Back to Journals » Infection and Drug Resistance » Volume 15
Clinicians’ Intention to Submit Microbiological Pathogenic Test Before Antibiotics Use and Its Influencing Factors: New Evidence from the Perspective of Hospital Management
Authors Wang Q, Zhang X ![]() , Zheng F, Wang L, Yu T
, Zheng F, Wang L, Yu T
Received 27 March 2022
Accepted for publication 27 May 2022
Published 11 June 2022 Volume 2022:15 Pages 3013—3023
DOI https://doi.org/10.2147/IDR.S366892
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Qianning Wang, Xinping Zhang, Feiyang Zheng, Lu Wang, Tiantian Yu
School of Medicine and Health Management, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China
Correspondence: Xinping Zhang, School of Medicine and Health Management, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China, Tel +133 4995 0095, Email [email protected]
Purpose: Antimicrobial resistance (AR) is a global public health problem, improving clinicians’ intention to submit microbiological pathogenic test (submission intention) can effectively increase the value for rational use antibiotics to curb AR. However, there are few studies on the factors influencing improvement of the submission intention, especially from the perspective of hospital management. This study will fill the gap and provide evidence that can continuously support improvement of antibiotics prescribing rationally.
Patients and Methods: A cross-sectional survey of clinicians was conducted in all public hospitals in Hubei, China. Dependent variables were submission intention of non-restricted-use, restricted-use and special-use antibiotics which were measured submission, not sure submission, no submission. Independent variables were frequency of training and publicity on submission, and hospital with or without submission performance assessment, guideline, information decision system and laboratory items, including bacterial culture item, fungal culture item and so on. Clinicians’ demographics were applied as control variables. Multinomial logistic regression was performed to model independent variables influencing submission intention.
Results: For non-restricted-use antibiotics, guideline (OR = 0.263; 95% CI = [0.188, 0.369]) (OR = 0.526; 95% CI = [0.375, 0.738]) and bacterial culture item (OR = 0.141; 95% CI = [0.074, 0.268]) (OR = 0.520; 95% CI = [0.292, 0.927]) are key factors that positively affect clinicians’ intention on submission and not sure submission; For restricted-use and special-use antibiotics, training frequency and bacterial culture item (OR = 0.155; 95% CI = [0.076, 0.315]) (OR = 0.092; 95% CI = [0.036, 0.232]) (OR = 0.106; 95% CI = [0.046, 0.248]) (OR = 0.027; 95% CI = [0.006, 0.117]) are key factors that positively affect clinicians’ intention on submission and not sure submission.
Conclusion: This study found that bacterial culture item, guideline, and training frequency are key factors that affect clinicians’ intention on submission and not sure submission, but various factors exist different effects level on different types of antibiotics. Consequently, a focus should be placed on the construction and implementation of management factors, as well as reformation of antimicrobial stewardship in hospitals according to the types of antibiotics.
Keywords: pathogenic microbial specimen, submission intention, hospital management, antimicrobial stewardship, effects assessment
Introduction
Antimicrobial resistance (AR), is a major public health issue and has attracted significant attention from various countries.1 It was estimated that about 25,000 and 23,000 people died as a direct result of AR each year in Europe and the United States, respectively.2 The Organization for Economic Cooperation and Development (OECD) reported that AR would contribute to more than 2 million deaths in Europe, North America and Australia by 2050 if effective and immediate actions were not taken.3 Irrational use of antibiotics is the main reason for AR.4 A recent study showed that 60.98% of COVID-19 patients received empirical antibiotics therapy, ratio was higher in ICU and suggested to increase the submission level of microbiological pathogenic test before the use of antibiotics,5–8 in order to reduce the excessive and unreasonable use of them.
Consistent intensification of antimicrobial stewardship has increased attention on microbiological pathogenic test around the world.9 Many countries have issued a series of test guidelines. For example, the Centers for Disease Control (CDC) in the US and Nigeria stressed that clinicians should prescribe antibiotics based on test reports and improve the level of the submission for the test.10,11 And the level requirements in Guiding Principles of Clinical Application of antibiotics were clearly defined as the rates of submission for test of pre-use of antibiotics in hospitalized patients not less than 30% for non-restricted-use antibiotics, not less than 50% for restricted-use antibiotics, and not less than 80% for special-use antibiotics in China in 2015.12 One of the National Medical Quality and Safety Improvement goals in 2021 was also improving the submission level of the test.13
Many studies have concluded that performance assessment, guideline, information decision system, education, training, and communication influence the test submission in hospitals. Liu found that performance assessment, information program, training, feedback and communication could increase the rate of pre-use microbiological specimen test of restricted-use and special-use antibiotics from 42.21%, 45.18%, and 74.71% to 53.54%, 55.68%, and 89.70%, respectively.14 One review found that audit and feedback, education, information processing, and guideline could prompt clinicians to make reasonable prescriptions based on the results of pathogenic test, resulting in shorter treatment times (1.95 days) for inpatients with resistant bacteria.15 Theory of Reasoned Action and KAP model indicated that an individual’s actual action is determined by behavioral intention,16,17 based on the fact that clinicians are the main body of professionals prescribing antibiotics in China, we claimed that factors such as performance assessment are indirect causes of test levels, while clinicians’ intention to submit microbiological pathogenic test (submission intention) is the primary cause. Wan intervened the submission intention by Quality Control Circle (QCC) management method, and found that the submission rate of microbiological pathogenic test before therapeutic use of antibiotics increased from 13.33% to 27.02% in surgical inpatients.18 Helou RI believed development of an application (APP) to guide antibiotics could increase clinicians’ awareness of antimicrobial stewardship, thereby improving the level of test.19
Findings showed that the implementation state of pathogen test submission was still severe according to reviews and practical evidence above.20 Although relevant guidelines have been issued, some studies have revealed that performance assessment, guideline, information decision system, education and training are important management factors, and submission intention has a direct influence on the level of test. Unfortunately, few studies have investigated the submission intention systematically to explore the influencing factors from the perspective of hospital management, especially the influence degree of each factor.21 Research on factors influencing submission intention and their degree can help identify key factors that increase clinicians’ intention to submit for test, leading to the appropriate allocation of resources for rational use of antibiotics and combating bacterial resistance, so the management factors affecting the clinicians’ intention to submit for test are worthy issues to research.22
Materials and Methods
Study Design and Participants
A cross-sectional survey was conducted in all public hospitals in Hubei, China. The survey was implemented in June 2021, 188 (17.94%) hospitals responded, each clinical department in hospitals was required at least 5 clinicians to fill questionnaire, and a total of 4366 questionnaires were received with an effective response rate of 80.21%. The questionnaire covered clinicians’ submission intention, hospital management and demographic factors.
