Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Elevated C-Reactive Protein and Erythrocyte Sedimentation Rate Correlates with Depression in Psoriasis: A Chinese Cross-Sectional Study
Authors Tan M ![]() , Luo Y, Hu J, Hu K, Li X, Yang J, Chen J, Zhu W
, Luo Y, Hu J, Hu K, Li X, Yang J, Chen J, Zhu W ![]() , Kuang Y
, Kuang Y
Received 18 December 2022
Accepted for publication 7 February 2023
Published 13 February 2023 Volume 2023:16 Pages 397—405
DOI https://doi.org/10.2147/CCID.S401934
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Minjia Tan,1– 3,* Yan Luo,4,* Jingjin Hu,1– 3 Kun Hu,1– 3 Xingyu Li,1– 3 Jing Yang,1– 3 Junchen Chen,1– 3 Wu Zhu,1– 3 Yehong Kuang1– 3
1The Department of Dermatology, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 2National Clinical Research Center for Geriatric Disorders (Xiangya Hospital), Changsha, People’s Republic of China; 3Hunan Engineering Research Center of Skin Health and Disease; Hunan Key Laboratory of Skin Cancer and Psoriasis (Xiangya Hospital), Changsha, People’s Republic of China; 4Department of Dermatology, Jiangxi Provincial People’s Hospital, Nanchang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yehong Kuang; Wu Zhu, Email [email protected]; [email protected]
Purpose: Psoriasis patients often suffers from anxiety and depression. Inflammation, anxiety, and depression have been associated with each other, but the relationship has not been examined in subjects with psoriasis. The primary objective was to investigate the relationship between the C-reactive protein (CRP) and the erythrocyte sedimentation rate (ESR) and depression among patients with psoriasis.
Methods: In this case-control, cross-sectional study, 239 individuals with psoriasis and 142 with healthy controls (HCs) were recruited. Psychological as well as clinical, and laboratory data were collected.
Results: 50.2% of subjects with psoriasis reported depressive symptoms, compared with 26.8% of HCs. 39.7% and 17.6% observed anxiety symptoms in psoriasis patients and HCs. The odds of anxiety (AOR= 3.123; 95% CI = 1.851– 5.269) and depression (AOR= 2.698; 95% CI = 1.690– 4.306) were higher in psoriasis patients relative to HCs. Furthermore, the elevated CRP (AOR =2.139; 95% CI = 1.249– 3.663) and ESR (AOR =1.827; 95% CI = 1.078– 3.096) were the risk factors of depression in patients with psoriasis. The threshold for distinguish psoriasis patients in depression was 3.24 (area under the curve [AUC], 0.605; sensitivity, 0.57; specificity, 0.64) for CRP and 26.5 (AUC, 0.632; sensitivity, 0.52; specificity, 0.73) for ESR.
Conclusion: A substantial prevalence of anxiety and depression symptoms was observed in Chinese psoriasis subjects, and the odds were much higher in psoriasis patients relative to HCs. The elevated CRP and ESR level was significantly associated with depression in psoriasis patients. Besides, the discrimination capability of CPR and ESR on depression further indicates the extra value of inflammatory biomarkers in the management of psoriasis patients.
Keywords: psoriasis, depression, anxiety, C-reactive protein, erythrocyte sedimentation rate
Introduction
Psoriasis is a common, chronic inflammatory psycho-physiological disease, affecting approximately 0.1–11.4% of the general global population and 0.47% of the Chinese.1–3 Recent systemic review indicated the prevalence of comorbid depression up to 62%4 and anxiety up to 32%5 in psoriasis, and our previous research also found a high prevalence of depression in psoriasis.6 Moreover, psychological disorders were proved to be more prevalent in patients with psoriasis than in healthy controls.7,8 Therefore, those mental disorders may independently predispose patients to the development of psoriasis, resulting in a substantial burden for individuals and society.4,9 Although there is an unequivocal link between depression/anxiety and psoriasis, the direction of this association remains unclear.
Recently, guidelines recommended depression and anxiety screening by dermatologists,10 yet underscreening of mental health in outpatients with psoriasis has been reported recently.11 A growing body of research investigate the correlation between demographic characteristic, clinical data, disease activity and anxiety and depression in psoriasis, but few focused on laboratory parameters. Recent research supposed that the possible cause is the overlap of peripheral inflammatory biomarkers in the pathogenesis of psoriasis and those psychological disorders. Despite a known correlation between inflammatory biomarkers such as CRP and ESR and depression,12,13 this relationship has not been reported in patients with psoriasis. Moreover, limited data is available on the relation of CRP or ESR to anxiety in psoriasis.14
Hence, investigation of the correlation between inflammation and depression and characterization of the burden of depression and anxiety using validated patient-reported measurements are urgently needed for patients with psoriasis in China. The present work aimed to describe the prevalence of depression and anxiety in subjects with psoriasis and assess the odds of depression and anxiety in adults with psoriasis compared with healthy controls (HCs). In addition, to identify the association between demographic and clinical factors, especially CRP and ESR, and anxiety and depression in psoriasis. Moreover, to evaluate whether the level of CRP or ESR could discriminate those disorders in psoriasis.
