Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Association of SCN1A Gene Polymorphisms with Sodium Valproate Resistance in Pediatric Epilepsy: A Retrospective Case-Control Study
Authors Wang H, Geng T, Deng N
Received 19 March 2025
Accepted for publication 25 July 2025
Published 7 August 2025 Volume 2025:21 Pages 1599—1609
DOI https://doi.org/10.2147/NDT.S529263
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Huiyu Wang,* Tingting Geng,* Na Deng
Department of Pediatric Intensive Care Unit, Shiyan Renmin Hospital, Hubei University of Medicine, Shiyan, Hubei Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Na Deng, Department of Pediatric Intensive Care Unit, Shiyan Renmin Hospital, Hubei University of Medicine, No. 39 Chaoyang Middle Road, Maojian District, Shiyan, Hubei Province, 442000, People’s Republic of China, Email [email protected]
Background: Epilepsy affects approximately 0.4– 0.7% of the Chinese population, with an estimated 20– 25% of patients developing resistance to antiepileptic drugs. Elucidating the genetic mechanisms underlying sodium valproate resistance could revolutionize personalized treatment strategies, particularly in pediatric epilepsy.
Objective: To explore the relationship between polymorphisms in the sodium channel α 1 subunit gene (SCN1A) and resistance to sodium valproate therapy in pediatric epilepsy patients.
Methods: A retrospective analysis included 89 pediatric patients with sodium valproate-resistant epilepsy (resistant group) and 89 patients responsive to sodium valproate (responder group), and 89 healthy controls. SCN1A gene polymorphisms were analyzed and compared among groups. Plasma valproate concentrations were evaluated across different genotypes. Multivariate logistic regression was performed to identify factors associated with drug resistance.
Results: Significant differences in SCN1A genotype distributions were observed among groups for five foci: rs166859148, rs166894396, rs166848482, rs166915162, and rs166870333-335 (P < 0.05). Mutations at these loci were significantly correlated with sodium valproate resistance (P < 0.05). Additionally, patients with mutant genotypes at rs166915162 and rs166870333-335 exhibited lower plasma valproate concentrations compared to those with wild-type alleles (P < 0.05). The rs166870333-335 variant was also significantly associated with generalized seizure types in drug-resistant patients (P < 0.05).
Conclusion: Mutation in the SCN1A gene, specifically rs166859148, rs166894396, rs166848482, rs166915162, rs166870333-335, may contribute to resistance to sodium valproate in pediatric epilepsy. Mutations in rs166915162 and rs166870333-335 were associated with reduced plasma levels of sodium valproate, while the rs166870333-335 mutation is linked to generalized seizure types in patients with drug-resistant epilepsy.
Keywords: SCN1A gene, sodium valproate, children, epilepsy, drug resistance, blood drug concentration
Introduction
Epilepsy is a common neurological disorder with a prevalence rate of 0.4% to 0.7% among the Chinese population and has been identified by the World Health Organization as one of the five major neuropsychiatric diseases that require global prevention and treatment initiatives.1,2 Despite therapeutic advances, drug resistance remains a significant clinical challenge, affecting an estimated 10% to 20% of children and 20% to 25% of adults with epilepsy.3–5
Recent advances in multi-omics technologies have transformed our understanding of epilepsy pathogenesis and drug resistance. Genomic studies have revealed mutations in ion channel genes such as sodium channel α1 subunit genes SCN1A and SCN2A that contribute to variability in therapeutic responses. Likewise, transcriptomic analyses reveal dysregulated neuronal excitability pathways in drug-resistant cases.6,7 These findings highlight the importance of molecular profiling for predicting treatment outcomes and developing personalized therapeutic strategies.
Voltage-gated sodium channels play a central role in regulating neuronal excitability, particularly the NaV1.1 subtype that is encoded by SCN1A. Loss-of-function mutations in SCN1A have been shown to impair inhibitory interneuron firing, thereby disrupting the excitatory/inhibitory imbalance and increasing susceptibility to seizures.8
Sodium valproate is a first-line, broad-spectrum antiepileptic drug that is used as both monotherapy and adjuvant therapy across various seizure types. However, clinical experience has revealed significant inter-individual differences in response to sodium valproate. The mechanisms driving this variability are not yet fully understood. While polymorphisms in genes such as ABCC2 (ATP-binding cassette subfamily C member 2) and MDR1 (multidrug resistance gene 1) are closely related to its occurrence and have been implicated in antiepileptic drug resistance, these factors do not fully account for all cases of sodium valproate resistance.9,10
The SCN1A gene, which is located on chromosome 2q24.3, consists of 26 exons and encodes the α1 subunit of voltage-gated sodium channel. It is closely associated with epilepsy syndromes such as generalized epilepsy with febrile seizures plus (GEFS+) and Dravet syndrome. However, its role in sodium valproate resistance, especially in childhood epilepsy, remains largely underexplored.11,12
Recent advances in precision medicine suggest that SCN1A gene polymorphisms may influence both seizure susceptibility but also antiepileptic drug responsiveness. These polymorphisms may alter sodium channel structure and function, thereby modulating the binding and efficacy of antiepileptic drugs. For instance, the rs3812718 variant has been associated with differential responses to carbamazepine, indicating that SCN1A polymorphisms may exert drug-specific pharmacogenetic effects.13,14
Despite all these insights, studies on the relationship between SCN1A polymorphisms and sodium valproate resistance remain limited, particularly among Chinese pediatric populations. To address this gap, this study investigates five previously underexplored SCN1A single nucleotide polymorphisms (SNPs) polymorphisms (rs166859148, rs166894396, rs166848482, rs166915162, and rs166870333-335). We examine their associations with plasma sodium valproate concentrations and drug-resistance phenotypes, with the goal of generating clinically relevant personalized treatment approaches in pediatric epilepsy (Figure 1).
