")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Prevalence and Associated Factors of Diabetes Mellitus Among Newly Enrolled Tuberculosis Patients in Lubumbashi (DRC)
Authors Kakisingi C , Mwamba C, Muteba MK, Kasamba E , Kabamba M , Tanon A, Situakibanza H
Received 16 October 2023
Accepted for publication 10 January 2024
Published 17 January 2024 Volume 2024:17 Pages 171—180
DOI https://doi.org/10.2147/RMHP.S436873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Christian Kakisingi,1 Claude Mwamba,1 Michel Kasongo Muteba,2 Eric Kasamba,3 Michel Kabamba,4 Aristophane Tanon,5 Hippolyte Situakibanza6
1Internal Medicine Department, University of Lubumbashi, Lubumbashi, Democratic Republic of the Congo; 2Division of Epidemiology and Biostatistics, University ofWitwatersrand, Johannesburg, Republic of South Africa; 3Department of Basics Sciences. University of Lubumbashi, Lubumbashi, Democratic Republic of the Congo; 4Public Health Department, University of Kamina, Kamina, Democratic Republic of the Congo; 5Specialities and Medicine Department, University of Félix Houphouët-Boigny of Abidjan Cocody, Abidjan, Ivory Coast; 6Internal Medicine Department, Tropical Diseases, Infectious and Parasitic Department, University of Kinshasa, Kinshasa, Democratic Republic of the Congo
Correspondence: Christian Kakisingi, Email [email protected]
Background: Tuberculosis and diabetes mellitus are major public health challenges worldwide. The two scourges have bidirectional relationship with high morbidity and mortality.
Objective: The present study was conducted to determine the prevalence of diabetes mellitus and identify related factors in patients with tuberculosis.
Methods: A cross-sectional study was conducted in 11 tuberculosis screening and treatment centers in Lubumbashi (DRC) from September to December 2022. Adult patient with a positive smear for tuberculosis were systematically screened for diabetes mellitus. Demographic characteristics, history and symptomatology were the variables of interest. Data was entered using Microsoft Excel software. STATA 16 software was used for analysis.
Results: A total of 255 tuberculosis patients were recruited and the prevalence of diabetes mellitus among these patients was 11.4% (ie, 29 out of 255). After uni and multivariate logistic regression, a BMI ≤ 18.5 Kg/m2, lack of employment, polyuria and intense thirst were the factors associated with diabetes mellitus in tuberculosis patients.
Conclusion: The prevalence of diabetes mellitus in smear positive tuberculosis patients in the present study was higher than the one observed in Central Africa.
Keywords: tuberculosis, diabetes mellitus, comorbidity, prevalence, associated factors
Introduction
Tuberculosis (TB) is a contagious disease and of the top 10 killers worldwide.1 Globally, an estimated 10.6 million (9.9–11 million) people have been infected with TB and 1.4 million (1.3–1.5 million) people have died of this disease in the year 2022. The Democratic Republic of Congo (DRC) is one of the 22 countries most affected by this condition.2 Previous studies by Kakisingi et al3,4 in the south of the DRC had shown the epidemiological impact of this scourge in terms of morbidity and mortality from this disease in Lubumbashi, in particular.
Currently, non-communicable diseases (NCDs) constitute a growing global epidemic that disproportionately affects low- and middle-income countries (LMICs) where, at the same time, the impact of infectious diseases is high.5 This phenomenon seems to be influenced by the advance of industrialization and urbanization which contribute to lifestyle changes, mainly in dietary habits, leading to increased rates of obesity and type 2 diabetes mellitus (DM).6 And some authors estimate that the number of people living with DM type 2 should double between 2000 and 2030.7 In the DRC, the prevalence of DM reported by the literature varies between 3.5 and 14% and nearly 23,000 deaths are attributed to DM.6,8,9
Studies have shown that DM and TB are two overlapping diseases.10,11 This strong coexistence is particularly accentuated in LMICs, where nearly 95% of the world’s population with TB and 70% with DM live.12,13 Systematic reviews suggest that people with DM are about three times more likely to develop TB than the general population.11,14 Additionally, people with TB-DM comorbidity on anti-TB treatment have a higher risk of treatment failure and higher death compared to people with TB alone.15
Worldwide, estimates of the prevalence of DM in TB patients differ depending on the geographic region and the socio-demographic characteristics of the patients examined.5 And recent studies have shown that the prevalence of DM among patients with TB is variable depending on the series and regions. This varies from 50% compared to some studies carried out in India, to around 30% in Mexico, to less than 10% in the United States of America, and to even lower values in certain African countries such as Benin. (1.5%).5,16,17 In the DRC, the approach to this subject has focused on assessing the knowledge of healthcare providers. In a study carried, Kakisingi et al, identified gaps in the recommendations of the national TB control programme.18
Globally, there is growing concern about this comorbidity19,20 and although DM screening in all newly diagnosed TB patients is recommended by the WHO, the Union Against Tuberculosis and Respiratory Diseases (UNION) and the DRC National Guidelines on the management of TB,1,21,22 this association has not yet been the subject of an in-depth analysis of the situation in the DRC.