Materials and Methods
Patients and Study Design
In this cross-sectional case-controlled study, we consecutively recruited adult psoriasis patients from the outpatient Dermatology Department of Xiangya Hospital and healthy subjects, matching for sex and age, from the medical examination center of the Xiangya Hospital from January 2019 to September 2020. One or more dermatologists diagnosed Psoriasis Vulgaris patients according to typical clinical manifestation or histopathological examination, and dermatologists and rheumatologists confirmed the PsA based on Classification Criteria for Psoriatic Arthritis.15 The healthy controls (HCs) with a history of psoriasis were excluded. All participants accomplished a detailed interview, including demographic characteristics, body mass index (BMI), nine-item patient health questionnaire (PHQ-9),16 and seven-item Generalized Anxiety Disorder Scale (GAD-7).17 The samples with psoriasis were also completed disease characteristics and inflammatory and metabolic indicators, which contained the family history of psoriasis, duration of psoriasis, the severity of psoriasis (Psoriasis Area and Severity Index [PASI],18 Body Surface Area [BSA]), dermatology-specific health-related quality of life (Dermatology Life Quality Index [DLQI]),19 fasting blood glucose, uric acid, serum lipid level, CRP and ESR. In total, 239 patients with psoriasis and 142 with HC were involved in the present work. Our research meets the ethical standards of the Declaration of Helsinki and was approved by the institutional research ethics committees of Xiangya Hospital of Central South University, Changsha, Hunan, China (approval number:201904105). All subjects gave informed written consent before the investigation.
Data Collection
Depression
We selected the PHQ-9 (range, 0–27), the valid and the most widely used self-assessment instrument, to measure the presence and severity of depression. No depressive and depressive symptoms were defined by the score of PHQ-9 <5, and ≥5, respectively.16 The Chinese version of this questionnaire has been validated and has been proved to be a reliable measure of depression severity.20,21
Anxiety
GAD-7 (range, 0–21) was performed to screen the symptoms of anxiety, which included seven items and was proved to be a reliable self-report questionnaire.17 A cut-point of 5 was chosen to define symptoms of anxiety. The Chinese version of this questionnaire was also validated previously.22
Psoriasis Severity and Quality of Life
The severity of psoriasis and quality of life were evaluated by PASI (range, 0–72), BSA (range, 0–100%) and DLQI (range, 0–30), respectively. A score of PASI below 10 is considered mild psoriasis, and a score of 10 or above 10 suggests moderate-to-severe psoriasis, with BSA (%) using the same cut-off value to distinguish severity of psoriasis. For DLQI, mild psoriasis and moderate-to-severe psoriasis were also defined by the cut-off of 10. These categories were based on values established in the literature.
Peripheral Blood Inflammation and Metabolic Markers
The serum CRP and ESR were tested to evaluate inflammation and was expressed as milligram per liter (mg/L) and millimeter per hour (mm/h). The elevated CRP level was considered as >3 mg/L),23 and the elevated ESR is defined as >21 mm/h according to the hospital standard. The metabolic indicators include total cholesterol (TC), low-density lipoprotein-cholesterol (LDL-C), triglyceride (TG), and high-density lipoprotein cholesterol (HDL-C). Hyperlipidemia was defined as plasma TC >6.2 mmol/L), LDL-C >4.1 mmol/L), or TG >2.3 mmol/L), or HDL-C <1.0 mmol/L) or using lipid-lowering drugs currently with diagnosed hyperlipidemia.24 Hyperuricemia was determined by urate >420 umol/L in male and by >360umon/L in female. Elbow vein blood was obtained under fasting status on the same day or within three days of completion of the clinical evaluation. The tests were conducted in the laboratory department of Xiangya Hospital.
Demographic, Anthropometric, and Metabolic Data
A standard Case Report Form was undertaken to gather demographic data, including age, gender, education level, marital status, history of smoking, and history of drinking. The body mass index (BMI) was calculated using measured weight and height (kg/m2). The cut-off values of 24 and 28 for overweight and obesity, respectively.25
Statistical Analysis
The Shapiro–Wilk normality test measured distribution normality. Descriptive statistics were displayed as mean (standard deviation) for normally distributed data and median (interquartile range, IQR) for data that were not normally distributed, which were properly compared using t-tests, Mann–Whitney, or Kruskal–Wallis test. Categorical variables were expressed as numbers (percentage) and compared with analysis of the chi-square test or Fisher’s exact test. Then, binary logistic regression was used to investigate the odds ratio of patients with depression and anxiety in psoriasis compared with the healthy control group. Moreover, multivariable logistic regression to investigate the risk factors associated with depression and anxiety in patients with psoriasis. Odds ratio (OR) and 95% confidence interval (CI) were used to display the effect size of the associations. Receiver–operator curve (ROC) was performed to determine the CRP/ESR thresholds for depression based on the maximal Youden’s index for sensitivity and specificity.26 We considered p < 0.05 (two-tailed) statistically significant and analyzed all data with SPSS 25 (IBM, SPSS Statistics 25).
Results
Characteristics of Participants
239 participants with psoriasis and 142 with HCs consecutively accepted the invitation. The median age in psoriasis was 41.0 (IQR 32.0–50.0) and the HC was 43.0 (IQR 31.8–51.0) (p =0.935). The minority of participants were women (psoriasis vs HC: 81 [33.9%] vs 43 [30.3%], p =0.467). Both groups were similar in demographic variables, with the exceptions of educational level, history of smoking, and BMI (p =0.037, p =0.011, and p =0.020, respectively). As expected, the median (IQR) scores of PHQ-9 and GAD-7 were higher in subjects with psoriasis compared with the HCs group (5 [IQR, 2–8] vs 2 [IQR, 0–5]; p<0.001) and (4 [IQR, 1–6] vs 2 [IQR, 0–5]; p=0.001), respectively (Table 1).
