")
Back to Journals » International Journal of Women's Health » Volume 14
Impact of the COVID-19 Pandemic on Breastfeeding Support Services and Women’s Experiences of Breastfeeding: A Review
Authors Lubbe W, Niela-Vilén H, Thomson G, Botha E
Received 18 June 2022
Accepted for publication 8 September 2022
Published 6 October 2022 Volume 2022:14 Pages 1447—1457
DOI https://doi.org/10.2147/IJWH.S342754
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Welma Lubbe,1 Hannakaisa Niela-Vilén,2 Gill Thomson,3 Elina Botha4
1School of Nursing Science/NuMIQ Research Focus Area, Faculty of Health Sciences, North-West University, Potchefstroom, South Africa; 2University of Turku, Department of Nursing Science, Turku, Finland; 3School of Community Health and Midwifery, University of Central Lancashire, Preston, UK; 4School of Social Services and Health Care, Tampere University of Applied Sciences, Tampere, Finland
Correspondence: Welma Lubbe, Email [email protected]
Objective: The aim of this systematic review was to explore the impact of the COVID-19 pandemic on breastfeeding support services and continuation rates.
Methods: Electronic searches were undertaken in seven databases: Academic Search Complete, Springer Nature Journals, CINAHL Medline, Health Source: Nursing/Academic Edition, Masterfile premier, and SocINDEX. Publications following the COVID-19 pandemic between January 2020 and March 2022 were searched for using the following keywords: impact or effect or influence and breastfeeding support and breastfeeding continuation and COVID-19 or coronavirus. Fifteen studies were included for investigation and extracted to identify seven themes related to breastfeeding support during COVID-19.
Results: Factors which impacted breastfeeding support during the COVID-19 pandemic included separation, lack of skin-to-skin contact, insufficient support, online breastfeeding support, the impact of the pandemic on breastfeeding rates and experiences, fears of the pandemic, and the need for additional support. The pandemic mostly influenced breastfeeding support negatively, with a small exception occurring where some mothers experienced lockdown as positive since it protected the mother-infant dyad from unwanted visitors. Virtual breastfeeding support was introduced in many contexts; however, practitioners and mothers reported that this could not replace the need for face-to-face support.
Conclusion: Breastfeeding is a lifesaving intervention, especially in the face of a disruption such as a pandemic. This work highlights the need for clear, consistent, and evidence-based information about risks, and for key practices to be maintained including not separating mothers and infants, promoting skin-to-skin contact, and ensuring availability of high-quality breastfeeding support.
Keywords: breastfeeding support, COVID-19, coronavirus, pandemic, effect
Introduction
The COVID-19 pandemic has disrupted everyday life since December 20191–3 when the outbreak began in Wuhan, central China. Apart from mortality and morbidity, the pandemic has also impacted all areas of health service delivery including breastfeeding.4 At the start of the pandemic, the medical and scientific community lacked information regarding the route of transmission of the virus, thus many preventative measures were launched to protect mothers and babies. When it became evident that it is a respiratory virus, the next question was whether mothers could infect their infants during breastfeeding.
Leaning towards the side of caution, exposed or infected mothers and babies were separated to prevent potential transmission.5 As more evidence became available highlighting that infants are unlikely to contract the virus, some practices changed and guidelines were published towards zero separation.6 However, despite these guidelines, some facilities did not support or enable breastfeeding particularly when mothers were exposed to or have contracted COVID-19. During the COVID-19 pandemic, breastfeeding support services, especially in hospitals, were limited if not ceased. The reason was to prevent potential transmission of the virus. Hospitals and healthcare facilities restricted all non-essential staff’s access to their institutions. In some cases, this even meant that parents were not allowed into the neonatal intensive care unit (NICU) for skin-to-skin contact or breastfeeding.7–10 A review by Lalor et al concluded that “parental experiences highlighted how maternity care during the COVID-19 pandemic did not adhere to World Health Organization standards of quality maternity care”.11
Breastfeeding and mother-infant closeness are strongly connected. Mother-infant separation therefore presents several challenges and complications. When separated, the infant is not being provided with the health benefits associated with breastfeeding, such as immuno-protection, transfer of antibodies,12 protection against diarrhea and severe respiratory syncytial virus (RSV) and being hospitalized.13 Separation of the mother and infant poses a risk for malnutrition and even death.13,14 While separation inevitably decreases breastfeeding rates, the mother-baby dyad is also deprived of the benefits of stimulating hormones and bonding.15–17 In order to protect and support breastfeeding, mothers and infants should never be separated, thus avoiding separation has been an essential component of breastfeeding support programs such as the Baby-friendly Hospital Initiative (BFHI)18 and Neonatal-BFHI.19 Further, immediate and early skin-to-skin contact is strongly recommended to support the initiation of breastfeeding.20
Breastfeeding support is rooted within international and national policies and recommendations, but in everyday life, it may range from mothers receiving peer or partner support to structured support provided by a professional.21 In this paper, breastfeeding support refers to practices and policies in birth hospitals and after discharge, as well as online methods such as healthcare professionals providing group or one-to-one breastfeeding support via Zoom, Microsoft Teams or other digital platforms.
