Back to Journals » Infection and Drug Resistance » Volume 19
Distribution of Pathogenic Bacteria and Changes in Drug Resistance of Urinary Tract Infections in Children in Southwest China, 2020–2024
Authors You Z ![]() , Huang X, Liu X, Yu H, Long S
, Huang X, Liu X, Yu H, Long S
Received 13 November 2025
Accepted for publication 16 January 2026
Published 24 January 2026 Volume 2026:19 581416
DOI https://doi.org/10.2147/IDR.S581416
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hazrat Bilal
Zhuorui You,1 Xiangning Huang,2 Xin Liu,2 Hua Yu,2 Shanshan Long2
1School of Medicine, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 2Department of Laboratory Medicine, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, 610072, People’s Republic of China
Correspondence: Shanshan Long, Email [email protected] Hua Yu, Email [email protected]
Objective: Urinary tract infection (UTI) is a major health concern in pediatric populations. By analysing temporal changes in pathogen distribution and antimicrobial resistance among children with UTIs in Southwest China from 2020 to 2024, we aim to provide a robust scientific basis for the empirical antibiotic therapy in this region.
Methods: We retrospectively analyzed non-duplicate pathogens isolated from urine specimens and their antimicrobial susceptibility results in 6598 children (≤ 14 years old) diagnosed with UTIs in southwest China from 2020 to 2024. These results were interpreted according to the M100 guidelines of the American Clinical and Laboratory Standards Institute (CLSI) and analysed using WHONET 5.6 software.
Results: A total of 7831 strains of pathogenic bacteria were detected, of which 60.1% were gram-negative and 39.9% were gram-positive. The top five bacteria detected were Escherichia coli (37.8%), Enterococcus faecium (26.3%), Enterococcus faecalis (7.5%), Klebsiella pneumoniae (6.9%) and Pseudomonas aeruginosa (2.5%). E. coli showed less than 10% resistance to piperacillin/tazobactam, cefoperazone/sulbactam, amikacin and nitrofurantoin, with resistance to quinolones ranging from 31.3% to 51.5%. K. pneumoniae showed resistance rates of 13.1% and 16.8% to imipenem and meropenem, respectively, from 2020 to 2024. E. faecium showed significantly higher resistance rates to the tested drugs than E. faecalis, particularly to ampicillin (95.1– 97.4% vs 4.9– 8.0%). Methicillin-resistant Staphylococcus aureus (MRSA) was detected at a rate of 33.8%. MRSA showed a higher level of resistance to penicillin, rifampicin, levofloxacin, clindamycin and erythromycin than methicillin-sensitive strains.
Conclusion: Over the past five years, the main pathogenic bacteria responsible for pediatric UTIs in southwestern China were E. coli, E. faecium and E. faecalis. Resistance patterns among major uropathogens revealed diverse trends, and the emergence of multidrug-resistant organisms presents a serious therapeutic challenge that warrants close surveillance.
Keywords: urinary tract infection, drug resistance, children, China, surveillance of drug resistance
Introduction
Urinary tract infections (UTIs) are among the most common infections worldwide, affecting approximately 150 million people and causing around 13,000 deaths annually.1,2 Within the paediatric population, preterm and newborn infants are at higher risk of UTIs than full-term infants.3 Around 8.4% of girls and 1.7% of boys under the age of seven are diagnosed with UTIs,4 and 30% of children develop recurrent infections within six months.5 UTIs are one of the most common causes of fever and bacteraemia in infants and young children.6 Approximately 5% of girls and 20% of boys under 2 months of age with a fever are diagnosed with a UTI.7 The clinical presentation of UTIs varies by age. Short-term symptoms usually include fever, dysuria and low back pain.8 If not properly treated, these symptoms often progress to recurrent UTIs, decreased renal function, renal scarring and serious consequences in adulthood such as hypertension and chronic renal insufficiency.9,10 Children are more likely than adults to develop urinary tract infections due to their immature immune systems, anatomical differences and congenital urinary tract abnormalities.11,12 As the signs and symptoms of UTIs in children are non-specific, and as infants and young children cannot clearly express symptoms, diagnosis and treatment are often delayed. The severe morbidity and sequelae place a heavy burden on families and society.13
Although antibiotic therapy is key to UTI management, several recent studies have shown that antibiotic resistance in paediatric urinary tract infections continues to rise. The proportion of multidrug-resistant E. coli has increased significantly in childhood urinary tract infections in Ukraine over the past 10 years.14 A meta-analysis in the United Kingdom revealed a high prevalence of antibiotic resistance in childhood urinary tract infections, particularly in countries or regions outside the Organisation for Economic Co-operation and Development (OECD).15 Data from Poland also revealed a substantial rise in E. coli resistance to amoxicillin/clavulanic acid, gentamicin and ceftazidime.16 According to a Chinese report, the drug resistance rate of Escherichia coli to third- and fourth-generation cephalosporins (eg, cefaclor, ceftazidime) as well as ceftazidime-avibactam often exceeds 30%–50%, and is even higher in some regions.17 As the distribution and resistance of urinary tract infections vary geographically and over time, experiences from different countries and regions can only be used as a reference, and clinicians must adapt their regimens to the latest local resistance data. In China, studies have reported on the distribution and resistance rates of urinary tract infection pathogens in the Jiaxing area (2020–2022), the Chongming area in eastern Shanghai (2018–2020) and the Sichuan province (2019–2023),18–20 but data specifically on paediatric UTI pathogen resistance remain scarce. Consequently, this study retrospectively analysed the distribution of pathogenic bacteria and drug sensitivity results of childhood urinary tract infections across 134 hospitals in southwestern China from 2020 to 2024, aiming to inform regional treatment strategies.
Materials and Methods
Source of Bacterial Isolates
The diagnosis of a urinary tract infection (UTI) in children was based on a combination of clinical manifestations, laboratory tests, imaging findings and guidelines, as well as clinical practice. The inclusion criteria were as follows: (1) outpatients and inpatients aged 0–14 years; (2) patients diagnosed with a urinary tract infection based on clinical symptoms, routine urinalysis and other examination results, in accordance with the Asian Guidelines for Urinary Tract Infections in Children;21 (3) patients presenting with clinical symptoms such as fever, cough, vomiting and diarrhoea. The exclusion criteria were as follows: (1) children with negative urine cultures; (2) children with contaminated urine samples; (3) children who did not meet the criteria for routine urinalysis; (4) those with incomplete clinical information; (5) children with blood disorders, immune system dysfunction and other serious complications (eg, severe liver and kidney dysfunction).