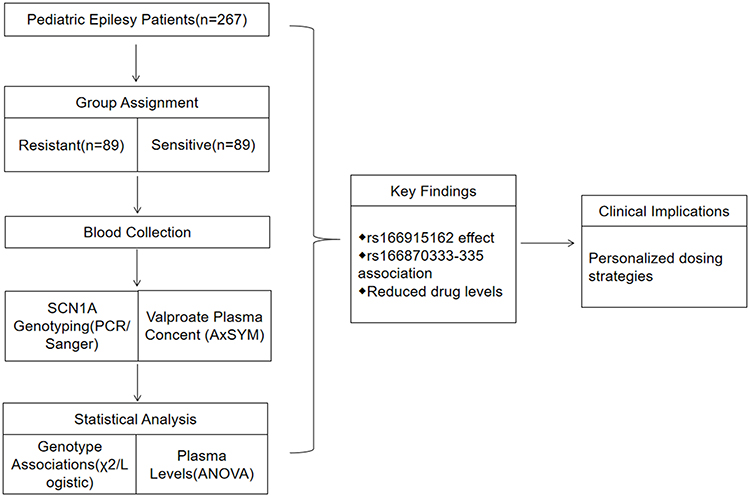 |
Figure 1 Workflow. |
Data and Methods
General Data
This retrospective study included 89 pediatric patients with sodium valproate-resistant epilepsy (drug-resistant group) and 89 patients who responded to sodium valproate treatment (responder group), all of whom were admitted to our hospital between January 2018 and February 2020. In addition, 89 healthy children were selected during the same period to serve as the control group.
Participants were eligible for inclusion if they were between 6 and 18 years of age, had been diagnosed with epilepsy based on the standard diagnostic criteria,15 and were treated with an anti-epileptic therapeutic regimen containing sodium valproate. The exclusion criteria included the presence of cerebral space-occupying lesions, hepatic or renal dysfunction, inherited metabolic disorders, or poor medication adherence.
Methods
Data Collection
Demographic and clinical data were collected for all participants, including age, disease duration, body mass, gender, ethnicity, seizure type, etiology, types of anti-epileptic drugs used, and permanent residence. Seizure types were classified according to the International League Against Epilepsy (ILAE) 2017 position paper, Operational classification of seizure types.16 Based on power calculations derived from previous pharmacogenetic studies (OR = 2.5, α = 0.05, power = 80%), a sample size of 89 participants per group was deemed sufficient to detect statistically meaningful differences.
Administration of Sodium Valproate and Monitoring of Plasma Concentrations
Extended-release sodium valproate tablets (Sanofi (Hangzhou) Pharmaceutical Co., Ltd.; National Medical Approval Number H20010595) were administered orally at a standard dose of 30 mg/kg/day.
Patients in the responder group were defined as those who had remained seizure-free for more than one year after anti-epileptic treatment, or whose post-treatment seizure-free period exceeded the longest pre-treatment interval. In contrast, the drug-resistant group was comprised of patients who, despite receiving standard antiepileptic treatment, with plasma valproate concentrations within the therapeutic range or at maximum tolerated dose, continued to experience uncontrolled seizures.15
After confirming each patient’s treatment classification (responder or drug-resistant), all participants continued sodium valproate administration for an additional five consecutive days. On the fifth day, 5 mL of blood was collected from the median cubital vein 30 minutes before the next scheduled dose. Plasma sodium valproate concentrations were measured using the Abbott AxSYM fully automated immunoassay system.
SCN1A Gene Polymorphism Detection
Peripheral blood samples were collected from all participants, and genomic DNA was extracted using the QIAamp DNA Blood Mini Kit (Qiagen, Germany), following the manufacturer’s protocol. Target regions of the SCN1A gene were amplified using the polymerase chain reaction (PCR), followed by Sanger sequencing for variant detection. The PCR primers were synthesized by Beijing TsingKe Biotech. Sequencing data were analyzed using DNASTAR software to identify and compare SCN1A gene polymorphisms across samples.
Outcome Measures
The primary and secondary outcome measures of this study were as follows:
(1) Comparison of clinical characteristics among the drug-resistant group, responder group, and healthy controls.
