Back to Journals » Infection and Drug Resistance » Volume 15
Association of Pre-Existing Comorbidities with Disease Severity Among COVID-19 Patients in Eastern Ethiopia
Authors Merga BT ![]() , Ayana GM
, Ayana GM ![]() , Raru TB
, Raru TB ![]() , Alemu A, Negash B, Bekana M, Birhanu A
, Alemu A, Negash B, Bekana M, Birhanu A ![]() , Dessie Y
, Dessie Y
Received 23 February 2022
Accepted for publication 27 May 2022
Published 1 June 2022 Volume 2022:15 Pages 2825—2834
DOI https://doi.org/10.2147/IDR.S362140
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Bedasa Taye Merga,1 Galana Mamo Ayana,1 Temam Beshir Raru,1 Addisu Alemu,1 Belay Negash,1 Miressa Bekana,2 Abdi Birhanu,2 Yadeta Dessie1
1School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2School of Medicine, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Bedasa Taye Merga; Galana Mamo Ayana, School of Public Health, College of Health and Medical Sciences, Haramaya University, P.O.Box.: 235, Harar, Oromia, Ethiopia, Email [email protected]; [email protected]
Background: Comorbidities and advanced age increase the risk of severe outcomes of COVID-19. In order to shift the possible unfavorable treatment outcome in patients with chronic illnesses, information related to the prevalence of chronic illness and its effect on severity of COVID-19 infection has paramount importance.
Objective: This study was aimed at assessing the prevalence of comorbidities and associated severity among COVID-19 patients admitted to COVID-19 treatment center, eastern Ethiopia.
Methods: An institution-based cross-sectional study design was employed among 422 COVID-19 patients admitted to COVID-19 treatment center, eastern Ethiopia from April 10, 2020, to August 10, 2021. Binary logistic regression was fitted to identify comorbidities and other factors associated with severe clinical outcome, associations were presented with adjusted odds ratios (AORs) and 95% confidence intervals (CIs). In all analyses statistical significance were declared at p-value < 0.05.
Results: More than half (52.4%) of the COVID-19 patients were presented with comorbid conditions. One third (34.6%) of the admitted COVID-19 patients were in severe clinical stages. Marital status (AOR=4.56; 95% CI: 1.40, 14.76), hypertension (AOR=2.08; 95% CI: 1.09, 3.97), diabetes mellitus (AOR=3.31; 95%:1.84, 5.98), and cardiovascular diseases (AOR=4.22; 95% CI: 2.18, 8.15) were identified as factors associated with severe clinical stages.
Conclusion: The comorbid conditions such as diabetes, hypertension, and cardiovascular diseases, and marital status were identified as significant predictors of severe outcomes of COVID-19. Therefore, identifying the people with chronic comorbidities as a risk group would help to anticipate and prevent the serious outcomes of COVID-19 infection.
Keywords: COVID-19, coronavirus, comorbidities, severe clinical stages, Ethiopia
Introduction
Coronavirus (COVID-19) is a respiratory infection with different degrees of clinical symptoms as mild, moderate, severe, and critical illness. Majority of patients with COVID-19 present with flu-like symptoms such as fever, dry cough, fatigue and dyspnea.1 Most patients with these flu like symptoms have a good prognosis, while only a small portion of patients progressing into severe or critical cases, and progresses to acute respiratory distress syndrome, septic shock, and multiple organ failure and death. The fatal complications and death are more common for the elderly and those with underlying diseases.2
Evidence indicates that many comorbidities associate with the severity of COVID-19.3–5 Patients having diabetes mellitus, obesity, and hypertension with COVID-19 have increased mortality and morbidity rate. Possible mechanisms for the increased severity and mortality among diabetic patients include hyperglycemia-induced changes in the immune system and increases in inflammatory cytokines.6 The severe course and worse outcome of SARS-Cov-2 infection in hypertensive patients, related to hyper-inflammatory response and cytokine storm development during the third phase of the disease.7 Cardiovascular diseases are also associated with the increased death rate of COVID-19.8
Synthesis of evidences revealed that the most prevalent comorbid condition in the confirmed COVID-19 patients was hypertension (21%), followed by diabetes mellitus (11%) and cardiovascular disease in 5.8%.9 Similarly, cerebrovascular disease in 2.4%, chronic kidney disease in 3.6%, chronic liver disease in 2.9%, chronic pulmonary disease in 2.0%, malignancy in 2.7%, and smoking in 8.7% of the patients was documented.9
Hence, in order to prevent the deterioration from mild and moderate conditions to the severe ones and death identifying the population group that is more vulnerable to the development of adverse outcomes of COVID-19 has paramount significance. Furthermore, the assessment of the prevalence of different comorbidities is beneficial to the special care of the targeted population. Thus, this study was aimed at assessing the prevalence of comorbidities and associated severity among COVID-19 patients admitted to COVID-19 treatment center, eastern Ethiopia.
