Back to Journals » Infection and Drug Resistance » Volume 19
Antimicrobial Resistance in Intensive Care Units in Somalia: A Commentary on Measurement Gaps and Facility-Level Priorities for Infection Prevention and Stewardship
Authors Hassan AM, Siyad AO ![]() , Hussein AM
, Hussein AM ![]()
Received 2 March 2026
Accepted for publication 15 May 2026
Published 18 May 2026 Volume 2026:19 606434
DOI https://doi.org/10.2147/IDR.S606434
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chi H. Lee
Abdukadir Mohamed Hassan,1 Ahmed Omar Siyad,1 Abdiwali Mohamed Hussein2
1Department of Intensive Care Unit, Dr. Sumait Hospital, SIMAD University, Mogadishu, Somalia; 2Department of Internal Medicine, Dr. Sumait Hospital, SIMAD University, Mogadishu, Somalia
Correspondence: Abdukadir Mohamed Hassan, Email [email protected]; [email protected]
Abstract: Antimicrobial resistance (AMR) is increasingly shaping intensive care unit (ICU) care, where high antibiotic exposure, invasive devices, and prolonged hospitalization create favorable conditions for resistant pathogens to emerge and spread. Somalia is expanding emergency and critical care capacity, yet many facilities still face gaps in infection prevention and control (IPC), routine microbiology, unit-level antibiograms, and structured antimicrobial stewardship (AMS). This commentary integrates frontline ICU experience in Mogadishu, targeted non-systematic selection of Somali hospital studies, and operational guidance from the World Health Organization (WHO) and the US Centers for Disease Control and Prevention (CDC) to discuss pragmatic priorities for ICU AMR response. The aim is not to estimate national prevalence or demonstrate intervention effectiveness. Available studies from Mogadishu suggest substantial multidrug-resistant organism burdens in adult ICU, pediatric ICU, and hospital-acquired infections, while national IPC assessment findings and local stewardship evidence indicate important systems constraints. We argue that a realistic starting point is a minimum facility-level ICU AMR starter package consisting of six linked actions: defined accountability, audited IPC essentials, useful microbiology outputs including quarterly antibiograms, 48– 72-hour antibiotic review, planned durations with stop dates, and protection of selected last-line agents using the WHO AWaRe framework. This package is presented as a pragmatic checklist for piloting and local adaptation rather than as a validated national framework. Strengthening measurement, IPC, and stewardship in sentinel hospitals may help generate the local data needed for future policy, quality improvement, and implementation research.
Keywords: intensive care unit, antimicrobial resistance, infection prevention and control, antimicrobial stewardship, multidrug-resistant organisms, antibiogram
Introduction
Antimicrobial resistance is a major global threat that makes infections harder to treat and increases risks during routine healthcare, including surgery, neonatal care, and critical illness management.1,2 AMR should also be understood within a broader One Health framework because resistant organisms and antimicrobial use are shaped by interactions across human, animal, and environmental systems, even though the present commentary focuses specifically on hospital ICU care.3
Recent international surveillance has reinforced that resistance is rising across common pathogen-antibiotic combinations and that large, standardized datasets are essential for targeting prevention, stewardship, and investment decisions.4 In ICU settings, this matters because severe illness, frequent device use, broad-spectrum antibiotic exposure, and prolonged admission create a high-risk ecology for the selection and transmission of multidrug-resistant organisms.
Somalia’s emergency and critical care services are expanding, particularly in urban areas, but facility readiness and systems remain variable.5 In addition, Somalia’s heavy reliance on out-of-pocket health expenditure can delay diagnostics and affect timely access to appropriate treatment during acute deterioration.6 Somalia’s National Action Plan on AMR identifies surveillance, IPC, and optimized antimicrobial use as priorities, but ICU-level implementation remains uneven as critical care services grow.7
Commentary Scope and Positioning
This paper is a commentary rather than a systematic review, implementation study, or policy evaluation. It combines three sources of insight: frontline ICU experience in Mogadishu, purposively selected Somali hospital-based literature relevant to ICU AMR, and international operational guidance from WHO and CDC. The purpose is to clarify a practical facility-level starting agenda for hospitals working under major resource constraints.