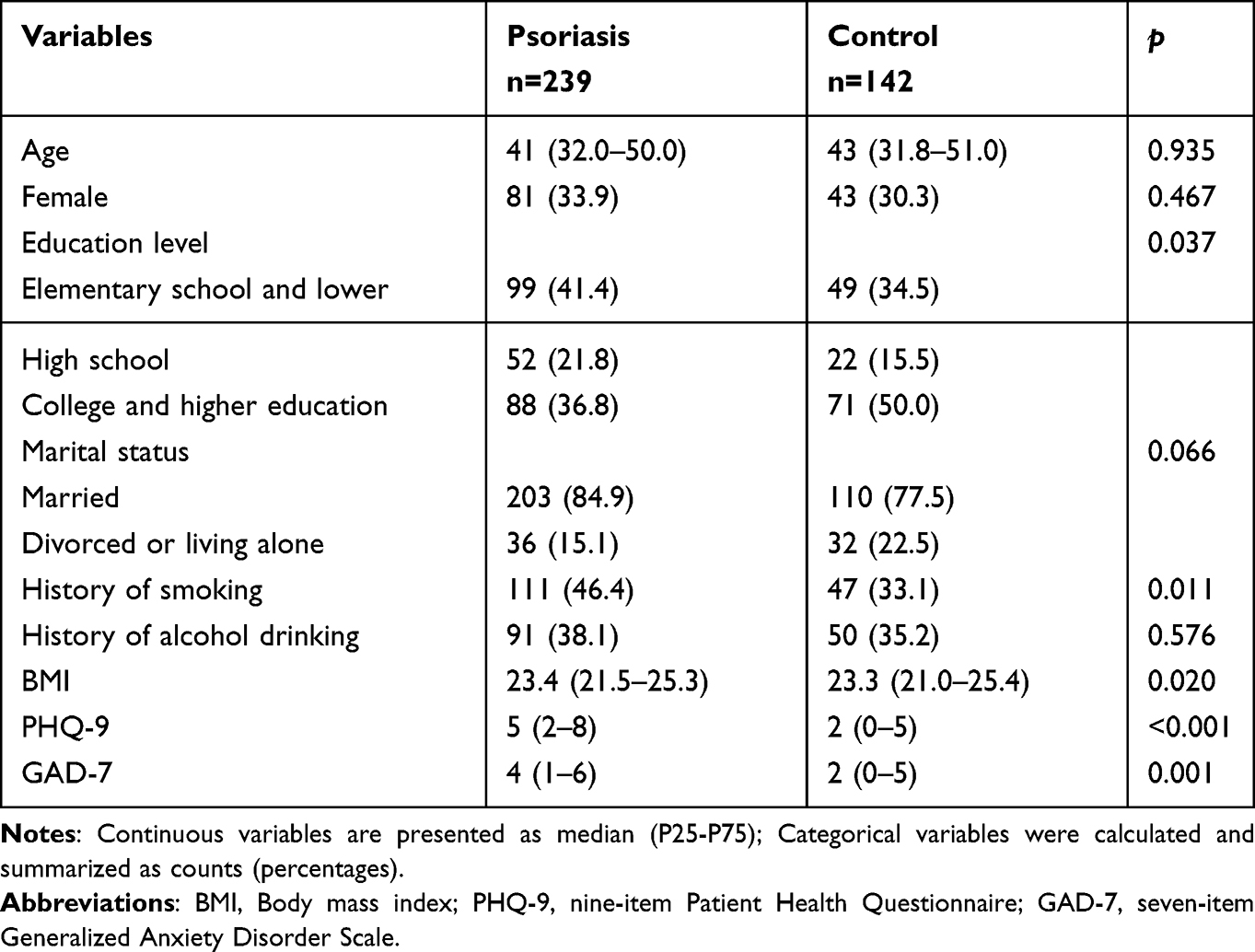 |
Table 1 Characteristics of the Cases and Healthy Controls |
Prevalence and Risk of Depression and Anxiety Were Higher in Patients with Psoriasis
The percentage of depression (PHQ-9 ≥5) and anxiety (GAD-7 ≥5) was 120 of 239 (50.2%) and 95 of 239 (39.7%), which were significantly higher than that of the HCs group (38/142 [26.8%] for depression and 25/142 [17.6%] for anxiety). Further multivariable analysis with adjustments indicated that the risk of depression in the psoriasis group was 2.698 times (adjusted OR [AOR] = 2.698; 95% CI = 1.690–4.306) and anxiety was 3.123 times (AOR =3.123; 95% CI = 1.851–5.269) higher than that in the healthy group (Table 2).
