")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Assessment of Electrolyte Imbalance and Associated Factors Among Adult Diabetic Patients Attending the University of Gondar Comprehensive Specialized Hospital, Ethiopia: A Comparative Cross-Sectional Study
Authors Eshetu B, Worede A, Fentie A , Chane E , Fetene G , Wondifraw H , Shimelis M, Girma M, Hadgu R, Demeke K, Fasil A
Received 23 January 2023
Accepted for publication 15 April 2023
Published 26 April 2023 Volume 2023:16 Pages 1207—1220
DOI https://doi.org/10.2147/DMSO.S404788
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Bruktawit Eshetu,1 Abebaw Worede,2 Alemie Fentie,3 Elias Chane,2 Getnet Fetene,2 Habtamu Wondifraw,2 Mahider Shimelis,3 Mahider Girma,4 Rishan Hadgu,5 Kassaw Demeke,6 Alebachew Fasil2
1Department of Medical Laboratory Science, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 2Department of Clinical Chemistry, School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Medical Laboratory Science, College of Medicine and Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 4Department of Medical Laboratory Science, College of Medicine and Health Sciences, Dire Dawa University, Dire Dawa, Ethiopia; 5Department of Medical Laboratory Science, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 6University of Gondar Comprehensive Specialized Hospital, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Alebachew Fasil, Department of Clinical Chemistry, School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar, Po Box. 196, Gondar, Ethiopia, Tel +251-918733171, Email [email protected]; [email protected]
Introduction: Electrolyte imbalance refers to altered electrolyte levels that predominantly affect diabetic patients due to hyperglycemia which rise plasma osmolality and impaired renal function, contributing to a change in electrolyte level. Therefore, this study aimed to assess the prevalence of electrolyte imbalance and its associated factors among diabetic patients and healthy control groups attending the University of Gondar Comprehensive Specialized Hospital.
Patients and Methods: A comparative cross-sectional study was conducted on 130 diabetic patients and 130 diabetes-free controls. Sociodemographic, behavioral and clinical data were collected using a structured questionnaire. After measuring anthropometric parameters, 5mL of the blood sample was collected. Electrolytes were measured based on ion-selective electrode methods. Fasting blood glucose, and creatinine were measured by spectrophotometric enzyme hexokinase, and Jaffe reaction methods, respectively. The data was entered into Epi-data version 4.6 and analyzed using STATA version 14. Mann–Whitney U-tests and independent t-tests were used for comparison. Multiple logistic regression analysis was done to determine the factors associated with electrolyte imbalances. P-value < 0.05 was considered statistically significant.
Result: The overall prevalence of electrolyte imbalance among diabetic patients and controls were 83.07% and 52.31%, respectively. The mean of Na+ and the median level of Mg2+ and Ca2+ were significantly decreased. However, the mean level of Cl− was significantly increased in diabetic patients as compared to control groups. In multivariable logistic regression: alcohol consumption AOR = 3.34 [1.02– 10.9], no formal education AOR = 5.38 [1.14– 25.4], hyperglycemia AOR = 6.32 [2.04– 19.5], and urbanization AOR = 5.6 [1.44– 22.3] showed significant association with electrolyte imbalance.
Conclusion: Diabetic patients have more likely to develop electrolyte imbalance than control groups. Diabetic participants showed significantly reduced Na+, Mg2+, and Ca2+ levels and significantly increasing CI− levels when compared to control groups. Hyperglycemia, alcohol drinking habits, urbanization, and no-formal education were statistically significantly associated with electrolyte imbalance.
Keywords: electrolyte imbalance, diabetes mellitus, associated factors, Ethiopia
Introduction
Electrolytes are electrically charged molecules that are required for normal metabolic reactions and homeostasis. Electrolytes sustain cell membrane functions, neuron conductivity, muscle contractility, hormone action, bone structure, and fluid and acid-base balance. Electrolyte imbalance occurs when the electrolyte level is abnormally high or low than the normal range as a result of a variety of pathophysiological factors, including nutritional status, concurrent acid-base imbalances, pharmaceuticals, other co-morbid disorders (mostly renal disease), or acute illness.1,2
Electrolyte imbalance predominantly affects diabetic people due to osmotic fluid changes brought on by hyperglycemia, and it has two important effects on the body’s electrolyte concentration. If water movement transports intracellular electrolytes to the extracellular space, it may have a dilutional effect, by lowering extracellular electrolyte concentrations or increasing extracellular concentrations, especially in an insulin-deficient state.3–5
These osmotic effects dilute serum sodium (Na+) levels, potentially resulting in hyponatremia (a serum Na+ concentration less than 135 mmol/L).5 The activity of the Na+/K+ ATPase depends on insulin. The transmembrane Na+ and K+ gradients are kept in place by this transporter. In diabetics with insufficient insulin production or insulin resistance, the activity of this transport protein may be reduced. Cellular K+ diffusion out of cells and cellular Na+ diffusion in cells are governed by trans-membrane electrical gradients. Changes in insulin levels of the hormone have an impact on serum electrolyte levels.6,7
Level of Magnesium (Mg2+) less than 1.7 mg/dL is a common complication of diabetes and is brought on by an insulin-resistant condition, or poor glycemic control. Insulin resistance may decrease the transient receptor potential of melastatin 6 (TRPM6) expression in the kidneys, which in turn may increase urine Mg2+ loss and decrease plasma Mg2+ concentration. Coexisting with hypomagnesemia also leads to hypokalemia as a result of decreased intracellular Mg2+, which reduces the magnesium-mediated control of renal outer medullary potassium channel (ROMK channels, and contributes to K+ waste.8,9 Reduced renal PO4− reabsorption via the Na-Pi transporters in the renal proximal tubule is one of the mechanisms causing hypophosphatemia (serum PO4−level less than 2.5 mg/dL) in diabetic individuals (due to acidosis and hyperglycemia).10,11
Diabetes mellitus is a serious public health problem linked to non-communicable diseases. It is the world’s largest pandemic, and its rapidly rising prevalence rate is a cause for concern.12 According to the International Diabetes Federation (IDF), diabetes was the cause of death for 6.7 million people worldwide in 2021, with 537 million adults suffering from the disease. By 2030, this number is predicted to rise to 643 million.13 DM is known to be like electrolyte imbalance which affects both community individuals and a wide range of patients (from asymptomatic to severely ill).14 Diabetes patients frequently experience hyponatremia, which increases morbidity and mortality.15 In non-hospitalized DM patients, hypomagnesemia has been documented to occur in 11–47.7% of cases. Diabetes patients with hypomagnesemia develop their disease more rapidly and are more likely to experience complications from their diabetes. This includes macrovascular conditions including peripheral artery disease and cardiovascular disease.9,16
When compared to the cost of normonatremic participants in the United States, hyponatremia was related to up to almost $3000 greater hospital costs per patient. It also has a higher economic cost and a higher risk of readmission.17 Electrolyte imbalance affects the management and progression of DM, which can be fatal in severe situations. Poor plasma Na+ management has been associated with two diseases with potentially fatal consequences (cerebral edema and osmotic demyelination syndrome). Renal impairment is frequently seen in people with DM, and this condition itself is an independent risk factor for hyperkalemia. Variations in K+ levels can cause dysrhythmias, impair the electrical conduction of the heart, and even result in sudden death.1,18 Electrolyte imbalance should be considered a serious illness, especially in diabetes patients, because these problems frequently occur in diabetic patients. However, there is a limited amount of information on the electrolyte profile of diabetic patients in Ethiopia.
Materials and Methods
Study Population, Area, Design, and Period
An institution-based cross-sectional study design and systematic random sampling techniques were used to carry out the study. The study was conducted at the UoGCSH. The hospital is located approximately 738 km northwest of Addis Ababa and 180 km north of Bahir Dar in central Gondar administrative zone of the Amhara regional state. The study was conducted from April 13, 2022, to June 15, 2022. All types of diabetic patients attending UoGCSH during the study period and who fulfilled the inclusion criteria of the study were included. Age and sex-matched healthy individuals who come to UoGCSH were also included as controls. Controls were interviewed for prior history of diabetes and fasting blood sugar was measured to make sure it is in the normal range.