To improve transparency, the Somali studies discussed here were identified through targeted searches of publicly available literature using combinations of the terms Somalia, Mogadishu, intensive care, ICU, nosocomial infection, antimicrobial resistance, and stewardship. The cited papers were selected because they were the most directly relevant available studies addressing adult ICU resistance, pediatric ICU resistance, hospital-acquired infection burden, ICU-related IPC context, or hospital stewardship practice in Somali settings.8–14 This was a purposive and non-systematic selection process, so the manuscript does not claim to provide a complete national evidence map.
Accordingly, the recommendations below should not be interpreted as proof of intervention effectiveness or as a validated national package. They are presented as pragmatic, hypothesis-generating priorities for hospital-level piloting, local adaptation, and future implementation research.
AMR in Somali ICUs: Separating Frontline Experience From Published Evidence
From frontline ICU experience in Mogadishu, clinicians may encounter patients with suspected infection who do not improve on initial empiric therapy and whose treatment is then escalated during the admission. These observations are experiential and are presented here as clinical context rather than as formal study findings. Their interpretation is nevertheless consistent with settings in which resistant organisms circulate, cultures are not consistently obtained, diagnostic turnaround is delayed, and results are not routinely used for de-escalation.8,14
Published evidence also supports the importance of systems factors in this cycle. Somalia’s AMR context has been described as constrained by limited surveillance and diagnostic capacity, which can push clinicians toward broader empiric regimens and longer durations because the infecting organism and susceptibility pattern are not visible in real time.8 When ICU teams lack routine unit antibiograms and simple feedback loops, escalation can become a common default pathway rather than a carefully justified exception.
IPC systems are a decisive factor in this cycle. A national assessment using the WHO Infection Prevention and Control Assessment Framework reported inadequate IPC levels across Somali healthcare facilities, indicating gaps in infrastructure, training, and monitoring that can enable healthcare-associated transmission in high-risk settings such as ICUs.9 WHO guidance also emphasizes that effective IPC programs reduce healthcare-associated infections and thereby reduce antibiotic exposure and AMR selection pressure.10
What Mogadishu Studies Suggest
Although Somalia does not yet have comprehensive national ICU AMR surveillance, hospital-based evidence from Mogadishu provides signals that ICU resistance burdens may already be substantial. In a tertiary adult ICU study from Mogadishu covering January 2019 to August 2024, more than half of bacterial isolates were classified as multidrug-resistant, with particularly high carbapenem resistance among important Gram-negative pathogens such as Klebsiella spp and Acinetobacter spp.11
Broader hospital-acquired infection data from a tertiary hospital in Mogadishu also showed a meaningful ICU contribution to nosocomial infections and resistance, with bloodstream infections prominently represented and multidrug-resistant organisms common among isolates.12 These patterns are clinically important because sepsis syndromes are time-sensitive and inappropriate early therapy may worsen outcomes.
Pediatric evidence aligns with this concern. A retrospective study from a Mogadishu pediatric ICU reported notable resistance across common pathogens and highlighted the practical need for updated unit antibiograms to guide empiric decisions and reduce unnecessary exposure to broader agents.13
Finally, stewardship capacity affects how resistance is amplified or contained. A study of doctors in a Mogadishu training and research hospital described knowledge and practice gaps, as well as contextual pressures that can drive inappropriate antibiotic use, underscoring the value of hospital structures that support rational prescribing and review.14 Taken together, these publications provide an important but still incomplete picture. They justify caution and action at facility level, but they are not sufficient to quantify the national ICU burden or support broad national generalization.
Closing the ICU Measurement Gap: A Pragmatic Facility-Level Framework
In Somali hospitals, ICU AMR control can be approached as a measurable patient-safety agenda rather than only as a microbiology agenda. A minimum measurement set can make resistance visible enough to influence practice: quarterly ICU antibiograms, basic counts of ICU-acquired bloodstream infection episodes, and tracking of device-days for ventilators, central lines, and urinary catheters to enable simple rates. When measurement improves, empiric guidance becomes more rational, review and de-escalation become more feasible, and IPC priorities become clearer.
