for targeted health funding, supporting services such as MBC that enable patients—particularly those with COPD—to better manage chronic breathlessness. This is especially relevant given the high healthcare costs associated with COPD, despite the use of guideline-directed pharmacological therapies.
Strengths and Limitations
The strength of this work is that it reports long-term outcomes for a relatively large, homogeneous population with moderately severe COPD. The study setting of urban Australia provides one of few reports from outside Europe. Additionally, a substantial proportion (10%) of our population identified as Aboriginal Australian. This exceeds the known indigenous representation within our local community and their inclusion implies successful engagement of a group subject to health outcome inequity. Nonetheless, due to the small numbers, stratified analysis according to Aboriginal status was not appropriate.
In addition to measures of breathlessness, we reported CAT score, which is a disease-specific measure of COPD symptom burden, routinely used both in research and in clinical practice to assess the impact of treatment interventions for COPD. The improvement in CAT score adds weight to our results and will be meaningful to clinicians working in the field, allowing the MBC to be more easily measured up against other treatment strategies used in this disease. We also included a pictorial measure of breathlessness29 to provide participants with additional means to describe their breathlessness severity without reliance on language or literacy, which may contribute to future solutions for assessing (and addressing) breathlessness needs, bypassing language barriers. In addition, we reported measures of psychological distress, which expands the understanding of MBC’s impact in a more holistic sense. Importantly, the assessment of 12-month data negates the seasonal influence of COPD exacerbations, which may impact data collected over shorter timeframes. Finally, we used the STROBE guidelines (Supplement file – STROBE statement) to increase reporting quality and transparency.
The study, although prospective, was a single-arm study hosted at a single center, limiting generalizability. We were aware of a randomized controlled trial19 in a nearby health district being conducted contemporaneously, using a model of care similar to our own. We thus preferred a non-randomized study design to address clinical need, whilst simultaneously demonstrating applicability to a different patient population and setting, accepting that this choice would be at the cost of research rigor. Similar to other BIS, we undertook some interventions in the home setting, allowing the intervention to be individualized to patients’ specific circumstances. We acknowledge that this is difficult to replicate in a conventional clinic, although this limitation may be somewhat mitigated by increased integration with available community-based healthcare services.
We acknowledge that our reported outcomes will be subject to selection bias, particularly from attrition. By 52 weeks, 15 participants had left the study, amounting to 17% of the study cohort. Losses from the study population prior to protocol completion may raise concerns about lack of intervention efficacy or poor tolerability, although the listed reasons for non-completion (see Figure 2) would not support this, with 85 of 89 (96%) completing the clinic intervention and most (11 of 89, 12%) departing the study due to changed circumstances or death. Hence, for our study, the main concern for attrition relates to generalizability, particularly if it was those with more severe disease who left our study prior to protocol completion. However, patient losses from the study were less than anticipated and we reduced impact of this potential bias by having patients act as their own controls. Moreover, comparison of baseline data between study completers and non-completers revealed few differences between the groups; only significantly greater pack years and lower MoCA scores in the non-completers (Table 4), with traditional markers of severity or prognosis, such as FEV1, BMI and CAT score not significantly different between the groups. Thus, the implications for selection bias are likely to be modest.
Finally, for a study with many key outcomes assessed via questionnaires, the mode of their administration needs consideration. Whilst having questionnaires interviewer-administered increases completion likelihood and can reduce time burden for participants, this provides potential for the interviewer to influence the responses recorded by unconsciously conveying their own expectations (observer bias), by guiding or interpreting answers. A second important concern is social acceptability bias, whereby presence of an interviewer and resulting anonymity loss may inhibit or influence the responses received. Further, due to staffing constraints in our study, outcome data were collected by a member of the clinical team, which potentially may have heightened the risk for social acceptability bias to affect patient-reported measures (due to the nature of the existing relationship between patient and clinician). Unfortunately, the extent to which these factors may have affected the study outcomes remains unclear.
Future Research
The majority of costs of COPD care are related to hospitalizations.28 Thus, reducing potentially avoidable hospitalizations by giving patients tools to manage breathlessness has the potential to impact HCU in the Australian setting and so further research into this question remains a priority. The wide variation in the characteristics of forerunner BIS – including clinic composition, clinical disciplines and specialty expertise, encounter format and schedule, component strategies, and intervention duration – highlights the need for future research to identify the attributes most critical for achieving positive outcomes and cost-effectiveness, in order to enhance the delivery of efficient healthcare models. In addition, reaching consensus on the most appropriate outcome measures remains a key priority.