From 2020 to 2024, a total of 6598 children were diagnosed with urinary tract infections in 134 hospitals located in southwestern China. For these children, drug sensitivity tests were performed on urine isolates according to the surveillance protocol. The initial strain of the pathogen from each patient was retained for the analysis, resulting in a total of 7831 strains being included in the study (multiple bacterial isolates were obtained from some patients). The ethical review of this retrospective study was approved by the Chinese Institutional Review Board of Sichuan Provincial People’s Hospital and the University of Electronic Science and Technology (No. 2025788).
Bacterial Culture
All clinical samples were cultured following standardized microbiological procedures. Midstream urine specimens were collected in sterile containers and transported to the clinical microbiology laboratory for quantitative culture within 2 hours. A sterile inoculation loop (10 μL) was used to streak the urine samples onto three types of agar plates, namely 5% sheep blood agar, MacConkey agar, and Chocolate agar plates. The inoculated plates were incubated aerobically at 35°C for 18–24 hours, during which colony morphology (size and shape) was closely observed. A urine culture was determined to be positive if the concentration of a single gram-negative bacterial species reached ≥105 CFU/mL, or if that of a single gram-positive bacterial species reached ≥104 CFU/mL.
Bacterial Identification and Susceptibility Testing
The identification of bacteria was conducted using the Vitek 2 automated system or the MALDI-TOF mass spectrometry system.
The drug susceptibility test was performed by the minimum inhibitory concentration (MIC) test and the Kirby-Bauer (K-B) method, which was conducted in accordance with the CLSI M100 34th edition guideline criteria.22 In this context, tigecycline was evaluated in alignment with the criteria stipulated by the US Food and Drug Administration (FDA).23
Quality Control
According to CLSI guidelines, Escherichia coli (ATCC 25922), Klebsiella pneumoniae (ATCC 700603), Staphylococcus aureus (ATCC 25923), Pseudomonas aeruginosa (ATCC 27853), and Enterococcus faecalis (ATCC 29212) were used as QC strains, and weekly QC tests were performed.
Statistical Analysis