Several practice advisories or guidelines to support breastfeeding, especially during a pandemic such as COVID-19, are available;19 however, little has been published to date to evaluate the influence of the pandemic on breastfeeding support and continuation. This review aimed to explore the impact of the COVID-19 pandemic on breastfeeding support services and continuation rates across the world and in all settings.
Materials and Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidance.22 The review question was formulated using the PIO format: Population: breastfeeding mothers, Intervention: COVID-19 pandemic, Outcome: breastfeeding support and continuation. The review question was: How did the COVID-19 pandemic impact breastfeeding support services and continuation rates?
Data Sources and Search Strategy
The following seven electronic databases were searched: Academic Search Complete (n=102), Springer Nature Journals (n=70), CINAHL with full text (n=13), Medline (n=6), Health Source: Nursing/Academic Edition (n=5), Masterfile premier (n=3), and SocINDEX with full text (n=1). The total number of hits at this point was 200. Keywords for this search (identified after various pilot searches) were impact or effect or influence and breastfeeding support and breastfeeding continuation and COVID-19 or coronavirus. The review question and keywords were agreed upon by all reviewers. An academic librarian was also consulted to support the development of the search strategy.
As we were only interested in studies undertaken in relation to the pandemic, we focused on studies published from 2020 and up to when the initial searches were undertaken (March 2022). Additional articles from reference lists were identified during the critical appraisal process and any suitable articles published between March and May 2022 were included (see Figure 1: PRISMA diagram).
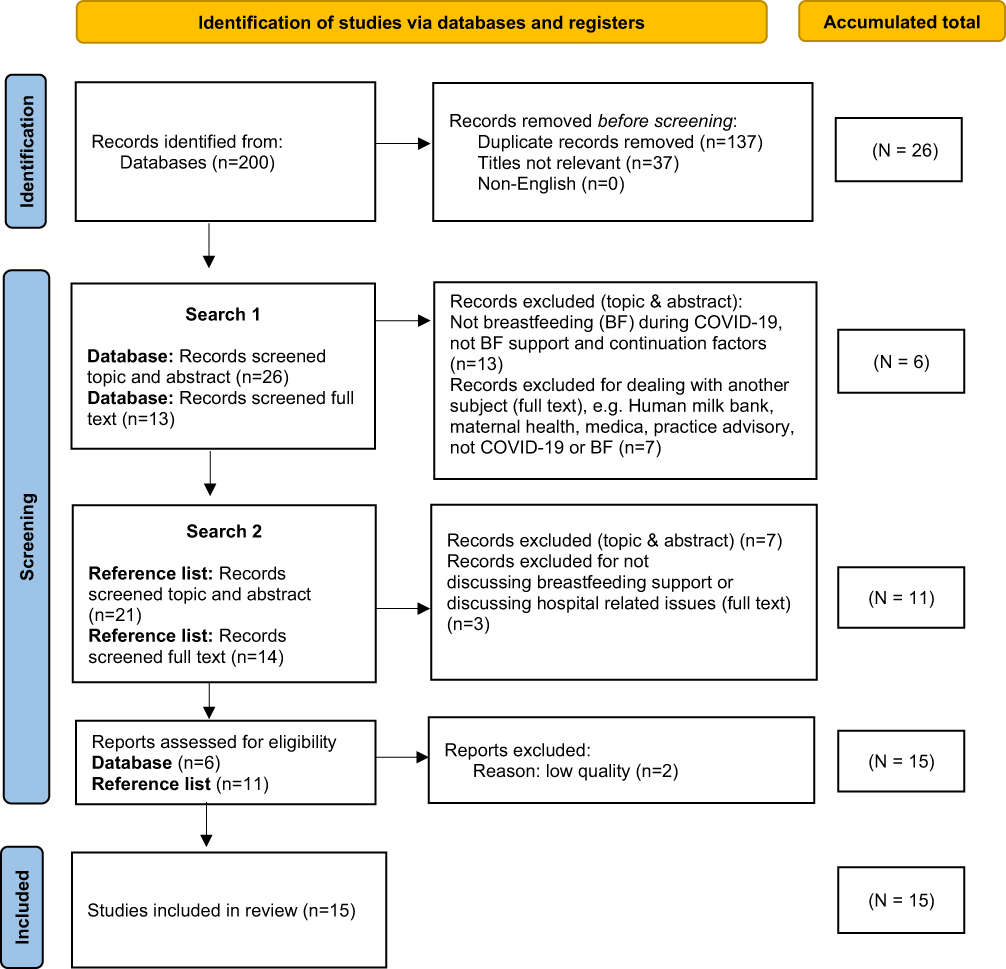 |
Figure 1 PRISMA diagram. Notes: Figure 1 depicts the flow diagram according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) used in this review to demonstrate the flow of information through the different phases. It maps the number of articles identified, included and excluded during the two searches, as well as reasons for exclusions. Adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. International Journal of Surgery 2021; 88: 105906.22 |
Inclusion and Exclusion Criteria
Studies were included if they discussed breastfeeding support (provided by healthcare professionals or peer-to-peer support) during or related to the COVID-19 pandemic and reported on primary research, discussion pieces as well as reviews. Studies reporting on breastfeeding rates and the effect of support interventions during COVID-19 were also included. Only studies written in English were included, since it is the language shared by all the review team members. However, no studies in other languages were located. Articles were excluded if they only suggested that breastfeeding support should be provided, but did not actually explore the effect of support, or if the support did not refer specifically to the COVID-19 pandemic (refer to Figure 1).