The objectives of this study are to determine the prevalence of diabetes mellitus and identify the factors associated in patients TB at TB screening and treatment centers (STC) in Lubumbashi.
Methods
Study Type, Period, Setting and Sampling
This was an analytical cross-sectional study conducted in Lubumbashi, DRC, over a three-month period from September to December 2022.
The city of Lubumbashi is divided into eleven medical districts (MD). The study was conducted in 6 MDs of Lubumbashi. Patients were recruited by a two-stage sampling technique. Initially, these MDs were selected from all of Lubumbashi’s MDs by simple random sampling. The study concerned the MDs of Kampemba, Kenya, Kisanga, Lubumbashi, Ruashi and Tshamilemba. In each selected MD, the first two STCs (one in Lubumbashi MD) notifying and treating the highest proportion of TB patients were identified and selected for the survey. A total of 11 STCs that offer TB care were selected for the survey.
The sample size was calculated using a single proportion formula with the assumption of a 95% CI and a margin of error of 5% and a DM hospital frequency of 8.5% in TB patients admitted to the Pulmonary Departments of Mulago National Referral and Teaching Hospital in Kampala, Uganda.23 This hospital frequency was chosen given the similarity between the populations of Uganda and the DRC. Thus, the calculated sample size obtained is 120.
n = [Zα2(p)*(1 - p) /d2] = [1.962*0.085*(1–0.085) /0.052] = 120 and with the addition of a twenty percent non-response rate, the minimum sample size has become 150.
Study Population
The study population consisted of patients who visited the selected STCs during the study period.
Selection Criteria
We included all newly diagnosed adult patients with smear positive confirmed tuberculosis (TB+) whose diagnosis of TB was performed in accordance with the standards issued by the national tuberculosis programme (NTP) using diagnostic tests such as the Gene Xpert MTB/RIF Ultra test or sputum microscopy.22
Exclusion criteria included Mycobacterium tuberculosis (Mtb) positive culture confirmed MDR-TB cases and patients with extra-pulmonary TB (EPT), patients under 18 years old and pregnant patients.
Operational Definitions
Case Definition in TB Control
- smear positive confirmed case of tuberculosis (TB+): Any patient whose biological sample has been established by smear microscopy, culture or WHO-endorsed Rapid Diagnostic Test (RDT) (eg, Xpert MTB/RIF).22
- Pulmonary tuberculosis (PT) refers to any case of smear positive confirmed tuberculosis (PT+) in which the pulmonary parenchyma or the tracheobronchial tree is affected.22
Diagnosis Criteria for Diabetes Mellitus
Is considered diabetic any patient whose:24,25
- Fasting blood glucose ≥ 126 mg/dL (7.0 mmol/L). Fasting is defined as no calorie intake for at least 8 hours.
- Blood glucose 2 h after a 75g glucose load during orally induced hyperglycemia ≥ 200 mg/dL (11.1 mmol/L).
- Glycated hemoglobin ≥ 6.5% (48 mmol/mol).
- Or when in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, a random blood glucose level ≥ 200 mg/dL (11.1 mmol/L).
Is considered prediabetic any patient whose blood sugar at the threshold considered normal and but below the threshold to confirm diabetes is a blood sugar between 140 and 199 mg / dl in case of random measurement of blood sugar and between 110 and 125 mg / dl in case of fasting blood glucose testing.26
Calculation of Body Mass Index
BMI (kg/m2) was calculated using the formula: BMI = Weight (kg)/Height2 (m2). Weight loss, normal weight, overweight and obesity were defined using the method described by Wikner et al 2012.27 The BMI threshold values for underweight, normal weight, overweight and obesity were respectively ˂ 18.5 kg/m2, 18.5 to 25 kg/m2, 25 to 30 kg/m2, > 30kg/m2.
Variables of Interest
The following parameters were analyzed:
- socio-demographic parameters: age, sex, BMI, marital status, level of education, place of residence, monthly income, employment.