(2) Comparison of SCN1A gene polymorphism frequencies among the three groups.
(3) Comparison of plasma sodium valproate concentrations across different SCN1A genotypes in pediatric epilepsy patients.
(4) Analysis of factors associated with sodium valproate resistance in children with epilepsy using multivariate statistical methods.
(5) Comparison of SCN1A gene polymorphism distributions among sodium valproate-resistant children with different types of epileptic seizures.
Statistical Analysis
All statistical analyses were conducted using SPSS version 22.0 software. Continuous variables with normal distribution were expressed as mean ± standard deviation and compared using one-way analysis of variance (ANOVA), followed by least significant difference (LSD) post-hoc tests for multiple comparisons. The Kruskal–Wallis test was applied for non-normally distributed data. Categorical variables were presented as frequencies and percentages (%) and analyzed using chi-square (χ²) tests or Fisher’s exact tests when appropriate. Genotype distributions were assessed for Hardy-Weinberg equilibrium using χ²-tests. The associations between SCN1A polymorphisms and valproate resistance were evaluated through multivariate logistic regression analysis. The results were expressed as odds ratios (ORs) with 95% confidence intervals (CIs). The model was adjusted for potential confounding factors, including age, sex, and seizure type.
Plasma valproate concentrations across different SCN1A genotypes were compared using independent t-tests. For all statistical analyses, a two-tailed P-value <0.05 was considered statistically significant. Effect sizes were accompanied by 95% CIs, and assumptions of homogeneity of variance as verified using Levene’s test.
Results
Comparison of General Data Among the Three Groups
The three groups consisted of individuals aged between 6 and 18 years. There were no statistically significant differences among the groups in terms of age, duration of illness, body mass, gender, ethnicity, seizure type, etiology, types of antiepileptic drugs used, or place of residence (P > 0.05) (Table 1).