Methods
Study Area, Period, and Design
An institution-based cross sectional study design was employed among COVID-19 patients admitted to COVID-19 treatment center, eastern Ethiopia between April 10, 2020, and August 10, 2021. Harar capital city of the region is located 522 kilometers away from Addis Ababa, the capital city of Ethiopia due east. The region has two public hospitals, one Federal Police Hospital, one Fistula center, Private Hospitals, and eight health centers. One of the public hospitals serves as COVID-19 treatment center. This study was conducted among patients admitted to COVID-19 treatment center. During this pandemic, the hospital is one of the ten regional centers designated by the Ethiopia Ministry of Health to manage the COVID-19 cases as a center in Eastern Ethiopia. Therefore, the hospital has been serving as COVID-19 treatment center in the eastern part of Ethiopia, where it serves more than six million populations in the catchment areas.
Participants and Eligibility Criteria
All patients with confirmed COVID-19 infection and admitted to COVID-19 treatment center between April 10, 2020, and August 10, 2021 were included in the study retrospectively. Patients whose clinical outcome were not identified until August 10, 2021 and had incomplete data for variable of interest were excluded from the study.
Sample Size Determination
The sample size was determined using single population proportion with the assumptions of margin of error=0.05, proportion of severe cases (0.5). The sample size was determined to be 384. Finally, by considering 10% of nonresponse rate, the sample was determined to be 422.
Study Variables and Measurements
The Outcome Variable
Clinical stages of COVID-19 categorized as severe and non-severe cases. There are four clinical stages as mild, moderate, severe, and critical defined clinically. In this study we dichotomized these four stages as non-severe (mild and moderate) and severe (severe and critical).
The Explanatory Variables
Comorbid conditions including hypertension, diabetes, cardiovascular disease, kidney diseases, lung diseases, asthma, cancer, and liver diseases were assessed both by history and objective criteria mentioned below. Socio-demographic variables such as gender, age, marital status, occupation, COVID-19 clinical characteristics, and clinical outcomes, use of ventilators, COVID-19 clinical management.
Diagnosis of COVID-19 was defined as the patient having a positive result on the oropharyngeal swab for SARS-CoV-2 by reverse transcriptase polymerase chain reaction (RT-PCR).10 Common radiological assessment included chest radiograph and computed tomography of the chest based on clinical decision-making.
Hypertension is diagnosed when systolic blood pressure is > 140 mmHg and/or diastolic blood pressure is > 90 mmHg.11
Diabetes mellitus was diagnosed with following criteria,11
1. Fasting plasma glucose (FPG) >126 mg/dl
2. Hemoglobin A1C > 6.5%
3. A random plasma glucose >200mg/dl, in patients with classic symptoms of hyperglycemia or hyperglycemic crisis
4. Two-hour plasma glucose >200 mg/dl during an oral glucose oral tolerance test.
Acute kidney disease/injury is diagnosed when one of the following criteria is met:11
- Serum creatinine rises by < 0.3 mg/dl within 48 hours or
- Serum creatinine rises < 1.5 fold from the baseline, which is known or presumed to have occurred within one week or
- Urine output is < 0.5mL/kg/hr for >6 consecutive hours
Chronic Kidney Disease
Kidney damage for >3 months, as defined by structural or functional abnormalities of the kidney, with or without decreased GFR manifest by either: Markers of kidney damage, including abnormalities in blood urea, creatinine or urine abnormalities or abnormalities in imaging tests – Pathological abnormalities – GFR < 60mL/minute/1.73m for > 3 months.11
COVID-19 Clinical Stages are Defined as Follows
Asymptomatic Infection
Individuals who test positive for SARS-CoV-2 using a virology test (ie, a nucleic acid amplification test [NAAT] or an antigen test) but who have no symptoms that are consistent with COVID-19.12
Mild Illness
Individuals who have any of the various signs and symptoms of COVID-19 (eg, fever, cough, sore throat, malaise, headache, muscle pain, nausea, vomiting, diarrhea, loss of taste and smell) but who do not have shortness of breath, dyspnea, or abnormal chest imaging.12
Moderate Illness
Individuals who show evidence of lower respiratory disease during clinical assessment or imaging and who have oxygen saturation (SpO2) ≥94% on room air at sea level.12
Severe Illness
Individuals who have SpO2 <94% on room air at sea level, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300 mm Hg, respiratory frequency >30 breaths/min, or lung infiltrates >50%.12
Critical Illness
Individuals who have respiratory failure, septic shock, and/or multiple organ dysfunctions.12
Data Collection Method and Procedures
Structured checklists were used to collect data from patient charts. The tool contains: socio-demographic and economic factors, clinical factors, comorbid conditions, and clinical stages of patients. Data extraction was conducted after two days training was given for both data collectors and supervisors. Five BSc degree holder Nurses were involved in the data extraction and two public health professionals were involved as supervisors.