The framework proposed in Table 1 is not intended as a validated conceptual model or a national standard. Rather, it is a pragmatic starter checklist adapted from WHO and CDC operational guidance and interpreted in light of the limited Somali evidence summarized above.10,15–17 Its main value is operational: to help hospitals begin measuring, auditing, and refining ICU AMR practice with feasible indicators.
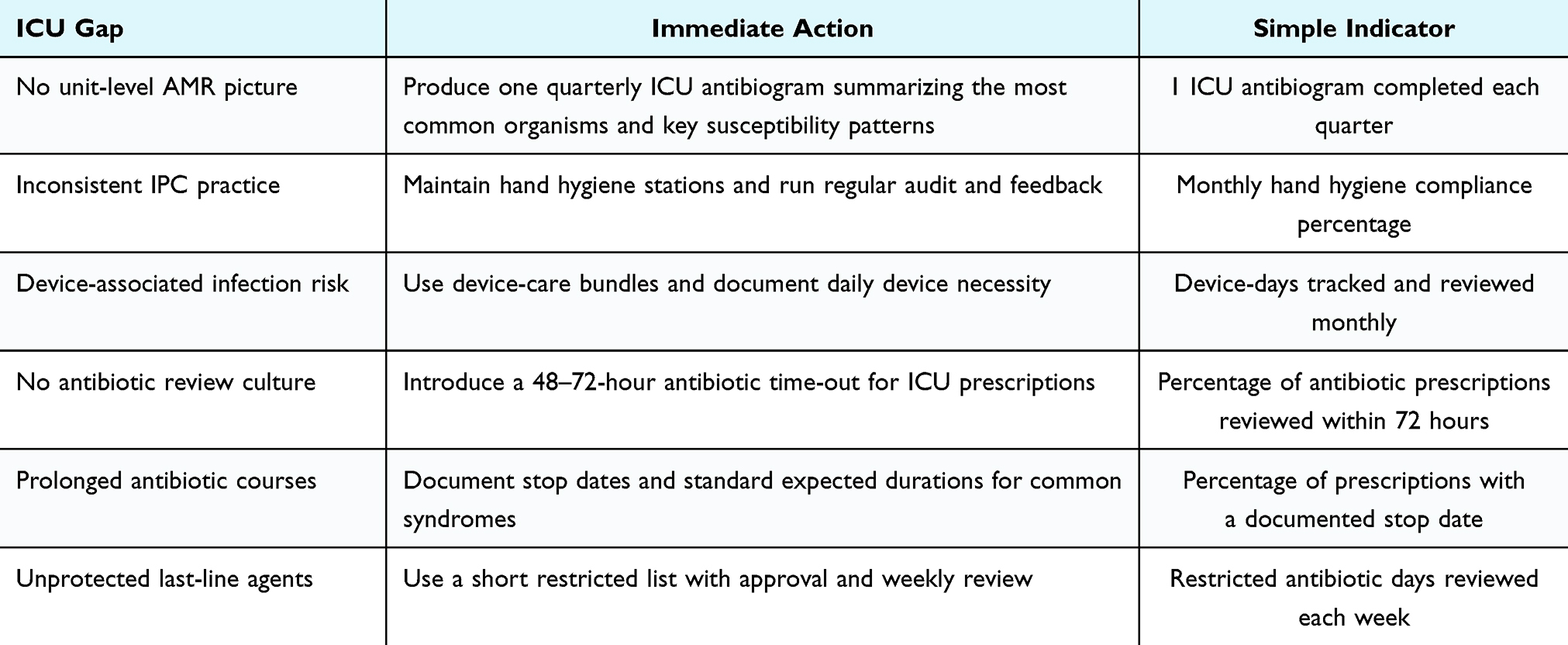 |
Table 1 Minimum Facility-Level ICU AMR Starter Package for Hospitals in Somalia (6-month Pilot Framework) |
A Feasible ICU Response Package for Hospitals in Somalia
- Governance: Assign responsibility and keep it simple. A workable starting point is an ICU AMR core group consisting of an ICU lead clinician, ICU nurse champion, pharmacist, laboratory focal person, and management representative. A short monthly agenda can review antibiogram trends, selected restricted antibiotic use, and IPC audit findings. WHO stewardship guidance emphasizes that accountability and basic measurement are foundational even before advanced capacity is available.15
- IPC essentials: Reduce infections to reduce antibiotic pressure. High-yield ICU IPC priorities include reliable hand hygiene supplies, defined environmental cleaning processes, and consistent device-care bundles with audit and feedback. WHO core components provide a practical structure for implementing and monitoring these essentials.10 In settings where multidrug-resistant organisms are already documented, preventing ICU-acquired infections is one of the fastest ways to reduce antibiotic exposure.