Conclusions
This study demonstrates statistically significant and clinically meaningful within-subject improvements in breathlessness mastery following a home-based multidisciplinary breathlessness intervention service, not only evident at nine weeks but sustained and further enhanced over 12 months. The durability of these improvements is particularly noteworthy given the progressive trajectory of COPD, which is typically characterized by gradual worsening of symptoms over time. In addition to the primary outcome, significant and lasting gains were also observed across key secondary measures, including dyspnea and overall symptom burden. These findings should be considered in the context of the non-randomised study design and inherent risks of bias. Nonetheless, they support the potential value of a home-based multidisciplinary breathlessness program as a viable, long-term intervention to enhance quality of life in individuals living with COPD.
Human/Animal Ethics Approval Declaration
This human study was performed in accordance with the Declaration of Helsinki and approved by South Western Sydney Local Health District Human Research Ethics’ Committee – approval: 2020/PID00145. The study’s clinical trial registration number is ACTRN12620001330932, listed with the Australian and New Zealand Clinical Trial Registry; https://www.anzctr.org.au/. All participants provided written informed consent to participate.
Abbreviations
COPD, chronic obstructive pulmonary disease; QoL, quality of life; MBC, Macarthur Breathless Clinic; FEV1, forced expiratory volume in one second; COVID-19, Coronavirus of 2019; BIS, breathlessness intervention service(s); PR, pulmonary rehabilitation; HCU, Healthcare utilisation; mMRC, modified Medical Research Council; MDT, multidisciplinary team; MNA-SF, Mini Nutritional Assessment – Short Form; EAT-10, Eating Assessment Tool; MoCA, Montreal Cognitive Assessment; CRQ-M, Chronic Respiratory Questionnaire – Mastery Subscale; MCID, minimal clinically important difference; BMI, body mass index; FEV1/FVC, ratio of FEV1 to forced vital capacity; DASS 21-D, Depression, Anxiety and Stress Scale 21 – Depression subscale; DASS 21-A, Depression, Anxiety and Stress Scale 21 – Anxiety subscale; CAT, COPD Assessment Test; EQ-VAS, European Quality of Life Visual Analogue Scale; NRS, numeric rating scale; CRQ-D, Chronic Respiratory Questionnaire – Dyspnoea Subscale; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
Acknowledgement is due to the patients and their carers, who were willing to try something new, to the staff at Rosemeadow Community Health Centre, to colleagues from the Department of Respiratory and Sleep Medicine at Macarthur (Camden and Campbelltown Hospitals) and the outpatient clinics, without whom this work would not have been possible. The authors would also convey thanks to Mr. W. Brakel and Mrs. J. Cochrane for their valuable contributions to image design and critiquing the manuscript.
Funding
Funding for this study was provided by GlaxoSmithKline (GSK), although GSK had no role in project development, study design/conduct, nor data analysis. GSK was provided opportunity for a courtesy review of a manuscript draft for accuracy only. However, the authors are solely responsible for final content and interpretation.
Disclosure
The abstract of this paper was presented at the 2025 European Respiratory Society Congress as a poster presentation with interim findings in the session “The next big trials: insights from qualitative and feasibility studies”. The poster’s abstract was published in Eur Respir J 2025; 66: Suppl. 69, PA1772 https://doi.org/10.1183/13993003.congress-2025.PA1772.
Belinda Cochrane received an investigator-sponsored study grant from GSK to conduct the research conducted for this manuscript, personal advisor/consultancy fees from GSK and Sanofi, speaker fees from Chiesi, Moderna, Astra Zeneca (AZ), Inside Practice and RX Global, and is a member of Lung Foundation Australia’s COPD Coordinating Committee, none of which represent direct COI with the work presented here.
Mohmedsaqib Akhunji has received funding from SWSLHD as contribution for travel and conference attendance to present research related to this project. This is relevant to the current manuscript but does not represent a COI.
Sheree Smith declares membership of the TSANZ Conference Committee but has no specific conflicts related to this work.
Soo Wei Foo has received speaker fees from AZ, Travel and accommodation support from GSK, Chiesi, AZ and Boehringer Ingelheim, none of which represent direct COI with the work presented here.
Teresa Kemp declares membership of the Respiratory Nurses Special Interest Group but has no specific conflicts related to this work.
Wei Xuan, Jonathan Lee, Tracy Smith and Luisa Garcia have no potential conflicts of interest to declare.