As part of the design in the questionnaire, items were compiled according to the 2015 edition of the Guiding Principles of Clinical Application of antibiotics, and experts were consulted to ensure its reliability and validity.
To prevent missing items and logical errors in the questionnaire, directors from each department checked the questionnaire prior to returning it.
Further details of research design and data collection are available in the Hubei Provincial Hospital Infection Center (whcdc.org).
The Variables and Their Description
In order to improve the submission-level accordance with the requirements of national policies, submission intention was selected as the dependent variable. They were submission intention of non-restricted-use, restricted-use, and special-use antibiotics which were measured submission, not sure submission, no submission. Submission, not sure submission, no submission refer to clinician tend to submit, not sure submit and no submit microbiological pathogenic test before antibiotics use. Table 2 shows that the submission intention level is different among various types of antibiotics, but the distribution is similar.
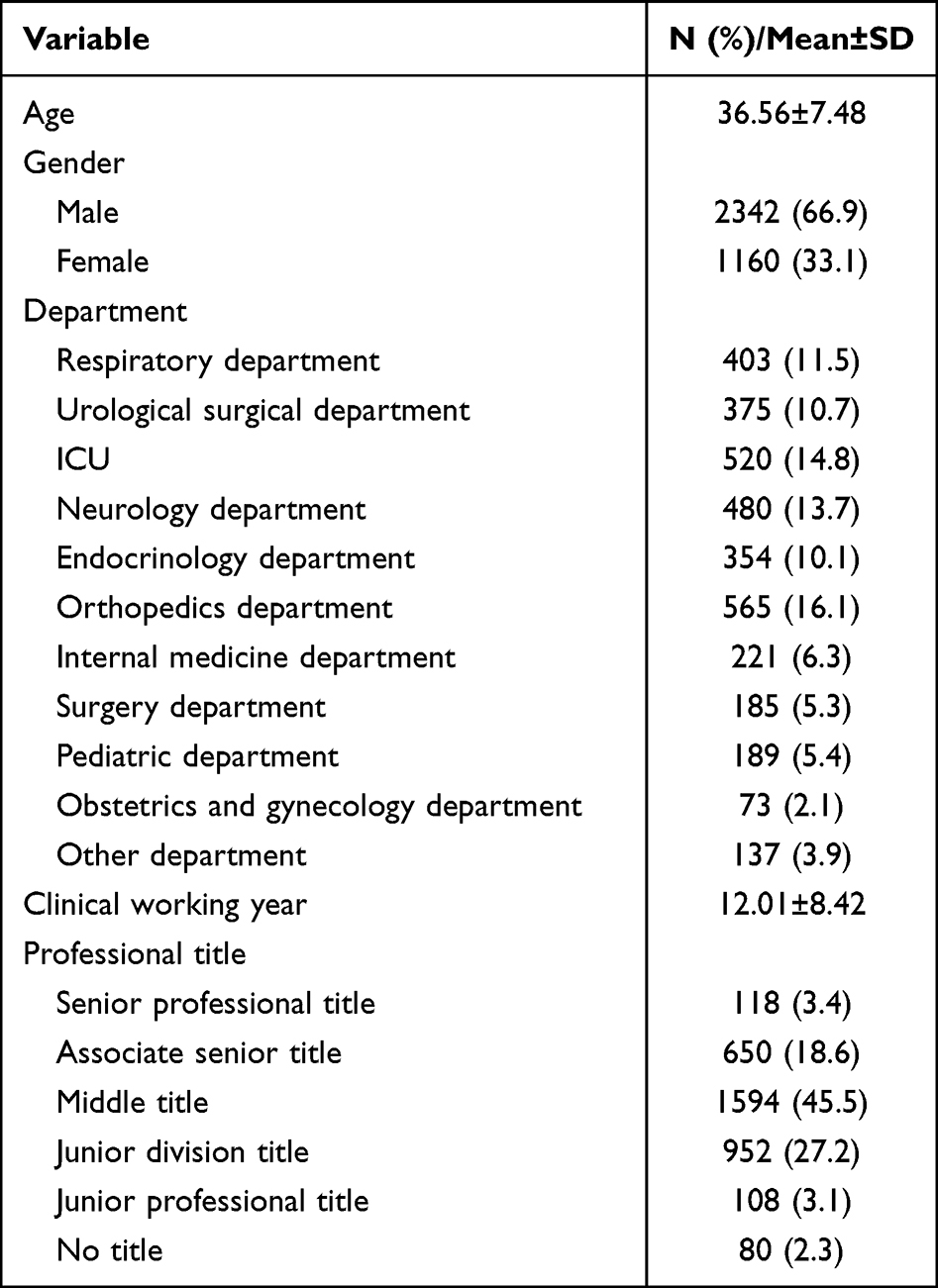 |
Table 1 Variables Distribution of Demographic Factors |
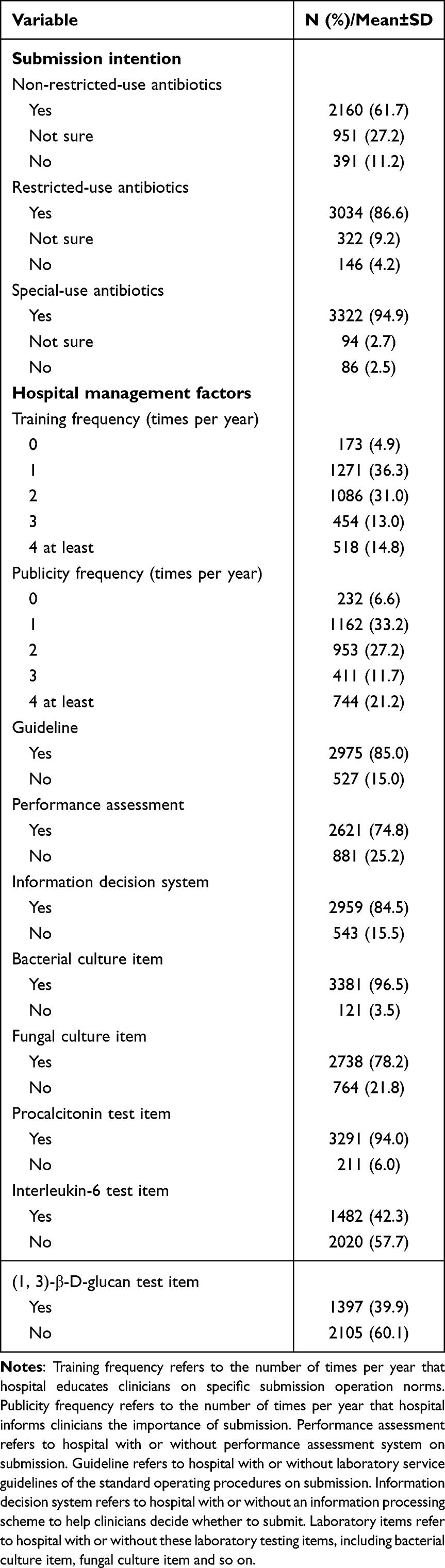 |
Table 2 Variables Distribution of Submission Intention and Hospital Management Factors |
According to the literature and policy requirements, training, publicity and other hospital management factors were selected as independent variables. They were measured as frequency of training and publicity on submission, and hospital with or without submission performance assessment, guideline, information decision system and laboratory items, including bacterial culture item, fungal culture item, procalcitonin test item, interleukin-6 test item and (1,3)-β-D-glucan test item. Training frequency refers to the number of times per year that hospital educates clinicians on specific submission operation norms. Publicity frequency refers to the number of times per year that hospital informs clinicians the importance of submission. Performance assessment refers to hospital with or without performance assessment system on submission. Guideline refers to hospital with or