Screening
In Figure 1, the number of articles identified and excluded at each stage of the screening process is detailed. Although 200 articles were originally identified from searching the databases, 137 were duplicates and excluded before screening, using the database search engine of the first author’s institution. A further 37 articles had titles that were clearly not answering the review question and were excluded. The initial screening search and deduplication were undertaken by WL. Two reviewers (WL and HNV) independently reviewed the titles and abstracts of the remaining 26 articles to determine whether full text should be read. While some of the articles had titles that suggested it may be relevant to the review question, upon reading the abstract, a further 13 were excluded. The full text of the remaining 13 articles was screened by WL and HNV, and another seven articles were excluded for reasons such as the articles discussing human milk banking, maternal health, the media, or not discussing COVID-19 or breastfeeding. At this point, six articles were eligible for inclusion in the critical appraisal phase.
The reference lists of eligible articles were then searched, and another 21 articles were identified. Seven were excluded at the abstract review stage for similar reasons as reported above. The full texts of the remaining 14 articles were read with a further three excluded for not discussing breastfeeding support or discussing hospital-related issues. Overall, this led to a final sample of 17 articles included for critical appraisal.
Study Quality Assessment Checklists and Procedures
The Johns Hopkins tools for research and non-research were used to determine the rigor and quality of each study (with permission).23 These tools assess research design, sampling, measurement, ethics, and outcomes. The evidence level of each article is rated from Level 1 being the highest level of evidence demonstrated through randomized controlled trials (RCTs), systematic reviews and meta-analyses, to Level 5 being the lowest and including experiential and non-research evidence, such as integrative reviews, literature reviews, quality improvement and program evaluations, as well as case reports and expert opinions. Within each of these levels, a quality rating was also given as: A – High quality, B – Good quality or C – Low quality or major flaws. Articles with a C rating were omitted from the review. Two reviewers (WL, HNV) independently rated the quality of all 17 articles with agreements made by consensus. Two articles were excluded due to poor quality of evidence, leaving a total of 15 articles for inclusion. Their evidence level and quality ratings are presented in Table 1.
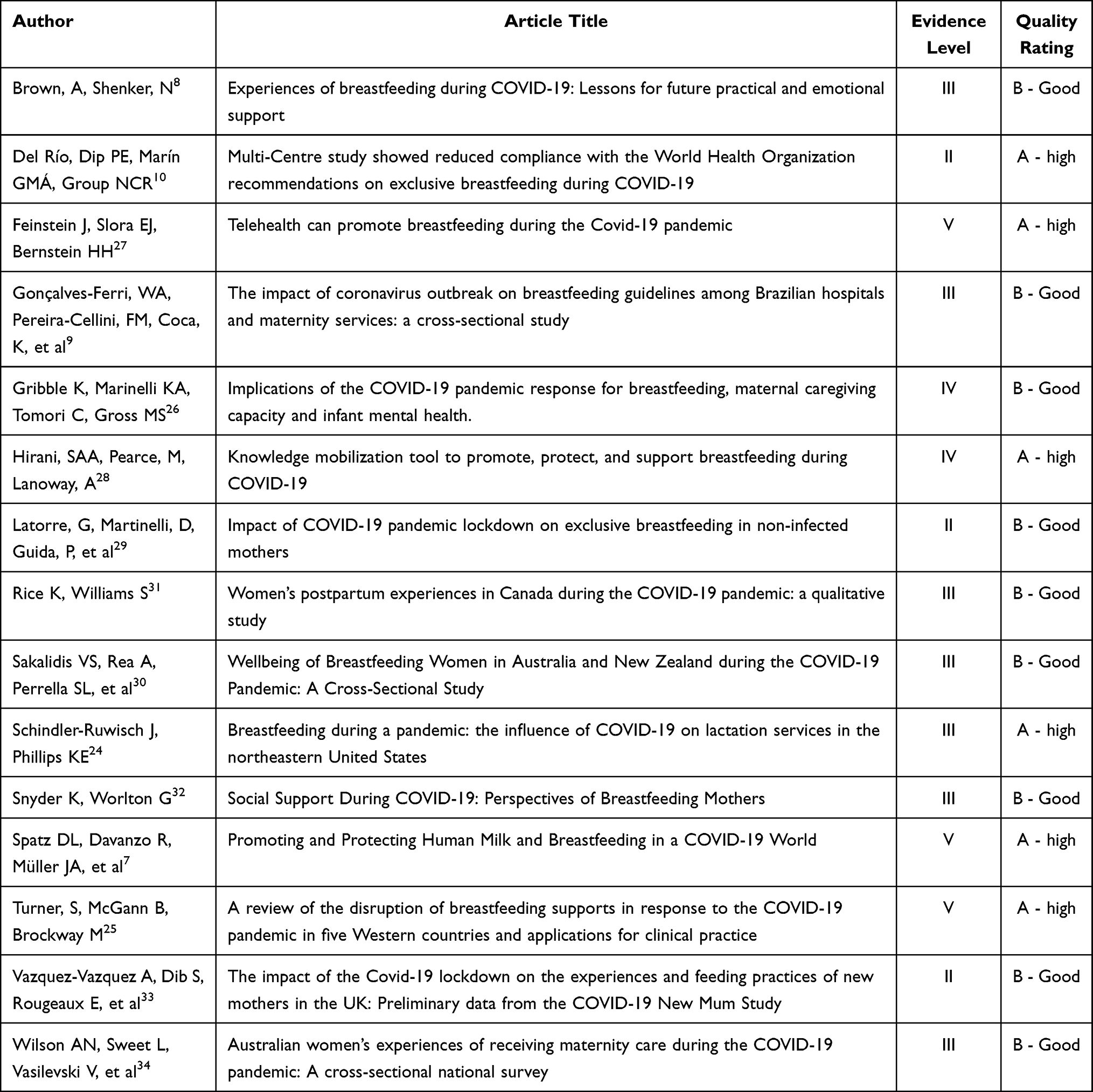 |
Table 1 Evidence Level and Quality Rating of Articles Included for Synthesis |
Results
Data Extraction Strategy
Fifteen studies of good quality and high levels of evidence were included as the final sample for this review. Data were extracted into a data extraction table (EB, GT) according to the following elements: Primary author(s), year and country of publication, purpose, design, sample, and key findings.