All data were analysed utilising WHONET5.6 data analysis software. The general steps of WHONET5.6 for statistical analysis of drug susceptibility result data are as follows: 1) the strain information, the antimicrobial drug name and the corresponding drug susceptibility test results must be entered into the software; 2) according to the statistical needs, the various types of analysis modes in the system must be selected, such as resistance analysis, sensitivity analysis and resistance spectrum analysis; 3) the analysis options must be set according to the data to be analysed. This involves selecting the source of strains, the types of strains, and the antimicrobial drugs of concern, among other considerations; 4) reports must be generated; 5) interpret the results; 6) export the data.
Results
Distribution of Pathogenic Bacteria in Urine Samples
A total of 7831 pathogenic isolates were detected in the 2020–2024 period, of which 4705 (60.1%) were gram-negative and 3126 (39.9%) were gram-positive. The top five detection rates were E. coli (37.8%), E. faecium (26.3%), E. faecalis (7.5%), K. pneumoniae (6.9%), P. aeruginosa (2.5%). The isolation rate of female patients (3636 strains, 55.1%) was found to be significantly higher than that of male patients (2962 strains, 44.9%). The highest isolation rate was identified in the age group of <28 days to ≤1 year (44.8%), and the lowest was identified in the age group of <1 year to ≤3 years (9.5%), as illustrated in Tables 1 and 2. The trend of detecting the top five bacteria causing urinary tract infections is demonstrated in Figure 1.
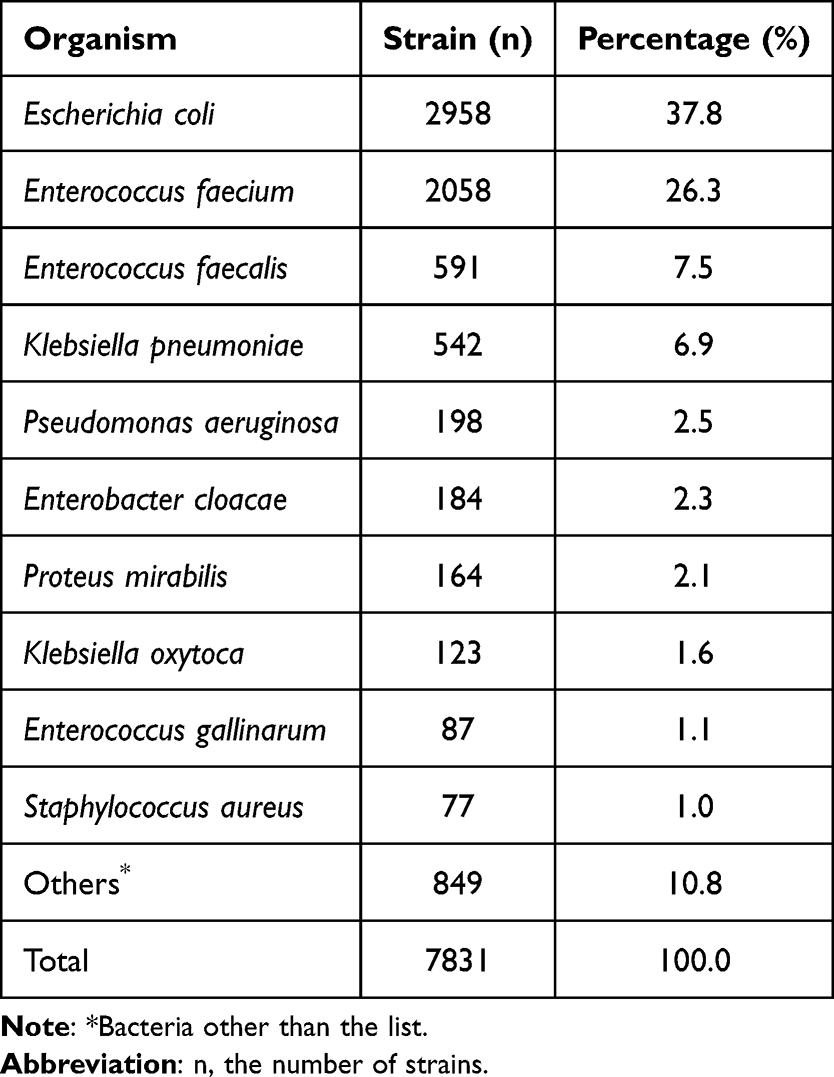 |
Table 1 Distribution of Bacterial Pathogens Isolated from Urine Specimens |
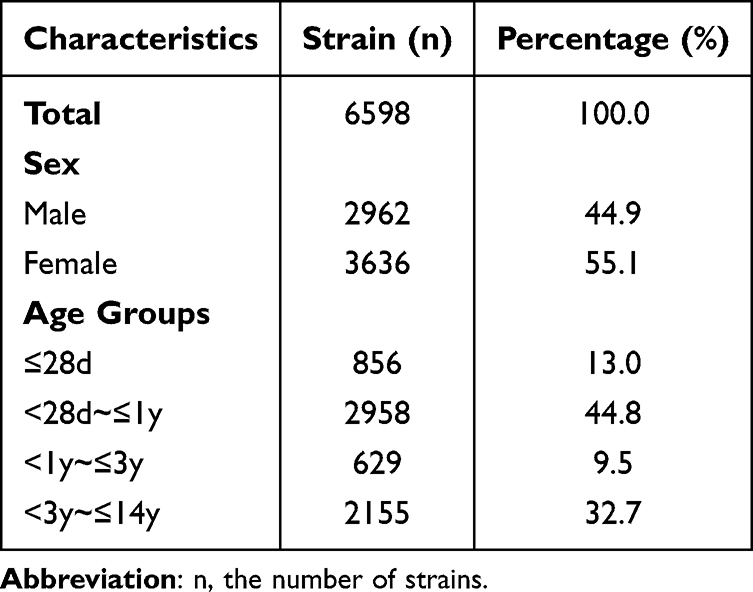 |
Table 2 Characteristics of Strains Isolated in Different Sex and Age Groups |
 |
Figure 1 Detection trends of the top 5 bacterial pathogens causing UTIs. |
Resistance of Main Gram-Negative Bacteria
From 2020 to 2024, E. coli demonstrated high susceptibility to piperacillin/tazobactam, cefoperazone/sulbactam, amikacin, and nitrofurantoin, with a resistance rate of less than 10%. The resistance rate to ceftriaxone and cefotaxime ranged from 57.4% to 67.3%, and to quinolones from 31.3% to 51.5%. There were insignificant changes in trends over the 5-year period, as illustrated in Table 3. The resistance rates of K. pneumoniae to ceftriaxone and cefotaxime ranged from 59.1% to 67.3%. The resistance rates to nitrofurantoin (18.6% to 24.7%) were considerably higher than those of