without laboratory service guidelines of the standard operating procedures on submission. Information decision system refers to hospital with or without an information processing scheme to help clinicians decide whether to submit. Laboratory items refer to hospital with or without these laboratory testing items, including bacterial culture item, fungal culture item and so on. As shown in Table 2, the distribution of variables in hospital management factors is discrepant at different levels.
Clinicians’ gender, age, clinical working year, department, title were applied as control variables. As shown in Table 1, clinicians’ average age is 36.56, average clinical working year is 12.01. The proportion of male (66.9%, n = 2342) middle title (45.5%, n = 1594) orthopedics department (16.1%, n = 565) clinicians is higher.
Statistics Analysis
Multinomial logistic regression is appropriately applied in this study because dependent variables are disorderly classification variables. The greatest advantage of using the regression is that separate logistic regression models are estimated for each indicator variable simultaneously, so mutually exclusive response categories can be analyzed with no need to overlap reference categories.23,24
In this study, IBM SPSS Statistics 24 was used to complete all the data analysis and processing. The model takes the form of equation (1), and J = 1 (yes), 2 (not sure), 3 (no), which indicate three disordered multinomial dependent variables “submission”, “not sure submission” and “no submission”, “J = 3” is the reference. “k” is the number of dependent variables, 1 ≤ k ≤ 15, Xi is the explanatory variable, i = 1, 2, …,15. The logistic regression model that affects the odds of clinicians’ submission choice is shown in equation (2), not sure submission choice is shown in equation (3). There were different types of antibiotics, thus this study ran this model for three times.


Results
Multinomial logistic regression is presented in Table 3. Each of the following columns lists the odds of submission intention before use: non-restricted-use, restricted-use and special-use antibiotics submission and not sure submission compared to the basic category of no submission. Statistically significant results (p<0.05) are in boldface.