Synthesis of the Extracted Evidence
GT analyzed the data by organizing the information into descriptive themes and subthemes, with all analytical decisions shared and agreed upon by all authors. Below, seven themes are presented that detail the key factors which impacted breastfeeding support and women’s experiences of breastfeeding during the COVID-19 pandemic: separation, lack of skin-to-skin contact, insufficient support, online breastfeeding support, the impact of the pandemic on breastfeeding experiences, fears of the pandemic, and the need for additional support.
Separation
Some of the papers highlighted the impact of separation between mothers and infants and between mothers and birth companions on breastfeeding rates.24,25 The papers by Gribble et al26 and Brown and Shenker8 highlighted the unnecessary and detrimental impact of separating mother-infant dyads after birth, and particularly for those with additional vulnerabilities due to being born premature and/or sick, with Gribble et al26 arguing how this occurred “despite no evidence of risks”. In the paper by Brown and Shenker, approximately a quarter of mothers who had an infant in the neonatal unit were told that they could not visit their infant, and this lack of contact was significantly associated with breastfeeding cessation.
The study by Del Río et al10 found a strong positive correlation in breastfeeding rates among mothers who had a companion present during the birth (r = 0.833), and a strong negative correlation between the percentage of newborn infants who were receiving exclusive breastfeeding at discharge and those who were separated from their mothers at birth (r = −0.862). Gonçalves-Ferri et al9 undertook a cross-sectional multicenter study at 24 hospitals in Brazil. They found that distancing and breastfeeding recommendations were carried out in all hospitals, with one hospital recommending dyad separation, and in the majority (83.3%), a companion was forbidden.
Lack of Skin-to-Skin Contact
Several studies reported on how the pandemic had restricted mother-infant skin-to-skin contact after birth. Brown and Shenker8 found that a small number of women surveyed were not supported to have skin-to-skin contact with their infant (7.8%) or to breastfeed soon after birth (4.6%). Del Rio et al10 found a strong positive correlation between the percentage of newborn infants who received exclusive breastfeeding at discharge and infants who received immediate skin-to-skin contact after birth. Gonçalves-Ferri et al9 also reported that most of the hospitals surveyed (79.1%) did not encourage or enable skin-to-skin contact immediately after birth. Moreover, Spatz et al7 highlighted that despite recommendations from the WHO to continue to promote early, direct breastfeeding and skin-to-skin contact, these recommendations were not being followed in the clinical setting.
Insufficient Support
The lack of professional support during the pandemic was highlighted, often associated with limited in-person breastfeeding support in the hospital unit and within the community,8,24,25,31 with some women reporting that they felt they were doing it “on their own”.34 While women were generally able to access different types of support, eg, health professionals and lactation consultations,32 the quality and quantity of support were restricted. However, it is interesting to note that in the study by Vazquez-Vazquez, it was found that while 45% of women reported insufficient feeding support during lockdown, between 57% and 69% of women reported decreased feeding support before lockdown.33
Spatz et al7 argued how families were not receiving breastfeeding support largely due to a lack of knowledge and miscommunication about the impact of COVID-19 on human milk, and how the care of childbearing families had been de-prioritized during the pandemic. Brown and Shenker, in a survey of United Kingdom (UK) mothers, highlighted how a lack of professional support was the most common reason for breastfeeding cessation. While only small numbers referred to a lack of support in hospital (21.2%), 70.3% of the sample highlighted a lack of face-to-face contact once home. Mothers reported that they struggled to relay their issues over the telephone and missed having someone observe their breastfeeding to help rectify any positioning issues. There were complaints of women not being given information on expressing milk, with under 40% perceiving that they received sufficient practical or emotional support, while those who considered that they had sufficient support were the most likely to continue breastfeeding. They also found that not being able to attend breastfeeding support groups and the closure of baby clinics were significantly associated with breastfeeding discontinuation. From those who had older children, 67% considered that they had had less support during the pandemic than with their other children.