- the patient’s history: personal history of diabetes, family history of diabetes, alcohol consumption, tobacco consumption, hypertension, HIV, contact with a TB patient.
- the patient’s symptoms: fever, anorexia, weight loss, clinical anemia, asthenia, dyspnea, hemoptysis, polyuria, intense thirst.
- biological parameters: glycaemia dosage.
DM Screening Procedure
All the patients included in the study were interviewed during their first visit, ie the initiation of their anti-TB treatment. Sociodemographic, anamnestic (complaints, personal and family history) and physical parameters were assessed. All eligible patients were screened for DM, irrespective of prior diabetes status, as follows: A fasting blood glucose test was performed: if the level was below 126 mg/dl, no further action was taken. If this was ≥ 126 mg/dl, the patient was asked to return for a fasting blood glucose test the next day.17 A glucometer (SD CodefreeTM Blood Glucose Monitoring System, SD Biosensor, INC., Cheongju-si, Chungcheongbuk-do, Republic of Korea) was used for DM screening and an ISO 13485:2016 certified CYANElite 290 analyzer was used in second intention.
Collecting Data
A structured questionnaire was administered to all participants to obtain information on sociodemographic characteristics, family history of SD, personal history of SD, tobacco use, alcohol consumption, education level, marital status, and physical signs. Anthropometric parameters, including height and weight, were measured by trained nurses according to standard procedures.