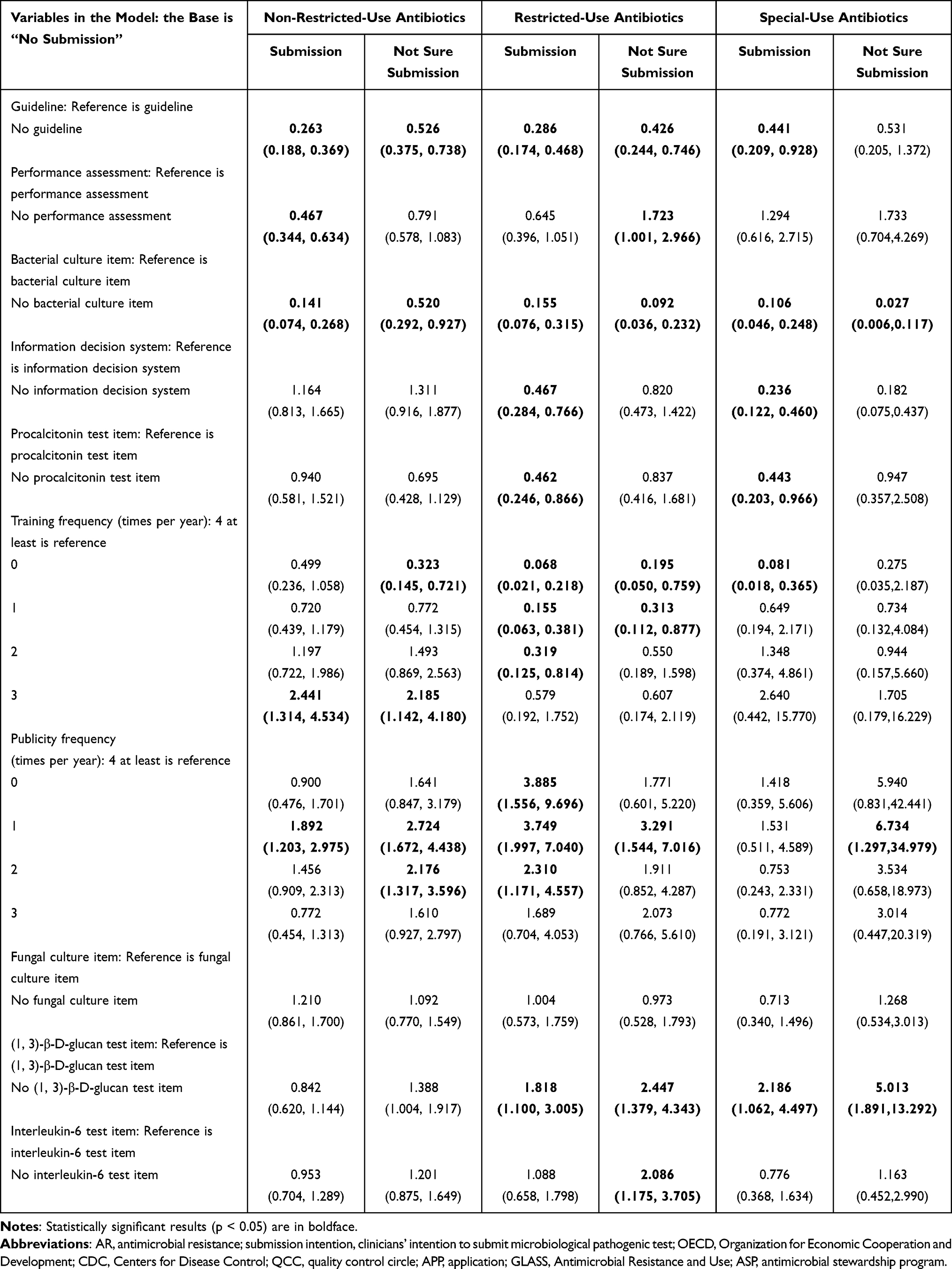 |
Table 3 Results of Multinomial Logistic Regression on Submission Intention |
Non-Restricted-Use Antibiotics
Submission Analysis
The odds of clinicians in hospital without guideline are 73.7% lower to submit test than in hospital with guideline. Similarly, clinicians in hospital without performance assessment have 53.3% lower odds to submit test. Clinicians in hospital without bacterial culture item have near 86% lower odds to submit test. However, the odds of clinicians who trained 3 times/year in hospital are 2.441 times higher to submit test than 4 or more times/year, and clinicians who received publicity 1 time/year in hospital are 1.892 times higher to submit test than 4 or more times/year.
Not Sure Submission Analysis
The odds of clinicians in hospital without guideline are 47.4% lower not sure to submit test than in hospital with guideline. There are 48% lower odds in not sure submitting test in hospital without bacterial culture item than in hospital with the item. The odds of clinicians not sure to submit for test in hospital with training frequency of 0 times/year are 67.7% lower than that with training frequency of 4 or more times/year, while clinicians’ training frequency of 3 times/year not sure to submit for test are 2.185 times higher than training frequency of 4 or more times/year. The odds of clinicians in hospital with publicity frequency of 1 time/year and 2 times/year not sure to submit for test are 2.724 and 2.176 times, respectively, higher than 4 or more times/year.
