Back to Journals » Nature and Science of Sleep » Volume 17

Advances in Machine Learning Prediction Models for the Screening of Obstructive Sleep Apnea in Adults
Authors Li S ![]() , Huang J
, Huang J ![]() , Xiao Z, Fan C
, Xiao Z, Fan C ![]()
Received 17 March 2025
Accepted for publication 1 September 2025
Published 7 October 2025 Volume 2025:17 Pages 2575—2595
DOI https://doi.org/10.2147/NSS.S526631
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Valentina Alfonsi
Shiyuan Li,1,2,* Jiewei Huang,1,* Ziheng Xiao,1,2,* Chunmei Fan1
1The Clinical Laboratory Center of The Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian Province, People’s Republic of China; 2The Graduate School of Fujian Medical University, Fuzhou, Fujian Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunmei Fan, The Clinical Laboratory Center of The Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian Province, People’s Republic of China, Tel +8615906069575, Email [email protected]
Abstract: Obstructive sleep apnea (OSA) is a global health problem. Patients with OSA may experience the upper airway collapsing during sleep, resulting in decreased oxygen saturation and sleep disruption, which is characterized by hypoxemia and sleep fragmentation, thereby reducing sleep quality and harming quality of life. In addition, OSA is associated with the occurrence of a variety of systemic diseases, which brings a huge burden to public health. Therefore, timely diagnosis of OSA is crucial. Polysomnography (PSG) is the most accurate method for diagnosing OSA at present, which can be used to determine the severity of sleep apnea and to monitor therapeutic efficacy. However, the PSG is difficult to be popularized because of its cumbersome operation, patients’ non-compliance, and expensive medical expenses. Therefore, it is imperative to find a convenient and fast OSA diagnosis method. In recent years, the development of machine learning prediction models and their application in the medical field have provided a new method for OSA severity diagnosis, making it possible to identify OSA severities efficiently and accurately. The purpose of this paper is to review relevant research on machine learning prediction models for OSA severity diagnosis and to provide sleep specialists with recommendations for more effective early identification and diagnosis of OSA. In addition, the challenges faced by machine learning at the level of diagnostic applications are summarized and future trends are envisioned.
Keywords: obstructive sleep apnea, machine learning, prediction model, obesity
Introduction
Obstructive sleep apnea (OSA) is a sleep disorder characterized by recurrent partial or complete collapse of the upper airway during sleep, resulting in decreased or paused breathing, leading to decreased oxygen saturation and sleep fragmentation.1 According to the 2007 guidelines of the American Academy of Sleep Medicine (AASM), the Apnea-Hypopnea Index (AHI) is commonly used to assess the severity of OSA.2 As research in this field has progressed, it has become clear that OSA is not merely a respiratory disorder3 but a serious health issue.4–7 However, the number of people with OSA remains high worldwide. Studies have shown that nearly 1 billion adults aged 30–69 years suffer from OSA globally, with the number of people with moderate to severe OSA estimated to be close to 425 million.8 In recent years, despite increasing awareness of OSA, the overall population prevalence still ranges between 9% and 38%.9 This situation is largely due to the lack of public awareness of OSA disease and the lack of medical resources.
Currently, polysomnography (PSG) is the gold standard of diagnostic tests for OSA, and a typical nocturnal PSG examination collects a large number of biological signals through multiple channels, such as electroencephalogram, electrooculogram, nasal airflow, electromyography, electrocardiogram (ECG), respiratory force, and blood oxygenation.10 The AASM emphasized the decisive role of PSG in the diagnosis of OSA in adults in its 2017 Clinical Practice Guidelines for Diagnostic Tests in Adults.11 However, the practical application of PSG has problems such as high cost, cumbersome operation, and high environmental requirements, so it is not realistic to use PSG screening to evaluate all suspected OSA patients. Scholars such as Cagle J L have suggested that Home Sleep Apnea Testing (HSAT) may be a cost- and time-saving screening tool for OSA.12 Currently, screening tools such as the Berlin questionnaire (BQ), STOP-bang questionnaire (SBQ), and Epworth sleepiness scale (ESS) have been widely used for the diagnosis of OSA. Among them, the SBQ has a higher diagnostic accuracy than portable PSG monitoring.13 The questionnaire meets the need for extensive screening, however, in practical application, it suffers from high subjectivity, recall bias, observation difficulties, high reading volume, and low accuracy.14 It can be seen that portable PSG tests and questionnaire screening tools also have their limitations in practical applications.
In recent years, with the advancement and development of machine learning (ML), the application of ML in medicine for prevention, early diagnosis, and treatment has gone beyond the theoretical realm and become a reality.15 Disease prediction and, in a broader context, medical informatics have received a great deal of attention from scholars, and research related to disease prediction models involving ML algorithms has proliferated.16
Many studies have focused on solving medical problems, especially disease diagnosis, through ML. There have been many studies in several medical fields to solve the problem of disease prediction or severity detection through ML methods, such as oncology, diabetes, heart disease, chronic kidney disease, Parkinson’s disease, and dermatology.17 At the same time, scholars have focused on research related to the realization of OSA severity diagnosis by conducting ML. The American Academy of Sleep Medicine guidelines suggest that clinical prediction algorithms can be used to screen patients with OSA.11 Currently, there have been a number of studies to realize OSA severity diagnosis by developing ML prediction models. The use of ML to develop disease prediction models mainly consists of the following three steps [Figure 1]: first, screening out possible predictors based on existing data; second, selecting appropriate ML algorithms for prediction models building and validation based on data characteristics and predictor characteristics; and finally, judging whether the prediction model achieves the modeling purpose as well as the desired efficacy based on a variety of evaluation metrics. Next, this paper will focus on these three topics to develop a review of the research progress of ML in adult OSA severity diagnosis.
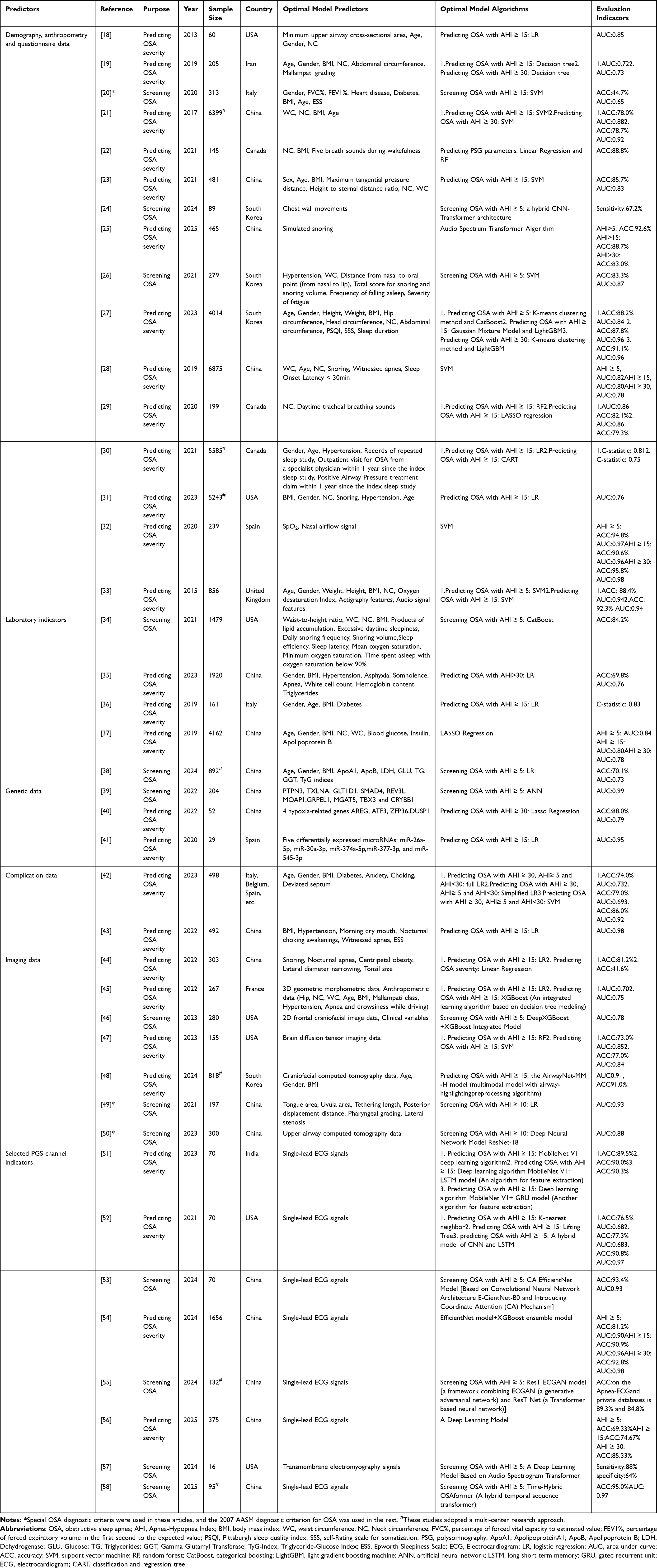 |
Table 1 Overview of Commonly Used Algorithms and Evaluation Metrics for Machine Learning Prediction Models of Obstructive Sleep Apnea |
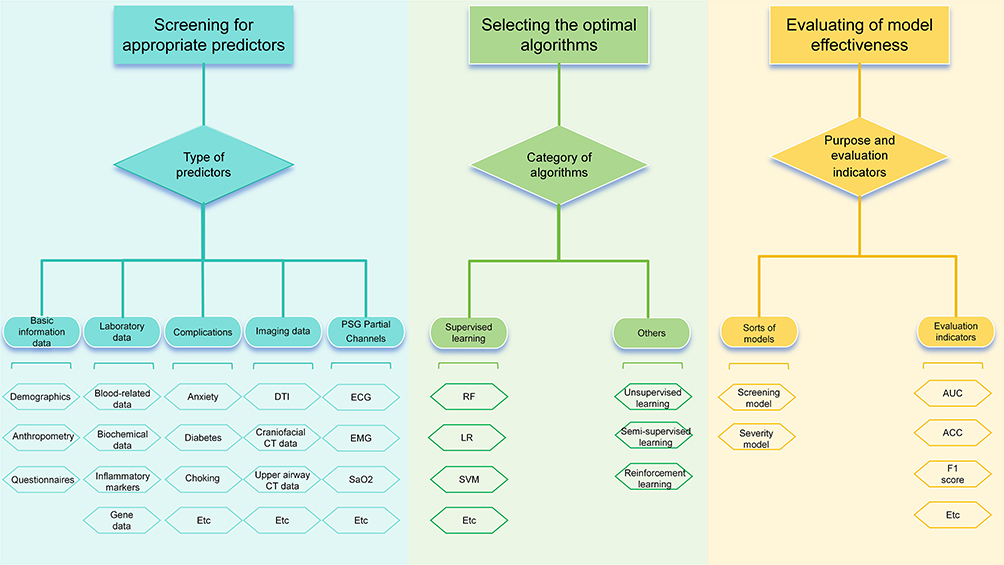 |
Figure 1 The main steps to building machine learning prediction models of obstructive sleep apnea. Abbreviations: DTI, diffusion tensor imaging; CT, computed tomography; ECG, electrocardiogram; EMG, electromyography; SaO2, blood oxygen saturation; RF, random forest; LR, logistic regression; SVM, support vector machine; K-Means, k-means clustering algorithm; GMM, gaussian mixture model; DBSCAN, density-based spatial clustering of applications with noise; AUC, area under curve; ACC, accuracy. |
Predictors Commonly Used in OSA Prediction Models
An important part for the development of any prediction model is to identify the characteristics used in the study, which are often referred to as predictors in statistics. Predictors are factors or variables, either quantitative or qualitative, that are used in predictive analysis to predict the target variable. Predictors are used to build prediction models to predict future values of the target variable. Predictors for OSA cover a wide range of areas, and choosing the right predictors is critical to building accurate prediction models. Given the rapid development and evolution of technology and algorithms, this review only searched PubMed for studies related to OSA prediction models published in the past decade and only included literature that successfully constructed models. The characteristics of each study and specific predictive factors are shown in Table 1.