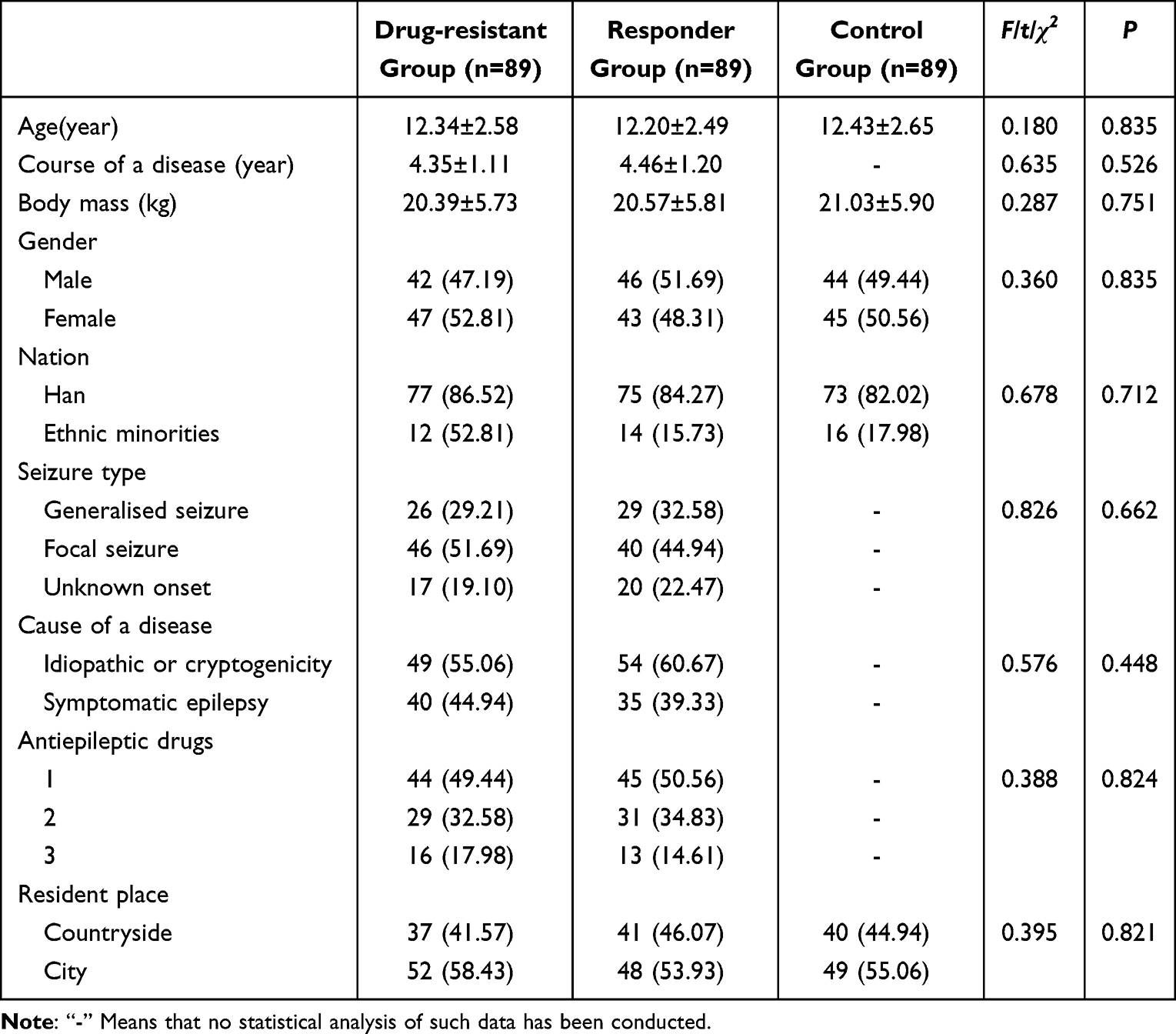 |
Table 1 Comparison of General Data Among Three Groups |
Comparison of SCN1A Gene Polymorphisms Among the Three Groups
The distribution of genotype frequencies in all three groups conformed to Hardy-Weinberg equilibrium (P > 0.05), indicating appropriate population representativeness for genetic analysis. Statistically significant differences were observed in the distribution of SCN1A genotypes at the following loci: rs166859148 (c.4118T>G), rs166894396 (c.2752C>T), rs166848482 (c.5270G>A), rs166915162 (c.301C>T), and rs166870333-335 (c.3879G>T) among the three groups (P < 0.05). In contrast, no significant differences were observed in the distribution of genotypes for rs166893018 (c.969T>G), rs166894396 (c.2294C>T), rs166894641 (c.2591T>G), rs166908376 (c.817C>G), 166900385 (c.1837C>T), and rs166848831 (c.4921G>T) (P > 0.05) (Table 2).
 |
Table 2 Comparison of SCN1A Gene Polymorphisms Among Three Groups |
Analysis of Factors Influencing Sodium Valproate Resistance in Childhood Epilepsy
Mutations in the SCN1A gene rs166859148 (c.4118T>G), rs166894396 (c.2752C>T), rs166848482 (c.5270G>A), rs166915162 (c.301C>T), and rs166870333-335 (c.3879G>T) were significantly associated with resistance to sodium valproate resistance in children with epilepsy (P < 0.05) (Table 3).
 |
Table 3 Logistic Regression Equation Analysis of Factors Affecting Drug Resistance of Sodium Valproate in Children with Epilepsy |
Comparison of Sodium Valproate Plasma Concentrations Among Children with Different SCN1A Genotypes
No statistically significant differences in plasma sodium valproate concentrations were observed between wild-type and mutant genotypes for the following SCN1A loci: rs166859148 (c.4118T>G), rs166893018 (c.969T>G), rs166894396 (c.2752C>T), rs166894396 (c.2294C>T), rs166894641 (c.2591T>G), rs166848482 (c.5270G>A), rs166908376 (c.817C>G), rs166900385 (c.1837C>T), and rs166848831 (c.4921G>T) (P > 0.05). However, the plasma sodium valproate concentrations were lower in individuals with mutant genotypes at rs166915162 (c.301C>T) and rs166870333-335 (c.3879G>T) compared to those with the corresponding wild-type genotypes (P < 0.05) (Table 4).