A survey study undertaken in America by Schindler-Ruwisch highlighted difficulties among lactation professionals in providing support when wearing personal protective equipment.24 For example, they referred to how the protective mask made their speech muffled and that they were unable to use their mouths to demonstrate infant latch, thereby negating the support they could provide. The Brazilian study by Gonçalves-Ferri et al9 found that 98.5% of the hospital services surveyed allowed breastfeeding while implementing respiratory hygiene practices to prevent transmission of COVID-19. However, most did not encourage breastfeeding in the first hour after birth (87.5%).
Some of the studies reported the impact of early hospital discharge, thereby limiting the amount of support to help women establish breastfeeding.7,24,33 In the study by Gonçalves-Ferri et al,9 it was found that hospital discharge was recommended within 24 to 48 hours in all but one hospital, whereas prior to the pandemic, neonatal discharge occurred after more than 48 hours. Furthermore, while all the hospitals surveyed recommended maintaining breastfeeding at home, there was a lack of community support reported in 83.3% of the hospital sites.
A particular issue reported in the study by Brown and Shenker related to a lack of specialist support in diagnosing and dividing tongue ties.8 This meant that women were having to express due to pain or poor latch, introduce formula, and stop breastfeeding prematurely. Issues of newborn weight not being taken consistently, coupled with a lack of knowledge of infant weight leading to increased use of formula, were also reported in the study by Schindler-Ruwisch.24
Online Breastfeeding Support
The move to providing online breastfeeding support via virtual visits had mixed results in some of the studies. For example, the study by Rice reported that online breastfeeding support was uniformly experienced as unhelpful.31 In the study by Schindler-Ruwisch,24 however, most participants reported that their patients largely preferred telehealth contacts (phone, FaceTime, Duo, Zoom, MyChart, WhatsApp, or HouseParty app). The professionals who provided the groups felt that they were less effective.24 Furthermore, in the review by Turner et al,25 it was highlighted how mothers expressed difficulties in receiving professional help with breastfeeding techniques online. Conversely, in the paper by Feinstein,27 converting an in-person breastfeeding support event to a telehealth environment, with parents viewing online breastfeeding sessions, was positively received. The authors argued that online methods may provide a solution for better breastfeeding support as they increased accessibility to free, high-quality telehealth care. Although, they acknowledged the challenges of mothers not being as comfortably able to demonstrate breastfeeding problems to the lactation experts when compared to face-to-face contact.
Impact of the Pandemic on Breastfeeding Rates and Experience
Several studies explored how the pandemic has impacted the prevalence of breastfeeding initiation and duration and women’s experiences of breastfeeding. Brown and Shenker8 asked participants in the UK whether they felt the lockdown had a positive or negative impact on their breastfeeding experience. Overall, 41.8% felt it was positive, 29.5% neutral, and 27.0% negative. A further 1.7% were unsure of its impact. The authors found little difference in mothers’ intentions to never introduce formula between those who gave birth before (70.6%) or after (67.7%) the pandemic. Furthermore, similar percentages of women who gave birth before and after the pandemic breastfed exclusively for longer than intended. This was similar to the findings by Vazquez-Vazquez who found that breastfeeding initiation did not differ between pre- and post-pandemic groups.33 However, in the study by Latorre et al29 in Italy, it was found that when comparing breastfeeding practices among women who gave birth before or during the pandemic, the use of infant formula was higher during the pandemic, and exclusive breastfeeding rates were reduced (74.2% vs 32.8%). Furthermore, the study by Sakalidis et al30 undertaken in Australia reported a reduction in the odds of exclusive breastfeeding as infant age increased, associated with low milk supply. Turner et al25 explored how the pandemic restrictions and positive COVID-19 status of the mother impacted breastfeeding initiation, duration, and mothers’ self-reported breastfeeding experiences in Australia, New Zealand, Canada, the UK and the United States of America (US). This work found that seven US studies and one UK study linked the pandemic to changes in breastfeeding initiation and duration, and that in most studies including COVID-19-positive mothers, a reduction in breastfeeding initiation and duration was observed.
Some studies highlighted how certain groups of women had been disproportionately affected in their ability to access breastfeeding support during the pandemic. These included minority groups, under-/uninsured, those who did not speak English as their first language, groups with higher rates of COVID-19, and COVID-19-positive women.24 Although, Vazquez-Vazquez33 found that among younger women (who are generally those less likely to breastfeed), 59% of infants were exclusively breastfed/mixed-fed during lockdown, compared to 39% before lockdown. In the study by Snyder,32 women also reflected on how breastfeeding would be particularly problematic for first-time mothers, with one mother stating:
It was hard for me to know if it was because of like COVID-19 but I really didn’t get help at all at the hospital. She did latch on pretty easily, but no one came in to help or you know anything like that. I never got any support at the hospital. (Caucasian, teacher).
Positive improvements in breastfeeding rates and experiences during the pandemic were associated with visitor restrictions in the postnatal units and within the home,34 greater partner support,25 and more time at home with infants to establish breastfeeding.24,32,34 There were also accounts of mothers being more likely to breastfeed due to limited formula availability or wanting to provide immunity to their infants from COVID-19.24,32 Turner et al25 also reported that while mothers did report positive experiences with breastfeeding, these were mentioned less frequently than negative experiences.