Eligibility Criteria
Inclusion Criteria
The inclusion criteria were adult diabetic patients who were willing to voluntarily participate in the study. All adult healthy individuals who were willing to participate in the study were included in the control groups.
Exclusion Criteria
Those study participants having known kidney disease, mental illness, pregnant diabetes patients, persistent diarrhea and vomiting, thyroid disorder, malignancy, diuretics users, and acute illness were excluded by reviewing their medical records and performing screening.
Sample Size Determination and Sampling Technique
The sample size was determined by using the double proportion formula. Open Epi, version-7 software was used by considering the following assumptions; a study done at Benin reported the proportion of at least one electrolyte abnormality for case groups (P1=41.3%) and control groups (P2=16.4%).19 Power (80%), r = ratio of control to case (1:1), and 95% CI. This gives a total of 236 after adding 10% non-response rate, 130 diabetes cases and 130 healthy controls were enrolled. A systematic sampling technique was employed to select study participants at UoGCSH.
Operational and Standard Definitions
Electrolyte imbalance; test results showing a changed level of at least one of the electrolytes (K+, Cl−, Na+, Ca++, Mg++, or PO4−).2 The following ranges were used to determine the imbalance for each electrolyte based on the reference range of the central laboratory of UoGCSH: Na+= 135–145 mmol/L, K+= 3.5–5.5 mmol/L, Ca2+= 2.1–2.55 mmol/L, Cl− = 98–107 mmol/L, Mg2+ =1.7–2.8 mg/dL, and PO4−= 2.5–4.6 mg/dl.
Body mass index is weight in kilogram divided by height in meter square and the diabetic patients will be classified as underweight (<18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30 kg/m2) based on WHO guideline category.20
Hypertension: hypertension is based on an average systolic BP (SBP) ≥140 mm Hg, diastolic BP (DBP) ≥90 mm Hg, or self-reported use of antihypertensive medication.21
Alcohol intake: Alcohol consumption is classified as non-drinkers (those who never drink any alcohol), regular drinkers (those who drink alcohol at least one day per week), and ex-drinkers (those who do not currently consume alcohol but have drunk alcohol in the past).22
Glycaemic control – fasting blood glucose (FBG) level, participants will be classified as with good glycaemic control (FBG <130 mg/dl) and poor glycaemic control (FBG ≥130 mg/dl).23
Data Collection and Laboratory Methods
The sociodemographic characteristics of study participants were collected by using a semi-structured questionnaire prepared for this study. Data for these characteristics were collected by trained nurses through a face-to-face interview. The study participants were interviewed after written informed consent was taken. Height and weight were measured by using a stadiometer and bio-electrical impedance (Seca Deutschland, Germany) instruments, respectively. During the measurement of height and weight, the study participants were asked to remove their shoes, hats, and any bulky clothing, and the participants were asked to look straight ahead, face forward, with the reader’s eye at the level of the headpiece. Then the height and weight were recorded. The body mass index (BMI) was calculated as weight divided by height square (kg/m2) and blood pressure (BP) was measured by using a Mercury sphygmomanometer from the left upper arm and positioned at the heart level.
Three successive blood pressure readings at an interval of at least one minute mean blood pressure was taken. After receiving informed consent from the study participants, 8–12 hours of fasting 5mL of venous blood was collected preferably at the antecubital area by applying a tourniquet. Before collecting the sample, the puncture area of the vein was disinfected by using 70% alcohol. The serum was collected using a serum separator tube at the medical ward department of UoGCSH. After collection, specimens were transported to the clinical chemistry unit of the UoGCSH laboratory for analysis. The collected blood sample was left for 30 minutes at room temperature. Then the blood samples were centrifuged for 5 minutes at 3500 revolutions per minute (rpm) to separate serum from formed elements. All these procedures were done by the laboratory technologist and principal investigator by applying standard operating procedures (SOPs). Electrolytes (Na+, K2+, Ca2+, Mg2+, Po4−, and Cl−) and concentration of FBS and creatinine were determined by Beckman Coulter DXC 700 AU and 600 AU (Danaher Corporation company, USA), respectively.
Data Quality Assurance and Management
After the completion of each questionnaire, cross-checking was done between the data collector and principal investigator to assure the completeness of the data collected. The label on the test tube and the study participants’ unique identification number on the questionnaire were checked. Before patient sample processing, quality controls were performed, and the study participants’ result was taken after confirmation of the controls results are within acceptable range.
Data Analysis and Interpretation
The data was checked for completeness and then inserted into EPI data version 4.6, then transferred to STATA version 14 for analysis. The model of fit was checked by Hosmer and Lemeshow’s goodness-of-fit statistic. The Kolmogorov–Smirnov and Shapiro–Wilk normality tests and skewness were conducted to check the normality of continuous variables. For continuous variables, Mann–Whitney U-tests for abnormally distributed data were used to determine the difference in medians. Independent t-tests were used to determine the mean difference for normally distributed data. The mean±SD was used to represent data with a normal distribution, while the medians and IQR were used to represent data with an abnormal distribution. Binary logistic regression was used to identify associated factors for electrolyte imbalance in DM, and variables with P-values of less than 0.25 were selected and shifted to multivariable logistic regression with an adjusted odds ratio. Variables with a P-value of less than 0.05 were considered statistically significant.
Ethical Consideration
Ethical clearance was obtained from research and ethical review committee of School of Biomedical and Laboratory Sciences, college of medicine and health sciences University of Gondar. Ethics approval number for the study is Ref No. SBMLS/271/2022. The study was conducted following the Declaration of Helsinki. Permission letter was also obtained from UoGCSH medical director. To ensure confidentiality of the study participant’s information and codes were used so that the name and any identifier of participants was not used on the questionnaire and laboratory requests. Data were collected after written informed consent was given for each participant. The collected data was not used for another purpose other than the present study. Participants with abnormal test results were communicated through data collectors and linked to University of Gondar comprehensive Specialized Hospital for treatment.
Result
Sociodemographic, Behavioural, and Anthropometric Characteristics of Study Participants
This study included 130 diabetic patients and 130 healthy control groups, with a response rate of 100%. Among the study groups, 138 (53.307%) were females. One hundred and fifty-seven (60.38) ranged from 40 to 64 years old. One hundred and ninety (73.07%) of study participants were urban residents, and 115 (44.2%) were married. Based on educational status, 105 (40.4%) had no formal education and 79 (30.38%) of those were public servants. Based on the lifestyle conditions 134 (51.1%) study participants had alcohol-drinking habits. One hundred and ninety (73.07%) of them were in the normal range of BMI level. Of all study participants, 227 (87.3%) and 236 (90.8%) had normal systolic and diastolic blood pressure, respectively (Table 1).