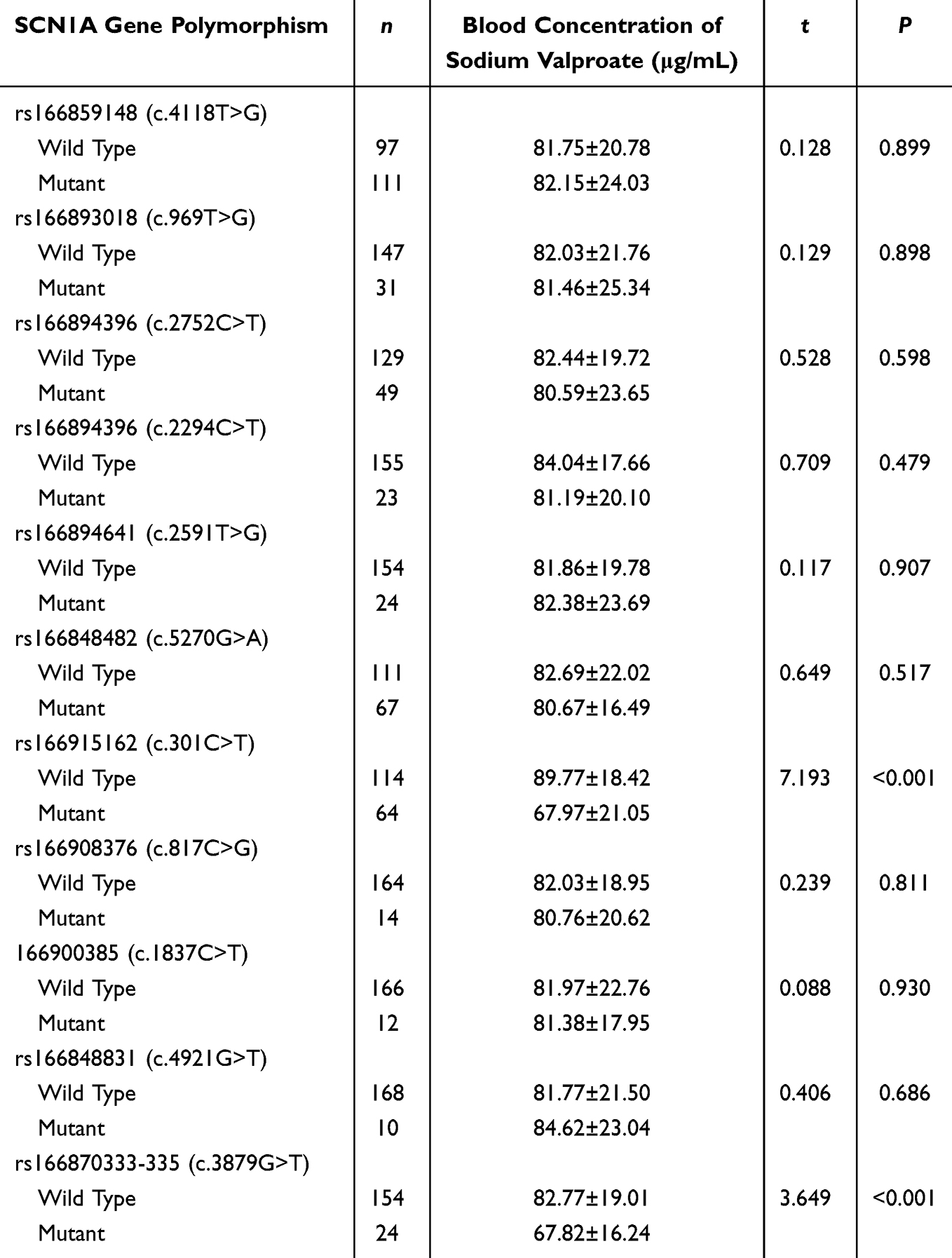 |
Table 4 Comparison of Sodium Valproate Plasma Concentrations Among Children With Different SCN1A Genotypes |
Comparison of SCN1A Gene Polymorphisms Among Sodium Valproate-Resistant Children with Different Types of Epileptic Seizures
No statistically significant differences were observed in the distribution of genotypes at the following SCN1A loci among sodium valproate-resistant children with different types of epileptic seizures: rs166859148 (c.4118T>G), rs166893018 (c.969T>G), rs166894396 (c.2752C>T), rs166894396 (c.2294C>T), rs166894641 (c.2591T>G), rs166848482 (c.5270G>A), rs166915162 (c.301C>T), rs166908376 (c.817C>G), rs166900385 (c.1837C>T), and rs166848831 (c.4921G>T) (P > 0.05). However, a statistically significant difference was found in the distribution of genotypes for SCN1A s166870333-335 (c.3879G>T). Children with generalized seizures exhibited a lower frequency of the GG genotype and a higher frequency of the GT and TT genotypes compared to those with focal seizures or seizures of unknown onset (P < 0.05) (Table 5).
 |
Table 5 Comparison of SCN1A Gene Polymorphisms Among Sodium Valproate-Resistant Children With Different Types of Epileptic Seizures |
Discussion
Voltage-gated sodium channels are key pharmacological targets in antiepileptic treatment and represent a central focus in drug development research.17 In this study, significant differences were observed in the distribution of SCN1A gene mutations specifically rs166859148 (c.4118T>G), rs166894396 (c.2752C>T), rs166848482 (c.5270G>A), rs166915162 (c.301C>T), and rs166870333-335 (c.3879G>T), across the drug-resistant, responder, and control groups. Logistic regression analysis further confirmed that mutations at these loci are strongly associated with sodium valproate resistance in pediatric epilepsy. This suggests that specific SCN1A polymorphisms may contribute to pharmacoresistance.