Statistical Analysis
The collected data were entered, coded, and recoded using Epi Data Version 3.1 and then exported to STATA version 14 for analysis. Descriptive statistics using frequency distribution, percentage, mean and standard deviation were computed to describe the study participants. Before fitting the model, chi-square assumption was checked. For each predictor variables bi-variable binary logistic regressions were fitted. Variables with p-value <0.25 in the bi-variable analysis were selected for multiple logistic regressions to examine their effects after adjusting for potential confounders. In the multivariable logistic regressions, predictor variables were presented with adjusted odds ratios (AORs) and 95% confidence intervals (CIs). In all analyses statistical significance were declared at p-value <0.05.
Ethical Statement
The Institutional Health Research Ethical Review Committee (IHRERC) of the College of Health and Medical Sciences of Haramaya University reviewed and approved the study protocol. As the study used secondary data, obtaining informed consent for this study was waived by the Ethical Review Committee. No personal identifiers, such as names, addresses, and any private information were collected. Data were handled confidentially during all phases of research activities using anonymous medical registration numbers as identification. All data extraction processes were conducted per the declaration of Helsinki.
Results
Socio-Demographic Factors
A total of 422 COVID-19 patients were enrolled into the study. The mean age of the study participants was 42.43 (±20.98) years. Majority (64.22%) of the patients were male. More than half (52.6%) of the patients were employed. About 73% of the patients were married (Table 1).
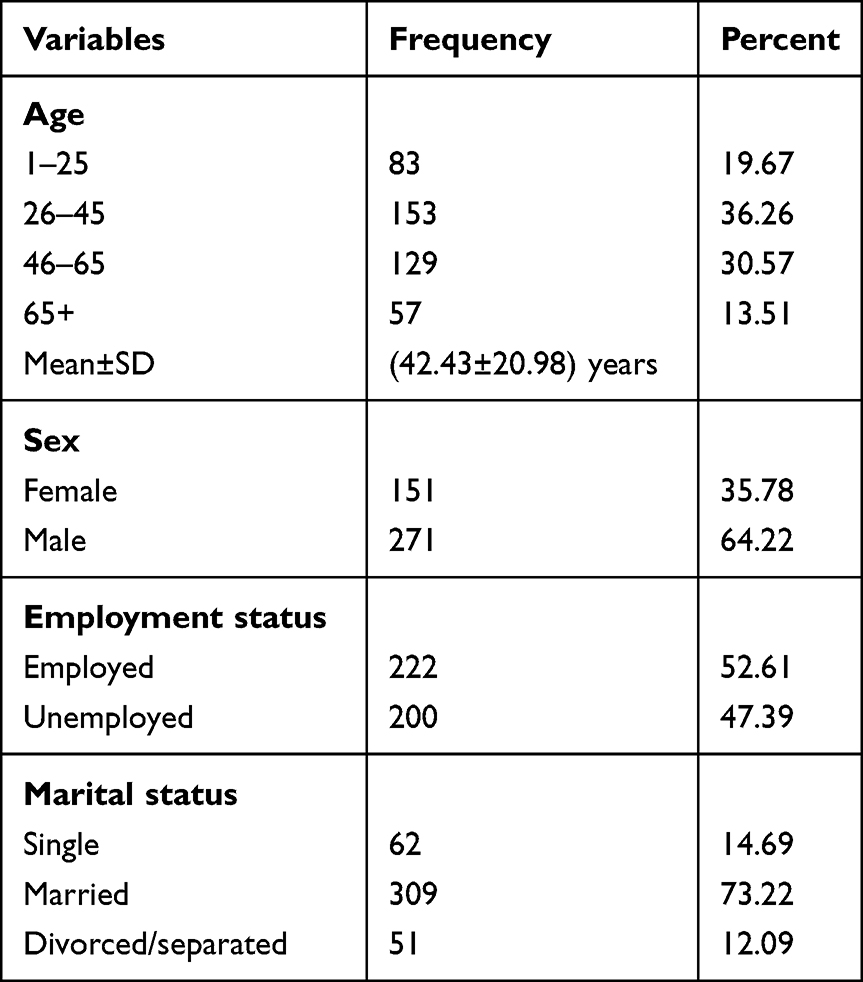 |
Table 1 Socio-Demographic Characteristics of COVID-19 Patients Admitted to COVID-19 Treatment Center in Harar, Eastern Ethiopia, 2021 |
Comorbidities Among COVID-19 Patients
More than half (52.4%) of the COVID-19 patients were presented with comorbid conditions. Diabetes mellitus (DM) accounted for the highest prevalence (22.3%), followed by hypertension (19.9%) and cardiovascular diseases (17.1%). Comorbid conditions such as renal disease (6.9%), lung diseases (9.2%), retroviral infections (RVI) (5.7%), and others (cancer, liver diseases) (5.7%) were identified in patients with COVID-19 diseases (Table 2).