Basic Information Data: Demographics, Anthropometry and Questionnaires
Demographic factors such as age, gender, ethnicity, geographic distribution, and socioeconomic status may influence the onset and manifestation of OSA; anthropometric indicators provide a simple and direct reflection of a patient’s physical condition;1 and questionnaires are an important tool to help physicians and researchers understand the symptoms and conditions of OSA in patients.13 In conclusion, demographics, anthropometrics, and questionnaires are important tools in the study and diagnosis of OSA and are often used as predictors in OSA prediction models.
Demographic Data
Age, gender, and other demographic data are commonly used in the construction of OSA prediction models. For example, Pamela N DeYoung et al used anthropometric data (end-expiratory upper airway minimum cross-sectional area, neck circumference) combined with demographic data (age, gender) to establish a prediction model that distinguishes between mild and severe OSA.18 Babak Amra et al used age and demographic indicators such as BMI, Mallampati index, and neck circumference to predict moderate to severe OSA.19 Corrado Mencar et al used demographic characteristics, spirometry, gas exchange (PaO2, PaCO2), and symptoms (ESS, snoring, etc.) for model development.20 They all achieved good predictive performance, with AUC values greater than 0.6.
Anthropometric Data
Adding anthropometric data to demographic data or using anthropometric data alone can also build an OSA prediction model with good performance. Wen-Te Liu et al developed a prediction model for the severity of OSA based on three anthropometric characteristics (neck circumference, waist circumference, and body mass index) and age.21 Ahmed Elwali et al predicted PSG-related parameters using five respiratory sounds during wakefulness with anthropometric characteristics.22 Liu Zhang et al conducted a cross-sectional study in a Chinese population and developed a sex-age-BMI-maximum incisor spacing-height to sternal distance ratio-neck and waist circumference (SABIHC2) model based on demographic and anthropometric data.23 In a prospective cohort study, Jae Won Choi et al successfully developed OSA dichotomous and quaternary prediction models using a contactless dual-radar approach to capture the participants’ chest movement and body movement signals.24 The AUC of the above models all reached 0.7, demonstrating the significant value of anthropometric data in OSA prediction. It is worth mentioning that in 2025, Chinese scholars Fang Lucheng et al established a prediction model using only simulated snoring data, and achieved an astonishing AUC of 0.926 in OSA screening.25
Questionnaire Data
Although survey questionnaires are inherently subjective, combining questionnaire data with objective indicators such as demographic and anthropometric data can also be used to construct effective predictive models. Young Jae Kim et al established an OSA prediction model using anthropometric data (waist circumference, length between the nasolabial muscle and oral muscle) and BQ questionnaire data, but the ratio of OSA patients to non-OSA patients was 3:1, and the data set consisted of only 279 individuals, which may have caused the model to be biased toward the OSA group.26 Increasing the amount of data should reduce this selection bias. A study by Han H et al involving 4,014 patients also confirmed this finding. They successfully established a predictive model using patient demographic data (gender, age), anthropometric data (height, weight, waist circumference, neck circumference, and hip circumference), and self-reported questionnaire results (ESS, Insomnia Severity Index), achieving an AUC of 0.96 in screening for severe OSA.27
Summary
Demographics, anthropometrics and questionnaires, which are characterized by low difficulty and low cost of acquisition, are common predictors of OSA prediction models. Gender, age, neck circumference, and BMI are the most commonly used indicators. In the future, if these indicators can be combined to build a model, it may achieve good predictive performance. Combined with simple machine learning algorithms, it may play a significant role in OSA home self-testing.
Laboratory Indicators
In recent years, cell biology research on OSA has made great progress, and some biomarkers of inflammation, oxidative stress, sympathetic activation, and metabolic activity, such as interleukin-6 (IL-6), nitric oxide (NO), cysteine, and apolipoproteins, have been identified,59,60 etc. In addition, a series of complications accompany OSA in the process of progression, which cause abnormalities in various indicators of the body, which are further reflected in the abnormalities of laboratory test indicators.
Blood-Related Indicators
Jayroop Ramesh et al used data from electronic health records, including laboratory blood reports, for the prediction of OSA.34 Yanqing Ye et al developed and validated a feasible clinical prediction model based on blood biochemical indicators such as white blood cell counts ≥9.5 × 109 /L and hemoglobin ≥175 g/L.35
Biochemical Indicators
Biochemical indicators can also be effectively applied to OSA prediction. Sofie Ahlin et al established a model for predicting OSA using predictive indicators such as blood glucose levels in biochemical tests. The model performed well in predicting severe OSA (C-statistic = 0.83), but no independent external validation group was established, and only internal validation was performed using the Bootstrap method, which may affect the external validity of the model.36 Huajun Xu et al used LASSO regression analysis to identify significant OSA predictors such as glucose, insulin, and apolipoprotein B, which can well identify individuals at risk for OSA.37 In a multicenter study in 2024, Huang et al established an OSA prediction model based on laboratory biochemical indicators such as γ-glutamyltransferase and triglycerides, combined with anthropological data such as age and body mass index, and validated it using an independent external test set, achieving good diagnostic results (AUC = 0.73).38
Inflammatory Markers
A review found that oxidative/nitrosative stress, increased pro-inflammatory markers, imbalanced NO production, and endothelial damage were significantly associated with OSA, and found that Continuous Positive Airway Pressure (CPAP) significantly ameliorated oxidative stress, inflammation, and endothelial dysfunction in patients with OSA.61 YifeiFang et al used ELISA to detect autoantibody levels of CRP, IL-6, IL-8, and TNF-α in the sera of 264 patients with OSA and 231 normal controls to explore the potential value of C-reactive protein, Interleukin-6, Interleukin-8, and tumor necrosis factor-α autoantibodies in the diagnosis of OSA and found that combining these four autoantibodies could improve the prediction of OSA very well.62 It can be seen that some inflammatory markers may be potential predictors in OSA prediction models, but there are currently few studies on prediction models using such indicators. Further research is needed to explore the value of such indicators in OSA prediction.
Gene Detection Index
Given the genetic factors associated with OSA, constructing a predictive model for OSA using genetic-related indicators is also a viable approach. Jie Zhu et al identified 360 significant differentially-expressed genes (DEGs) associated with OSA and 393 DEGs associated with CPAP, and selected the top 10 genes in terms of importance as the variables for developing models.39 Xiaofeng Wu et al evaluated the hypoxia-related significant DEGs for the diagnostic value of OSA and screened 16 DEGs to develop multiple OSA prediction models (AUCs>0.7).40 In addition, other researchers explored the link between Alzheimer’s disease patients and OSA and found that microRNA signaling in plasma was associated with the presence of OSA in AD patients. They observed a difference in the expression of 15 microRNAs in OSA and non-OSA patients, 10 of which were significantly correlated with the severity of OSA, and developed a prediction model based on this (AUC = 0.95).41 Except for the predictive model constructed by Xiaofeng Wu et al with an AUC of 0.79, the AUC values of all other studies exceeded 0.95, and only genetic factors related to OSA were included. This indicates that such indicators hold great promise for OSA prediction, and further exploration of the underlying mechanisms in this area is warranted in the future. With the future development of in vitro genetic diagnostic technologies, these factors may emerge as new diagnostic biomarkers. Except for the predictive model constructed by Xiaofeng Wu et al, which had an AUC of 0.79, the AUC values of the remaining studies all reached 0.95 or higher. Notably, these studies with higher AUC values only included genetic factors related to OSA. This suggests that, despite current differences in the construction of predictive models, genetic factors in OSA demonstrate significant potential in OSA prediction, implying the presence of important genetic mechanisms in the development of OSA. With the continuous advancement of in vitro genetic diagnostic technologies in the future, these genetic-related indicators are expected to emerge as new risk factors in the field of OSA, providing more precise and effective evidence for early diagnosis, risk assessment, and treatment decisions for OSA, while also opening up new research directions for exploring the genetic pathogenesis of OSA.