E. coli (0.8% to 2.0%). As demonstrated in Table 4, the resistance rates of K. pneumoniae to imipenem and meropenem decreased from 16.7% and 24.2% in 2020 to 13.1% and 16.8% in 2024, respectively. This indicates a slight downward trend; however, it remains significantly higher than the resistance rates of E. coli to carbapenems (0.3–1.6%). Furthermore, the data demonstrates that the resistance rate of Enterobacter cloacae to aminoglycosides was less than 8.4%, to levofloxacin 4.1%, and to amikacin with a sensitivity of 100%. The resistance rate of Proteus mirabilis to ciprofloxacin and levofloxacin was 30.7% and 22.8%, respectively. P. aeruginosa demonstrated a resistance rate of less than 6.1% to each of the tested drugs and exhibited high activity, as shown in Table 5.
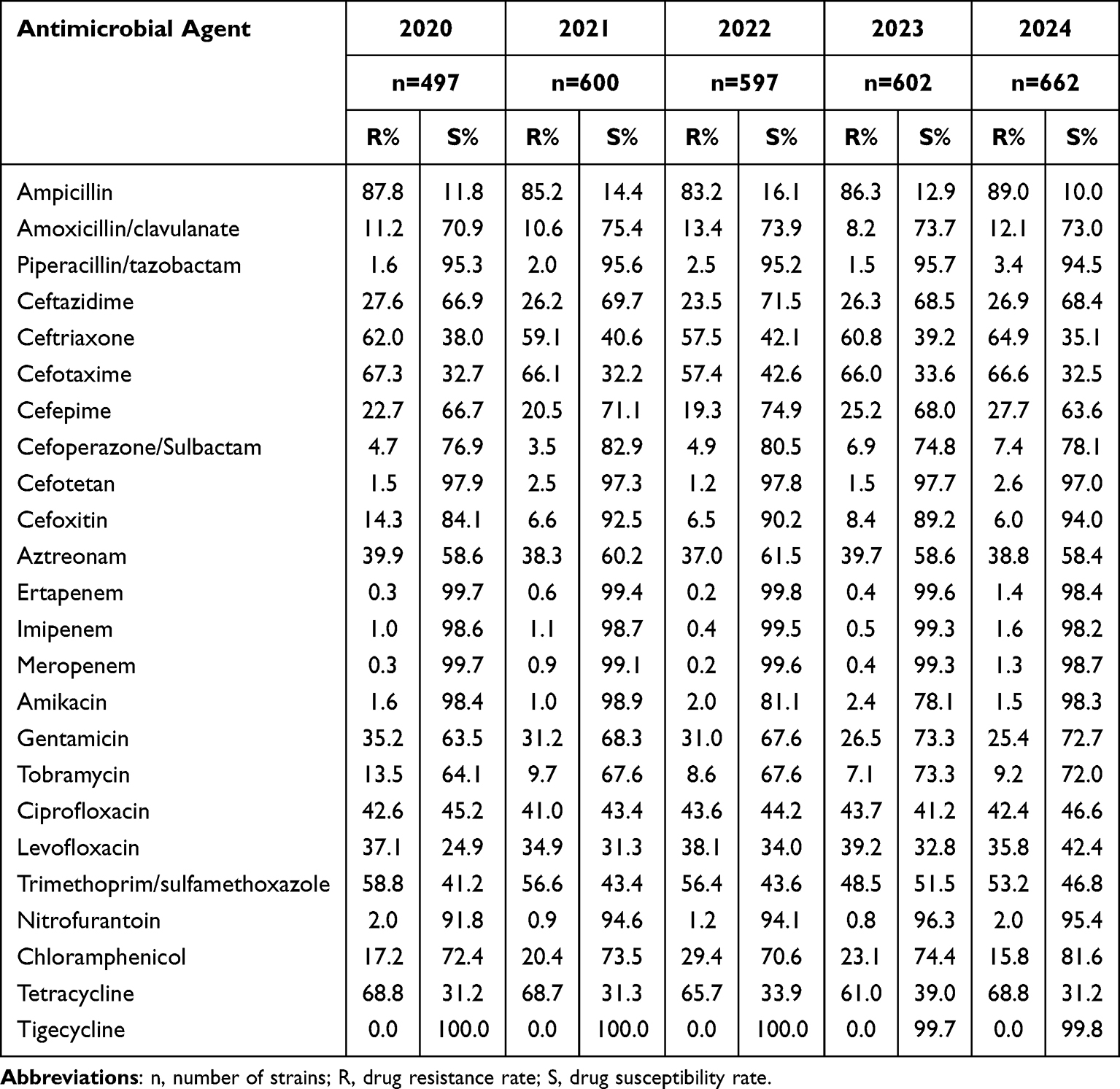 |
Table 3 Antibiotic Resistance of Escherichia coli |
 |
Table 4 Antibiotic Resistance of Klebsiella pneumoniae |
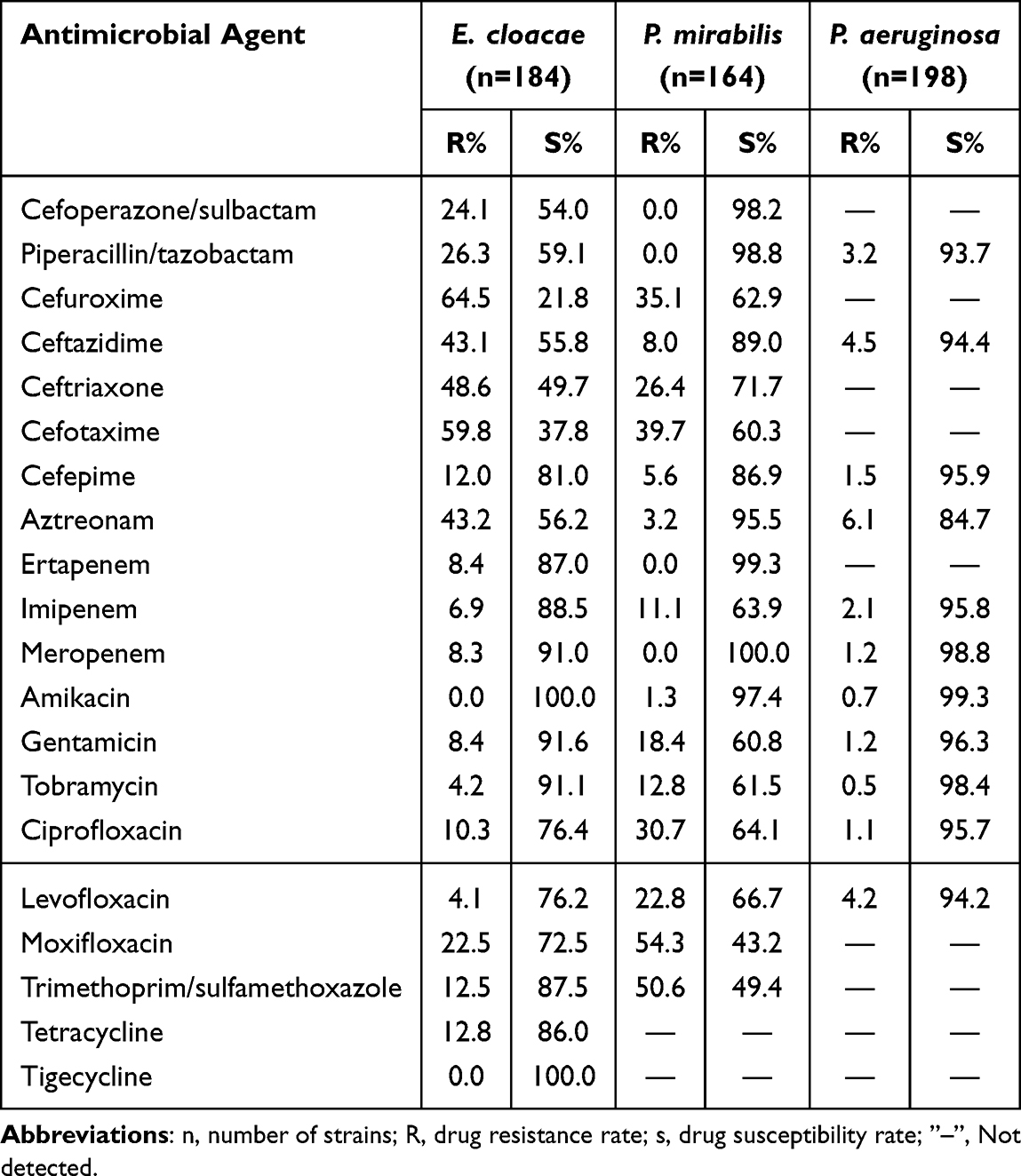 |
Table 5 Antibiotic Resistance of Enterobacter cloacae, Proteus mirabilis and Pseudomonas aeruginosa |
Drug Resistance in Main Gram-Positive Bacteria
A total of 2058 strains of E. faecium (26.3%) and 591 strains of E. faecalis (7.5%) were detected. E. faecium demonstrated a substantially higher degree of resistance to the drugs in question than E. faecalis, particularly with regard to ampicillin (95.1–97.4% VS 4.9–8.0%), resistance to ciprofloxacin and levofloxacin (greater than 53.4%), and a decline in resistance to nitrofurantoin from 11.4% in 2020 to 5.5% in 2024. E. faecalis demonstrated a high rate of resistance to rifampicin, ranging from 38.5% to 52.9%, and a susceptibility rate of >94.0% to linezolid and teicoplanin, with no vancomycin-resistant strains detected, as shown in Table 6.
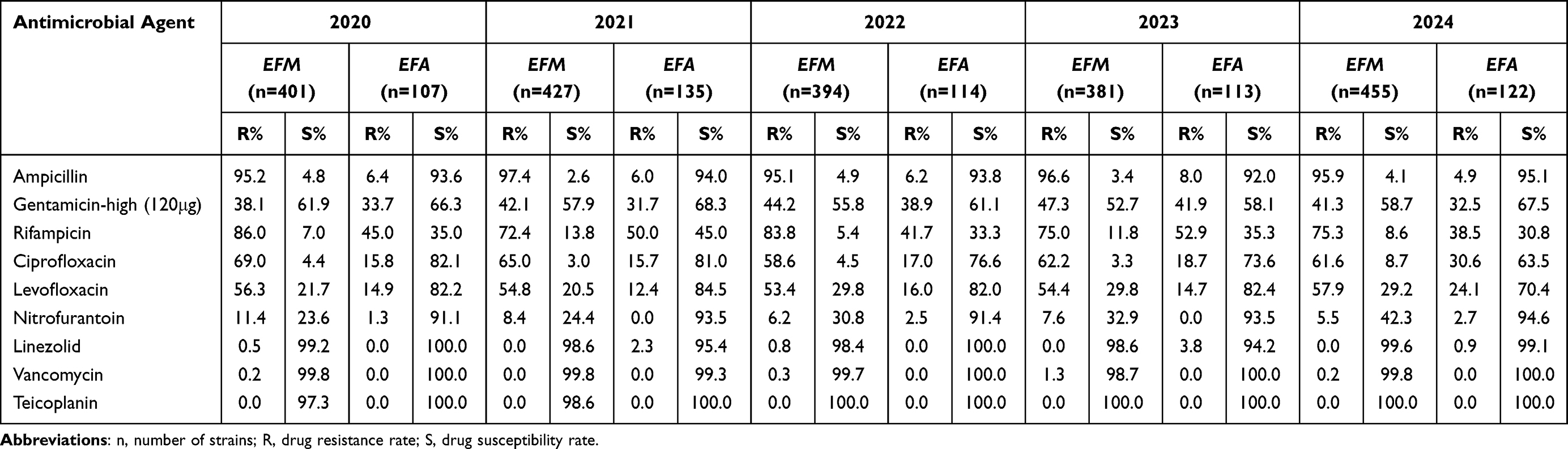 |
Table 6 Resistance Rates of Enterococcus faecium and Enterococcus faecalis to Antimicrobial Agents |
A total of 77 S. aureus strains were isolated from urine, and the detection rate of methicillin-resistant S. aureus was 33.8% (26/77). The resistance rate of MRSA to penicillin, rifampicin, levofloxacin, clindamycin and erythromycin was higher than that of methicillin-susceptible strains; MSSA exhibited a higher resistance rate to trimethoprim/sulfamethoxazole than MRSA (18.0% vs 4.3%) No strains resistant to vancomycin, linezolid, teicoplanin, and nitrofurantoin were detected, as shown in Table 7.