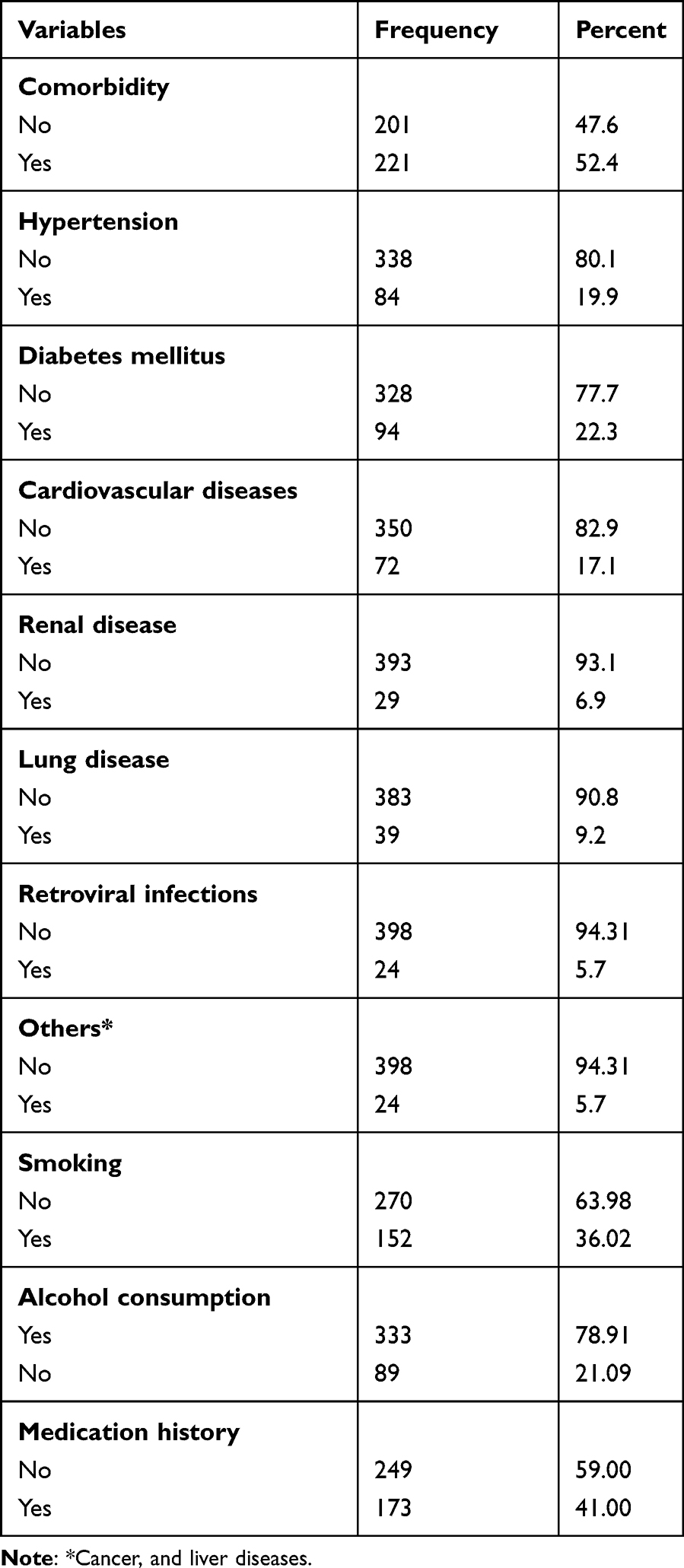 |
Table 2 Comorbidities and Other Risk Factors Among Patients with COVID-19 Admitted to the COVID-19 Treatment Center in Harar, Eastern Ethiopia, 2021 |
Coexisting Comorbidities Among COVID-19 Patients
From a total of 221 patients presented with comorbidities, 117 (27.7%) presented with single comorbid conditions, whereas 70 (16.6%), 27 (6.4%), and 7 (1.7%) of them presented with two, three, and four coexisting comorbid conditions respectively (Figure 1). Hypertension is more prevalent among age group >65 years than those aged less than 24 years (43.9% vs 3.6%). Diabetes is more prevalent among age group >65 years than those aged less than 24 years (33.3% vs 7.2%) (Table 3).