Summary
In summary, there are numerous laboratory indicators related to OSA prediction, ranging from common and easily accessible clinical blood routine, biochemical indicators and inflammatory indicators to biomarkers at the gene level. Prediction models that incorporate objective indicators are more difficult to generalize and obtain indicators than traditional models, but have better assessment capabilities.42 If the OSA prediction model based on objective laboratory indicators is widely adopted, it will not only reduce the subjective bias inherent in questionnaire-based prediction factors but may also address the shortcomings of inadequate medical facilities in primary care hospitals, enabling such facilities to conduct OSA screening. This would help reduce the rate of missed diagnoses and facilitate early diagnosis, treatment, and prevention.
Complications
There is a close relationship between OSA and complications. OSA may lead to a lack of oxygen in the body, which may trigger hypertension, arrhythmias, and coronary atherosclerotic heart disease.63 OSA may also lead to chronic pulmonogenic heart disease and respiratory failure, as well as ischemic or hemorrhagic encephalopathy.64 Untreated or inadequately treated OSA may lead to mental health problems such as depression or manic psychosis.65 At the same time, OSA may be complicated by diabetes.66 Therefore, comorbidities are also often included as predictors in relevant studies. Common comorbidities that are used as predictors in prediction models for OSA include obesity,36 diabetes,36,42 asphyxi,35,42,43 mood disorders,42 and hypertension.35,43
Imaging Data
Craniofacial structures are one of the important factors in the development of OSA. In patients with OSA, most of them have abnormalities of craniofacial structures, such as nasal stenosis, oral stenosis, and tonsillar hypertrophy, etc. These factors may lead to the obstruction of the airway during sleep, and may also affect the quality of sleep, which may aggravate the symptoms of OSA.67–69 Therefore, imaging data that focus on craniofacial structures are also often used as predictors in OSA prediction models.
Shuai He et al developed a logistic regression prediction model (AUC = 0.90) based on upper airway structural imaging data incorporating tongue area, uvula area, tethering length, and posterior tilt distance in combination with general demographic features.49 In addition, this researcher also used imaging anthropometrics data between the tonsils and the airway, and the palatopharyngeal arch and the tongue diameter for modeling, and achieved better prediction results.44 Fabrice Monna et al used 3D maxillofacial models for ML modeling and found that adding anthropometric data further improved the AUC. However, the study was limited to adult Caucasian males and excluded obese patients, which may have introduced selection bias.45 Ziyu Su et al proposed a DeepXGBoost model based on two-dimensional frontal craniofacial images, which performed well in predicting the severity of OSA, with an average AUC value of 0.78, significantly better than the traditional STOP-BANG questionnaire (AUC of 0.52).46 Min-Jung Kim et al developed a feature-based knowledge extraction OSA diagnostic model based on lateral cephalometric slices to avoid the effects caused by modal differences.70 Another researcher redeveloped the patient’s Computed Tomography (CT) image into 3 types (skeletal structure, external skin structure, and airway structure) and captured the redevelopment model in 6 directions (anterior, posterior, parietal, basal, left lateral plane, and right lateral plane) to achieve better predictive efficacy.50 As research continues, imaging data other than craniofacial structures have also been incorporated as predictors in OSA prediction models, Bo Pang et al proposed brain diffusion tensor imaging (DTI) as a predictor, and developed a prediction model using RF and SVM, both of which achieved good predictive efficacy [AUC(RF) = 0.85, AUC(SVM) = 0.84] and can be used for OSA screening in specific populations.47 In 2024, Kim et al developed a multimodal deep learning model based on sinus CT data combined with clinical data (age, gender, BMI, etc)., which also demonstrated excellent performance in assessing the severity of OSA (AUC = 0.91).48
Overall, most current studies on model development for imaging data are single-center studies with limited sample sizes. Only one study conducted in South Korea was multi-center and included a larger sample size (n=1018), which may introduce statistical bias in the results. This may be due to the difficulty in obtaining imaging data, the high hardware requirements, and the complex data processing procedures involved. The overall predictive performance for OSA is good, with AUC values reaching approximately 0.8. However, multicenter, large-sample studies can achieve superior predictive performance, such as Kim et al’s model with an AUC of 0.9156. Future research should focus on large-sample data studies.
PSG Partial Channels
Typical nocturnal PSG examination contains multiple channels to collect a large number of biological signals, scholars in related fields try to use one of the multiple channels of PSG as a predictor of OSA severity and combine other predictors to complete the task of OSA severity prediction through ML modeling, to achieve the prediction efficacy similar to that of PSG, with a view to realizing the usability and popularization of OSA prediction and diagnostic technology.
Prashant Hemrajani et al designed various ML algorithms using single lead signals such as ECG, oxygen saturation, etc., all of which achieved more than 90% accuracy and they developed a wearable device for monitoring ECG signals, which made the prediction of OSA more convenient.51 A similar study was done by Alaa Sheta et al who proposed a computer-aided diagnostic system for the automatic diagnosis of apnea events based on ECG, which achieved an accuracy of 86.25% in the validation phase.52 Yuxing Lin et al used wavelet transform to convert 1D ECG signal into 2D time-frequency image for the development of OSA prediction model, and the accuracy and AUC were higher than 90% when using the Dice loss function for training.53 And MengHsuan Liu et al also achieved excellent results by converting a single-lead ECG signal into a spectrogram to develop OSA prediction model, which showed good generalization ability (AUC=0.944) on the PhysioNet dataset.54 Zhiya Wang et al developed an OSA prediction framework using electrocardiograms (ECG), which was developed based on deep learning techniques combined with Effective Connectivity Networks, and it showed good generalization ability in cross-database testing.55 Yitong Zhang et al also utilized single-lead ECG signals to build a deep learning model, and the accuracy of each ECG signal can reach 91.66% when validated in a public database.56 In addition to using ECG signals, some scholars have also used other PSG partial channel signals. For example, Ross Mandeville et al developed an OSA diagnostic model based on transmembrane EMG data, which achieved better results in distinguishing between control, neurogenic and sleep apnea patients.57 Because it is difficult to extract single-lead ECG information by ML technology alone, Lingxuan Hou et al developed a hybrid OSA prediction model based on a hybrid architecture of dilated convolutional and long- and short-term memory neural networks combined with a multiscale feature fusion strategy to improve the extraction of ECG signals, which was shown to be effective in improving the accuracy of OSA diagnosis.58
It is worth noting that most of the above studies using ECG data have utilized the same public database. As the complexity of the algorithms and computational capabilities improve, the overall accuracy and AUC of the models have also increased, indicating that there is still significant room for development in model algorithms. In the future, it is anticipated that more precise predictive models based on ECG data can be constructed. However, this also increases the difficulty of model translation and implementation, as improvements in model performance rely on increased computational resources during training and inference processes, and higher complexity can lead to reduced interpretability. Similar to imaging-based predictive factors, most studies have employed small sample sizes; only one study from Taiwan in 2024 included a larger sample size (n=1,656). This suggests that future research could leverage larger sample sizes to develop more scientifically sound and reliable predictive models.
Commonly Used Machine Learning Algorithms in OSA Prediction
As early as the 1950s, Arthur Samuel used the term “machine learning”, defined as “the field of study that gives computers the ability to learn without being explicitly programmed”71 The main types of ML are supervised learning and unsupervised learning, in addition to semi-supervised learning and reinforcement learning.72
Supervised learning is most commonly used to solve classification tasks and regression tasks.73,74 Common supervised learning algorithms are decision trees, random forests, support vector machines, plain Bayes, artificial neural networks, etc.75,76 The OSA prediction models included in this paper were mostly constructed using the above algorithms for classification. For example, Zhang L et al used SVM to construct a machine learning model, which achieved good predictive performance in predicting moderate and severe OSA, with AUC values of 0.88 and 0.92, respectively.21 Unsupervised learning is most commonly used for clustering, dimensionality reduction, density estimation, feature learning, finding association rules, anomaly detection, etc.73 Some scholars also use unsupervised learning to process data before constructing OSA prediction models. For example, Han H et al used K-means clustering to process data before constructing OSA models, achieving AUC values of 0.84 and 0.96.27
Evaluation metrics for machine learning models have become increasingly sophisticated, and in classification problems, common evaluation metrics for models are AUROC, accuracy, F1 score, etc, while in regression problems, it is common to use mean squared error (MSE), mean absolute error (MAE), or the coefficient of determination (R2) to evaluate models.77 The algorithms and evaluation metrics that have been successfully used to develop OSA classification prediction models are shown in [Table 1].