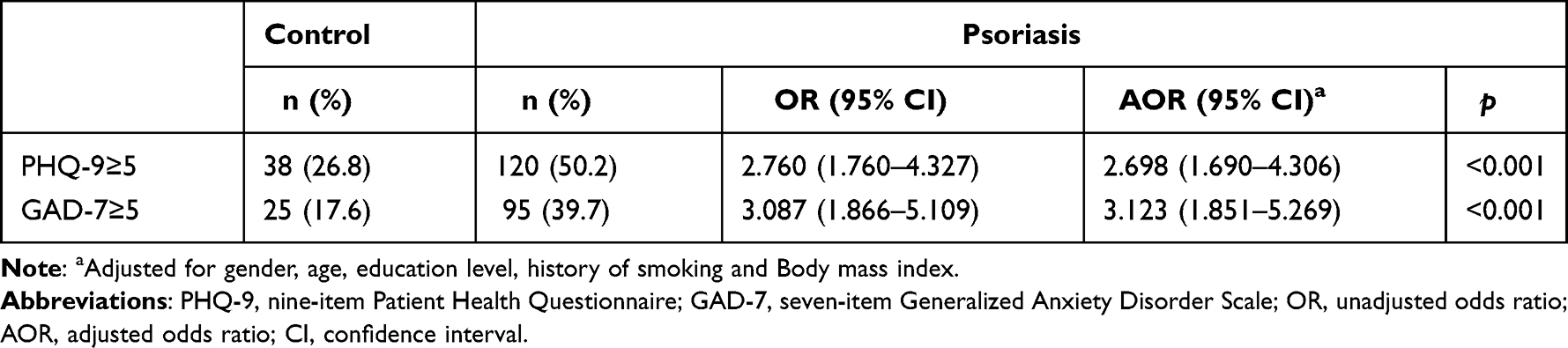 |
Table 2 The Association Between Depression and Anxiety of the Participants Among Psoriasis and Control Group Based on the Questionnaires |
Comparison of Demographics, Disease Characteristics, and Laboratory Parameters in Psoriasis Regarding Depression and Anxiety
Then, we compared the demographics, disease characteristics, and laboratory parameters regarding depression and anxiety in psoriasis. Gender, duration of psoriasis, PASI, BSA, DLQI, CRP, and ESR were significantly different between patients with depression and those without. The proportion of adults with depression was significantly higher in PASI ≥ 10 (55.0.2% VS 42.0%, p=0.045), BSA ≥10 (57.8% VS 42.2%, p=0.012), DLQI ≥10 (34.2% VS 18.5%, p=0.003), CRP levels >3 mg/L (60.0% VS 42.0%), and ESR >21 mm/h (59.2% VS 42.0%). No statistical differences were found for age, educational level, marital status, history of smoking, history of drinking, BMI, psoriasis subtype, family history of psoriasis, BSA, uric acid, presence of hyperuricemia, TG, TC, HDL, LDL, and presence of hyperlipidemia between depression status. Significant differences between the anxiety and no anxiety groups were recognized for PASI and DLQI. Additionally, the anxiety group had more percentage of PASI ≥10 (36.8% VS 19.4%, p=0.037), BSA ≥10 (62.1% VS 47.9%, p=0.031) and DLQI ≥10 (60.0% VS 42.0%, p=0.003) than the no anxiety group. Other variables showed a similar trend in the anxiety and no anxiety group (Table 3). Further logistic analysis suggested that only DIQI was associated with the increased risk of anxiety (Table S1).
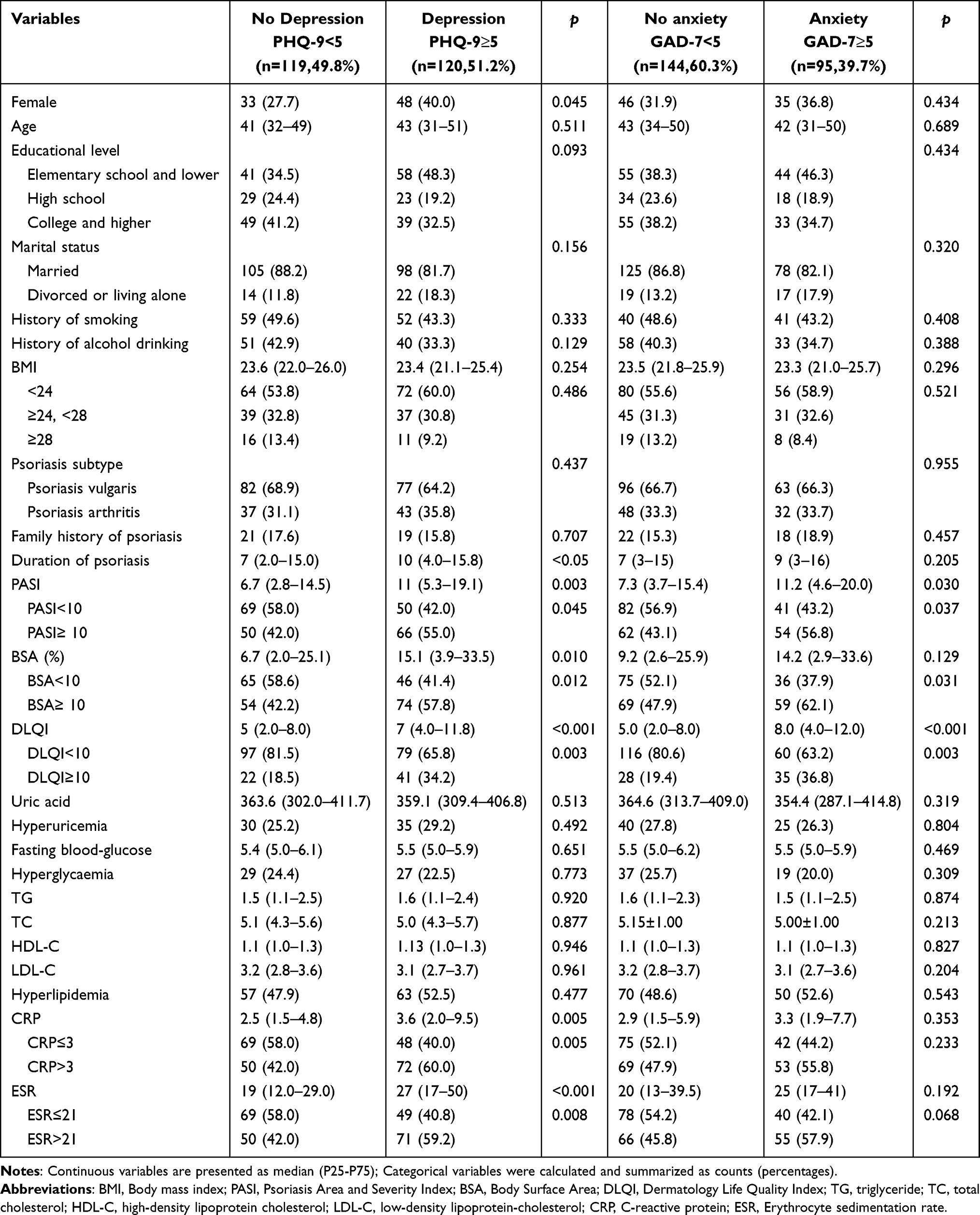 |
Table 3 Comparison of Demographics, Disease Characteristics, and Laboratory Parameters in Psoriasis with Regard to Depression and Anxiety |