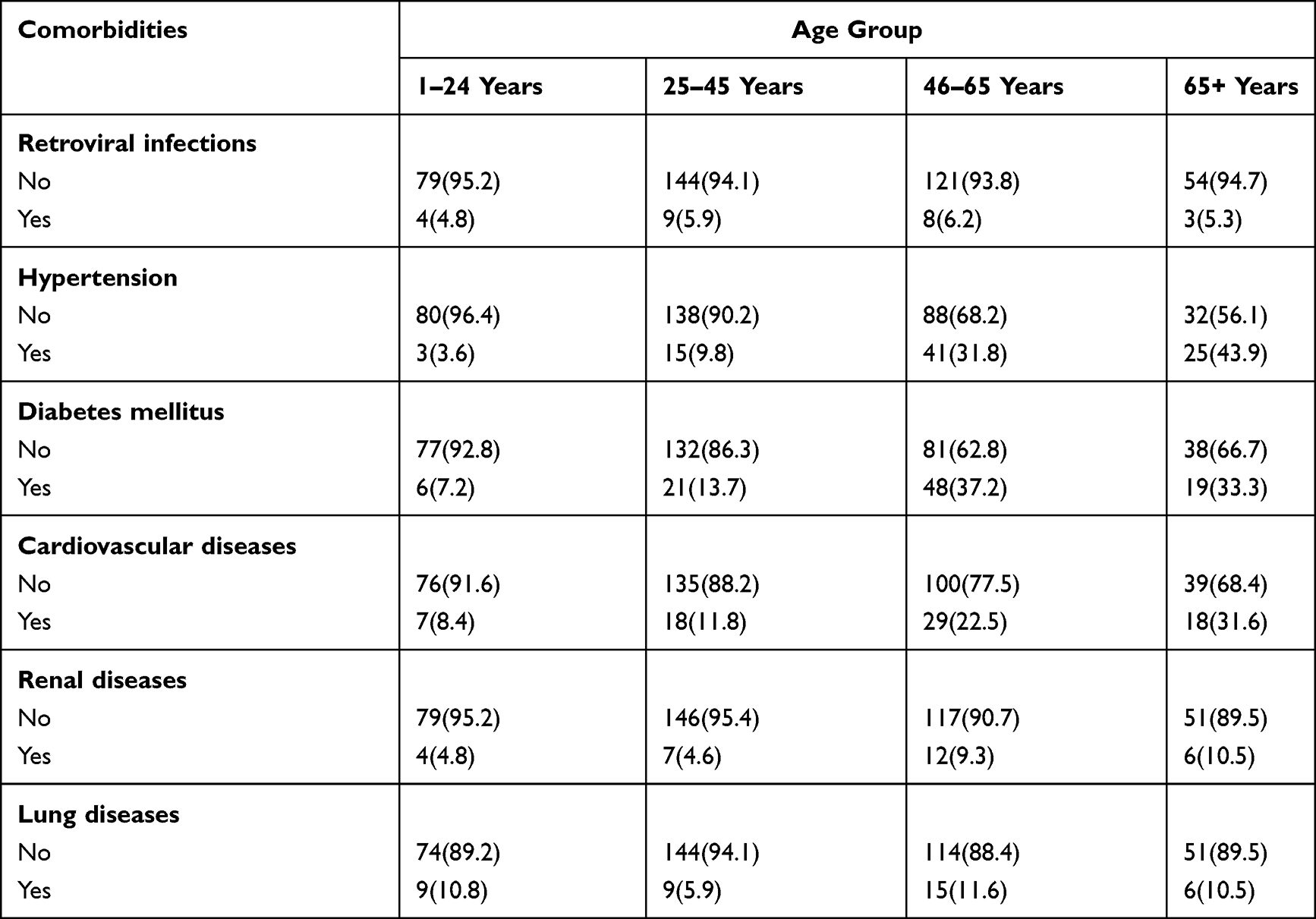 |
Table 3 Comorbidities Distribution Among Different Age Groups Among Patients with COVID-19 Admitted to the COVID-19 Treatment Center in Harar, Eastern Ethiopia, 2021 |
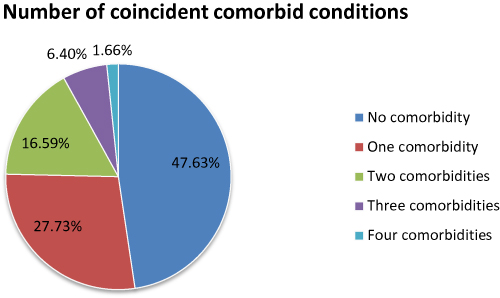 |
Figure 1 Number of coexisting comorbid conditions among COVID 19 patients admitted at Hospitals in Harar, Eastern Ethiopia, 2021. |
Factors Associated with Severity of COVID-19 Infections
More than one third (34.6%) of the admitted COVID-19 patients were in severe clinical stages. In bivariate analysis variables with p<0.25 were retained for multivariable logistic regressions. In bivariate analysis age, marital status, employment status, hypertension, diabetes mellitus, cardiovascular diseases, renal diseases, smoking status and alcohol consumption were found to be significant. After adjusting for the effect of confounders in multivariable logistic regression model marital status, hypertension, diabetes mellitus, and cardiovascular diseases were associated with severity of COVID-19 cases.
The odds of severe clinical stage were 4.56 times higher among divorced/separated compared to single (AOR=4.56; 95% CI: 1.40, 14.76). The odds of severe clinical stage were 2.08 times higher among hypertensive patients compared to non-hypertensive (AOR=2.08; 95% CI: 1.09, 3.97). The odds of severe clinical stage were 3.31 times higher among diabetic patients compared to non-diabetics (AOR=3.31; 95%:1.84, 5.98).
The odds of severe clinical stage were 4.22 times higher among cardiovascular patients compared to those without cardiovascular diseases (AOR=4.22; 95% CI: 2.18, 8.15) Table 4.