Restricted-Use Antibiotics
Submission Analysis
In hospital without guideline, clinicians have 71.4% lower submission odds than that with guideline. Clinicians in hospital without bacteria culture item have 84.5% lower odds of submitting test than that with the item. In hospital without information decision system, clinicians get 53.3% lower submission odds than that with the system. The odds of clinicians’ submission intention in hospital without procalcitonin test item are 53.8% lower than in hospital with the item. In hospital with training frequency of 0 times/year, 1 time/year, and 2 times/year, the odds of clinicians’ submission intention are 93.2%, 84.5%, and 68.1% lower than that of 4 or more training per year. However, the odds of clinicians’ submission intention in hospital with publicity frequency of 0 times/year, 1 time/year, and 2 times/year are 3.885, 3.749, and 2.310 times higher than that of 4 or more times/year, respectively. The odds of clinicians are 1.818 times higher to submit test in hospital with (1, 3)-β-D-glucan test item than in hospital without the item.
Not Sure Submission Analysis
The odds of clinicians in hospital without guideline not sure submitting for test are 57.4% lower than that with guideline. The odds of clinicians in hospital without performance assessment are 1.723 times higher not sure to submit test than clinicians in hospital with the assessment. Clinicians in hospital without bacterial culture item have 90.8% lower odds not sure to submit test than in hospital with the item. The not sure submission odds of clinicians in hospital with 0 times/year and 1 time/year training frequency are 80.5% and 68.7% lower than 4 times/year, respectively. The not sure submission odds of clinicians in hospital with 1 time/year publicity frequency are 3.291 times higher than 4 or more times/year. The odds of clinicians in hospital without (1, 3)-β-D-glucan test item are 2.447 times higher not sure to submit test than that in hospital with the item, and clinicians in hospital without interleukin-6 test item are 2.086 times higher not sure to submit test than that in hospital with the item.
Special-Use Antibiotics
Submission Analysis
The clinicians’ submission odds are 55.9% lower in hospital without guideline than in hospital with guideline. Clinicians in hospital without bacterial culture item have 89.4% lower odds of submitting intention than hospital with the item. The clinicians’ submission odds in hospital without information decision system are 76.4% lower than that with the system. The odds of clinicians’ submission intention in hospital without procalcitonin test item are 55.7% lower than in hospital with the item. The odds of clinicians’ submission intention in hospital with training frequency of 0 times/year are 91.9% lower than in hospital with training frequency of 4 or more times/year. The odds of clinicians are 2.186 times higher to submit test in hospital with (1, 3)-β-D-glucan test item than in hospital without the item.
Not Sure Submission Analysis
The odds of clinicians in hospital without bacterial culture item not sure submitting test are 97.3% lower than hospital with the item. In hospital without information decision system, the odds that clinicians not sure submitting for test are 81.8% lower than in hospital with the system. The odds of clinicians in hospital with 1 time/year publicity frequency not sure submitting for test are 6.734 times higher than frequency of 4 or more times/year. The odds of clinicians in hospital without (1, 3)-β-D-glucan test item are 5.013 times higher not sure to submit test than in hospital with the item.
Discussion
Main Findings
For non-restricted-use antibiotics, the key to improve the submission intention lies in guideline, whereas restricted-use and special-use antibiotics lie in training frequency. Bacterial culture item has a significant impact on the improvement of submission intention of all types of antibiotics. As shown in Table 3, the degree of influence is different, but guideline, training frequency and bacterial culture item are related to various types of antibiotics submission intention. Meanwhile, information decision system is related to restricted-use and special-use antibiotics submission intention. The results are consistent with one-way ANOVA and the findings in similar fields of antimicrobial prescribing by clinicians.25 The possible reason for the results is the use of non-restricted-use antibiotics is mostly for mild patients, the guideline of standard operating procedures on submission can generally help clinicians meet the standard level of national policies. However, restricted-use and special-use antibiotics are mostly used by patients with severe diseases and long hospital stay, empirically therapy usually be carried out by clinicians,26 thus training and establishment of convenient information system are needed in hospital to further avoid empirically therapy and improve the submission intention. The discussion stresses on the following points.
The Effect Degree of Guideline Influencing Submission Intention of Various Antibiotics
Guideline has a significant impact on submission intention. A survey of 340 physicians and microbiologists in 58 middle- and low-income countries confirmed that guideline was the most effective antimicrobial stewardship intervention method and was effective in changing clinicians’ antibiotics prescription behavior.27 Hansen MJ found that decision support tools which provided clinician guideline recommendations had a lower antibiotic prescription rate of 98.7 prescriptions per 1000 patient years while the usual care group was 107.6 during the 12-month intervention period.28 But for different antibiotics, guideline has different effects. After standardizing hospital guideline, the submission rate of restricted-use antibiotics soared from 36.97% to 59.23%, special-use antibiotics soared from 73.5% to 93.37%, an increase of 22.26% and 19.87%, respectively.29 The results showed that guideline had a better effect on improving the submission intention of restricted-use antibiotics compared to special-use antibiotics, but it is pity that there are no empirical research results on non-restricted-use antibiotics. Our study reveals that guideline shows the best effect on non-restricted-use antibiotics submission intention, than restricted-use and special-use antibiotics.