Elevated CRP and ESR Were the Risk Factor for Depression in Psoriasis
Furthermore, to investigate the association between elevated CRP and ESR and depression among psoriasis, the above-mentioned significant variables were selected to perform logistic regressions with adjustments of sex, duration of psoriasis, PASI, and DLQI. As we expected, high CRP level (CRP>3 mg/L: AOR =2.049; 95% CI = 1.190–3.527) was the strongest factor correlated with depression. In addition, to a lesser extent, we identified elevated ESR (AOR =1.827; 95% CI = 1.078–3.096) as a significant factor associated with the depression of psoriasis (Table 4). Further subgroup analysis of those patients with psoriasis vulgaris shown the similar trend (Table 5). Due to the CRP and ESR levels being similar in the anxiety and no anxiety group, we did not perform the multivariable analyses to evaluate the association between CRP, ESR and anxiety.
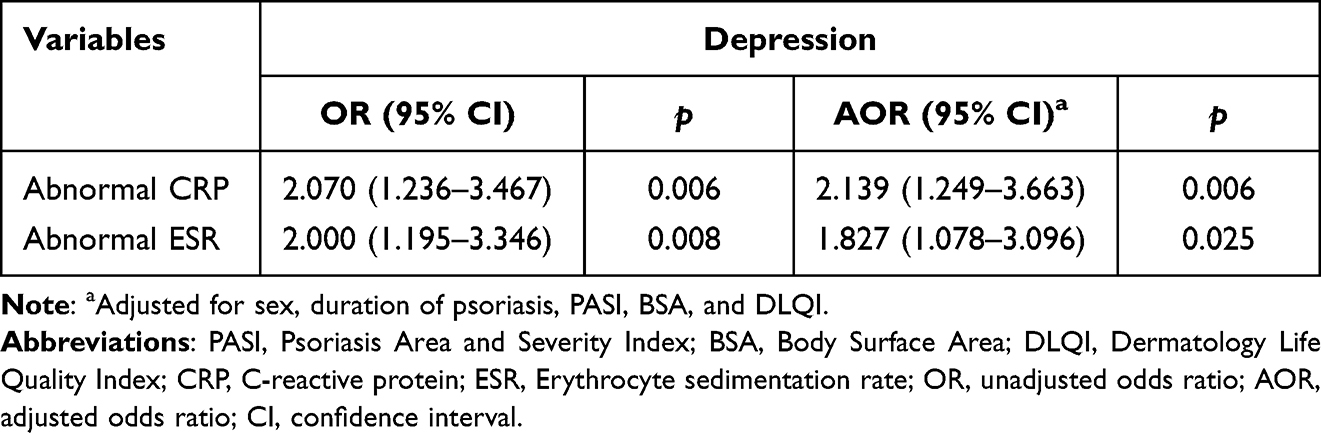 |
Table 4 Factors Associated with Depression in Psoriasis |
 |
Table 5 Subgroup Analysis for Factors Associated with Depression in Psoriasis Vulgaris (n=159) |
Diagnostic Efficacy of CRP or ESR on Depression in Psoriasis
ROC was conducted to determine the diagnostic efficacy of CRP or ESR on depression in psoriasis based on the maximal Youden’s index for sensitivity and specificity. The threshold for CRP was 3.24 in differentiating psoriasis cases in depression from those not (Figure 1A). The area under the curve (AUC) was 0.605 (95% CI = 0.533–0.677) with a sensitivity of 0.57 and specificity of 0.64. The cut-off value of ESR was calculated to be 26.5, and the AUC was 0.632 (95% CI = 0.562–0.703) with a sensitivity of 0.52 and specificity of 0.73 (Figure 1B). Thus, CRP and ESR had limited ability to distinguish between depression and no depression among psoriasis.