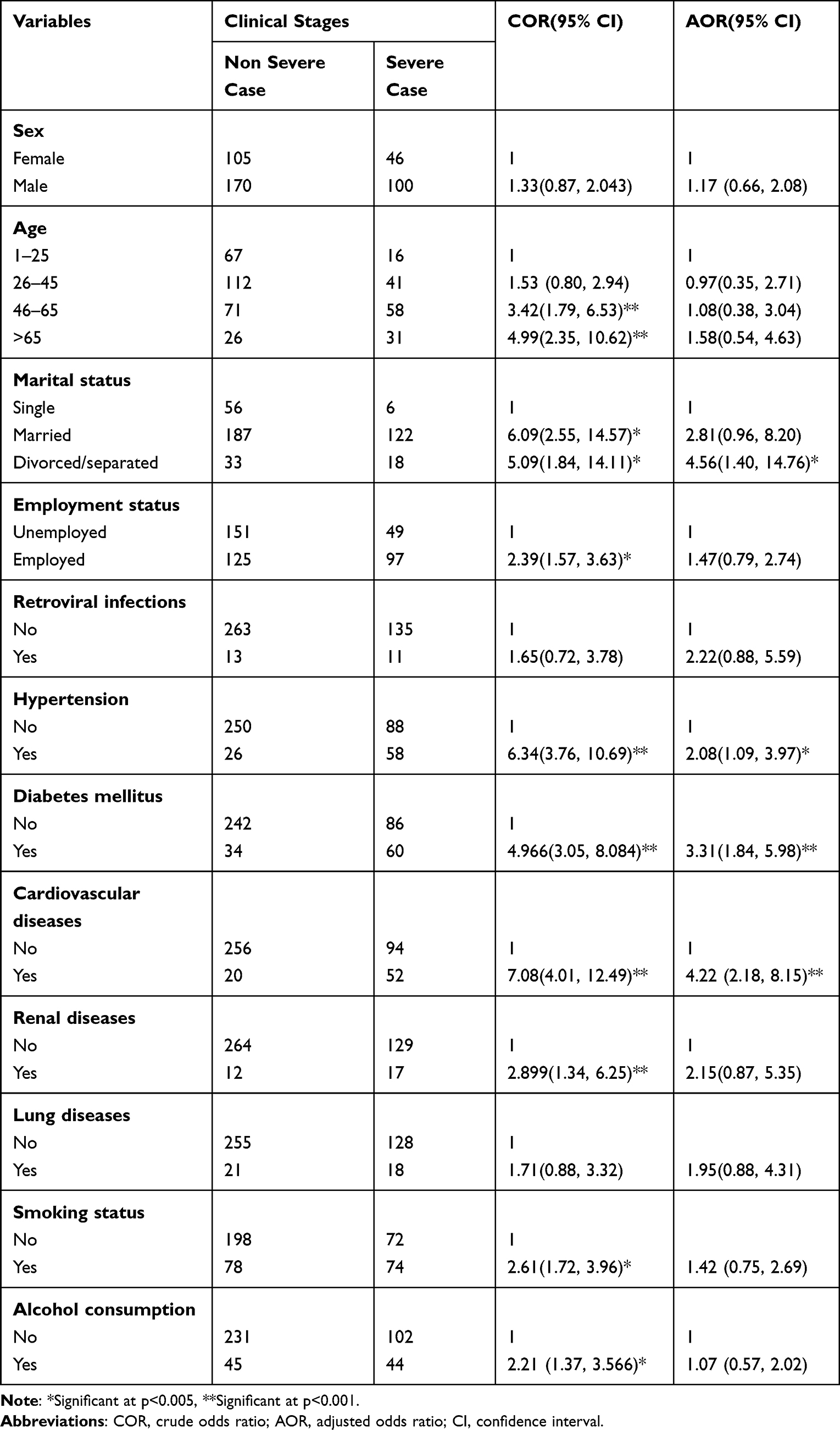 |
Table 4 Multivariable Logistic Regressions for Factors Associated with Severe Outcomes of COVID-19 Among Patients Admitted to COVID-19 Treatment Center in Harar, Eastern Ethiopia, 2021 |
Discussions
More than half (52.4%) of the COVID-19 patients presented with comorbid conditions. Diabetes was the most common comorbid (22.3%) condition in our study which was much higher than the incidence of diabetes found in a study conducted in Wuhan, China (10% to 15%).13–16 The second most prevalent comorbid condition in the confirmed COVID-19 patients was hypertension (19.9%), which was comparable with findings from systematic and meta-analysis conducted in China and Taiwan (21%).9
In the current study cardiovascular comorbidity was found to increase the odds of severe clinical stage among COVID-19 patient. This finding is supported with findings from Saudi Arabia.17 Another study also identified cardiac diseases as risk factors for the worse outcomes in COVID-19 patients.18 This association might be justified by the fact that SARS-CoV infections lead to immune dysregulation that could help explain the escalated risk of cardiac diseases, bone diseases and malignancy.19 Therefore, immune disruption and persistent inflammation might lead to poor clinical outcomes in patients with COVID-19. Another evidence suggests the possibility that SARS-CoV-2 infection could cause arrhythmias.20
Hypertension was found to be significantly associated with severe outcomes of COVID-19 patients. Studies support this finding, that hypertensive patients are more vulnerable to develop serious complications of COVID-19.21 The association of hypertension and serious COVID-19 involves endothelial dysfunction and renin angiotensin system (RAS) dysregulation. SARS-CoV entry to the host cell involves angiotensin converting enzyme 2 (ACE2), which is an important enzyme in blood pressure homeostasis.21 Therefore, alteration of RAS may affect the development and progression of COVID-19 to severe clinical stages. Moreover, studies have found increased circulating levels of HSP60 (60-kDa heat shock protein) in hypertensive patients, as well as enhanced HSP60 expression and membrane translocation in the hypertrophic myocardium.7 These could provide a possible pathophysiological explanation of the severe course and worse outcome of severe acute respiratory syndrome coronavirus 2 infection in hypertensive patients, related to hyperinflammatory response and cytokine storm development during the third phase of the disease.