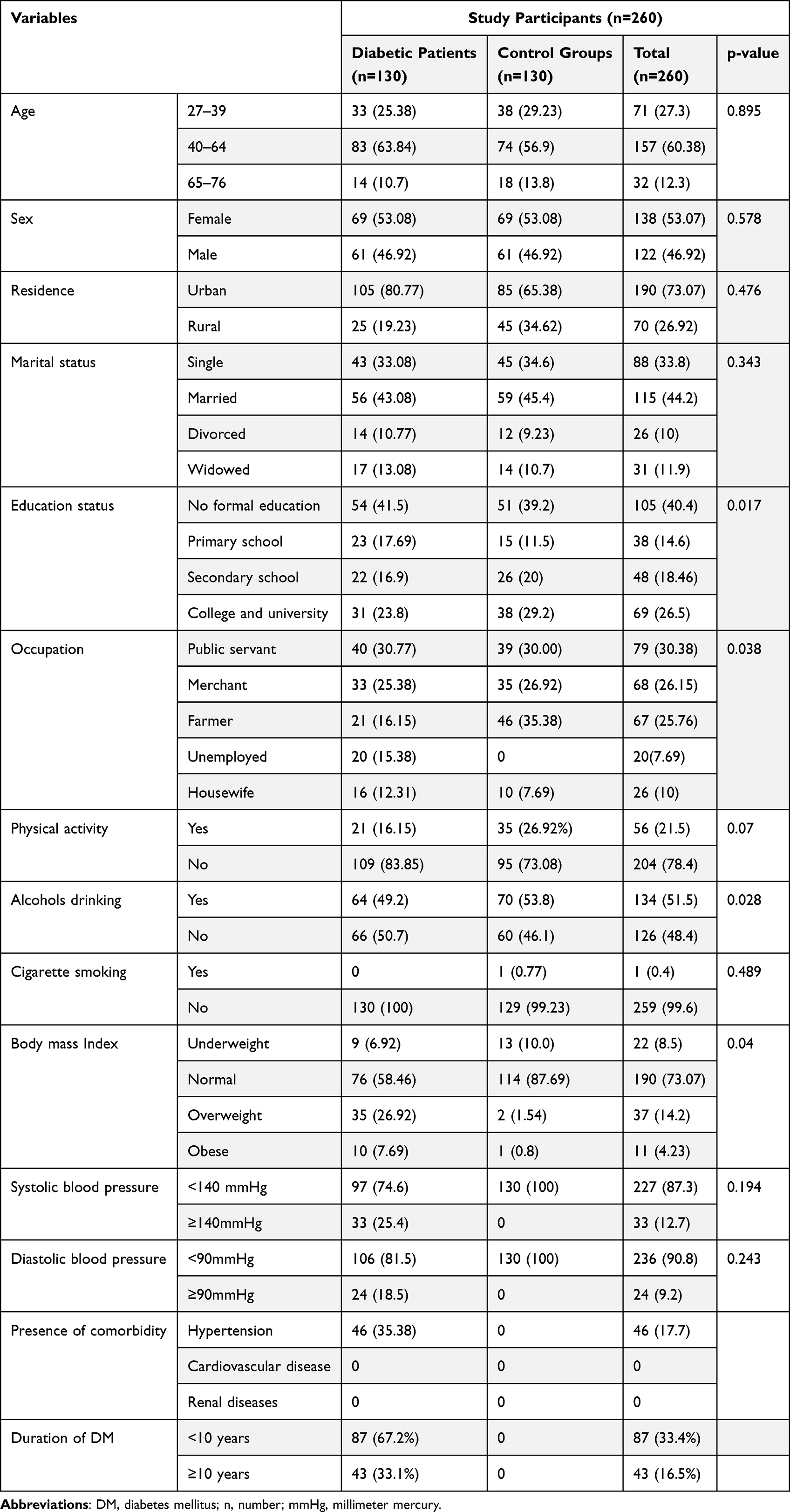 |
Table 1 Socio-Demographic, Behavioural, and Anthropometric Characteristics of Participants (n = 260, UOGCSH, Gondar, 2022), Pearson’s Chi-Square Test) |
Prevalence of Electrolyte Imbalance Among Diabetic Patients and Control Group
In diabetic patients, the prevalence of electrolyte imbalance in at least one of the parameters among the six electrolyte parameters was 83.07% (108/130), (95% CI: 75.5–88.6%) among cases and 52.31% (68/130), (95% CI: 43.6–60.9%) among control groups. The prevalence of electrolyte imbalance among diabetic patients was 51 (39.2%) hyponatremia, 41 (31.5%) hypomagnesemia, 35 (26.9%) hyperchloraemia, 30 (23.0%) hypophosphatemia, and 29 (22.3%) hypokalaemia. Whereas the prevalence of electrolyte imbalance among control groups was 22 (16.9%), 15 (11.5%), and 11 (8.46%), hypophosphatemia, hyperchloraemia, and hypocalcemia, respectively (Table 2).
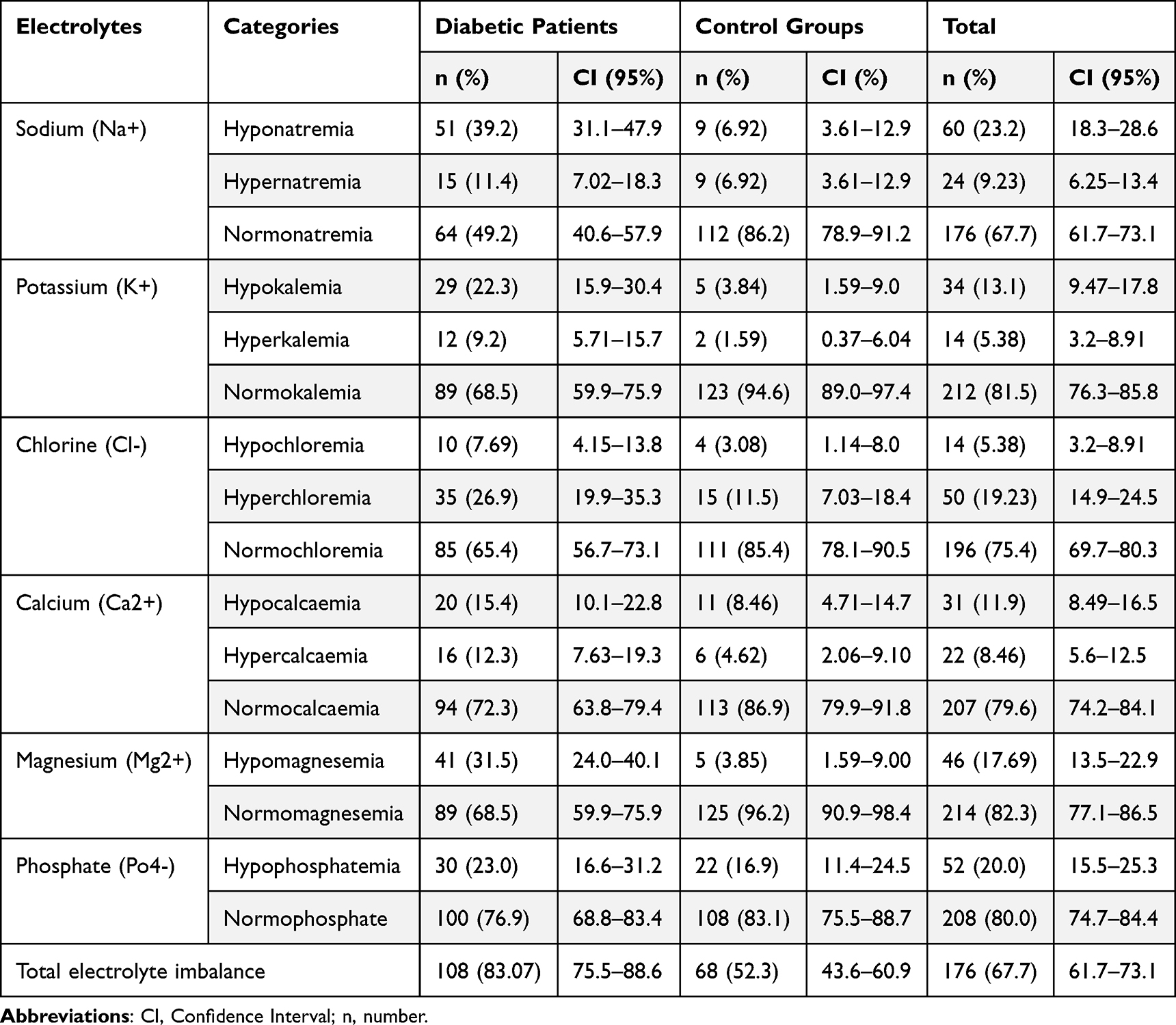 |
Table 2 Prevalence of Electrolyte Imbalance Among Diabetic Patients and Control Group (n = 260, UOGCSH, Gondar, 2022) |
Factors Associated with Electrolyte Imbalance Among Diabetes Patients and Controls
After performing bivariable regression analysis, alcohol drinking habits, occupation, body mass index, educational status, and presence of diabetes reported significant association with EI. Diabetic patients were 4.60 [AOR = 4.60, 95% CI = 2.28–9.24, P = 0.000] times more likely to develop electrolyte imbalance than non-diabetic patients, and alcohol drinkers were 2.06 [AOR = 2.06, 95% CI = 1.15–3.70, P = 0.015] times more likely to develop electrolyte imbalance than non-alcohol drinkers in multivariable regression with P-value <0.05 (Table 3).