The American Academy of Sleep Medicine (AASM) guidelines clearly state that “clinical prediction algorithms can be used in patients with suspected OSA in the sleep clinic, but should not necessarily be used as a substitute for PSG”, and that “in the non-sleep clinic setting, these tools may be more helpful in identifying patients at increased risk for OSA”11 Initial OSA screening for identifying OSA risk is valuable. In addition to questionnaire-based screening tools, decision-support models for OSA can utilize statistical machine-learning techniques to predict clinical outcomes, thereby facilitating clinical decision-making at a lower cost.78
Currently, most of the machine learning algorithms used to realize OSA rank prediction are supervised learning. Next, this paper will briefly expand the description of the basic application characteristics of commonly used machine learning algorithms in OSA prediction.
Logistic Regression
Logistic regression (LR) is computationally small, fast, with low storage resources,79 can solve multicollinearity problems,80 and is easy to understand and implement. However, when the feature space is large, the performance of LR is not very well, it can only deal with binary classification problems, it is easy to underfit, and the general accuracy is not high.79 LR is a powerful tool to analyze multiple explanatory variables at the same time, LR is used to obtain dominance ratios in the presence of multiple explanatory variables to solve dichotomous problems while reducing the effect of confounding factors.81
Linear Regression
Linear regression belongs to the more traditional models that include simple linear regression and multiple linear regression.82 Simple linear regression is used when the outcome variable is continuous and the researcher is trying to understand how a single independent variable correlates with the dependent variable; in real-world research, there are often multiple independent variables, and solving the multiple independent variable problem in a multiple linear regression model is relatively easy to implement and computationally simple.83 However, it cannot fit nonlinear data.
Random Forest
Random forest (RF) is one of the best-performing learning algorithms, RF easily adapts to nonlinearities in the data, and the algorithm is well suited for medium to large data sets,84 linear regression and logistic regression algorithms will not work when the number of independent variables is greater than the number of observations, whereas RF is effective because it does not use all the predictor variables at the same time.85 RF is extremely accurate, can effectively run on large datasets, is not prone to overfitting, has good resistance to noise, is fast to train, and is able to obtain an order of importance of the variables, but when it comes to a large number of decision trees in RF, the space and time required for training will be large, which will result in a slower model.86,87
Bayesian Method
The Bayesian method is based on the Bayesian principle and uses the knowledge of probability statistics to classify the sample dataset, and due to its solid mathematical foundation, the misclassification rate of the Bayesian method is very low.88 The Bayesian method is characterized by combining a priori and a posteriori probabilities ie, it avoids the subjective bias of using only a priori probabilities and the overfitting phenomenon of using sample information alone.89 Bayesian methods show high accuracy with large data sets, while the algorithm itself is relatively simple.90
K-Nearest Neighbor Method Algorithm
The K- Nearest Neighbor (KNN) algorithm can be used for nonlinear classification91 and is theoretically simple and easy to implement.92 The idea of the method supports adding new data directly to the dataset without retraining.93 The shortcomings of the method are the large computational effort, the large memory requirement, and the poor handling of sample imbalance.94
Decision Trees
Decision trees deal with interactions between features in a non-parametric way and it is easier to extract rules and have a faster runtime when testing datasets.95 However, they are prone to overfitting and ignore the interconnections of attributes in the dataset.96 Decision tree techniques are very similar to human reasoning and can be analyzed visually and are more comprehensible, so they are widely used for building classification models;97 the disadvantages of decision trees are that one drawback is the increased storage space and computational effort.98
XGBoost
XGBoost is a kind of many tree models integrated to form a very strong classifier, the algorithm adds regular terms to simplify the model and prevent the model from overfitting the situation, the model is fast, efficient, and has a strong generalization ability.99 However, the XGBoost algorithm requires more parameters to be adjusted, and it produces problems such as slow convergence and falling into local optimums.100
Support Vector Machines
Support Vector Machine (SVM) is a linear and nonlinear classification method proposed by Vapnik in 1995 based on statistical learning theory, which can be used for classification and regression.101 In recent years, SVM has been used to solve a variety of medical problems and has been widely used in the biomedical field, showing good performance.102–104 SVM is suitable for small sample size research, and the algorithm has low requirements for data distribution and wide applicability.105 Its advantage is that SVM maps nonlinear data to a high-dimensional space through the kernel function and develops the optimal hyperplane to realize the classification role, avoiding a large number of complex operations,106 which can classify and discriminate the nonlinear data, but the algorithm is sensitive to missing data, consumes a large amount of memory, and has little explanatory power.107
Artificial Neural Networks
Artificial neural networks (ANN) are mathematical tools that effectively simulate the structure of biological neural networks,108 and are used in many fields, such as achieving disease prediction, disease classification, and image analysis.109–111 ANN models have the characteristics of parallel distributed data storage and data processing, good fault tolerance, handling of high-level nonlinearities, strong adaptive ability, self-learning ability, etc.112 The main disadvantage of ANN is that it is not applicable to small samples and has high requirements for the selection of predictor variables.60
Choice of ML Algorithms
A review of ML methods for OSA found that the most common for developing models was logistic regression (35/63, 56%), followed by linear regression (16/63, 25%), support vector machines (9/63, 14%), neural networks (8/63, 13%), decision trees (8/63, 13%), Bayesian networks (4/63, 6%), and so on.113 It can be seen that logistic regression algorithms, which are computationally fast and can solve the multicollinearity problem, are more favored by a wide range of researchers in ML research for OSA diagnosis. This paper also conducted a statistical analysis of the included literature. Among the 41 included studies, a total of 58 OSA prediction models were constructed. In terms of the distribution of model numbers, single-model studies were the most numerous (28), followed by dual-model studies (9), while studies constructing three or more models were relatively few (4). In terms of algorithm selection, similar to Ferreira-Santos D’s study, the most popular algorithm was the regression model, followed closely by deep learning algorithms, and then SVM [Figure 2]. Considering sampling errors and the reliability of the results, this study only conducted a longitudinal analysis of algorithms with more than 10 models constructed over time to gain insight into algorithm selection trends. We found that traditional machine learning algorithms LR and SVM were quite popular after 2020, but in the past two years, they have gradually lost momentum compared to the rapid development of deep learning [Figure 3]. This trend may stem from the rapid advancement of algorithms, particularly the growing prominence of deep learning’s capabilities in handling complex, high-dimensional data. However, this does not imply that traditional algorithms will lack competitiveness in the future. Specifically, in research utilizing emerging and complex data sources such as electrocardiograms and imaging data, deep learning models are preferred due to their superior feature extraction and pattern recognition capabilities; whereas in studies based on relatively structured, low-dimensional data such as demographic characteristics, anthropometric indicators, and routine laboratory tests, traditional algorithms like regression models and SVM are more widely applied. As Eiseman et al analyzed a large sleep-related cardiovascular health study database and successfully constructed a model with good predictive performance using the SVM algorithm.114 Similarly, Wen-Chi Huang et al constructed a predictive model based on basic data such as gender and age of 6,875 Chinese patients suspected of having OSA, combined with the SVM algorithm, which also demonstrated excellent performance.28 Additionally, Farahnaz Hajipour et al used low-dimensional data such as neck circumference and respiratory sounds to build an OSA prediction model, finding that the RF algorithm achieved good predictive performance.29 In a large-scale study conducted in Canada, researchers used 32 health and wellness indicators for modeling, and the results indicated that LR achieved the expected predictive performance.30 When applied to relatively complex data such as electrocardiograms, deep learning algorithm models are more commonly used [Table 2].
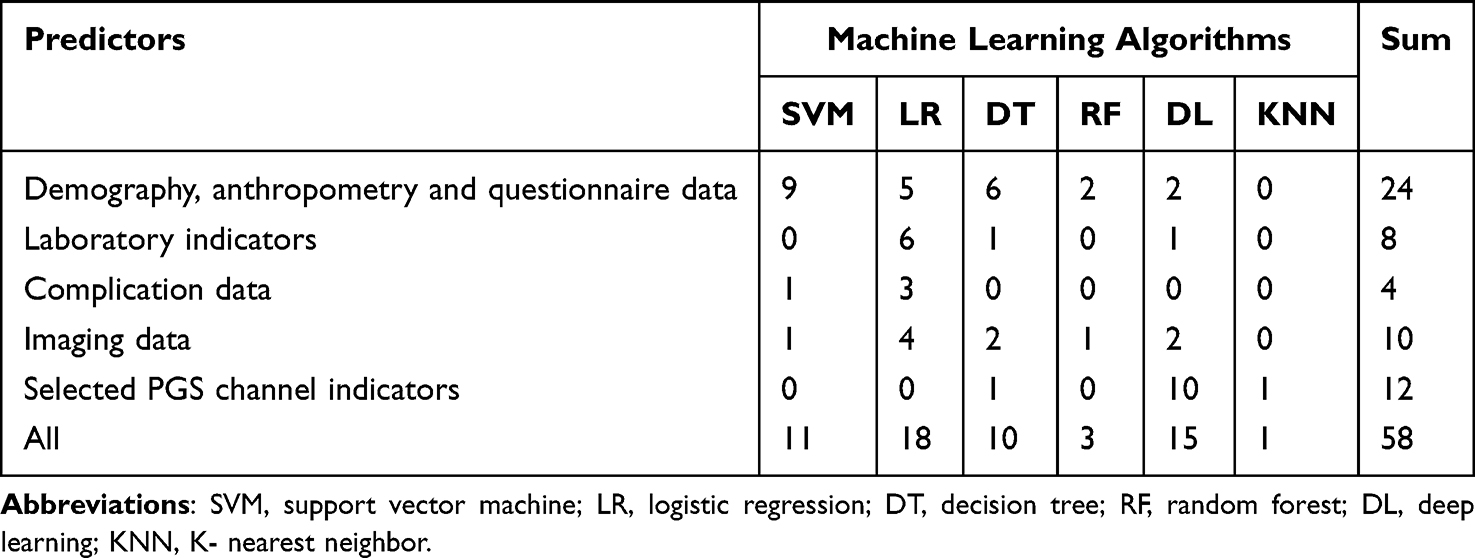 |
Table 2 Application Distribution of Machine Learning Algorithms in Various Predictive Variables |
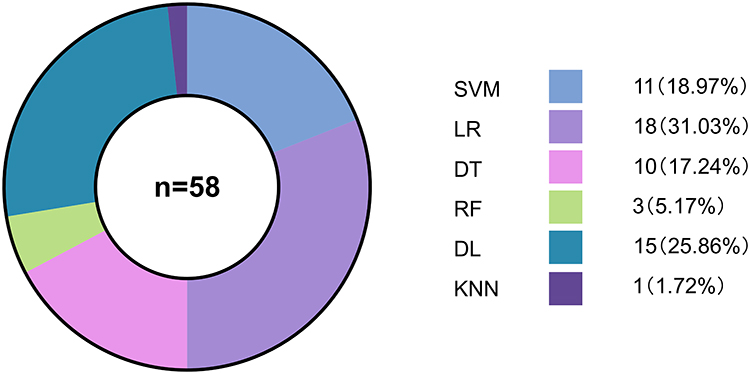 |
Figure 2 Summary of various algorithms used in the model. Abbreviations: SVM, support vector machine; LR, logistic regression; DT, decision tree; RF, random forest; DL, deep learning; KNN, K- nearest neighbor. |
 |
Figure 3 Comparison of the application trends of SVM, LR, and DL algorithms in the construction of obstructive sleep apnea prediction models from 2013 to 2024. Abbreviations: SVM, support vector machine; LR, logistic regression; DL, deep learning. Note: The number of articles for 2024 includes those published from January 2024 to March 2025. All other years are normal. |
The above analysis shows that current OSA prediction model research is showing a clear trend toward differentiation in algorithm selection. Traditional statistical models (such as regression) maintain their advantage in structured data scenarios, while deep learning is rapidly rising and occupying an important position in the processing of emerging complex data types. It can be seen that for studies with different data characteristics and model purposes, different ML algorithms are chosen to have different predictive efficacy and generalizability. In order to select the best model corresponding to the study, the current mainstream method is to develop multiple machine learning algorithm models first, and then select the best model by comparing the model evaluation indexes and then selecting the best model.