The Effect Degree of Training Frequency Influencing Submission Intention of Various Antibiotics
Training frequency has a significant impact on submission intention. Training is considered to be one of the most effective antibiotics stewardship interventions.27 Many countries’ hospital and organization have facilitated antibiotics education and training, such as implementing early on-the-job training for primary surgeons in Egypt, offering education and training in villages through Columbia International Medical Research and Training Center.30 In a rural Kenyan hospital, a checklist of high-quality antibiotics prescription practices resulted in a 40% reduction in average monthly antibiotics costs and a significant improvement in physician prescriptions.31 But for different antibiotics, training has diverse effects. A study revealed that after adapting education and training measures, the submission rate of restricted-use antibiotics was 7.1% higher than that of non-restricted-use antibiotics, showing that restricted-use antibiotics were more sensitive to training.32 Our study findings are consistent with this conclusion.
The Effect Degree of Bacterial Culture Item Influencing Submission Intention of Various Antibiotics
Bacterial culture item has a significant impact on submission intention. Bacterial culture item is the most accurate standard to diagnose infectious disease.33 The key role of bacterial culture item in guiding clinicians in antimicrobial prescribing has been reported in a number of literature from around the world.34,35 However, some hospitals did not carry out bacterial culture item due to long culture time, local poor development and so on.36 One study also demonstrated that availability of accessibility personnel, test technology and other resources affected the effectiveness of antimicrobial stewardship.37 Studies have suggested that basic diagnostic test is the primary strategy to ensure effective implementation of antimicrobial stewardship in middle- and low-income countries.27 Our study results with hard evidence show the impact of implementing bacterial culture item on the submission intention of various antibiotics.
The Effect Degree of Information Decision System Influencing Submission Intention of Various Antibiotics
Information decision system has a significant impact on submission intention. Firstly, Burke believed that antibiotics misuse was more attributed to inadequate information.38 Secondly, the WHO policy on Global Surveillance System for Antimicrobial Resistance and Use (GLASS) was launched to support antimicrobial resistance management in 2015.39 In practice, an antimicrobial stewardship program (ASP) enabled APP was downloaded more than 3000 times and accessed more than 9000 times in 14 months, most downloaded by hospital clinicians (88%), and it most likely affected the doctor’s prescription.40 Other valuable opinions were that one goal of using informatics to support clinical decisions was to prevent unnecessary antibiotics use,41 and clinical computer system can help implement the goal, specifically as an expert system that can provide patient-specific data and advice in the ward area.42 In addition, management programs such as computer technology and information system should be strengthened to monitor and track progress and develop innovative strategies.43 It is worthwhile to note that for different antibiotics, the influence degree of information decision system is different. After implementing the information processing scheme, prescription rate of restricted-use antibiotics decreased from 63.65% to 41.76%, special-use antibiotics decreased from 36.98% to 7.92%, 21.89% and 29.06% dropped in them, respectively, showed that submission intention of special-use antibiotics was more sensitive to information decision system.44 Our study reveals the same conclusion.
Our research also has some limitations. This study only explores submission intention from the perspective of hospital management because of poor access to the data. In the future, submission behavior and more other factors such as patient’s condition, etc., will be measured and used as a reference to reveal the submission intention and behavior, even include more hospital management factors in order to understand the submission behavior deeply and systemically.
Conclusion
In this study, multinomial logistic regression was used to model the influencing factors of submission intention before antibiotics use. The main study findings show that bacterial culture item, guideline, and training frequency are the key factors that affect submission intention, but various factors exist different effects level on different types of antibiotics. For non-restricted-use antibiotics, the key to improve submission intention lies in the guideline, for restricted-use and special-use antibiotics lies in training frequency. Bacterial culture item has a significant impact on the improvement of submission intention of all types of antibiotics. It is suggested that thoughtful attention must be given to the construction and implementation of management factors, as well as the reformation of antimicrobial stewardship in hospitals according to the types of antibiotics.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
The study was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology (2021-S063). As the study used anonymous, pooled, and retrospective data, the Ethics Committee waived the need for participants to provide written informed consent. The study complies with the Declaration of Helsinki.
Acknowledgments
The authors would like to thank the National Natural Science Foundation of China for providing research funding and Wuhan centre for disease control & prevention for providing the research data. The authors would also like to acknowledge the following individuals who helped collect data or polished language: Zhou Qian, Wang Ying, Wei Ming, Xie Lewei, Duan Zhonghong, Wang Yongyi, Lu Junyu, Janelle Julien.
Funding
This work was supported by the National Natural Science Foundation of China (72074085, http://www.nsfc.gov.cn/). The funders played no role in the process of manuscript preparation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goossens H, Ferech M, Vander SR, Elseviers M; ESAC Project Group. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet. 2005;365(9459):579–587. doi:10.1016/S0140-6736(05)
2. Sabtu N, Enoch DA, Brown NM. Antibiotic resistance: what, why, where, when and how? Br Med Bull. 2015;116:105–113. doi:10.1093/bmb/ldv041
3. OECD [Website on the Internet]. Antimicrobial resistance policy insights. Paris; 2016. Available from: https://www.oecd.org/health/health-systems/AMR-Policy-Insights-November2016.pdf.
4. WHO [Website on the Internet]. Antimicrobial resistance. Geneva; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance.