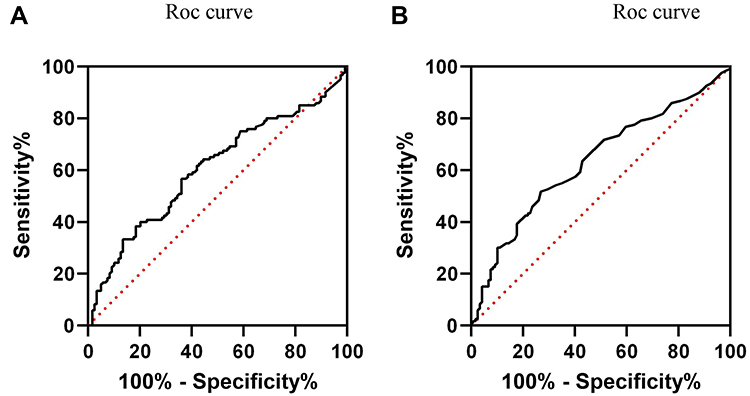 |
Figure 1 Depression cut-off points for the CRP and ESR scores. (A) The ROC analysis for the CRP threshold for depression. A CRP score of 3.24 best differentiated psoriasis patients in depression. (B) The ROC analysis for the ESR threshold for depression. A ESR score of 26.5 best differentiated psoriasis patients in depression. Abbreviations: CRP, C-reactive protein; ESR, Erythrocyte sedimentation rate; ROC, receiver–operator curve. |
Discussion
We conducted a cross-sectional case-controlled work and found a high rate of 50.2% for depression symptoms and 39.7% for anxiety symptoms in psoriasis. And the risk of depression and anxiety in psoriasis was 2.698 times and 3.123 times higher than in controls. Additionally, the elevated CRP level (>3 mg/L), to a lesser extent, and the elevated ESR level (>21 mm/h) were associated with the increased risk of depression in psoriasis. Both the CRP and ESR showed limited capability in distinguishing depression symptoms from those not in psoriasis patients.
Based on the PHQ-9 and GAD-7, validated structured questionnaires, the current study discovered that the percentage of depression and anxiety symptoms were 50.2% and 39.7% in psoriasis and 26.8% and 17.6% in matched non-psoriasis cases, respectively. Consequently, the prevalence of depression and anxiety were higher in participants with psoriasis relative to healthy cases. Recently, a nationwide population-based cross-sectional study also reported the prevalence of depression was more prevalent in psoriasis than in general individuals.27 Moreover, systemic reviews have been separately described in psoriatic patients up to 62% for depressive symptoms and 48% of for anxiety symptoms.4,5,7,8 The prevalence of both psychological disorders in psoriasis were slightly inconsistent with previous study, which could be explained in each case by methodological and sample factors. Additionally, psoriasis with an adjusted prevalence ratio of 2.698 (95% CI 1.690–4.306) regarding depression and 3.123 (95% CI 1.851–5.269) regarding anxiety compared with general population. Therefore, the relationship between depression and anxiety and psoriasis persists after adjusting lifestyle and demographic factors, which conforms previous study and systematic review.8,27 Nevertheless, the data reported in the current work was slightly different from previously reported in our team.6 The main reason for this discrepancy was the stricter definition conducted in the preceding research. Additionally, most of the participants experienced the Coronavirus disease 2019 epidemic, and mental health was more prevalent during this period.28,29 Collectively, future efforts ought to focus on improving screening for depression and anxiety comorbidity in psoriasis.11
We also showed here that the elevated serum level of CRP and ESR in psoriasis have statistically significant risk factors for developing depression. The present result supports and extends the previous findings that adults with high CRP levels were more likely to have depression symptoms than those with low CRP levels,12 as well as in psoriasis. There may be numerous explanations for the correlation between CRP and depression in psoriasis. Elevated inflammatory mediators such as CRP seems to be present in both psoriasis and depression. The emerging evidence presented in recent work indicated that the possible cause of the relationship between depression and psoriasis was the overlap of peripheral inflammatory biomarkers in the pathogenesis of psoriasis and those psychological disorders.12,30 Moreover, the elevated ESR increased the risk of depression amongst psoriasis in the current study. The correlation between the ESR and depression was controversial. Li et al showed that no correlation between ESR and depression in rheumatoid arthritis.31 While Bianciardi et al reported increase of ESR serum level in perinatal women and comorbid depression, which was in agreement with our findings.13 However, we found that there was no statistically significant relationship between ESR and symptoms of anxiety in psoriasis patients, which was consistent with previous work conducted in Cerebral Small Vessel Disease.32 Taken together, these findings suggest a close relationship between CRP and ESR level and depression in psoriasis, which may encourage clinicians to screen for depression and to control inflammatory levels may relieve depression in psoriasis patients.
Furthermore, we demonstrated that both CRP and ESR performed a limited diagnostic efficacy of depression in psoriasis. Previous studies reported the ability of CRP to discriminate depression status or depression from bipolar II disorder, whose AUC was higher than the present work.33–35 This discrepancy may be due to the sample size and the use of different questionnaires. Of note, to our knowledge, this was the first study to examine the diagnostic efficacy of ESR on psoriasis with mental disorder and exhibits a capability in differentiating depression. Both CRP and ESR are readily available, inexpensive, and reproducible, allowing us to identify depression in psoriatic patients in busy outpatient, intervene early, assess dynamically, and relieve patients’ disease burden.