Purpose and Effectiveness of Forecasting Models
Early identification and treatment is the key to reducing the incidence of OSA, and rational intervention treatment in the early stages of OSA can help prevent its further development and avoid complications.115 ML provides early diagnosis and classification of OSA by incorporating corresponding predictors, analyzing variable correlations, and building prediction models with algorithmic fitting. Currently, machine learning prediction models for OSA are predominantly developed for two purposes: to screen for the presence of OSA and to predict its severity [Table 2].
OSA Screening Model
The current OSA screening model development process is typically designed based on different diagnostic thresholds. Most researchers tend to follow the AASM OSA diagnostic criteria and set AHI at 5 as the cutoff threshold [Table 1]. As demonstrated by Young Jae Kim et al, who employed the SVM algorithm and set the OSA diagnostic threshold to 5 for model construction, the best predictive performance was achieved, with sensitivity, specificity, and AUC values of 80.33%, 86.96%, and 0.87,26 respectively. A study conducted in 2025 that used deep learning algorithms to build a predictive model also set the OSA diagnostic threshold to 5 and achieved excellent performance, with an AUC of 0.97. Some scholars advocate using AHI=1049 or AHI=1520 as thresholds. He S et al used the logistic regression algorithm to construct an OSA prediction model based on photometric measurement with AHI≥10 as the threshold, achieving an AUC of 0.9049 at the optimal cutoff point. This suggests that most scholars consider AHI>5 as a more appropriate standard for early OSA screening and can achieve good predictive performance.
OSA Severity Prediction Model
The above articles have established better predictive screening models for OSA. However, all of these studies focused only on the diagnosis of OSA without taking the severity of OSA as an outcome variable, which for specific populations can directly or indirectly affect the course of their condition. Therefore, it is extremely important to assess the presence of OSA in the clinical setting and even to make a precise graded diagnosis. There are currently two main ways of developing OSA severity prediction models. The first method is to develop different models based on multiple AHI thresholds, each corresponding to a different degree of OSA severity. Another method is to predict AHI values through fitting, and then classify the severity based on the predicted AHI values.58
The logistic regression prediction model developed by Zerah-Lancner et al is currently the best method for screening out OSA, with a sensitivity value of 100% for predicting OSA with an AHI ≥15.116 Pona Park et al conducted a study on a large Korean population, using 11 heart rate variability variables and 14 feature indicators (such as age, gender, and body mass index) to establish a moderate-to-severe OSA risk model using LR. The model demonstrated good predictive performance at AHI values of 5, 15, and 30, with the best predictive performance at AHI = 30.117 Cheng-Yu Tsai et al also conducted a similar study, using anthropometric characteristics and water and fat levels in various body parts as feature indicators to establish two RF models for predicting moderate-to-severe OSA risk (AHI ≥15/AHI<15, accuracy rate 84.74%) and severe OSA risk (AHI ≥30/AHI<30, with an accuracy rate of 72.61%).118 Jiayan Huo et al developed an ML-derived questionnaire. They input the questionnaire answers of diagnosed patients into the model and screened them based on the correlation between feature factors and AHI, using AHI = 15 as the OSA classification criterion. They established the model using two LR classifiers, and the results showed that both classifiers had good efficacy in screening patients with moderate to severe OSA.31
In addition, some studies have focused on the translation and practical application of prediction models, with Daniel Álvarez et al using modeling of SpO2 and airflow parameters in homebound PSG patients for widespread routine screening for OSA in the home.32 Other researchers have signal-processed the model, ported it to Java along with the algorithm, and integrated it into the cell phone application SleepAp, providing a new, easy-to-use, low-cost, and widely available model that serves as a good replication.33
Limitation
Given the differences in evaluation metrics across various literature models, this study only summarized two overall evaluation metrics: AUC and ACC. It did not comprehensively summarize multi-dimensional metrics such as sensitivity, specificity, F1 score, calibration, and decision curves for each model. Future research should strive to comprehensively organize and present multi-dimensional evaluation results to more comprehensively reveal the strengths and weaknesses of previous models, providing precise references for the optimization and clinical translation of subsequent models.
Additionally, this paper only included studies related to OSA prediction models published in PubMed over the past decade, which limits the strength of the evidence and its clinical guidance value. Future work that follows the PRISMA-IPD or CHARMS guidelines, conducts systematic searches, strictly includes and excludes studies, and performs meta-analyses, is likely to generate higher-level evidence-based guidelines that truly serve the improvement and practical application of OSA prediction models.
Summary and Prospects
This paper discusses the research progress of ML in adult OSA diagnosis and reviews three aspects: common predictors of OSA prediction models, commonly used machine learning algorithms for OSA prediction models, and the purpose and efficacy of OSA prediction models. Because ML algorithms have powerful data processing capabilities, developing risk prediction models remains an important hotspot and direction in OSA diagnosis research.
At this stage, despite the proliferation of ML-related studies on OSA severity diagnosis, its application is not fully mature, mainly limited by conditions such as the lack of medical data, the lack of maturity of data processing and analyzing techniques, and inconsistent data standards. The prediction models derived from related studies generally have the following problems: first, most studies only use predictors from individual domains to build prediction models; however, OSA is also affected by various factors in multiple domains, and most of the studies have not comprehensively evaluated and selected predictors. Second, many of the studies were not externally validated, and even of those that were, most had geographic limitations of both internal and external validation and were not validated across ethnic groups and populations. Third, most of the studies are retrospective, leaving no way for the study design to be carried out with optimal protocols and limiting the ability to collect socioeconomic information, and there is value in integrating and analyzing socioeconomic factors to provide a more comprehensive understanding of sleep disorders and their correlates. Fourth, although many studies have developed OSA severity prediction models based on ML, few of these models have been translated in a rational way to be applied to real clinical practice. This may be due to the fact that different models use different predictive factors and are only applicable to specific clinical settings. On the other hand, it may be because the models only provide risk level results and cannot provide targeted indicator contributions and treatment plans.
A review of the evolution of machine learning in the diagnosis of adult OSA reveals that predictive factors have expanded from early demographic and anthropometric indicators to high-resolution imaging, electrocardiograms, and electromyograms, among other non-invasive data. Algorithms have also transitioned from traditional models to complex architectures centered on deep learning. Therefore, if the above issues can be resolved, it is recommended to divide the application scenarios into two categories based on this dual upgrade path: At the primary care/community screening level, low-cost, easily accessible low-dimensional data should remain the primary focus, with lightweight traditional algorithms employed and sensitivity deliberately optimized to minimize false negatives and achieve early detection. At the specialty/tertiary hospital level, high-dimensional data and deep learning should be leveraged to enhance overall performance while emphasizing specificity, reducing false positives, and aiming to replace polysomnography (PSG) examinations to minimize medical waste.
With the advancement of medical science and technology and the continuous development of hospital informatization, many medical big data platforms and databases have been put into development and application, which has pushed clinical medical care into the digital era. It will provide ideal and comprehensive data sources for the development and validation of the future OSA severity prediction model, and provide a basis for the cross-region validation of the model. On the other hand, big data analytics technology continues to innovate and machine learning algorithms continue to advance, which will provide better ML algorithms for future OSA severity prediction models, leading to better model performance. In addition, if the above points can be achieved while focusing on the contribution of each indicator to the results when developing predictive models and further inferring the disease pathways that may lead to such results, it should be possible to better assist doctors in their decision-making and thereby accelerate the advancement of medical transformation.