The α1 subunit, encoded by SCN1A, is the primary structural and functional component of voltage-gated sodium channels in the central nervous system.18,19 Anti-epileptic drugs such as sodium valproate typically exert their effects by interacting with these channels, thereby modulating channel function, reducing peak sodium currents, stabilizing membrane potential, and suppressing high-frequency neuronal discharges.17,20,21 Mutations in SCN1A may alter channel conformation and kinetics, potentially disrupting drug-channel interactions and thereby reducing therapeutic efficacy. While these mechanisms offer a plausible explanation for the observed drug resistance, they remain hypothetical and require validation through additional functional studies.22,23
Sodium valproate is a widely used broad-spectrum antiepileptic drug, administered either as monotherapy or in combination with other agents for the treatment of different types of epileptic seizures. It has a half-life ranging from 8 to 20 hours and typically achieves a steady-state plasma concentration of 50 to 100 µg/mL. However, substantial inter-individual pharmacokinetic variability has been observed in clinical practice, leading to a nonlinear relationship between the administered dose and resulting plasma levels. Subtherapeutic plasma concentrations may lead to ineffective seizure control, whereas excessively high plasma concentrations increase the risk of adverse effects.24–26
In this study, carriers of SCN1A mutation at rs166915162 (c.301C>T) and rs166870333-335 (c.3879G>T) exhibited significantly lower plasma valproate concentrations compared to those with wild-type genotypes. The findings suggest that these mutations may contribute to drug resistance by reducing systemic drug availability. While the underlying mechanism remains unclear, it is hypothesized that these mutations may impair sodium valproate’s binding efficiency to voltage-gated sodium channels in the cerebral tissue of the brain. This indirectly affects systemic concentration levels.27,28 Consequently, identifying SCN1A polymorphism status before initiating treatment could inform personalized dosing strategies. In patients carrying the rs166915162 (c.301C>T) and rs166870333-335 (c.3879G>T) variants, cautious dosage escalation, guided by therapeutic drug monitoring, may improve clinical outcomes while minimizing the risk of toxicity.
Beyond mechanistic insights, the findings of this study offer meaningful translational potential for the clinical management of pediatric epilepsy. The strong association between specific SCN1A variants (rs166915162-CT/TT and rs166870333-335-GT/TT) and sodium valproate resistance (OR = 2.9–4.9) supports the development of a clinical decision-making algorithm.
First, pre-treatment genotyping could be employed to stratify patients into high-risk and standard-risk groups. Those with high-risk genotypes may benefit from early consideration of alternative first-line agents, particularly in cases of generalized seizures, where rs166870333-335 variants were associated with a 3.2-fold higher prevalence of drug resistance. Second, therapeutic drug monitoring protocols may require genotype-adjusted plasma concentration targets. Carriers of these variants demonstrated 24–32% lower plasma sodium valproate levels at standard doses. This emphasizes the need for individualized dosing. Implementation considerations include establishing cost-effectiveness thresholds for routine genetic screening (estimated at $50-$75/test) and validating resistance-related cutoffs across diverse populations. These are objectives that are currently being addressed in our ongoing multicenter trial. These precision medicine strategies have the potential to reduce the typical 6–9 month “trial-and-error” period for identifying effective treatment in drug-resistant cases by an estimated 40–60%, all while maintaining safety margins.
According to the International League Against Epilepsy (ILAE) guidelines, epileptic seizures are broadly categorized into generalized, focal (previously called “localized”), and seizures of unknown onset types.29 Numerous SCN1A gene mutations have been identified in children with Dravet syndrome, substantially expanding the spectrum of known pathogenic variants. The resulting phenotypes are strongly correlated with the degree of SCN1A dysfunction. Mild impairments may lead to isolated seizures, whereas moderate to severe functional loss is often associated with generalized epilepsy accompanied by febrile convulsions. Truncating mutations that eliminate SCN1A function can cause severe neurological disorders, including Dravet syndrome.30–32
Despite this established relationship, limited evidence exists regarding the association between SCN1A variants and the seizure type classification of epileptic children who are resistant to sodium valproate. In the present study, significant differences were observed in the genotype distribution of the SCN1A rs166870333-335 (c.3879G>T) among children with sodium valproate-resistant epilepsy. Specifically, the GG genotype was less prevalent in patients with generalized seizures than in those with focal or unknown onset seizures, whereas the GT and TT genotypes were more frequently observed. This suggests a potential association between the rs166870333-335 (c.3879G>T) and generalized seizure phenotypes. Although these findings offer novel insights, they should be interpreted with caution. The genotype–phenotype correlations reported here have not yet been corroborated by other studies, highlighting the need for further investigation in larger, ethnically diverse cohorts.
Several limitations of this study should be acknowledged. First, the single-ethnicity design, which was exclusively focused on the Chinese Han population, may limit the generalizability of findings due to their inter-population variability in allele frequencies. Second, the observed pharmacokinetic differences require mechanistic validation through complementary techniques such as electrophysiological assays and metabolomic profiling. Third, potential confounding factors like medication adherence, were not directly measured and may have influenced treatment outcomes. Fourth, the exclusive focus on SCN1A polymorphisms does not account for possible polygenic contributions from other pharmacogenetically relevant genes.
Despite these constraints, the strong observed effect sizes (eg, OR = 4.88 for rs166870333-335) provide compelling preliminary justification for clinical relevance, particularly in high-risk subgroups. Ongoing multi-center studies that involve ethnically diverse cohorts and functional characterization approaches are underway to address these gaps and further refine the proposed precision medicine framework.