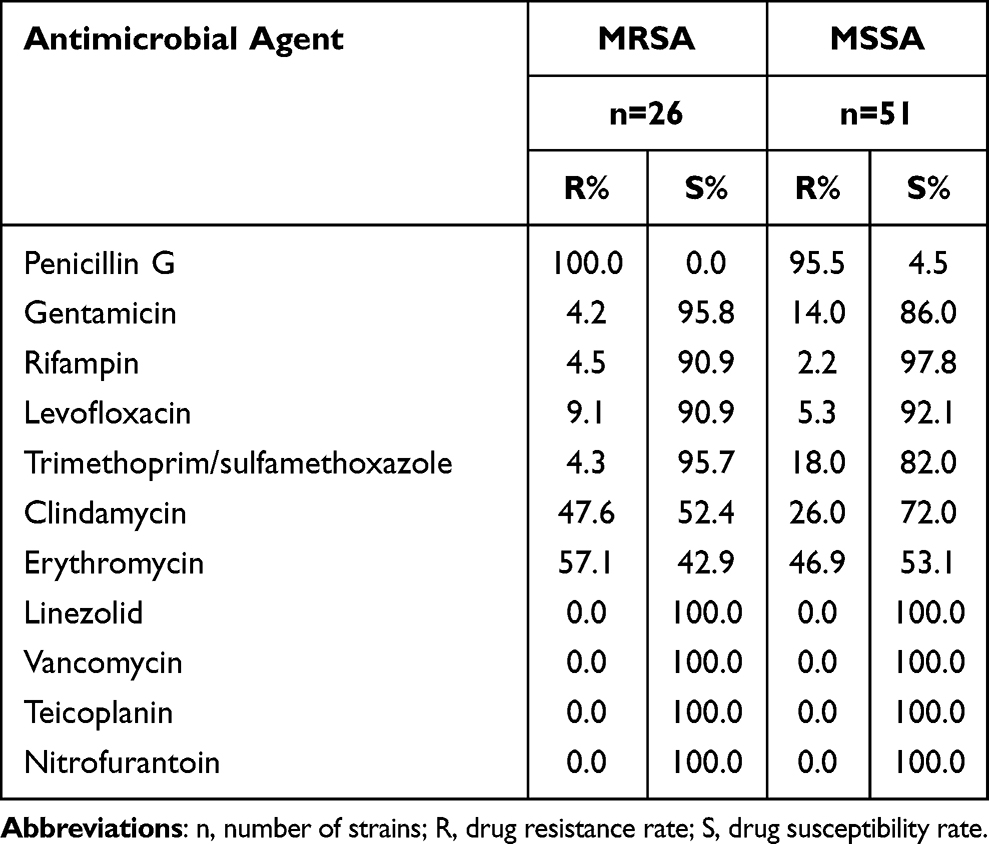 |
Table 7 Resistance Rates of Staphylococcus aureus to Antimicrobial Agents |
Multidrug-Resistant Bacteria Changes
Among the multi-drug resistant bacteria detected in the period 2020–2024, carbapenem-resistant E. coli (CR-ECO) and vancomycin-resistant Enterococci (VRE) remained at a low level, carbapenem-resistant K. pneumoniae (CR-KPN) showed a jagged distribution, and methicillin-resistant S. aureus (MRSA) showed a significant decrease in 2024, as shown in Figure 2.
 |
Figure 2 Distribution of multi-drug resistant strains in 2020–2024. Abbreviations: CR-ECO, Carbapenem-resistant Escherichia coli; CR-KPN, Carbapenem-resistant Klebsiella pneumoniae; MRSA, methicillin-resistant Staphylococcus aureus; VRE, Vancomycin-resistant Enterococcus; CTX/CRO-R-ECO, cefotaxime/ceftriaxone-resistant Escherichia coli; CTX/CRO-R-KPN, cefotaxime/ceftriaxone-resistant Klebsiella pneumoniae. |
Discussion
The present study revealed that a total of 6598 children were diagnosed with urinary tract infections, and 7831 pathogenic bacteria were isolated from 134 hospitals in Southwest China from 2020 to 2024. The top five detection rates were E. coli (37.8%), E. faecium (26.3%), E. faecalis (7.5%), K. pneumoniae (6.9%) and P. aeruginosa (2.5%). A plethora of studies from different regions have demonstrated discrepancies in the distribution of pathogens associated with urinary tract infections in children. For instance, in Chongqing, China, E. coli (40.5%), E. faecium (15.0%) and K. pneumoniae (8.9%) were predominantly detected;24 in Brazil, E. coli (56.9%), K. pneumoniae (18.5%) and E. faecalis (7.7%) were predominantly present;25 and in Nepal, the most prevalent pathogens were E. coli (53.0%), followed by E. faecalis (22.0%) and K. pneumoniae (7.0%).26 Conversely, in the Middle East, E. coli accounted for 88.6% of the total, with the remaining common pathogens comprising K. pneumoniae (10.3%) and P. mirabilis (4.7%).27 This finding indicates that the distribution of pathogens across different regions may be influenced by a variety of factors, including the local environment, medical conditions, and antibiotic use habits. In this study, the prevalence of urinary tract infections was highest (44.8%) in the infant group (<28d to ≤1y), which may be related to anatomical structure (eg, bladder neck position, shorter urethra) and immature immune system in infancy.