5. Karami Z, Knoop BT, Dofferhoff ASM, et al. Few bacterial co-infections but frequent empiric antibiotic use in the early phase of hospitalized patients with COVID-19: results from a multicentre retrospective cohort study in The Netherlands. Infect Dis. 2021;53(2):102–110. doi:10.1080/23744235.2020.1839672
6. Langford BJ, So M, Raybardhan S, et al. Bacterial co-infection and secondary infection in patients with COVID-19: a living rapid review and meta-analysis. Clin Microbiol Infect. 2020;26(12):1622–1629. doi:10.1016/j.cmi.2020.07.016
7. Wang L, Amin AK, Khanna P, et al. An observational cohort study of bacterial co-infection and implications for empirical antibiotic therapy in patients presenting with COVID-19 to hospitals in North West London. J Antimicrob Chemother. 2021;76(3):796–803. doi:10.1093/jac/dkaa475
8. Lansbury L, Lim B, Baskaran V, Lim WS. Co-infections in people with COVID-19: a systematic review and meta-analysis. J Infect. 2020;81(2):266–275. doi:10.1016/j.jinf.2020.05.046
9. Song M, Nie L, Wu X. The influence of comprehensive intervention on submission rate of clinical pathogenic microorganism specimens. Mod Prev Med. 2015;42(16):3066–3068.
10. Sanchez GV, Fleming-Dutra KE, Roberts RM, Hicks LA. Core elements of outpatient antibiotic stewardship. MMWR Recomm Rep. 2016;65(6):1–12. doi:10.15585/mmwr.rr6506a1
11. NCDC [Website on the Internet]. National treatment guidelines for antimicrobial use in infectious diseases. New Delhi; 2016. Available from: https://ncdc.gov.in/WriteReadData/l892s/File622.pdf.
12. People’s medical publishing house [Website on the Internet]. Guiding principles of clinical application of antibiotics. Beijing; 2015. Available from: http://www.gov.cn/xinwen/2015-08/27/content_2920799.htm.
13. The People’s Republic of China [Website on the Internet]. Notice of the general office of the national health commission on the issuance of the national target for improving medical quality and safety in 2021. Beijing; 2021. Available from: http://www.gov.cn/zhengce/zhengceku/2021-02/22/content_5588240.htm.
14. Liu S, Li JS, Shi JX, et al. Clinical effect of comprehensive intervention on submission rates of microbiological specimens. Chin J Infect Control. 2018;17(2):5.
15. Davey P, Marwick CA, Scott CL, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev. 2017;2(2):CD003543. doi:10.1002/14651858.CD003543.pub3
16. Park HS. Relationships among attitudes and subjective norms: testing the theory of reasoned action across cultures. Commun Stud. 2000;51(2):162–175. doi:10.1080/10510970009388516
17. Wang H, Feng Z, Xu S. Impacts of characteristic personal behaviors on physicians’ drug prescription behaviors based on KABP model. Chin J Hospital Admin. 2012;2012:544–547.
18. Wan Y, Cao J, Liu Y, Gao K, Liu Y, Chen J. Application of quality control circle to improve pathogen detection rate before therapeutic use of antibacterial drugs in surgical inpatients. Chin J Nosocomiology. 2017;27(4):4.
19. Helou RI, Foudraine DE, Catho G, Peyravi Latif A, Verkaik NJ, Verbon A. Use of stewardship smartphone applications by physicians and prescribing of antimicrobials in hospitals: a systematic review. PLoS One. 2020;15(9):e0239751. doi:10.1371/journal.pone.0239751
20. Zhao L, Gao T. Application of PDCA method in the management of antimicrobial use intensity in our department. Chin Pharm. 2014;5:410–412.
21. Bertollo LG, Lutkemeyer DS, Levin AS. Are antimicrobial stewardship programs effective strategies for preventing antibiotic resistance? A systematic review. Am J Infect Control. 2018;46(7):824–836. doi:10.1016/j.ajic.2018.01.002
22. Murray PR. The clinician and the microbiology laboratory. Arch Pathol Lab Med. 2015;191. doi:10.1016/B978-1-4557-4801-3.00016-3
23. Agresti A. An Introduction to Categorical Data Analysis. New York: John Wiley; 2019.
24. Anderson CJ, Rutkowski L. Multinomial Logistic Regression. CA: Sage Publications; 2008.
25. Katsios CM, Burry L, Nelson S, et al. An antimicrobial stewardship program improves antimicrobial treatment by culture site and the quality of antimicrobial prescribing in critically ill patients. Crit Care. 2012;16(6):R216. doi:10.1186/cc11854
26. Samarkos M, Skouloudi M, Anastasopoulou A, Markogiannakis A. Restricted antimicrobial prescribing in an area of highly prevalent antimicrobial resistance. Infect Dis Now. 2021;51(6):526–531. doi:10.1016/j.idnow.2021.05.002
27. Cox JA, Vlieghe E, Mendelson M, et al. Antibiotic stewardship in low- and middle-income countries: the same but different? Clin Microbiol Infect. 2017;23(11):812–818. doi:10.1016/j.cmi.2017.07.010
28. Hansen MJ, Carson PJ, Leedahl DD, Leedahl ND. Failure of a best practice alert to reduce antibiotic prescribing rates for acute sinusitis across an integrated health system in the midwest. J Manag Care Spec Pharm. 2018;24(2):154–159. doi:10.18553/jmcp.2018.24.2.154
29. Qiao J, Qin Y, Chen F, Yao H, Zeng T. Application of target management in improving the inspection rate of pathogenic microbial specimens. Pract J Med Pharm. 2021;4:1243–1247.