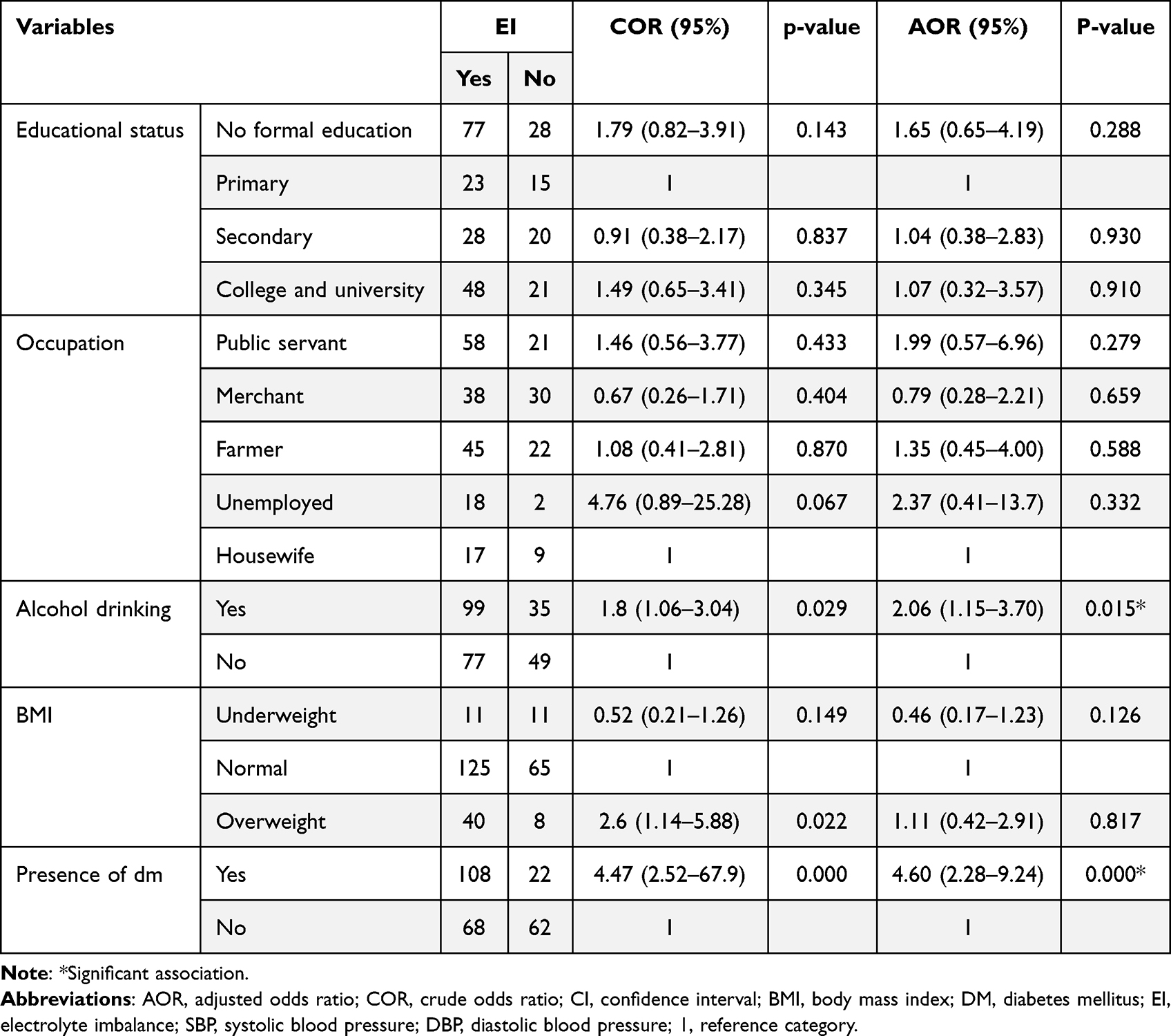 |
Table 3 Bivariate and Multivariable Logistic Regression Analysis of Factors Associated with Electrolyte Imbalance Among Study Individuals (n = 260, UOGCSH, Gondar, 2022) |
Factors Associated with Electrolyte Imbalance Among Diabetic Patients
After performing bivariable analysis fasting blood glucose, alcohol drinking, residence, educational status, and medication of DM showed significant association with EI.
In multivariable analysis, hyperglycemia diabetic patients were 6.32 [AOR: 6.32, 95% CI = 2.04–19.59, P = 0.001] times more likely to develop an electrolyte imbalance as compared to normoglycemic. Diabetic patients who had alcohol drinking habits were 3.34 [AOR: 3.34, 95% CI = 1.02–10.9, P = 0.046] times more likely to develop EI compared to non-drinkers. Diabetic patients who had no formal education had 5.38 [AOR; 5.38, 95% CI = 1.14–25.4, P = 0.033] time more likely to develop electrolyte imbalance as compared to those with higher educational status, and diabetic patients who lived in urban areas were 5.67 [AOR: 5.67, 95% CI = 1.44–22.3, P = 0.013] time more likely to develop electrolyte imbalance as compared to rural residents (Table 4).