Pathogenic bacterial resistance testing is an important reference for guiding the rational use of clinical medications. Local resistance patterns can be used as supportive data to optimise the treatment regimen of empirical medications used in the region. This can reduce the mortality rate and healthcare costs of patients. The results of this surveillance study revealed that the resistance rate of Escherichia coli to piperacillin/tazobactam, cefoperazone/sulbactam, amikacin, and cefotetan was less than 10.0%. This finding indicates a high level of sensitivity, which is comparable to the 2019–2023 situation in this region reported by Zhong Min and the national data for 2015–2021.20,28 The resistance rate of Escherichia coli to nitrofurantoin ranged from 0.8% to 2.0%, and the drug continues to be used empirically since it has been demonstrated to inhibit bacteria in the urine significantly more than in the bloodstream in the treatment of urinary tract infections. However, in India, the resistance rate of Escherichia coli to nitrofurantoin was reported to be 78.7%,29 suggesting that antibiotic resistance patterns vary considerably between regions and countries.
The carbapenem resistance rate of E. coli was found to be less than 1.6%, with high activity and resistance to ceftriaxone and cefotaxime >57.4%, and quinolone resistance in the range of 31.3%–51.5%. K. pneumoniae demonstrated a resistance rate to ceftriaxone and cefotaxime in the range of 59.1%–67.3%, and quinolone resistance in the range of >15.6%. This result was consistent with the data reported by Niu et al in the Jiaxing region, where they found that the resistance rates of E. coli to ceftriaxone and quinolones exceeded 50.0%, while the resistance rates to carbapenems (1.0%), nitrofurantoin (1.8%), and piperacillin/tazobactam (0.7%) were relatively low.19 The utilisation of quinolones is proscribed for individuals under the age of 18 years in China, and the emergence of quinolone-resistant strains may be attributable to the extensive utilisation of such pharmaceuticals in adults to induce bacterial resistance, which is then transmitted through the bacterial plasmid, resulting in hospitalised paediatric pathogens also becoming resistant to them.
In the period 2020–2024, the detection rates for CTX/CRO-R-ECO remained high (55.6–63.9%) and the detection rates for CTX/CRO-R-KPN ranged from 43.6% to 60.2%. This rate was higher than the national average (49.2%) reported by the China Antimicrobial Surveillance Network (CHINET) in 2024,30 and far higher than the 12.9% reported in the United States.31 This was due to the emergence of strains resistant to third-generation cephalosporins (3GC) as a result of the production of ultrabroad-spectrum β-lactamases (ESBLs) or AmpC enzymes. This phenomenon has been widely exacerbated by the widespread use of third-generation cephalosporins.32 In the Bacterial Priority Pathogens List 2024 (BPPL-2024) published by the World Health Organization (WHO),33 3GCRE have been individually categorized as a key priority, there by adding to the burden of low- and middle-income countries and vulnerable populations due to their high rate of therapeutic failures and increased healthcare costs. Studies have demonstrated that significant discrepancies exist in the treatment regimens for urinary tract infections (UTIs) across different regions worldwide, indicating that therapeutic strategies should be formulated based on local antimicrobial resistance profiles.34 The data of the present study were collected from 134 hospitals in Southwest China, which are representative of the bacterial resistance patterns in this region. Our findings suggest that third-generation cephalosporins may no longer be suitable for the treatment of pediatric UTIs in this area. Given that antibiotic-resistant UTIs are associated with prolonged hospital stays and extended treatment courses,35 Therefore, it is imperative for clinical practice to promptly establish antibiotic administration and feedback mechanisms, implement a prescription review system, and intervene in irrational antibiotic use. Meanwhile, patients infected with drug-resistant bacteria should be isolated, and disinfection of ward environments should be strengthened to prevent the transmission of such pathogens.
Studies have demonstrated that carbapenems may serve as effective alternatives. However, it should be noted that the detection rate of carbapenem-resistant K. pneumoniae (CRKPN) among isolates increased from 13.6% in 2020 to 16.4% in 2024, which is slightly lower than the CHINET 2015–2021 surveillance results,36 and the detection rate of carbapenem-resistant E. coli (CRECO) fluctuated between 0.5% and 1.7%. In China, the drug resistance of carbapenem-resistant Enterobacterales (CRE) is mainly driven by the plasmid-mediated transmission of KPC-2/ST11 and NDM-5/ST48 clones, which is distinct from that in Western countries (eg, the KPC-2/ST258 clone prevalent in the United States).37–39 This dual feature of high pathogenicity plus high drug resistance renders the clinical treatment extremely challenging. Although in vitro drug sensitivity tests have demonstrated the presence of good antimicrobial activity of tigecycline against CRE, it is not recommended for the treatment of urinary tract infections caused by CRE because it does not reach effective therapeutic concentrations in urine. The Infectious Diseases Society of America (IDSA) has issued guidelines recommending the utilisation of ciprofloxacin, levofloxacin, and TMP/SMX as preferred treatment options for uncomplicated bladder infections caused by CRE. For cases of pyelonephritis or complicated urinary tract infections caused by CRE, the aforementioned three drugs are recommended if they are susceptible to sensitization tests; otherwise, ceftazidime-avibactam, meropenem-vaborbactam, imipenem-relebactam, and cefdinir are preferred.40 Given the contraindication of quinolones in paediatric patients, ceftazidime/avibactam represents the sole antibiotic currently available in China for treatment of CRE infections in children, thereby significantly restricting the range of therapeutic options. However, the most recent study demonstrated that New Delhi metallo-β-lactamase (NDM) accounted for as many as 68.0% of carbapenem-resistant Klebsiella pneumoniae (CRKP) infections in neonates. Since the metalloenzyme NDM is capable of hydrolyzing ceftazidime/avibactam, the role of the latter in the treatment of CRKP infections has been drastically limited.41 Consequently, there is a necessity for heightened vigilance with regard to CRE infections in the paediatric population. Moreover, there is a requirement for the continuous promotion and implementation of prevention and control initiatives for multidrug-resistant bacterial infections, including rectal swab screening of key populations, environmental disinfection, and the management of family visitors. It is encouraging that phage therapy has demonstrated positive outcomes in the treatment of CRKP-induced urinary tract infections, thus providing a more extensive range of clinical treatment options.42
Of the enterococci that cause urinary tract infections, E. faecium (2058 strains, 26.3%) and E. faecalis (591 strains, 7.5%) predominate. Surveillance in this region revealed that E. faecium exhibited higher resistance rates to most of the drugs tested than E. faecalis, especially ampicillin (95.1–97.4% vs 4.9–8.0%). Furthermore, E. faecalis demonstrated a sensitivity rate of >91.0% to nitrofurantoin and a sensitivity rate of 100.0% to teicoplanin. A low prevalence of Enterococci was observed to demonstrate resistance to vancomycin (<1.3%) and linezolid (<3.8%), a figure that was marginally higher than the national average.28 In China, the drug resistance of vancomycin-resistant Enterococcus (VRE) is mainly attributed to the horizontal transfer of the vanA gene carried by enterococci via plasmids, accompanied by the expansion of the ST78 clone.43 Consequently, enterococcal urinary tract infections in children can be treated with scientifically empirical antimicrobial therapy based on this large resistance monitoring data.