Statistical Analysis
The data collected was analyzed using STATA 16 software (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC).
A descriptive analysis of the study population was performed using summary statistics including means and standard deviations for continuous variables when the data distribution was normal, and medians and their interquartile ranges when the data distribution was asymmetric. Categorical variables were characterized by frequencies and proportions.
To identify factors associated with TB-DM comorbidity, simple logistic regression was performed, and odds ratios, 95% confidence intervals, and p-values were calculated for each independent variable at a significance level of 5%. In multivariate logistic regression, independent variables with p-value less than 0.10 were included to control for potential confounders and generate a final model, which was then assessed using the fit test.
Ethical Considerations
The approval of the Ethics Committee of the University of Lubumbashi (UNILU/CEM/113/2022) was obtained after administrative authorization from the Provincial Health Division (N° DPS/H KAT/900/PX 000962/JMK /2022).
Written informed consent was taken from all eligible participants before enrolment. The information obtained from our patients was treated confidentially, and the analysis of this data was carried out anonymously in accordance with the Helsinki declaration.
No conflicts of interest were reported in the conduct of the study.
Results
In the present study, 255 smear positive tuberculosis patients were included, among whom 29 (11.4%) had TB-DM comorbidity. The results are reported in Tables 1–4.
 |
Table 1 General Characteristics of Smear Positive TB Patients |
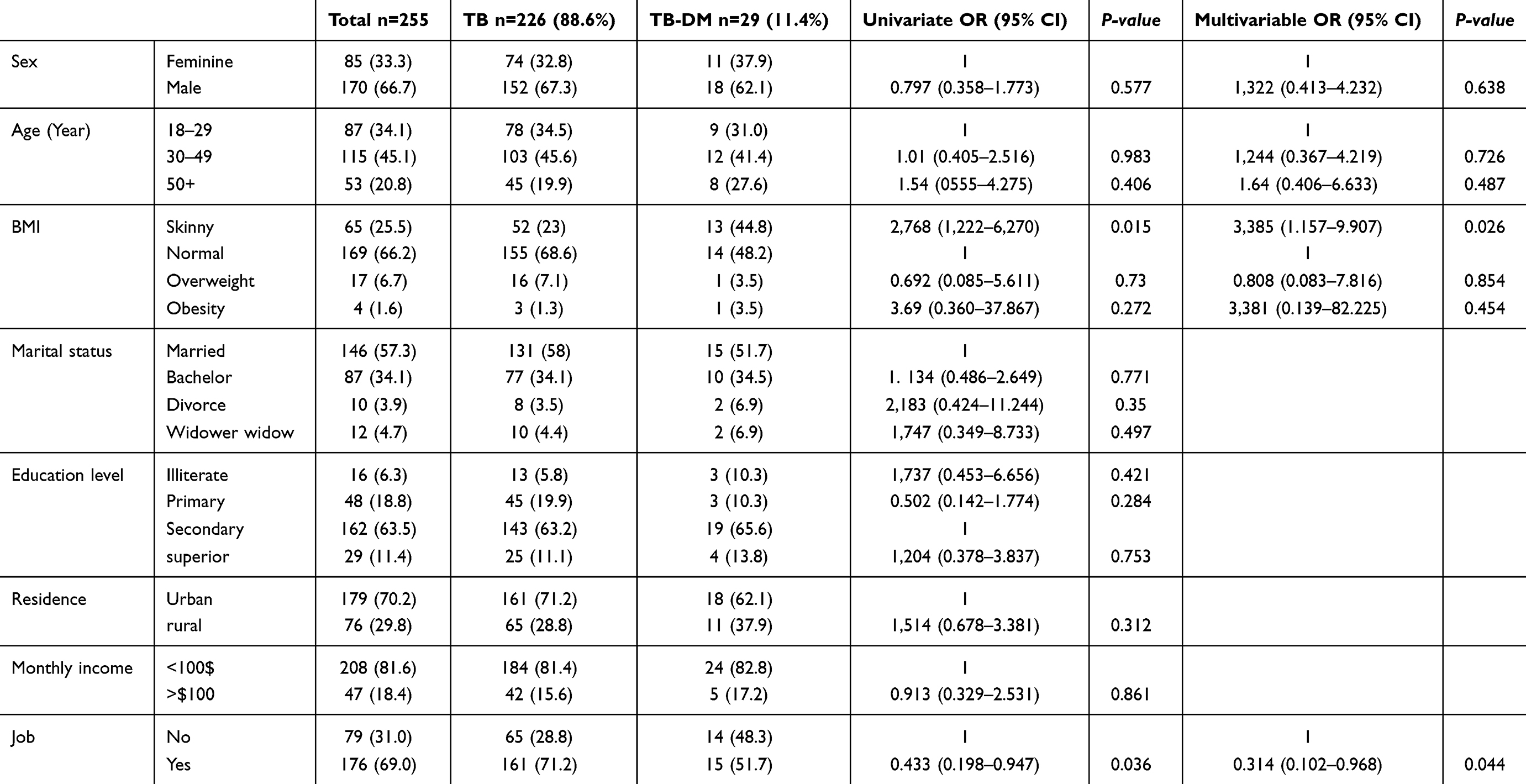 |
Table 2 Patients Socio-Demographics Details |
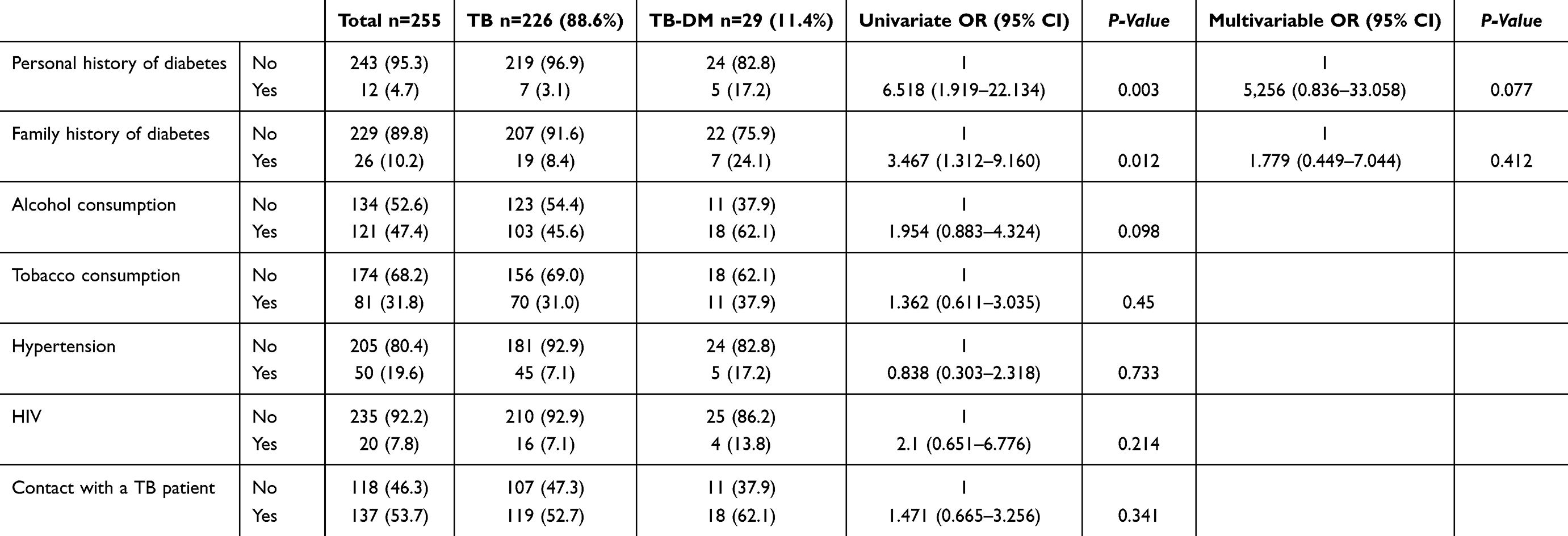 |
Table 3 Clinical History Data at Enrolment |
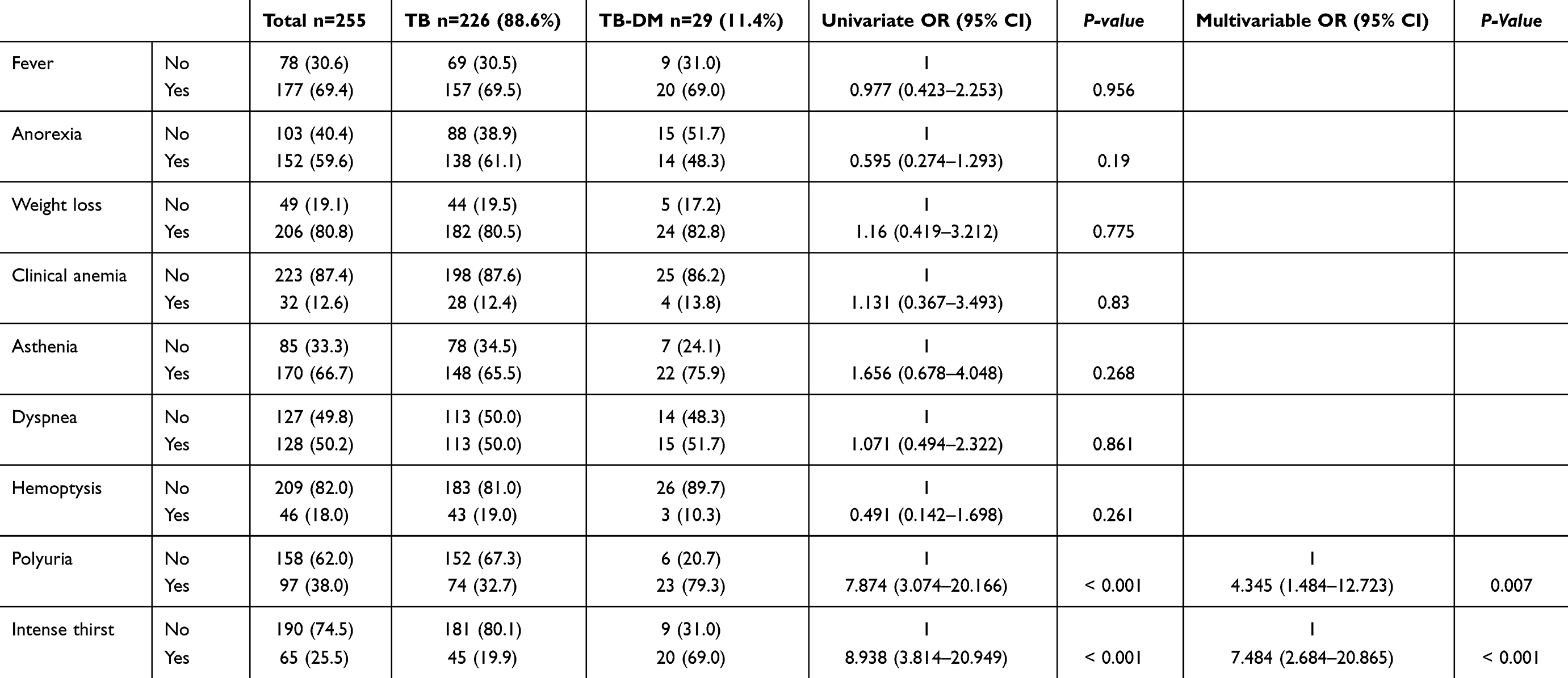 |
Table 4 Distribution of TB Patients According to Symptomatology |
Table 1 indicates that the median age of our patients was approximately 35 years, and that the median BMI was within the normal range. It also shows that 33.3% of the study population had a blood sugar level compatible with prediabetes.
The socio-demographic characteristics of the patients studied are presented below in Table 2. We observe a predominantly male population (66.7%°) whose distribution of age groups is similar in patients with TB and TB-DM. It appears, also in this table, that a BMI lower than the normal and having a job are factors with a significant association after adjustment.