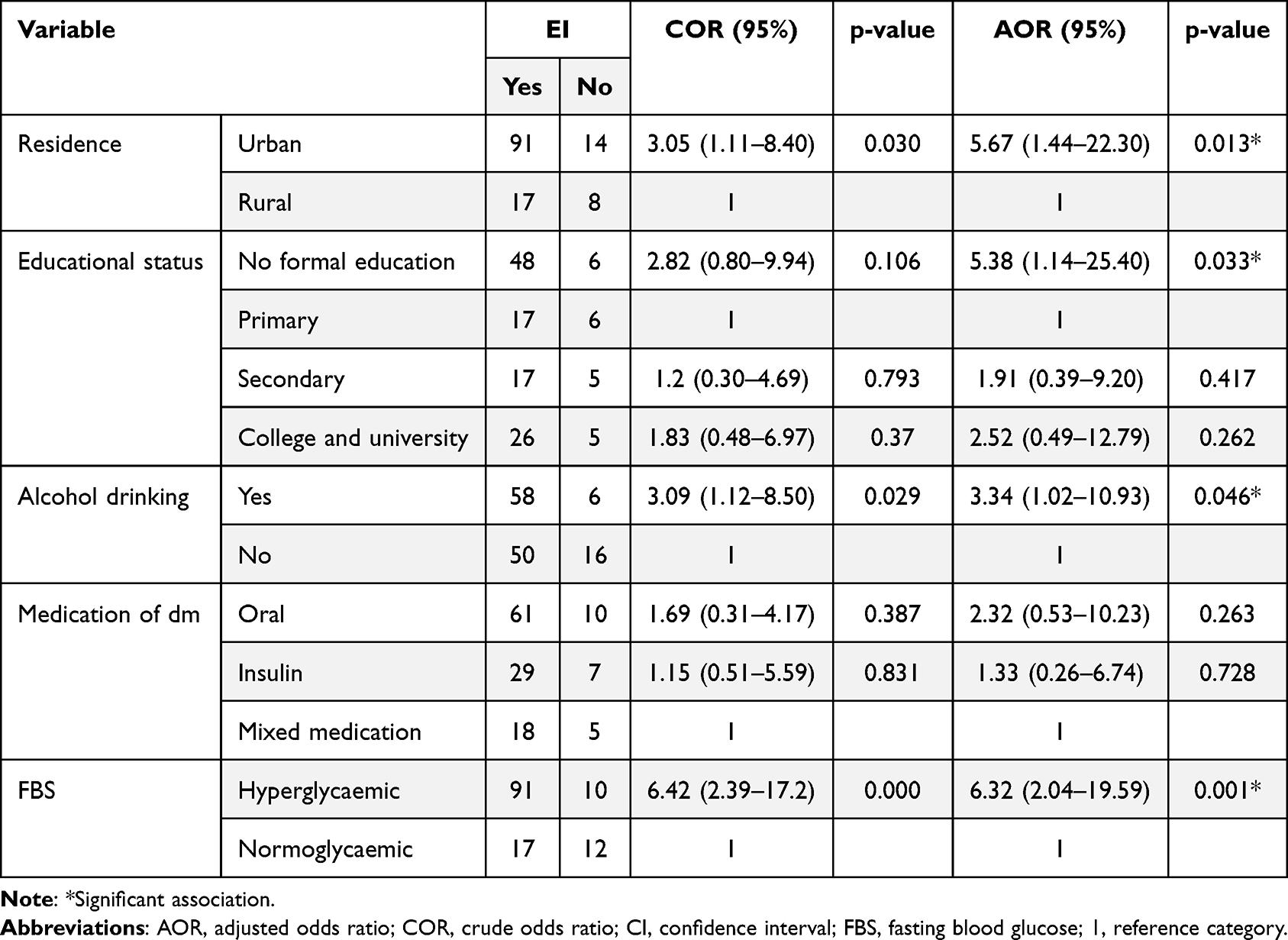 |
Table 4 Bivariate and Multivariable Logistic Regression Analysis of Factors Associated with Electrolyte Imbalance Among Diabetic Patients (n = 130, UOGCSH, Gondar, 2022) |
Comparison of Electrolyte Level Among Diabetic Patients and Control Groups
After checking the distribution of variables, we used both t-tests and Mann–Whitney U-tests to compare the mean and median variables, respectively. The mean levels of serum Na+ and Cl− showed statistically significant differences between diabetic patients and control groups (P < 0.05). The median level of serum K+ and PO4− did not show a statistically significant difference between diabetic patients and control groups (P = 0.176 and P = 0.142, respectively). But the median serum level of Mg2+ and Ca2+ showed a statistically significant difference between diabetic patients and control groups (P < 0.05) (Table 5 and Table 6).
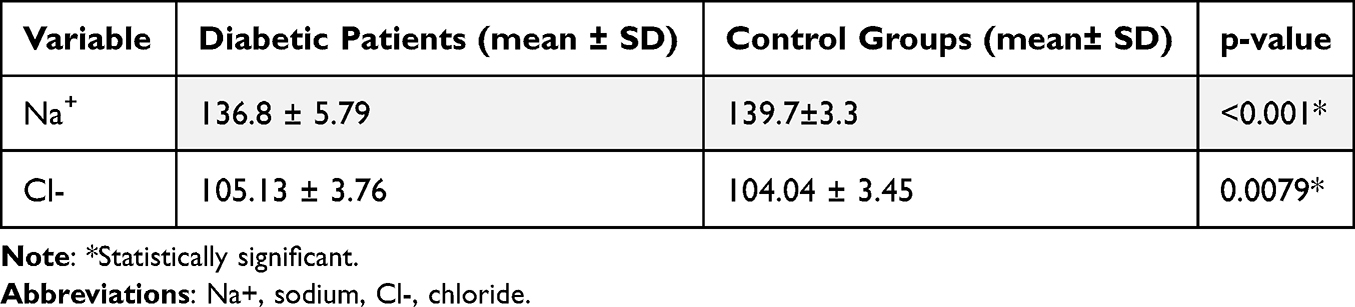 |
Table 5 Mean Comparison of Electrolytes Parameters Between Diabetic Patients and Control Groups (t-test) (n = 260, UOGCSH, Gondar, 2022) |
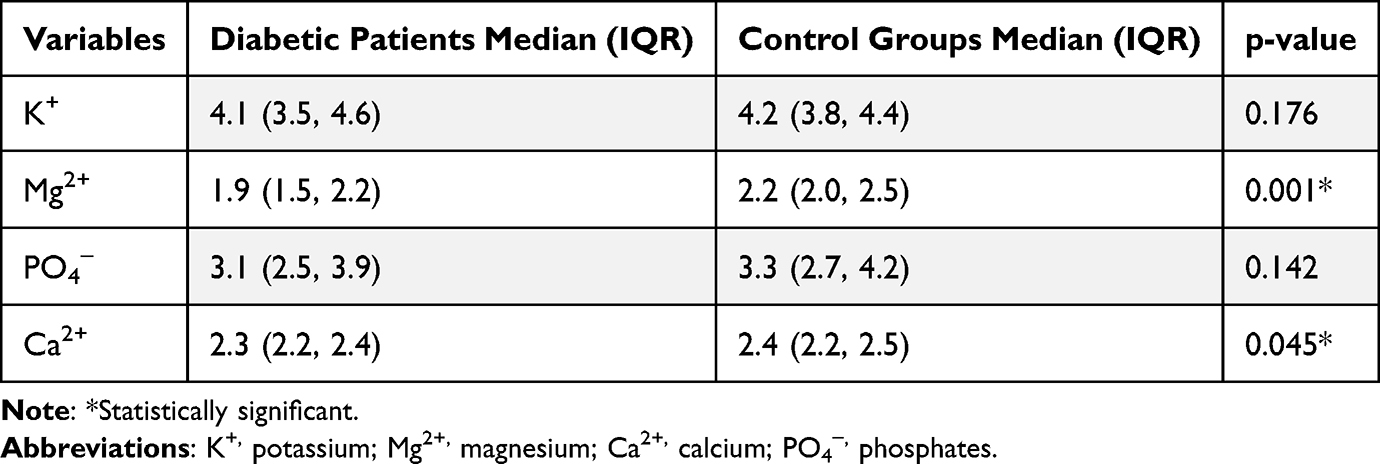 |
Table 6 Median Comparison of Electrolytes Parameters Between Diabetic Patients and Control Groups (Mann-Whitely U-Test) (n = 260, UOGCSH, Gondar, 2022) |
Discussion
This study showed that the majority of the diabetic patients had a high prevalence of one or more electrolyte imbalances when compared with the control subjects 83.07%, and 52.31%, respectively. Hyponatremia was the most common abnormality among the serum electrolytes measured in diabetic patients, with a prevalence of 39.2% [95% CI: 31.1–47.9] similar to those reported in Ethiopia (40.6%), Southern India (33%), and Benin (45.3%).6,24,25 Due to the osmotically active nature of glucose, diabetes can cause a drop in serum Na+ levels by causing a dilution effect that moves water from intracellular to extracellular compartments.26 However, our study finding was lower than studies done in Bangladesh (63.3%) and Kerala (75%).27,28 The difference could be those studies done in admitted diabetic patients included diuretics medication takers and the majority of participants had diabetic nephropathy, both of which are major contributors to hyponatremia. This study also showed that there was hypernatremia of 11.4% [95% CI: 7.02–18.3] due to osmotic diuresis increasing urination if the water is not replaced sufficiently leading to hypernatremia.4 Our result is consistent with Benin (17.3%) and Nigeria (15.6%).24,29
The secondary electrolyte imbalance in our study was hypomagnesemia with 31.5% [95% CI: 24.0–40.1]. Our finding is consistent with the prevalence of hypomagnesemia in the Netherlands (30.6%).30 Hypomagnesemia might be associated to decreased tubular Mg2+ reabsorption brought on by insulin resistance.31 While our finding was lower than Pakistan (57.3%), Nepal (50%), and India (44%).9,32,33 Variation in the targeted groups may be related to dietary habits, the severity of DM, and the heterogeneity of the selected patient.