Conclusion
Our findings demonstrate that SCN1A gene mutations (rs166859148, rs166894396, rs166848482, rs166915162, and rs166870333-335) are significantly associated with sodium valproate resistance in pediatric epilepsy. Notably, carriers of the rs166915162 and rs166870333-335 variants exhibited reduced plasma concentrations of sodium valproate, suggesting a plausible pharmacokinetic mechanism underlying diminished therapeutic efficacy due to subtherapeutic drug levels. Furthermore, the rs166870333-335 variant was specifically associated with generalized seizure phenotypes among drug-resistant patients, thereby reinforcing its potential clinical significance. Collectively, these results highlight the utility of SCN1A genotyping to support personalized dosing strategies and enable early identification of patients at elevated risk for treatment failure.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
All procedures involving human participants were conducted in accordance with the ethical standards of the national research committee and with the 1964 Declaration of Helsinki as well as its later amendments or comparable ethical standards. The study was approved by the Ethics Committee of Shiyan Renmin Hospital. Legal guardians of all pediatric participants received comprehensive study information and provided written consent.
Funding
This research received no external funding.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Zhu X, Li X, Zhang T, et al. Risk factors for valproic acid-induced hyperammonaemia in Chinese paediatric patients with epilepsy. Basic Clin Pharmacol Toxicol. 2018;123(5):628–634. doi:10.1111/bcpt.13049
2. Miao P, Feng J, Guo Y, et al. Genotype and phenotype analysis using an epilepsy-associated gene panel in Chinese pediatric epilepsy patients. Clin Genet. 2018;94(6):512–520. doi:10.1111/cge.13441
3. Xu S, Liu L, Chen Y, et al. Population pharmacokinetics of lamotrigine co-administered with valproic acid in Chinese epileptic children using nonlinear mixed effects modeling. Eur J Clin Pharmacol. 2018;74(5):583–591. doi:10.1007/s00228-018-2414-8
4. Ni G, Qin J, Chen Z, et al. Associations between genetic variation in one-carbon metabolism and leukocyte DNA methylation in valproate-treated patients with epilepsy. Clin Nutr. 2018;37(1):308–312. doi:10.1016/j.clnu.2017.01.004
5. Feng W, Mei S, Han J, et al. Lack of association between valproic acid response and polymorphisms of its metabolism, transport, and receptor genes in children with focal seizures. Neurol Sci. 2019;40(3):523–528. doi:10.1007/s10072-018-3681-y
6. Du Y, Li R, Fu D, et al. Multi-omics technologies and molecular biomarkers in brain tumor-related epilepsy. CNS Neurosci Ther. 2024;30(4):e14717. doi:10.1111/cns.14717
7. Du Y, Li Z, Liu Z, et al. Nonrandom occurrence of multiple de novo coding variants in a proband indicates the existence of an oligogenic model in autism. Genet Med. 2020;22(1):170–180. doi:10.1038/s41436-019-0610-2
8. Mantegazza M, Curia G, Biagini G, Ragsdale DS, Avoli M. Voltage-gated sodium channels as therapeutic targets in epilepsy and other neurological disorders. Lancet Neurol. 2010;9(4):413–424. doi:10.1016/S1474-4422(10)70059-4
9. Li G, Yin XJ, Li Y, et al. Association of MDR1 gene polymorphisms with refractory epilepsy in children. Chinese Journal of Medical Genetics. 2019;36(11):1073–1076. doi:10.3760/cma.j.issn.1003-9406.2019.11.004
10. Yang YL, Hu X, Shu D, et al. The role of ABCC2 gene in drug-resistant epilepsy. Journal of Chinese Physician. 2018;20(6):836–838, 843.
11. Yang ZX, Mei SY, Chen GH, et al. Deletion and repetition of SCN1A gene segment in children with Dravet syndrome. Journal of Chinese Practical Diagnosis and Therapy. 2019;33(12):1185–1187.
12. Ma QL, Wang B, Chen GF, et al. Association between SCN1A rs3812718 polymorphism and generalized epilepsy with febrile seizures plus. Chinese Journal of Contemporary Pediatrics. 2018;20(2):130–133. doi:10.7499/j.issn.1008-8830.2018.02.010
13. Zhang X, Liu J, Ye J. Association between SCN1A polymorphism and carbamazepine responsiveness in epilepsy: a meta-analysis. Epilepsy Res. 2021;176:106627. doi:10.1016/j.eplepsyres.2021.106627
14. Zhao GX, Zhang Z, Cai WK, et al. Associations between CYP3A4, CYP3A5 and SCN1A polymorphisms and carbamazepine metabolism in epilepsy: a meta-analysis. Epilepsy Res. 2021;173:106615. doi:10.1016/j.eplepsyres.2021.106615
15. China anti-epilepsy association. Guide to Clinical Diagnosis and Treatment Epilepsy Volume. Beijing: The People’s Health Press Co. Ltd; 2015:8–17.