The present study was subject to certain limitations. Firstly, it is important to note that antibiotic exposure has the capacity to affect the positivity rate and microbiologic profile of urine cultures, due to the retrospective nature of the analysis, it was not possible to ascertain whether the patients had previously used antibiotics. Secondly, the contamination of infant faeces is a matter that requires resolution, given its direct impact on the detection of pathogenic bacteria in urine cultures. Furthermore, it should be noted that not all hospitals employ precisely the same testing methods (due to a lack of personnel, equipment, facilities, and/or methodology), which may have an impact on the results.
Conclusion
In the contemporary context of Southwest China, the epidemiology of paediatric urinary tract infections is characterised by a predominance of Escherichia coli, followed by Enterococcus faecium and Enterococcus faecalis. There is an observed rise in infections with multidrug-resistant organisms, underscoring the necessity for a focused investigation of CRE and VRE. Clinicians are advised to send urine specimens for microbial culture as early as possible, develop treatment strategies based on the drug sensitivity results, and isolate patients with isolation of multidrug-resistant bacteria to prevent the spread of MDR within the hospital. In order to facilitate a more profound comprehension of the molecular epidemiological characteristics of multidrug-resistant bacteria in the region, it is recommended that the changes of drug-resistant gene profiles be monitored, thus enabling the tracking of clone/plasmid transmission in real time and the implementation of targeted interventions.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, China (No. 2025788). The ethics committee waived the need for written informed consent provided by participants due to the retrospective nature of this study. Patients’ anonymous information was provided from the microbiology hospital laboratory, which isolated the strains. The study completely followed the principles outlined in the Declaration of Helsinki.
Acknowledgment
We are grateful to all the authors for their contributions to this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Khoshnood S, Heidary M, Mirnejad R, et al. drug-resistant gram-negative uropathogens: a review. Biomed Pharmacother. 2017;94:982–13. doi:10.1016/j.biopha.2017.08.006
2. Kumar MS, Das AP. Emerging nanotechnology based strategies for diagnosis and therapeutics of urinary tract infections: a review. Adv Colloid Interface Sci. 2017;249:53–65. doi:10.1016/j.cis.2017.06.010
3. Brandström P, Hansson S. Urinary tract infection in children. Pediatr Clin North Am. 2022;69(6):1099–1114. doi:10.1016/j.pcl.2022.07.003
4. Chuanyang L, Gaofu Z. Prevention of recurrent urinary tract infections in children. J Pediatr Pharm. 2019;25(03):57–60. doi:10.13407/j.cnki.jpp.1672-108X.2019.03.018
5. Korbel L, Howell M, Spencer JD. The clinical diagnosis and management of urinary tract infections in children and adolescents. Paediatr Int Child Health. 2017;37(4):273–279. doi:10.1080/20469047.2017.1382046
6. Qian S. Guidelines for diagnosis and treatment of pediatric urinary tract infections. Chin J Pract Pediatrics. 2021;36(5):337–341.
7. Simões e Silva AC, Oliveira EA. Update on the approach of urinary tract infection in childhood. J Pediatr. 2015;91(6 Suppl 1):S2–S10. doi:10.1016/j.jped.2015.05.003
8. Buettcher M, Trueck J, Niederer-Loher A, et al. Swiss consensus recommendations on urinary tract infections in children. Eur J Pediatr. 2021;180(3):663–674. doi:10.1007/s00431-020-03714-4
9. Nuutinen M, Uhari M. Recurrence and follow-up after urinary tract infection under the age of 1 year. Pediatr Nephrol. 2001;16(1):69–72. doi:10.1007/s004670000493
10. Desai DJ, Gilbert B, McBride CA. Paediatric urinary tract infections: Diagnosis and treatment. Aust Fam Physician. 2016;45(8):558–563.
11. Simões E, Silva AC, Oliveira EA, Mak RH. Urinary tract infection in pediatrics: an overview. J Pediatr. 2020;96 Suppl 1(Suppl 1):65–79. doi:10.1016/j.jped.2019.10.006
12. Bryant PA, Bitsori M, Vardaki K, et al. Guidelines for complicated urinary tract infections in children: a review by the european society for pediatric infectious diseases. Pediatr Infect Dis J. 2025;44(6):e211–e223. doi:10.1097/INF.0000000000004790
13. Steiger SN, Comito RR, Nicolau DP. Clinical and economic implications of urinary tract infections. Expert Rev Pharmacoecon Outcomes Res. 2017;17(4):377–383. doi:10.1080/14737167.2017.1358618
14. Budnik TV, Bevzenko TB. A ten-year analysis of changes in the sensitivity of the leading uropathogen to antibacterial agents in children with urinary tract infection in the nephrology department. Wiad Lek. 2020;73(7):1360–1364.
15. Bryce A, Hay AD, Lane IF, et al. Global prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli and association with routine use of antibiotics in primary care: systematic review and meta-analysis. BMJ. 2016;352:i939. doi:10.1136/bmj.i939
16. Werbel K, Jankowska D, Wasilewska A, et al. Clinical and epidemiological analysis of children’s urinary tract infections in accordance with antibiotic resistance patterns of pathogens. J Clin Med. 2021;10(22):5260. doi:10.3390/jcm10225260
17. Lin Y, Xu WH. Pathogen characteristics and drug resistance analysis of urinary tract infections in children. Zhejiang Clin Med J. 2025;27(01):43–45.
18. Li J, Jiang F, Xie A, Jiang Y. Analysis of the distribution and drug resistance of pathogens in patients with urinary tract infection in the Eastern Chongming area of Shanghai from 2018 to 2020. Infect Drug Resist. 2022;15:6413–6422. doi:10.2147/IDR.S384515
19. Niu X, Hou B, Yang L, et al. Patterns of drug resistance and bacterial pathogen distribution in patients with urinary tract infections in the Jiaxing Region from 2020 to 2022. Infect Drug Resist. 2023;16:5911–5921. doi:10.2147/IDR.S424158
20. Zhong M, Huang X, Liu X, et al. Analysis of the distribution characteristics and changes of drug resistance of pathogens in patients with urinary tract infection across Southwest China from 2019 to 2023. Infect Drug Resist. 2025;18:1491–1502. doi:10.2147/IDR.S512409
21. Ss Y, Jd T, Kanematsu A, et al. Asian guidelines for urinary tract infection in children. J Infect Chemother. 2021;27(11):1543–1554. doi:10.1016/j.jiac.2021.07.014
22. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. CLSI. 2024;2024:1.
23. U.S.Food and Drug Administration. FDA-identified interpretive criteria[EB/OL]. 2022. Available from: https://www.fda.gov/drugs/development-resources/tigecycline-injection-products.