The strength of this research was firstly represented the relationship between CRP and ESR and depression, anxiety among psoriasis. Beyond that, we performed a matched analysis in which we were able to determine whether psoriasis was significantly associated with depression and anxiety after adjusting for demographic characteristics (age, gender, education level, history of smoking and BMI). However, some limitations should not be ignored. Firstly, inflammation is not present in all cases of depression in the psoriasis setting and may not represent a causal relationship, given the cross-sectional nature of this study. Secondly, there might be a selection bias in more severely affected psoriasis patients seen in the large tertiary academic medical center. Secondly, because the participating center is a large tertiary dermatology hospital, there might be a potential selection bias in this study is represented by the fact that included patients were represented a more severe psoriasis. Given these limitations, future research would be encouraged to address these issues to generate stronger evidence.
Conclusion
In conclusion, the percentage of psoriasis subjects who have depression symptoms or anxiety symptoms was substantial, and the odds were much higher in psoriasis relative to matched healthy cases. Additionally, the current study demonstrated the significant relationship between elevated CRP, ESR levels and depression in psoriasis. We revealed that elevated CRP levels (CRP >3 mg/L) and elevated ESR levels (ESR >21 mm/h) were associated with depression among psoriasis. Besides, the discrimination capability of CPR and ESR on depression further indicates the extra value of inflammatory biomarkers in managing psoriasis.
Acknowledgments
We thank the patients who contributed clinical samples to the studies herein and the researchers who gathered and analyzed the data. Minjia Tan and Yan Luo are co-first authors for this study.
Funding
The work was granted by National Natural Science Foundation of China (82073447, 81974479, 81773329, 82003354).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet Lond Engl. 2021;397:1301–1315. doi:10.1016/S0140-6736(20)32549-6
2. Michalek IM, Loring B, John SM. A systematic review of worldwide epidemiology of psoriasis. J Eur Acad Dermatol Venereol. 2017;31:205–212. doi:10.1111/jdv.13854
3. Ding X, Wang T, Shen Y, et al. Prevalence of psoriasis in China: a population-based study in six cities. Eur J Dermatol. 2012;22:663–667. doi:10.1684/ejd.2012.1802
4. Bell KA, Balogh EA, Feldman SR. An update on the impact of depression on the treatment of psoriasis. Expert Opin Pharmacother. 2021;22:695–703. doi:10.1080/14656566.2020.1849141
5. Jalenques I, Bourlot F, Martinez E, et al. Prevalence and odds of anxiety disorders and anxiety symptoms in children and adults with psoriasis: systematic review and meta-analysis. Acta Derm Venereol. 2022;102:adv00769. doi:10.2340/actadv.v102.1386
6. Jing D, Xiao H, Shen M, et al. Association of psoriasis with anxiety and depression: a case-control study in Chinese patients. Front Med. 2021;8:771645. doi:10.3389/fmed.2021.771645
7. Dowlatshahi EA, Wakkee M, Arends LR, Nijsten T. The prevalence and odds of depressive symptoms and clinical depression in psoriasis patients: a systematic review and meta-analysis. J Invest Dermatol. 2014;134:1542–1551. doi:10.1038/jid.2013.508
8. Fleming P, Bai JW, Pratt M, et al. The prevalence of anxiety in patients with psoriasis: a systematic review of observational studies and clinical trials. J Eur Acad Dermatol Venereol. 2017;31:798–807. doi:10.1111/jdv.13891
9. Nadeem A, Ahmad SF, Al-Harbi NO, et al. IL-17A causes depression-like symptoms via NFκB and p38MAPK signaling pathways in mice: implications for psoriasis associated depression. Cytokine. 2017;97:14–24. doi:10.1016/j.cyto.2017.05.018
10. Elmets CA, Leonardi CL, Davis DMR, et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with awareness and attention to comorbidities. J Am Acad Dermatol. 2019;80(4):1073–1113. doi:10.1016/j.jaad.2018.11.058
11. Singh P, Silverberg JI. Underscreening of depression in U.S. outpatients with atopic dermatitis and psoriasis. Br J Dermatol. 2020;182:1057–1059. doi:10.1111/bjd.18629
12. Howren MB, Lamkin DM, Suls J. Associations of depression with C-reactive protein, IL-1, and IL-6: a meta-analysis. Psychosom Med. 2009;71:171–186. doi:10.1097/PSY.0b013e3181907c1b
13. Bianciardi E, Barone Y, Lo Serro V, et al. Inflammatory markers of perinatal depression in women with and without history of trauma. Riv Psichiatr. 2021;56:237–245. doi:10.1708/3681.36671
14. Liukkonen T, Räsänen P, Jokelainen J, et al. The association between anxiety and C-reactive protein (CRP) levels: results from the Northern Finland 1966 birth cohort study. Eur Psychiatry J Assoc Eur Psychiatr. 2011;26(6):363–369. doi:10.1016/j.eurpsy.2011.02.001