30. Goff DA, Kullar R, Goldstein EJC, et al. A global call from five countries to collaborate in antibiotic stewardship: united we succeed, divided we might fail. Lancet Infect Dis. 2017;17(2):e56–e63. doi:10.1016/S1473-3099(16)30386-3
31. Amdany HK, McMillan M. Metronidazole intravenous formulation use in in-patients in Kapkatet District Hospital, Kenya: a best practice implementation project. JBI Evid Synth. 2014;12(3):419–432. doi:10.11124/jbisrir-2014-1381
32. Li Y, Zhao J. Conduct an investigation and analysis of the application of antimicrobial drugs in hospitalized patients before and after antimicrobial management. Today Nurse. 2016;29:1805–1810.
33. Grąźlewska W, Ferra B, Rudzińska M, Holec-Gąsior L. Borrelia burgdorferi BmpA-BBK32 and BmpA-BBA64: new recombinant chimeric proteins with potential diagnostic value. Pathogens. 2021;10(6):767. doi:10.3390/pathogens10060767
34. Rawson TM, Wilson RC, Holmes A. Understanding the role of bacterial and fungal infection in COVID-19. Clin Microbiol Infect. 2021;27(1):9–11. doi:10.1016/j.cmi.2020.09.025
35. Samore MH, Bateman K, Alder SC, et al. Clinical decision support and appropriateness of antimicrobial prescribing: a randomized trial. JAMA. 2005;294(18):2305–2314. doi:10.1001/jama.294.18.2305
36. Lin J, Chen L, Jiang W, Zhang H, Shi Y, Cai W. Rapid detection of low-level HeLa cell contamination in cell culture using nested PCR. J Cell Mol Med. 2019;23(1):227–236. doi:10.1111/jcmm.13923
37. Pakyz AL, Moczygemba LR, VanderWielen LM, Edmond MB, Stevens MP, Kuzel AJ. Facilitators and barriers to implementing antimicrobial stewardship strategies: results from a qualitative study. Am J Infect Control. 2014;42(10 Suppl):S257–S263. doi:10.1016/j.ajic.2014.04.023
38. Burke JP. Antibiotic resistance–squeezing the balloon? JAMA. 1998;280(14):1270–1271. doi:10.1001/jama.280.14.1270
39. WHO [Website on the Internet]. Global Antimicrobial Resistance and Use Surveillance System. Geneva; 2015. Available from: https://www.who.int/initiatives/glass.
40. Hoff BM, Ford DC, Ince D, et al. Implementation of a mobile clinical decision support application to augment local antimicrobial stewardship. J Pathol Inform. 2018;9:10. doi:10.4103/jpi.jpi_77_17
41. Ohl CA, Luther VP. Antimicrobial stewardship for inpatient facilities. J Hosp Med. 2011;6(Suppl 1):S4–S15. doi:10.1002/jhm.881
42. MacDougall C, Polk RE. Antimicrobial stewardship programs in health care systems. Clin Microbiol Rev. 2005;18(4):638–656. doi:10.1128/CMR.18.4.638-656.2005
43. Walia K, Ohri VC, Madhumathi J, Ramasubramanian V. Policy document on antimicrobial stewardship practices in India. Indian J Med Res. 2019;149(2):180–184. doi:10.4103/ijmr.IJMR_147_18
44. Du M. Effect of information technology on management of reasonable use of antibiotics in four years. Chin J Nosocomiology. 2016;26(18):4.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Investigating Knowledge of Antibiotics, Antimicrobial Resistance and Antimicrobial Stewardship Concepts Among Final Year Undergraduate Pharmacy Students in Northern Nigeria
Abdu-Aguye SN, Barde KG, Yusuf H, Lawal BK, Shehu A, Mohammed E
Integrated Pharmacy Research and Practice 2022, 11:187-195
Published Date: 23 December 2022
Reflections on Drivers for the Emergence and Spread of Antimicrobial Resistant Bacteria Detected from Chickens reared on Commercial Layer Farms in Mukono District, Uganda
Kakooza S, Tayebwa DS, Njalira KR, Kayaga EB, Asiimwe I, Komugisha M, Wanyana M, Kisekka R, Kyabarongo A, Kiryabwire DH, Nabatta E, Eneku W
Veterinary Medicine: Research and Reports 2023, 14:209-219
Published Date: 6 December 2023
Healthcare Professionals’ Knowledge and Attitudes Toward Antimicrobial Stewardship Programs in Aseer, Saudi Arabia: A Cross-Sectional Study
Bahamdan AK, Alavudeen SS, Bahamdan GK, Bahamdan KA, Asiri SMA, Alshahrani NAM, Abdulziz Alqahtani S, Ibrahim ARN
Risk Management and Healthcare Policy 2025, 18:855-867
Published Date: 12 March 2025
Healthcare Workers’ Knowledge, Awareness, and Practices Regarding Antimicrobial Use, Resistance, and Stewardship in Saudi Arabia
Abdallah MS, Al Meanazel OT, Alruwaili MM, AlRasheed HA
Infection and Drug Resistance 2025, 18:6035-6050
Published Date: 19 November 2025
Seven-Year Surveillance and AI-Based Forecasting of Antimicrobial Resistance in Pediatric Escherichia coli Infections in Northern China (2018–2024)
Chen Y, Song Z, Di R, Zhao Q, Liu J, Song H, Wang J, Chen Y
Infection and Drug Resistance 2026, 19:566930
Published Date: 9 January 2026