- Make microbiology useful: Quarterly ICU antibiograms and priority cultures. A realistic first diagnostic goal is not complex technology; it is a quarterly ICU antibiogram based on routine cultures and a small set of priority culture pathways, such as blood cultures for suspected sepsis, lower respiratory cultures when ventilator-associated pneumonia is suspected and feasible, and urine cultures when clinically indicated. The adult ICU data from Mogadishu show why local susceptibility patterns matter, particularly where carbapenem resistance is high.11
- Stewardship that fits ICU workflow: Document, review, and de-escalate. WHO’s toolkit for low- and middle-income countries recommends stepwise actions that can fit real-world clinical constraints.15 Three ICU rules are enough to start: document antibiotic indication and planned duration, enforce a 48–72-hour antibiotic review with a stop, narrow, or continue decision, and standardize usual durations for common syndromes while documenting justified exceptions.
- Use AWaRe to protect last-line agents. WHO’s AWaRe framework supports monitoring and improving antibiotic use and proposes a target in which at least 60% of national antibiotic consumption should come from the Access group while unnecessary Watch use is reduced and Reserve agents are protected.16 In hospitals where resistance to key agents is already documented, a short restricted list of selected last-line antibiotics can be linked to approval and weekly review.
- Use accepted stewardship core elements as a checklist. CDC’s Core Elements provide a practical checklist comprising leadership commitment, accountability, pharmacy expertise, action, tracking, reporting, and education.17 These elements can be simplified for Somali hospitals and used to monitor progress over time.
Implications for Practice and Policy
AMR in Somali ICUs should be treated as an immediate patient-safety concern because available Mogadishu studies document multidrug-resistant organisms in adult ICU, pediatric ICU, and hospital-acquired infections.11–13 A practical minimum standard at hospital level is to document antibiotic indication and planned review or stop date, obtain cultures before starting or changing therapy when clinically feasible, and enforce a 48–72-hour antibiotic time-out to stop, narrow, or continue therapy.15,18 Embedding this review into daily multidisciplinary ICU rounds may improve antibiotic use and related outcomes.18
Stewardship alone will have limited impact without stronger IPC. Somalia’s national IPCAF assessment indicates inadequate IPC performance in many facilities, making reliable hand hygiene, environmental cleaning accountability, and device-care bundles with audit and feedback essential ICU readiness measures.9,10 In practical terms, hospitals expanding ICU capacity should also build minimum AMR readiness: an IPC focal team, basic culture pathways, quarterly ICU antibiograms, and a simple stewardship routine.
At policy level, the current evidence base supports phased strengthening of sentinel hospitals rather than immediate national standardization of a single ICU package. As more facility data become available, AMR implementation under the Somali National Action Plan could incorporate ICU-relevant outputs such as hospital antibiograms, hospital-acquired infection indicators, and stewardship process measures.7,16
Limitations of This Commentary
This commentary has several limitations. First, it is not a systematic review and therefore cannot claim comprehensive coverage of all Somali AMR evidence. Second, much of the directly relevant published evidence comes from a limited number of hospitals in Mogadishu, which restricts generalizability to other parts of the country. Third, the practice-based observations included here reflect frontline clinical experience and should not be interpreted as formal outcome data. Finally, the framework proposed in Table 1 has not been tested for effectiveness in Somali ICUs and should be viewed as a practical starting point for piloting, audit, and refinement rather than as a proven intervention package.