15. Helliwell PS, Taylor WJ. Classification and diagnostic criteria for psoriatic arthritis. Ann Rheum Dis. 2005;64(Suppl 2):ii3–8. doi:10.1136/ard.2004.032318
16. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–613. doi:10.1046/j.1525-1497.2001.016009606.x
17. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166:1092–1097. doi:10.1001/archinte.166.10.1092
18. Fredriksson T, Pettersson U. Severe psoriasis--oral therapy with a new retinoid. Dermatologica. 1978;157:238–244. doi:10.1159/000250839
19. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19:210–216. doi:10.1111/j.1365-2230.1994.tb01167.x
20. Ye X, Shu H-L, Feng X, et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire-9 (C-PHQ-9) in patients with psoriasis: a cross-sectional study. BMJ Open. 2020;10(7):e033211. doi:10.1136/bmjopen-2019-033211
21. Liu Z-W, Yu Y, Hu M, et al. PHQ-9 and PHQ-2 for screening depression in Chinese rural elderly. PLoS One. 2016;11(3):e0151042. doi:10.1371/journal.pone.0151042
22. Tong X, An D, McGonigal A, Park S-P, Zhou D. Validation of the Generalized Anxiety Disorder-7 (GAD-7) among Chinese people with epilepsy. Epilepsy Res. 2016;120:31–36. doi:10.1016/j.eplepsyres.2015.11.019
23. Felger JC, Li Z, Haroon E, et al. Inflammation is associated with decreased functional connectivity within corticostriatal reward circuitry in depression. Mol Psychiatry. 2016;21(10):1358–1365. doi:10.1038/mp.2015.168
24. Michos ED, McEvoy JW, Blumenthal RS, Jarcho JA. Lipid management for the prevention of atherosclerotic cardiovascular disease. N Engl J Med. 2019;381:1557–1567. doi:10.1056/NEJMra1806939
25. Chen CM. Overview of obesity in Mainland China. Obes Rev off J Int Assoc Study Obes. 2008;9(Suppl 1):14–21. doi:10.1111/j.1467-789X.2007.00433.x
26. Youden WJ. Index for rating diagnostic tests. Cancer. 1950;3:32–35. doi:10.1002/1097-0142(1950)3:1<32::AID-CNCR2820030106>3.0.CO;2-3
27. Hu -SC-S, Chen G-S, Tu H-P. Epidemiology of depression in patients with psoriasis: a nationwide population-based cross-sectional study. Acta Derm Venereol. 2019;99:530–538. doi:10.2340/00015555-3145
28. Liu S, Yang L, Zhang C, et al. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry. 2020;7(4):e17–e18. doi:10.1016/S2215-0366(20)30077-8
29. Zhai Y, Du X. Mental health care for international Chinese students affected by the COVID-19 outbreak. Lancet Psychiatry. 2020;7:e22. doi:10.1016/S2215-0366(20)30089-4
30. Hölsken S, Krefting F, Schedlowski M, Sondermann W. Common fundamentals of psoriasis and depression. Acta Derm Venereol. 2021;101:adv00609. doi:10.2340/actadv.v101.565
31. Li F, Ai W, Ye J, et al. Inflammatory markers and risk factors of RA patients with depression and application of different scales in judging depression. Clin Rheumatol. 2022;41:2309–2317. doi:10.1007/s10067-022-06174-3
32. Shan -L-L, Wang Y-L, Qiao T-C, et al. Association of serum interleukin-8 and serum amyloid A with anxiety symptoms in patients with cerebral small vessel disease. Front Neurol. 2022;13:938655. doi:10.3389/fneur.2022.938655
33. Tang C-Z, Zhang Y-L, Wang W-S, Li W-G, Shi J-P. Serum levels of high-sensitivity c-reactive protein at admission are more strongly associated with poststroke depression in acute ischemic stroke than homocysteine levels. Mol Neurobiol. 2016;53:2152–2160. doi:10.1007/s12035-015-9186-2
34. Chang HH, Wang T-Y, Lee IH, et al. C-reactive protein: a differential biomarker for major depressive disorder and bipolar II disorder. World J Biol Psychiatry. 2017;18:63–70. doi:10.3109/15622975.2016.1155746
35. Cheng L-S, Tu W-J, Shen Y, Zhang L-J, Ji K. Combination of high-sensitivity C-reactive protein and homocysteine predicts the post-stroke depression in patients with ischemic stroke. Mol Neurobiol. 2018;55:2952–2958. doi:10.1007/s12035-017-0549-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Anxiety and Depression in People with Eczema or Psoriasis: A Comparison of Associations in UK Biobank and Linked Primary Care Data
Matthewman J, Mansfield KE, Hayes JF, Adesanya EI, Smith CH, Roberts A, Langan SM, Henderson AD
Clinical Epidemiology 2023, 15:891-899
Published Date: 7 August 2023
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Mushrooms, Microdosing, and Mental Illness: The Effect of Psilocybin on Neurotransmitters, Neuroinflammation, and Neuroplasticity
Kinderlehrer DA
Neuropsychiatric Disease and Treatment 2025, 21:141-155
Published Date: 29 January 2025
Predictors of Quality of Life in Psoriasis Patients: Insights from a Cross-Sectional Study
Walniczek P, Ponikowska M, Kolarczyk EB, Spaleniak P, Mróz-Kijowska K, Czapla M, Uchmanowicz I
Psoriasis: Targets and Therapy 2025, 15:163-174
Published Date: 24 April 2025