From the history as presented in Table 3, we note that, among the patients with TB-DM comorbidity, 17.2% declared having a personal history of DM and 24.1% a family history of DM. Also, 7.2% of them had HIV-TB co-infection. It is also observed that no factor related to the history, after multivariate analysis, is found to be significantly associated with this comorbidity, although factors such as a personal history of DM and family history of DM were after simple analysis.
Table 4 summarizes the symptoms experienced by our study population and shows the classic signs of TB are expressed by the latter without significant association and that, in relation to DM, we note the symptoms related to DM are significantly associated with TB-DM comorbidity (Polyuria ORa = 4.345 p = 0.007 and Intense thirst ORa = 7.484 p < 0.001).
Discussion
The present study aimed to determine the prevalence of DM among smear positive tuberculosis patients and to identify the various factors that may be associated with this comorbidity.
This study reveals a prevalence of 11.4% of DM in TB patients. In sub-Saharan Africa, studies published between 1980 and 2017 indicate a prevalence ranging from 1.9% to 38%.5,23 The results observed in the present study are comparable to those obtained by Ogbera et al28 in Nigeria but remain different from those obtained by other authors such as Owiti et al and Fonkeng et al which have respectively prevalences of 6.7% and 9.5%, which are lower prevalences than our observation.29,30 It has also been found that our observation is inferior not only to certain results obtained in Africa by Ekeke et al14 in southern Nigeria, but also in some studies conducted around the world.17,31 The difference in methodology in terms of sample size and/or type of study could be the first reason to mention to explain this discordance of observation in the world. However, we believe that these arguments are not sufficient to justify the discrepancy alone. Therefore, we believe that the socio-demographic characteristics, the morbidity, and mortality due to these two scourges combined could be additional arguments to explain this variable. Several studies conducted in Guinea-Bissau and Benin have shown that the prevalence of TB-DM comorbidity seems to be lower in countries where the prevalence of TB or DM is also low; On the other hand, others think that eating habits should not be neglected as regards the appearance of DM in some people; which could be a factor that could influence the frequency of this comorbidity.17
A prevalence for prediabetes of 33.3% was observed among our patients and this appears to be identical to that observed by Sheuly et al in Bangladesh where a prevalence of 34% is proven and lower than that obtained by Viswanathan et al in India (41.1%).32,33 Many literatures claim that prediabetes progresses in 25% of cases to DM within 3–5 years, and up to 70% of people known to be prediabetic develop DM during their lifetime.26,34,35 Hostalek et al,26 report, in a literature review, that prediabetes is increasingly recognized as an important metabolic condition; in addition to predisposing individuals to a high probability of future progression to DM, people with prediabetes are at an increased risk of developing many of the complications normally associated with this disease.
A few associated factors were identified in the present study, namely a lower than normal BMI (ORa = 3.385 [1.157–9.907]), being unemployed (ORa = 0.314 [0.102–0.968]), the existence of a history diabetes in the TB patient (ORa = 5.226 [0.836–33.058]), the existence of a family history of SD in the tuberculosis patient (ORa = 1.779 [0.449–7.041]) and among the patient’s complaints, the presence of polyuria (ORa = 4.345 [1.484–12.723]) and that of intense thirst (ORa = 7.484 [2.684–20.865]). These factors identified in our study population are different from those observed in the studies of Adane et al and Ekeke et al17,24 Their studies mention that the age of the patients would be a non-negligible factor in TB-DM comorbidity, and consider that the greater the age, the greater the susceptibility to suffer from this co-morbidity.17,24 In relation to this observation, our results, like those obtained by Fonkeng et al30 in Cameroon, make the same observation, although no significant difference could be found.
As for the associated factors related to the history and symptomatology of the patients concerned, these can be considered as factors with collinear effects. Notwithstanding this fact, it remains, all the same, important to take them into account regarding their orientation character for the diagnosis or a targeted screening of SD in a setting with limited resources such as the DRC.
The main strength of this study is that it is, is, to our knowledge, the first of its kind in the DRC. TP+ patients were systematically screened for DM at the start of their antituberculosis treatment. Also, it is of undeniable interest in the organization of the fight against TB and its comorbidities because:
- Early detection of DM in tuberculosis patients is of vital importance in view of the harmful effects of this scourge in the DRC and the increasing morbidity due to DM in the country. And the implementation of strategies adapted to the epidemiological context of our country can improve the intervention capacities to achieve the objectives proposed by the NTP.