Research Agenda
Priority research should focus on what changes care. First, sentinel ICU surveillance should measure device-days, ICU-acquired infections, and routine antibiograms to close the measurement gap.7,11 Second, feasible stewardship interventions such as antibiotic time-outs, audit and feedback, and de-escalation pathways should be evaluated using implementation designs and outcomes such as antibiotic days of therapy, mortality, and length of stay.15,18 Third, AWaRe should be applied to antibiotic use measurement to assess whether stewardship policies shift prescribing toward more appropriate patterns.16 Fourth, IPC implementation studies are needed to identify what works under Somali constraints including supplies, staffing, and crowding.9,10 Finally, economic and equity research should examine how out-of-pocket costs influence access to cultures and appropriate treatment during critical illness.6
Conclusion
Available hospital data from Mogadishu suggest that AMR in ICU care deserves urgent attention, but they do not yet quantify the national burden or prove the effectiveness of any proposed response package. This commentary therefore offers a cautious facility-level starting agenda: make resistance visible, strengthen the most basic IPC processes, and build stewardship into everyday ICU workflow. The immediate value of this approach is not that it guarantees outcomes, but that it creates a measurable foundation from which Somali hospitals can learn, adapt, and generate the stronger local evidence that future policy will require.
Abbreviations
AMR, antimicrobial resistance; AMS, antimicrobial stewardship; AWaRe, Access, Watch, Reserve; CDC, Centers for Disease Control and Prevention; ICU, intensive care unit; IPC, infection prevention and control; MDR, multidrug-resistant; WHO, World Health Organization.
Data Sharing Statement
No new datasets were generated or analyzed in this study.
Ethics Approval and Informed Consent
Ethics approval and informed consent were not required for this commentary because it did not involve primary data collection, human participant recruitment, intervention, or identifiable patient information.
Acknowledgments
The authors acknowledge frontline clinicians and families in Somali hospital settings whose experiences continue to inform efforts to improve context-responsive and patient-centered critical care delivery.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work received institutional support from the Center of Research and Development, SIMAD University, Mogadishu, Somalia. The supporter had no role in literature selection, interpretation, drafting of the manuscript, or the decision to submit the article for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Antimicrobial resistance. Fact sheet; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance.
2. Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–6. doi:10.1016/S0140-6736(21)02724-0
3. World Health Organization. One health. Fact sheet; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/one-health.
4. World Health Organization. Global antibiotic resistance surveillance report 2025; 2025. Available from: https://www.who.int/publications/i/item/9789240116337.
5. Njiru HN, Relan P, Malik SMMR, et al. Emergency and critical care services in Somalia: a cross-sectional nationwide hospital assessment using the WHO Hospital Emergency Unit assessment tool. BMC Emerg Med. 2025;25:89. doi:10.1186/s12873-025-01234-8
6. Mohamud KM, Warei SY, Abubakr AHA, et al. Burden or benefit? Unveiling the impact of out-of-pocket health expenditures in Somalia’s healthcare system. Health Econ Rev. 2025;16:5. doi:10.1186/s13561-025-00703-x
7. World Health Organization. Somalia: national action plan on combating antimicrobial resistance; 2022. Available from: https://www.who.int/publications/m/item/Somalia-national-action-plan-on-combating-antimicrobial-resistance.
8. Hassan SA, Dirie AM, Ahmed NR, Omar AI. Update on antimicrobial resistance in Somalia: current status, challenges, opportunities, and future perspectives. Heliyon. 2024;10:e39434. doi:10.1016/j.heliyon.2024.e39434
9. Adam AA, Mohamed HD, Anyiam FE. Assessment of infection prevention and control in Somali healthcare facilities using the WHO Infection Prevention and Control Assessment Framework. Antimicrob Resist Infect Control. 2025;14:103. doi:10.1186/s13756-025-01584-9
10. World Health Organization. Guidelines on core components of infection prevention and control programmes at the national and acute health care facility level; 2016. Available from: https://www.who.int/publications/i/item/9789241549929.