In summary, the application of machine learning in OSA prediction model development will be more fully demonstrated, better utilized, and more widely promoted.
Data Sharing Statement
Data sharing is not applicable to this review as no data were created or analysed in this study.
Author Contributions
Shiyuan LI: Investigation, Visualization, Methodology, Writing – Original Draft Preparation, Writing – review & editing.
Jiewei Huang: Investigation, Visualization, Methodology, Writing – Original Draft Preparation, Writing – review & editing.
Ziheng Xiao: Investigation, Visualization, Methodology, Writing – Original Draft Preparation, Writing – review & editing.
Chunmei Fan: Conceptualization, Investigation, Visualization, Methodology, Writing – Original Draft Preparation, Writing – review & editing, Supervision.
All authors have approved the version to be published; agreed on the journal to which the article will be submitted; and agreed to take responsibility for all aspects of this study.
Funding
No funding was received.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. Lancet. 2014;383(9918):736–747. doi:10.1016/S0140-6736(13)60734-5
2. Malhotra A, Ayappa I, Ayas N, et al. Metrics of sleep apnea severity: beyond the apnea-hypopnea index. Sleep. 2021;44(7):zsab030. doi:10.1093/sleep/zsab030
3. Léger D, Stepnowsky C. The economic and societal burden of excessive daytime sleepiness in patients with obstructive sleep apnea. Sleep Med Rev. 2020;51:101275. doi:10.1016/j.smrv.2020.101275
4. Nagayoshi M, Punjabi NM, Selvin E, et al. Obstructive sleep apnea and incident type 2 diabetes. Sleep Med. 2016;25:156–161. doi:10.1016/j.sleep.2016.05.009
5. Hui L, Benca R. The bidirectional relationship between obstructive sleep apnea and chronic kidney disease. J Stroke Cerebrovasc Dis. 2021;30(9):105652. doi:10.1016/j.jstrokecerebrovasdis.2021.105652
6. Santos M, Hofmann RJ. Ocular manifestations of obstructive sleep apnea. J Clin Sleep Med. 2017;13(11):1345–1348. doi:10.5664/jcsm.6812
7. Rajagopalan N. Obstructive sleep apnea: not just a sleep disorder. J Postgrad Med. 2011;57(2):168–175. doi:10.4103/0022-3859.81866
8. Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687–698. doi:10.1016/S2213-2600(19)30198-5
9. Senaratna CV, Perret JL, Lodge CJ, et al. Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med Rev. 2017;34:70–81. doi:10.1016/j.smrv.2016.07.002
10. Guo J, Xiao Y. New metrics from polysomnography: precision medicine for OSA interventions. Nat Sci Sleep. 2023;15:69–77. doi:10.2147/NSS.S400048
11. Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American academy of sleep medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479–504. doi:10.5664/jcsm.6506
12. Cagle JL, Young BD, Shih MC, et al. Portable sleep study device versus polysomnography: a meta-analysis. Otolaryngol Head Neck Surg. 2023;168(5):944–955. doi:10.1002/ohn.179
13. Chiu HY, Chen PY, Chuang LP, et al. Diagnostic accuracy of the Berlin questionnaire, STOP-BANG, STOP, and epworth sleepiness scale in detecting obstructive sleep apnea: a bivariate meta-analysis. Sleep Med Rev. 2017;36:57–70. doi:10.1016/j.smrv.2016.10.004
14. Gamaldo C, Buenaver L, Chernyshev O, et al. Evaluation of clinical tools to screen and assess for obstructive sleep apnea. J Clin Sleep Med. 2018;14(7):1239–1244. doi:10.5664/jcsm.7232
15. de Mattos PG, Santos BC, de Araujo RM, Ribeiro MH, de Moraes JL, Ribeiro AL. Machine learning in medicine: review and applicability. Arq Bras Cardiol. 2022;118(1):95–102. doi:10.36660/abc.20200596
16. Uddin S, Khan A, Hossain ME, Moni MA. Comparing different supervised machine learning algorithms for disease prediction. BMC Med Inform Decis Mak. 2019;19(1):281. doi:10.1186/s12911-019-1004-8
17. Jayatilake SMDAC, Ganegoda GU. Involvement of machine learning tools in healthcare decision making. J Healthc Eng. 2021;2021:6679512. doi:10.1155/2021/6679512
18. Deyoung PN, Bakker JP, Sands SA, et al. Acoustic pharyngometry measurement of minimal cross-sectional airway area is a significant independent predictor of moderate-to-severe obstructive sleep apnea. J Clin Sleep Med. 2013;9(11):1161–1164. doi:10.5664/jcsm.3158
19. Amra B, Pirpiran M, Soltaninejad F, Penzel T, Fietze I, Schoebel C. The prediction of obstructive sleep apnea severity based on anthropometric and Mallampati indices. J Res Med Sci. 2019;24(1):66. doi:10.4103/jrms.JRMS_653_18
20. Mencar C, Gallo C, Mantero M, et al. Application of machine learning to predict obstructive sleep apnea syndrome severity. Health Inform J. 2020;26(1):298–317. doi:10.1177/1460458218824725
21. Liu WT, Wu HT, Juang JN, et al. Prediction of the severity of obstructive sleep apnea by anthropometric features via support vector machine. PLoS One. 2017;12(5):e0176991. doi:10.1371/journal.pone.0176991
22. Elwali A, Moussavi Z. Predicting polysomnography parameters from anthropometric features and breathing sounds recorded during wakefulness. Diagnostics. 2021;11(5):905. doi:10.3390/diagnostics11050905
23. Zhang L, Yan YR, Li SQ, et al. Moderate to severe OSA screening based on support vector machine of the Chinese population faciocervical measurements dataset: a cross-sectional study. BMJ open. 2021;11(9):e048482. doi:10.1136/bmjopen-2020-048482
24. Choi JW, Koo DL, Kim DH, et al. A novel deep learning model for obstructive sleep apnea diagnosis: hybrid CNN-transformer approach for radar-based detection of apnea-hypopnea events. SLEEP. 2024;47(12):zsae184. doi:10.1093/sleep/zsae184
25. Fang L, Cai J, Huang Z, Tuohuti A, Chen X. Assessment of simulated snoring sounds with artificial intelligence for the diagnosis of obstructive sleep apnea. Sleep Med. 2025;125:100–107. doi:10.1016/j.sleep.2024.11.018
26. Kim YJ, Jeon JS, Cho SE, Kim KG, Kang SG. Prediction models for obstructive sleep apnea in Korean adults using machine learning techniques. Diagnostics. 2021;11(4):612. doi:10.3390/diagnostics11040612
27. Han H, Oh J. Application of various machine learning techniques to predict obstructive sleep apnea syndrome severity. Sci Rep. 2023;13(1):6379. doi:10.1038/s41598-023-33170-7
28. Huang WC, Lee PL, Liu YT, Chiang AA, Lai F. Support vector machine prediction of obstructive sleep apnea in a large-scale Chinese clinical sample. Sleep. 2020;43(7):zsz295. doi:10.1093/sleep/zsz295
29. Hajipour F, Jozani MJ, Moussavi Z. A comparison of regularized logistic regression and random forest machine learning models for daytime diagnosis of obstructive sleep apnea. Med Biol Eng Comput. 2020;58(10):2517–2529. doi:10.1007/s11517-020-02206-9
30. Kendzerska T, Van Walraven C, McIsaac DI, et al. Case-ascertainment models to identify adults with obstructive sleep apnea using health administrative data: internal and external validation. CLEP. 2021;13:453–467. doi:10.2147/CLEP.S308852
31. Huo J, Quan SF, Roveda J, Li A. BASH-GN: a new machine learning–derived questionnaire for screening obstructive sleep apnea. Sleep Breath. 2023;27(2):449–457. doi:10.1007/s11325-022-02629-8
32. Álvarez D, Cerezo-Hernández A, Crespo A, et al. A machine learning-based test for adult sleep apnoea screening at home using oximetry and airflow. Sci Rep. 2020;10(1):5332. doi:10.1038/s41598-020-62223-4
33. Behar J, Roebuck A, Shahid M, et al. SleepAp: an automated obstructive sleep apnoea screening application for smartphones. IEEE J Biomed Health Inform. 2015;19(1):325–331. doi:10.1109/JBHI.2014.2307913
34. Ramesh J, Keeran N, Sagahyroon A, Aloul F. Towards validating the effectiveness of obstructive sleep apnea classification from electronic health records using machine learning. Healthcare. 2021;9(11):1450. doi:10.3390/healthcare9111450
35. Ye Y, Yan ZL, Huang Y, et al. A novel clinical tool to detect severe obstructive sleep apnea. Nat Sci Sleep. 2023;15:839–850. doi:10.2147/NSS.S418093
36. Ahlin S, Manco M, Panunzi S, et al. A new sensitive and accurate model to predict moderate to severe obstructive sleep apnea in patients with obesity. Medicine. 2019;98(32):e16687. doi:10.1097/MD.0000000000016687
37. Xu H, Zhao X, Shi Y, et al. Development and validation of a simple-to-use clinical nomogram for predicting obstructive sleep apnea. BMC Pulm Med. 2019;19(1):18. doi:10.1186/s12890-019-0782-1
38. Huang J, Zhuang J, Zheng H, et al. A machine learning prediction model of adult obstructive sleep apnea based on systematically evaluated common clinical biochemical indicators. Nat Sci Sleep. 2024;16:413–428. doi:10.2147/NSS.S453794
39. Zhu J, Sanford LD, Ren R, Zhang Y, Tang X. Multiple machine learning methods reveal key biomarkers of obstructive sleep apnea and continuous positive airway pressure treatment. Front Genet. 2022;13:927545. doi:10.3389/fgene.2022.927545
40. Wu X, Pan Z, Liu W, et al. The discovery, validation, and function of hypoxia-related gene biomarkers for obstructive sleep apnea. Front Med. 2022;9:813459. doi:10.3389/fmed.2022.813459
41. Targa A, Dakterzada F, Benítez ID, et al. Circulating MicroRNA profile associated with obstructive sleep apnea in Alzheimer’s disease. Mol Neurobiol. 2020;57(11):4363–4372. doi:10.1007/s12035-020-02031-z