Being a diabetic patient increased the odds of severe outcomes of COVID-19 compared to those non-diabetics. Another study also revealed that diabetic patients have increased severe outcomes of the disease and have been linked to more hospital admissions and intensive care unit admissions.16 A cohort study that recruited a total of 7337 patients with COVID-19 shown that those with type 2 diabetes required increased interventions for their hospital stay that were non-diabetic.22 The association of diabetes and severe outcomes of COVID-19 may be due to the effect of diabetes on viral entry into cell and inflammatory response to the infection.16 This implies, parallel with management of COVID-19, the importance of controlling blood glucose in patients who are infected with COVID-19. Moreover, evidence suggests that in most groups of high risk patients, common mechanism favoring development of excessive inflammation and cytokine storm is persistently present proinflammatory situation.23,24 Such chronic proinflammatory state can occur either due to hypersecretion of proinflammatory adipokines in obese patients,24 lack of anti- inflammatory signaling in diabetic, and insulin-resistant patients.25
Marital status was significantly associated with severe outcomes of COVID-19. Divorced/separated participants had higher odds of severe outcomes of COVID-19 than those single patients. This may be because patients who are divorced and separated from their partner may have less social and psychological support that could lead them to severe clinical outcomes.26
Conclusions
The comorbid conditions were presented in more than half of the COVID-19 patients. Diabetes, hypertension, cardiovascular diseases, and marital status are significant predictors of severe outcomes of COVID-19. This implies that patients with comorbidities suffer from severe COVID-19 outcome that may eventually lead to increased risk of death. Therefore, identifying the people with chronic comorbidities as a risk group would help to anticipate and prevent the serious outcomes of COVID-19 infection. Moreover, giving special attention for patients who are separated or divorced from their partner may help reduce severe outcomes from COVID-19 infections.
Data Sharing Statement
The datasets used in this study can be available from correspondent author up on reasonable request.
Acknowledgment
The authors are thankful to Hiwot Fana Hospital for an authorization to access the data. The authors are also grateful to data collectors for their genuine effort to bring reliable data and participants for their participation.
Author Contributions
All authors made a significant contribution to the conception, study design, execution, data acquisition, analysis and interpretation. All authors took part in drafting, critically reviewing the article, gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Yang J, Zheng Y, Gou X, et al. Prevalence of comorbidities in the novel Wuhan coronavirus (COVID-19) infection: a systematic review and meta-analysis. Int J Infect Dis. 2020;10:
2. Guan W-J, Liang W-H, Zhao Y, et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis. Eur Respir J. 2020;55(5):2000547. doi:10.1183/13993003.00547-2020
3. Grasselli G, Zangrillo A, Zanella A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020;323(16):1574–1581. doi:10.1001/jama.2020.5394
4. Cummings MJ, Baldwin MR, Abrams D, et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: a prospective cohort study. Lancet. 2020;395(10239):1763–1770. doi:10.1016/S0140-6736(20)31189-2
5. Wu C, Chen X, Cai Y, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. 2020;180(7):934–943. doi:10.1001/jamainternmed.2020.0994
6. Schuetz P, Castro P, Shapiro NI. Diabetes and sepsis: preclinical findings and clinical relevance. Diabetes Care. 2011;34(3):771–778. doi:10.2337/dc10-1185
7. Jakovac H. COVID-19 and hypertension: is the HSP60 culprit for the severe course and worse outcome? Am J Physiol Heart Circulat Physiol. 2020;319(4):H793–H796. doi:10.1152/ajpheart.00506.2020
8. Li X, Xu S, Yu M, et al. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J Allerg Clin Immunol. 2020;146(1):110–118. doi:10.1016/j.jaci.2020.04.006
9. Baradaran A, Ebrahimzadeh MH, Baradaran A, Kachooei AR. Prevalence of comorbidities in COVID-19 patients: a systematic review and meta-analysis. Archiv Bone Joint Surg. 2020;8(Suppl 1):247. doi:10.22038/abjs.2020.47754.2346
10. Sanyaolu A, Okorie C, Marinkovic A, et al. Navigating the diagnostics of COVID-19. SN Comprehens Clin Med. 2020;2(9):1393–1400. doi:10.1007/s42399-020-00408-8
11. World Health Organization. Food, medicine and healthcare administration and control authority of Ethiopia. In: Standard Treatment Guidelines for General Hospital. World Health Organization; 2015.