Fears of the Pandemic
A few of the studies described pandemic-related fears. Brown and Shenker highlighted how just over 30% of the women surveyed did not contact health professionals for support due to pandemic-related anxieties. A very small percentage of women (~4%) were told that breastfeeding might not be safe during COVID‐19, and ~3% were advised that they would not be “allowed” to breastfeed if they had symptoms. Just over 20% of mothers were worried about the safety of feeding, and 6.5% stopped breastfeeding due to COVID‐19 symptoms. Furthermore, those who had stopped breastfeeding were more likely to have been told by a health professional, friends, and/or family that breastfeeding was not safe or that breastfeeding would not be allowed with symptoms of COVID‐19.
Increased stress as well as isolation among new mothers were reported in the papers by Snyder32 and Wilson.34 In the review by Turner et al,25 they highlighted how some women had fears of developing low milk supply due to the stress of living in the pandemic. The lactation staff in the paper by Schindler24 also expressed concerns that breastfeeding was an additional stressor in an already stressful life period. Moreover, Spatz7 expressed fears that these fundamental changes in the care of childbearing families imposed by social distancing and lockdown measures would be permanently adopted.
Need for Additional Support
Several of the papers highlighted the need for additional support to rectify harmful practices instilled during the pandemic. This included re-lactation support, use of donor milk, appropriate use of formula, responsive formula feeding, sensitive caregiving, and attachment development.26 Sakalidis et al30 also highlighted the need for good mental health support due to the number of women who suffered psychological issues during the pandemic.
Spatz et al7 argued that the need to promote messages of breastfeeding is a lifesaving intervention and all families should have equal access to lactation education and practical support. Hirani et al28 described innovative practices that highlight the importance of engagement and collaboration with community partners to protect breastfeeding during the pandemic. They developed an animated video on “Breastfeeding during COVID-19: An Information Guide” and described how an informational, evidence-based, user-friendly e-resource that shares knowledge on the benefits of breastfeeding can help sustain breastfeeding in areas where access to healthcare services is compromised. Turner et al25 stated how professional recommendations need to reflect best evidence and how a precautionary approach can lead to breastfeeding being deprioritized. They suggest further work to evaluate how the pandemic affected professional guidelines to help protect breastfeeding during future pandemics.
Discussion
For many years, the international professional community has influenced culture in all maternity care settings towards positive breastfeeding practices with initiatives such as the Baby-friendly Hospital Initiative, lactation consultant services, and more. However, the pandemic seems to have disrupted these breastfeeding successes both by limiting mother-infant closeness and the de-prioritization of support services. The lack of knowledge and continuous misinformation about the pandemic and its potential impacts for breastfeeding have affected mothers and families around the world.
Evidence from this review highlights that mothers and infants have been separated against evidence of any need during the COVID-19 pandemic.9,10,24,25 Further, skin-to-skin contact has been restricted. While the intention was to protect mother-infant dyads and families, as these practices were in contrast with available evidence, they created much more far-reaching risks. There is clear evidence on the benefits of couplet care, where the mother-infant dyad is never separated. With close proximity and skin-to-skin contact, not only is breastfeeding ensured, but it can help the bonding process and facilitate a positive mother-newborn, two-way relationship where milk production is enabled, the newborn is protected with powerful life-enabling nutrition, and the mother recovers faster from childbirth.35 Closeness can help to stabilize the hormonal balance of both mother and infant and supports mental health.36 Keeping the family together can reduce feelings of stress, isolation, anxiety, and depression. There is a high risk for this disruptive policy that surfaced during the pandemic crisis to subtly become standard practice.
Mothers reported both positive and negative experiences of breastfeeding during the pandemic. Some mothers enjoyed lockdown, since it brought the family into a cocoon of peace and calm. Mothers felt that they could focus on their newborn and practice breastfeeding without the disruptions of guests and visitors. Positive factors also included greater partner support. However, there were mothers who felt isolated and afraid.8,24 They feared, for instance, that they would develop a low milk supply due to the stress of living in the pandemic.25 It was evidenced in the wider literature that mothers need face-to-face (peer and professional) support to ensure successful breastfeeding,37 but the pandemic did not provide these circumstances. A lack of breastfeeding support contributed towards early breastfeeding cessation, before the mothers felt ready to do so. Good mental health and quality lactation services are required to support breastfeeding continuation.30
Breastfeeding support services changed during the pandemic.24 Mothers reported a lack of care provided in the hospital25 and in the community.7,24 Breastfeeding support visit frequency decreased, as did referrals to lactation support.24
Some breastfeeding support transferred to online modes.33 Some professionals reported that their breastfeeding women preferred telehealth contact sessions, although, in one study, 70% of professionals who provided support via online groups felt they were less effective compared to in-person groups.24 Mothers also reported that the online breastfeeding support they received was inadequate,25 which could be due to difficulties in receiving remote professional help with breastfeeding techniques.24 It is noteworthy to highlight that although some studies verified positive aspects of the pandemic, these positive aspects, for example, online support, are restricted to families with better socioeconomic conditions. This suggests that the pandemic affected vulnerable families more seriously.