42. Maniaci A, Riela PM, Iannella G, et al. Machine learning identification of obstructive sleep apnea severity through the patient clinical features: a retrospective study. Life. 2023;13(3):702. doi:10.3390/life13030702
43. Yan X, Wang L, Liang C, et al. Development and assessment of a risk prediction model for moderate-to-severe obstructive sleep apnea. Front Neurosci. 2022;16:936946. doi:10.3389/fnins.2022.936946
44. He S, Li Y, Xu W, Han D. Using clinical data to predict obstructive sleep apnea. J Thorac Dis. 2022;14(2):227–237. doi:10.21037/jtd-20-3139
45. Monna F, Ben Messaoud R, Navarro N, et al. Machine learning and geometric morphometrics to predict obstructive sleep apnea from 3D craniofacial scans. Sleep Med. 2022;95:76–83. doi:10.1016/j.sleep.2022.04.019
46. Su Z, Kumar S, Tavolara TE, Gurcan MN, Segal S, Niazi MKK. Predicting obstructive sleep apnea severity from craniofacial images using ensemble machine learning models. Proc SPIE Int Soc Opt Eng. 2023;12465:124652P. doi:10.1117/12.2654353
47. Pang B, Doshi S, Roy B, et al. Machine learning approach for obstructive sleep apnea screening using brain diffusion tensor imaging. J Sleep Res. 2023;32(1):e13729. doi:10.1111/jsr.13729
48. Kim JW, Lee K, Kim HJ, et al. Predicting obstructive sleep apnea based on computed tomography scans using deep learning models. Am J Respir Crit Care Med. 2024;210(2):211–221. doi:10.1164/rccm.202304-0767OC
49. He S, Li Y, Xu W, et al. The predictive value of photogrammetry for obstructive sleep apnea. J Clin Sleep Med. 2021;17(2):193–202. doi:10.5664/jcsm.8836
50. Zhang Z, Feng Y, Li Y, Zhao L, Wang X, Han D. Prediction of obstructive sleep apnea using deep learning in 3D craniofacial reconstruction. J Thorac Dis. 2023;15(1):90–100. doi:10.21037/jtd-22-734
51. Hemrajani P, Dhaka VS, Rani G, Shukla P, Bavirisetti DP. Efficient deep learning based hybrid model to detect obstructive sleep apnea. Sensors. 2023;23(10):4692. doi:10.3390/s23104692
52. Sheta A, Turabieh H, Thaher T, et al. Diagnosis of obstructive sleep apnea from ECG signals using machine learning and deep learning classifiers. Appl Sci. 2021;11(14):6622. doi:10.3390/app11146622
53. Lin Y, Zhang H, Wu W, Gao X, Chao F, Lin J. Wavelet transform and deep learning-based obstructive sleep apnea detection from single-lead ECG signals. Phys Eng Sci Med. 2024;47(1):119–133. doi:10.1007/s13246-023-01346-0
54. Liu MH, Chien SY, Wu YL, et al. EfficientNet-based machine learning architecture for sleep apnea identification in clinical single-lead ECG signal data sets. Biomed Eng Online. 2024;23(1):57. doi:10.1186/s12938-024-01252-w
55. Wang Z, Pan X, Mei Z, et al. ECGAN-assisted ResT-net based on fuzziness for OSA detection. IEEE Trans Biomed Eng. 2024;71(8):2518–2527. doi:10.1109/TBME.2024.3378508
56. Zhang Y, Shi Y, Su Y, et al. Detection and severity assessment of obstructive sleep apnea according to deep learning of single‐lead electrocardiogram signals. J Sleep Res. 2025;34(1):e14285. doi:10.1111/jsr.14285
57. Mandeville R, Sedghamiz H, Mansfield P, et al. Deep learning enhanced transmembranous electromyography in the diagnosis of sleep apnea. BMC Neurosci. 2024;25(1):80. doi:10.1186/s12868-024-00913-9
58. Hou L, Zhuang Y, Zhang H, et al. Time-hybrid OSAformer (THO): a hybrid temporal sequence transformer for accurate detection of obstructive sleep apnea via single-lead ECG signals. Comput Methods Programs Biomed. 2025;260:108558. doi:10.1016/j.cmpb.2024.108558
59. Ramasamy I. Recent advances in physiological lipoprotein metabolism. Clin Chem Lab Med. 2014;52(12):1695–1727. doi:10.1515/cclm-2013-0358
60. Bin W, fen FH, Ping H, Jing Z, yin YJ. Application of artificial neural network in prediction of severe hand-foo-mouth disease. Mod Prev Med. 2018;11(45):1921–1924+1947.
61. Orrù G, Storari M, Scano A, Piras V, Taibi R, Viscuso D. Obstructive sleep apnea, oxidative stress, inflammation and endothelial dysfunction-an overview of predictive laboratory biomarkers. Euro Rev Med Pharmacolog Sci. 2020;24(12):6939–48.
62. Fang Y, Su J, Zhang B. Autoantibodies of inflammatory cytokines as serum biomarkers in OSA patients. Clin Chim Acta. 2023;547:117399. doi:10.1016/j.cca.2023.117399
63. Chinese Medical Association Respiratory Disease Branch Sleep-Disordered Breathing Disease Working Group. Guidelines for the diagnosis and treatment of obstructive sleep apnea-hypopnea syndrome (draft). Chin J Intern Med. 2003;(08):69–72.
64. Binyu L, Shihan X, Yiwen L, et al. Causal associations between obstructive sleep apnea and cardiovascular diseases: a two-sample Mendelian randomized study. Chinese J of Evid Based Med. 2023;10(23):1137–1142.
65. Tong ZHOU, Ping XU. The research progress in obstructive sleep apnea syndrome and mental disorders. Medical Recapitulate. 2016;22:4470–4475.
66. R S, M B. Obstructive sleep apnea and diabetes: a state of the art review. Chest. 2017;152(5). doi:10.1016/j.chest.2017.05.009
67. Yuqin FAN, Lizhong LIU. Relationship between adult craniofacial structures and development of obstructive sleep apnea-hypopnea syndrome. J Clin Otorhinolaryngol Head Neck Surg. 2010;11(24):502–505.
68. Yan C, Yan ZX, Wei YX. Correlation study between obesity and upper airway form and craniofacial structure and severity in patients with obstructive sleep apnea syndrome. Guizhou Med J. 2010;2(34):103–107.
69. Liping H, Xuehui C, Xin H, Xuemei G. Craniofacial characteristics and influencing factors in patients with obstructive sleep apnea. Procee Nat Acad Conf Chin Sleep Res Soc. 2020;70–71. doi:10.26914/c.cnkihy.2020.017732
70. Kim MJ, Jeong J, Lee JW, et al. Screening obstructive sleep apnea patients via deep learning of knowledge distillation in the lateral cephalogram. Sci Rep. 2023;13(1):17788. doi:10.1038/s41598-023-42880-x
71. Kim YK, Na KS. Application of machine learning classification for structural brain MRI in mood disorders: critical review from a clinical perspective. Prog Neuropsychopharmacol Biol Psych. 2018;80(Pt B):71–80. doi:10.1016/j.pnpbp.2017.06.024
72. Choi RY, Coyner AS, Kalpathy-Cramer J, Chiang MF, Campbell JP. Introduction to machine learning, neural networks, and deep learning. Transl Vis Sci Technol. 2020;9(2):14. doi:10.1167/tvst.9.2.14
73. Sarker IH. Machine learning: algorithms, real-world applications and research directions. SN Comp Sci. 2021;2(3):160. doi:10.1007/s42979-021-00592-x
74. Kufel J, Bargieł-łączek K, Kocot S, et al. What is machine learning, artificial neural networks and deep learning?-examples of practical applications in medicine. Diagnostics. 2023;13(15):2582. doi:10.3390/diagnostics13152582
75. Awaysheh A, Wilcke J, Elvinger F, Rees L, Fan W, Zimmerman KL. Review of medical decision support and machine-learning methods. Veterinary Pathol. 2019;56(4):512–525. doi:10.1177/0300985819829524
76. J T, Jl G, Aj R. Supervised machine learning: a brief primer. Behavior Therapy. 2020;51(5). doi:10.1016/j.beth.2020.05.002
77. Handelman GS, Kok HK, Chandra RV, et al. Peering into the black box of artificial intelligence: evaluation metrics of machine learning methods. AJR Am J Roentgenol. 2019;212(1):38–43. doi:10.2214/AJR.18.20224
78. Bozkurt S, Bostanci A, Turhan M. Can statistical machine learning algorithms help for classification of obstructive sleep apnea severity to optimal utilization of polysomnography resources? Methods Inf Med. 2017;56(4):308–318. doi:10.3414/ME16-01-0084
79. Whitaker T, Beranger B, Sisson SA. Logistic regression models for aggregated data. J Comput Graph Stat. 2021;30(4):1049–1067. doi:10.1080/10618600.2021.1895816
80. Pourhoseingholi M, Mehrabi Y, Alavi-Majd H, Yavari P. Using latent variables in logistic regression to reduce multicollinearity, a case-control example: breast cancer risk factors. Italian J Public Health. 2024. doi:10.2427/5857
81. Sperandei S. Understanding logistic regression analysis. Biochem Med. 2014;24(1):12–18. doi:10.11613/BM.2014.003
82. Schober P, Vetter TR. Linear regression in medical research. Anesth Analg. 2021;132(1):108–109. doi:10.1213/ANE.0000000000005206
83. Kasza J, Wolfe R. Interpretation of commonly used statistical regression models. Respirology. 2014;19(1):14–21. doi:10.1111/resp.12221
84. Hu J, Szymczak S. A review on longitudinal data analysis with random forest. Brief Bioinform. 2023;24(2):bbad002. doi:10.1093/bib/bbad002
85. Schonlau M, Zou RY. The random forest algorithm for statistical learning. Stata J. 2020;20(1):3–29. doi:10.1177/1536867X20909688
86. Sarica A, Cerasa A, Quattrone A. Random forest algorithm for the classification of neuroimaging data in Alzheimer’s disease: a systematic review. Front Aging Neurosci. 2017;9:329. doi:10.3389/fnagi.2017.00329
87. Salman HA, Kalakech A, Steiti A. Random forest algorithm overview. Babylonian J Mach Learn. 2024;2024:69–79. doi:10.58496/bjml/2024/007
88. Goligher EC, Heath A, Harhay MO. Bayesian statistics for clinical research. Lancet. 2024;404(10457):1067–1076. doi:10.1016/S0140-6736(24)01295-9
89. Courey K, Wu F, Oswald F, Pedroza C. Dealing with small samples in disability research: do not fret, Bayesian analysis is here. Rehab Psychol. 2024;69(4):335–346. doi:10.1037/rep0000579