The study also reported hyperchloremia and hypochloremia of 26.9% [95% CI: 19.9–35.3] and 7.69% [95% CI: 4.15–13.8], respectively. Our finding inconsistency with Southern India and Nigeria studies reported hyperchloremia and hypochloremia was (2.7% vs 31%) and (8.9% vs 40.1%).25,29 The difference could be that studies performed on hospital admitted diabetic patients having high-risk factors such as vomiting and excessive diuretic use, as well as diabetic neuropathy which is the most common cause of hypochloremia, whereas in our study hyperchloremia was higher than those studies because ketoacidosis lowers blood pH, upsetting the acid-base balance and elevating CI− levels. Diabetic ketoacidosis may be responsible for the rise in CI− levels in DM patients.34
Our study also showed the prevalence of hypophosphatemia which is 23% [95% CI: 16.6–31.2], and it is similar to Ukraine study (21.8%).35 Decreased renal phosphate reabsorption via the Na-Pi transporters in the renal proximal tubule (due to acidosis and hyperglycemia). Phosphorus moves from the extracellular to the intracellular compartment during insulin therapy, resulting in hypophosphatemia.36 This study also showed the prevalence of hypokalemia, and hyperkalemia 22.3% [95% CI: 15.9–30.4] and 9.23% [95% CI: 5.71–15.7] in diabetic patients, respectively. Changes in intracellular Mg2+ concentration can lead to hypokalemia in diabetics, and insulin therapy can also promote the K+ shift into cells.37 On the other hand, hyperglycemia causes a redistribution of K+ from the intracellular to extracellular fluid compartment due to factors that impair cellular uptake, leading to hyperkalemia.27 Our funding is greater than the prevalence of hypophosphatemia in Jordan (10%),11 as well as hypokalemia and hyperkalemia in Thailand (6.7% and 2.9%), respectively.38 This discrepancy may be explained by the sociodemographic differences among the study participants, including their levels of education and living conditions.
In our study, the prevalence of hypocalcemia and hypercalcemia were 15.3% (95% CI: 10.1–22.8) and 12.3% (95% CI: 7.63–19.3), respectively. Hypercalcemia in diabetic patients may be caused by hypophosphatemia and increased renal calcium absorption, hypocalcemia due to renal failure in diabetic individuals is linked to hypomagnesemia.39 Our finding is much lower than the prevalence of hypocalcemia and hypercalcemia reported in Benin (41.3% vs 23.3%) and Cameron (48% vs 30%), respectively.19,24 The disparity might be due to the diversity of the targeted populations, and it might be related to the severity of DM cases.
The mean serum level of Na+ (136.8±5.79 vs 139.7±3.), P = 0.001 was significantly decreased in diabetic patients when compared to control groups. This result is similar to the finding of different studies in Saudi, Nigeria, Sudan, Iraq, and China.34,40–43 Because hyperglycemia causes water to be driven out of intracellular fluids, sodium levels are reduced through dilution, and elevated glucose levels reduce Na+-K+-ATPase activity, which is thought to be linked to hyponatremia.5,7
The mean level of Cl− was significantly higher than control groups (105.13±3.76vs104.04±3.45). This result is in line with those studies in India and Iraq42,44 but it is inconsistent with a study conducted in Kerala.28 Elevated serum CI− levels in diabetic patients may be caused by a drop in blood pH brought by ketoacidosis, which causes an acid-base imbalance that results in elevated Cl− levels.34
The median Ca2+ levels were significantly reduced in participants with DM compared to control groups. Our result is supported by those findings conducted in Nigeria, China, and India.43,45,46 Due to hyperglycemia, which is common in DM patients, can cause varying degrees of renal impairment, which can then result in poor phosphorus clearance and eventually build in the blood and bind Ca2+, causing hypocalcemia. Additionally, hypomagnesemia can also cause hypocalcemia.39
The median level of Mg2+ concentration was significantly decreased in diabetic patients than in control groups. Our findings were comparable with a study done in Pakistan and India.32,47 Due to insulin’s role in regulating Mg2+ reabsorption in the kidney through the TRPM 6 channel. Insulin resistance or insulin deficit decreased renal magnesium absorption by blocking the TRPM 6 channel, which led to urine magnesium wasting.48
Educational level was also found associated with electrolyte imbalance. It was found that DM patients had no formal education 5.3 higher odds of having electrolyte imbalance among diabetic patients [AOR: 5.38; 95% CI: 1.14.–25.40, P = 0.033] when compared to those patients with higher education status. This finding was in agreement with a study done in Ethiopia.2 The rationale might be people with higher levels of education are more likely to be aware of using health services than those with lower levels. Additionally, knowledge is essential for unlocking any closed doors to life in the world and enabling everyone to live a healthy lifestyle through behavioral modification.
The participants who lived in urban were five times more likely [AOR: 5.67, 95% CI: 1.44–22.30] to develop electrolyte imbalance than those who lived in rural. There may be several explanations for this including a shift in diet with greater consumption of sugar and saturated fat, as well as a more sedentary lifestyle and increased alcohol use, which are observed globally. Overall, urbanization could have exacerbated DM causing an electrolyte imbalance.49
Electrolyte imbalance was 3.34 times more common in alcoholics than non-alcoholics [AOR: 3.34, 95% CI: 1.02–10.93, P = 0.046] this finding was agreed with studies done in Ethiopia and Southern India.2,50 Alcohol exposure can cause a variety of electrolyte imbalances such as hypophosphatemia, hypomagnesemia, and hypokalemia multiple factors were identified as the causes of this, including inadequate nutrition, increased excretion through increased urine osmolality, internal redistribution, and decreased tubular cell reabsorptive ability.2,51,52
Patients with hyperglycemic had increased the likelihood of electrolyte imbalance by 6.3 times more than patients with normoglycemic [AOR = 6.32, 95% CI: 2.04–19.59, P = 0.001]. Similar findings were reported from Ethiopia, Bangladesh, and Nepal.6,27,53 The plausible explanation could be that elevated blood sugar levels cause hyperosmolarity, which shifts fluids and causes intracellular dehydration and electrolyte loss. Na+ and K+ are the two electrolytes that are most significantly reduced. A dispersed electrolyte concentration results from the body’s attempt to eliminate blood glucose by increasing urine production.4,5
The odds of electrolyte imbalance in diabetic patients were 4.60 times higher than in control groups (AOR = 4.60; 95% CI, 2.28–9.24, P = 0.000). This is due to several underlying mechanisms that have been proposed for electrolyte imbalance in DM due to hyperglycemia-induced osmotic fluid shifts or to total-body deficits brought about by osmotic diuresis. Complications of diabetic nephropathy and certain medications used in the management of diabetes may also contribute to electrolyte imbalance.4,5
Conclusion
In conclusion, diabetic patients have more likely to develop electrolyte imbalance than control groups. Diabetic participants showed a significantly decreasing Na+, Mg2+, and Ca2+ level and a significantly increased level of CI− when compared to control groups. There was a statistically significant association of hyperglycemia, alcohol drinking habits, urbanization, and education status with electrolyte imbalance.
Recommendation
Routing monitoring and assessment of serum electrolyte profile including magnesium and phosphates are important for rational measures taken for DM management. Patients with DM should be assessed for their serum electrolyte level, strict good glycaemic control, and reducing their alcohol consumption to reduce electrolyte imbalance and its complication.
Strengths and Limitations of the Study
Strength of the Study
In contrast to most of the previous studies, this study incorporated most biochemical liver function test parameters than any other previous study conducted, and the study tried to compare the prevalence of electrolyte imbalance between case and control groups.