Midwives and nurses are in key positions to support breastfeeding during exceptional circumstances.5 Lessons learnt from this pandemic should be shared to enable professionals to stand in guard of evidence-based practices to promote successful breastfeeding and to ensure that families have the best start.
Limitations
In this review, data and publications were mostly available for high-income countries. The authors acknowledge this finding and highlight that this review did not intentionally exclude low- and middle-income countries (LMICs) but recognize that this may relate to slower rates of recording and publishing from these settings. The lack of evidence from LMICs provides a gap in evaluating the impact across different contexts and should be further explored. Several practice advisories were published since the COVID-19 pandemic started; however, less research on the actual impact of the pandemic in general is available.
Recommendations
This review highlights the importance of women and professionals being provided with clear and consistent evidence-based guidance regarding the actual risks of transmission. It also calls for zero separation, especially during a pandemic, to ensure optimal initiation and continuation of breastfeeding and to help protect parental mental health. Strategies evidenced to be effective in supporting breastfeeding need to be continued, such as promoting and enabling skin-to-skin contact and providing early and proactive breastfeeding support (virtual, if necessary, and face to face, where possible). Although the available published articles reported mostly on high-income countries, the support needs to be observed in low- and middle-income countries as well and research to determine the impact of the COVID-19 pandemic in diverse settings is needed.
Conclusion
Many publications on practice advisories for breastfeeding support from the World Health Organization to country and hospital level are available. However, to date, there is limited research that explores and measures the actual practices and impact of the pandemic on breastfeeding, particularly in low- and middle-income settings. Good research evidence on the protective benefits of breastfeeding, the importance of zero separation, the importance of early and proactive support towards successful initiation, and the continuation of breastfeeding is common knowledge and included in recommended practice over the past decades. However, these practices were largely neglected once the COVID-19 pandemic began, and preference was given to precautionary measures.
Breastfeeding has been established as a lifesaving intervention in all environments. Breastfeeding should be guiding the medical care of the newborn and young infant, especially in the face of a pandemic, to successfully prevent and decrease mortality and morbidity of mothers and infants. Breastfeeding is the protective measure infants require for a good start in life and contributes greatly to maternal health and should therefore be protected and supported.
Acknowledgments
The authors would like to thank their respective universities for supporting them to write this review.
Funding
No financial support was provided for this publication.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Zhu H, Wang L, Fang C, et al. Clinical analysis of 10 neonates born to mothers with 2019-nCoV pneumonia. Transl Pediatr. 2020;9:51. doi:10.21037/tp.2020.02.06
2. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395:507–513. doi:10.1016/S0140-6736(20)30211-7
3. Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N Engl J Med. 2020;382:1199–1207. doi:10.1056/NEJMoa2001316
4. Van Goudoever JB, Spatz DL, Hoban R, et al. Updating clinical practices to promote and protect human milk and breastfeeding in a COVID-19 era. Front Pediatr. 2022;10. doi:10.3389/fped.2022.867540
5. Warner SA, Arevalo JL. Literature review of mothers diagnosed with COVID-19 and the impact on breastfeeding their newborns. Nurs Womens Health. 2022;26:234–241. doi:10.1016/j.nwh.2022.03.010
6. Lubbe W, Botha E, Niela-Vilen H, Reimers P. Breastfeeding during the COVID-19 pandemic–a literature review for clinical practice. Int Breastfeed J. 2020;15:1–9. doi:10.1186/s13006-020-00319-3
7. Spatz DL, Davanzo R, Müller JA, et al. Promoting and protecting human milk and breastfeeding in a COVID-19 world. Front Pediatr. 2021;8:1000. doi:10.3389/fped.2020.633700
8. Brown A, Shenker N. Experiences of breastfeeding during COVID‐19: lessons for future practical and emotional support. Matern Child Nutr. 2021;17:e13088. doi:10.1111/mcn.13088
9. Gonçalves-Ferri WA, Pereira-Cellini FM, Coca K, et al. The impact of coronavirus outbreak on breastfeeding guidelines among Brazilian hospitals and maternity services: a cross-sectional study. Int Breastfeed J. 2021;16:1–11. doi:10.1186/s13006-021-00377-1
10. Del Río R, Dip Perez E, Marín Gabriel MÁ. Multi-centre study showed reduced compliance with the World Health Organization recommendations on exclusive breastfeeding during COVID-19. Acta Paediatr. 2021;110:935–936. doi:10.1111/apa.15642
11. Lalor JG, Sheaf G, Mulligan A, et al. Parental experiences with changes in maternity care during the Covid-19 pandemic: a mixed-studies systematic review. Women Birth. 2022. doi:10.1016/j.wombi.2022.08.004
12. Hanson LA. Breastfeeding provides passive and likely long-lasting active immunity. Annals Allergy Asthma Immunol. 1998;81:523–537. doi:10.1016/S1081-1206(10)62704-4
13. Eidelman AI. Breastfeeding and the use of human milk: an analysis of the American Academy of Pediatrics 2012 breastfeeding policy statement. Breastfeed Med. 2012;7:323–324. doi:10.1089/bfm.2012.0067
14. Victora CG, Bahl R, Barros AJ, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387:475–490. doi:10.1016/S0140-6736(15)01024-7
15. Conti MG, Natale F, Stolfi I, et al. Consequences of early separation of maternal-newborn dyad in neonates born to SARS-CoV-2 positive mothers: an observational study. Int J Environ Res Public Health. 2021;18:5899. doi:10.3390/ijerph18115899
16. Tomori C, Gribble K, Palmquist AE, Ververs MT, Gross MS. When separation is not the answer: breastfeeding mothers and infants affected by COVID‐19. Matern Child Nutr. 2020;16:e13033. doi:10.1111/mcn.13033
17. Moore ER, Bergman N, Anderson GC, Medley N. Early skin‐to‐skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev. 2016;2016. doi:10.1002/14651858.CD003519.pub4