90. Jun Z, Wenbo H. Recent advances in bayesian machine learning. J Comp Res Develop. 2015;01(52):16–26.
91. Deng Z, Zhu X, Cheng D, Zong M, Zhang S. Efficient kNN classification algorithm for big data. Neurocomputing. 2016;195:143–148. doi:10.1016/j.neucom.2015.08.112
92. Zhang Z. Introduction to machine learning: k-nearest neighbors. Ann Transl Med. 2016;4(11):218. doi:10.21037/atm.2016.03.37
93. Gui Z, Sun S, Li R, et al. kNN-CLIP: retrieval enables training-free segmentation on continually expanding large vocabularies. ArXiv. 2024:
94. Zhang S. Challenges in KNN classification. IEEE Trans Knowl Data Eng. 2022;34(10):4663–4675. doi:10.1109/TKDE.2021.3049250
95. Wang X, Liu X, Pedrycz W, Zhang L. Fuzzy rule based decision trees. Pattern Recogn. 2015;48(1):50–59. doi:10.1016/j.patcog.2014.08.001
96. Smith S, McConnell S. The use of artificial neural networks and decision trees: implications for health-care research. Open Comp Sci. 2024;14(1):20220279. doi:10.1515/comp-2022-0279
97. Mienye ID, Jere N. A survey of decision trees: concepts, algorithms, and applications. IEEE Access. 2024;12:86716–86727. doi:10.1109/ACCESS.2024.3416838
98. Kotsiantis SB. Decision trees: a recent overview. Artif Intell Rev. 2013;39(4):261–283. doi:10.1007/s10462-011-9272-4
99. Junbo ZHANG, Chuan HE, Jian YAN, Fangyin WU, Wei MENG. Discussion on the applicability of XGBoost algorithm based on cross validation in prediction of rockburst intensity classification. Tunnel Construction. 2020;S1(40):247–253.
100. Chunfu Z, Song W, Yadong W, Yong W, Hongying Z. Diabetes risk prediction based on GA_Xgboost model. Comput Eng. 2020;03(46):315–320. doi:10.19678/j.issn.1000-3428.0054109
101. Cherkassky V. The nature of statistical learning theory~. IEEE Trans Neural Netw. 1997;8(6):1564. doi:10.1109/TNN.1997.641482
102. Zilong Z, Yingjian H, Tao O. Application value of random forest and support vector machine in diagnosing breast lesions by using ultrasonic image features. Chin J Health Statist. 2018;05(35):684–688.
103. Vijayarajeswari R, Parthasarathy P, Vivekanandan S, Basha AA. Classification of mammogram for early detection of breast cancer using SVM classifier and hough transform. Measurement. 2019;146:800–805. doi:10.1016/j.measurement.2019.05.083
104. Wang H, Tang ZR, Li W, et al. Prediction of the risk of C5 palsy after posterior laminectomy and fusion with cervical myelopathy using a support vector machine: an analysis of 184 consecutive patients. J Orthop Surg Res. 2021;16(1):332. doi:10.1186/s13018-021-02476-5
105. Li X, Dong S, Guo S, Zheng C. Applying support vector machines to a diagnostic classification model for polytomous attributes in small-sample contexts. Br J Math Stat Psychol. 2025;78(1):167–189. doi:10.1111/bmsp.12359
106. Wang H, Li W. Fast ramp fraction loss SVM classifier with low computational complexity for pattern classification. Neural Netwk. 2025;184:107087. doi:10.1016/j.neunet.2024.107087
107. Xie S, Ogden RT. Functional support vector machine. Biostatistics. 2024;25(4):1178–1194. doi:10.1093/biostatistics/kxae007
108. Hu X, Cammann H, Meyer HA, Miller K, Jung K, Stephan C. Artificial neural networks and prostate cancer--tools for diagnosis and management. Nat Rev Urol. 2013;10(3):174–182. doi:10.1038/nrurol.2013.9
109. Gu Y, Liang Z, Hagihira S. Use of multiple EEG features and artificial neural network to monitor the depth of anesthesia. Sensors. 2019;19(11):2499. doi:10.3390/s19112499
110. Jafari-Marandi R, Davarzani S, Soltanpour Gharibdousti M, Smith BK. An optimum ANN-based breast cancer diagnosis: bridging gaps between ANN learning and decision-making goals. Appl Soft Comput. 2018;72:108–120. doi:10.1016/j.asoc.2018.07.060
111. Yun MR, ze LH, Bai T, et al. Artificial neural network model for preoperative prediction of severe liver failure after hemihepatectomy in patients with hepatocellular carcinoma. Surgery. 2020;168(4):643–652. doi:10.1016/j.surg.2020.06.031
112. Naushad SM, Janaki Ramaiah M, Pavithrakumari M, et al. Artificial neural network-based exploration of gene-nutrient interactions in folate and xenobiotic metabolic pathways that modulate susceptibility to breast cancer. Gene. 2016;580(2):159–168. doi:10.1016/j.gene.2016.01.023
113. Ferreira-Santos D, Amorim P, Silva Martins T, Monteiro-Soares M, Pereira Rodrigues P. Enabling early obstructive sleep apnea diagnosis with machine learning: systematic review. J Med Internet Res. 2022;24(9):e39452. doi:10.2196/39452
114. Eiseman NA, Westover MB, Mietus JE, Thomas RJ, Bianchi MT. Classification algorithms for predicting sleepiness and sleep apnea severity. J Sleep Res. 2012;21(1):101–112. doi:10.1111/j.1365-2869.2011.00935.x
115. Kapoor M, Greenough G. Home sleep tests for obstructive sleep apnea (OSA). J Am Board Family Med. 2015;28(4):504–509. doi:10.3122/jabfm.2015.04.140266
116. Zerah-Lancner F, Lofaso F, D’Ortho MP, et al. Predictive value of pulmonary function parameters for sleep apnea syndrome. Am J Respir Crit Care Med. 2000;162(6):2208–2212. doi:10.1164/ajrccm.162.6.2002002
117. Park P, Kim JW. A classifying model of obstructive sleep apnea based on heart rate variability in a large Korean population. J Korean Med Sci. 2023;38(7):e49. doi:10.3346/jkms.2023.38.e49
118. Tsai CY, Huang HT, Cheng HC, et al. Screening for obstructive sleep apnea risk by using machine learning approaches and anthropometric features. Sensors. 2022;22(22):8630. doi:10.3390/s22228630
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Using Machine Learning Algorithms to Predict High-Risk Factors for Postoperative Delirium in Elderly Patients
Liu Y, Shen W, Tian Z
Clinical Interventions in Aging 2023, 18:157-168
Published Date: 8 February 2023
Ten-Year Multicenter Retrospective Study Utilizing Machine Learning Algorithms to Identify Patients at High Risk of Venous Thromboembolism After Radical Gastrectomy
Liu Y, Song C, Tian Z, Shen W
International Journal of General Medicine 2023, 16:1909-1925
Published Date: 18 May 2023
Development of Machine Learning Models for Predicting Osteoporosis in Patients with Type 2 Diabetes Mellitus—A Preliminary Study
Wu X, Zhai F, Chang A, Wei J, Guo Y, Zhang J
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1987-2003
Published Date: 30 June 2023
Prediction of the Risk of Bone Mineral Density Decrease in Type 2 Diabetes Mellitus Patients Based on Traditional Multivariate Logistic Regression and Machine Learning: A Preliminary Study
Zhang J, Xu Z, Fu Y, Chen L
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2885-2898
Published Date: 19 September 2023
Risk Prediction of Diabetes Progression Using Big Data Mining with Multifarious Physical Examination Indicators
Chen X, Zhou S, Yang L, Zhong Q, Liu H, Zhang Y, Yu H, Cai Y
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1249-1265
Published Date: 11 March 2024