Limitations of the Study
Despite the comparative cross-sectional nature of our study, it is challenging to demonstrate a cause-and-effect relationship.
Abbreviations
BMI, Body mass index; Ca+2, Calcium; Cl−, Chloride; DBP, Diastolic blood pressure; DM, Diabetes mellitus; FBS, Fasting blood sugar; IDF, International Diabetic Federation; K+, Potassium; Mg2+, Magnesium; Na+, Sodium; Po4−, Phosphate; ROMK, Renal outer medullary potassium channel; SBP, Systolic blood pressure; T2DM, Type 2 diabetes mellitus; TRPM6, Transient Receptor Potential Cation Channel Subfamily M Member 6; UoGCSH, University of Gondar Comprehensive Specialized Hospital.
Data Sharing Statement
Most of the data generated or analysed during this study are included in this published article. Additional files and full data will be available from the corresponding author upon a reasonable request.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Research and Ethical Review Committee of the School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar. Data collected only after full written informed consent was obtained.
Acknowledgments
We would like to thank all the study participants for being voluntary to participate in the study. We would also like to acknowledge the clinical directors of the University of Gondar comprehensive specialized hospital. Finally, we would like to acknowledge the Clinical chemistry laboratory staff of UoGCSH.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Lee J. Fluid and electrolyte disturbances in critically ill patients. Electrolyte Blood Pressure. 2010;8(2):72–81. doi:10.5049/EBP.2010.8.2.72
2. Timerga A, Kelta E, Kenenisa C, Zawdie B, Habte A, Haile K. Serum electrolytes disorder and its associated factors among adults admitted with metabolic syndrome in Jimma Medical Center, South West Ethiopia: facility based crossectional study. PLoS One. 2020;15(11):E0241486. doi:10.1371/journal.pone.0241486
3. Khanduker S, Ahmed R, Khondker F, Aharama A, Afrose N, Chowdhury M. Electrolyte disturbances in patients with diabetes mellitus. Bangladesh Journal of Medical Biochemistry. 2018;10:27–35. doi:10.3329/bjmb.v10i1.36698
4. Palmer B, Clegg D. Electrolyte and acid-base disturbances in patients with diabetes mellitus. N Engl J Med. 2015;373(6):548–559. doi:10.1056/NEJMra1503102
5. Liamis G, Liberopoulos E, Barkas F, Elisaf M. Diabetes mellitus and electrolyte disorders. World J Clin Cases. 2014;2(10):488–496. doi:10.12998/wjcc.v2.i10.488
6. Woyesa S, Gebisa W, Anshebo D. Assessment of selected serum electrolyte and associated risk factors in diabetic patients. Diabetes Metabol Syndr Obes. 2019;12:2811–2817. doi:10.2147/DMSO.S233053
7. Rajagopal L, Ganesan V, Abdullah S, Arunachalam S, Kathamuthu K, Ramraj B. Exploring the interrelationship between electrolytes, anemia, and glycosylated hemoglobin (Hba1c) levels in type 2 diabetics. Asian J Pharma Clin Res. 2018;11:251–256. doi:10.22159/ajpcr.2018.v11i1.22533
8. Sadiq F, Nawaz M. Hypomagnesemia in patients with type 2 diabetes. Pak J Med Health Sci. 2014;8:983–985.
9. Kumar P, Bhargava S, Agarwal P, Garg A, Khosla A. Association of serum magnesium with type 2 diabetes mellitus and diabetic retinopathy. J Family Med Primary Care. 2019;8(5):1671. doi:10.4103/jfmpc.jfmpc_83_19
10. Vorum H, Ditzel J. Disturbance of inorganic phosphate metabolism in diabetes mellitus: its relevance to the pathogenesis of diabetic retinopathy. J Ophthalmol. 2014;2014:1–8. doi:10.1155/2014/135287
11. Rashed R, Hyassat D, Batieha A, et al. Prevalence and correlates of hypophosphatemia among type 2 diabetic patients attending the National Center for Diabetes, Endocrinology and Genetics (Ncdeg). Ann Med Surg. 2022;78:103770. doi:10.1016/j.amsu.2022.103770
12. Roglic G. Who global report on diabetes: a summary. Int J Noncommun Dis. 2016;1(1):3. doi:10.4103/2468-8827.184853
13. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
14. Liamis G, Rodenburg E, Hofman A, Zietse R, Stricker B, Hoorn E. Electrolyte disorders in community subjects: prevalence and risk factors. Am J Med. 2013;126(3):256–263. doi:10.1016/j.amjmed.2012.06.037
15. Khan R, Saba F, Kausar S, Siddiqui M. Pattern of electrolyte imbalance in type 2 diabetes patients: experience from a tertiary care hospital. Pak J Med Sci. 2019;35(3):797. doi:10.12669/pjms.35.3.844
16. Arpaci D, Tocoglu A, Ergenc H, Korkmaz S, Ucar A, Tamer A. Associations of serum magnesium levels with diabetes mellitus and diabetic complications. Hippokratia. 2015;19(2):153.
17. Corona G, Giuliani C, Parenti G, et al. The economic burden of hyponatremia: systematic review and meta-analysis. Am J Med. 2016;129(8):823–35. E4. doi:10.1016/j.amjmed.2016.03.007
18. Baldrighi M, Sainaghi P, Bellan M, Bartoli E, Castello L. Hyperglycemic hyperosmolar state: a pragmatic approach to properly manage sodium derangements. Curr Diabetes Rev. 2018;14(6):534–541. doi:10.2174/1573399814666180320091451
19. Sayouba J, Asanghanwa M, Njouendou A, Kamga H, Assob J. Electrolyte imbalance in type 2 diabetes: a case study from the west region of Cameroon. Int J Res Med Sci. 2020;8:2017–2022. doi:10.18203/2320-6012.ijrms20202236
20. Circumference WW. Waist-Hip Ratio Report of a WHO Expert Consultation. Data Wlcip, Editor; 2008.
21. Al-Makki A, Dipette D, Whelton P, et al. Hypertension pharmacological treatment in adults: a World Health Organization guideline executive summary. Hypertension. 2022;79(1):293–301. doi:10.1161/HYPERTENSIONAHA.121.18192
22. Megerssa Y, Gebre M, Birru S, Goshu A, Tesfaye D. Prevalence of undiagnosed diabetes mellitus and its risk factors in selected institutions at Bishoftu Town, East Shoa, Ethiopia. J Diabetes Metab. 2013;8:S12.
23. American Diabetes Association. Standards of medical care in diabetes-2017: summary of revisions. Diabetes Care. 2017;40(Suppl 1):S4–S5. doi:10.2337/dc17-S003
24. Anago E, Medehouenou T, Akpovi C, Tchehouenou H. Electrolyte disturbances in diabetic patients in Cotonou, Benin. Int J Res Med Sci. 2016;4(12):5430–5435. doi:10.18203/2320-6012.ijrms20164223
25. Karuppan A, Sahay M, Ravindranathan R, Haripriya P, Sriram D, George M. Electrolyte disturbances among diabetic patients admitted in a multi-specialty hospital in Southern India. J Clin Diagn Res. 2019;13(2):54.
26. Ahmed S, Nur F, Ullah M, et al. Factors influencing hyponatremia in hospitalized diabetic patients- a cross sectional study. Med Today. 2014;26:04–08. doi:10.3329/medtoday.v26i1.21301
27. Ahmed S, Nur F, Ullah M, et al. Electrolyte imbalance in admitted diabetic patients: patterns and factors responsible- a cross sectional study. Kyamc J. 2017;5(1):458–466. doi:10.3329/kyamcj.v5i1.32317
28. Antony S. A study of electrolyte imbalance in diabetic patients at a teritary care hospital in Kerala. Int J Contemp Med. 2019;7(1):132. doi:10.5958/2321-1032.2019.00006.8
29. Unachukwu M, Engwa G, Nwalo F, et al. Influence of type 2 diabetes on serum electrolytes and renal function indices in patients. J Clin Diagn Res. 2018;12(6):87.