11. Çelik AK, Türkan M, Ali TA, et al. Prevalence and antimicrobial susceptibility of multi drug-resistant bacteria isolates in adult intensive care units: a six-year retrospective study from a tertiary hospital in Mogadishu, Somalia. BMC Infect Dis. 2026;26:137. doi:10.1186/s12879-025-12315-1
12. Sheikh Omar NMS, Erismis B, Muse Osman M, et al. Retrospective evaluation of nosocomial bacterial infections and their antimicrobial resistance patterns among hospitalized patients in Mogadishu, Somalia. Infect Drug Resist. 2023;16:705–720. doi:10.2147/IDR.S398387
13. Orhan Z, Mohamud SM, Doğan S, et al. Microorganisms and antibiotic resistance in pediatric ICU patients: a retrospective study, Mogadishu, Somalia. Southeast Asian J Trop Med Public Health. 2025;56(4):464–488.
14. Kıratlı K, Aysin M, Ali MA, et al. Evaluation of doctors’ knowledge, attitudes, behaviors, awareness and practices on rational antimicrobial stewardship in a training and research hospital in Mogadishu-Somalia. Infect Drug Resist. 2024;17:2759–2771. doi:10.2147/IDR.S463197
15. World Health Organization. Antimicrobial stewardship programmes in health-care facilities in low- and middle-income countries: a WHO practical toolkit; 2019. Available from: https://www.who.int/publications/i/item/9789241515481.
16. World Health Organization. AWaRe classification of antibiotics for evaluation and monitoring of use (2023); 2023. Available from: https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2023.04.
17. Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs; 2019. Available from: https://www.cdc.gov/antibiotic-use/core-elements/hospital.html.
18. Mishima Y, Nawa N, Asada M, et al. Impact of antibiotic time-outs in multidisciplinary ICU rounds for antimicrobial stewardship program on patient survival: a controlled before-and-after study. Crit Care Explor. 2023;5:e0837. doi:10.1097/CCE.0000000000000837
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinicians’ Intention to Submit Microbiological Pathogenic Test Before Antibiotics Use and Its Influencing Factors: New Evidence from the Perspective of Hospital Management
Wang Q, Zhang X, Zheng F, Wang L, Yu T
Infection and Drug Resistance 2022, 15:3013-3023
Published Date: 11 June 2022
Investigating Knowledge of Antibiotics, Antimicrobial Resistance and Antimicrobial Stewardship Concepts Among Final Year Undergraduate Pharmacy Students in Northern Nigeria
Abdu-Aguye SN, Barde KG, Yusuf H, Lawal BK, Shehu A, Mohammed E
Integrated Pharmacy Research and Practice 2022, 11:187-195
Published Date: 23 December 2022
Bacterial Epidemiology and Antimicrobial Resistance Profiles of Respiratory Specimens of Children with Pneumonia in Hainan, China
Mai W, Liu Y, Meng Q, Xu J, Wu J
Infection and Drug Resistance 2023, 16:249-261
Published Date: 12 January 2023
Reflections on Drivers for the Emergence and Spread of Antimicrobial Resistant Bacteria Detected from Chickens reared on Commercial Layer Farms in Mukono District, Uganda
Kakooza S, Tayebwa DS, Njalira KR, Kayaga EB, Asiimwe I, Komugisha M, Wanyana M, Kisekka R, Kyabarongo A, Kiryabwire DH, Nabatta E, Eneku W
Veterinary Medicine: Research and Reports 2023, 14:209-219
Published Date: 6 December 2023
Healthcare Professionals’ Knowledge and Attitudes Toward Antimicrobial Stewardship Programs in Aseer, Saudi Arabia: A Cross-Sectional Study
Bahamdan AK, Alavudeen SS, Bahamdan GK, Bahamdan KA, Asiri SMA, Alshahrani NAM, Abdulziz Alqahtani S, Ibrahim ARN
Risk Management and Healthcare Policy 2025, 18:855-867
Published Date: 12 March 2025