24. Lu J, Liu X, Wei Y, et al. Clinical and microbial etiology characteristics in pediatric urinary tract infection. Front Pediatr. 2022;10:844797. doi:10.3389/fped.2022.844797
25. Lo DS, Rodrigues L, Koch VHK, et al. Clinical and laboratory features of urinary tract infections in young infants. J Bras Nefrol. 2018;40(1):66–72. doi:10.1590/1678-4685-JBN-3602
26. Shrestha LB, Baral R, Poudel P, et al. Clinical, etiological and antimicrobial susceptibility profile of pediatric urinary tract infections in a tertiary care hospital of Nepal. BMC Pediatr. 2019;19(1):36. doi:10.1186/s12887-019-1410-1
27. Shaaban OA, Mahmoud NA, Zeidan AA, et al. Prevalence and resistance patterns of pediatric urinary tract infections in Bahrain. Cureus. 2021;13(12):e20859. doi:10.7759/cureus.20859
28. Li Y, Zou M, Liu W, et al. Distribution and antimicrobial resistance changes of urinary isolates in CHINET from 2015 to 2021. Chin J Infection Chemother. 2024;24(03):287–299. doi:10.16718/j.1009-7708.2024.03.006
29. Prakash D, Saxena RS. Distribution and antimicrobial susceptibility pattern of bacterial pathogens causing urinary tract infection in urban community of Meerut City, India. ISRN Microbiol. 2013;2013:749629. doi:10.1155/2013/749629
30. Guo Y, Ding L, Hu FP, et al. CHINET surveillance of bacterial resistance in China, 2024. Chin J Infection Chemother. 2025;25(06):597–607. doi:10.16718/j.1009-7708.2025.06.002
31. Mark DG, Hung YY, Salim Z, Tarlton NJ, Torres E, Frazee BW. Third-generation cephalosporin resistance and associated discordant antibiotic treatment in emergency department febrile urinary tract infections. Ann Emerg Med. 2021;78(3):357–369. doi:10.1016/j.annemergmed.2021.01.003
32. European Food Safety Authority; European Centre for Disease Prevention and Control. The European Union summary report on antimicrobial resistance in zoonotic and indicator bacteria from humans, animals and food in 2017. EFSA J. 2019;17(2):e05598. doi:10.2903/j.efsa.2019.5598.
33. Jesudason T. WHO publishes updated list of bacterial priority pathogens. Lancet Microbe. 2024;5(9):100940. doi:10.1016/j.lanmic.2024.07.003
34. Wong SW, Tullus K, Chan YHE. Controversies in treating febrile infantile urinary tract infection caused by extended-spectrum beta-lactamase producing Enterobacteriaceae: an international multi-centre survey. Pediatr Nephrol. 2025;40(7):2253–2266. doi:10.1007/s00467-025-06700-w
35. Chan EY. Community-acquired urinary tract infections caused by ESBL-producing Enterobacteriaceae in infants less than 2 years of age. Pediatr Nephrol. 2022;37(5):1167–1168. doi:10.1007/s00467-022-05443-2
36. Meng Q, Zhou L, Chen Y, et al. Distribution characteristics and evolution of antimicrobial resistance in clinically isolated bacteria from pediatric patients in CHINET, 2015–2021. Chin J Infection Chemother. 2025;25(01):48–58. doi:10.16718/j.1009-7708.2025.01.008
37. Guo L, Wang L, Zhao Q, et al. Genomic analysis of KPC-2-producing Klebsiella pneumoniae ST11 isolates at the respiratory department of a tertiary care hospital in Beijing, China. Front Microbiol. 2022;13:929826. doi:10.3389/fmicb.2022.929826
38. Wang Q, Jin L, Sun S, et al. Occurrence of high levels of cefiderocol resistance in carbapenem-resistant escherichia coli before its approval in China: a report from China CRE-network. Microbiol Spectr. 2022;10(3):e0267021. doi:10.1128/spectrum.02670-21
39. Li M, Yu M, Yuan Y, et al. Designing a conjugate vaccine targeting Klebsiella pneumoniae ST258 and ST11. Heliyon. 2024;10(5):e27417. doi:10.1016/j.heliyon.2024.e27417
40. TTamma PD, Aitken SL, Bonomo RA, et al. Infectious Diseases Society of America 2022 Guidance on the Treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin Infect Dis. 2022;75(2):187–212. doi:10.1093/cid/ciac268
41. Fu P, Luo X, Shen J, et al. The molecular and epidemiological characteristics of carbapenemase-producing Enterobacteriaceae isolated from children in Shanghai, China, 2016-2021. J Microbiol Immunol Infect. 2023;56(1):48–56. doi:10.1016/j.jmii.2022.07.012
42. Qin J, Wu N, Bao J, et al. Heterogeneous Klebsiella pneumoniae co-infections complicate personalized bacteriophage therapy. Front Cell Infect Microbiol. 2021;10:608402. doi:10.3389/fcimb.2020.608402
43. Shen C, Luo L, Zhou H, et al. Emergence and ongoing outbreak of ST80 vancomycin-resistant Enterococcus faecium in Guangdong province, China from 2021 to 2023: a multicenter, time-series and genomic epidemiological study. Emerg Microbes Infect. 2024;13(1):2361030. doi:10.1080/22221751.2024.2361030
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Parental Attitudes Towards Vaccination Against COVID-19 in China During Pandemic
Lu L, Gu W, Xie H, Wang X, Cao L, Shan M, Wu P, Tian Y, Zhou K
Infection and Drug Resistance 2022, 15:4541-4546
Published Date: 15 August 2022
Association of SCN1A Gene Polymorphisms with Sodium Valproate Resistance in Pediatric Epilepsy: A Retrospective Case-Control Study
Wang H, Geng T, Deng N
Neuropsychiatric Disease and Treatment 2025, 21:1599-1609
Published Date: 7 August 2025
Sociodemographic and Clinical Correlates of Multidrug-Resistant Uropathogens in Hospitalized Children
Muhsen K, Haleem S, Mansour B, Shapira M, Pitashny M, Masarwa M, Omar M, Na’aminh W, Kassem E
Infection and Drug Resistance 2026, 19:588989
Published Date: 8 April 2026
Macrolide Resistance of Mycoplasma pneumoniae Among Children in Hangzhou: A 2024–2025 Post-Pandemic Surveillance Study
Xu X, Xiao X, Zhou J, Zhao X
Infection and Drug Resistance 2026, 19:607500
Published Date: 26 May 2026
Prolonged Suppression of Bacterial Growth in Urine Culture Following Fluoroquinolone Therapy in an Elderly Diabetic Patient: A Diagnostic Pitfall
Roshdi Maleki M
Infection and Drug Resistance 2026, 19:599561
Published Date: 3 June 2026