30. Kurstjens S, De Baaij J, Bouras H, Bindels R, Tack C, Hoenderop J. Determinants of hypomagnesemia in patients with type 2 diabetes mellitus. Eur J Endocrinol. 2017;176(1):11–19. doi:10.1530/EJE-16-0517
31. Waanders F, Dullaart R, Vos M, et al. Hypomagnesaemia and its determinants in a contemporary primary care cohort of persons with type 2 diabetes. Endocrine. 2020;67(1):80–86. doi:10.1007/s12020-019-02116-3
32. Paladiya R, Pitliya A, Choudhry A, et al. Association of low magnesium level with duration and severity of type 2 diabetes. Cureus. 2021;13(5):E15279. doi:10.7759/cureus.15279
33. Pokharel D, Khadka D, Sigdel M, et al. Association of serum magnesium level with poor glycemic control and renal functions in Nepalese patients with type 2 diabetes mellitus. Diabetes Metab Syndr. 2017;11:S417–S23. doi:10.1016/j.dsx.2017.03.028
34. Mustafa A, Abubaker N, Suliman A, Ibrahim M, Hamza A, Elfaki E. Assessment of electrolytes level among type 2 diabetes Sudanese patients. J Glob Biosci. 2020;9(3):6921–6926.
35. Halushko O, Boliuk M, Hypophosphatemia in patients with acute stroke and diabetes mellitus: diagnosis and treatment. Emerg Med. 2021;(2.89):53–57. doi:10.22141/2224-0586.2.89.2018.126603
36. Ditzel J, Lervang H. Disturbance of inorganic phosphate metabolism in diabetes mellitus: clinical manifestations of phosphorus-depletion syndrome during recovery from diabetic ketoacidosis. Diabetes Metabol Syndr Obes. 2010;3:319–324. doi:10.2147/DMSO.S13476
37. Ahmed S, Nur F, Ullah M, Mamun A, Aminul M. Factors precipitating hypokalemia in diabetic patients: a cross sectional study. J Enam Med Coll. 2014;4:145–150. doi:10.3329/jemc.v4i3.20940
38. Janma J, Changsirikulchai S, Sangthawan P, Thokanit N, Rattanamongkolgul S, Thinkhamrop B. Serum potassium levels in Thai patients with T2dm and Egfr greater than or equal to 90 ml/min/1.73 m2. Trends Med. 2019;19. doi:10.15761/TiM.1000178
39. Ahn C, Kang J, Jeung E. Calcium homeostasis in diabetes mellitus. J Vet Sci. 2017;18(3):261–266. doi:10.4142/jvs.2017.18.3.261
40. Al-Jameil N. Estimation of serum electrolytes in diabetes patients of Saudi region. Life Sci J. 2014;11(7):378–380.
41. Amballi A, Kayode B, Odusan O, et al. Cortisol and electrolyte levels in type 2 diabetic patients attending a state university teaching hospital, Ogun State, Nigeria. Int J Biomed Health Sci. 2019;14(2):175.
42. Talabani N. Serum electrolytes and lipid profiles in non-insulin dependent diabetes mellitus patients. Asian J Med Sci. 2014;6(3):38–41. doi:10.3126/ajms.v6i3.11088
43. Wang S, Hou X, Liu Y, et al. Serum electrolyte levels in relation to macrovascular complications in Chinese patients with diabetes mellitus. Cardiovasc Diabetol. 2013;12(1):1–10. doi:10.1186/1475-2840-12-146
44. Rajagambeeram R, Malik I, Vijayan M, Gopal N, Ranganadin P. Evaluation of serum electrolytes and their relation to glycemic status in patients with T2dm. Int J Clin Biochem Res. 2020;6:10.
45. Nwankwor H, Nwatu C, Okwara C, et al. Low serum calcium levels occur in Nigerian adults with type 2 diabetes and correlates negatively with their glycosylated hemoglobin levels: a case‑control study. Niger J Med. 2020;29(2):229–233. doi:10.4103/NJM.NJM_25_20
46. Najeeb Q, Aziz R, Hamid S. To evaluate the levels of glycated hemoglobin, serum calcium, magnesium, phosphate, uric acid and microalbuminuria in patients with newly diagnosed type 2 diabetes mellitus. Int J Res Med Sci. 2014;2(4):1462–1465. doi:10.5455/2320-6012.ijrms20141140
47. Mishra S, Padmanaban P, Deepti G, Sarkar G, Sumathi S, Toora B. Serum magnesium and dyslipidemia in type-2 diabetes mellitus. Biomed Res. 2012;23(2):295–300.
48. Winzer E, Grabovac I, Ludvik B, et al. Differences in serum magnesium levels in diabetic and non-diabetic patients following one-anastomosis gastric bypass. Nutrients. 2019;11(9):1984. doi:10.3390/nu11091984
49. Yunka T, Mogas S, Zawdie B, et al. The hidden burden of diabetes mellitus in an urban community of Southwest Ethiopia. Diabetes Metabol Syndr Obes. 2020;13:2925. doi:10.2147/DMSO.S269386
50. Pannem R, Munamala C. An observational study on effects of hypomagnesemia among critically ill patients at a tertiary care hospital. Int J Adv Med. 2018;5:1347. doi:10.18203/2349-3933.ijam20184254
51. Palmer BF, Clegg DJ. Electrolyte disturbances in patients with chronic alcohol-use disorder. N Engl J Med. 2017;377(14):1368–1377. doi:10.1056/NEJMra1704724
52. Elisaf M, Kalaitzidis R. Metabolic abnormalities in alcoholic patients: focus on acid base and electrolyte disorders. J Alcohol Drug Depend. 2015;2015:26.
53. Parmar S, Singh S, Singh G. Role of hyperglycemia in the pathogenesis of Na±/K±disturbance. Int J Res Med Sci. 2016;4(4):1167–1171. doi:10.18203/2320-6012.ijrms20160803
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
High Magnitude of Fecal Carriage of Extended-Spectrum Beta-Lactamase-Producing Enterobacteriaceae at Debre Berhan Comprehensive Specialized Hospital, Ethiopia
Shenkute D, Legese MH, Yitayew B, Mitiku A, Engidaye G, Gebremichael S, Asrat D, Woldeamanuel Y
Infection and Drug Resistance 2022, 15:2445-2458
Published Date: 9 May 2022
Assessment of Blood Donation Practice and Its Associated Factors Among Wollega University Undergraduate Students, Ethiopia
Shama AT, Teka G, Lemu SY, Tesfaye B, Ebisa H, Gebre DS, Terefa DR
Journal of Blood Medicine 2022, 13:711-724
Published Date: 24 November 2022
Caregivers’ Satisfaction of Teleconsultations and Associated Factors During COVID-19 Pandemic at Pediatric Clinics of Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia: A Cross-Sectional Study
Abegaz AK, Tamire AH, Asfaw H
Pediatric Health, Medicine and Therapeutics 2023, 14:185-196
Published Date: 29 May 2023
Prevalence and Associated Factors of Diabetes Mellitus Among Newly Enrolled Tuberculosis Patients in Lubumbashi (DRC)
Kakisingi C, Mwamba C, Muteba MK, Kasamba E, Kabamba M, Tanon A, Situakibanza H
Risk Management and Healthcare Policy 2024, 17:171-180
Published Date: 17 January 2024
Prevalence of Diabetes and Associated Factors Among Government Employees of Mizan-Aman Town and Zonal Sector Office, Bench Sheko Zone, Southwest Ethiopia Region, 2022
Zegeye MY, Yosef T, Asres A
Diabetes, Metabolic Syndrome and Obesity 2024, 17:725-738
Published Date: 12 February 2024