16. Fisher RS, Helen Cross J, French JA, et al. Operational classification of seizure types by the international league against epilepsy: position paper of the ILAE commission for classification and terminology. Epilepsia. 2017;58(4):522–530. doi:10.1111/epi.13670
17. Chilcott E, Díaz JA, Bertram C, et al. Genetic therapeutic advancements for Dravet syndrome. Epilepsy Behav. 2022;132:108741. doi:10.1016/j.yebeh.2022.108741
18. Ding J, Li X, Tian H, et al. SCN1A mutation-beyond Dravet syndrome: a systematic review and narrative synthesis. Front Neurol. 2021;12:743726. doi:10.3389/fneur.2021.743726
19. Brunklaus A, Pérez-Palma E, Ghanty I, et al. Development and validation of a prediction model for early diagnosis of SCN1A-related epilepsies. Neurology. 2022;98(11):e1163–e1174. doi:10.1212/WNL.0000000000200028
20. Sills GJ, Rogawski MA. Mechanisms of action of currently used antiseizure drugs. Neuropharmacology. 2020;168:107966. doi:10.1016/j.neuropharm.2020.107966
21. Gao K, Lin Z, Wen S, et al. Potassium channels and epilepsy. Acta Neurol Scand. 2022;146(6):699–707. doi:10.1111/ane.13695
22. Van Hugte EJH, Lewerissa EI, Wu KM, et al. SCN1A-deficient excitatory neuronal networks display mutation-specific phenotypes. Brain. 2023;146(12):5153–5167. doi:10.1093/brain/awad245
23. Clatot J, Parthasarathy S, Cohen S, et al. SCN1A gain-of-function mutation causing an early onset epileptic encephalopathy. Epilepsia. 2023;64(5):1318–1330. doi:10.1111/epi.17444
24. Tan S, Js N, Tang C, et al. Subcutaneous sodium valproate in palliative care: a systematic review. Palliat Med. 2024;38(4):492–497. doi:10.1177/02692163241234597
25. Crespo Pimentel B, Kuchukhidze G, Xiao F, et al. Sodium valproate is associated with cortical thinning of disease-specific areas in juvenile myoclonic epilepsy. J Neurol Neurosurg Psychiatry. 2024;96(1):11–14. doi:10.1136/jnnp-2024-333703
26. Burstein AH, Cox DS, Mistry B, Eddington ND. Phenytoin pharmacokinetics following oral administration of phenytoin suspension and fosphenytoin solution to rats. Epilepsy Res. 1999;34(2–3):129–133. doi:10.1016/S0920-1211(98)00107-7
27. Haerian BS, Baum L, Tan HJ, et al. SCN1A IVS5N+5 polymorphism and response to sodium valproate: a multicenter study. Pharmacogenomics. 2012;13(13):1477–1485. doi:10.2217/pgs.12.127
28. Feng W, Mei S, Zhu L, et al. Effects of UGT2B7, SCN1A and CYP3A4 on the therapeutic response of sodium valproate treatment in children with generalized seizures. Seizure. 2018;58:96–100. doi:10.1016/j.seizure.2018.04.006
29. Duan Y, Zhang Z, Zhao X, et al. Validation of different predictive scoring scales in patients with new-onset epileptic seizures or epilepsy related to neuronal surface antibody-mediated autoimmune encephalitis. Epilepsy Behav. 2023;147:109403. doi:10.1016/j.yebeh.2023.109403
30. Yu L, Meng Y, Tang B, et al. Influence of SCN1A intronic mutations in mRNA splicing and relation of mRNA splicing changes with phenotype in febrile seizures related epilepsy. Chinese Journal of Neuromedicine. 2018;17(8):757–764.
31. Zhang H, Hd C, Zy C, et al. Localization of pathogenic gene and mutation detection of GEFS+ gene in children with Dravet syndrome Journal of Clinical Pediatrics. 2019;37(9):665–668.
32. Gs W, Yf Z, Li S, et al. Screening of pathogenic genes and analysis of early medication in two families with Dravet syndrome Zhejiang Medical Journal. 2019;41(4):373–376.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fracture Rates in Children with Cerebral Palsy: A Danish, Nationwide Register-Based Study
Granild-Jensen JB, Pedersen AB, Kristiansen EB, Langdahl B, Møller-Madsen B, Søndergaard C, Farholt S, Vestergaard ET, Rackauskaite G
Clinical Epidemiology 2022, 14:1405-1414
Published Date: 22 November 2022
Poor Seizure Control Among Children Attending a Tertiary Hospital in South Western Uganda – A Retrospective Study
Namusisi J, Kyoyagala S, Nantongo J, Kyewalyanga M, Sabiiti S, Murorunkwere A, Najjuma JN, Nakibuuka J, Kaddumukasa M, Sajatovic M, Kalubi P
International Journal of General Medicine 2023, 16:895-904
Published Date: 7 March 2023
Clinical Characteristics, Treatment Outcome and Associated Factors of Epilepsy Among Children at Hospitals of North-West Ethiopia
Nasir M, Abebaw E, Ahmed M, Ketema DB
Pediatric Health, Medicine and Therapeutics 2023, 14:385-404
Published Date: 31 October 2023
Distribution of Pathogenic Bacteria and Changes in Drug Resistance of Urinary Tract Infections in Children in Southwest China, 2020–2024
You Z, Huang X, Liu X, Yu H, Long S
Infection and Drug Resistance 2026, 19:581416
Published Date: 24 January 2026