References
1. Augusti AG, Vogelmeier C. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease (2024 report). 2024.
2. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–15. doi:10.1016/S2213-2600(21)00511-7
3. Toelle BG, Xuan W, Bird TE, et al. Respiratory symptoms and illness in older Australians: the Burden of Obstructive Lung Disease (BOLD) study. Med J Aust. 2013;198(3):144–148. doi:10.5694/mja11.11640
4. Global health estimates 2021: deaths by cause, age, sex, by country and by region, 2000-2021. World Health Organization; 2024.
5. Health AIo, Welfare. Australian Burden of Disease Study 2024. Canberra: AIHW; 2024.
6. Health AIo, Welfare. Disparities in Potentially Preventable Hospitalizations Across Australia, 2012-13 to 2017-18. Canberra: AIHW; 2020.
7. Health AIo. Welfare. Chronic Obstructive Pulmonary Disease. Canberra: AIHW; 2024.
8. Blinderman CD, Homel P, Billings JA, Tennstedt S, Portenoy RK. Symptom distress and quality of life in patients with advanced chronic obstructive pulmonary disease. J Pain Symptom Manage. 2009;38(1):115–123. doi:10.1016/j.jpainsymman.2008.07.006
9. Bausewein C, Schunk M, Schumacher P, et al. Breathlessness services as a new model of support for patients with respiratory disease. Chron Respir Dis. 2018;15(1):48–59. doi:10.1177/1479972317721557
10. Brighton LJ, Miller S, Farquhar M, et al. Holistic services for people with advanced disease and chronic breathlessness: a systematic review and meta-analysis. Thorax. 2019;74(3):270–281. doi:10.1136/thoraxjnl-2018-211589
11. Chin C, Massou E, Burkin J, Booth S, Spathis A. P-111 Cambridge breathlessness intervention service: impact on hospital attendance. British Med J Publishing Group. 2018.
12. Seidl H, Schunk M, Le L, et al. Cost-effectiveness of a specialized breathlessness service versus usual care for patients with advanced diseases. Value Health. 2023;26(1):81–90. doi:10.1016/j.jval.2022.08.002
13. Takemura N, Maddocks M, Brighton LJ. Advances in breathlessness support services for people with serious illness. Curr Opin Support Palliat Care. 2024;18(4):199–205. doi:10.1097/SPC.0000000000000723
14. Farquhar MC, Prevost AT, McCrone P, et al. The clinical and cost effectiveness of a Breathlessness Intervention Service for patients with advanced non-malignant disease and their informal carers: mixed findings of a mixed method randomised controlled trial. Trials. 2016;17(1):1–16. doi:10.1186/s13063-016-1304-6
15. Higginson IJ, Bausewein C, Reilly CC, et al. An integrated palliative and respiratory care service for patients with advanced disease and refractory breathlessness: a randomised controlled trial. Lancet Respir Med. 2014;2(12):979–987. doi:10.1016/S2213-2600(14)70226-7
16. Schunk M, Le L, Syunyaeva Z, et al. Effectiveness of a specialized breathlessness service for patients with advanced disease in Germany: a pragmatic fast-track randomized controlled trial (BreathEase). Eur Resp J. 2021;58(2):2002139. doi:10.1183/13993003.02139-2020
17. O’Donnell DE, Milne KM, James MD, de Torres JP, Neder JA. Dyspnea in COPD: new mechanistic insights and management implications. Adv Ther. 2020;37(1):41–60. doi:10.1007/s12325-019-01128-9
18. Calverley P. Exercise and dyspnoea in COPD. Eur Respir Rev. 2006;15(100):72–79. doi:10.1183/09059180.00010004
19. McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y; Cochrane Airways Group. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Systematic Rev. 1996;2015(4)
20. Keating A, Lee A, Holland AE. What prevents people with chronic obstructive pulmonary disease from attending pulmonary rehabilitation? A systematic review. Chron Respir Dis. 2011;8(2):89–99. doi:10.1177/1479972310393756
21. Smith TA, Roberts MM, Cho J-G, et al. Protocol for a single-blind, randomized, parallel-group study of a nonpharmacological integrated care intervention to reduce the impact of breathlessness in patients with chronic obstructive pulmonary disease. Palliative Med Rep. 2020;1(1):296–306. doi:10.1089/pmr.2020.0081
22. Rubenstein LZ, Harker JO, Salvà A, Guigoz Y, Vellas B. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol a Biol Sci Med Sci. 2001;56(6):M366–M72. doi:10.1093/gerona/56.6.M366
23. Vellas B, Villars H, Abellan G, et al. Overview of the MNA--Its history and challenges. J Nutr Health Aging. 2006;10(6):456.