- Targeted screening of patients over the age of 50, with even a BMI even below normal, who present polyuria and/or intense thirst among the complaints, could be a first way to ensure early detection given our current results and the technical platform of our STCs.
However, the study has some limitations. Indeed, the results cannot be generalized to all tuberculosis patients because:
- the study only focused on patients from a few STCs in Lubumbashi.
- it did not include smear negative tuberculosis patients and those with EPT.
Also, the use of only FGG and IFG screening tests in the study requires further work by exploiting, among other things, glycated hemoglobin for its high sensitivity despite its high cost for DM screening in tuberculosis patients.
Conclusion
The present study showed a prevalence of TB-DS comorbidity higher than that revealed in the Central African zone. Strategies for early detection of diabetes mellitus in tuberculosis patients need to be put in place, given the epidemiological, clinical, and technical context. In the fight against TB-DM comorbidity, considering the rural environment is necessary for the definition of its real mapping.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Tuberculosis. Geneva: World Health Organization; 2022.
2. World Health Organization. Global Tuberculosis Report 2022. Geneva: World Health Organization; 2022.
3. Ngama CK, Muteya MM, Lukusha YII, et al. Epidemiological and clinical profile of tuberculosis in the health zone of Lubumbashi (DR Congo). Pan Afr Med J. 2014;17:70. doi:10.11604/pamj.2014.17.70.2445
4. Kakisingi C, Mukuku O, Kajimb P, et al. Treatment outcome of tuberculosis patients with HIV under directly observed treatment short course (dots) in Lubumbashi (DR Congo). J Infect Dis Med Microbiol. 2018;2(2):26–31.
5. Alebel A, Wondemagegn AT, Tesema C, et al. Prevalence of diabetes mellitus among tuberculosis patients in sub-saharan Africa: a systematic review and meta-analysis of observational studies. BMC Infect Dis. 2019;19(1):254. doi:10.1186/s12879-019-3892-8
6. International Diabetes Federation. IDF. Available from: https//www.diabetesatlas.org.
7. Faurholt-Jepsen D, Range N, PrayGod G, et al. Diabetes is a risk factor for pulmonary tuberculosis: a case control study from Mwanza, Tanzania. PLoS One. 2011;6(8):e24215. doi:10.1371/journal.pone.0024215
8. Katshunga P, Masumbuko B, Hermans M, M’Buyamba-Kabangu J, Hermans M-P, M’Buyamba-Kabangu J-R. Age and living in an urban environment are major determinants of diabetes among South Kivu Congolese adults. Diabetes Metab. 2012;38(4):324–337. doi:10.1016/j.diabet.2012.02.008
9. Longo-Mbenza B, Nguma DV, Nahimana D, et al. Screen detection and the WHO stepwise approach to the prevalence and risk of arterial hypertension in Kinshasa. Eur J Cardiovas Prev Rehab. 2008;15(5):530–538. doi:10.1097/HJR.0b013e3282f21640
10. Jeon CY, Murray MB. Diabetes mellitus increases the risk of active tuberculosis: a systematic review of 13 observational studies. PLoS Med. 2008;5(7):e152. doi:10.1371/journal.pmed.0050152
11. Cy J, Ad H, Ma B, et al. Bi-directional screening for tuberculosis and diabetes: a systematic review. Too Med Int Health. 2010;15(11):1300–1314. doi:10.1111/j.1365-3156.2010.02632.x
12. Sen T, Joshi SR, Udwadia ZF. Tuberculosis and diabetes mellitus: merging epidemics. J Assoc Physic India. 2009;57(1):399–404.
13. Sousa GGS, Pascoal LM, Costa ACPJ, et al. Trend and factors associated with tuberculosis-diabetes mellitus comorbidity in a northeastern Brazilian municipality. Rev Bras Enferm. 2021;74(3):e20201238. doi:10.1590/0034-7167-2020-1238
14. Omar N, Wong J, Thu K, Ma A, Chaw L. Prevalence and associated factors of diabetes mellitus among tuberculosis patients in Brunei Darussalam: a 6-year retrospective cohort study. Inter J Infect Dis. 2021;105:267–273. doi:10.1016/j.ijid.2021.02.064
15. Ma B, Ad H, Cy J, et al. The impact of diabetes on tuberculosis treatment: a systematic review. BMC Med. 2011;9:81. doi:10.1186/1741-7015-9-81
16. Alturki S, Al Amad M, Mahyoub E, Al Hanash N, Alhammadi A. Prevalence of diabetes mellitus among patients with tuberculosis and its associated factors in Sana’a, Yemen, 2021. Epidemiologia. 2023;4(2):202–211. doi:10.3390/epidemiologia4020021
17. Ekeke N, Ukwaja KN, Chukwu JN, et al. Screening for diabetes mellitus among tuberculosis patients in southern Nigeria: a multi-centre implementation study under program settings. Sci Rep. 2017;7:44205. doi:10.1038/srep44205
18. Kakisingi C, Kabamba M, Muteba M, et al. Health care providers’ knowledge of tuberculosis and diabetes mellitus comorbidity in Lubumbashi, Democratic Republic of the Congo DRC. J Multidiscip Healthc. 2023;31:16.