12. National Institutes of Health. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Clinical Spectrum of SARS-CoV-2 Infection. USA: National Institutes of Health. 2021:48-56.
13. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
14. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
15. Liu K, Fang -Y-Y, Deng Y, et al. Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province. Chin Med J. 2020;133(9):1025. doi:10.1097/CM9.0000000000000744
16. Singh AK, Gupta R, Ghosh A, Misra A. Diabetes in COVID-19: prevalence, pathophysiology, prognosis and practical considerations. Diabetes Metabol Syndr Clin Res Rev. 2020;14(4):303–310. doi:10.1016/j.dsx.2020.04.004
17. Shaikh FS, Aldhafferi N, Buker A, et al. Comorbidities and risk factors for severe outcomes in COVID-19 patients in Saudi Arabia: a retrospective cohort study. J Multidiscip Healthc. 2021;14:2169. doi:10.2147/JMDH.S317884
18. Khan A, Althunayyan S, Alsofayan Y, et al. Risk factors associated with worse outcomes in COVID-19: a retrospective study in Saudi Arabia. East Mediterran Health J. 2020;26:11. doi:10.26719/emhj.20.130
19. Moni MA, Liò P. Network-based analysis of comorbidities risk during an infection: SARS and HIV case studies. BMC Bioinform. 2014;15(1):1–23. doi:10.1186/1471-2105-15-333
20. Morais-Almeida M, Pité H, Aguiar R, Ansotegui I, Bousquet J. Asthma and the coronavirus disease 2019 pandemic: a literature review. Int Arch Allergy Immunol. 2020;181(9):680–688. doi:10.1159/000509057
21. Muhamad S-A, Ugusman A, Kumar J, Skiba D, Hamid AA, Aminuddin A. COVID-19 and hypertension: the what, the why, and the how. Front Physiol. 2021;12:589. doi:10.3389/fphys.2021.665064
22. Zhu L, She Z-G, Cheng X, et al. Association of blood glucose control and outcomes in patients with COVID-19 and pre-existing type 2 diabetes. Cell Metab. 2020;31(6):1068–1077. e1063. doi:10.1016/j.cmet.2020.04.021
23. Kralj M, Jakovac H. Vitamin D and COVID-19 in an immunocompromised patient with multiple comorbidities—a case report. Clin Case Rep. 2021;9(4):2269–2275. doi:10.1002/ccr3.4010
24. Mohammad S, Aziz R, Al Mahri S, et al. Obesity and COVID-19: what makes obese host so vulnerable? Immun Ageing. 2021;18(1):1–10. doi:10.1186/s12979-020-00212-x
25. Abu-Farha M, Al-Mulla F, Thanaraj TA, et al. Impact of diabetes in patients diagnosed with COVID-19. Front Immunol. 2020;10:3112. doi:10.3389/fimmu.2019.03112
26. Yang X, Yang X, Kumar P, Cao B, Ma X, Li T. Social support and clinical improvement in COVID-19 positive patients in China. Nurs Outlook. 2020;68(6):830–837. doi:10.1016/j.outlook.2020.08.008
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Willingness to receive the COVID-19 vaccine and associated factors among residents of Southwestern Ethiopia: A cross-sectional study
Jabessa D, Bekele F
Patient Preference and Adherence 2022, 16:1177-1185
Published Date: 3 May 2022
Baseline Thrombocytopenia and Disease Severity Among COVID-19 Patients, Tibebe Ghion Specialized Hospital COVID-19 Treatment Center, Northwest Ethiopia
Asrie F, Tekle E, Gelaw Y, Dagnew M, Gelaw A, Negash M, Kassa E, Bizuneh S, Wudineh D
Journal of Blood Medicine 2022, 13:315-325
Published Date: 10 June 2022
COVID-19 Case Fatality Rate and Factors Contributing to Mortality in Ethiopia: A Systematic Review of Current Evidence
Girma D, Dejene H, Adugna L, Tesema M, Awol M
Infection and Drug Resistance 2022, 15:3491-3501
Published Date: 4 July 2022
Impact of the COVID-19 Pandemic on Breastfeeding Support Services and Women’s Experiences of Breastfeeding: A Review
Lubbe W, Niela-Vilén H, Thomson G, Botha E
International Journal of Women's Health 2022, 14:1447-1457
Published Date: 6 October 2022
Re-Emerging COVID-19: Controversy of Its Zoonotic Origin, Risks of Severity of Reinfection and Management
Chala B, Tilaye T, Waktole G
International Journal of General Medicine 2023, 16:4307-4319
Published Date: 20 September 2023