18. WHO. Guideline: Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services. WHO; 2017.
19. WHO. Protecting, Promoting and Supporting Breastfeeding: The Baby-Friendly Hospital Initiative for Small, Sick and Preterm Newborns. Geneva Switzerland: WHO; 2020.
20. Gupta N, Deierl A, Hills E, Banerjee J. Systematic review confirmed the benefits of early skin‐to‐skin contact but highlighted lack of studies on very and extremely preterm infants. Acta Paediatrica. 2021;110:2310–2315.
21. Louis-Jacques AF, Stuebe AM. Enabling breastfeeding to support lifelong health for mother and child. Obstetr Gynecol Clin. 2020;47:363381. doi:10.1016/j.ogc.2020.04.001
22. Page MJ, McKenzie JE, Bossuyt, PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. International Journal of Surgery. 2021;88:105906. https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-021-01626-4.
23. Institute for Johns Hopkins Nursing. Johns Hopkins EBP model and tools permission. Institute for Johns Hopkins Nursing; 2022. Available from: https://www.ijhn-education.org/node/18409/done?sid=92115&token=9ba2dc1106a599adf11785b2e1d9c042.
24. Schindler-Ruwisch J, Phillips KE. Breastfeeding during a pandemic: the influence of COVID-19 on lactation services in the Northeastern United States. J Human Lactation. 2021;37:260–268. doi:10.1177/08903344211003898
25. Turner S, McGann B, Brockway MM. A review of the disruption of breastfeeding supports in response to the COVID-19 pandemic in five Western countries and applications for clinical practice. Int Breastfeed J. 2022;17:1–13. doi:10.1186/s13006-022-00478-5
26. Gribble K, Marinelli KA, Tomori C, Gross MS. Implications of the COVID-19 pandemic response for breastfeeding, maternal caregiving capacity and infant mental health. J Human Lactation. 2020;36:591–603. doi:10.1177/0890334420949514
27. Feinstein J, Slora EJ, Bernstein HH. Telehealth can promote breastfeeding during the COVID-19 pandemic. Catalyst Innov Care Deliv. 2021;2. doi:10.1056/cat.21.0158
28. Hirani SAA, Pearce M, Lanoway A. Knowledge mobilization tool to promote, protect, and support breastfeeding during COVID-19. Can J Public Health. 2021;112:599–619. doi:10.17269/s41997-021-00532-5
29. Latorre G, Martinelli D, Guida P, Masi E, De Benedictis R, Maggio L. Impact of COVID-19 pandemic lockdown on exclusive breastfeeding in non-infected mothers. Int Breastfeed J. 2021;16. doi:10.1186/s13006-021-00382-4
30. Sakalidis VS, Rea A, Perrella SL, et al. Wellbeing of breastfeeding women in Australia and New Zealand during the COVID-19 pandemic: a cross-sectional study. Nutrients. 2021;13(6):1831. doi:10.3390/nu13061831
31. Rice K, Williams S. Women’s postpartum experiences in Canada during the COVID-19 pandemic: a qualitative study. Can Med Assoc Open Access J. 2021;9:E556–E562.
32. Snyder K, Worlton G. Social support during COVID-19: perspectives of breastfeeding mothers. Breastfeed Med. 2021;16:39–45. doi:10.1089/bfm.2020.0200
33. Vazquez-Vazquez A, Dib S, Rougeaux E, Wells JC, Fewtrell M. The impact of the Covid-19 lockdown on the experiences and feeding practices of new mothers in the UK: preliminary data from the COVID-19 New Mum Study. Appetite. 2021;156:104985. doi:10.1016/j.appet.2020.104985
34. Wilson AN, Sweet L, Vasilevski V, et al. Australian women’s experiences of receiving maternity care during the COVID‐19 pandemic: a cross‐sectional national survey. Birth. 2022;49:30–39. doi:10.1111/birt.12569
35. Dykes F, Flacking R. Encouraging breastfeeding: a relational perspective. Early Hum Dev. 2010;86:733–736. doi:10.1016/j.earlhumdev.2010.08.004
36. Flacking R, Lehtonen L, Thomson G, et al. Closeness and separation in neonatal intensive care. Acta Paediatr. 2012;101:1032–1037. doi:10.1111/j.1651-2227.2012.02787.x
37. Trickey H, Thomson G, Grant A, et al. A realist review of one-to-one breastfeeding peer support experiments conducted in developed country settings. Matern Child Nutr. 2018;14:e12559. doi:10.1111/mcn.12559
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.