24. Belafsky PC, Mouadeb DA, Rees CJ, et al. Validity and reliability of the Eating Assessment Tool (EAT-10). Ann Otolaryngol. 2008;117(12):919–924.
25. Hobson J. The Montreal cognitive assessment (MoCA). Occup Med. 2015;65(9):764–765. doi:10.1093/occmed/kqv078
26. Spathis A, Booth S, Moffat C, et al. The breathing, thinking, functioning clinical model: a proposal to facilitate evidence-based breathlessness management in chronic respiratory disease. NPJ Prim Care Respir Med. 2017;27(1):27. doi:10.1038/s41533-017-0024-z
27. Guyatt GH. Chronic respiratory diseases questionnaire: American thoracic society. 2002. Available from: http://qol.thoracic.org/sections/instruments/ae/pages/crq.html.
28. Ekström M, Currow DC, Johnson MJ. Outcome measurement of refractory breathlessness: endpoints and important differences. Curr Opin Support Palliat Care. 2015;9(3):238–243. doi:10.1097/SPC.0000000000000147
29. Pianosi PT, Zhang Z, Hernandez P, Huebner M. Measuring dyspnea and perceived exertion in healthy adults and with respiratory disease: new pictorial scales. Sports Med Open. 2016;2(1):1–8. doi:10.1186/s40798-015-0038-4
30. Jones PW, Harding G, Berry P, Wiklund I, Chen W-H, Kline Leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
31. Kon SSC, Canavan JL, Jones SE, et al. Minimum clinically important difference for the COPD assessment test: a prospective analysis. Lancet Respir Med. 2014;2(3):195–203. doi:10.1016/S2213-2600(14)70001-3
32. Lovibond SH, Lovibond PF. Manual for the Depression Anxiety Stress Scales.
33. Yohannes AM, Dryden S, Hanania NA. Validity and responsiveness of the depression anxiety stress scales-21 (DASS-21) in COPD. Chest. 2019;155(6):1166–1177. doi:10.1016/j.chest.2018.12.010
34. Non-pharmacological intervention to improve breathlessness mastery in COPD: pilot study. In: Smith T, Roberts M, Cho J, Wheatley J, editors. Respirology. NJ, USA: WILEY 111 RIVER ST, HOBOKEN 07030-5774; 2019.
35. Henry JD, Crawford JR. The short-form version of the Depression Anxiety Stress Scales (DASS-21): construct validity and normative data in a large non-clinical sample. Br J Clin Psychol. 2005;44(2):227–239. doi:10.1348/014466505X29657
36. Jones P, Harding G, Wiklund I, Berry P, Leidy N. Improving the process and outcome of care in COPD: development of a standardised assessment tool. Prim Care Respir J. 2009;18(3):208–215. doi:10.4104/pcrj.2009.00053
37. Luckett T, Roberts M, Swami V, et al. Maintenance of non-pharmacological strategies 6 months after patients with chronic obstructive pulmonary disease (COPD) attend a breathlessness service: a qualitative study. BMJ Open. 2021;11(5):e050149. doi:10.1136/bmjopen-2021-050149
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Experiences, Values and Goals of People Living with Obstructive Hypertrophic Cardiomyopathy: Exploratory Patient Interviews
Fifer S, Pendleton A, Ingles J, Godsell J, Zhong Y, Krause T
Patient Preference and Adherence 2026, 20:554609
Published Date: 14 May 2026
Psychological-Symptom Mismatch Phenotypes and Their Clinical Implications in Patients with Chronic Obstructive Pulmonary Disease
Cai Y, Ren X, Wang K, Cheng H
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:593901
Published Date: 11 June 2026
Blood-Based Inflammatory and Metabolic Biomarkers for Assessing Symptom Burden and Quality of Life in Older Adults with Cancer: A Narrative Review
Lu L, Zhang Y
Therapeutics and Clinical Risk Management 2026, 22:611486
Published Date: 18 June 2026
Multidisciplinary Palliative Care and Its Impact on Symptom Burden and Quality of Life in Advanced Cancer Patients in Ethiopia: A Pre–Post Quasi-Experimental Study

Fentie AM, Seife E, Ozawa S, Fenta TG
Cancer Management and Research 2026, 18:624631
Published Date: 17 July 2026