19. Dooley KE, Chaisson RE. Tuberculosis and diabetes mellitus: convergence of two epidemics. Lancet Infect Dis. 2009;9(12):737–746. doi:10.1016/S1473-3099(09)70282-8
20. Bailey SL, Ayles H, Beyers N, Godfrey-Faussett P, Muyoyeta MToit E. et al.. The association of hyperglycaemia with prevalent tuberculosis: a population-based cross-sectional study. BMC Infect Dis. 2016;16(1):733. (). doi:10.1186/s12879-016-2066-1
21. International union against tuberculosis and lung disease.Tuberculosis management essentials guide; 2019.
22. National Tuberculosis Control Program. Tuberculosis care guide PATI 6.; 2021.
23. Kibirige D, Ssekitoleko R, Mutebi E, Worodria W. Overt diabetes mellitus among newly diagnosed Ugandan tuberculosis patients: a cross sectional study. BMC Infect Dis. 2013;13(1):122. doi:10.1186/1471-2334-13-122
24. World Health Organization. Diabetes. Geneva: Elsevier; 2023.
25. Elsayed N, Aleppo G, Aroda VR, et al. Classification and diagnosis of diabetes: standards of care in diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S19–S40. doi:10.2337/dc23-S002
26. Hostalek U. Global epidemiology of prediabetes - present and future perspectives. Clin Diabetes Endocrinol. 2019;5(1):5. doi:10.1186/s40842-019-0080-0
27. Wikner C, Gigante B, Hellénius ML, de Faire U, Leander K. The risk of type 2 diabetes in men is synergistically affected by parental history of diabetes and overweight. PLoS One. 2012;8(4):e61763. doi:10.1371/journal.pone.0061763
28. Ogbera OA, Adeyeye O, Odeniyi IA, Adeleye O. Knowledge of diabetes mellitus in tuberculosis amongst healthcare workers in Nigeria. Indian J Endocr Metab. 2013;17(4):704–708. doi:10.4103/2230-8210.113765
29. Owiti P, Keter A, Harries AD, et al. Diabetes and pre-diabetes in tuberculosis patients in western Kenya using point-of-care glycated haemoglobin. Public Health Action. 2017;7(2):147–154. doi:10.5588/pha.16.0114
30. Fonkeng LS, Ali IM, Noubom Met al. Prevalence, predictors and treatment outcome of type 2 diabetes among newly diagnosed sputum positive pulmonary tuberculosis patients in western Cameroon. J Infect Dis Epidemiol. 2017;3(2):031. doi:10.23937/2474-3658/1510031
31. Du Q, Wang L, Long Q, Zhao Y, Abdullah AS. Systematic review and meta-analysis: prevalence of diabetes among patients with tuberculosis in China. Trop Med Int Health. 2021;26(12):1553–1559. doi:10.1111/tmi.13686
32. Sheuly AH, Arefin ZH, Barua L, Zaman MS, Chowdhury HA. Prevalence of type 2 diabetes and pre-diabetes among pulmonary and extrapulmonary tuberculosis patients of Bangladesh: a cross-sectional study. Endocrinol Diab Metab. 2022;5(3):e00334. doi:10.1002/edm2.334
33. Viswanathan V, Devarajan A, Kumpatla S, Dhanasekaran M, Babu S, Kornfeld H. Having prediabetes before detection of tuberculosis: does it have a negative influence on treatment. Diabetes. 2020;69(1):1478–P. doi:10.2337/db20-1478-P
34. Tabak AG, Herder C, Rathmann W, Brunner EJ, Kivimaki M. Prediabetes: a high-risk state for diabetes development. Lancet. 2012;379(9833):2279–2290. doi:10.1016/S0140-6736(12)60283-9
35. de Souza CF, Gross JL, Gerchman F, Leitao CB. Pre-diabetes: diagnosis, evaluation and treatment of chronic complications. Arq Arm Endocrinol Metab. 2012;56:5.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.